 Majed Almutairi
Majed Almutairi Gerry McKenna
Gerry McKenna Ibrahim Alsumaih
Ibrahim Alsumaih Rasha Alhazzaa
Rasha Alhazzaa Ciaran O’Neill
Ciaran O’Neill
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oral. Health , 15 December 2023
Sec. Oral Health Promotion
Volume 4 - 2023 | https://doi.org/10.3389/froh.2023.1208929
Background: The funding and delivery of healthcare including dental care in the Kingdom of Saudi Arabia (KSA, or Saudi Arabia) is undergoing a process of reform. To inform this process, it is important that policymakers are aware of the relationships between service use, specific types of use, and the factors that influence this. Currently, there is a paucity of research in this area in KSA that examines dental service use for checkups at a national level and none that examines differences in this use across regions or that examines explicitly the role of income.
Aims: This study uses the most recent version of the Saudi Health Interview Survey (SHIS) to examine the relationships between the use of dental services for a checkup and socio-demographic characteristics of respondents. Particular focus is given to the differences between regions in service use and the role of socio-demographics within regions.
Methods: Data were taken from SHIS 2013. Descriptive statistics (means and standard errors) were used to characterize the sample. Logistic regression analyses were used to examine the relationship between checkups in the past 12 months and a range of covariates including income and region. The analysis was repeated for sub-samples based on specific regions. No attempt was made to impute missing values.
Results: A sample of 7603 respondents provided complete data for analysis. Fifty-one per cent of the respondents were male, 29% were educated at least to degree level, 25% reported that they floss at least once per day, 69% reported that they brushed their teeth at least once per day, and 11% reported that they had visited the dentist for a checkup in the preceding 12 months. Logistic regression analyses revealed income, region, and oral hygiene habits to be among the significant determinants of the likelihood of dental checkup in the preceding 12 months. In logistic regression analyses at the regional level, different relationships were evident between checkups and socio-demographic characteristics across regions.
Conclusion: Region and income are significant determinants of dental service use for checkups. Differences exist between regions in the relationship between socio-demographic characteristics and the likelihood of getting checkups. Policy changes should reflect the potential differences they might have across regions for which the role of socio-demographic characteristics varies.
All healthcare systems face the common challenge of resource scarcity. In recent years, for many systems these challenges have been exacerbated by a combination of factors that have affected demand and supply. With respect to demand, factors such as population aging (1, 2) and lifestyle choices related to diet (3, 4) and exercise (5, 6) have helped fuel an increase in non-communicable disease, multi-morbidity, and expenditures on healthcare associated with meeting that demand. With respect to supply, the seeming paradox of rapid technological advance coupled with slow productivity growth has also served to produce spiraling healthcare expenditures, and among those systems wherein access to care relies heavily on public funding, pressures on public funds (7–9). These pressures extend to oral healthcare, where many countries also face challenges of how to meet the needs of their populations for dental care (10). These challenges include finance issues, shortage of manpower, and issues of equity of access (11).
Dental health services play an important role in oral health, which has in turn been shown to affect individual general health, quality of life, and self-esteem (12–14). Regular dental checkups play a role in care. For instance, according to Petersen (2003), most tooth loss occurs due to the progression of diseases mainly because people do not make use of dental services (15). It is also worth noting that major oral disorders are among the 35 causes of disability adjusted life years (DALYs) as indicated by Vos et al.’s (2012) research findings (16). This highlights the importance of dental checkups, in preventing and managing oral diseases, which ultimately leads to better global health outcomes. In the Kingdom of Saudi Arabia (KSA, or Saudi Arabia), the provision of healthcare is a government priority (17). As the government has sought to diversify the economy and introduce structural reforms under Saudi Arabia's Vision 2030 initiatives, so the need to consider how best to fund and deliver services has grown (18). The reforms have included efforts to increase tax and reduce government subsidization of public services—generally as well as by the promotion of privately provided and funded healthcare (19). This has seen significant changes in healthcare in recent years (17).. Access to care is seen as a fundamental right—the constitution of Saudi Arabia stating that the government is responsible for providing healthcare, and that every citizen and resident has a right to access these services (20, 21). This had led to the government of the KSA paying for all basic dental care (22). Health services are provided to the people by public (governmental) and separately private health sectors. The government also allocates funds annually to other government sectors, including the Ministry of Interior, the Ministry of National Guard, the Ministry of Defence, and the Ministry of Education, who operate health insurance programs and facilities for their employees and families, and to the public in general in, for example, the event of an emergency (20, 23). However, it is unlikely that this approach will persist.
A number of studies have examined the use of dental services as well as oral hygiene habits/self-care in Saudi Arabia using both national and regional specific datasets (24–28). According to El Bcheraoui et al., 1.5 million individuals (that is 11.5% of the population) in Saudi Arabia visited a dental clinic for routine checkup in 2013, 71.5% reported brushing their teeth at least once a day. Up to 30.3% used Miswak—akin to a toothpick—at least once a day (24). Studies on the use of dental services in Saudi Arabia have produced conflicting results with respect to the role of socio-economic status. Some have shown utilization of dental services to exhibit a pro-rich socio-economic gradient with respect to income and/or education, though other studies found no relationship between education or income and dental service use in Saudi Arabia (24–26, 28, 29).
Location can play an important role in access to care and, as a result, in relation to utilization of care (30, 31). Whether as a result of where dentists choose to practice or where government chooses to provide services, both of which may see services concentrated in population centers, travel costs may add to the costs of consuming dental care borne by the user/parent and as a result deter utilization of the service for those who, for example, reside away from urban centers. Consistent with this, studies in Saudi Arabia have shown that utilization of oral services was lower in rural areas than in urban areas (27). Similarly, various socio-demographic factors may contribute to differences in either costs or perceived benefits from use of services and underpin differences in use. For example, those who are more affluent may be better able to afford dental care—where their exist co-pays—and/or may attach a higher value to oral health in monetary terms than those who are less well-off and as a result be expected to be more likely to visit the dentist (32). This will similarly apply to education—likely to be positively correlated with income—in that those who are better educated may have higher degrees of health literacy and be better able to identify needs, including that for preventive care, and be expected to make greater use of the services as a result (32, 33). Other studies in Saudi Arabia have also shown income and education to be related to oral health and to use of dental services (34). The number of patients who use dental services was higher among patients whose income was higher in Abha, a city in Saudi Arabia (25). A study conducted in the city of Jazan in Saudi Arabia similarly shows that individuals who had completed only their primary education were half as likely to having regular dental appointments compared with those who had completed higher levels of education (26).
