 Hua Huang
Hua Huang Xiaomin Yu2
Xiaomin Yu2 Jumei Zeng
Jumei Zeng Yuqing Li
Yuqing Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oral. Health , 18 March 2025
Sec. Oral Infections and Microbes
Volume 6 - 2025 | https://doi.org/10.3389/froh.2025.1566355
This study aims to ameliorate the management of VAP in clinical practice and deliver more precise care in the ICU. Study selection using the appropriate critical appraisal tools was undertaken by three authors. This review provides an overview of empirical antibiotics, chlorhexidine, and povidone-iodine, which are currently commonly used in critical care. It also discusses oral medications and preparations that may be used to prevent and treat ICU ventilator-associated pneumonia, including new antibiotics, hydrogen peroxide solutions, sodium bicarbonate, octenidine, and oral herbal medicines. It also discusses ongoing research and potential applications, such as the antimicrobial effects of these agents in ICU oral hygiene. Pharmaceuticals and formulations used in oral hygiene are effective or have huge application potential in the prevention and treatment of VAP, but further research is needed to standardize oral health assessment and care practices to develop evidence-based personalized oral hygiene for critically ill patients.
Ventilator-associated pneumonia (VAP) is a pulmonary parenchymal infection that develops in patients admitted to intensive care unit (ICU) and subjected to invasive mechanical ventilation for a minimum of forty eight hours (1). VAP is cause by a range of microorganisms affecting the respiratory system, which include Gram-negative bacterial such as Klebsiella spp., Escherichia coli, and Pseudomonas aeruginosa, as well as Gram-positive bacterial such as Staphylococcus aureus, including methicillin-resistant S. aureus (MRSA) (2). The advances in molecular diagnostic methods, which are deepening the comprehension of VAP microbiology, recent investigations discovered the presence of Mycoplasma in the bronchial lavage of patients diagnosed with VAP (3). Future therapeutic approaches will focus more on these microorganisms to prevent and treat VAP thanks to the deepening the understanding of the microbiome (4). The pathogenic mechanism of VAP is shown in Figure 1.
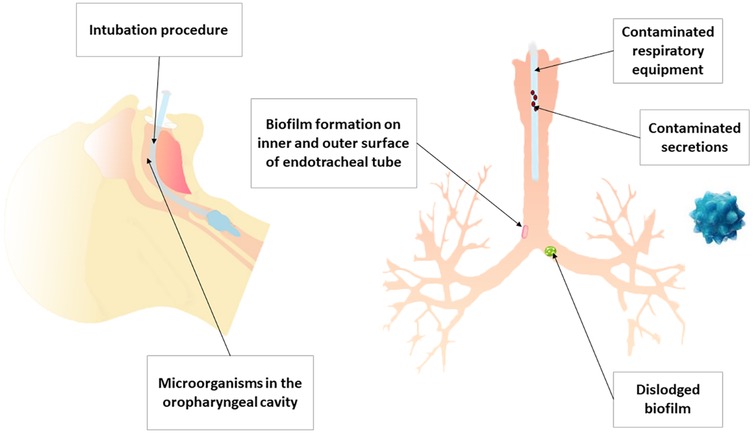
Figure 1. The pathogenic mechanism of VAP.
Endotracheal intubation represents a significant risk factor for VAP. VAP affects the body's airway defenses, hinders the ability to cough and clear mucus, and causes the accumulation of secretions containing bacteria above the inflatable cuff of the endotracheal tube that are aspirated (5), causing lower respiratory tract infections in ICU patients.
Previous studies indicated that dental plaque represents a significant reservoir for a variety of pathogens, since it contains a range of microorganisms associated with VAP (6). A study by Cindy L. Munro et al. (7) concluded that higher plaque scores increase the risk of VAP in more severely ill patients, especially those in the ICU. Therefore, the development of VAP may be reduced by a good and regular oral hygiene to prevent plaque accumulation and stimulate local oral immunity early in hospitalization (7, 8). Another study by Seok-Mo Heo et al. found that respiratory pathogens isolated from the lungs are often genetically indistinguishable from identical strains isolated from the oral cavity, suggesting that dental plaque is an important reservoir for respiratory pathogens in mechanically ventilated patients (9).
Numerous international organizations, such as the Centers for Disease Control and Prevention (CDC) and the American Association for Respiratory Care (AARC), promote the rigorous oral hygiene as a means of preventing VAP in patients undergoing mechanical ventilation (10). Figure 2 shows various suggested methods to avoid VAP.
