 Vincenzo D’Antò1
Vincenzo D’Antò1 Vittoria De Simone1
Vittoria De Simone1 Silvia Caruso2Paolo Bucci3Rosa Valletta1Roberto Rongo1
Silvia Caruso2Paolo Bucci3Rosa Valletta1Roberto Rongo1 Rosaria Bucci1*
Rosaria Bucci1*
- 1Department of Neurosciences, Reproductive Sciences and Oral Sciences, Section of Orthodontics and Temporomandibular Disorders, University of Naples Federico II, Naples, Italy
- 2Department of Life, Health and Environmental Sciences, University of L'Aquila, L'Aquila, Italy
- 3Department of Public Health, Section of Hygiene, University of Naples Federico II, Naples, Italy
Introduction: In recent years, the use of Clear aligners (CA) has been diffused among children and adolescents. This systematic review aimed to summarize the literature regarding the effects of CA therapy in growing patients, including dentoalveolar and skeletal effects, periodontal changes, and quality of life measurements.
Methods: An electronic search on four databases was performed until September 2023, and studies including patients <18 years, treated with CA were selected. Studies with less than 10 patients and in vitro/laboratory studies were excluded. Study selection, data extraction, and risk of bias assessment were independently performed by two reviewers. The “Risk of Bias 2” (RoB 2) and the “Risk of Bias in Non-randomized Studies of Interventions” (ROBINS-I) tools were applied to assess the methodological quality of the included studies. Due to the heterogeneity in methodologies and outcomes encountered in the included studies, a qualitative synthesis of the results was provided.
Results and conclusions: The search resulted in 32 papers (3 RCTs), with sample sizes ranging between 15 and 113. The overall risk of bias in the RCT was low, while the risk of bias in the non-RCT ranged between moderate and serious for most of the included studies. Dentoskeletal and periodontal effects were the most frequently reported outcomes. The most common comparison group was multibracket fixed therapy, while only 5 studies had an untreated control group. Significant changes in the transversal maxillary arch width after treatment with CA were reported in some studies. However, while dentoalveolar effects have been reported consistently, controversial findings were found regarding the changes in skeletal bases after treatment with CA. Concerning the results on the sagittal plane, the current literature does not support the effectiveness of CA with mandibular advancement features in correcting dentoskeletal Class II, compared to traditional functional orthopedic appliances. In the short-term evaluation, periodontal variables and bacterial levels seemed to be better controlled during CA therapy, compared to the fixed multibracket therapy. With regard to quality of life measurements, there are inconsistent findings to support differences between CA therapy and fixed multibracket appliances. Nevertheless, additional high-quality studies are required to formulate more reliable conclusions.
Systematic Review Registration: https://osf.io/wmerq.
1 Introduction
Several orthodontic problems should already be treated at an early age to prevent the necessity of future complex and expensive procedures (1). The primary goals of early orthodontic interventions are to prevent or reduce the developmental of dentoskeletal abnormalities, to maintain space following premature loss of deciduous teeth, to manage functional habits that could contribute to malocclusion, and to minimize the invasiveness of the second treatment phase (2).
Previous studies have demonstrated that appliance acceptability, social impact, and quality of life, represent key elements in achieving good patient compliance and to improve treatment efficacy (3–5). Furthermore, it has been recognized that patient's aspect with orthodontic appliance could affect physical, social, and psychological well-being (6).
In this context, orthodontic devices with limited aesthetic impact, such as clear aligners (CA), observed a huge increase in their use in the last decades (7–9). As a result, there has been a substantial expansion in research focused on CA treatment (10). Possible advantages of these devices include the ability to remove the appliance during meals and oral hygiene procedures, and the reduction in the pain levels experienced by patients (11).
For many years, orthodontic treatments with CA were directed only to adult patients with full permanent dentition, with the aim to treat mild to moderate malocclusions (12). Over time, with the evolution of technologies and the improvement of material properties, the indications for CA use have increased, and this treatment approach has been extended also to more complex cases (13). One of the most recent frontiers of CA therapy concerns orthodontic treatment in growing patients (14–16).
Some authors have reported significative improvements in maxillary arch width of growing patients treated with CA (17–22), suggesting that CA could be a reasonable alternative to traditional slow maxillary expanders (18). Furthermore, CA with mandibular advancement (MA) systems have been found to be effective in treating Class II growing patient with a retrognathic mandible (23–29). Therefore, the aim of the present study was to systematically search the literature and summarize the current available scientific evidence regarding the effect of CA treatment in children and adolescent patients, and evaluate the advantages of aligners treatment compared to traditional appliances in term of dentoskeletal effects, periodontal health and quality of life.
2 Materials and methods
2.1 Protocol and registration
The study protocol was established and registered in the OSF registries (https://osf.io/wmerq).
The current systematic review was conducted in accordance to the PRISMA guideline (30). The review question was structured based on the PICO approach (31):
P (patients): humans, both males and females, less than 18 years of age (children and adolescents),
I (intervention): orthodontic treatment with CA,
C (comparison): other orthodontic treatments, no treatment or no comparison,
O (outcome): dentoalveolar and skeletal effects (primary outcome); adverse effects, periodontal effects, compliance, quality of life, aesthetics (secondary outcome).
2.2 Literature search and study selection
An electronic search without time or language restrictions was performed in December 2021 on the following electronic databases: PubMed, Scopus, The Cochrane Library and Literature in the Health Sciences in Latin America and the Caribbean (LILACS), as shown in Table 1. A manual search was also performed among the references of the included articles to identify possible items not listed in the electronic search. The following inclusion criteria were used for the study selection: human study in children and adolescent patients (<18 years of age); studies with at least one group of treated patients (CA treatment). Randomized clinical trial (RCT), prospective and retrospective non-randomized clinical trials, and studies without control group were included. Case series and case reports (<10 patients), in vitro/laboratory studies, systematic review, narrative reviews, editorials, opinion articles or letter from authors, were excluded. Two authors (RB and VDS) independently screened the list of title and abstract of potentially eligible studies, using the Rayyan (http://rayyan.qcri.org) software (32). If the title and abstract did not provide sufficient information, or if the abstract was not available, articles were included for full-text assessment. Disagreements between the two investigators were resolved through discussion and if necessary, a third operator (VD) was contacted for final decision.
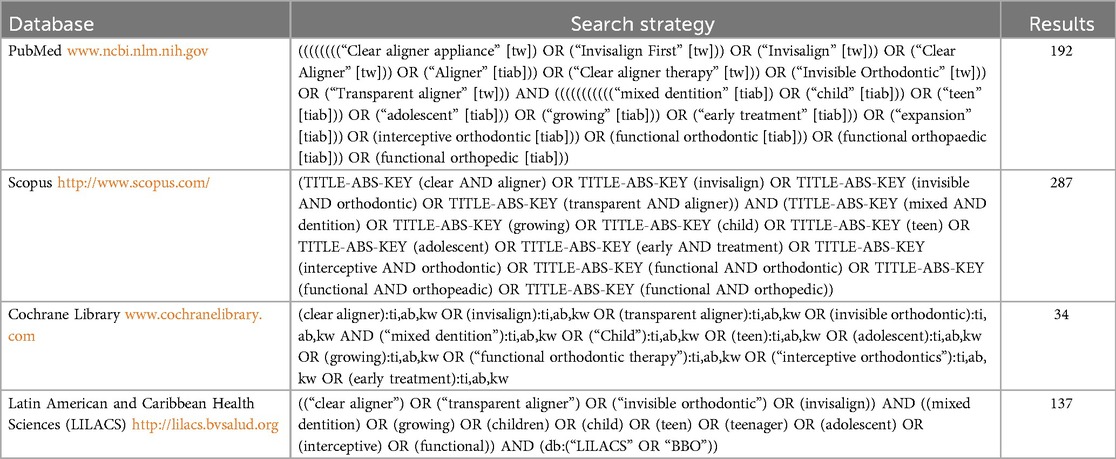
Table 1. Search strategy for each database and relative results.
