 Clara Yan-Yu Yeung
Clara Yan-Yu Yeung Chun-Hung Chu
Chun-Hung Chu Ollie Yiru Yu
Ollie Yiru Yu- Faculty of Dentistry, The University of Hong Kong, Hong Kong, Hong Kong SAR, China
Chewing gum has been endorsed as a caries preventive agent by the FDI World Dental Federation, the American Dental Association, and the European Food Safety Authority. This review discusses the mechanism and provides an update of the use of chewing gum for caries prevention. Chewing gum typically consists of a water-insoluble gum base, water-soluble added ingredients, and active ingredients. It can be classified as sugar-containing or sugar-free, as well as nonmedicated or medicated. Chewing gum prevents dental caries through a range of mechanisms, including the clearance of the oral cavity, neutralization of oral acidity, inhibition of cariogenic bacterial growth, remineralization of enamel, and reduction of appetite. Recent clinical studies have evaluated the efficacy of sugar-free chewing gum for caries prevention, with most demonstrating positive results, although some studies have reported contradictory outcomes. To achieve optimal caries prevention, it is generally recommended that individuals chew sugar-free gum for five minutes after meals, three times daily.
1. Introduction
Dental caries is one the most prevalent health conditions worldwide. Half of the world's population is affected by untreated caries. It can cause pain and infections and undermines one's general health and quality of life (1). Treating dental caries can be expensive. The World Health Organization (WHO) reported that 5%–10% of healthcare budgets were used for the treatment of dental caries in industrialized countries (2). Therefore, effective and cost-effective preventive strategies for caries prevention are essential and beneficial to the population and the health care system.
Chewing gum can be used for caries prevention with economic benefits to the healthcare sector (3–5). Chewing gum is a sweetened and flavoured insoluble plastic material used for chewing. Humans have a long history of using chewing gum-like agents. Chewing betel was found in Asia and Oceania 4,000 years ago, and chewing coca leaf was found in ancient Andes 3,000 years ago (6, 7). Despite thousands of years of history, modern chewing gum was developed and commercialized in 1,848 (8).
Chewing gum contains a water-insoluble gum base, water-soluble added ingredients, and active ingredients (9, 10). The water-insoluble gum base is composed of elastomers, elastomer solvents, and fillers. They are nonnutritive and cannot be dissolved during the chewing process. Water-soluble added ingredients include bulking agents, flavouring agents, antioxidants, sweeteners, colourants, opacifiers, softeners, emulsifiers, anti-tack agents, and anti-caking agents. They optimize the physical and chemical properties of chewing gum (11). Active ingredients can also be added to the chewing gum for therapeutic use. With the addition of active ingredients, some chewing gum can be used for medical purpose, such as nicotine-containing chewing gum for smoke cessation or aspirin-containing chewing gum for pain relief (9, 10). Because this review focused on the role of chewing gum as a caries preventive agent, medicated chewing gum, which does not have the caries preventive function, is not discussed in this review. Examples of the active ingredient of chewing gum for dental use includes casein phosphopeptide–amorphous calcium phosphate-nanocomplexes (CPP-ACP), fluoride, carbamide, or chlorhexidine (Table 1) (20).
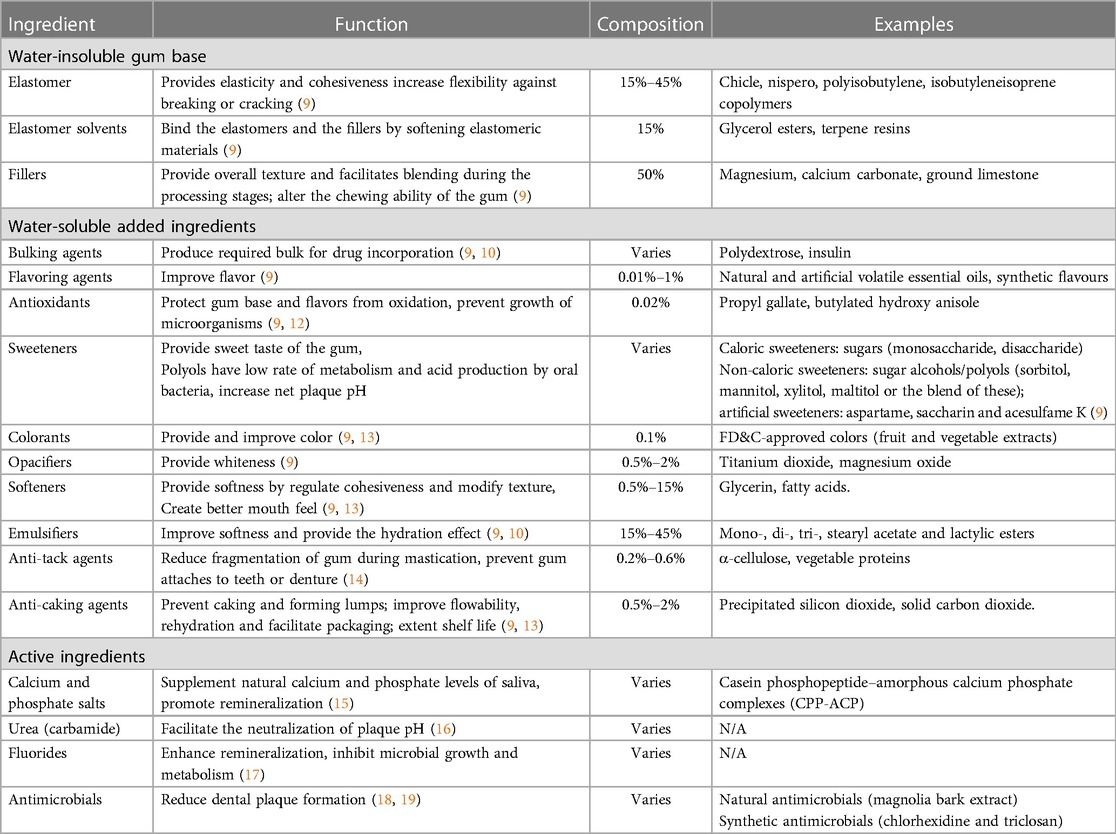
Table 1. Composition of the chewing gum.
