 Kateryna Lokes1*
Kateryna Lokes1* Anatolii Kiptilyi1
Anatolii Kiptilyi1 Margaryta Skikevych1
Margaryta Skikevych1 Dmytro Steblovskyi1
Dmytro Steblovskyi1 Vitaliy Lychman1
Vitaliy Lychman1 Serhii Bilokon2
Serhii Bilokon2 David Avetikov1
David Avetikov1
- 1Department of Oral and Maxillofacial Surgery, Poltava State Medical University, Poltava, Ukraine
- 2Department of Pediatric Oral Surgery, Poltava State Medical University, Poltava, Ukraine
: Odontogenic infections can become life-threatening. The aim of the study was to determine the effectiveness of quercitin and its combination with ethylmethylhydroxypyridine succinate in the complex treatment of odontogenic infections by assessing the microbial population of the infection site.
Materials and methods: The cross-sectional study included 75 patients. Purulent exudate was collected from the infection site. The number of colony-forming units was counted using the standard plate method.
Results: The microbiological examination of purulent exudate obtained from the patients revealed the general prevalence of Gram-positive cocci. On the seventh day of treatment, the total number of microorganisms in the purulent exudate of patients in group I, whose treatment included a combination of the standard protocol with quercitin, significantly decreased compared to the first day of the same group. The results of treatment of patients in group II, which included the standard protocol in combination with quercitin and 2-ethyl-6-methyl-3-hydroxypyridine succinate, demonstrate a significant decrease in the total number of bacteria in the infection focus on the fifth day of treatment compared to this indicator of the group at the beginning of the study.
Conclusions: When quercitin was used as part of complex treatment, the total treatment period was reduced by 1.4 days. However, the combined use of quercitin and ethylmethylhydroxypyridine succinate against the background of standard treatment of patients with odontogenic infection contributed to a reduction in hospital stay by 2 days.
1 Introduction
About 30.0% of patient visits for emergency surgical care are associated with odontogenic infection in highly developed countries, and in developing countries this figure is even higher (1, 2). Odontogenic diseases of maxillofacial localization are characterized by a rapid aggressive course against the background of a sharp deterioration in the patient's general condition with further spread of inflammation from one anatomical part to another. That is why today, despite the rapid development of surgical dentistry, the mortality rate associated with odontogenic infection in the world ranges from 10.0% (3, 4).
Odontogenic infections can become life-threatening if left untreated, and increase the physical costs of treatment for the patient and the financial costs for the health care system (1, 5). Therefore, the issue of improving the effectiveness of treatment of odontogenic diseases of the maxillofacial area by combining standard treatment protocols with new substances that have anti-inflammatory, antimicrobial, immunomodulatory or other properties is a priority for both scientists and practitioners.
For example, quercitin is a type of natural flavonoid, which has recently been widely used in medicine due to its rich spectrum of bioactive properties. The anti-apoptotic, anti-inflammatory, antioxidant and antibacterial effects of quercitin make it a potential substance for the development of new therapeutic combinations. That is why quercitin is used to treat such diseases as bone metabolic diseases, gastrointestinal diseases, cardiovascular, cerebrovascular diseases and dental infections. However, the quantitative evidence base for the use of quercitin is currently insufficient and it is more often used as a dietary supplement (6).
2-ethyl-6-methyl-3-hydroxypyridine is most often crystallized in the form of succinate to achieve antioxidant, nootropic, neuroprotective, anti-inflammatory and other pharmacological effects. Preliminary studies prove the role of ethylmethylhydroxypyridine succinate in enhancing the antibacterial action of some antibiotics. Therefore, it is interesting to study the use of 2-ethyl-6-methyl-3-hydroxypyridine succinate in combination with other substances to identify possible synergism (7).
It is known that odontogenic diseases have a bacterial genesis and develop as a result of the spread of pathogens in necrotized pulp in complicated caries, periodontal pockets in periodontitis or pericoronitis in case of difficult eruption of retained teeth into the underlying tissues (2, 4). It becomes obvious that, along with pathogenic representatives, the oral normobiota in such cases can acquire pathogenic properties and serve as a reservoir of infection (8). Given this fact, the microbial population of the infection focus is the target of etiotropic treatment and can act as markers of its effectiveness (9, 10).