Other studies have shown differences in use related to gender that may be grounded in the value attached to the aesthetic benefits of good oral health or simply in the commonly observed greater likelihood of women to use medical services than men (35). These findings have been echoed in other studies in Saudi Arabia, with men exhibiting a lower likelihood of visiting the dentist when adjusted for covariates than women (28). Other factors that may influence use include marital status (through, e.g., pester power—the spouse pestering their partner to use the services) and age as a result of increasing oral health needs. Studies in Saudi Arabia have demonstrated the role of marital status, one study in the city of Abha in Saudi Arabia finding that participants who were single were more likely to not use dental services than participants who were married (25). In addition, a lack of perceived dental needs was found to be the most significant barrier, which prevented 70.2% of the people from getting dental treatment in Jazan, Saudi Arabia (26).
While studies within Saudi Arabia have examined the role of socio-demographic characteristics in service use, they have not hitherto examined differences in use between regions and only one study has used national data to examine the role of income (36). The study by El Bcheraoui et al. (24), which also used national data to examine use of services for checkups, did not look at the role of income or region where potentially distinct issues in access or cultural norms may give rise to different patterns of service use for checkups (11, 24). The purpose of this analysis was to add to our body of knowledge by looking at the role of income, region, and income within regions (the potential for its role to differ across regions) in utilization of dental services for checkups. In addition to examining the role of socio-demographic status at a national level, the study seeks to determine if the roles of socio-demographic variables and socio-economic status in particular differ between regions, providing insights into patterns of service use for checkups of potential value to policymakers. While the study by El Bcheraoui et al. also contains details on use of services for “dental complaints” as this was a rather broad term, covering the gamut of restorative services, orthodontics, and periodontics, we focused attention on checkups to give sharper focus to the examination.
The Saudi Health Information Survey (SHIS) is a national multistage survey of individuals aged over 15 years old. The survey used in this study was conducted on behalf of the Ministry of Health across 13 administrative regions in Saudi Arabia in 2013. These regions are Al Riyadh; AlQassim; Makkah Al Moukarrama; Tabuk; Hail; Al-Jouf; Al-Baha; Eastern Region; Northern Borders; Madinah; Jazan; Aseer; and Najran. To recruit study participants and to ensure that the survey findings were representative of the population of Saudi Arabia, survey respondents were recruited using a multistage stratified probability sampling method. The stratification was based on the Kingdom's 13 regions. Approximately 12,000 households were randomly selected for participation in the survey from across the 13 regions. A total of 10,827 individuals completed the survey and were contacted by local primary care centers to participate in this study. The primary sampling units are tiny clusters of households that have been broken up and designated by the Census Bureau of the Kingdom of Saudi Arabia. On average, there are approximately 140 households in each of these clusters. The survey gathers information on a wide variety of socio-demographic factors, including age, gender, educational achievement, marital status, and income. The questionnaire also provides data on life style factors such as diet, level of physical activities, and utilization of healthcare services (24).
Descriptive statistics—mean, standard errors, and 95% confidence intervals—across the sample and for sub-samples based on specific regions were used to describe the data and compare differences across regions. Multivariable logistic regression analyses were used to examine the relationship between use of dental services for checkups and respondent characteristics including age, gender (male vs. female), marital status and oral hygiene habits. Service use was dichotomized to capture use in the past 12 months (=1) vs. non-use in this time period (=0). (While the survey identified once and more than once as options, we redefined it as having visited or not, for ease of exposition.) Income was entered into the analysis as a series of categories matching the eight groups contained in the survey—less than 3,000 riyals per month, 3,000–5,000 riyals per month, 5,000 Riyals to less than 7,000 Riyals per month, 7,000 Riyals to less than 10,000 Riyals per month, 10,000 Riyals to less than 15,000 Riyals per month, 15,000 Riyals to less than 20,000 Riyals per month, 20,000 Riyals to less than 30,000 Riyals per month, and 30,000 Riyals or more per month. The corresponding values in Euro are reported in Supplementary Appendix S2. The lowest income group provided the base category against which each of the others was compared. Region was also entered as a series of categorical variables matching the 13 in the survey with Riyadh providing the base category against which the others were compared. Precise details of the survey wording are available from the SHIS results (37). The analysis was confined to those respondents who provided complete data; no attempt was made to impute data. As attention was given to variations among individuals rather than attempting to provide national estimates, no attempt was made to weight the data.
To allow for the possibility that distinct relationships may exist between the likelihood of dental checkup use and respondent characteristics across regions, logistic regression analyses were rerun for sub-groups based on individual regions. Separate analyses for each region were undertaken rather than using models in which interaction terms between, for example, region and individual characteristics were used to allow for the possibility of distinct relationships between covariates and checkup use across regions. A hierarchical logistic regression was also undertaken to evidence the value-added from the inclusion of income and region among the explanatory variables. In the interest of brevity, not all regional analyses are reported, rather those for which the existence of significant differences between regions were evident are reported. Odds ratios were compared across regions based on the point estimate and the associated 95% confidence interval.
Variables were selected for use in the regression analysis based on the Andersen model (38). The model (39) seeks to understand checkup use in terms of factors that can be grouped under headings of need, predisposing, and enabling (40). Predisposing factors, for example, may be related to age or education where perceived risk of tooth decay, for example, may vary across groups for whom the risk of tooth decay varies due to the accumulation of restorative care over time (13) or between whom degrees of health literacy and perceived risk of dental problems varies with education (13). Similarly, with respect to enabling factors, aspects such as income were included, which may affect the affordability of the service or the ability to travel to consume it, and thus the likelihood of use (41). With respect to needs such as arising from the experience of dental pain, unsurprisingly these were not captured directly in a survey of this type though oral hygiene habits—such as use of brushing and flossing that are captured in the survey—may offer an indirect measure of them. While some care is warranted in the grouping of variables under particular headings—for example, oral hygiene could equally be interpreted as a predisposing factor—in as much as they help identify variables that may explain variations in use, the approach has been shown to be helpful (39).
All analyses were conducted using the software Stata Version 16.0.
A total of 7,603 usable responses—with complete data—were obtained from the survey. Table 1 presents the descriptive statistics for this sample. As shown, 11% had visited the dentist for a checkup in the preceding 12 months. 51.5% were male, 18% of the respondents were smokers, and 29.2% were educated to degree level or above. With respect to age, those between 25 and 34 represent the largest age group in the sample, with 27.4%. Approximately 67% of the participants were married. Participants who reported that they floss their teeth at least once a day were 25% of the sample, while 69% reported that they brush their teeth at least once a day. Roughly 3.5% of the sample reported that they use Miswak (tooth stick) at least once a day. The lowest income group comprised 16.5% of the sample, while the highest income group represented 2.4% of the sample. Across the 13 regions in Saudi Arabia, participants from Riyadh region were the largest group, with 15.96% of the sample.
