 Vanda Urzal
Vanda Urzal Tainá Iunes
Tainá Iunes Afonso Pinhão-Ferreira2
Afonso Pinhão-Ferreira2

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Oral. Health, 06 July 2023
Sec. Preventive Dentistry
Volume 4 - 2023 | https://doi.org/10.3389/froh.2023.1235134
Crossbite is an alteration of the interarch relationship (1) that can occur in the anterior, posterior, or both regions (2). Worldwide, the prevalence of malocclusion is 56% (3), being 10% of crossbite in primary dentition, 11% in mixed dentition, and 5% in permanent dentition. Etiology is multifactorial (4) and may be related to heredity, oral breathing, sucking habits, and factors of occlusal kinetic origin (e.g., interference caused by deciduous canines) among others (5, 6).
The early diagnosis of this anomaly is essential to reduce the risk of dental, alveolar, and skeletal malocclusions. According to the severity of the established malocclusion, it may also present an aesthetic issue with psychosocial impact (7). The age at which the therapy is performed has psychological effects on the patient (8) and the occurrence of crossbite in primary dentition promote altered craniofacial growth with deleterious consequences that are proportional to the child's chronological age (9).
In pediatric patients, this orthodontic treatment is controversial. For some clinicians, crossbite resolution in the primary dentition will occur through physiological self-correction based on the growth process, although for others the treatment should be done in mixed dentition or when almost all permanent teeth are erupted (7, 10). Furthermore, in specific cases of crossbite intervention in primary dentition may also prevent an increasing abnormal skeletal growth that could lead to functional and aesthetic disorders (11).
This study aims to present a new treatment technique for children with crossbite, with the goal of reducing possible severe craniofacial treatments in the future.
Buttons and elastic chains are applying in a four-year-old child patient with an anterior and unilateral crossbite of the dental arches, whose etiological factor of such dysmorphia was the lateral deviation of the mandible in the kinesics of closure (Figure 1).

Figure 1. Pre-treatment of extraoral and intraoral photographs.
The treatment was carried out using four attachments to dental surface and an elastic chain. Control of the device was done carefully at short periods of time (Figure 2).

Figure 2. Intraoral photographs during treatment.
With this simple device, the correction of this malocclusion was achieved in four months, improving the dental inter-arch relationship, and promoting bilateral simultaneous skeletal growth (Figure 3). This technique has abolished the inconvenience of using a removable orthodontic appliance at this very tender age when children are not aware of treatment and the compliance is reduced.
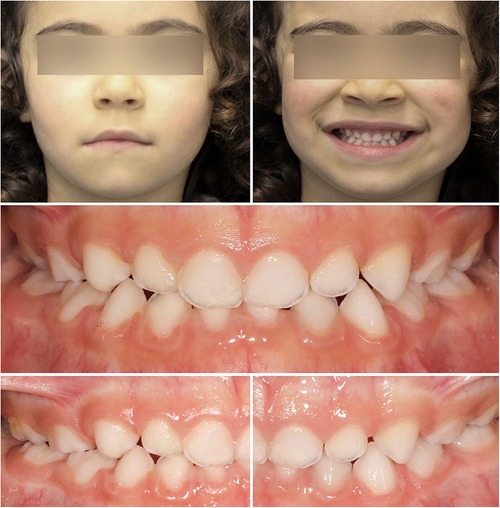
Figure 3. Post-treatment extraoral and intraoral photographs.
Elastic chains introduced in the 1960s, composed of polyurethane, are used to close or prevent spaces (12) and have such advantages as easy use, a decrease in intraoral trauma, a large range of different colors, a cost-effectiveness and a low compliance required from patients. Their behavior has been studied in many aspects: force decay over time (13–16), force decay at different levels of activation (13, 17), simulated space closure (15, 16, 18), pre stretching of elastic chains (13, 19) (causing 5% less force decrease), environmental factors and storage media (14, 19, 20) and the chains designs (13, 18).
Over time the elastic chains decrease their strength, so selecting the best quality is important. The force applied in orthodontics is complex (21) and is related to several factors: individual tissue reaction, type of applied force, and biomechanical principles involved. In any research the force, besides being measured, should be very light at its beginning, to avoid areas of hyalinization in the periodontal fibers on the pressure side. The ideal start force should be 40 gf in young people and 25 gf in adults (22). There are three types of forces: continuous, interrupted continuous, and intermittent. This is directly related to the reaction of the tissues and mechanical principles involved: a tooth with a short root will be tipped considerably and the supporting tissues will respond more favorably to interrupted or intermittent forces than to a continuous one (22). The adult tooth is tipped less than the young one due to the apical fiber bundle, and in this case, light continuous forces must be applied. In both cases, the force applied per square millimeter is higher in tipping compared to bodily movement.