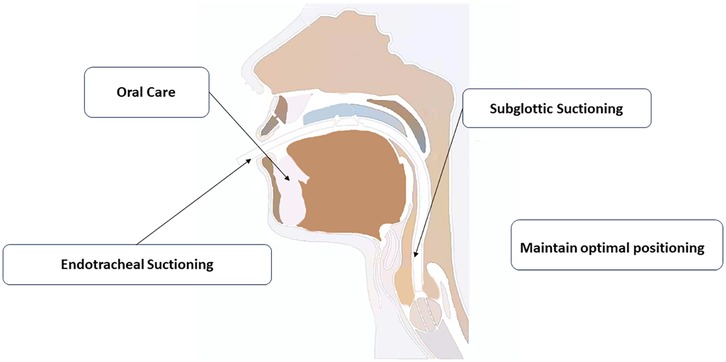
Figure 2. Various suggested methods to avoid VAP.
Empirical antibiotics are the main drugs for preventing ventilator-associated pneumonia, but due to their potential side effects and the risk of antibiotic resistance, they need to be used with caution. Therefore, research on new drugs for ICU oral care is imminent.
Oral hygiene medications possess antimicrobial properties, thus used to prevent and treat infections of the oral cavity. Several antimicrobial agents commonly used in oral care encompass chlorhexidine and povidone iodine. This review provides a list of medications. It particularly emphasizes strategies for the effective prevention and management of oral issues in individuals who are unable to care for their oral hygiene and explores the potential application of drugs currently under research or development for oral hygiene in the ICU.
References for this review were identified through searches of PubMed for articles published from January, 1964, to April, 2024, by use of the terms “VAP”, “ICU care”, “oral care”, “oral medication and formulation”, “antibiotics”, “chlorhexidine”, “octenidine”, “povidone iodine”, “sodium bicarbonate” and “H2O2”. We reviewed guidelines for the management of VAP published by Centers for Disease Control and Prevention (CDC) and the American Association for Respiratory Care (AARC). We added articles through searches of the authors’ personal files. We also reviewed relevant references cited in retrieved articles. Articles published in English, Japanese and Portuguese were included. Pre-defined inclusion criteria were used.
Antibiotic prophylaxis in VAP refers to the preventive administration of antibiotics to patients undergoing mechanical ventilation to reduce the incidence of this serious infection. The primary goal is to minimize the risk of VAP, particularly in high-risk populations, without significantly impacting mortality rates. Studies indicate that prophylactic antibiotics, especially when delivered via nebulization, can significantly lower VAP rates compared to control groups (11, 12). Compared with early empirical treatment, the use of prophylactic antibiotics is mainly aimed at reducing pathogen colonization and preventing the occurrence of VAP rather than treating existing infections (13).
Antibiotic prophylaxis in preventing VAP can be approached through systemic antibiotics, nebulized/inhaled antibiotics, and selective oropharyngeal decontamination (SOD). Each method has its commonly used agents and varying effectiveness. Systemic antibiotics, such as intravenous ampicillin-sulbactam, have shown efficacy in reducing VAP incidence, with a risk ratio (RR) of 0.62 in meta-analyses. However, these approaches do not significantly impact mortality rates or length of ICU stays (12). Nebulized antibiotics, particularly tobramycin and aminoglycosides, have demonstrated a significant reduction in VAP risk (RR of 0.69). The use of nebulized antibiotics was not associated with increased mortality or adverse events, making it a viable option for preventing VAP and the most interesting option for researchers (11, 14). SOD involves the use of topical antibiotics to reduce oropharyngeal colonization (15), though specific studies on its effectiveness compared to nebulized or systemic antibiotics are limited in the provided literature.
However, concerns about antimicrobial resistance (AMR) in the prevention of VAP are multifaceted, involving the need for effective infection control, judicious antibiotic use, and the development of preventive strategies. VAP is a significant concern in ICUs due to its association with high mortality rates and the frequent use of antibiotics, which can exacerbate AMR (16, 17). Long-term or extensive use of antibiotics, even when applied topically, may alter the local microbial ecology and selectively promote the growth of resistant strains, thereby increasing the risk of resistance. Its main mechanism includes antibiotic inactivation, that is, directly degrading the antibiotic or replacing the active group, destroying the structure of the antibiotic, thereby making the antibiotic lose its original function. Another mechanism is the cell efflux pump (18).
Besides, antibiotics induce adverse reactions such as diarrhea, nausea, vomiting, and allergic responses (19). While antibiotics are essential for reducing rates of VAP, their use needs careful consideration because of the above potential side effects and the risk of developing antibiotic resistance (20).
Chlorhexidine is a commonly used antiseptic agent in diverse healthcare environments, including ICU. It is effective against a wide range of bacteria, both Gram-positive and Gram-negative linked to VAP (21); thus, it has been incorporated into oral hygiene regimens for ICU patients in hospitals worldwide (22). Several international organizations, such as the American Thoracic Society and the European Society of Intensive Care Medicine, support the use of chlorhexidine for oral hygiene in mechanically ventilated patients as a part of a complete treatment set for preventing VAP (23).