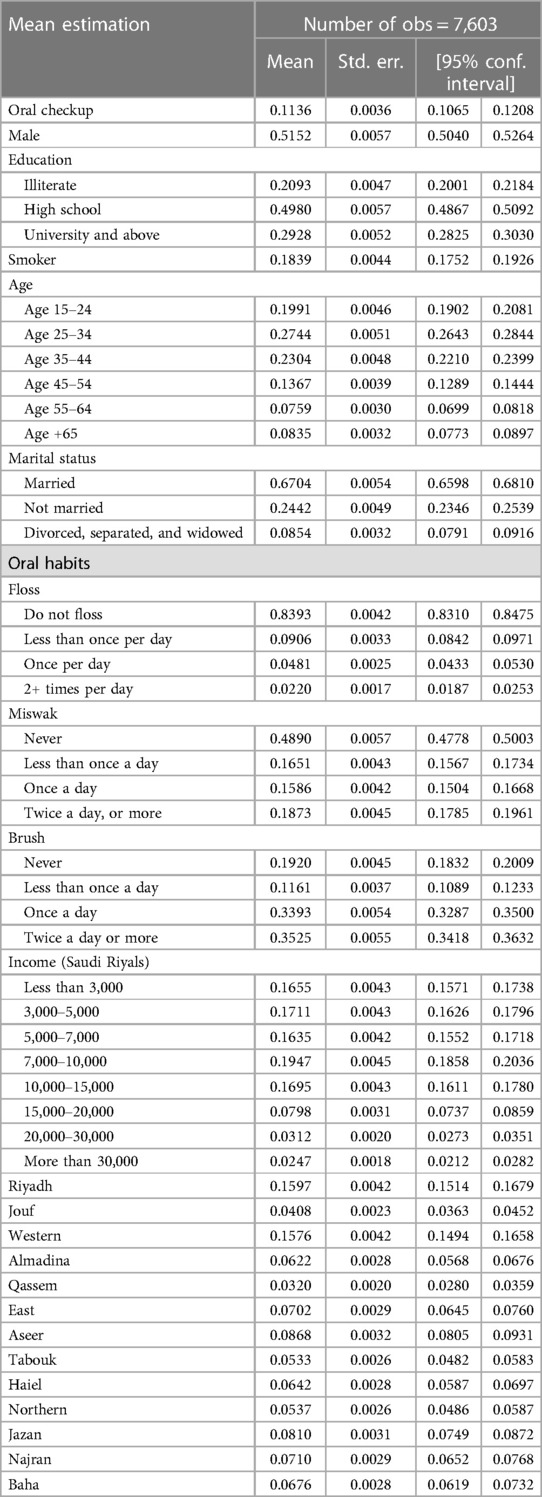
Table 1. Descriptive statistics of the usable sample.
In Table 2, the results of a logistic regression show that there are differences in the likelihood of a visit for a checkup inter alia by region and income. People in the higher-income groups were more likely to have visited the dentist for a checkup in the last 12 months compared with those in the lowest-income group. Similarly, people who were better educated were more likely to have visited a dentist for a checkup than those who were less well educated. Participants aged 15–24 were more likely to have visited a dentist for a checkup in the last 12 months than other age groups. Notably differences in the likelihood of a checkup visit were evident across regions. In Tables 3a–c, moreover, it is seen that differences in the role of socio-demographic variables also exist between regions. While income is a significant determinant of the likelihood of a checkup in Riyadh and Jazan, for example, this is not the case in Baha; similarly, while age is significant in both the former regions, this is not the case in Baha. In Table 4, the results of the hierarchical model are reported. As can be seen from the likelihood ratio results and from the Akaike information criterion (AIC) statistics, the inclusion of income and region add to the explanatory power of the model.
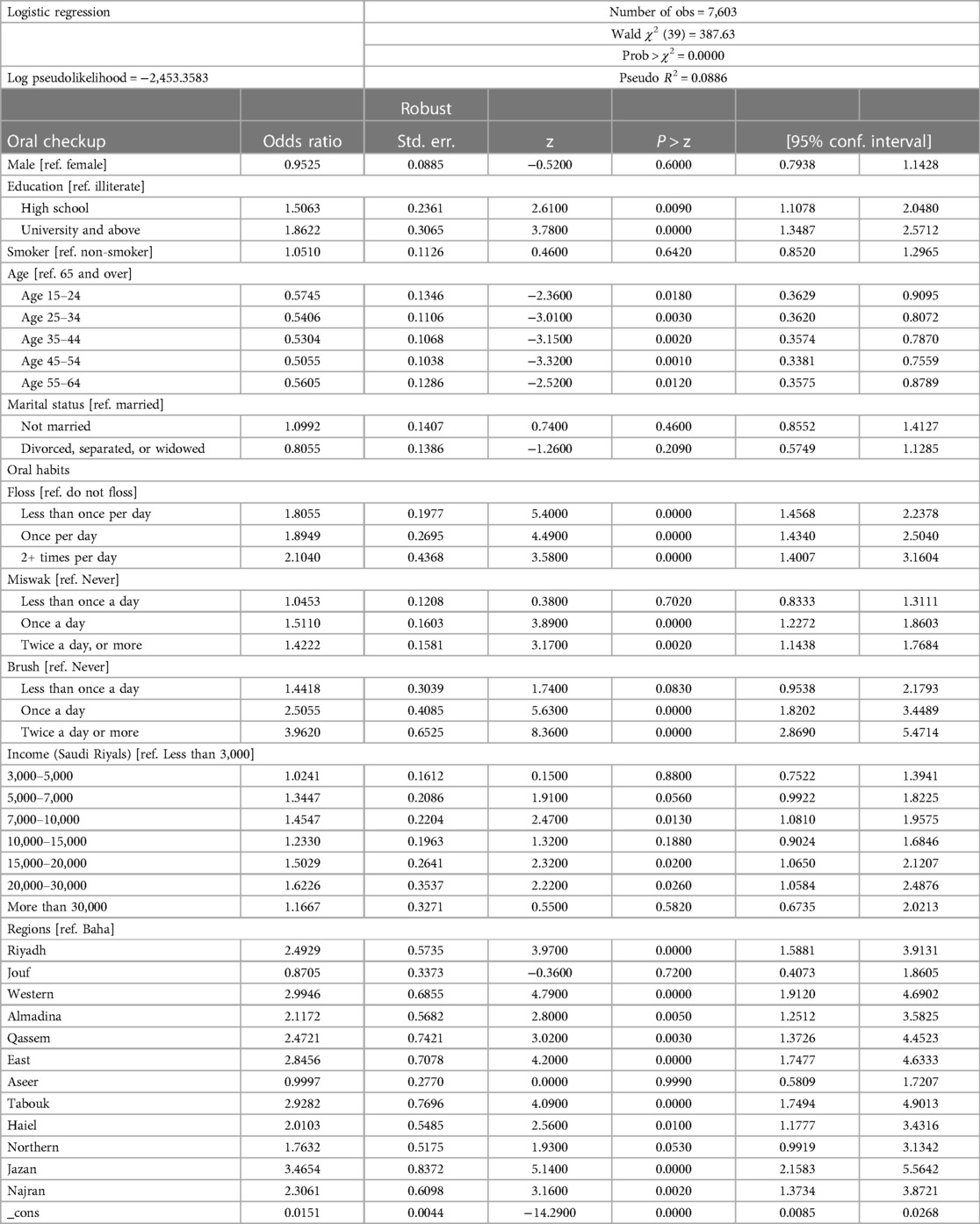
Table 2. Logistic regression of oral checkup for the entire sample.