2.3 Data extraction
Data were independently extracted by two authors (RB and VDS) using a customized extraction form. The authors were not contacted for further details. The following data were extracted: author; year and country of publication; study design (RCT, CCT, Ret etc.) and sample size; baseline orthodontic diagnosis; presence of control group; appliance; wearing time; aligners change (days); mean number of aligners; dropout; follow-up; methods of measurement; study aim; outcome; and author's conclusions.
2.4 Methodological quality of the included studies
To evaluate the risk of bias of randomized controlled trials (RCT), the Cochrane Collaboration “risk of bias” (RoB-2) tool was used (33). Risk of bias was assessed and judged as low risk, high risk, or unclear risk of bias for seven domains.
For non-randomized studies, the Cochrane Collaboration “risk of bias in non- randomized studies of interventions” (ROBINS-I) tool was applied (34), and studies were rated as low, moderate, serious or critical risk of bias.
3 Results
3.1 Search results
The PRISMA flow chart describing the study identification process is presented in Figure 1.
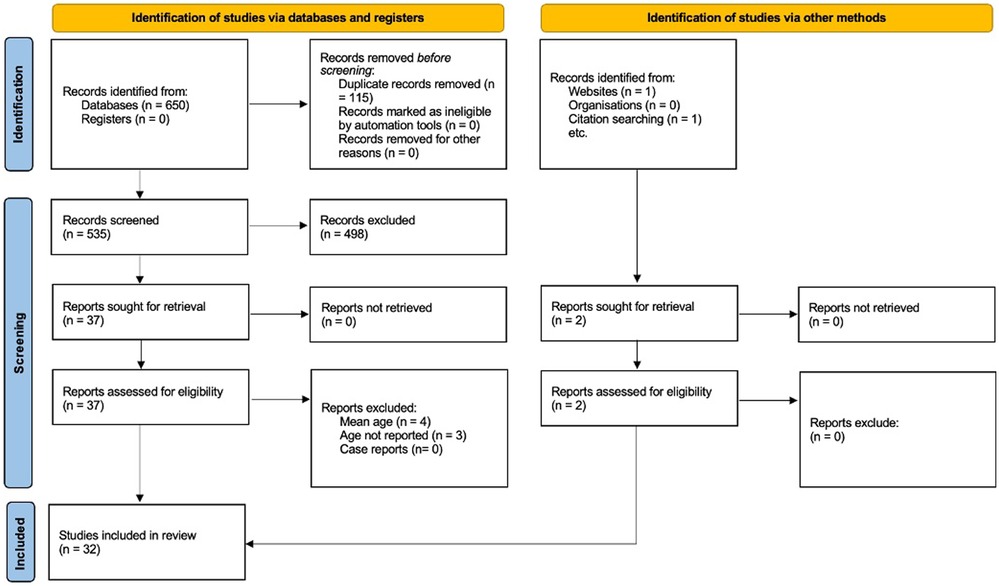
Figure 1. PRISMA flow ndiagram of the included studies.
A total of 650 records were identified through electronic and manual searches. After duplicates removal, title and abstracts of 535 records were screened, of which 37 met the inclusion criteria and were considered as potentially eligible. After full-text reading, seven studies were excluded, with the most common reason for exclusion being the age of the study sample (Table 2). One article was retrieved from sources other than database (25), while another study was found through additional hand-searching of the reference lists of selected studies (29). Thus, 32 articles were finally included in this systematic literature review (4, 5, 11, 14, 17–21, 23–29, 35–50).
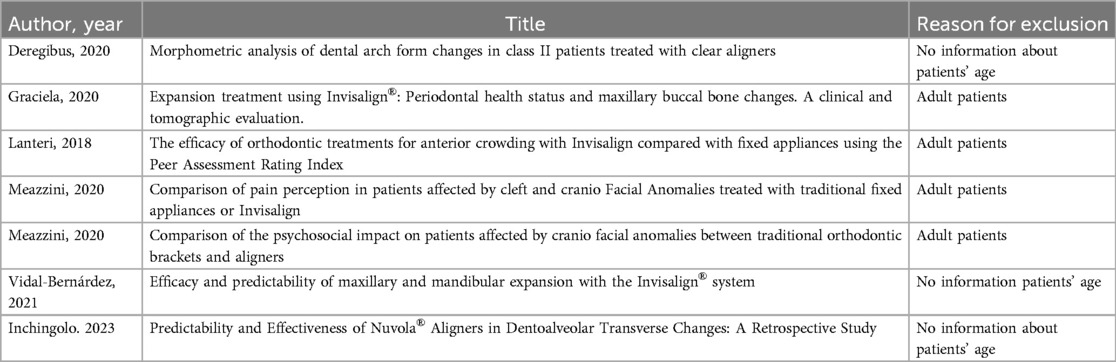
Table 2. List of full text excluded and reason for exclusion.
3.2 Characteristics of the studies
Data extracted from the 32 studies are presented in Table 3. The studies included in the present review were conducted between 2015 and 2023. The number of total subjects included in each review ranged between 15 and 113, and the median age was 8.7 years (IQR 7.6–9.8 years).
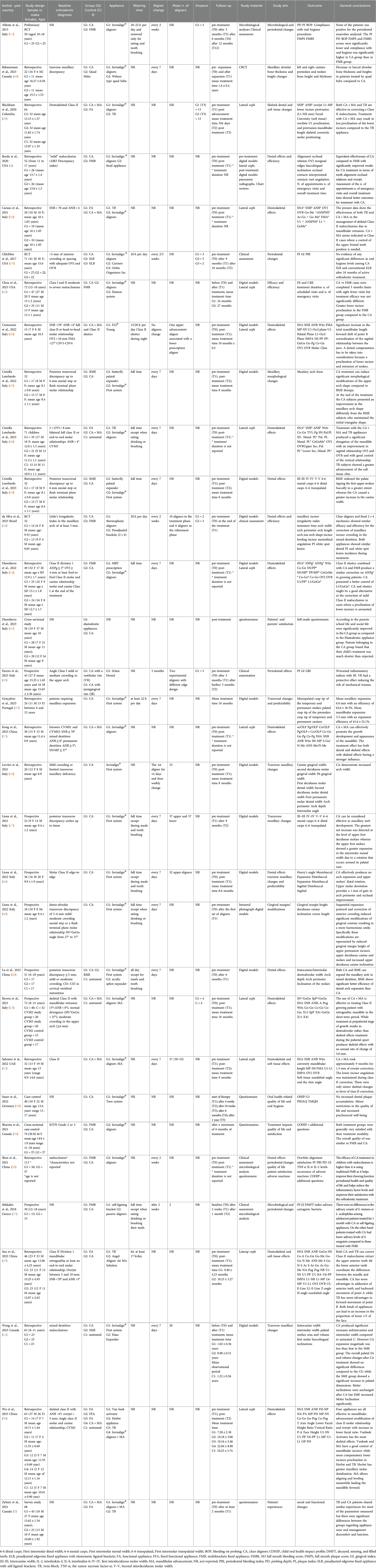
Table 3. Data extracted from the 32 included studies.