Chewing gum has been recognized as a caries preventive agent by several professional organizations, including the European Food Safety Authority since 2010, FDI world dental association since 2015, and the American Dental Association since 2021 (21). Although two recent systematic reviews reported the caries preventive effect of sugar-free chewing gum and xylitol-containing sugar-free chewing gum, respectively (21, 22), the evidence and knowledge of chewing gum in caries prevention has not been comprehensively updated (21). Therefore, this review article aims to provide an overview and update on chewing gum as a caries preventive agent.
2. Methods
2.1. Data sources and selection
The literature search was conducted in three databases, including PubMed/Medline, Web of Science, and Scopus to identify the available studies evaluating the prevention of caries lesions with chewing gum.
2.2. Search strategy
The search strategy was developed as follows:
1. “demineralization” OR “tooth demineralization” OR “teeth demineralization” OR “caries” OR “carious” OR “tooth decay” OR “teeth decay” OR “dental caries” OR “caries susceptibility”
2. “chewing gum” OR “sugar-free gum”
3. “[1]” AND “[2]”
2.3. Inclusion criteria
English articles on the caries preventive effect of chewing gum in children or adults published from 2012 to 2022 were included. Randomized controlled trials, cross-sectional studies, pre-post trials, and any clinical studies designed with a comparative arm were identified and analysed for eligibility of further quantitative analysis (Figure 1).
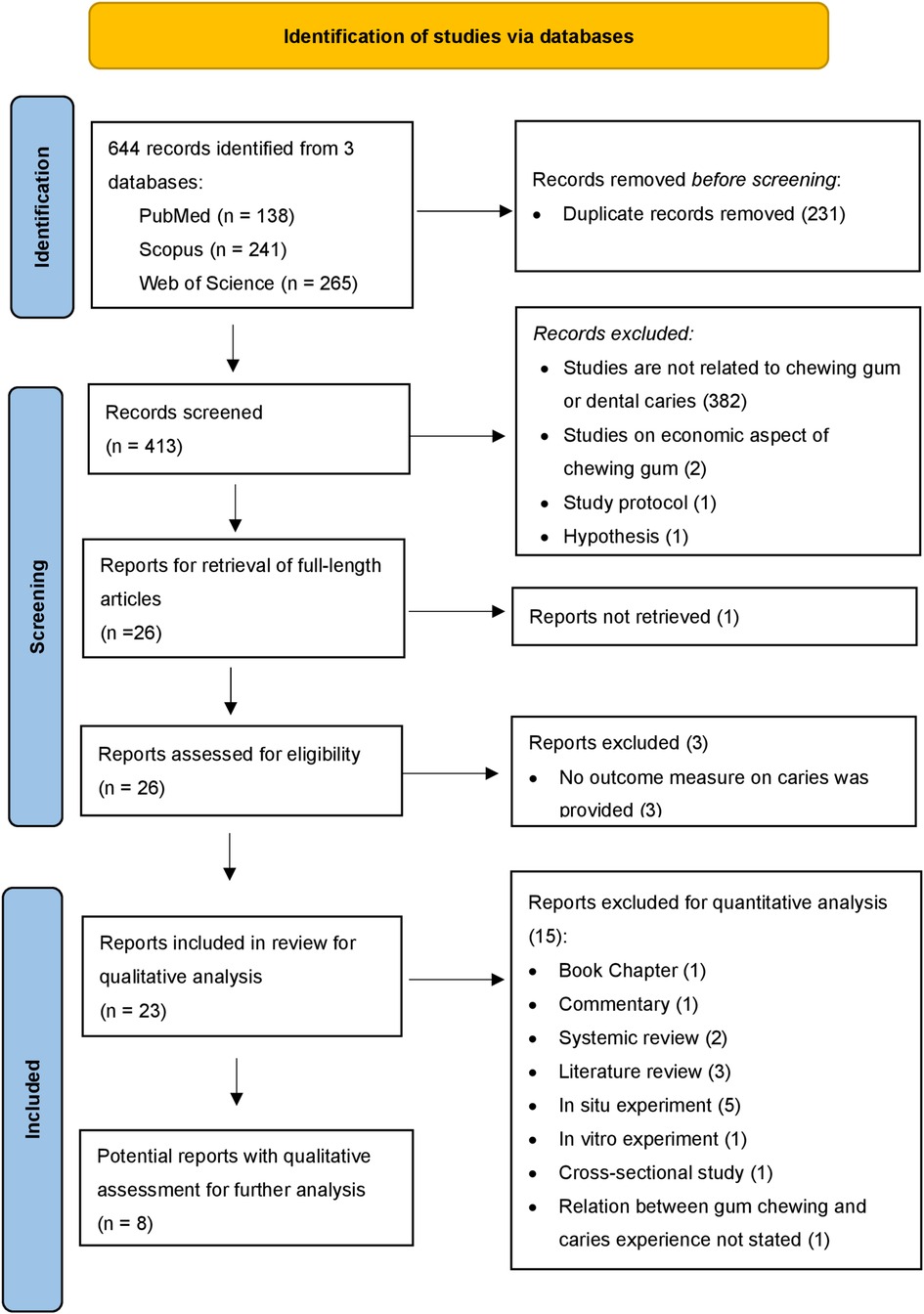
Figure 1. Flow chart of study identification, screening, and inclusion.