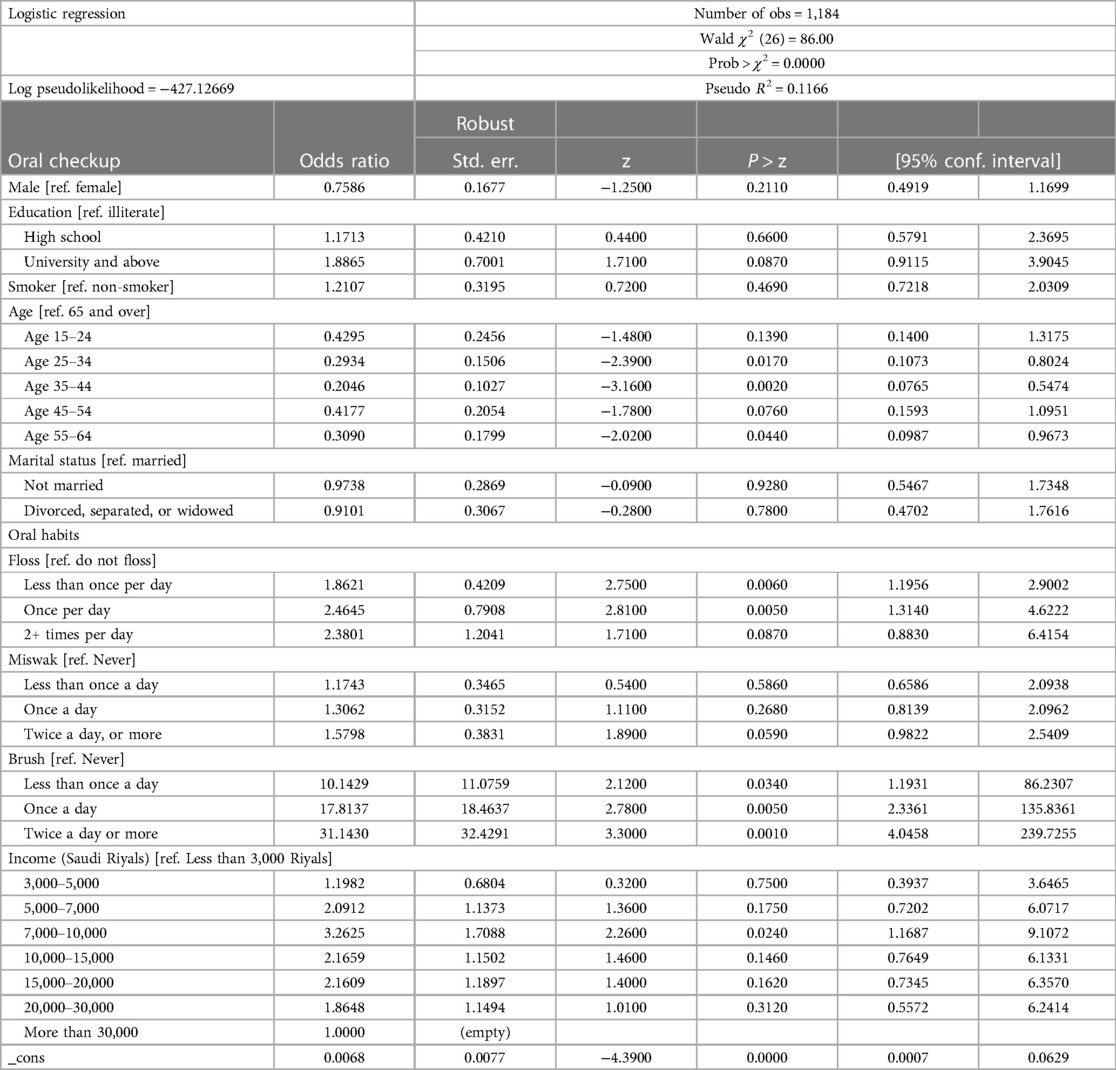
Table 3a. Logistic regression of regions Riyadh.
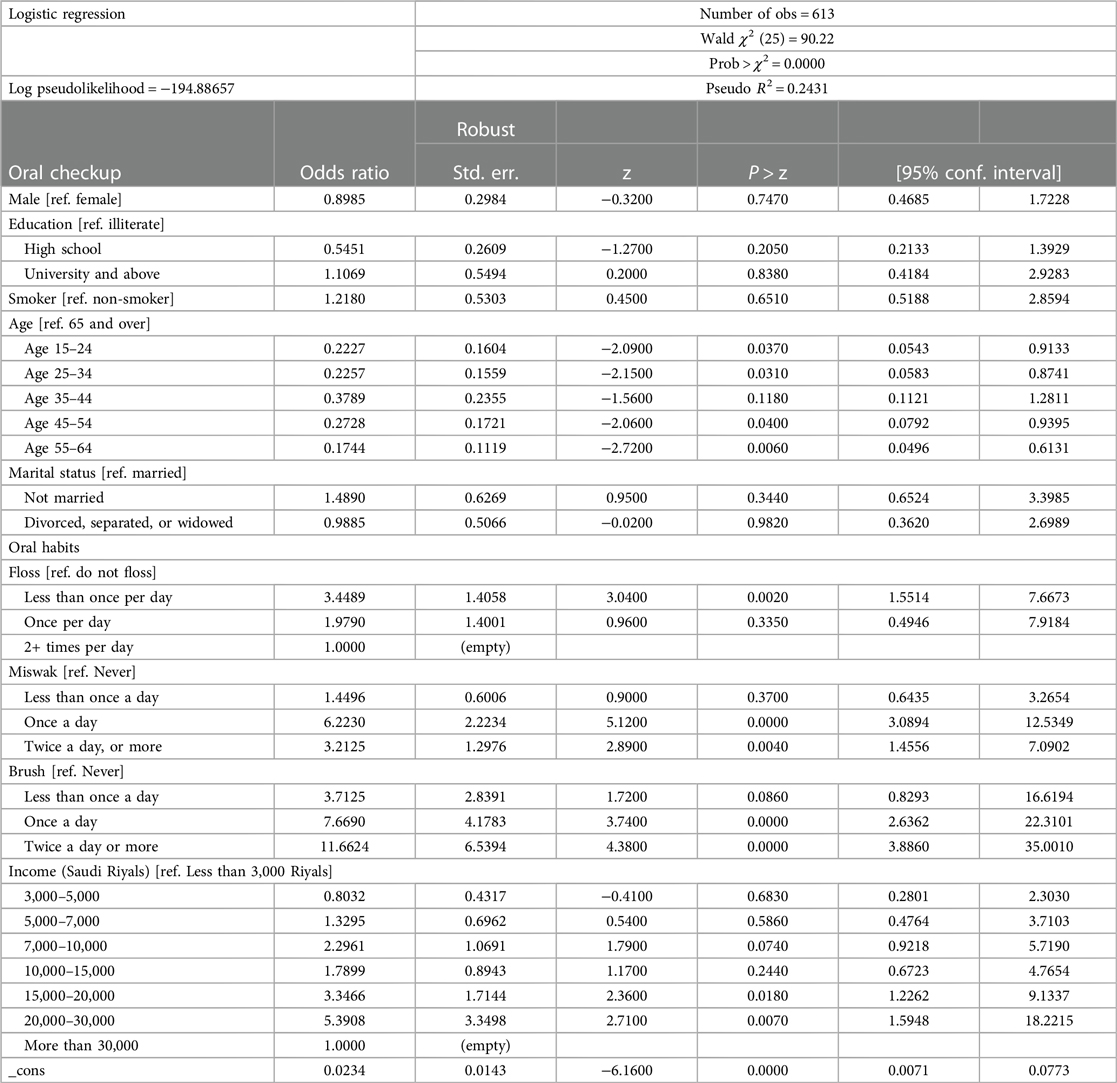
Table 3b. Logistic regression of Jazan.
