 Manal Awad1,2*
Manal Awad1,2* Wegdan Bani Issa1,3
Wegdan Bani Issa1,3 Hadia Radwan1,4
Hadia Radwan1,4 Randa Fakhry1,3
Randa Fakhry1,3 Nabeel Al-Yateem1,3,5Rachel Rossiter5
Nabeel Al-Yateem1,3,5Rachel Rossiter5
- 1Research Institute for Medical and Health Sciences, University of Sharjah, Sharjah, United Arab Emirates
- 2Department of Preventive & Restorative Dentistry, College of Dental Medicine, University of Sharjah, Sharjah, United Arab Emirates
- 3Department of Nursing, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates
- 4Department of Clinical Nutrition and Dietetics, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates
- 5School of Nursing, Paramedicine and Healthcare Sciences, Faculty of Science and Health, Charles Sturt University, Wagga Wagga, NSW, Australia
Background: Obesity and dental caries among adolescents is a growing worldwide public health issue. They share some common and modifiable influences. The objective of this study was to evaluate the association between obesity and dental caries among adolescents in the United Arab Emirates (UAE).
Methods: This pilot cross-sectional study enrolled 161 adolescents 13–19 years old from private and public schools in the UAE. Participants were classified as normal weight, underweight, overweight or obese. Dental caries was diagnosed according to the criteria recommended by the World Health Organization (WHO). Independent t-tests were used to compare average number of decayed, missing and filled surfaces (DMFS) by age, sex, school type, mothers’ employment, BMI categories, waist circumference, oral health habits and plaque index. Additionally, a multiple linear regression model was applied to analyze the association between BMI, waist circumference and dental caries, adjusted for confounding factors considered in this study.
Results: The average age of the participants was 16.2 ± 1.4 years old. The prevalence of overweight/obesity was 42% (N = 68) measured by BMI. In addition, 82% (N = 132) had average waist circumference and 18% (N = 29) with above average waist circumference. Overall, the average DMFS score was 4.35 ± 4.5, with significantly lower dental caries rates among girls ([3.3 (SD:4.0)] than boys (6.7 (SD:5.3), (p < 0.05). The linear regression model revealed that, being a male, attending a public school and having average waist circumference were all positively and significantly associated with dental caries (p < 0.05).
Conclusion: Obesity measured by waist circumference was significantly associated with dental caries among adolescents in the UAE. Further research is required to investigate the complex association between obesity and dental caries and how dietary habits, oral hygiene habits, and parental socioeconomic status mediate the association between obesity and dental caries.
Introduction
Dental caries remains one of the most prevalent chronic diseases worldwide (1–3). However, previous reports suggest that the profile of dental caries is heterogeneous across developing and developed countries, with large disparities reported between and within groups (3, 4). In 2017, dental caries affected 621 million children worldwide (3). Furthermore, in 2010, it has been estimated that 298 billion USD was spent on direct costs associated with dental caries, accounting for a substantial percentage of the total financial global expenditure (3). A recent systematic review in the MENA region (2) showed that there is a relatively high prevalence of dental caries in most MENA countries. For example, in Saudi Arabia, studies published from 2008 to 2018 showed a prevalence that ranged from 49%–91% (5). In the UAE, the prevalence of dental caries among school age children 11–17 years old was reported to be 75% and the mean DMFT score was 3.19 (SD:2.9) (2).
Dental caries is strongly influenced by sugar intake from energy-rich foods and drinks, which also play an important role in the development of obesity. Despite the number of studies conducted on this topic (6–16), the association between BMI and dental caries is still not clear (10, 12–23). Some studies demonstrated a positive association between BMI and dental caries (12–15), while others reported an inverse relationship (16–21) or no relationship (22–24). Findings from systematic reviews were also inconclusive (7, 12, 24–26). For example, based on their systematic review, Manohar et al. (26) concluded that there was a positive association between dental caries and obesity/overweight and that both conditions were associated with parental lower income and level of education. Hooley et al. (27) showed that almost half of the studies included in their systematic review reported no association between dental caries and BMI, as well as negative and positive associations between the two factors. They argued that this finding could be attributed to several factors including socioeconomic characteristics. Given the evidence from this systematic review, as well as, other studies (6, 10), it is possible that the association between obesity and dental caries is culturally dependent. For example, in some countries, higher rates of dental caries are observed among children of lower socioeconomic status (28). While in other countries the reverse is observed, and children from high socioeconomic groups eat more fermentable carbohydrates and may be at an increased risk of dental caries (29).
Dental caries and obesity are two conditions that could be associated with long term negative health consequences such as cardiovascular diseases and diabetes (30, 31). Furthermore, reports from previous studies showed that both diseases are directly linked to poorer quality of life among adolescents (32–34). Therefore, implementation of effective public health measures to address both conditions necessitates a better understanding of the nature of the association, in the context in which tailored interventions will be applied.