The administered oral chlorhexidine in the interventions varies in concentrations from 0.12% to 2%, and is provided in solution or gel form (24). A study among many on the comprehensive analysis of existing research regarding the influence of chlorhexidine on VAP revealed that 0.12% chlorhexidine is effective in preventing VAP in patients who subjected to cardiac surgery (24). Moreover, two studies by Koeman et al. and Hua et al. (21, 25), indicated that the oral administration of chlorhexidine from 0.12% to 2% reduces the incidence of VAP among a diverse group of critically ill patients, being used in various medical fields. Concurrently, a meta-analysis revealed a 37% decrease in the risk of VAP associated with the use of chlorhexidine (0.02%, 0.12%, 0.2%) (26).
The development of resistance to antimicrobials is a significant and ongoing consequence in the use of chlorhexidine. A higher prevalence of chlorhexidine-resistant strains is present in the genera Enterobacter, Pseudomonas, Proteus, Providencia, and Enterococcus, especially Enterococcus faecalis (27). Chlorhexidine resistance is also present in multidrug-resistant strains, including Klebsiella pneumoniae. Several studies indicate that long-term exposure to chlorhexidine increases the probability of developing resistance to specific antibiotics (28, 29).
The predominant adverse effects associated with chlorhexidine mouthwash and gels are xerostomia, dysgeusia, alterations in tongue pigmentation, as well as calculus formation and extrinsic tooth discoloration after a prolonged use. Less frequently observed adverse effects include swelling of the parotid gland, sensation of a foreign body in the mouth, tongue pain, and desquamation of the oral mucosa (30). These effects are generally minor and reversible after stopping the use of this product (31). Chlorhexidine is banned in some countries due to cases of anaphylactic shock (32). Furthermore, an in vitro study demonstrated that chlorhexidine induces genotoxic and cytotoxic effects on human lymphocytes in a dose-dependent manner (33). Therefore, the risks of chlorhexidine should be taken into consideration to manage all relevant effects on the mouth.
Povidone-iodine is widely considered as one of the most effective antimicrobial agents in the reduction of the occurrence of respiratory infections, including VAP (34). It is effective against a wide spectrum of bacteria, including those frequently linked to VAP, and inhibits the development of biofilms on medical equipment (35).
In some countries, such as Japan, the use of chlorhexidine is restricted because of documented cases of anaphylactic shock; thus, povidone-iodine is preferred as an alternative substance (32). A randomized controlled study in Japan demonstrated that the topical administration of 10% povidone-iodine instead of 0.12% chlorhexidine for oral cleaning and irrigation effectively suppresses bacterial growth in the oropharyngeal fluid of mechanically ventilated patients without disturbing oral homeostasis (36). Another Japanese study found that the use of povidone-iodine mouthwash swabs, brushing teeth, and rinsing with 300 ml of acidic water reduces the risk of VAP in mechanically ventilated patients (37). A RCT study in France showed that the regular administration of povidone-iodine is an effective strategy to reduce the incidence of VAP in patients with traumatic brain injury (38).
However, a multicenter, randomized controlled trial did not find any evidence of the effect of povidone-iodine in preventing VAP; on the contrary, it increases the incidence of acute respiratory distress syndrome in patients with brain injury or cerebral hemorrhage (39). However, further research is recommended to investigate potential adverse effects considering the high possibility of bias in the included studies (40).
Hydrogen peroxide (H2O2) is a clear, colorless liquid with no odor. It is used in dentistry since the early 20th century, either alone or in conjunction with salts (41). The use of 3% H2O2 as a temporary oral debridement agent was approved by the FDA (42).
A study published in the Brazilian Journal of Infectious Diseases reported that individuals who used 3% H2O2 mouthwash twice daily experienced a 2.6-fold decrease in the risk of developing VAP in comparison to those who used saline mouthwash (43). Another study published in the journal of infection prevention reported that the incorporation of H2O2 mouthwash into a comprehensive VAP prevention system was linked to an evident decrease in VAP rates (44).
H2O2 also has some side effects. Of particular concern are the reports on the genotoxic effects of H2O2 in bacteria and mammalian cells. The prolonged use of 3% H2O2 in animal experiments results in a slight increase in the formation of precancerous lesions and tumors (45). Additional research is needed to confirm the long-term safety and effectiveness of H2O2 in the prevention of VAP. It is recommended to use caution when using it and to incorporate it as part of a comprehensive strategy to prevent VAP.