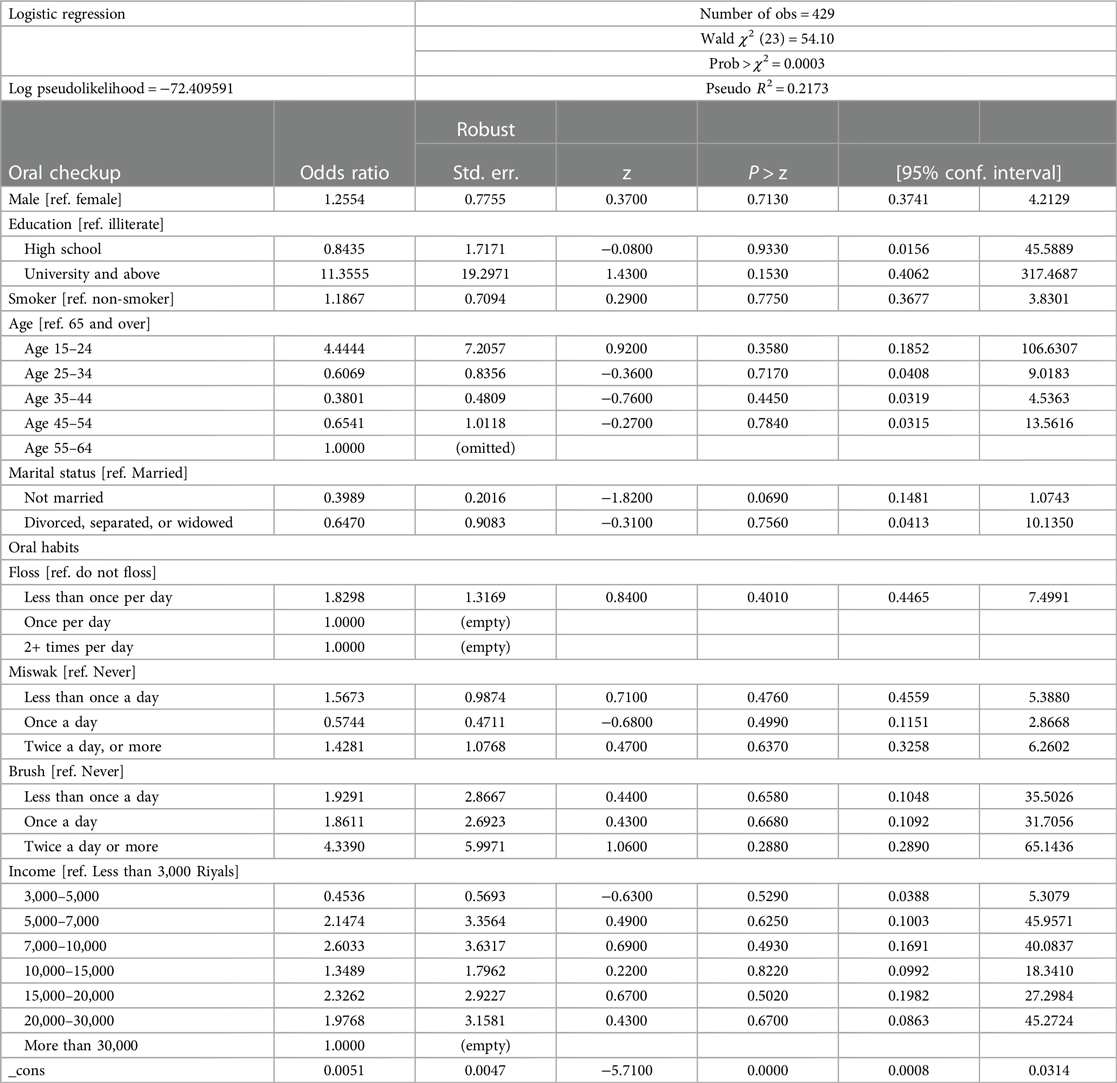
Table 3c. Logistic regression of Baha.