Early treatment is effective and desirable in certain situations, with the clinician deciding, on a case-by-case analysis, when to perform it (23). The association of aesthetic buttons applied to the teeth with an elastic chain, and the application of a very light force, in other words, gentle stretching of the initial length of the rings, is a challenge for the possibility of earlier treatment, with less psychological interference, avoiding the patient's cooperation and preventing asymmetrical facial growth. Thus, earliest the treatment is delivered, short is the treatment length (10, 24). In the primary dentition, therapeutic options are a removable appliance and/or a McNamara disjunctor (orthopedic appliance) according to the severity and the dental age (25–27).
This simple appliance, requires excellent skills and expertise to control the movement with elastic chains in the deciduous dentition. Nevertheless, it is very important because it has solved the problem of malocclusion treatment without requiring the patient's collaboration. According to recent research, occlusion stability and adaptation to the new function are only achieved six months after conclusion and require regular assessments (28).
A technique was delivered to a four-year-old child with crossbite, whose etiological factor of such dysmorphia was the lateral deviation of the mandible in the kinesics of closure. With this simple device, the correction of this malocclusion was achieved in a short period, i.e., four months, improving the interarch relationship and promoting bilateral simultaneous skeletal growth (Figures 1, 2). However, it is important to follow up after this treatment has been concluded. Through interceptive orthodontics the malocclusion was corrected allowing normal dental, alveolar and skeletal growth, and development (29).
This study presents a simple technique that uses aesthetic buttons and elastic chains, with the aim of correcting the crossbite with great aesthetics and a short treatment time at earlier age.
VU and TI conceived the ideas; VU and TI collected the data; VU and AP analyzed the data; VU and TI and AP led the writing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Agostino P, Uggolini A, Signori A, Silvestrini-Biavati A, Harrison JE, Ortho RP. Orthodontic treatment for posterior crossbites. Cochrane Database Syst Rev. (2014) 8:CD000979. doi: 10.1002/14651858.CD000979.pub2
2. Kutin G, Hawes RR, Rochester NY. Posterior cross-bites in the deciduous and mixed dentitions. Am J Orthod. (1969) 56:491–504. doi: 10.1016/0002-9416(69)90210-3
3. Lombardo G, Vena F, Negri P, Pagano S, Barilotti C, Paglia L, et al. Worldwide prevalence of malocclusion in the different stages of dentition: a systematic review and meta-analysis. Eur J Paediatr Dent. (2020) 21:115–22. doi: 10.23804/ejpd.2020.21.02.05
4. Katz CR, Rosenblatt A, Gondim PP. Nonnutritive sucking habits in Brazilian children: effects on deciduous dentition and relationship with facial morphology. Am J Orthod Dentofacial Orthop. (2004) 126:53–7. doi: 10.1016/j.ajodo.2003.06.011
5. Melki-Frèrejouand C, Naulin-Ifi C. Endoalveolia/endognathia: how can transverse abnormalities be treated? Rev Odont Stomat. (2018) 47:223–40.
6. Urzal V, Braga AC, Ferreira AP. Oral habits as risk factors for anterior open bite in the deciduous and mixed dentition - cross-sectional study. Eur J Paediatr Dent. (2013) 14:299–302. PMID: 24313582
7. Borrie F, Bearn D. Early correction of anterior crossbites: a systematic review. J Orthod. (2011) 38:175–84. doi: 10.1179/14653121141443
8. Tung AW, Kiyak HA. Psychological influences on the timing of orthodontic treatment. Am J Orthod Dentofacial Orthop. (1998) 113:29–39. doi: 10.1016/S0889-5406(98)70274-4
9. Bishara SE, Khadivi P, Jakobsen JR. Changes in tooth size-arch length relationships from the deciduous to the permanent dentition: a longitudinal study. Am J Orthod Dentofacial Orthop. (1995) 108:607–13. doi: 10.1016/S0889-5406(95)70006-4
10. McNamara JA Jr. Early intervention in the transverse dimension: is it worth the effort? Am J Orthod Dentofacial Orthop. (2002) 121:572–4. doi: 10.1067/mod.2002.124167