2.4. Data collection and analysis
The data on the clinical performance of chewing gum in caries prevention were extracted and analysed.
3. Classification
3.1. Classification by sugar contents
Based on the sugar content, chewing gum can be classified as sugar-containing chewing gum or sugar-free chewing gum. Sugar-containing chewing gum is chewing gum that contains simple carbohydrates, such as monosaccharides and disaccharides, in which monosaccharides include glucose, fructose, and galactose, and disaccharides include maltose, sucrose, and lactose. Chewing gum containing any of these are considered sugar-containing chewing gum (9, 10, 12, 20). Sugar-free chewing gum does not contain simple carbohydrates. It can be further classified into chewing gum containing sugar alcohol and chewing gum containing other sweeteners. Sugar alcohol includes polyols, such as xylitol, sorbitol, etc. Non sugar alcohol-containing gum is sugar-free chewing gum. They might contain other sweeteners, such as artificial sweeteners like aspartame and saccharin. Non sugar alcohol-containing gum can also be sweetener-free, which is plain chewing gum (9, 10, 12, 20).
3.2. Classification by active ingredients
Chewing gum can be classified by its active ingredients. Based on whether the chewing gum contains bioactive drug content or not, chewing gum can be classified as medicated chewing or nonmedicated chewing gum. Medicated chewing gum contains active ingredients. Examples include CPP-ACP-containing chewing gum, carbamide-containing chewing gum, fluoride-containing chewing gum, and chlorhexidine-containing gum (9, 10, 12, 20).
4. Effectiveness in caries prevention
Conducting a meta-synthesis was not feasible in the current review due to the high heterogeneity among studies. The included clinical studies on the caries preventive effect of chewing gum used various outcomes to assess the caries experience of the participants, including increments of decayed, missing, filled teeth (DMFT), increments of decayed, missing, filled surfaces (DMFS), increments of decayed surfaces (DS), increments of International Caries Detection and Assessment System (ICDAS) coding, and volume change of demineralized lesions. Therefore, the details of the included clinical studies were presented without further processing of the data (Table 2). The results of the included studies were summarized as follows.
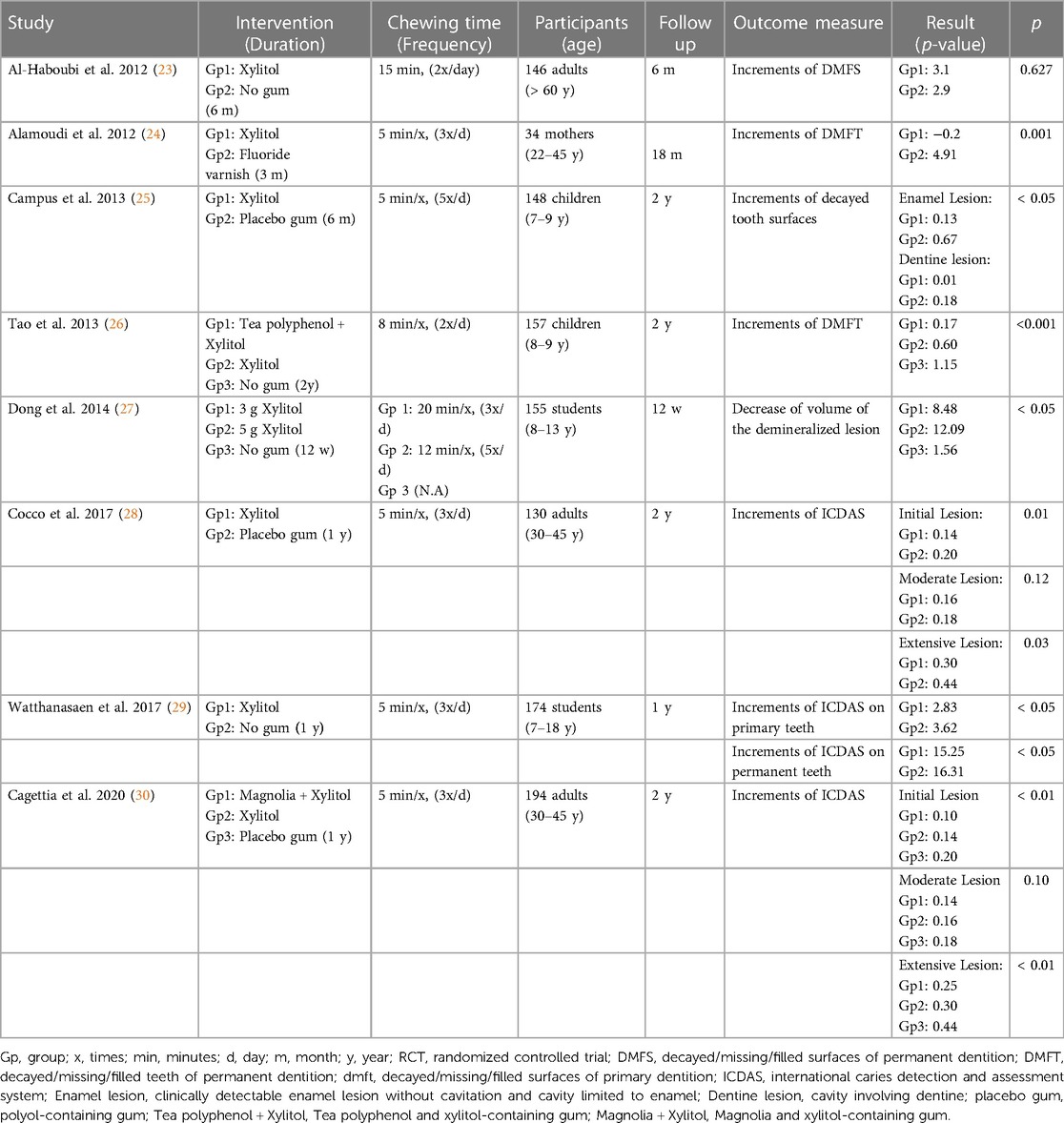
Table 2. Randomized clinical trials of chewing gum published from 2012 to 2022.
4.1. Effects of chewing gum compared to no gum
Four studies investigated the caries preventive effect of chewing gum compared to no gum (23, 26, 27, 29). Three out of four studies showed that chewing gum lowered caries increments in comparison to no gum use, with prevention ranging from 6.95% to 85.2% (26, 27, 29). One study did not find a caries preventive effect of chewing gum (23).
4.2. Effects of chewing gum compared to fluoride varnish
One study investigated the use of chewing gum compared to fluoride varnish (24). It showed chewing gum reduced more caries formation in comparison to fluoride varnish.
4.3. Types of chewing gum on caries preventive effects