Baseline orthodontic diagnoses were transverse maxillary deficiency (seven studies), crowding (three studies), and Class II (12 studies); however, not all of the studies clearly specified the initial diagnosis. Three studies included patients with different degree of malocclusion (according to standardized indices such as the ABO malocclusion index, IOTN and Little's Irregularity index), while seven studies did not mention the baseline malocclusion as an inclusion criterion.
Of the 32 included studies, three were RCTs, and 29 were non-randomized studies (18 retrospective, eight prospective, and three cross-sectional studies). A comparison with fixed orthodontic appliance was performed in nine studies (4, 11, 14, 35–38, 42, 44), two of which adopted self-ligating appliances (35, 37). Five studies compared the effects of CA and mandibular advancement (MA) with those of the Twin-Block appliance (TB) (5, 24, 25, 28, 29), or other functional appliances (50). Four studies compared the effects of CA with rapid maxillary expander (RME) with different designs (19–21, 45), or Quad Helix (48). Only five studies included a sample of untreated subjects as a control group (20, 21, 23, 28, 50), and eight studies had no control group (17, 18, 27, 39, 40, 46, 47, 49). Concerning the treatment protocol for CA use, five studies recommended aligners change every 2/3 weeks (11, 35–37, 44). 12 studies recommended a weekly change of the aligners (14, 17, 19–21, 29, 40, 45–48, 52). One study proposed the use of the first pairs of aligners for two weeks, and then the change every seven days (18). In the study conducted by Favero et al. (43), two experimental aligners with different edge design were used in the same treatment group, with the device change occurring after three months (33). In one study there was no change in aligners, as only one upper advancement aligner associated with a lower prescription aligner was used during treatment (26). Furthermore, in another study, only two pairs of passive experimental CA were adopted, with the first pair being changed after two weeks (37). Twelve studies did not mention a specific wearing time protocol, suggesting adherence to the manufacturer's recommendations (4, 5, 23–25, 27, 29, 38, 39, 41, 42, 50). The mean number of aligners required to complete the therapy was reported only in six studies, ranging between 28 and 37 (17, 18, 21, 44, 46, 52). The follow-up data ranged from two weeks up to 24 months (7, 12, 17–22, 24, 37–39, 41–48, 50, 52, 53).
3.3 Risk of bias (quality assessment) of the included studies
3.3.1 RCT
The three RCTs (11, 35, 44) were judged to be at an overall low risk of bias (Table 4).

Table 4. Risk of bias in randomized trials (RoB 2 tool).
3.3.2 Non-randomized studies
Out of the seven prospective studies (17, 20, 22, 37, 40, 43, 46), two were rated with a low risk of bias (20, 37), two with moderate risk (17, 46), and three at severe risk of bias (23, 40, 43). Among the 18 retrospective studies, five were graded as having a serious risk of bias (4, 24, 26–28), and 13 (14, 18, 19, 21, 25, 29, 36, 42, 45, 47, 48, 50, 52) as moderate risk of bias. Four cross-sectional studies (5, 38, 39, 41) were judge to have a serious risk of bias (Table 5). Common reasons for loosing points in the quality assessment were poor or no description of the sample's diagnosis at baseline, differences in age variability among study groups, lack of appliance descriptions (wearing time, aligner change, mean number of aligners), and lack of standardization in study outcomes.
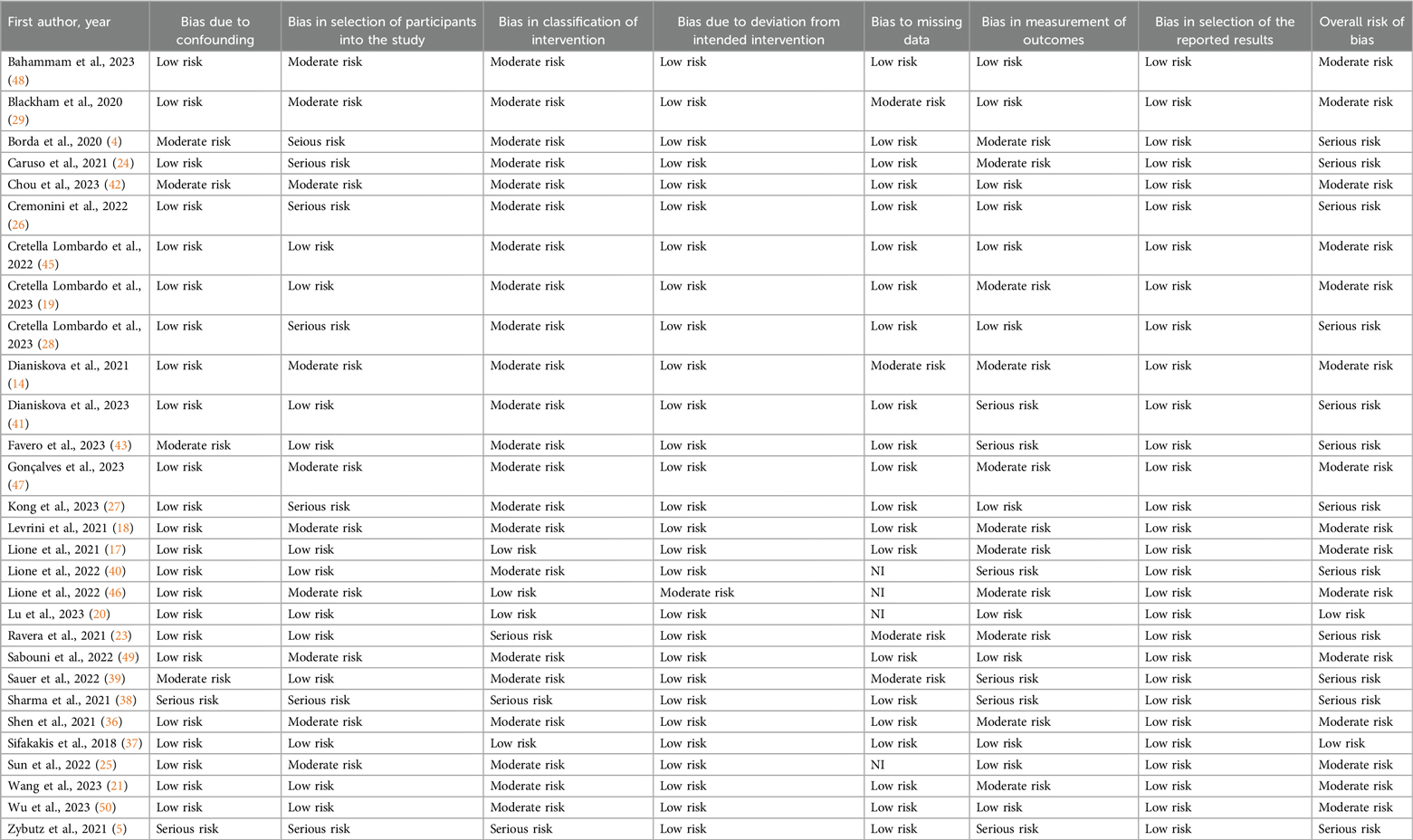
Table 5. Risk of bias in non-randomized studies (ROBINS-I tool).
3.4 Study findings
3.4.1 Dentoskeletal effects
Of the 32 studies, 21 analyzed the dentoskeletal effects of CA (4, 14, 17–21, 23, 24, 26–29, 36, 44–48, 50, 52).