Therefore, the aim of the study was to determine the effectiveness of quercitin and its combination with ethylmethylhydroxypyridine succinate in the complex treatment of odontogenic phlegmon and maxillofacial abscesses by assessing the microbial population of the infection site.
2 Materials and methods
2.1 Study population
The cross-sectional study included 75 patients who were treated for abscesses and phlegmon of the facial area in the Department of Maxillofacial Surgery of the Municipal Enterprise “M.V. Sklifosovsky Poltava Regional Clinical Hospital of the Poltava Regional Council” during 2023. The criteria for inclusion of patients in the study were: a clinical diagnosis of L02.00—facial skin abscess, L03.20—facial phlegmon according to ICD-10 of odontogenic genesis with the involvement of no more than two tissue spaces with the patient's personal consent to participate in the study. The exclusion criteria were: inconsistency of diagnosis L02.00 and L03.20 according to ICD-10, spread of the infectious process to three or more tissue spaces, diabetes mellitus, pregnancy, mental disorders, congenital and acquired immunodeficiencies, self-medication with antibiotics before admission to the hospital, and lack of desire to participate in the study.
Prior to the study, written informed consent was obtained from each participant after a detailed explanation of the purpose and protocols of the study, which were in line with the ethical principles of the Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects. The study was approved by the Biomedical Ethics Committee of PSMU (Minutes No.220, from 25.10.2023).
Patients were empirically divided into three groups with an even distribution of patients by age and gender (Figure 1).
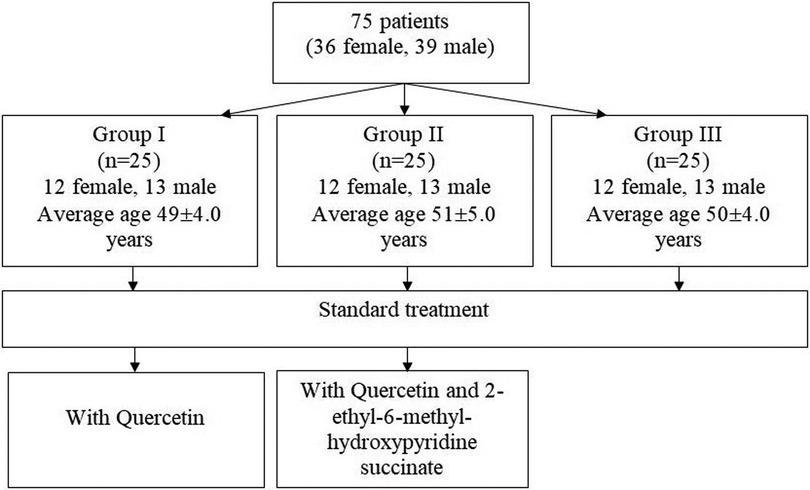
Figure 1. Flowchart of distribution of patients by groups.
All patients (the first, second and third groups) underwent standard treatment according to the protocol, which included extraction of the causative tooth/teeth or roots, dissection of the infection site, followed by antiseptic treatment with 0.5% chlorhexidine and drainage with a corrugated rubber drain. Antibiotic therapy included Ceftriaxone 1.0 g 12-hourly and Metronidazole 100 mg daily. If it was necessary to replace the above antibacterial agents in case of allergy, the patient was automatically excluded from the study group. Pain control was performed with Ibuprofen 400 mg three times daily.
In patients included in the first group, conservative therapy included quercitin 1 g two times a day for 14 days (Quercitin, PJSC “Research and Production Center ‘Borshchahivskiy Chemical and Pharmaceutical Plant’”, Kyiv, Ukraine) additionally. The contents of a sachet with granules (2 g) were dissolved in 10 ml of water at about 50 degrees Celsius and infused for 15 min until homogeneous.