Three studies investigated the caries preventive effect of xylitol-containing chewing gum compared to polyol-containing chewing gum (25, 28, 30). One study showed that xylitol-containing chewing gum had a better caries preventive effect than other polyol-containing chewing gum in both initial enamel caries and dentine caries (25). Another two studies were conducted with the same clinical trial (28, 30). They showed xylitol-containing chewing gum had a better caries preventive effect for initial and extensive lesions as defined in the ICDAS than other polyol-containing chewing gum. However, such an effect was insignificant in moderated lesions. One study investigated the caries preventive effect of tea polyphenol-containing chewing gum compared to xylitol-containing chewing gum (26). The study showed that tea polyphenol-containing chewing gum had a superior caries preventive effect in comparison to xylitol-containing chewing gum. Another study investigated the caries preventive effect of magnolia-containing chewing gum compared to xylitol-containing chewing gum (30). The results indicated that magnolia-containing chewing gum had a superior caries preventive effect in comparison to xylitol-containing chewing gum for initial and extensive lesions but not moderate (30).
4.4. Duration of the intervention on caries preventive effects
The caries preventive effect of chewing gum compared to no gum was found in a varied intervention period of daily chewing gum use, ranging from 12 weeks to two years (24, 26, 27, 29). With as short as a 12-week daily use of chewing gum, a reduced caries experience was observed (27).
4.5. Frequency and duration of chewing on caries preventive effects
One study compared the caries preventive effects of chewing gum to no gum with two different frequencies and durations (5 times a day and 12 min each time vs. 3 times a day and 20 min each time) yet the same daily total duration of 60 min (27). The group with higher frequency and lower duration of chewing gum daily presented a superior remineralization effect. However, it should also be noted that the total daily intake of xylitol is higher in the former group (5 g) than the latter (3 g).
4.6. Effects of chewing gum on different age groups
Three studies investigated the caries preventive effect of chewing gum compared to no gum on children and adolescents (26, 27, 29). All studies showed that chewing gum lowered caries increments in comparison to no gum use, with prevention ranging from 6.95% to 85.2% (26, 27, 29). One study investigated the use of chewing gum on participants above 60 years old and compared to no gum (23). The results did not show chewing gum reduce caries experience on elderly. No included studies investigated the use of chewing gum compared to no gum on adults.
5. Mechanism in caries prevention
Sugar-free chewing gum prevents dental caries by clearing the oral cavity, neutralizing the acidity of oral cavity, remineralizing enamel, inhibiting the growth of cariogenic bacteria, and reducing appetite.
5.1. Oral cavity clearance
Chewing gum prevents caries by clearing the oral cavity. Two systemic reviews concluded the anti-plaque effect of sugar free chewing gum (31, 32). When debris of food containing fermentable carbohydrates is retained in the oral cavity, it can be fermented by cariogenic bacteria to produce acid (33). Chewing gum can facilitate the mechanical removal of food debris, which contains dietary sugars (34). In addition, chewing gum increases salivary flow rates, which creates an increased flushing effect against food debris. Through stimulating saliva and reducing plaque mechanically, chewing gum can improve oral hygiene (35).