3.4.1.1 Transversal changes
Seven studies (17–21, 45, 48) evaluated differences in transversal maxillary arch width after expansion treatment with CA. Studies without control group (17, 18) showed significant increase in all linear interdental distances measured on digital models after treatment treatment with CA. Among the studies that compared CA with RME (19–21, 45) three reported increased transversal expansion after RME treatment compared to the CA group (19–21), accompanied by significant buccal tipping of the upper first molars. However, no significant differences were found in the CA group for this parameter. One study (19) pointed out a greater increase in the inter-canine width in the CA group compared to the RME group. In a previous study, the authors also found significative differences in morphological changes of the upper arch in the aligners group compared to the RME group (45).
When CA treatment was compared with the Quad Helix appliance (48), a retrospective study on CBCT demonstrated a significative decrease in bone height and width in the group treated with the Quad Helix.
The predictability of the transversal expansion following CA treated has been assessed in two studies without a control group (46, 47). Both studies supported that approximately 60% of the predicted expansion movement was achieved (46).
3.4.1.2 Sagittal changes
Ten studies assessed sagittal dentoskeletal changes in Class II patients (14, 23–29, 49, 50) following CA + MA treatment. Three retrospective studies (26, 27, 49) without a control group, reported significative improvements in mandibular position after treatment with CA + MA in growing patients. However, the study by Sabouni et al. (49) pointed out only small changes the ANB angle, with no relevant changes in the SNB angle after treatment, suggesting that there were only minimal skeletal effects favoring Class II correction. The prospective study by Ravera et al. (23) compared the CA + MA treatment with untreated controls and supported increased correction of the ANB angle in the aligner group, particularly when the treatment was performed during the pubertal stage. Five retrospective studies (24, 25, 28, 29, 50) compared the effects of CA + MA with traditional functional appliances such as the Twin Block (TB), among others (50); of these studies, three also presented an untreated control group (28, 29, 50). Wu et al. (50) and Sun et al. (25) found more advanced mandibular position (SNB angle) in the TB group compared to the CA group. Caruso et al. (24) described significant differences between groups in the ANB angle after treatment, with more significative changes for the TB group, while the SNB angle increased similarly in both groups. The authors hypotheses that the difference was due to the increased retroclination of the upper incisors in the TB group compared to the CA group, as well as the difference in the mean ANB at the baseline. In contrast with these results, Cretella Lombardo et al. (28), showed no between-groups differences in the changes of the ANB angle after treatment.
Two retrospective studies (14, 42) evaluated the effects of Class II correction with intermaxillary elastics in the fixed multibracket (FMB) group compared to the CA group. Chou et al. (42) found that CA were more efficient in terms of treatment duration; furthermore, superimpositions indicated greater lower incisor proclination in the FMB group compared with the CA group. Dianiskova and colleagues (14) did not observe any statistically significant improvement in the sagittal skeletal relationship in the two groups, while a better control of lower incisors proclination was found with CA.
The reported effects of CA + MA on the inclination of maxillary and mandibular incisors are controversial. When compared with the TB appliance, three studies (24, 29, 50) found significantly increased retroclination of the upper incisors in the TB group and better control of the lower incisors in the CA group. Conversely, Sun et al. reported a significant reduction in the inclination of the upper incisors in both groups, with a greater difference observed in the aligner group, while lower incisor inclination increased similarly (25). Consistent with these results, the prospective study by Ravera et al. reported a significant reduction in the proclination of the upper incisors with CA + MA compared to untreated controls, when treatment was performed during the prepubertal stage of growth (23). Kong et al. also found that CA + MA treatment led to an average decrease of 3.44° in the inclination of the upper incisors, while the inclination of lower incisors increased by a mean of 2.62° (27). In contrast, Lombardo et al. (28) suggested that both appliances are effective in controlling incisor inclination during mandibular advancement. Cremonini et al. (26) also reported the control of upper and lower incisor inclination during treatment with CA + MA, although in a study without a control group.
3.4.1.3 Crowding, OVJ and OVB
The retrospective study by Shen et al. (36), compared rate of overbite correction and alignment between CA and FMB, concluding that the effective rate was higher in the CA group. Conversely, the RCT by Merino da Silva and colleagues (44) demonstrated similar efficacy and efficiency for maxillary incisors crowding correction in mixed dentition between CA and fixed 2 × 4 mechanics. Borda and co-workers (4) pointed out similar effectiveness of CA compared to fixed therapy in terms of dentoalveolar correction, except for tooth alignment, overjet and occlusal relationship, which were significantly improved in the CA group. Caruso et al. (24) found overbite correction after treatment with CA + MA, while no differences were observed in the TB group. In contrast with these results, two retrospective studies (25, 28) showed that both CA + MA and TB appliances were able to reduce the overjet and overbite, with no differences between the groups. Finally, Wu and co-workers (50) reported that Van Beek Activator accounted the highest proportion of skeletal effects in reducing overjet (74.73%), compared to CA, TB, a Herbst appliance, and untreated controls.
3.4.2 Oral health and periodontal changes
Six studies (11, 35–37, 44, 54) evaluated periodontal changes after treatment with CA in growing patients. The most commonly measured variables were the plaque index (PI), the gingival index (GI), the probing depth (PD), and the periodontal bleeding index (PBI). Two RCTs compared the effects of CA with FMB treatment (35, 44): Chhibber et al. (35) demonstrated no difference in periodontal health between subjects treated with CA, self-ligated brackets, or elastomeric-ligated brackets after 18 months of treatment. In agreement with these results, the RCT by Merino da Silva et al. (35, 44) reported similar PI during treatment both with both fixed 2 × 4 appliances and CA. In contrast, another RCT (11) and one prospective study (37), reported reductions in periodontal indices and bacterial levels, respectively, in the aligner group compared to patients treated with fixed appliances. Similarly, the retrospective study by Shen et al. (36) found that periodontal indices increased after treatment in both CA and fixed therapy groups, but the values in the between-group comparison were significantly higher in the FMB group. The cross-sectional study by Sauer et al. (39) showed that home oral hygiene with CA was intensified, and no dental plaque accumulation was observed. In the prospective study by Favero and colleagues (43) two experimental aligners with different edge designs were used to evaluate periodontal changes after three months. The results demonstrated that inflammatory indices worsened in the group with juxtagingival rims compared to vestibular rims.
3.4.3 Quality of life, satisfaction and other outcomes
Five studies (5, 36, 38, 39, 41) evaluated the quality of life and satisfaction of CA treatment in growing patients. The case-control study by Sharma et al. adopted the Child Oral Health Impact Profile Short Form- 19 (COHIP-SF 19) and supplementary questions, concluding that there were no significant differences in mean quality of life and satisfaction between the CA group and the FMB group (38), after a minimum of six months of treatment. Similarly, the cross-sectional study by Sauer et al. (39) found that periodontal indices increased after treatment in both CA and fixed therapy groups, but the values in the between-group comparison were significantly higher in the FMB group. The cross-sectional study by Sauer et al. (5). The results highlighted that, although there were some differences between the treatment groups, their experiences with their appliance were overall comparable, and most patients in both groups reported high levels of satisfaction with their treatment.
However, the retrospective study by Shen et al. (36) showed that the quality of life and satisfaction were significantly higher in CA group compared to the FMB group, with a total satisfaction rate of 98.25% and 69.64%, respectively. Dianiskova et al. (41) founded similar results when comparing CA with the elastodontic therapy. Furthermore, one study retrospectively evaluated the treatment efficiency through questionnaires about the number of appointments, number of emergency visits, and treatment duration; all of these outcomes resulted in favor of the CA group compared to the FMB (4).