Arab adolescents exhibit different dietary habits and lifestyle factors compared to other countries and the prevalence of both obesity and dental caries is relatively high (35–37). In a recent study, it was reported that the prevalence of overweight and obesity among adolescents in the UAE was 34% (35). Moreover, Khadir et al. study (37) demonstrated that among 11–17 year old school children, 72% had at least one decayed tooth. However, information about the association between the two conditions is scarce. Therefore, the aim of the present study was to assess the association between obesity and dental caries among adolescents in the UAE.
Subjects and methods
Study design and setting
Data collected in the present study is part of a larger cross-sectional study that reported the prevalence of overweight/obesity among adolescents in the UAE (34). In the study, a one-stage cluster sampling technique was utilized and a sample of 932 adolescents aged 13–19 years old was recruited from intermediate and high schools (secondary education). Schools were randomly selected from lists obtained from the Ministry of Education and other private/public school governing bodies in the UAE's seven emirates (Sharjah, Dubai, Abu Dhabi, Ajman, Ras Al Khaimah, Fujairah, and Umm Al Quwain). The data used in this study comprised a sample of 161 adolescents who participated in the original cross-sectional study. To increase cooperation of the schools’ staff in data collection, and reduce interruptions to educational activities, principals of the selected schools were asked to choose the classes from grades 9–12 that would be available to participate in the study. All students in the selected classrooms were invited to take part in this research.
Participants in this study were male and female students in grades 9–12 who attended private or public schools, of any nationality and whose parents consented for them to take part in the study. Because management of chronic conditions requires following certain dietary and other life practices which may affect anthropometric measurements, students were excluded if they had any chronic condition, such as diabetes, cancer and mental conditions.
Data collection
Participating students completed a self-report questionnaire that included questions about sociodemographic characteristics, frequency of tooth brushing and number of visits to the dentist. Trained research assistants administered the questionnaire in the selected classrooms. Participating students were then directed to the on-site school clinic where anthropometric measurements were taken by the same research team using standardized techniques. This was done to maintain consistency and uniformity in the data collection process across different sites. Two calibrated dentists conducted the oral examinations. Data were collected from September 2018 to May 2019, which was a regular school period excluding the summer holiday. In the UAE, there are no large seasonal variations during this part of the year and the temperature falls to an acceptable range; therefore, we anticipated no seasonal differences in anthropometric measurements.
Measurements
The self-reported questionnaire included sociodemographic data (age, sex, nationality: nationals vs. non-nationals), and type of school (private vs. public) and mothers’ employment (employed/unemployed). Participants were also asked about the frequency of visits to the dentist (once a year or less than once a year) and frequency of tooth brushing (2–3 times/day or less than once/day).
Anthropometric measurements and indices
To ensure study reliability, a training and calibration process was carried out by one of the research team members who is an expert on anthropometric measurements (HR). Anthropometric indices included height (cm), weight (kg) and waist circumference (WC). For these measurements, students removed their shoes and wore minimal light-weight clothing as per World Health Organization (WHO) guidelines (37). Participants’ heights (to the nearest 0.1 cm) and weights (to the nearest 0.1 kg) were measured using a telescopic measuring rod (Seca 220) for column scales. Measurement for WC was recorded for each participant using an inextensible anthropometric tape (Seca 201). These measurements were taken while participants stood erect with their arms by their sides and feet close together. BMI (weight in kg divided by height in m2) was calculated and classified according to WHO criteria: underweight = BMI <3rd percentile; normal weight = BMI between the 3rd and 85th percentile; overweight = BMI between the 85th and 97th percentile; and obesity = BMI >97th percentile (37–39). However, because there are clinical limitations in using BMI to estimate obesity in adolescent populations and due to the lack of a gold standard to define obesity, in this study, we also reported WC as an obesity index. In the present study, waist circumference was categorized as average or above average using cutoff points for Arab adolescents (40).
Oral health measurements
Oral examination was performed in the school premises using a portable dental chair and each student was comfortably seated. The dentists assessed oral hygiene status on a one-to-one basis using a disposable dental mirror with a light-emitting diode (LED) light and ball-end Community Periodontal Index (CPI) probe. Food debris was gently removed to avoid the under-recording of dental caries.
The dental caries activities in the participants were expressed as number of decayed, missing and filled teeth (DMFS). In this study, dental caries was recorded following the WHO recommendation (41). A tooth is recorded as missing due to caries if there was a history of extraction because of pain and or the presence of a cavity prior to extraction. Prevalence of plaque was assessed using the modified Quigley-Hein plaque index, in which, 0 = no plaque and 5 = plaque covering two-thirds or more of the crown of the tooth. Students lined up in a classroom and all examinations were conducted by two trained dentists who were calibrated for diagnosing decayed teeth and the plaque index. The degree of agreement was assessed, and the kappa coefficients were more than 0.80.