5.2. Neutralization of acidity
The acidity of oral cavity will reduce after the oral cavity being exposure to fermentable carbohydrates. When the pH level is below 5.5, the critical pH of enamel, demineralization of the underlying enamel occurs (36). Chewing gum can increase the secretion of saliva. The increased salivary stimulation can last for 9 min with a 187% increase of saliva in the first minute, and a 86% increase in the subsequent minute in comparison to unstimulated status (37). Besides, the buffering capacity of stimulated saliva is higher compared to unstimulated saliva (38, 39). Furthermore, some studies suggested that there will be a slight increase of the unstimulated salivary pH (40). All these facilitate the neutralization of acidity in the oral cavity and reduced enamel demineralization.
5.3. Remineralization of enamel
Chewing gum can stimulate the production of saliva, which is supersaturated with calcium and phosphate ions. These ions can precipitate to the demineralized enamel surface and promote remineralization (34, 41).
5.4. Inhibition of cariogenic bacteria growth
Previous studies show that xylitol-containing chewing gum can reduce the level of Streptococcus mutans in the oral cavity by inhibiting the attachment of S. mutans to the tooth surface (42, 43). In addition, xylitol cannot be metabolized by S. mutans, but it can compete with mono- and polysaccharides in the metabolic pathways of S. mutans and inhibit the production of lactic acid by the bacteria (44).
5.5. Reduction of appetite
Consuming chewing gum after a meal might lower the appetite of the consumer and subsequent snack intake (33). A clinical trial reported that the group chewing gum after lunch experienced a lower level of snack intake, desire for sweet food, and subjective feeling of hunger in comparison to the no-gum group (45). In another trial, the group chewing gum after lunch also experienced a lower level of snack intake, especially carbohydrate-containing food in comparison to the no-gum group (46).
6. Application
Despite the anti-caries effect of chewing gum, using chewing gum alone is insufficient to achieve caries prevention. Chewing gum should be used in adjunction with tooth brushing with fluoridated toothpaste twice a day and daily cleaning of interdental area (47).
6.1. Daily intake
In order to achieve the caries preventive effects of chewing gum, the amount, duration, and time of intake is important. According to the included clinical studies, a positive caries preventive effect was found with participants chewing gum after a meal at least 3 times per day. Therefore, the best time to chew gum is after a snack or meal at least 3 times per day. The European Food Safety Authority suggests chewing gum for 20 min each time (48). However, the anti-caries effect of chewing gum can be achieved after 5 min of chewing per use according to the included studies (47).
6.2. Choice of chewing gum
Sugar-free gum is suggested for caries prevention. Despite multiple clinical studies (49) favouring xylitol-containing gum over sorbitol-containing gum, a systemic review in 2012 (49) suggested that the current evidence supporting xylitol over sorbitol is contradictory. More research is needed on the topic. Although studies showed a superior caries preventive effect of magnolia bark extract-containing gum and tea polyphenol-containing gum in comparison to xylitol-containing gum (20, 25, 30), they are not available commercially. Research on the caries preventive effect of chewing gum containing other active ingredients, such as CPP-ACP, fluoride, and urease, is lacking.
7. Potential adverse effects if overuse or abuse
Despite the multiple advantages of chewing gum and the caries prevention effects as stated above, some studies have suggested the potential adverse effects of chewing gum (20), often relating to the excessive chewing process and the excessive consumption of ingredients in chewing gum. The potential adverse effects include choking, jaw muscle pain, temporo-mandibular joint disorder, headache, mercury release from amalgam restoration, and diarrhoea.
7.1. Choke
There have been incidents of choking on chewing gum, especially in young children (50, 51). According to the U.S. Department of Agriculture, children under the age of 4 should not chew gum. As for children above that age, the risk of chewing during eating is smaller. Good eating habits are believed to prevent choking (52).
7.2. Jaw muscle pain and temporo-mandibular joint disorder (TMD)
There are studies reporting arthralgia and myofascial pain after the excessive chewing of gum for over three hours per day (53, 54). The prolonged exercise of the jaw muscle which exceeds its capacity may lead to temporo-mandibular joint disorder (TMD) and a pain in the jaw muscles (55). It is, therefore, important to avoid prolonged gum chewing.
7.3. Headache
Some studies suggested excessive chewing gum use is related to chronic headaches among adolescents (56). The mechanism behind this is still unclear. The chronic headache is hypothesized to be related to the temporo-mandibular joint dysfunction provoked by excessive gum chewing or the consumption of aspartame that chewing gum contains (56, 57).
7.4. Mercury release
Chewing gum can accelerate the release of mercury for individuals with dental amalgam fillings. The amount of mercury in plasma and urine for individuals with regular gum chewing habits are significantly higher than those without such habits (58).
7.5. Diarrhoea
There are cases reporting diarrhoea and abdominal discomfort after chewing gum consumption (59). This can be related to the over consumption of polyols in gum, which can cause gastrointestinal disturbances and lead to irritable bowel syndrome. This negative effect is dose-dependent (60). The amount of polyol in chewing gum is low and would not cause any gastrointestinal effects in most individuals (60, 61).