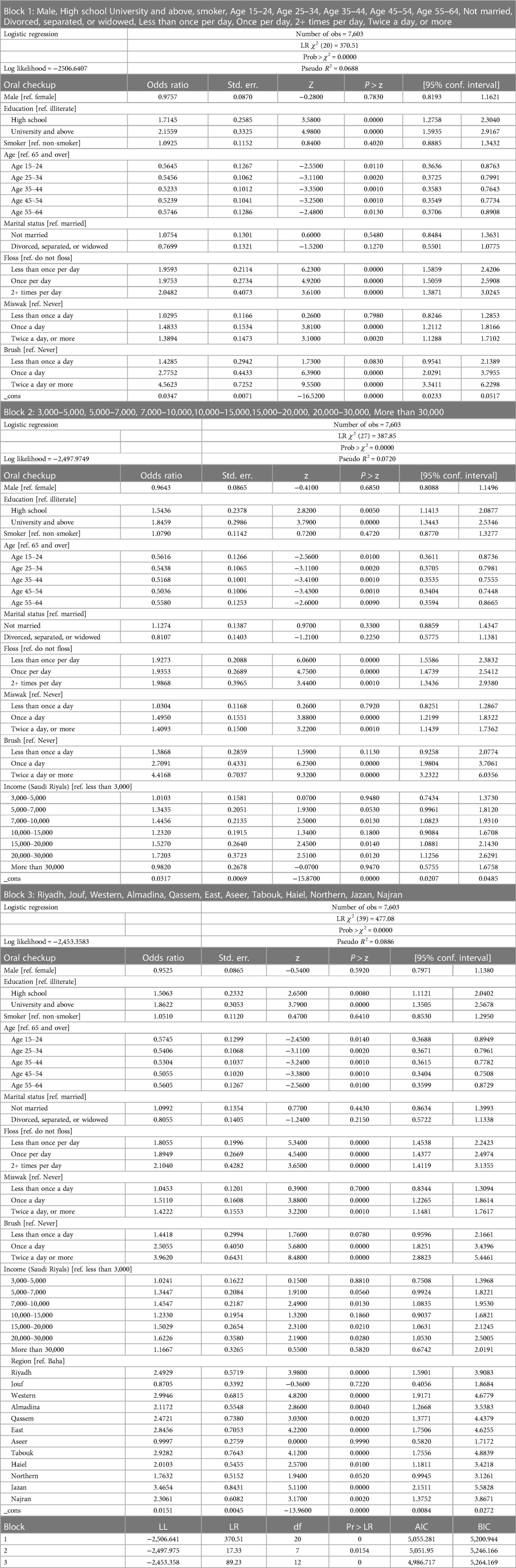
Table 4. Hierarchical logistic regression.
Saudi Arabia has embarked on a swath of reforms in an effort to reduce its dependence on oil revenues for public finance. The healthcare reforms under Vision 2030 in Saudi Arabia are transforming the healthcare landscape, including dental care (42). These reforms have the potential to provide long-lasting financial support, particularly for dental care. This strategy could greatly help in overcoming the obstacles that currently prevent people with lower incomes from accessing oral health services (43). The healthcare reforms in Saudi Arabia are working toward creating a future in which dental services are easily available, integrated into the healthcare system, and in line with a broader goal of total wellbeing. Large, nationally representative surveys can provide valuable insights to help guide these policy reforms by identifying those factors that influence utilization and that government may need to take cognizance of when devising policies to address particular barriers or facilitators to service use. This includes the role of income and region, where the role of region can extend beyond rurality (44). Small localized studies are limited in their ability to shed light on such issues, perhaps lacking statistical power or representation across a breadth of regions. Similarly, the opportunity to pool results from smaller local studies is limited by the heterogeneity in sampling methods, the covariates included, and even how utilization is framed in survey questions (39). Only larger national studies provide an opportunity to examine variation in service use generally, including that for checkups as examined here, using data collected in a consistent manner. Of the two previous studies that have examined dental service use in Saudi Arabia using national data (24, 36), one included income but did not examine region while the other examined neither the role of region nor income. A recent systematic review of the literature on inequalities in dental service has demonstrated that those with lower incomes are consistently less likely to use dental services (29). The findings of Sahab et al. (36) echo this for Saudi Arabia and underscore the value of its inclusion in studies of service use. Our own findings echo this with respect to checkups. Our results are broadly consistent with those of Sahab et al., which suggest the relationship with income is non-linear, increasing before falling.
The same review has highlighted differences between geographic areas differentiated by rurality—those from rural areas exhibiting lower utilization (29)—a finding at variance with that by Sahab et al. though echoed in studies undertaken subsequent to this review (45, 46). In this study, we clearly demonstrate in Tables 2 and 4 the importance of including region and income among the list of explanatory variables when examining the likelihood of getting a checkup, while Tables 3a–3c underscore the potential for the role of individual characteristics to vary between regions. This study provides evidence that points to the existence of differences between regions in the likelihood of a checkup—those in Jazan being more likely to visit a dentist while those in Jouf and Aseer were less likely to visit one than were those in Riyadh—and of distinct patterns within regions between the likelihood of a checkup and socio-demographic variables. Interestingly, this is seen not just with respect to income or age but also oral hygiene habits where, for example, in Riyadh these were positively related to the likelihood of a checkup (as was the case nationally), but in Baha there is no significant relationship. The existence of regional effects—differences between regions and in relationships within regions—suggests a one-size-fits-all model whether related to financial support for access or health education messages that may lack nuance. Rather differences between regions that may reflect differences in customs—for example, how westernized diets are or how sharp income inequalities are within regions—may require adjustments to policy. For example, in those areas where diet is an issue health education may be prioritized, while in those areas where access to dental checkups is an issue, increased supply may be prioritized. Interestingly perhaps, given the role of cultural norms around chaperoning of women, there were no differences in the likelihood of a checkup related to gender. That women do not seem to have experienced an additional barrier arising from this cultural norm is reassuring given the importance of checkups for prevention.
Clearly, the use of dental services for checkups in Saudi Arabia is influenced by the interplay of region and other individual level variables including income and age. Tables 3a–3c, highlight the complex connection between individual socio-economic variables and regions that may relate to the availability of oral healthcare services in different geographical areas—enabling factors in the Andersen framework. Urban areas typically provide a broader choice of dentists within close proximity of each other that may serve to encourage regular dental checkups (and perhaps induce demand from the public). Conversely, rural regions sometimes encounter challenges related to inadequate accessibility to dental facilities (36). Equally though, there could be differences in culture between regions that have a significant effect on patterns of use. Similarly, with respect to income, this could directly impact use of checkups as an enabling factor—how easy it is for a person, for example, to travel to the dentist—as well as indirectly, for example, in terms of the value to them of investments in preventive care—those with lower incomes typically facing financial barriers that lead to delayed or skipped checkups (47). This may help explain the role of these variables in our analysis, but further research on rurality, access, and income are warranted.
Unlike Sahab et al, this study was able to explore the role of oral health habits that those with good oral hygiene habits are more likely to use services for checkups is consistent with previous work by the authors (39) that highlighted the importance of differentiating between the types of need and types of care provided when examining utilization. While we were unable to examine the relationship between hygiene habits and use of dentists for specific treatment, it may well be the case that distinct relationships exist in this regard. The absence of income and region in previous analyses—which we have shown to be significant—demonstrates their importance (44) and the importance of their inclusion (36).
Comparing the sample that we used with that we did not use due to non-response in particular items, we can see that among those who provide complete responses, the percentage of men is higher, 52% of the respondents were male compared with 42% in the excluded sample (reported in Supplementary Appendix S1 Table S5), while the percentage of individuals with higher education is higher in the used sample than in the excluded sample (those with degrees were 29% in the used sample and 17% in the excluded sample). We can only speculate as to why they did not provide complete responses, although it is conceivable that women and those who are less well educated may encounter greater barriers in completing surveys of this type. While the usable sample differs in some respects from the full sample in terms of its representativeness, it is unlikely given its size and the numbers across distinct groups we were able to use that this had a material effect on results.