Dental caries experience was measured via the decayed–missing–filled surface (DMFS) index. DMFS is a cumulative measurement obtained by summing the number of decayed (D), missing (M), and filled (F) surfaces. A tooth surface that is decayed but has not been filled would be recorded as decayed (D). When a tooth was extracted due to caries, it would be recorded as missing (M). A tooth was recorded as filled (F) when it was permanently filled without caries.
Data analysis
We used SPSS version 26 for all statistical analyses. Descriptive characteristics were calculated (frequency, percentage, mean, and standard deviation). Next, we used bivariate analysis to assess the differences in categorical variables and DMFS scores using independent t-test and analysis of variance (ANOVA).
A multilevel regression model was performed to take into account the schools cluster. In the first phase a “null model” without any independent variables was analyzed to verify whether there was a significant variation across the clusters (schools) regarding DMFS scores. The “null model” indicated that there was no significant clustering effects and all of the observations in the data can be treated as independent using single level model.
Therefore, Linear multiple regression was utilized to assess the association between dental caries (DMFS) (the dependent variable) and obesity (BMI and WC) (the independent variable) adjusted for sociodemographic factors, school, and plaque index. Results of the linear regression model using alpha level 0.05 (two-sided) was considered statistically significant.
Ethics
Ethical approval to conduct this study was obtained from the University of Sharjah Research Ethics Committee (REC/15/12/10) and the UAE Ministry of Health and Prevention (MOHAP REC-11). Parental consent was obtained for each student that agreed to participate.
Results
Participants’ characteristics, dental caries activities and oral health habits
Table 1 presents the participants’ characteristics. The mean age of the participants was 16.2 (SD: 1.4). In this study 109 (67.7%) attended public schools, and 41 (25%) children indicated that their mothers were employed. The mean DMFS scores was 4.35 ± 4.5. The prevalence rate of overweight/obesity was 42% (N = 68) (BMI ≥85th percentile).
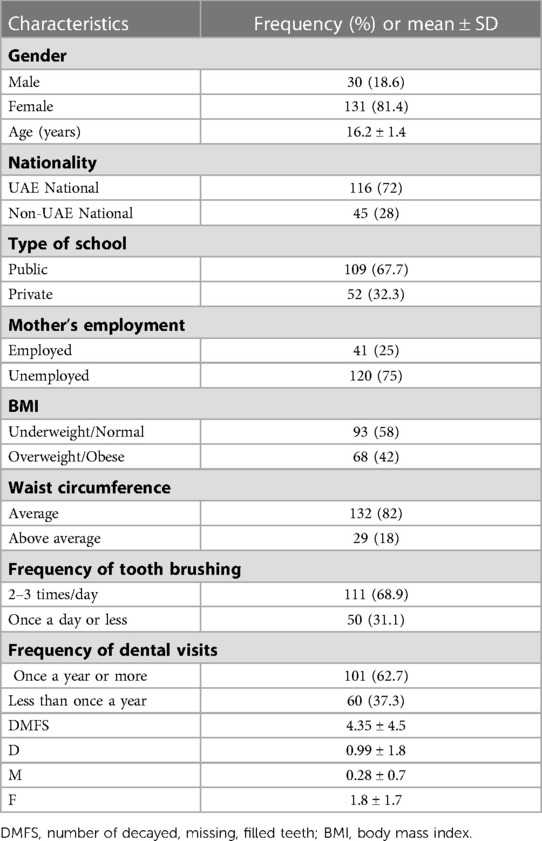
Table 1. Characteristics of participating adolescents (n = 161).
Table 2 shows the associations between sociodemographic factors, school, and obesity-related indices by DMFS total and separate component scores. UAE nationals had significantly higher DMFS scores and higher D scores compared to non-nationals (p < 0.05). In addition, children who attended private schools had significantly lower DMFS scores compared to children in public schools ((mean DMFS: 1.38 (SD: 1.9) and 5.2 (SD: 4.7), respectively)). Frequency of teeth brushing, visits to the dentist and BMI were not associated with dental caries activities.