The standard treatment of patients in the second group included quercitin 1 g two times a day in combination with intravenous drip administration of 2-ethyl-6-methyl-3-hydroxypyridine succinate according to the regimen (Armadin, LLC SPC “Microkhim”, Rubizhne, Ukraine) additionally to the standard treatment:
1st day 50 mg 2 two times a day
2–3 days, 100 mg 2 two times a day
4th day, 100 mg 1 two times a day
5–6 days, 50 mg 1 two times a day
2.2 Microbiological studies
Purulent exudate was collected from the infection site using a sterile probe-tampon and placed in tubes with Amies medium for further transportation to the bacteriological laboratory of the Department of Microbiology, Virology and Immunology of PSMU within 24 h on the first, third, fifth, seventh, ninth, tenth and eleventh days of treatment. The samples were cultured on Columbia agar with 5% sheep blood (bioMarieux, France) and Thioglycolic medium (bioMarieux, France), at 37 °C under aerobic atmosphere for 24 h followed by culture isolation by standard culture method. The number of colony-forming units (CFUs) was counted using the standard plate method and expressed in decimal logarithms (lg). The conclusion about the etiological significance of the microorganism in the infectious-inflammatory process was made after isolation of microorganism in a monoculture or in the amount of 106 CFUs or more. The final identification of isolates was carried out by morphological, tinctorial, cultural and biochemical characteristics using STROPTOtest 24, STAPHYtest 24 and ENTEROtest 16 (Erba, Czech Republic), according to the manufacturer's instructions.
2.3 Statistical analysis
The variational and statistical processing of the study results was performed using Microsoft Excel 2019 and 2022 GraphPad Software with the determination of the main variational indicators: mean values (M), standard errors (m), p-value (p). A one-way analysis of variance (ANOVA: one factor) was used to compare the results of the three groups of data. The Bonferroni correction adjusted the significance level to control for the overall probability of errors (false positives) for testing multiple hypotheses. The result was considered significant if the p-value was less than 0.05.
3 Results
The microbiological examination of purulent exudate obtained from the foci of odontogenic infection revealed the general prevalence of Gram-positive cocci (Table 1).
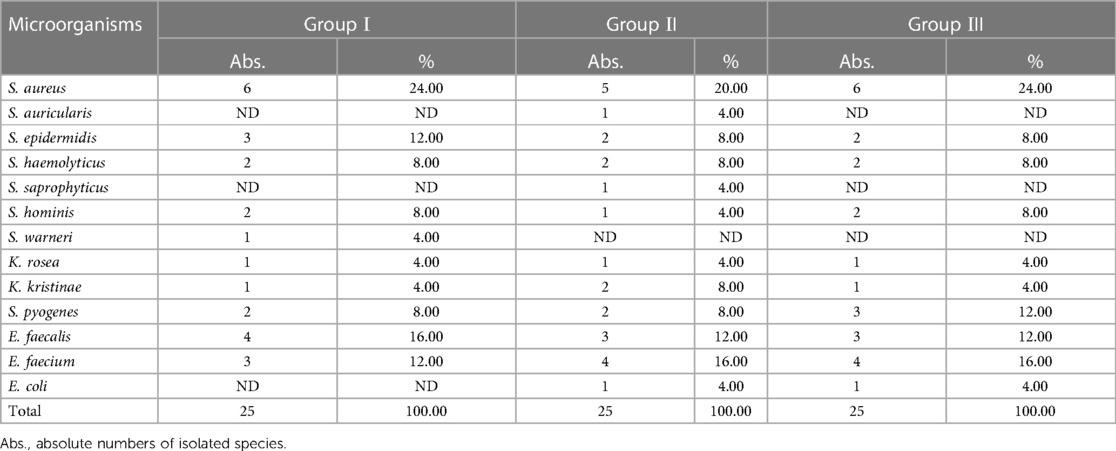
Table 1. Characterization of the qualitative composition of the microbiota of infection foci in phlegmon and abscesses of maxillofacial localization.
Representatives of the genus Staphylococcus were isolated on average from 50.67% of patients, 22.67% of which were S. aureus isolates. The most numerous species among coagulase-negative staphylococci (CoNS) were Staphylococcus epidermidis (S. epidermidis) and Staphylococcus haemolyticus (S. haemolyticus), with a frequency of 9.33% and 8.00%, respectively. Representatives of the genus Enterococcus were isolated in more than a quarter of patients (28.00%). Moreover, E. faecalis and E. faecium were found with almost equal frequency among patients of all three groups. It is worth noting that Streptococcus spp. as pathogens of maxillofacial abscesses and phlegmon were identified in only 7 patients, which was 9.33% of cases. A similar result was demonstrated by K. rosea and K. kristinae, the proportion of which was 9.33% in total. In turn, Gram-negative bacilli were isolated among the causative agents of abscesses and phlegmon of maxillofacial localization in only two patients, accounting for 2.67% of the total microbiota of the infection sites.