Sodium bicarbonate, commonly referred to as baking soda, has various uses in the oral cavity. It is known for its safety, minimal abrasiveness, and bactericidal properties, making it a patient-friendly option for mouthwash, and as a component in toothpaste and chewing gum. It can be used as a long-term treatment as an adjunct with virtually no side effects (46). As a result, sodium bicarbonate has a significant potential for application in the oral hygiene in the ICU to prevent VAP.
Sodium bicarbonate possesses bactericidal and neutralizing properties, making its use suitable as a mouthwash (47), decreasing the quantity of bacteria in the oral cavity. This action disrupts the adherence of bacteria to the tooth, consequently reducing plaque formation.
Toothpaste containing sodium bicarbonate possesses superior bactericidal activity compared to other toothpastes due to its safety, low cost, low abrasiveness, water solubility, buffering capacity, and compatibility with fluoride (48). Toothpastes containing sodium bicarbonate are effective in removing plaque and higher concentrations of sodium bicarbonate are associated with greater efficacy (49, 50). Another study indicated that baking soda toothpaste is more effective than those without baking soda. Antibacterial toothpaste is effective in removing plaque after just one brushing session and maintain significantly lower plaque levels during four weeks of twice-daily and unsupervised brushing (51). Toothpaste containing sodium bicarbonate effectively removes plaque before it irreversibly binds to the teeth, thus ensuring an environment for good oral health (52).
Nevertheless, individuals with hypertension and those adhering to a low-sodium diet should be careful when considering the use of sodium bicarbonate mouthwash (50). Further research is necessary to evaluate the concentration and duration needed for its bactericidal effect without causing harmful effects on the oral mucosa.
Octenidine(OCT) has lower systemic toxicity than chlorhexidine (53, 54), which may be due to the lack of amide and ester structures in its molecule (55). It has a broad range of antimicrobial activity, affecting Gram-positive bacteria, Gram-negative bacteria, Chlamydia, Mycoplasma and fungi (56).
A study indicated that 0.1% OCT is an effective antiplaque agent. Compared with placebo, octinoxate inhibited plaque formation by up to 93%, which is comparable to chlorhexidine (57). Another study showed that OCT 0.1% mouthwash inhibits plaque formation for more than 5 days. Therefore, it can be recommended when regular oral hygiene is temporarily impaired (58). Moreover, OCT can inhibit the colonization of Staphylococcus aureus and Pseudomonas aeruginosa on tracheotomy tubes and reduce the colonization and biofilm formation on the surface of polymer tracheotomy tubes, which has potential application value in the prevention and treatment of VAP (59).
Although the safety of OCT has been confirmed by research, potential risks still exist. The use of OCT solution may penetrate wounds or skin and cause chronic inflammation (60, 61). However, these findings have limitations and need to be verified by more precise studies.
To improve patient outcomes through continued research into ventilator-associated pneumonia, attention should be focused on the development and improvement of diagnostic methods and therapeutic drugs. More specific diagnostic methods are needed to select the appropriate antimicrobial drugs for specific pathogens. It is also crucial to further study the mechanisms of antibiotic resistance and specific characteristics of oral microorganisms. This could help address multi-drug resistance of oral microorganisms, thus improving the effectiveness of oral medications in the treatment of VAP.
In terms of diagnosis, point-of-care (POCT) tools are diagnostic tests that can be used at or near the bedside, with delays ranging from minutes to hours. The use of POCTs for the diagnosis of VAP allows for faster diagnosis and adjustment of antimicrobial therapy. New testing methods such as multiplex polymerase chain reaction (MPCR), exhaled breath group analysis, and chromogenic tests have also been developed (62).
In terms of therapy, multidrug-resistant bacteria are a growing concern in the medical field. According to a recent article published in Frontiers in Bioengineering and Biotechnology, nanocarrier systems can be used to design and develop efficient antimicrobials for multidrug-resistant bacteria (63). These nano-sized antimicrobials have a predominance over traditional antibiotics because their small size helps them in better interaction with bacterial cells. Moreover, surface engineering of nanocarriers offers significant advantages of targeting and modulating various resistance mechanisms, thus owe superior qualities for overcoming bacterial resistance (63).
However, the development of new drugs is a complex process that requires extensive research and testing. It is important to note that the development of new drugs is highly regulated by government agencies such as the FDA in the United States. The process typically involves several stages, including preclinical testing, clinical trials, and regulatory review (8).
In terms of developing new drugs to treat multidrug-resistant bacteria based on the multidrug resistance of oral microorganisms, it is important to conduct extensive research on the mechanisms of antibiotic resistance and the specific characteristics of oral microorganisms. This research can help identify potential targets for drug development and inform the design of new drugs (63).