11. Malandris M, Mahoney EK. Aetiology, diagnosis and treatment of posterior cross-bites in the primary dentition. Int J Paediatr Dent. (2004) 14:155–66. doi: 10.1111/j.1365-263X.2004.00546.x
12. Buchmann N, Senn C, Ball J, Brauchli L. Influence of initial strain on the force decay of currently available elastic chains over time. Angle Orthod. (2012) 82:529–35. doi: 10.2319/062011-399.1
13. Andreasen GF, Bishara S. Comparison of alastik chains with elastics involved with intra-arch molar to molar forces. Angle Orthod. (1970) 40:151–8. doi: 10.1043/0003-3219(1970)040%3C0151:COACWE%3E2.0.CO;2
14. Ash JL, Nikolai RJ. Relaxation of orthodontic elastomeric chains and modules in vitro and in vivo. J Dent Res. (1978) 57:685–90. doi: 10.1177/00220345780570050301
15. De Genova DC, McInnes-Ledoux P, Weinberg R, Shaye R. Force degradation of orthodontic elastomeric chains - a product comparison study. Am J Orthod. (1985) 87:377–84. doi: 10.1016/0002-9416(85)90197-6
16. Wong AK. Orthodontic elastic materials. Angle Orthod. (1976) 46:196–205. doi: 10.1043/0003-3219(1976)046%3C0196:OEM%3E2.0.CO;2
17. Lu TC, Wang WN, Tarng TH, Chen JW. Force decay of elastomeric chain—a serial study. Part II. Am J Orthod Dentofacial Orthop. (1993) 104:373–7. doi: 10.1016/S0889-5406(05)81336-8
18. Hershey HG, Reynolds WG. The plastic module as an orthodontic tooth-moving mechanism. Am J Orthod. (1975) 67:554–62. doi: 10.1016/0002-9416(75)90300-0
19. Young J, Sandrik JL. The influence of preloading on stress relaxation of orthodontic elastic polymers. Angle Orthod. (1979) 49:104–9. doi: 10.1043/0003-3219(1979)049%3C0104:TIOPOS%3E2.0.CO;2
20. Brantley WA, Salander S, Myers LC, Winders RV. Effects of prestretching on force degradation characteristics of plastic modules. Angle Orthod. (1979) 49:37–43. doi: 10.1043/0003-3219(1979)049%3C0037:EOPOFD%3E2.0.CO;2
21. Fiorelli G, Melsen B, Modica C. The design of custom orthodontic mechanics. Clin Orthod Res. (2000) 3:210–9. doi: 10.1034/j.1600-0544.2000.030407.x
22. Reitan KD. Some factors determining the evaluation of forces in orthodontics. Am J Orthod. (1957) 43:32–45. doi: 10.1016/0002-9416(57)90114-8
23. Kluemper GT, Beeman CS, Hicks EP. Early orthodontic treatment: what are the imperatives? J Am Dent Assoc. (2000) 131:613–20. doi: 10.14219/jada.archive.2000.0235
24. Jang SJ, Choi DS, Jang I, Jost-Brinkmann PG, Cha BK. Quantitative comparison of incisal tooth wear in patients receiving one-phase or two-phase treatment for skeletal class III malocclusion with anterior crossbite. Angle Orthod. (2018) 88:151–6. doi: 10.2319/080817-532.1
25. Bell RA. A review of maxillary expansion in relation to rate of expansion and patient’s age. Am J Orthod. (1982) 81:32–7. doi: 10.1016/0002-9416(82)90285-8
26. Caroccia F, Moscagiuri F, Falconio L, Festa F, D’Attilio M. Early orthodontic treatments of unilateral posterior crossbite: a systematic review. J Clin Med. (2020) 24:10–33. doi: 10.3390/jcm10010033
27. Pereira da Silva HCF, Batista de Paiva J, Rino Neto J. Traitement de l’occlusion croisée antérieure en denture temporaire: à propos de trois cas cliniques. Int Orthod. (2018) 16:514–29. doi: 10.1016/j.ortho.2018.06.028
28. Yawaka Y, Hironaka S, Akiyama A, Matzuduka I, Takasaki C, Oguchi H. Changes in occlusal contact area and average bite pressure during treatment of anterior crossbite in primary dentition. J Clin Pediatr Dent. (2003) 28:75–9. doi: 10.17796/jcpd.28.1.25472t792t36p50m
Keywords: malocclusion, crossbite, early diagnosis, elastic chains, orthodontics
Citation: Urzal V, Iunes T and Pinhão-Ferreira A (2023) A new challenge for crossbite treatment. Front. Oral. Health 4:1235134. doi: 10.3389/froh.2023.1235134
Received: 5 June 2023; Accepted: 21 June 2023;
Published: 6 July 2023.
Edited by:
Guglielmo Campus, Universität Bern, SwitzerlandReviewed by:
Thakur Prasad Chaturvedi, Banaras Hindu University, India© 2023 Urzal, Iunes and Pinhão-Ferreira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vanda Urzal dmFuZGF1cnphbEB1ZnAuZWR1LnB0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.