4 Discussion
Clear aligners (CA) have recently taken center stage in terms of their applicability and ability to successfully correct diverse types of malocclusions in all age groups, including early orthodontic treatments. The introduction of improved staging patterns, new aligner materials, and the implementation of hybrid therapies with different auxiliaries has increased the application of CA (55, 56). The aim of the present systematic review was to analyze and summarize the current scientific literature concerning the effects of CA treatment in children and adolescent patients. The main reported outcomes collected from the included studies were dentoskeletal effects, periodontal effects, quality of life, and satisfaction after CA treatment.
4.1 Dentoskeletal effects
4.1.1 Transversal changes
In recent literature, some articles address the use of CA for the treatment of early transverse discrepancy. Two studies (17, 18) with moderate risk of bias found significant changes in transverse maxillary arch width after treatment with CA. However, in both studies, patients were recruited if they presented minor transversal discrepancy at the baseline. In fact, in the study by Lione et al. (17), 11 patients exhibited a crossbite involving one or two teeth, while the other 11 patients had no crossbite, and none presented a bilateral crossbite. Also, the studies included small sample sizes without a control group and had a short observational period (8 months), not accounting for possible relapse. Four studies (19–21, 45) evaluated transversal effects after expansion treatment with bonded RME compared to CA. The prospective study by Lu et al. (20), graded at low risk of bias, showed that RME allows a significantly greater expansion then CA, while CA produce dentoalveolar effects by delivering a certain amount of force on the dental crown. These results were supported by Cretella Lomardo et al., who highlighted that RME widened the palate to a greater extent (19), while CA induce maxillary arch shape modifications during expansion, in contrast with RME (45). Similarly, Wang et al. (21) reported that inter-canine width increased significantly in CA group compared to untreated controls, but the expansion amount was smaller than that achieved with SME. Three of these studies found significant buccal tipping of the upper first molars in the RME group, while no significant differences were found in the CA group (19–21). This was related to the possibility of planning an overcorrection of buccal root torque of the upper molars with CA treatment to avoid the side effects of dental tipping during expansion. In contrast with these results, the study by Bruni et al. (22) concluded that the more significant increase in intermolar width at the gingival level was observed in the RME group compared to the CA group, suggesting the occurrence of buccal tipping in the molar area using CA. However, all of the measurements of these studies were based on soft tissue and dental landmarks. Based on these evaluations, we can conclude that CA produce a certain amount of dentoalveolar expansion with the advantage of modifying arch form from early stages, and could be useful when mild transversal discrepancies are present. When skeletal expansion of the upper jaw is required, RME is considered more effective than CA, as it generates significantly higher forces leading to a predominantly skeletal effect (57). The greater magnitude of force produced by RME facilitates maxillary expansion by inducing structural changes in the bone, whereas CA primarily exert forces that are limited to dental movement. As a result, RME is particularly advantageous for addressing skeletal discrepancies and achieving substantial changes in maxillary morphology (57).
4.1.2 Sagittal changes
Most of the included studies evaluated the sagittal skeletal effects of CA with MA in growing Class II patients with mandibular retrusion. Three retrospective studies without a control group observed some mandibular advancement in the short term (26, 27, 49). Differently, Sabouni et al. found that only the ANB angle significantly decrease (−0.55°) after treatment with CA + MA (49); however, the change was less than previously reported in the literature (23, 24). When comparing CA + MA with an untreated control group, Ravera et al. (23) found no differences in the SNB angle after treatment with CA + MA in the treated groups at different stages of growth, with significative changes only for the intermaxillary sagittal relationship in the CVM2 group (ANB −1.30°, P = 0.01) in the short time (18 months). A significant increase was noted in the CVM3 group regarding the linear growth of the mandible (Co-Gn +8.75 mm, P = 0.03). However, it is not clear how it is possible that no physiological mandibular growth occurred in the untreated control group (T0 = 113.24 ± 6.18; T1 = 113.07 ± 6.04). Five studies (24, 25, 28, 29, 50), graded at moderate or severe risk of bias, compared the effects of traditionally used functional appliances as the TB with those produced by CA + MA appliance. Caruso et al. (24) showed significantly higher decrease in the ANB angle in the TB group compared with the MA group, while the SNB angle increased significantly without differences between groups. However, the mean ANB value was significantly different between groups at the baseline. Furthermore, the TB group presented significant reduction in the SNA angle, which was related to the retroclination of the upper incisors, a finding not found in the CA group. In contrast, Sun et al. (25) demonstrated that SNB angle increase significantly only in the TB group, while the ANB angle and mandibular length (Co-Gn) were significantly different in both groups. However, the lack of comparison with an untreated control group, differences in age at the baseline between groups, and the short observational period represent limitations for considering these results reliable and to exclude the influence of natural mandibular growth. Conversely, three retrospective studies (28, 29, 50), graded at moderate and severe risk of bias, demonstrated significant changes in the ANB and SNB angles after both treatments with TB and CA + MA, with no differences between groups. In conclusion, the results obtained from this systematic review about sagittal effects of CA in correcting dentoskeletal class II are controversial. Thus, well conducted studies with large sample sizes and long-term follow-up periods are needed to establish the effectiveness of CA with MA compared to the traditional functional appliances.
4.1.3 Dental effects
Interestingly, some included studies reported that CA provide good control of incisors inclination during sagittal correction of Class II malocclusion, both with MA (24, 26, 29, 50) and with intermaxillary elastics (14). In particular, the proclination of lower incisors is often an unwanted side effect of sagittal Class II correction, which is especially important in patients who already present increased proclination of lower incisors at the baseline before starting orthodontic treatment. Similarly, the retroclination of the upper incisors is frequently observed after Class II treatment, both with orthopedic devices and with fixed orthodontic appliances, and is often associated with retropositioning of the A point. The greater control provided by CA is likely associated with the intrinsic geometry of the aligner, which provides full coverage of the dental crown and maintains the entire dental arch through a unified structure (14, 51). Another possible explanation for the better control of lower incisor proclination might be linked to space management through digital setup: for instance, arch expansion, IPR, or the presence of preexisting spaces are conditions that offer the possibility for retroclination of the lower incisors. One more explanation could also be the incomplete correction of the curve of Spee. Authors have reported that controlling lower incisor inclination during Class II treatment offers promising effects in sagittal skeletal correction with CA and MA, since limited proclination of the lower incisors reduces the dentoalveolar compensation, thus providing more OVJ for guiding the mandible forward (49, 58).
4.2 Periodontal effects
The effects of CA on periodontal health have been evaluated in six studies, three of which were RCTs considered at low risk of bias (11, 35, 44). The 3-arm parallel-group prospective RCT by Chhibber et al. (35) found no evidence of differences in oral hygiene levels among CA, self-ligated brackets, and conventional elastomeric ligated brackets after 18 months of active orthodontic treatment. However, the short-term outcomes (after 9 months of treatment) show that the CA group participants had better GI and PBI scores than the fixed therapy groups (35). Similar findings were observed among adults when comparing CA with conventional multibracket therapy (59). Authors have reported that, when followed by a dental hygienist, patients undergoing orthodontic treatment with fixed appliances and CA do not show differences in gingival health. This was confirmed by the RCT of da Silva et al. (44), sustaining that there were no differences in plaque index in both treated groups in the short time (8 months). However, the value was very close to a level of significance in favor of a better oral hygiene for the CA group (44). Conversely, the preliminary RCT conducted by Abbate et al. (11) showed that during 12 months of orthodontic therapy, teenagers treated with removable appliances demonstrated better compliance with oral hygiene and presented less plaque and gingival inflammatory reactions as compared to their peers with fixed appliances. Similar results were reported in the retrospective study by Shen et al. (36) in a children population of 113 subjects, suggesting that bracketless invisible orthodontic treatment helps to improve periodontal health more than traditional fixed orthodontic treatment.