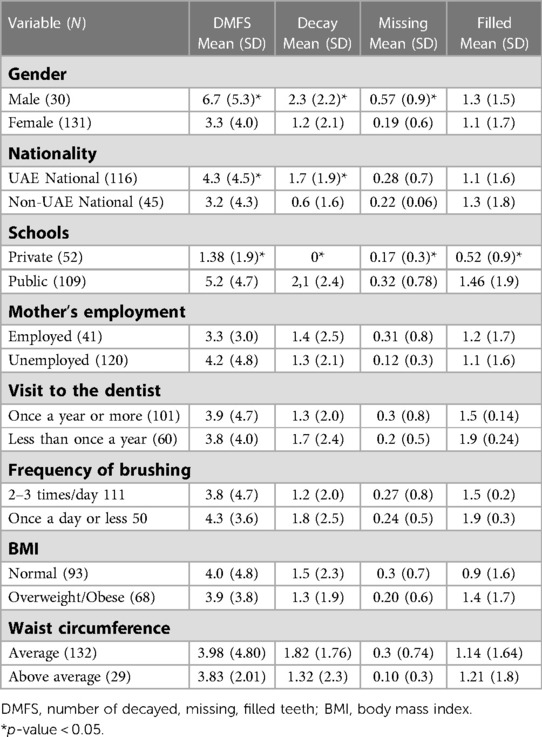
Table 2. DMFS scores according to factors considered in the study (n = 161).
The results of the multiple linear regression (Table 3) show that females had significantly lower DMFS scores compared to males (B = −2.71, 95% CI: −4.50, −0.91). Having above average waist circumference was also associated with significantly lower DMFS scores (B = −2.11, 95%CI: −4.05,0.0). Higher plaque index was associated with significantly higher DMFS scores (B = 3.02, 95% CI: 0.85, 5.2). In the regression model, BMI was not associated with DMFS scores.
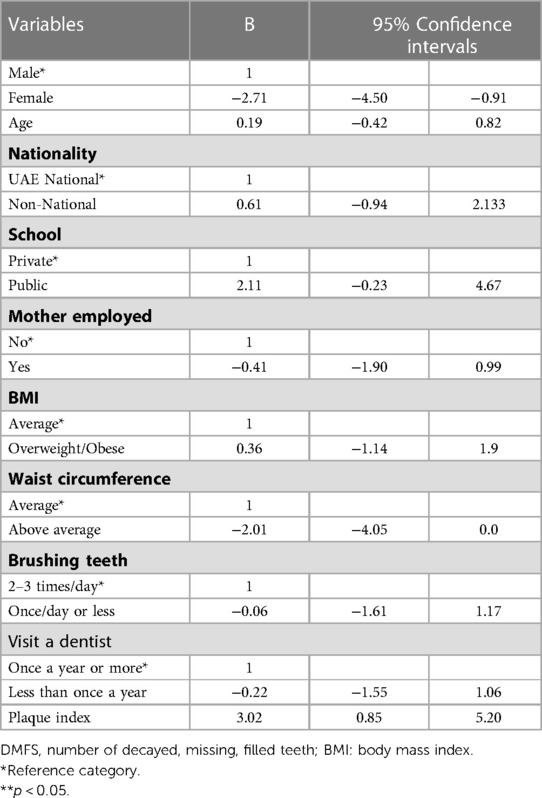
Table 3. Linear regression analysis for the association between DMFS and oral health habits and BMI.
Discussion
The main objective of this study was to assess the association between obesity and dental caries among adolescents in the UAE. The chief finding of the present pilot study is that among adolescents, obesity measured by BMI was not associated with dental caries activities. To the contrary, our findings show that adolescents with above average waist circumference had significantly less tooth decay that those with average waist circumference. This relationship was persistent after adjusting for age, sex, type of school, mother’s employment status, oral health habits and plaque index. This significant association is in agreement with the findings reported by Yang et al. (20), in which data from their study among Chinese children suggested that overweight children had lower rates of tooth decay. Similar findings were also reported in the Philippines among 1951 children aged 11–13 years, in which, there was a significant association between dental caries and below average BMI (42). One possible explanation is that sedentary lifestyle and lack of exercise among adolescents are important contributors to obesity, since these two factors are not directly related to dental caries, an inverse relationship between obesity and dental caries is possible. Another explanation is that malnutrition can cause enamel hypoplasia, salivary glandular hypofunction, and salivary compositional changes which lead to the development of tooth decay (17).
To the contrary, findings from Norway (43), and Saudi Arabia (44) showed that above average waist circumference was significantly associated with increase in dental caries among adolescents. It has been suggested that waist circumference is a more accurate anthropometric measure of central adiposity and more sensitive than BMI. WC probably reflects visceral and subcutaneous fat and hence total fatness, while BMI does not distinguish between fat and fat–free masses. This may explain the significant association with dental caries (43, 44). Nevertheless, we used waist circumference to assess obesity and our findings support a negative association between above average waist circumference and dental caries.