The contribution of oral bacteria to the development of pneumonia is well known. However, there is controversy regarding best practices for achieving optimal oral health care in the context of critical care. Drugs and formulations used in oral hygiene are effective in preventing VAP, but they still have inherent drawbacks. Studies of some other drugs have demonstrated their promise in ICU oral care instead of empirical antibiotics, and the development of new drugs is also worth looking forward to, but there is still a long way to go to transfer microbiology and drug research from the laboratory to the clinic, and promising technologies require more research before they become widely available. Further research is needed to standardize oral health assessment and care practices to develop evidence-based personalized oral hygiene for critically ill patients. Our hope is that this review might serve as a useful reference for ICU oral care and the prevention of VAP.
HH: Conceptualization, Data curation, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. XY: Conceptualization, Data curation, Investigation, Writing – review & editing. CH: Conceptualization, Data curation, Investigation, Writing – review & editing. JZ: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Writing – review & editing. YL: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by grants from the Sichuan Science and Technology Program (2025ZNSFSC0770), the Technological Innovation and Development Project of Chengdu Bureau of Science and Technology (2024-YF05-00571-SN), the Research and Develop Program, West China Hospital of Stomatology Sichuan University (RD-03-202402).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. (2020) 46(5):888–906. doi: 10.1007/s00134-020-05980-0
2. Malhan N, Usman M, Trehan N, Sinha A, Settecase VA, Fried AD, et al. Oral care and ventilator-associated pneumonia. Am J Ther. (2019) 26(5):e604–7. doi: 10.1097/MJT.0000000000000878
3. Nolan TJ, Gadsby NJ, Hellyer TP, Templeton KE, McMullan R, McKenna JP, et al. Low-pathogenicity Mycoplasma spp. alter human monocyte and macrophage function and are highly prevalent among patients with ventilator-acquired pneumonia. Thorax. (2016) 71(7):594–600. doi: 10.1136/thoraxjnl-2015-208050
4. King A. Exploring the lung microbiome's role in disease. Nature. (2024). doi: 10.1038/d41586-024-01123-3
5. Hutchins K, Karras G, Erwin J, Sullivan KL. Ventilator-associated pneumonia and oral care: a successful quality improvement project. Am J Infect Control. (2009) 37(7):590–7. doi: 10.1016/j.ajic.2008.12.007
6. Oliveira J, Zagalo C, Cavaco-Silva P. Prevention of ventilator-associated pneumonia. Rev Port Pneumol. (2014) 20(3):152–61. doi: 10.1016/j.rppneu.2014.01.002
7. Munro CL, Grap MJ, Elswick RK, McKinney J, Sessler CN, Hummel RS. Oral health status and development of ventilator-associated pneumonia: a descriptive study. Am J Crit Care. (2006) 15(5):453–60. doi: 10.4037/ajcc2006.15.5.453
8. Xie X, Lyu J, Hussain T, Li M. Drug prevention and control of ventilator-associated pneumonia. Front Pharmacol. (2019) 10:298. doi: 10.3389/fphar.2019.00298
9. Heo S, Haase EM, Lesse AJ, Gill SR, Scannapieco FA. Genetic relationships between respiratory pathogens isolated from dental plaque and bronchoalveolar lavage fluid from patients in the intensive care unit undergoing mechanical ventilation. Clin Infect Dis. (2008) 47(12):1562–70. doi: 10.1086/593193
10. Kharel S, Bist A, Mishra SK. Ventilator-associated pneumonia among ICU patients in WHO southeast Asian region: a systematic review. PLoS One. (2021) 16(3):e0247832. doi: 10.1371/journal.pone.0247832
11. Li J, Lyu S, Luo J, Liu P, Albuainain FA, Alamoudi OA, et al. Prophylactic antibiotics delivered via the respiratory tract to reduce ventilator-associated pneumonia: a systematic review, network meta-analysis, and trial sequential analysis of randomized controlled trials. Crit Care Med. (2024) 52(10):1612–23. doi: 10.1097/CCM.0000000000006323