A recent systematic review authored by Di Spirito et al. (60) evaluated the long-term effects of CA compared to fixed multibracket therapy on periodontal health status, without age restrictions. The authors pointed out that CA provided slightly better control of PI and GI compared to fixed orthodontic appliances, especially in the short and medium terms, but no differences were found during the long-term follow-up (from the baseline to 12 months or more). Authors concluded that the impact of orthodontic treatment with CA and FMB on periodontal health should be considered comparable.
The meta-analysis conducted by Jiang et al. (53) in 2018 demonstrated that CA allowed relatively better periodontal health conditions (PI, GI, and PD) compared to fixed appliances, but the quality of evidence was medium. These findings are also in accordance with a previous review by Rossini et al. (61).
Therefore, it seems that while for adults no major differences are reported in terms of periodontal health, children and adolescents undergoing CA therapy exhibit better compliance with oral hygiene, reduced gingival indices, and improved periodontal status, especially in the short term.
4.3 Quality of life and satisfaction
Patient-Reported Outcomes Measures (PROMs) are the instruments used to assess information directly reported by the patient, without the interpretation of a clinician regarding their health, Quality of Life (QoL), or functional status associated with healthcare or treatment, among which satisfaction is one of the most important factors. Patient satisfaction and quality of life were examined in five studies (5, 36, 38, 39, 41). Sharma et al. (38) concluded that both the CA and fixed therapy groups were generally very satisfied with their treatment modalities. The overall quality of life of adolescent orthodontic patients undergoing treatment with fixed appliances and CA for a minimum of 6 months was comparable. Similarly, Sauer and colleagues (39) reported that oral health-related quality of life is only slightly affected during the first year of CA treatment in adolescents. These results are in line with previous findings by Flores-Mir et al. (62), who found that both the bracket-based and CA treated patients had statistically similar satisfaction outcomes across all dimensions analyzed in adults, except for the eating and chewing domain, in which the CA group reported more satisfaction. The retrospective study by Shen et al. (36) involving 113 children divided into two groups, concluded that CA treatment in children improves chewing function, quality of life, and satisfaction when compared with the FMB appliance. Similarly, a previous cross-sectional study by Azaripur et al. (63) demonstrated that patients treated with CA had greater satisfaction and reported less impairment in general well-being (6% vs. 36%) during orthodontic treatment than patients treated with fixed appliances. Zybutz et al. (5) compared CA with MA and TB appliance and reported that patients shared similar experiences for most of the parameters measured, but there were significant differences between the groups regarding appliance wear and management, discomfort, and function. A more recent systematic review (2023) by Kaklamanos et al. (6) assessing the patients’ health related quality of life following CA therapy, concluded that treatment with CA could be associated with better oral health related quality of life ratings compared to treatment with conventional labially placed metal fixed appliances. However, further high-quality studies are needed to reach safer conclusions.
5 Limitations
This systematic review highlights several limitations. The included studies are highly heterogeneous in design, patient characteristics, treatment protocols and outcomes, making comparisons difficult. Small sample sizes reduce statistical power and generalizability, while varying follow-up durations limit long-term data on treatment stability and effectiveness. Additionally, the lack of high-quality randomized controlled trials prevents drawing definitive conclusions about the relative effectiveness of early treatment with CA.
6 Conclusions
Based on the studies available in the literature, albeit the existing limitations, the following main conclusions about the effects of CA treatment in growing patients can be made:
• In the case of a mild transverse maxillary deficiency, CA produce dentoalveolar expansion during mixed dentition, but there is no evidence of skeletal effects.
• The effectiveness of CA + MA compared to traditional functional appliances in the correction of dentoskeletal Class II cannot be supported.
• There is no agreement in literature about the effects of CA on the upper and lower incisors; however, some studies reported that CA provide good control of incisor inclination during sagittal correction, when needed.
• In the short term, few studies support the notion that periodontal health and bacterial levels are better controlled in children and adolescents undergoing CA therapy compared to conventional fixed multibracket therapy.
• There are inconsistent findings to support that quality of life and patient satisfaction in growing patients are enhanced with invisible aligner therapy compared to fixed appliances.
These results suggest that early treatment with CA may be effective in certain type of malocclusions, but the evidence is inconsistent and does not always support advantages over traditional treatments, particularly regarding skeletal effects, Class II correction, and overall patient satisfaction.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
VD'A: Conceptualization, Project administration, Supervision, Validation, Writing – review & editing. VD: Data curation, Investigation, Writing – review & editing. SC: Validation, Writing – review & editing. PB: Validation, Writing – review & editing. RV: Supervision, Writing – review & editing. RR: Formal Analysis, Writing – review & editing. RB: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Di Spirito F, Cannatà D, Schettino V, Galdi M, Bucci R, Martina S. Perceived orthodontic needs and attitudes towards early evaluation and interventions: a survey-based study among parents of Italian school-aged children. Clin Pract. (2024) 14(3):1159–70. doi: 10.3390/clinpract14030092
2. Marsico E, Gatto E, Burrascano M, Matarese G, Cordasco G. Effectiveness of orthodontic treatment with functional appliances on mandibular growth in the short term. Am J Orthod Dentofacial Orthop. (2011) 39:24–36. doi: 10.1016/j.ajodo.2010.04.028