8. Summary
Chewing gum can be classified as sugar-containing chewing gum or sugar-free chewing gum based on the sugar content or as nonmedicated chewing gum or medicated chewing gum based on the active ingredients. Chewing gum prevents dental caries by clearing the oral cavity, neutralizing the acidity in the oral cavity, inhibiting the growth of cariogenic bacteria, remineralizing enamel, and reducing the appetite. The caries preventive effect of the sugar-free chewing gum has been proved in many clinical studies, though a few included studies showed a contradictory result. A proper duration of chewing gum for 5 min after a meal for 3 times per day is recommended to avoid potential adverse effects.
Author contributions
Conceptualization, writing, and proofreading: CY-YY, OYY. Proofreading: C-HC. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the General Research Fund of Research Grants Council of Hong Kong SAR, China (grant no. 17100019).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Sugars and dental caries (2017). Available at: https://www.who.int/news-room/fact-sheets/detail/sugars-and-dental-caries.
2. World Health Organization. Oral health (2022). Available at: https://www.who.int/news-room/fact-sheets/detail/oral-health#:∼:text=Globally%2C%20an%20estimated%202%20billion,and%20changes%20in%20living%20conditions.
3. Du S, Zhang C, Wang W, Liu J, Yuan C, Yu Y, et al. The economic benefits of increased sugar-free chewing gum in China: a budget impact analysis. BMC Oral Health. (2021) 21(1):436. doi: 10.1186/s12903-021-01786-8
4. Rychlik R, Kreimendahl F, Blaich C, Calache H, Garcia-Godoy F, Kay E, et al. A global approach to assess the economic benefits of increased consumption of sugar-free chewing gum. Am J Dent. (2017) 30(2):77–83.29178768
5. Claxton L, Taylor M, Kay E. Oral health promotion: the economic benefits to the NHS of increased use of sugarfree gum in the UK. Br Dent J. (2016) 220(3):121–7. doi: 10.1038/sj.bdj.2016.94
6. Aufderheide AC, Rodríguez-Martín C, Langsjoen O. The Cambridge Encyclopedia of Human Paleopathology. Cambridge: Cambridge University Press (2011).
7. Weiss E. Paleopathology in Perspective: Bone Health and Disease Through Time. Maryland: Rowman & Littlefield Publishers (2014).
8. Imfeld T. Chewing gum–facts and fiction: a review of gum-chewing and oral health. Crit Rev Oral Biol Med. (1999) 10(3):405–19. doi: 10.1177/10454411990100030901
9. Aslani A, Rostami F. Medicated chewing gum, a novel drug delivery system. J Res Med Sci. (2015) 20(4):403–11.26109999
10. Chaudhary SA, Shahiwala AF. Medicated chewing gum – a potential drug delivery system. Expert Opin Drug Delivery. (2010) 7(7):871–85. doi: 10.1517/17425247.2010.493554
11. Zyck DJ, Greenberg MJ, Barkla DG, Marske SW, Schnell PG, Mazzone P. Method of Making Coated Chewing Gum Products Containing Various Antacids. Chicago, United States: WM. Wrigley Jr. Company (2003). 635–45.
12. Rassing M. Chewing gum as a drug delivery system. Adv Drug Delivery Rev. (1994) 13(1-2):89–121. doi: 10.1016/0169-409X(94)90028-0
13. Al Hagbani T, Nazzal S. Medicated chewing gums (MCGs): composition, production, and mechanical testing. AAPS PharmSciTech. (2018) 19(7):2908–20. doi: 10.1208/s12249-018-1123-z
14. Krunal SV, Raval Harshad A, Dhaval D. Chewing gum: a modern approach to oral mucosal drug delivery (2012).
15. Vogel GL, Zhang Z, Carey CM, Ly A, Chow LC, Proskin HM, et al. Composition of plaque and saliva following use of an alpha-tricalcium-phosphate-containing chewing gum and a subsequent sucrose challenge. J Dent Res. (2000) 79(1):58–62. doi: 10.1177/00220345000790010901
16. Imfeld T, Birkhed D, Lingström P. Effect of urea in sugar-free chewing gums on pH recovery in human dental plaque evaluated with three different methods. Caries Res. (1995) 29(3):172–80. doi: 10.1159/000262065
17. Lamb WJ, Corpron RE, More FG, Beltran ED, Strachan DS, Kowalski CJ. In situ remineralization of subsurface enamel lesion after the use of a fluoride chewing gum. Caries Res. (1993) 27(2):111–6. doi: 10.1159/000261527
18. Greenberg M, Urnezis P, Tian M. Compressed mints and chewing gum containing magnolia bark extract are effective against bacteria responsible for oral malodor. J Agric Food Chem. (2007) 55(23):9465–9. doi: 10.1021/jf072122h
19. Simons D, Brailsford S, Kidd EA, Beighton D. The effect of chlorhexidine acetate/xylitol chewing gum on the plaque and gingival indices of elderly occupants in residential homes. J Clin Periodontol. (2001) 28(11):1010–5. doi: 10.1034/j.1600-051X.2001.281104.x