Assessing the relationship between obesity and dental caries is challenging, because findings from our study, as well as previous studies (6–9, 12, 24, 26, 30, 43–45), raise several questions regarding our understanding of the association between obesity and dental caries. It is well known that dental caries is mainly caused by sugar consumption, while obesity is not specifically related to sugar consumption, but to the consumption of a diet that is high in fat and consumption of large portion sizes (24, 46). Accordingly, it is possible that obese adolescents maintain good oral hygiene reflected in lower caries activities, while also consuming energy-dense diets (24). Therefore, the lack of association between dental caries and obesity would be understandable. However, given our findings, as well as that of other researchers (6–9, 10, 23, 43), it appears that the association between body weight and dental caries is complex. Rather than assuming a causal pathway, the possibility that the two conditions share common risk factors, such as diet and socioeconomic status should not be ruled out (6, 10). Common risk factors make studies that addressed the association between obesity and dental caries relevant from a public health perspective, in the development of preventive measures that target both health problems in a cost-effective manner (47, 48).
Despite the lack of an association between frequency of tooth brushing and number of visits to the dentist with DMFS scores observed in this study, the positive significant association between plaque scores and dental caries suggests poor oral hygiene practices, leading to the retention of dental plaque, the increase in streptococcus mutans colonization and possible loss of enamel.
Interestingly, females in our study had significantly lower prevalence of tooth decay than males. Usually, females are expected to exhibit a higher caries rate due to earlier tooth eruption, and thus longer exposure to cariogenic processes (49). However, sex related behaviors also likely contribute to differences in caries. It is also possible that in some cultures boys often have more access to sweets and calorie rich foods than girls (6), along with girls’ desire to stay slim, could contribute to the reduction in consumption of sugar and consequently reflected in lower prevalence of tooth decay.
Overall, adolescents in this study had relatively high prevalence of dental caries compared to their counterparts from Norway (43), Egypt (50) and China (51). Protecting permanent teeth from tooth decay is critical to reduce negative psychological, health and well-being consequences. Therefore, oral and dental health education and promotion should be more comprehensively integrated into adolescents’ schools. Our findings confirm previous studies in the UAE (36, 51–53), that showed significantly higher DMFS scores among students in public schools. In this study participants from private schools did not have any decayed teeth, indicating that being in private schools maybe associated with better utilization of dental services and better oral hygiene practices. These findings call for necessary public health initiatives to reduce the relatively high incidence rate of dental caries that is repeatedly reported in public schools in the UAE.
Strengths and limitations
Our findings are the first to assess the association between obesity and dental caries among adolescents in the UAE. We also considered multivariate models that took into account the contribution of several factors in addressing this relationship. Our results highlight the complexity of the association and the need for longitudinal studies to confirm or contest the relationship between obesity and dental caries. However, our study has certain methodologic limitations, including that this is a pilot study, and a larger sample size is needed to establish the association between obesity and dental caries in this population. We also did not include specific information about socioeconomic status of the study participants. However, school type is indicative of parental economic status in the UAE (54). Because this is a cross-sectional study, we cannot assume causality between obesity and dental caries. In addition, sugar intake was not assessed in this study. The majority of participants were females, and with more representation from public than private schools. Future studies may apply the International Caries Detection and Assessment System (55) to have a more comprehensive assessment of dental caries status among adolescents.
Conclusions
To conclude, in the present study, waist circumference was significantly associated with dental caries. However, obesity and dental caries are both multifactorial; therefore, further research is needed to determine the direction and strength of the association. Our finding of the relatively high prevalence of dental caries among adolescents in the UAE underscores the importance of public health measures to increase oral health promotion efforts.
Finally, given the complexity of the association between obesity and dental caries, cohort studies are recommended to clarify the mechanisms of the association between BMI and dental caries.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author/s.
Ethics statement
Ethical approval to conduct this study was obtained from the Research Ethics Committee of the principal investigator’s institution, the UAE Ministry of Health and Prevention, and the UAE Ministry of Education. Parental consent was obtained for each student that agreed to participate in this study. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
WB, HR, RR, RF, NA, and MA: conceived the presented idea. WB, HR, MA: involved in conducting the statistical analyses. MA, WB, HR, RF: wrote the initial draft of the manuscript. MA WB, HR, RF MA: contributed to writing the initial results and provided critical review of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the University of Sharjah/Research Institute for Medical and Health Sciences/Health Promotion Research Group (Grant number 150310).