According to the results of the study, the total number of microorganisms colonizing the infection site in conditions of maxillofacial abscesses and phlegmon was on average 9.05 ± 0.50 log CFUs/ml. It is worth noting that the total microbial load in the three groups of patients on the day of admission to the hospital was at the same level and did not differ significantly (Table 2).
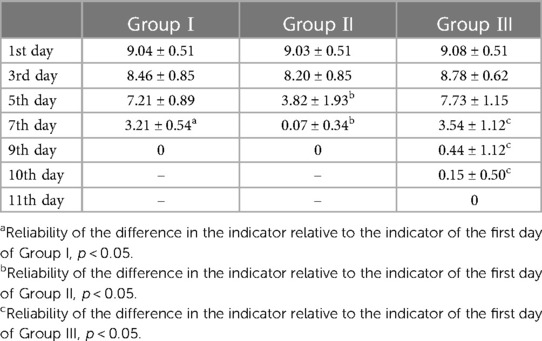
Table 2. Dynamics of microbial colonization of postoperative wounds in phlegmon and maxillofacial abscesses according to the type of treatment, CFUs/ml, log.
Despite the fact that on the third and fifth days of treatment in patients of group I, the total microbial colonization of the infection sites decreased by 0.58 log and 1.83 log, respectively, the results did not have a significant difference from the baseline. It is worth noting that only on the seventh day of treatment, a significant decrease of 5.83 log in the total number of microorganisms in the purulent exudate of patients in group I, whose treatment included a combination of the standard protocol with quercitin, was observed compared to the first day of the same group (р < 0.05).
Analyzing the results of treatment of patients in group II, a slightly faster antimicrobial effect can be noted, as a significant decrease in the total number of bacteria by 5.21 log in the infection site was determined on the fifth day of treatment compared to this group at the beginning of the study (р < 0.05). However, there was one patient in this group with a severe course, who continued to isolate microorganisms in the amount of 1.70 log CFU/ml from the surgical wound on day 7 of treatment. Therefore, the complete eradication of microorganisms in patients in groups I and II was established on day 9 of the study.
In contrast, when treated according to the standard protocol, patients in group III showed a significant decrease in microbial colonization by 5.54 logs only on day seven, compared with the baseline of this group of patients (р < 0.05). However, on the ninth day, there were still 4 patients (16.0%), and on the tenth day, 2 (8.0%), whose purulent exudate was found to contain microorganisms. Therefore, complete eradication of postoperative wounds in patients of group III was recorded only on the eleventh day of treatment.
The data of microbiological studies correlated with the clinical data of objective examination of patients. Thus, a significant decrease in the number of microorganisms in the postoperative wound, compared with this indicator on the first day of treatment, coincided in time with a decrease or complete absence of purulent discharge, the appearance of granulations in the wound, and a decrease in collateral edema.
The study found that the average duration of treatment of maxillofacial abscesses and phlegmon according to the standard protocol was 8.4 ± 0.96 days. When quercitin was used as part of a complex treatment, this period was reduced by 1.4 days. However, the combined use of quercitin and ethylmethylhydroxypyridine succinate against the background of standard treatment of patients with odontogenic infection helped to reduce the length of stay in the hospital to an average of 6.1 ± 0.4 days.
4 Discussion
The frequency of isolation of staphylococci as a causative agent of inflammatory processes does not exceed 30%. About 15.0% of cases are isolates of S. aureus and the rest of them—coagulase-negative staphylococci. According to the literature, it is clear that Gram-positive cocci, including genera of Staphylococcus, Streptococcus, and Enetrococcus, prevail in the development of odontogenic infections of soft tissues (4, 11). The results obtained by us fully confirm this fact. After all, Gram-positive cocci have a wide arsenal of virulence factors, such as surface proteins that provide adhesion to epithelial cells, the ability to form biofilms and penetrate the bloodstream with subsequent spread throughout the body. All this contributes to the development of severe septic conditions (4, 8, 11).