20. Dodds MW. The oral health benefits of chewing gum. J Ir Dent Assoc. (2012) 58(5):253–61.23573702
21. Newton JT, Awojobi O, Nasseripour M, Warburton F, Di Giorgio S, Gallagher JE, et al. A systematic review and meta-analysis of the role of sugar-free chewing gum in dental caries. JDR Clin Trans Res. (2020) 5(3):214–23. doi: 10.1177/2380084419887178
22. ALHumaid J, Bamashmous M. Meta-analysis on the effectiveness of xylitol in caries prevention. J Int Soc Prev Community Dent. (2022) 12(2):133–8. doi: 10.4103/jispcd.JISPCD_164_21
23. Al-Haboubi M, Zoitopoulos L, Beighton D, Gallagher JE. The potential=benefits of sugar-free chewing gum on the oral health and quality of life of older people living in the community: a randomized controlled trial. Community Dent Oral Epidemiol. (2012) 40(5):415–24. doi: 10.1111/j.1600-0528.2012.00685.x
24. Alamoudi NM, Hanno AG, Masoud MI, Sabbagh HJ, Almushayt AS, Masoud IM. Effects of xylitol on salivary mutans streptococcus, plaque level, and caries activity in a group of Saudi mother-child pairs an 18-month clinical trial. Saudi Med J. (2012) 33(2):186–92. doi: 10.17796/jcpd.36.1.d4g77616714w3372
25. Campus G, Cagetti MG, Sale S, Petruzzi M, Solinas G, Strohmenger L, et al. Six months of high-dose xylitol in high-risk caries subjects-a 2-year randomised, clinical trial. Clin Oral Investig. (2013) 17(3):785–91. doi: 10.1007/s00784-012-0774-5
26. Tao DY, Shu CB, Lo EC, Lu HX, Feng XP, et al. A randomized trial on the inhibitory effect of chewing gum containing tea polyphenol on caries. J Clin Pediatr Dent. (2013) 38(1):67–70. doi: 10.17796/jcpd.38.1.c0tm02w572488064
27. Dong Y, Yin W, Hu D, Zhang X, Xu L, Dodds WJ, et al. Remineralization of early caries by chewing sugar-free gum: a clinical study using quantitative light-induced fluorescence. Am J Dent. (2014) 27(6):291–5.25707081
28. Cocco F, Carta G, Cagetti MG, Strohmenger L, Lingström P, Campus G, et al. The caries preventive effect of 1-year use of low-dose xylitol chewing gum. A randomized placebo-controlled clinical trial in high-caries-risk adults. Clin Oral Investig. (2017) 21(9):2733–40. doi: 10.1007/s00784-017-2075-5
29. Watthanasaen S, Merchant AT, Luengpailin S, Chansamak N, Pisek A, Pitiphat W. Xylitol-containing chewing gum for caries prevention in students with disabilities: a randomised trial. Oral Health Prev Dent. (2017) 15(6):519–27. doi: 10.3290/j.ohpd.a39668
30. Cagetti MG, Cocco F, Carta G, Maspero C, Campus G. Long-term efficacy of magnolia bark extract and xylitol administered through chewing gums on caries in adults: a 2-year randomized controlled intervention trial. J Funct Foods. (2020) 68:103891. doi: 10.1016/j.jff.2020.103891
31. Keukenmeester RS, Slot DE, Putt MS, Van der Weijden GA. The effect of sugar-free chewing gum on plaque and clinical parameters of gingival inflammation: a systematic review. Int J Dent Hyg. (2013) 11(1):2–14. doi: 10.1111/j.1601-5037.2012.00562.x
32. Muniz FWMG, Zanatta FB, Muñoz MDS, Aguiar LM, Silva FH, Montagner AF. Antiplaque and antigingivitis efficacy of medicated and non-medicated sugar-free chewing gum as adjuncts to toothbrushing: systematic review and network meta-analysis. Clin Oral Investig. (2022) 26(2):1155–72. doi: 10.1007/s00784-021-04264-1
33. Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, et al. Dental caries. Nature Reviews Disease Primers. (2017) 3:1–16. doi: 10.1038/nrdp.2017.30
34. Lenander-Lumikari M, Loimaranta V. Saliva and dental caries. Adv Dent Res. (2000) 14:40–7. doi: 10.1177/08959374000140010601
35. Choo A, Delac DM, Messer LB. Oral hygiene measures and promotion: review and considerations. Aust Dent J. (2001) 46(3):166–73. doi: 10.1111/j.1834-7819.2001.tb00277.x
36. Garcia-Godoy F, Hicks MJ. Maintaining the integrity of the enamel surface - the role of dental biofilm, saliva and preventive agents in enamel demineralization and remineralization. J Am Dent Assoc. (2008) 139:25S–34S. doi: 10.14219/jada.archive.2008.0352
37. Bots CP, Brand HS, Veerman EC, van Amerongen BM, Nieuw Amerongen AV. Preferences and saliva stimulation of eight different chewing gums. Int Dent J. (2004) 54(3):143–8. doi: 10.1111/j.1875-595X.2004.tb00270.x
38. Proctor GB. The physiology of salivary secretion. Periodontol 2000. (2016) 70(1):11–25. doi: 10.1111/prd.12116
39. Stookey GK. The effect of saliva on dental caries. J Am Dent Assoc. (2008) 139:11S–7S. doi: 10.14219/jada.archive.2008.0347
40. Dodds MW, Hsieh SC, Johnson DA. The effect of increased mastication by daily gum-chewing on salivary gland output and dental plaque acidogenicity. J Dent Res. (1991) 70(12):1474–8. doi: 10.1177/00220345910700120101