12. Zha S, Niu J, He Z, Fu W, Huang Q, Guan L, et al. Prophylactic antibiotics for preventing ventilator-associated pneumonia: a pairwise and Bayesian network meta-analysis. Eur J Med Res. (2023) 28(1):348. doi: 10.1186/s40001-023-01323-z
13. Fanning J, Panigada M, Li Bassi G. Nosocomial pneumonia in the mechanically ventilated patient. Semin Respir Crit Care Med. (2022) 43(3):426–39. doi: 10.1055/s-0042-1749448
14. Gao M, Yu X, Liu X, Xu Y, Zhou H, Zhu Y. Effects of prophylactic nebulized antibiotics on the prevention of ICU-acquired pneumonia: a systematic review and meta-analysis. PeerJ. (2024) 12:e18686. doi: 10.7717/peerj.18686
15. Landelle C, Nocquet Boyer V, Abbas M, Genevois E, Abidi N, Naimo S, et al. Impact of a multifaceted prevention program on ventilator-associated pneumonia including selective oropharyngeal decontamination. Intensive Care Med. (2018) 44(11):1777–86. doi: 10.1007/s00134-018-5227-4
16. Sallam M, Snygg J, Allam D, Kassem R. From protection to prevention: redefining vaccines in the context of antimicrobial resistance. Cureus. (2024) 16(5):e60551. doi: 10.7759/cureus.60551
17. Piddock LJV. The crisis of no new antibiotics–what is the way forward? Lancet Infect Dis. (2012) 12(3):249–53. doi: 10.1016/S1473-3099(11)70316-4
18. Munita JM, Arias CA. Mechanisms of antibiotic resistance. Microbiol Spectr. (2016) 4(2):10.1128/microbiolspec.VMBF-0016-2015. doi: 10.1128/microbiolspec.VMBF-0016-2015
19. Cunha BA. Antibiotic side effects. Med Clin North Am. (2001) 85(1):149–85. doi: 10.1016/S0025-7125(05)70309-6
20. Yang R, Huang T, Shen L, Feng A, Li L, Li S, et al. The use of antibiotics for ventilator-associated pneumonia in the MIMIC-IV database. Front Pharmacol. (2022) 13:869499. doi: 10.3389/fphar.2022.869499
21. Koeman M, Van Der Ven AJAM, Hak E, Joore HCA, Kaasjager K, De Smet AGA, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. (2006) 173(12):1348–55. doi: 10.1164/rccm.200505-820OC
22. Klompas M, Speck K, Howell MD, Greene LR, Berenholtz SM. Reappraisal of routine oral care with chlorhexidine gluconate for patients receiving mechanical ventilation: systematic review and meta-analysis. JAMA Intern Med. (2014) 174(5):751. doi: 10.1001/jamainternmed.2014.359
23. Guidelines for Preventing Health-Care-Associated Pneumonia, 2003: Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee: (548652006-001). (2004). Available at: https://doi.apa.org/doi/10.1037/e548652006-001 (Accessed April 12, 2024).
24. Rabello F, Araújo V, Magalhães S. Effectiveness of oral chlorhexidine for the prevention of nosocomial pneumonia and ventilator-associated pneumonia in intensive care units: overview of systematic reviews. Int J Dent Hyg. (2018) 16(4):441–9. doi: 10.1111/idh.12336
25. Hua F, Xie H, Worthington HV, Furness S, Zhang Q, Li C. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst Rev. (2016) 10(10):CD008367. doi: 10.1002/14651858.CD008367.pub3
26. Evidence-Based Complementary and Alternative Medicine. Retracted: Meta-analysis of the efficacy and safety of chlorhexidine for ventilator-associated pneumonia prevention in mechanically ventilated patients [retraction of: Evid Based Complement Alternat Med. 2022 Jul 30;2022:5311034. doi: 10.1155/2022/5311034.]. Evid Based Complement Alternat Med. (2023) 2023:9873478. doi: 10.1155/2023/9873478
27. Nakonieczna J, Wozniak A, Pieranski M, Rapacka-Zdonczyk A, Ogonowska P, Grinholc M. Photoinactivation of ESKAPE pathogens: overview of novel therapeutic strategy. Future Med Chem. (2019) 11(5):443–61. doi: 10.4155/fmc-2018-0329
28. Kampf G. Acquired resistance to chlorhexidine – is it time to establish an ‘antiseptic stewardship’ initiative? J Hosp Infect. (2016) 94(3):213–27. doi: 10.1016/j.jhin.2016.08.018
29. Septimus EJ, Schweizer ML. Decolonization in prevention of health care-associated infections. Clin Microbiol Rev. (2016) 29(2):201–22. doi: 10.1128/CMR.00049-15
30. Brookes ZLS, Bescos R, Belfield LA, Ali K, Roberts A. Current uses of chlorhexidine for management of oral disease: a narrative review. J Dent. (2020) 103:103497. doi: 10.1016/j.jdent.2020.103497