The obtained results demonstrate the effectiveness of the standard protocol for the treatment of phlegmon and maxillofacial abscesses with the addition of quercitin or its combination with ethylmethylhydroxypyridine succinate.
In the last decade, a significant number of scientific studies have emerged indicating the use of flavanoids, including quercitin, in the treatment of metabolic bone diseases, gastrointestinal disorders, cardiovascular disorders, immunosuppression, and cerebrovascular diseases, including Alzheimer's disease (12–14). Preliminary in vitro studies prove the antimicrobial effect of different concentrations of quercitin on bacteria of different groups and fungi. Moreover, Gram-positive microorganisms showed the greatest sensitivity to this flavonoid (15, 16). Given the wide potential of quercitin bioactivity, the results of its use in the complex therapy of patients with phlegmon and maxillofacial abscesses were quite natural. After all, it has been previously proven that quercitin promotes the regeneration of hard and soft tissues of the human body by inhibiting the inflammatory mediator PGE2 and increasing the activity of alkaline phosphatase (17). In addition, this flavonoid suppresses the expression of cytokines and inducible nitric oxide synthase due to its ability to inhibit the NF-kappaB pathway without modifying the activity of c-Jun N-terminal kinase (18). We observed a significant decrease in the number of microorganisms in the infection site when quercitin was administered as part of the complex treatment of patients, which could be due to its ability to block the surface proteins of Gram-positive bacteria responsible for adhesion and biofilm formation (19, 20). Due to its antioxidant properties, anti-inflammatory, immunomodulatory, and antimicrobial effects, and the presence of an analgesic effect, quercitin promotes faster wound cleansing and healing and is quite promising for use in surgical dentistry (11).
It is known that 2-ethyl-6-methyl-3-hydroxypyridine succinate has anti-ischemic, antihypoxic, neuroprotective, anti-stress, nootropic, and geroprotective properties, so it is widely used in neurology, cardiology, and surgery (21, 22). Recently, there have been reports on the antibacterial effect of 2-ethyl-6-methyl-3-hydroxypyridine succinate, namely its ability to inhibit the growth of Staphylococcus spp., Streptococcus spp., E. coli, and yeast-like fungi of the genus Candida (22). Given the fact that among the microorganisms isolated by us from patients with phlegmon and maxillofacial abscesses, representatives of the genera Staphylococcus and Streptococcus prevailed, it is natural to reduce the overall microbial population of surgical wounds when using the drug as part of complex therapy (23). The authors are of the opinion that 2-ethyl-6-methyl-3-hydroxypyridine succinate has a bacteriostatic effect by inhibiting protein synthesis in the microbial cell, and also affects the structure and function of membranes and surface proteins (21).
In addition, 2-ethyl-6-methyl-3-hydroxypyridine succinate has been shown to have synergistic effects with traditional antimicrobials, enhancing their activity against microorganisms in vitro (21). Therefore, when it is combined with conventional treatment and quercitin, it is also possible to potentiate the effect of both the latter and the antibiotic used. However, this fact requires further investigation.
5 Conclusion
Gram-positive cocci, mainly Staphylococcus spp. and Streptococcus spp. play a dominant role in purulent exudate obtained from foci of odontogenic infection.
On the seventh day of treatment, the total number of microorganisms in the purulent exudate of patients in group I, whose treatment included a combination of the standard protocol with quercitin, significantly decreased by 5.83 log compared to the first day of the same group. The results of treatment of patients in group II, which included the standard protocol in combination with quercitin and 2-ethyl-6-methyl-3-hydroxypyridine succinate, demonstrate a significant decrease in the total number of bacteria by 5.21 log in the infection focus on the fifth day of treatment compared to this indicator of the group at the beginning of the study.
When quercitin was used as part of complex treatment, the total treatment period was reduced by 1.4 days. However, the combined use of quercitin and ethylmethylhydroxypyridine succinate against the background of standard treatment of patients with odontogenic infection contributed to a reduction in hospital stay to an average of 6.1 ± 0.4 days.
5.1 Limitations of the study
The study was conducted during the wartime, which may have affected the results due to the increased use of antibiotics and antiseptics.