Acknowledgments
The authors would like to thank the Ministry of Education for facilitating the data collection process. Also, we would like to thank all schools’ personnel and students for their time and effort during the data collection process. Finally, we would like to acknowledge the effort of the research assistants in the data collection process.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization https://www.who.int/news-room/fact-sheets/detail/oral-health (Accessed March 2023)
2. Elamin A, Garemo M, Mulder A. Determinants of dental caries in children in the middle east and north Africa region: a systematic review based on literature published from 2000 to 2019. BMC Oral Health. (2021) 21:237. doi: 10.1186/s12903-021-01482-7
3. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and meta regression. J Dent Res. (2015) 94:650–8. doi: 10.1177/0022034515573272
4. Kastenbom L, Falsen A, Larsson P, Sunnegårdh-Grönberg K, Davidson T. Costs and health-related quality of life in relation to caries. BMC Oral Health. (2019) 19:187. doi: 10.1186/s12903-019-0874-6
5. Al-Ansari AA. Prevalence, severity, and secular trends of dental caries among various Saudi populations: a literature review. Saudi J Med Med Sci. (2014) 2:142. doi: 10.4103/1658-631X.142496
6. Uerlich MF, Baker SR, Day PF, Brown L, Vettore MV. Common determinants of dental caries and obesity in children: a multi-ethnic nested birth cohort study in the United Kingdom. Int J Environ Res Public Health. (2021) 18(23):12561. doi: 10.3390/ijerph182312561
7. Paisi M, Kay E, Bennett C, Kaimi I, Witton R, Nelder R, et al. Body mass index and dental caries in young people: a systematic review. BMC Pediatr. (2019) 19:122. doi: 10.1186/s12887-019-1511-x
8. Paglia L, Scaglioni S, Torchia V, De Cosmi V, Moretti M, Marzo G, et al. Familial and dietary risk factors in early childhood caries. Eur J Paediatr Dent. (2016) 17:93–9. doi: 10.1186/s12903-019-0874-6
9. Kim K, Han K, Yang S. Association between overweight, obesity and incidence of advanced dental caries in south Korean adults: a 10-year nationwide population-based observational study. PLoS One. (2020) 15(2):e0229572. doi: 10.1371/journal.pone.0229572
10. Silva MJ, Kilpatrick NM, Craig JM, Manton DJ, Leong P, Ho H, et al. A twin study of body mass index and dental caries in childhood . Sci Rep. (2020) 10:568. doi: 10.1038/s41598-020-57435-7
11. Ravaghi V, Rezaee A, Pallan M, Morris AJ. Childhood obesity and dental caries: an ecological investigation of the shape and moderators of the association. BMC Oral Health. (2020) 20:338. doi: 10.1186/s12903-020-01329-7
12. Chen D, Zhi Q, Zhou Y, Tao Y, Wu L, Lin H. Association between dental caries and BMI in children: a systematic review and meta-analysis. Caries Res. (2018) 52(3):230–45. doi: 10.1159/000484988
13. Gupta P, Gupta N, Singh HP. Prevalence of dental caries in relation to body mass index, daily sugar intake, and oral hygiene status in 12-year-old school children in mathura city: a pilot study. Int J Pediatr. (2014) 2014:921823. doi: 10.1155/2014/921823
14. Alswat K, Mohamed WS, Wahab MA, Aboelil AA. The association between body mass index and dental caries: cross-sectional study. J Clin Med Res. (2016) 8(2):147–52. doi: 10.14740/jocmr2433w
15. Vazquez-Nava F, Vazquez-Rodriguez EM, Saldivar-Gonzalez AH, Lin-Ochoa D, Martinez-Perales GM, Joffre-Velazquez VM. Association between obesity and dental caries in a group of preschool children in Mexico. J Public Health Dent. (2010) 70(2):124–30. doi: 10.1111/j.1752-7325.2009.00152.x
16. Lempert SM, Froberg K, Christensen LB, Kristensen PL, Heitmann BL. Association between body mass index and caries among children and adolescents. Community Dent Oral Epidemiol. (2014) 42:53–60. doi: 10.1111/cdoe.12055
17. Shi R, Lin C, Li S, Deng L, Lin Z, Xiu L. Obesity is negatively associated with dental caries among children and adolescents in huizhou: a cross-sectional study. BMC Oral Health. (2022) 22(1):76. doi: 10.1186/s12903-022-02105-5
18. Quadri MF, Hakami BM, Hezam AA, Hakami RY, Saadi FA, Ageeli LM, et al. Relation between dental caries and body mass index-for-age among schoolchildren of Jazan city, kingdom of Saudi Arabia. J Contemp Dent Pract. (2017) 18(4):277–82. doi: 10.5005/jp-journals-10024-2031
19. Farsi DJ, Elkhodary HM, Merdad LA, Farsi NM, Alaki SM, Alamoudi NM, et al. Prevalence of obesity in elementary school children and its association with dental caries. Saudi Med J. (2016) 37(12):1387–94. doi: 10.15537/smj.2016.12.15904
20. Yang F, Zhang Y, Yuan X, Yu J, Chen S, Chen Z, et al. Caries experience and its association with weight status among 8-year-old children in Qingdao, China. J Int Soc Prev Community Dent. (2015) 5(1):52–8. doi: 10.4103/2231-0762.151978
21. da Silva RA, Barreiros D, Oliveira S, da Silva LA, Nelson-Filho P, Küchler EC. Association between body mass index and caries experience in Brazilian children and adolescents. J Dent Child. (2016) 83(3):146–51.