31. Jhingta P, Bhardwaj A, Sharma D, Kumar N, Bhardwaj VK, Vaid S. Effect of hydrogen peroxide mouthwash as an adjunct to chlorhexidine on stains and plaque. J Indian Soc Periodontol. (2013) 17(4):449–53. doi: 10.4103/0972-124X.118315
32. Amano Y, Matsuura A, Tamura T, Kato Y, Kameyama N, Takazawa T, et al. Life-threatening chlorhexidine anaphylaxis caused by skin preparation before chlorhexidine-free central venous catheter insertion: a case report and literature review. J Anesth. (2023) 37(3):474–81. doi: 10.1007/s00540-023-03189-1
33. Arabaci T, Türkez H, Çanakçi CF, Özgöz M. Assessment of cytogenetic and cytotoxic effects of chlorhexidine digluconate on cultured human lymphocytes. Acta Odontol Scand. (2013) 71(5):1255–60. doi: 10.3109/00016357.2012.757646
34. Challacombe SJ, Kirk-Bayley J, Sunkaraneni VS, Combes J. Povidone iodine. Br Dent J. (2020) 228(9):656–7. doi: 10.1038/s41415-020-1589-4
35. Emami Zeydi A, Parvizi A, Haddadi S, Karkhah S, Hosseini SJ, Mollaei A, et al. Effect of oral care with povidone-iodine in the prevention of ventilator-associated pneumonia; a systematic review and meta-analysis. Arch Acad Emerg Med. (2023) 11(1):e31. doi: 10.22037/aaem.v11i1.1874
36. Tsuda S, Soutome S, Hayashida S, Funahara M, Yanamoto S, Umeda M. Topical povidone iodine inhibits bacterial growth in the oral cavity of patients on mechanical ventilation: a randomized controlled study. BMC Oral Health. (2020) 20(1):62. doi: 10.1186/s12903-020-1043-7
37. Mori H, Hirasawa H, Oda S, Shiga H, Matsuda K, Nakamura M. Oral care reduces incidence of ventilator-associated pneumonia in ICU populations. Intensive Care Med. (2006) 32(2):230–6. doi: 10.1007/s00134-005-0014-4
38. Seguin P, Tanguy M, Laviolle B, Tirel O, Mallédant Y. Effect of oropharyngeal decontamination by povidone-iodine on ventilator-associated pneumonia in patients with head trauma. Crit Care Med. (2006) 34(5):1514–9. doi: 10.1097/01.CCM.0000214516.73076.82
39. Seguin P, Laviolle B, Dahyot-Fizelier C, Dumont R, Veber B, Gergaud S, et al. Effect of oropharyngeal povidone-iodine preventive oral care on ventilator-associated pneumonia in severely brain-injured or cerebral hemorrhage patients: a multicenter, randomized controlled trial. Crit Care Med. (2014) 42(1):1–8. doi: 10.1097/CCM.0b013e3182a2770f
40. Niedner R. Cytotoxicity and sensitization of povidone-iodine and other frequently used anti-infective agents. Dermatol Basel Switz. (1997) 195(Suppl 2):89–92. doi: 10.1159/000246038
41. Vergara-Buenaventura A, Castro-Ruiz C. Use of mouthwashes against COVID-19 in dentistry. Br J Oral Maxillofac Surg. (2020) 58(8):924–7. doi: 10.1016/j.bjoms.2020.08.016
42. Rosling BG, Slots J, Webber RL, Christersson LA, Genco RJ. Microbiological and clinical effects of topical subgingival antimicrobial treatment on human periodontal disease. J Clin Periodontol. (1983) 10(5):487–514. doi: 10.1111/j.1600-051X.1983.tb02180.x
43. Nobahar M, Razavi MR, Malek F, Ghorbani R. Effects of hydrogen peroxide mouthwash on preventing ventilator-associated pneumonia in patients admitted to the intensive care unit. Braz J Infect Dis. (2016) 20(5):444–50. doi: 10.1016/j.bjid.2016.06.005
44. Lev A, Aied AS, Arshed S. The effect of different oral hygiene treatments on the occurrence of ventilator associated pneumonia (VAP) in ventilated patients. J Infect Prev. (2015) 16(2):76–81. doi: 10.1177/1757177414560252
45. Walsh LJ. Safety issues relating to the use of hydrogen peroxide in dentistry. Aust Dent J. (2000) 45(4):257–69. doi: 10.1111/j.1834-7819.2000.tb00261.x
46. Madeswaran S, Jayachandran S. Sodium bicarbonate: a review and its uses in dentistry. Indian J Dent Res. (2018) 29(5):672. doi: 10.4103/ijdr.IJDR_30_17
47. Beiswanger BB, McClanahan SF, Bartizek RD, Lanzalaco AC, Bacca LA, White DJ. The comparative efficacy of stabilized stannous fluoride dentifrice, peroxide/baking soda dentifrice and essential oil mouthrinse for the prevention of gingivitis. J Clin Dent. (1997) 8(2):46–53.9238873
48. Drake DR, Vargas K, Cardenzana A, Srikantha R. Enhanced bactericidal activity of arm and hammer dental care. Am J Dent. (1995) 8(6):308–12.8695008