The study only included bacteria from the patients of one hospital, which may limit the generalizability of the findings to other clinics.
The study only considered a limited number of antioxidants and did not explore the effectiveness of others.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Biomedical Ethics Committee of PSMU (Minutes No. 220, from 25.10.2023). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KL: Conceptualization, Methodology, Supervision, Writing – original draft. AK: Data curation, Formal analysis, Investigation, Software, Writing – original draft, Writing – review & editing. MS: Data curation, Methodology, Resources, Software, Writing – review & editing. DS: Formal analysis, Investigation, Visualization, Writing – review & editing. VL: Data curation, Investigation, Methodology, Writing – review & editing. SB: Data curation, Investigation, Software, Supervision, Writing – review & editing. DA: Project administration, Supervision, Validation, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fu B, McGowan K, Sun JH, Batstone M. Increasing frequency and severity of odontogenic infection requiring hospital admission and surgical management. Br J Oral Maxillofac Surg. (2020) 58(4):409–15. doi: 10.1016/j.bjoms.2020.01.011
2. Ullah M, Irshad M, Yaacoub A, Carter E, Thorpe A, Zoellner H, et al. Dental infection requiring hospitalisation is a public health problem in Australia: a systematic review demonstrating an urgent need for published data. Dent J (Basel). (2023) 11(4):97. doi: 10.3390/dj11040097
3. Pham Dang N, Delbet-Dupas C, Mulliez A, Devoize L, Dallel R, Barthélémy I. Five predictors affecting the prognosis of patients with severe odontogenic infections. Int J Environ Res Public Health. (2020) 17(23):8917. doi: 10.3390/ijerph17238917
4. Faustova M, Nazarchuk O, Avetikov D, Ananieva M, Chumak Y, Havryliev V. Microbiological aspects concerning the etiology of acute odontogenic inflammatory diseases in the soft tissues of the head and neck region. Open Access Maced J Med Sci. (2022) 10(F):636–40. doi: 10.3889/oamjms.2022.10535
5. Avetikov DS, Lychman VO, Lokes KP, Steblovsky DV, Bondarenko VV, Shlykova OA, et al. Treatment of odontogenic phlegmons in patients taking into account the biorithm of life. Wiad Lek. (2021) 74(6):1346–8. doi: 10.36740/WLek202106111
6. Chen J, Li G, Sun C, Peng F, Yu L, Chen Y, et al. Chemistry, pharmacokinetics, pharmacological activities, and toxicity of quercitrin. Phytother Res. (2022) 36(4):1545–75. doi: 10.1002/ptr.7397
7. Bobrova NA, Vazhnichaya EM, Loban GA, Faustova MO, Ananieva MM. Staphylococcus warneri clinical isolate susceptibility to antibiotics and its modification by emoxypine. Int J Med Med Res. (2020) 6(1):61–7. doi: 10.11603/ijmmr.2413-6077.2020.1.10893
8. Faustova MO, Ananieva MM, Basarab YO, Dobrobolska OV, Vovk IM, Loban GA. Bacterial factors of cariogenicity (literature review). Wiad Lek. (2018) 71(2 Pt 2):378–82.29786589
9. Nazarchuk O, Dmyrtriiev D, Babina Y, Faustova M, Burkot V. Research of the activity of local anesthetics and antiseptics regarding clinical isolates of Acinetobacter baumannii as pathogens of postoperative infectious complications. Acta Biomed. (2022) 93:e2022003. doi: 10.23750/abm.v93i1.11842
10. Petrushanko TA, Tchereda VV, Loban GA. The screening diagnostic of micro ecological disorders of oral cavity. Klin Lab Diagn. (20146) 6:48–50 (in Russian).25335401
11. Nazarchuk O, Faustova M, Kolodii S. Microbiological characteristics of infectious complications, actual aspects of their prevention and treatment in surgical patients. Novosti Khirurgii. (2019) 3:318–27. doi: 10.18484/2305-0047.2019.3.318