3. El-Huni A, Colonio Salazar FB, Sharma PK, Fleming PS. Understanding factors influencing compliance with removable functional appliances: a qualitative study. Am J Orthod Dentofacial Orthop. (2019) 155(2):173–81. doi: 10.1016/j.ajodo.2018.06.011
4. Borda AF, Garfinkle JS, Covell DA, Wang M, Doyle L, Sedgley CM. Outcome assessment of orthodontic clear aligner vs fixed appliance treatment in a teenage population with mild malocclusions. Angle Orthod. (2020) 90(4):485–90. doi: 10.2319/122919-844.1
5. Zybutz T, Drummond R, Lekic M, Brownlee M. Investigation and comparison of patient experiences with removable functional appliances: invisalign teen with mandibular advancement versus twin block. Angle Orthod. (2021) 91(4):490–5. doi: 10.2319/050520-393.1
6. Kaklamanos EG, Makrygiannakis MA, Athanasiou AE. Oral health-related quality of life throughout treatment with clear aligners in comparison to conventional metal fixed orthodontic appliances: a systematic review. Int J Environ Res Public Health. (2023) 20(4):3537. doi: 10.3390/ijerph20043537
7. Vaid NR. Digital technologies in orthodontics—an update. Semin Orthod. (2018) 24(4):373–5. doi: 10.1053/j.sodo.2018.10.001
8. Vaid N, Doshi V, Vandekar M. What’s “trend”ing in orthodontic literature? APOS Trends Orthod. (2016) 6:1–4. doi: 10.4103/2321-1407.125741
10. Bruni A, Serra FG, Gallo V, Deregibus A, Castroflorio T. The 50 most-cited articles on clear aligner treatment: a bibliometric and visualized analysis. Am J Orthod Dentofacial Orthop. (2021) 159(4):e343–62. doi: 10.1016/j.ajodo.2020.11.029
11. Abbate GM, Caria MP, Montanari P, Mannu C, Orrù G, Caprioglio A, et al. Parodontale gesundheit von teenagern mit herausnehmbaren alignern und festsitzenden kieferorthopädischen apparaturen. J Orofac Orthop. (2015) 76(3):240–50. doi: 10.1007/s00056-015-0285-5
12. Papadimitriou A, Mousoulea S, Gkantidis N, Kloukos D. Clinical effectiveness of invisalign® orthodontic treatment: a systematic review. Prog Orthod. (2018) 19:37. doi: 10.1186/s40510-018-0235-z
13. Haouili N, Kravitz ND, Vaid NR, Ferguson DJ, Makki L. Has invisalign improved? A prospective follow-up study on the efficacy of tooth movement with invisalign. Am J Orthod Dentofacial Orthop. (2020) 158(3):420–5. doi: 10.1016/j.ajodo.2019.12.015
14. Dianiskova S, Rongo R, Buono R, Franchi L, Michelotti A, D’Antò V. Treatment of mild class II malocclusion in growing patients with clear aligners versus fixed multibracket therapy: a retrospective study. Orthod Craniofac Res. (2022) 25(1):96–102. doi: 10.1111/ocr.12500
15. Pinho T, Rocha D, Ribeiro S, Monteiro F, Pascoal S, Azevedo R. Interceptive treatment with invisalign® first in moderate and severe cases: a case series. Children. (2022) 9(8):1176. doi: 10.3390/children9081176
16. Inchingolo AD, Dipalma G, Ferrara I, Viapiano F, Netti A, Ciocia AM, et al. Clear aligners in the growing patient: a systematic review. Children. (2024) 11(4):385. doi: 10.3390/children11040385
17. Lione R, Cretella Lombardo E, Paoloni V, Meuli S, Pavoni C, Cozza P. Upper arch dimensional changes with clear aligners in the early mixed dentition: a prospective study. J Orofac Orthop. (2023) 84(1):33–40. doi: 10.1007/s00056-021-00332-z
18. Levrini L, Carganico A, Abbate L. Maxillary expansion with clear aligners in the mixed dentition: a preliminary study with invisalign® first system. Eur J Paediatr Dent. (2021) 22(2):125–8. doi: 10.23804/ejpd.2021.22.02.7
19. Cretella Lombardo E, Fanelli S, Pavoni C, Cozza P, Lione R. Maxillary response induced by rapid palatal expansion vs. clear aligners: a short-term retrospective evaluation of the dento-alveolar effects in mixed dentition. Appl Sci. (2023) 13(15):8675. doi: 10.3390/app13158675
20. Lu L, Zhang L, Li C, Yi F, Lei L, Lu Y. Treatment effects after maxillary expansion using invisalign first system vs. acrylic splint expander in mixed dentition: a prospective cohort study. BMC Oral Health. (2023) 23(1):598. doi: 10.1186/s12903-023-03312-4
21. Wang J, Bukhari A, Tai SK, Zou B. Dimensional changes in the palate associated with invisalign first system: a pilot study. Angle Orthod. (2023) 93(5):524–30. doi: 10.2319/110422-755.1
22. Bruni A, Ferrillo M, Gallo V, Parrini S, Garino F, Castroflorio T, et al. Efficacy of clear aligners vs rapid palatal expanders on palatal volume and surface area in mixed dentition patients: a randomized controlled trial. Am J Orthod Dentofacial Orthop. (2024) 166(3):203–14. doi: 10.1016/j.ajodo.2024.04.006
23. Ravera S, Castroflorio T, Galati F, Cugliari G, Garino F, Deregibus A, et al. Short term dentoskeletal effects of mandibular advancement clear aligners in class II growing patients. A prospective controlled study according to STROBE guidelines. Eur J Paediatr Dent. (2021) 22(2):119–24. doi: 10.23804/ejpd.2021.22.02.6
24. Caruso S, Nota A, Caruso S, Severino M, Gatto R, Meuli S, et al. Mandibular advancement with clear aligners in the treatment of skeletal class II. A retrospective controlled study. Eur J Paediatr Dent. (2021) 22(1):26–30. doi: 10.23804/ejpd.2021.22.01.05
25. Sun Z, Pan Y, Lin T, Lu H, Ai H, Mai Z. Comparison of cephalometric measurements of the twin block and A6 appliances in the treatment of class II malocclusion: a retrospective comparative cohort study. Ann Transl Med. (2022) 10(16):876. doi: 10.21037/atm-22-3762
26. Cremonini F, Cervinara F, Siciliani G, Lombardo L. Class II treatment in growing patients: preliminary evaluation of the skeletal and dental effects of a new clear functional appliance. Appl Sci. (2022) 12(11):5622. doi: 10.3390/app12115622
27. Kong L, Liu XQ. Efficacy of invisible advancement correction for mandibular retraction in adolescents based on pancherz analysis. World J Clin Cases. (2023) 11(6):1299–309. doi: 10.12998/wjcc.v11.i6.1299
28. Lombardo EC, Lione R, Franchi L, Gaffuri F, Maspero C, Cozza P, et al. Dentoskeletal effects of clear aligner vs twin block—a short-term study of functional appliances. J Orofac Orthop. (2023) 85(5):317–26. doi: 10.1007/s00056-022-00443-1
29. Spencer Sonntag Blackham DMD by. A study of short-term skeletal, dental, and soft tissue effects of class ii malocclusions treated with invisalign® with mandibular advancement feature or twin block appliance compared with historical controls [Internet]. (cited 2023 Jun 11). Available online at: https://open.library.ubc.ca/soa/cIRcle/collections/ubctheses/24/items/1.0392341
30. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
31. da Costa Santos CM, de Mattos Pimenta CA, Nobre MRC. The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem. (2007) 15(3):508–11. doi: 10.1590/S0104-11692007000300023
32. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.5. Cochrane (2024). Available online at: www.training.cochrane.org/handbook (Updated August 2024).
33. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. Br Med J. (2019) 366:l4898. doi: 10.1136/bmj.l4898
34. Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. Br Med J. (2016) 355:i4919. doi: 10.1136/bmj.i4919
35. Chhibber A, Agarwal S, Yadav S, Kuo CL, Upadhyay M. Which orthodontic appliance is best for oral hygiene? A randomized clinical trial. Am J Orthod Dentofacial Orthop. (2018) 153(2):175–83. doi: 10.1016/j.ajodo.2017.10.009
36. Shen X, Yu Z. The effects of bracketless invisible orthodontics on the PLI, SBI, SPD, and GI and on the satisfaction levels in children with malocclusions. Am J Transl Res. (2021) 13(5):5066–72.34150093
37. Sifakakis I, Papaioannou W, Papadimitriou A, Kloukos D, Papageorgiou SN, Eliades T. Salivary levels of cariogenic bacterial species during orthodontic treatment with thermoplastic aligners or fixed appliances: a prospective cohort study. Prog Orthod. (2018) 19(1):25. doi: 10.1186/s40510-018-0230-4
38. Sharma R, Drummond R, Wiltshire W, Schroth R, Lekic M, Bertone M, et al. Quality of life in an adolescent orthodontic population. Angle Orthod. (2021) 91(6):718–24. doi: 10.2319/062820-592.1
39. Sauer MK, Drechsler T, Peron PF, Schmidtmann I, Ohlendorf D, Wehrbein H, et al. Aligner therapy in adolescents: first-year results on the impact of therapy on oral health-related quality of life and oral hygiene. Clin Oral Investig. (2022) 27(1):369–75. doi: 10.1007/s00784-022-04741-1
40. Lione R, Gazzani F, Moretti S, Danesi C, Cretella Lombardo E, Pavoni C. Gingival margins’ modifications during orthodontic treatment with invisalign first®: a preliminary study. Children. (2022) 9(10):1423. doi: 10.3390/children9101423
41. Dianiskova S, Bucci R, Solazzo L, Rongo R, Caruso S, Caruso S, et al. Patient and parental satisfaction following orthodontic treatment with clear aligners and elastodontic appliances during mixed dentition: a cross-sectional case–control study. Appl Sci. (2023) 13(7):4074. doi: 10.3390/app13074074
42. Chou B, Nickel JC, Choi D, Garfinkle JS, Freedman HM, Iwasaki LR. Outcome assessment of orthodontic clear aligner vs fixed appliance treatment in adolescents with moderate to severe malocclusions. Angle Orthod. (2023) 93(6):644–51. doi: 10.2319/020923-94.1
43. Favero R, Libralato L, Balestro F, Volpato A, Favero L. Edge level of aligners and periodontal health: a clinical perspective study in young patients. Dental Press J Orthod. (2023) 28(1):e2321124. doi: 10.1590/2177-6709.28.1.e2321124.oar
44. da Silva VM, Ayub PV, Massaro C, Janson G, Garib D. Comparison between clear aligners and 2 × 4 mechanics in the mixed dentition: a randomized clinical trial. Angle Orthod. (2023) 93(1):3–10. doi: 10.2319/032322-237.1
45. Cretella Lombardo E, Paoloni V, Fanelli S, Pavoni C, Gazzani F, Cozza P. Evaluation of the upper arch morphological changes after two different protocols of expansion in early mixed dentition: rapid maxillary expansion and invisalign® first system. Life. (2022) 12(9):1323. doi: 10.3390/life12091323
46. Lione R, Paoloni V, De Razza FC, Pavoni C, Cozza P. The efficacy and predictability of maxillary first molar derotation with invisalign: a prospective clinical study in growing subjects. Appl Sci. (2022) 12(5):2670. doi: 10.3390/app12052670
47. Gonçalves A, Ayache S, Monteiro F, Silva FS, Pinho T. Efficiency of invisalign first® to promote expansion movement in mixed dentition: a retrospective study and systematic review. Eur J Paediatr Dent. (2023) 24(2):112–23. doi: 10.23804/ejpd.2023.1754
48. Bahammam M, El-Bialy T. Comparison of alveolar bone thickness and height after slow expansion using quad-helix or clear aligners. Saudi Dent J. (2023) 35(3):255–62. doi: 10.1016/j.sdentj.2023.02.006
49. Sabouni W, Hansa I, Al Ali SM, Adel SM, Vaid N. Invisalign treatment with mandibular advancement: a retrospective cohort cephalometric appraisal. J Clin Imaging Sci. (2022) 12:42. doi: 10.25259/JCIS_64_2022
50. Wu Y, Yu Q, Xia Y, Wang B, Chen S, Gu K, et al. Does mandibular advancement with clear aligners have the same skeletal and dentoalveolar effects as traditional functional appliances? BMC Oral Health. (2023) 23(1):65. doi: 10.1186/s12903-023-02709-5
51. Rongo R, Dianišková S, Spiezia A, Bucci R, Michelotti A, D’Antò V. Class II malocclusion in adult patients: what are the effects of the intermaxillary elastics with clear aligners? A retrospective single center one-group longitudinal study. J Clin Med. (2022) 11(24):7333. doi: 10.3390/jcm11247333
52. Sabouni W, Eichelberger A, Des Georges O. Traitement des classes II pour les patients au cours de la croissance par gouttières thermoformées: quel protocole? Orthod Fr. (2019) 90(1):13–27. doi: 10.1051/orthodfr/2019003
53. Jiang Q, Li J, Mei L, Du J, Levrini L, Abbate GM, et al. Periodontal health during orthodontic treatment with clear aligners and fixed appliances. The Journal of the American Dental Association. (2018) 149(8):712–20.e12. doi: 10.1016/j.adaj.2018.04.010
54. Favero R, Volpato A, Favero L. Managing early orthodontic treatment with clear aligners. J Clin Orthod. (2018) 52(12):701–9.30576293
55. D’Antò V, Valletta R, De Simone V, Pisano M, Martina S. Clear aligners treatment of class III subdivision with an extraction of a lower bicuspid. Int J Environ Res Public Health. (2023) 20(4):3550. doi: 10.3390/ijerph20043550
56. Bocchino T, Martina S, Sangiuolo C, Galdi M, Valletta A, D’Antò V. Maxillary impacted canine and upper lateral incisor agenesis treatment with “canine first technique” and clear aligners: a case report. Healthcare. (2023) 11(16):2345. doi: 10.3390/healthcare11162345
57. Bruni A, Abate A, Maspero C, Castroflorio T. Comparison of mechanical behavior of clear aligner and rapid palatal expander on transverse plane: an in vitro study. Bioengineering. (2024) 11(2):103. doi: 10.3390/bioengineering11020103
58. Männchen R, Serafin M, Fastuca R, Caprioglio A. Does early treatment improve clinical outcome of class II patients? A retrospective study. Children. (2022) 9(2):232. doi: 10.3390/children9020232
59. Pango Madariaga AC, Bucci R, Rongo R, Simeon V, D’Antò V, Valletta R. Impact of fixed orthodontic appliance and clear aligners on the periodontal health: a prospective clinical study. Dent J (Basel). (2020) 8(1):4. doi: 10.3390/dj8010004
60. Di Spirito F, D’Ambrosio F, Cannatà D, D’Antò V, Giordano F, Martina S. Impact of clear aligners versus fixed appliances on periodontal Status of patients undergoing orthodontic treatment: a systematic review of systematic reviews. Healthcare. (2023) 11(9):1340. doi: 10.3390/healthcare11091340
61. Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Periodontal health during clear aligners treatment: a systematic review. Eur J Orthod. (2015) 37(5):539–43. doi: 10.1093/ejo/cju083
62. Flores-Mir C, Brandelli J, Pacheco-Pereira C. Patient satisfaction and quality of life status after 2 treatment modalities: invisalign and conventional fixed appliances. Am J Orthod Dentofacial Orthop. (2018) 154(5):639–44. doi: 10.1016/j.ajodo.2018.01.013
Keywords: clear aligners appliance, mixed dentition, early treatment, interceptive treatment, functional orthodontic
Citation: D’Antò V, De Simone V, Caruso S, Bucci P, Valletta R, Rongo R and Bucci R (2025) Effects of clear aligners treatment in growing patients: a systematic review. Front. Oral. Health 5:1512838. doi: 10.3389/froh.2024.1512838
Received: 17 October 2024; Accepted: 16 December 2024;
Published: 6 January 2025.
Edited by:
Riccardo Nucera, University of Messina, ItalyReviewed by:
Alessandro Bruni, University of Modena and Reggio Emilia, ItalyVinicius Augustus Merino Da Silva, University of São Paulo, Brazil
Copyright: © 2025 D'Antò, De Simone, Caruso, Bucci, Valletta, Rongo and Bucci. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosaria Bucci, cm9zYXJpYS5idWNjaUB1bmluYS5pdA==