49. Putt MS, Milleman KR, Ghassemi A, Vorwerk LM, Hooper WJ, Soparkar PM, et al. Enhancement of plaque removal efficacy by tooth brushing with baking soda dentifrices: results of five clinical studies. J Clin Dent. (2008) 19(4):111–9.19278079
50. Zambon JJ, Mather ML, Gonzales Y. A microbiological and clinical study of the safety and efficacy of baking-soda dentifrices. Compend Contin Educ Dent Suppl. (1997) 18(21):S39–47.12017933
51. Ghassemi A, Vorwerk LM, Hooper WJ, Putt MS, Milleman KR. A four-week clinical study to evaluate and compare the effectiveness of a baking soda dentifrice and an antimicrobial dentifrice in reducing plaque. J Clin Dent. (2008) 19(4):120–6.19278080
52. Taschieri S, Tumedei M, Francetti L, Corbella S, Del Fabbro M. Efficacy of 67% sodium bicarbonate toothpaste for plaque and gingivitis control: a systematic review and meta-analysis. J Evid-Based Dent Pract. (2022) 22(2):101709. doi: 10.1016/j.jebdp.2022.101709
53. Schmidt J, Zyba V, Jung K, Rinke S, Haak R, Mausberg RF, et al. Cytotoxic effects of octenidine mouth rinse on human fibroblasts and epithelial cells - an in vitro study. Drug Chem Toxicol. (2016) 39(3):322–30. doi: 10.3109/01480545.2015.1121274
54. Schmidt J, Zyba V, Jung K, Rinke S, Haak R, Mausberg RF, et al. Effects of octenidine mouth rinse on apoptosis and necrosis of human fibroblasts and epithelial cells - an in vitro study. Drug Chem Toxicol. (2018) 41(2):182–7. doi: 10.1080/01480545.2017.1337124
55. Assadian O. Octenidine dihydrochloride: chemical characteristics and antimicrobial properties. J Wound Care. (2016) 25(3 Suppl):S3–6. doi: 10.12968/jowc.2016.25.Sup3.S3
56. Koburger T, Hübner NO, Braun M, Siebert J, Kramer A. Standardized comparison of antiseptic efficacy of triclosan, PVP-iodine, octenidine dihydrochloride, polyhexanide and chlorhexidine digluconate. J Antimicrob Chemother. (2010) 65(8):1712–9. doi: 10.1093/jac/dkq212
57. Grover V, Mahendra J, Gopalakrishnan D, Jain A. Effect of octenidine mouthwash on plaque, gingivitis, and oral microbial growth: a systematic review. Clin Exp Dent Res. (2021) 7(4):450–64. doi: 10.1002/cre2.386
58. Jockel-Schneider Y, Schlagenhauf U, Petsos H, Rüttermann S, Schmidt J, Ziebolz D, et al. Impact of 0.1% octenidine mouthwash on plaque re-growth in healthy adults: a multi-center phase 3 randomized clinical trial. Clin Oral Investig. (2021) 25(7):4681–9. doi: 10.1007/s00784-021-03781-3
59. Zumtobel M, Assadian O, Leonhard M, Stadler M, Schneider B. The antimicrobial effect of octenidine-dihydrochloride coated polymer tracheotomy tubes on Staphylococcus aureus and Pseudomonas aeruginosa colonisation. BMC Microbiol. (2009) 9(1):150. doi: 10.1186/1471-2180-9-150
60. Lachapelle JM. A comparison of the irritant and allergenic properties of antiseptics. Eur J Dermatol EJD. (2014) 24(1):3–9. doi: 10.1684/ejd.2013.2198
61. Franz T, Vögelin E. Aseptic tissue necrosis and chronic inflammation after irrigation of penetrating hand wounds using Octenisept®. J Hand Surg Eur Vol. (2012) 37(1):61–4. doi: 10.1177/1753193411414353
62. Millot G, Voisin B, Loiez C, Wallet F, Nseir S. The next generation of rapid point-of-care testing identification tools for ventilator-associated pneumonia. Ann Transl Med. (2017) 5(22):451. doi: 10.21037/atm.2017.11.05
Keywords: ventilator-associated pneumonia, intensive care unit, oral medication and formulation, oral care, precise care
Citation: Huang H, Yu X, Huang C, Zeng J and Li Y (2025) Oral care medications for the prevention and treatment of ventilator-associated pneumonia in intensive care unit. Front. Oral Health 6:1566355. doi: 10.3389/froh.2025.1566355
Received: 24 January 2025; Accepted: 5 March 2025;
Published: 18 March 2025.
Edited by:
Katarzyna Garbacz, Medical University of Gdansk, PolandReviewed by:
Marta Katkowska, Medical University of Gdansk, PolandCopyright: © 2025 Huang, Yu, Huang, Zeng and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jumei Zeng, emVuZ2p1bWVpQHNjdS5lZHUuY24=; Yuqing Li, bGl5dXFpbmdAc2N1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.