The study has a number of limitations. First, the data on which the analyses are based are over 10 years old. Given various factors including service provision, access, oral hygiene habits, and income may have changed in the intervening period, the relationships described may have altered somewhat since. That said, the study provides a snapshot of relationships at that time that will provide a useful comparator for future work it will hopefully encourage. Second, we were unable to look at different types of needs that may have prompted a checkup, for example, pain, routine behavior, and worry related to another oral health issue (39). Data on how frequently the respondent visited the dentist might provide further useful insights into patterns of use—in addition to how recently they visited, but this was not available. Third, the used sample of respondents was more likely to be better educated and male than the sample excluded due to non-response. This may have introduced an element of non-response bias, although large numbers of both genders and all education groups remained in the used sample. Fourth, the data are cross-sectional, which prevents us from looking at how patterns of use changed as individual circumstances changed. Our findings must therefore be interpreted as associations rather than causal. Further research could address these issues and examine how patterns of service use change in light of any reforms enacted in Saudi Arabia.
National surveys can provide valuable insights into the associations between socio-demographic characteristics and utilization of dental services for policymakers. While previous studies in Saudi Arabia have examined the role of income and provided insights into differences between regions, only two studies have made use of large national datasets to examine these issues. Only one study has examined income, and neither has examined the potential for differences across regions. Our study echoes the previous national study with respect to income and identifies the existence of differences between regions in service use related to checkups as well as patterns of service use. That there exists evidence to suggest that across and within regions there are inequalities in uptake of checkups suggests policymakers should undertake further work to satisfy themselves that these are not grounded in differential access rather than the preferences of respondents, and if they are, adopt bespoke policies to address the barriers that exist.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
MA led the overall study, contributed to the data collection and interpretation, and wrote the article. CO contributed to the data collection, data analysis, and article edits. GM contributed to the data interpretation and article edits. IA contributed to article edits. RA contributed to article edits and organized the database. All authors contributed to the article and approved the submitted version.
The study was undertaken as part of a PhD funded by the Ministry of Education, Saudi Arabia.
The authors would like to thank all participants who participated in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2023.1208929/full#supplementary-material
1. Ageing and health expenditure—UK Health Security Agency. Available at: https://ukhsa.blog.gov.uk/2019/01/29/ageing-and-health-expenditure/ (Accessed October 12, 2022).
2. Howdon D, Rice N. Health care expenditures, age, proximity to death and morbidity: implications for an ageing population. J Health Econ. (2018) 57:60–74. doi: 10.1016/j.jhealeco.2017.11.001
3. Withrow D, Alter DA. The economic burden of obesity worldwide: a systematic review of the direct costs of obesity. Obes Rev. (2011) 12:131–41. doi: 10.1111/j.1467-789X.2009.00712.x
4. Economic Costs. Obesity Prevention Source | Harvard T.H. Chan School of Public Health. Available at: https://www.hsph.harvard.edu/obesity-prevention-source/obesity-consequences/economic/ (Accessed October 12, 2022).
5. Spending Review 2021: what it means for health and social care. Available at: https://www.health.org.uk/news-and-comment/charts-and-infographics/spending-review-2021-what-it-means-for-health-and-social-care (Accessed October 12, 2022).
6. Heron L, O’Neill C, McAneney H, Kee F, Tully MA. Direct healthcare costs of sedentary behaviour in the UK. J Epidemiol Community Health. (2019) 73:625–9. doi: 10.1136/jech-2018-211758
7. Hartwig J. What drives health care expenditure?—Baumol’s model of “unbalanced growth” revisited. J Health Econ. (2008) 27:603–23. doi: 10.1016/j.jhealeco.2007.05.006
8. Smith S, Newhouse JP, Freeland MS. Income, insurance, and technology: why does health spending outpace economic growth? Health Aff (Millwood). (2009) 28:1276–84. doi: 10.1377/hlthaff.28.5.1276
9. Health expenditure per capita | Health at a Glance 2021: OECD Indicators | OECD iLibrary. Available at: https://www.oecd-ilibrary.org/sites/154e8143-en/index.html?itemId=/content/component/154e8143-en (Accessed October 12, 2022).
10. Dental Services Market Size, Growth, Trends 2022-2030 | BioSpace. Available at: https://www.biospace.com/article/dental-services-market-size-growth-trends-2022-2030/ (Accessed October 12, 2022).
11. Health workforce. Available at: https://www.who.int/health-topics/health-workforce#tab=tab_1 (Accessed October 12, 2022).
12. Raftery J. NICE: faster access to modern treatments? Analysis of guidance on health technologies. BMJ. (2001) 323:1300. doi: 10.1136/bmj.323.7324.1300
13. Hill KB, Chadwick B, Freeman R, O’Sullivan I, Murray JJ. Adult Dental Health Survey 2009: relationships between dental attendance patterns, oral health behaviour and the current barriers to dental care. Br Dent J. (2013) 214:25–32. doi: 10.1038/sj.bdj.2012.1176
14. Mouradian WE, Wehr E, Crall JJ. Disparities in children’s oral health and access to dental care. JAMA. (2000) 284:2625–31. doi: 10.1001/jama.284.20.2625
15. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century—the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. (2003) 31(Suppl. 1):3–24. doi: 10.1046/j..2003.com122.x
16. Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. (2012) 380:2163–96. doi: 10.1016/S0140-6736(12)61729-2
17. Almalki M, Fitzgerald G, Clark M. Health care system in Saudi Arabia: an overview. East Mediterr Health J. (2011) 17:784–93. doi: 10.26719/2011.17.10.784
18. Saudi Arabia 2030 vision. Vision2030. Available at: https://www.vision2030.gov.sa/media/rc0b5oy1/saudi_vision203.pdf (Accessed October 12, 2022).