22. Narksawat K, Boonthum A, Tonmukayakul U. Roles of parents in preventing dental caries in the primary dentition among preschool children in Thailand. Asia Pac J Public Health. (2011) 23(2):209–16. doi: 10.1177/1010539509340045
23. Alkarimi HA, Watt RG, Pikhart H, Sheiham A, Tsakos G. Dental caries and growth in school-age children. Pediatrics. (2014) 133(3):e616–23. doi: 10.1542/peds.2013-0846
24. Aoun E, Ballo L, Elhabony S, Arheiam A. Association between dental caries and obesity among Libyan schoolchildren during the armed conflict in Benghazi. BMC Oral Health. (2023) 23:44. doi: 10.1186/s12903-023-02728-2
25. Li LW, Wong HM, Peng SM, McGrath CP. Anthropometric measurements and dental caries in children: a systematic review of longitudinal studies. Adv Nutr. (2015) 6(1):52–63. doi: 10.3945/an.114.006395
26. Manohar N, Hayen A, Fahey P, Arora A. Obesity and dental caries in early childhood: a systematic review and meta-analyses. Obes. Rev. (2020) 21:e12960. doi: 10.1111/obr.12960
27. Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N. Body mass index and dental caries in children and adolescents: a systematic review of literature published 2004 to 2011. Syst Rev. (2012) 1:57. doi: 10.1186/2046-4053-1-57
28. Cheng1 Y-H, Liao Y, Chen D-Y, Wang Y, Wu Y. Prevalence of dental caries and its association with body mass index among school-age children in Shenzhen, China. BMC Oral Health. (2019) 19:270. doi: 10.1186/s12903-019-0950-y
29. Masood M, Masood Y, Newton T. Impact of national income and inequality on sugar and caries relationship. Caries Res. (2012) 46(6):581–8. doi: 10.1159/000342170
30. Jebeile H, Kelly AS, O'Malley G, Baur LA. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. (2022) 10(5):351–65. doi: 10.1016/S2213-8587(22)00047-X
31. Sabharwal A, Stellrecht E, Scannapieco FA. Associations between dental caries and systemic diseases: a scoping review. BMC Oral Health. (2021) 21(1):472. doi: 10.1186/s12903-021-01803-w
32. Junior CA R, Vettore MV, Rebelo Vieira JM, de Queiroz AP C, de Queiroz AC, Pereira JV, et al. The role of dental pain and psychosocial factors on the relationship between dental caries and oral health-related quality of life in children. BMC Oral Health. (2022) 22(1):340. doi: 10.1186/s12903-022-02372-2
33. Buttitta M, Iliescu C, Rousseau A, Guerrien A. Quality of life in overweight and obese children and adolescents: a literature review. Qual Life Res. (2014) 23(4):1117–39. doi: 10.1007/s11136-013-0568-5
34. Araujo DS, Marquezin M, Barbosa TS, Fonseca F, Fegadolli C, Castelo PM. Assessment of quality of life, anxiety, socio-economic factors and caries experience in Brazilian children with overweight and obesity. Int J Dent Hyg. (2017) 15(4):e156–62. doi: 10.1111/idh.12248
35. Baniissa W, Radwan H, Rossiter R, Fakhry R, Al-Yateem N, Al-Shujairi A, et al. Prevalence and determinants of overweight/obesity among school-aged adolescents in the United Arab Emirates: a cross-sectional study of private and public schools. BMJ Open. (2020) 10(12):1–11. doi: 10.1136/bmjopen-2020-038667
36. Al Anouti F, Abboud M, Papandreou D, Haidar S, Mahboub N, Rizk R. Oral health of children and adolescents in the United Arab Emirates: a systematic review of the past decade. Front Oral Health. (2021) 2:1–17. doi: 10.3389/froh.2021.744328
37. Khadri F, Gpoinath VK, Hector MP, Davenport ES. Evaluating the risk factors that link obesity and dental caries in 11–17-year-old school going children in the United Arab Emirates. Eur J Dent. (2018) 12(02):217–24. doi: 10.4103/ejd.ejd_29_18
38. World Health Organization. Waist circumference and waist–hip ratio: Report of a WHO Expert Consultation Geneva, 8–11 December 2008. Available at: https://apps.who.int/iris/bitstream/handle/10665/44583/9789241501491_eng.pdf?sequence=1 (Accessed 8August 2019).