12. Ananieva ММ, Faustova MO, Loban’ GA, Avetikov DS, Basarab YO, Ksonz VI. Microbiological aspects of chlorophyllipt extract used for prevention of candida postoperative complications. EuroMediterranean Biomed J. (2018) 13:178–80. doi: 10.3269/1970-5492.2018.13.40
13. Aborode AT, Pustake M, Awuah WA, Alwerdani M, Shah P, Yarlagadda R, et al. Targeting oxidative stress mechanisms to treat Alzheimer’s and Parkinson’s disease: a critical review. Oxid Med Cell Longev. (2022) 2022:7934442. doi: 10.1155/2022/7934442
14. Wang L, Sun J, Miao Z, Jiang X, Zheng Y, Yang G. Quercitrin improved cognitive impairment through inhibiting inflammation induced by microglia in Alzheimer’s disease mice. Neuroreport. (2022) 33(8):327–35. doi: 10.1097/WNR.0000000000001783
15. Lupoae P, Cristea V, Borda D, Lupoae M, Gurau G, Dinica RM. Phytochemical screening: antioxidant and antibacterial properties of Potamogeton Species in order to obtain valuable feed additives. J Oleo Sci. (2015) 64(10):1111–23. doi: 10.5650/jos.ess15023
16. Nayeem N, Karvekar M. Anti microbial and anti-oxidant properties of the isolated compounds from the methanolic extract from the leaves of Tectona grandis. J Basic Clin Pharm. (2011) 2(4):163–5.24826018
17. Gómez-Florit M, Monjo M, Ramis JM. Quercitrin for periodontal regeneration: effects on human gingival fibroblasts and mesenchymal stem cells. Sci Rep. (2015) 5:16593. doi: 10.1038/srep16593
18. Comalada M, Camuesco D, Sierra S, Ballester I, Xaus J, Gálvez J, et al. In vivo quercitrin anti-inflammatory effect involves release of quercetin, which inhibits inflammation through down-regulation of the NF-kappaB pathway. Eur J Immunol. (2005) 35(2):584–92. doi: 10.1002/eji.200425778
19. Hasan S, Singh K, Danisuddin M, Verma PK, Khan AU. Inhibition of major virulence pathways of Streptococcus mutans by quercitrin and deoxynojirimycin: a synergistic approach of infection control. PLoS One. (2014) 9(3):e91736. doi: 10.1371/journal.pone.0091736
20. Dolzhkovyi S, Cherkun O, Sheyko V, Kasian V, Hryn V. Infectious complications of acute pancreatitis: spectrum of causative agents and approaches to antibacterial therapy. Surgical Chronicles. (2021) 26(1):22–4.
21. Vazhnichaya EM, Bobrova NA, Devyatkina TA, Loban’ GA, Devyatkina NN. Influence of emoxypine and mexidol on the development of cultures of etalon strains of microorganisms and their susceptibility to antibiotics. Exp Clin Pharm. (2019) 2:16–20. doi: 10.30906/0869-2092-2019-82-2-16-20 (in Russian).
22. Lyakhovskyi VI, Lobahn GA, Gancho OV, Vazhnycha OM, Kolomiyets SV, Jaber V. Dynamics of bacteriological and planimetric indices of the wound under the action of the silver nanoparticles, stabilized by mexidol and polyvinylpyrrolidone. Klin Khir. (2016) 4:67–9 (in Ukrainian).
Keywords: odontogenic infections, quercitin, 2-ethyl-6-methyl-3-hydroxypyridine succinate, phlegmones, abscesses, maxillofacial area
Citation: Lokes K, Kiptilyi A, Skikevych M, Steblovskyi D, Lychman V, Bilokon S and Avetikov D (2024) Microbiological substantiation of the effectiveness of quercitin and its combination with ethylmethylhydroxypyridine succinate in the complex treatment of odontogenic phlegmon and maxillofacial abscesses. Front. Oral. Health 5:1338258. doi: 10.3389/froh.2024.1338258
Received: 14 November 2023; Accepted: 9 January 2024;
Published: 19 January 2024.
Edited by:
Sameh Attia, Justus-Liebig University Giessen, GermanyReviewed by:
Dmytro Dmytriiev, National Pirogov Memorial Medical University, UkraineCarla Paola Lozano, University of Chile, Chile
© 2024 Lokes, Kiptilyi, Skikevych, Steblovskyi, Lychman, Bilokon and Avetikov. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kateryna Lokes ay5sb2tlc0BwZG11LmVkdS51YQ==