19. Rahman R. The privatization of health care system in Saudi Arabia. Health Serv Insights. (2020) 13:1178632920934497. PMID: 32636636; PMCID: PMC7315664. doi: 10.1177/1178632920934497
20. Walston SL, Al-Harbi Y, Al-Omar B. The changing face of healthcare in Saudi Arabia. Ann Saudi Med. (2008) 28:243. doi: 10.5144/0256-4947.2008.243
21. Healthcare Development Strategies in the Kingdom of Saudi Arabia. Healthcare Development Strategies in the Kingdom of Saudi Arabia. 2002. doi: 10.1007/B112322
22. Shubayr MA, Kruger E, Tennant M. Access to dental-care services in Jazan, Saudi Arabia: a scoping review. Saudi J Health Syst Res. (2021) 2:9–19. doi: 10.1159/000517661
23. Aldossary A, While A, Barriball L. Health care and nursing in Saudi Arabia. Int Nurs Rev. (2008) 55:125–8. doi: 10.1111/j.1466-7657.2007.00596.x
24. El Bcheraoui C, Tuffaha M, Daoud F, Kravitz H, Almazroa MA, Al Saeedi M, et al. Use of dental clinics and oral hygiene practices in the Kingdom of Saudi Arabia, 2013. Int Dent J. (2016) 66:99. doi: 10.1111/idj.12210
25. Almutlaqah MA, Baseer MA, Ingle NA, Assery MK, Al Khadhari MA. Factors affecting access to oral health care among adults in Abha City, Saudi Arabia. J Int Soc Prev Community Dent. (2018) 8:431. doi: 10.4103/jispcd.JISPCD_205_18
26. Quadri FA, Jafari FA, Albeshri AT, Zailai AM. Factors influencing patients’ utilization of dental health services in Jazan, Kingdom of Saudi Arabia. Int J Clin Pediatr Dent. (2018) 11:29. doi: 10.5005/jp-journals-10005-1479
27. Orfali SM, Aldossary MS. Saudi Journal of Oral and Dental Research Abbreviated Key Title: Saudi J Oral Dent Res ISSN. 2020. doi: 10.36348/sjodr.2020.v05i03.002
28. Al-Jaber A, Da’ar OB. Primary health care centers, extent of challenges and demand for oral health care in Riyadh, Saudi Arabia. BMC Health Serv Res. (2016) 16:1–8. doi: 10.1186/s12913-016-1876-6
29. Reda SF, Reda SM, Murray Thomson W, Schwendicke F. Inequality in utilization of dental services: a systematic review and meta-analysis. Am J Public Health. (2018) 108:e1–7. doi: 10.2105/AJPH.2017.304180
30. Jo O, Kruger E, Tennant M. Disparities in the geographic distribution of NHS general dental care services in England. Br Dent J. (2021) PMID: 34045676. doi: 10.1038/s41415-021-3005-0 [Epub ahead of print].
31. Davis J, Liu M, Kao D, Gu X, Cherry-Peppers G. Using GIS to analyze inequality in access to dental care in the district of Columbia. AMA J Ethics. (2022) 24:41–7. doi: 10.1001/amajethics.2022.41
32. Gao X, Ding M, Xu M, Wu H, Zhang C, Wang X, et al. Utilization of dental services and associated factors among preschool children in China. BMC Oral Health. (2020) 20:1–10. doi: 10.1186/s12903-019-0991-2
33. Piovesan C, Antunes JLF, Guedes RS, Ardenghi TM. Influence of self-perceived oral health and socioeconomic predictors on the utilization of dental care services by schoolchildren. Braz Oral Res. (2011) 25:143–9. doi: 10.1590/S1806-83242011005000004
34. Ellakany P, Madi M, Fouda SM, Ibrahim M, Alhumaid J. The effect of parental education and socioeconomic status on dental caries among Saudi children. Int J Environ Res Public Health. (2021) 18(22):11862. PMID: 34831618; PMCID: PMC8619270. doi: 10.3390/ijerph182211862
35. Lipsky MS, Su S, Crespo CJ, Hung M. Men and oral health: a review of sex and gender differences. Am J Mens Health. (2021) 15(3). doi: 10.1177/15579883211016361
36. Sahab DA, Bamashmous MS, Ranauta A, Muirhead V. Socioeconomic inequalities in the utilization of dental services among adults in Saudi Arabia. BMC Oral Health. (2022) 22:1–11. doi: 10.1186/s12903-022-02162-w
37. Saudi Health Interview Survey Results. Available at: https://www.healthdata.org/sites/default/files/files/Projects/KSA/Saudi-Health-Interview-Survey-Results.pdf (Accessed November 20, 2023).
38. Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Q. (2005) 83(4):10.1111/j.1468-0009.2005.00428.x. PMCID: PMC2690261. doi: 10.1111/j.1468-0009.2005.00428.x
39. Almutairi M, McKenna G, O’Neill C. A comparative examination of the role of need in the relationship between dental service use and socio-economic status across respondents with distinct needs using data from the Scottish Health Survey. BMC Public Health. (2023) 23:1–10. doi: 10.1186/s12889-023-15078-z
40. Baker SR, Baker S. Applying Andersen’s behavioural model to oral health: what are the contextual factors shaping perceived oral health outcomes? Community Dent Oral Epidemiol. (2009) 37:485–94. doi: 10.1111/j.1600-0528.2009.00495.x
41. Hajek A, Kretzler B, König HH. Factors associated with dental service use based on the Andersen model: a systematic review. Int J Environ Res Public Health. (2021) 18(5):2491. PMID: 33802430; PMCID: PMC7967618. doi: 10.3390/ijerph18052491
42. Aldossary MS. Dental governance and the Saudi vision 2030: a narrative review. Saudi J Health Syst Res. (2022):1–7. doi: 10.1159/000526361
43. Alasiri AA, Mohammed V. Healthcare transformation in Saudi Arabia: an overview since the launch of vision 2030. Health Serv Insights. (2022) 15:11786329221121214. PMID: 36081830; PMCID: PMC9445529. doi: 10.1177/11786329221121214
44. Hartley D. Rural health disparities, population health, and rural culture. Am J Public Health. (2004) 94(10):1675–8. PMID: 15451729; PMCID: PMC1448513. doi: 10.2105/ajph.94.10.1675
45. Smith S, Jiang JJ, Normand C, O’Neill C. The price of private dental services: results from a national representative survey of Ireland. Ir J Med Sci. (2023) 192:973–83. doi: 10.1007/S11845-022-03041-7
46. Kamil W, Kruger E, McGeachie J, Jean G, Tennant M. Distribution of Australian dental practices in relation to the ageing population. Gerodontology. (2022) 39:302–9. doi: 10.1111/ger.12585
Keywords: Saudi Arabia, dental service use, regional variation, dental checkup, income
Citation: Almutairi M, McKenna G, Alsumaih I, Alhazzaa R and O’Neill C (2023) Factors influencing the likelihood of dental service checkup: results from a survey in Saudi Arabia. Front. Oral. Health 4:1208929. doi: 10.3389/froh.2023.1208929
Received: 15 May 2023; Accepted: 24 November 2023;
Published: 15 December 2023.
Edited by:
Mihajlo (Michael) Jakovljevic, Hosei University, JapanReviewed by:
Mir Faeq Ali Quadri, University of Washington, United States© 2023 Almutairi, McKenna, Alsumaih, Alhazzaa and O’Neill. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Majed Almutairi bWFsbXV0YWlyaTAyQHF1Yi5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.