39. de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Org. (2007) 85(9):660–7. doi: 10.2471/BLT.07.043497
40. Al-Hazzaa HM, Al-Sobayel HI, Musaiger AO. Convergent validity of the arab teens lifestyle study (ATLS) physical activity questionnaire. Int J Environ Res Public Health. (2011) 8(9):3810–20. doi: 10.3390/ijerph8093810
41. World Health Organization Oral Health Surveys: Basic Methods-5th Edition 2013. Available at: https://apps.who.int/iris/handle/10665/97035 (Accessed 18 January 2021)
42. Benzian H, Heinrich-Weltzien BMR, Hobdell M, Mulder J, van Palenstein Helderman W. Untreated severe dental decay: a neglected determinant of low body mass index in 12-year-old Filipino children. BMC Public Health. (2011) 11:558. doi: 10.1186/1471-2458-11-558
43. Stangvaltaite-Mouhat L, Furberg AS, Drachev SN, Trovik TA. Commosn social determinants of overeweight and obesity, and dental caries among adolescents in Northern Norway: a cross-sectional study from the tromso study fit futures cohort. BMC Oral Health. (2021) 21(53):1-12. doi: 10.1186/s12903-021-01406-5
44. Gudipaneni RK, Albilasi RM, Alrewili O, Alam M, Patil SR, Saeed F. Association of body mass Index and Waist circumference with dental caries and consequences of untreated dental caries among 12- to 14-year-old boys: a cross-sectional study. Int Dent J. (2021) 71:522–9. doi: 10.1016/j.identj.2021.01.009
45. Marya CM, Dhingra S, Panwar NK, Gupta A, Mohan A, Arora R. Study on relationship between the nutritional status and dental caries in 8–12 year old children in Udaipur city, India. Kathmandu Univ Med J (KUMJ). (2014) 12(45):26–31.25219990
46. Radwan H, Ballout RA, Hasan H, Lessan N, Karavetian M, Rizk R. The epidemiology and economic burden of obesity and related cardiometabolic disorders in the United Arab Emirates: a systematic review and qualitative synthesis. J Obes. (2018) 2018:2185942. doi: 10.1155/2018/2185942
47. Chi DL, Luu M, Chu F. A scoping review of epidemiologic risk factors for pediatric obesity: implications for future childhood obesity and dental caries prevention research. J Public Health Dent. (2017) 77(Suppl 1):S8–S31. doi: 10.1111/jphd.12221
48. Sheiham A, Watt RG. The common risk factor approach: a rational basis for promoting oral health. Community Dent Oral Epidemiol. (2000) 28:399–406. doi: 10.1034/j.1600-0528.2000.028006399.x
49. Ferraro M, Vieira AR. Explaining gender differences in caries: a multifactorial approach to a multifactorial disease. Int J Dent. (2010):649643. doi: 10.1155/2010/649643
50. Abbass MS, Mahmoud SA, El Moshy S, Rady D, AbuBakr N, Radwan IA, et al. The prevalence of dental caries among Egyptian children and adolescences and its association with age, socioeconomic status, dietary habits and other risk factors. A cross-sectional study. F1000Res. (2019) 8:8. doi: 10.12688/f1000research.17047.1
51. Yang Q, Xi Y, Liu H, Luo J, Ouyang Y, Sun M, et al. Free sugars intake among Chinese adolescents and its association with dental caries: a cross-sectional study. Nutrients. (2021) 13(3):765. doi: 10.3390/nu13030765
52. Hashim R, Williams SM, Thomson WM, Awad MA. Caries prevalence and intra-oral pattern among young children in ajman. Community Dent Health. (2010) 27(2):109–13.20648888
53. Al Junaibi A, Abdulle A, Sabri S, Hag-Ali M, Nagelkerke N. The prevalence and potential determinants of obesity among school children and adolescents in Abu Dhabi, United Arab Emirates. Int J Obes. (2013) 37(1):68–74. doi: 10.1038/ijo.2012.131
54. Marquez J, Lambert L, Ridge NY, Walker S. The PISA performance gap between national and expatriate students in the United Arab Emirates. J Res Int Educ. (2022) 21(1):22–45. doi: 10.1177/14752409221090440
Keywords: dental caries, obesity, BMI—body mass index, waist circumference, cross sectional study, adolescents
Citation: Awad M, Bani Issa W, Radwan H, Fakhry R, Al-Yateem N and Rossiter R (2023) Association between obesity and dental caries among adolescents in UAE: a pilot cross sectional study. Front. Oral. Health 4:1160428. doi: 10.3389/froh.2023.1160428
Received: 7 February 2023; Accepted: 15 May 2023;
Published: 27 June 2023.
Edited by:
Arheiam Arheiam, University of Benghazi, LibyaReviewed by:
Balgis Gaffar, Imam Abdulrahman Bin Faisal University, Saudi ArabiaEntesar Mohamed, Dental public health and preventive department, Libya
© 2023 Awad, Bani Issa, Radwan, Fakhry, Al-Yateem and Rossiter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manal Awad YXdhZEBzaGFyamFoLmFjLmFl