41. Humphrey SP, Williamson RT. A review of saliva: normal composition, flow, and function. J Prosthet Dent. (2001) 85(2):162–9. doi: 10.1067/mpr.2001.113778
42. Al-Joburi W, Clark C, Fisher R. A comparison of the effectiveness of two systems for the prevention of radiation caries. Clin Prev Dent. (1991) 13(5):15–9.1809524
43. Nasseripour M, Newton JT, Warburton F, Awojobi O, Di Giorgio S, Gallagher JE. A systematic review and meta-analysis of the role of sugar-free chewing gum on plaque quantity in the oral cavity. Front Oral Health. (2022) 3:845921. doi: 10.3389/froh.2022.845921
44. Nasseripour M, Newton JT, Warburton F, Awojobi O, Di Giorgio S, Gallagher JE, et al. A systematic review and meta-analysis of the role of sugar-free chewing gum on Streptococcus mutans. BMC Oral Health. (2021) 21(1):217. doi: 10.1186/s12903-021-01517-z
45. Hetherington MM, Boyland E. Short-term effects of chewing gum on snack intake and appetite. Appetite. (2007) 48(3):397–401. doi: 10.1016/j.appet.2006.10.001
46. Park E, Edirisinghe I, Inui T, Kergoat S, Kelley M, Burton-Freeman B. Short-term effects of chewing gum on satiety and afternoon snack intake in healthy weight and obese women. Physiol Behav. (2016) 159:64–71. doi: 10.1016/j.physbeh.2016.03.002
47. Association, A.D. Chewing Gum. (2021). Available at: https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/chewing-gum#:∼:text=To%20date%2C%20the%20only%20chewing,teeth%20and%20reducing%20tooth%20decay (cited September 28, 2022).
48. EFSA Panel on Dietetic Products, N. and Allergies. Scientific opinion on the substantiation of a health claim related to sugar free chewing gum and reduction of tooth demineralisation which reduces the risk of dental caries pursuant to article 14 of regulation (EC) No 1924/2006. EFSA J. (2010) 8(10):1775. doi: 10.2903/j.efsa.2010.1775
49. Gales MA, Nguyen T-M. Sorbitol compared with xylitol in prevention of dental caries. Ann Pharmacother. (2000) 34(1):98–100. doi: 10.1345/aph.19020
50. Njau SN. Adult sudden death caused by aspiration of chewing gum. Forensic Sci Int. (2004) 139(2-3):103–6. doi: 10.1016/j.forsciint.2003.09.021
51. Karuparthy V, Kaneda K, Bellinger A, Han TH. Chewing gum: a potential cause of airway obstruction. J Anesth. (2009) 23(1):168–9. doi: 10.1007/s00540-008-0683-6
53. Correia D, Real Dias MC, Castanho Moacho A, Crispim P, Luis H, Oliveira M, et al. An association between temporomandibular disorder and gum chewing. Gen Dent. (2014) 62(6):e33–6.25369399
54. Farella M, Bakke M, Michelotti A, Martina R, et al. Effects of prolonged gum chewing on pain and fatigue in human jaw muscles. Eur J Oral Sci. (2001) 109(2):81–5. doi: 10.1034/j.1600-0722.2001.00991.x
55. Tabrizi R, Karagah T, Aliabadi E, Hoseini SA, et al. Does gum chewing increase the prevalence of temporomandibular disorders in individuals with gum chewing habits? J Craniofac Surg. (2014) 25(5):1818–21. doi: 10.1097/SCS.0000000000000993
56. Watemberg N, Matar M, Har-Gil M, Mahajnah M. The influence of excessive chewing gum use on headache frequency and severity among adolescents. Pediatr Neurol. (2014) 50(1):69–72. doi: 10.1016/j.pediatrneurol.2013.08.015
57. Blumenthal HJ, Vance DA. Chewing gum headaches. Headache. (1997) 37(10):665–6. doi: 10.1046/j.1526-4610.1997.3710665.x
58. Sällsten G, Thorén J, Barregård L, Schütz A, Skarping G. Long-term use of nicotine chewing gum and mercury exposure from dental amalgam fillings. J Dent Res. (1996) 75(1):594–8. doi: 10.1177/00220345960750011301
59. Bauditz J, Norman K, Biering H, Lochs H, Pirlich M. Severe weight loss caused by chewing gum. Br Med J. (2008) 336(7635):96–7. doi: 10.1136/bmj.39280.657350.BE
60. Lenhart A, Chey WD. A systematic review of the effects of polyols on gastrointestinal health and irritable bowel syndrome. Adv Nutr. (2017) 8(4):587–96. doi: 10.3945/an.117.015560
Keywords: chewing gum, sugar-free gum, dental caries, caries management, cariology, preventive dentistry, oral health
Citation: Yeung Clara Yan-Yu, Chu C-H and Yu OY (2023) A concise review of chewing gum as an anti-cariogenic agent. Front. Oral. Health 4:1213523. doi: 10.3389/froh.2023.1213523
Received: 28 April 2023; Accepted: 25 May 2023;
Published: 13 June 2023.
Edited by:
May Lei Mei, University of Otago, New ZealandReviewed by:
Bhojraj Nandlal, JSS Dental College and Hospital, India© 2023 Yeung, Chu and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ollie Yiru Yu b2xsaWV5dUBoa3UuaGs=