 Margherita Gobbo1
Margherita Gobbo1 Elisabetta Merigo2
Elisabetta Merigo2 Praveen R. Arany3
Praveen R. Arany3 René-Jean Bensadoun4
René-Jean Bensadoun4 Alan Roger Santos-Silva5
Alan Roger Santos-Silva5 Luiz Alcino Gueiros6
Luiz Alcino Gueiros6 Giulia Ottaviani7*
Giulia Ottaviani7*- 1Unit of Oral and Maxillofacial Surgery, Ca' Foncello Hospital, Treviso, Italy
- 2Faculty of Dentistry, Côte d'Azur University, Nice, France
- 3Oral Biology, Surgery and Biomedical Engineering, University at Buffalo, Getzville, NY, United States
- 4Department of Radiation Oncology, Centre de Haute Energie, Nice, France
- 5Oral Diagnosis Department, Piracicaba Dental School, University of Campinas, São Paulo, Brazil
- 6Department of Clinic and Preventive Dentistry, Federal University of Pernambuco, Recife, Brazil
- 7Department of Surgical, Medical and Health Sciences, University of Trieste, Trieste, Italy
Background: Radiotherapy and chemotherapy are frequently employed in head and neck cancer (HNC) patients causing significant side effects that impair life quality and prognosis. Photobiomodulation (PBM) has become a growing approach to managing such oral complications. Despite its proven efficacy and absence of contraindications, there is still a lack of universally accepted disease-specific PBM protocols.
Objective: A narrative review was conducted to identify the current proposals relating to the use of PBM to treat complications of oncological treatments in HNC patients.
Methods: An electronic search in PubMed and Scopus databases was performed with the following keywords: (“photobiomodulation” OR “PBM” OR “laser therapy” OR “LLLT” OR “laser”) AND (“head and neck cancer” OR “oral cancer”) AND (“mucositis” OR “oral mucositis” OR “dysgeusia” OR “oedema” OR “xerostomia” OR “dermatitis” OR “trismus”) until October 2021.
Results: A total of 35 papers were included in the narrative review. Oral mucositis was the most studied complication, and advisable protocols are conceivable. Although there is a growing interest in PBM to manage of xerostomia, radiodermatitis, pain, and trismus, literature is still scarce to propose a universally feasible protocol.
Conclusions: PBM therapy could significantly prevent or reduce the severity of many side effects related to cancer therapies. More research is needed to obtain recommendations over the preferable parameters.
Introduction
Head and neck cancer (HNC) is primarily treated with surgery in combination with radiotherapy (RT) and/or chemotherapy (CT). RT and/or CT in the head and neck region (HNR) have several side effects that can be debilitating and heavily affect patients' quality of life (QoL) and prognosis. The most common side effects include oral mucositis (OM), xerostomia, dysgeusia, oedema, radiation caries, radiodermatitis, and trismus [1]. These spectra of ailments share a common etiopathology of these complications involving sensitization and tissue damage by the oncotherapy agent. Photobiomodulation (PBM) is a non-invasive light therapy increasingly being applied in supportive care for cancer patients. Its main properties cover the field of wound healing and inflammation. However, there is still no clear consensus over the standard protocols and devices to employ. Recent insights have been made about molecular mechanisms, biological responses, and biomarkers for safe and effective PBM treatments [2, 3]. Concurrently, there have been significant advancements with device technologies, increasing availability of wavelengths, and precise control of the beam and output parameters [4]. Therefore, the objective of the present paper was to produce a narrative review of the available scientific evidence to identify the current proposals and related protocols of PBM to manage the most prevalent complications of oncological treatments in the HNR.
Methods
An electronic search in the PubMed and Scopus databases was conducted with the following keywords: (“photobiomodulation” OR “PBM” OR “laser therapy” OR “LLLT” OR “laser”) AND (“head and neck cancer” OR “oral cancer”) AND (“mucositis” OR “oral mucositis” OR “dysgeusia” OR “oedema” OR “xerostomia” OR “dermatitis” OR trismus) until October 2021. Papers in languages different from English, Italian, Spanish, Portuguese, and French were excluded. Only original articles and reviews were initially included, excluding short reports and case reports. Further, articles not specifying laser protocol were also excluded. A global group of experts in oral medicine, oncology, radiation biology, and PBM examined and discussed this literature to further develop consensus.
Results
A total of 148 studies were obtained after the electronic search. Two different reviewers read all abstracts. After the abstract screening, 58 were excluded, and 90 were subdivided among reviewers' full-text analyses performed independently by two reviewers. After the full-text screening, 35 papers were included in the narrative review. The majority of papers were about preventing or treating more than one side-effect. Twenty-seven studies dealt with OM, 10 with xerostomia, 4 with radiodermatitis, and 2 with pain and trismus. Other interesting topics included the evaluation of QoL outcomes, systemic analgesia, functional impairment, nutritional status, survival, interruption of RT, adherence, cost-effectiveness, safety, feasibility, and tolerability of PBM. In general, no adverse effects were reported, and all authors supported safety and tolerability. Although clinical time constraints and patient compliance were often considered limitations to PBM therapy, feasibility was high. Further detailed analysis of these results will be conducted in another review by our group. In the phase of full-text screening, reviews and systematic reviews were excluded as they did not mention detailed laser parameters.
Study Characteristics
Overall, 7 papers were published between 1999 and 2010, 19 papers between 2011 and 2019, and 9 papers in the last 2 years, witnessing the increasing interest in the field of PBM applied to supportive care in cancer patients (Table 1). A total of 14 studies investigated the role of PBM in preventing the onset of the side effect, 13 in treating the complications, and 8 studies mentioned both protocols. Twenty-two studies included HNC patients subjected to RT sessions alone or combined with surgery, whereas 13 studies included HNC patients subdued to combined CT and RT, with exclusive regimens or as adjuvants to surgical treatments.
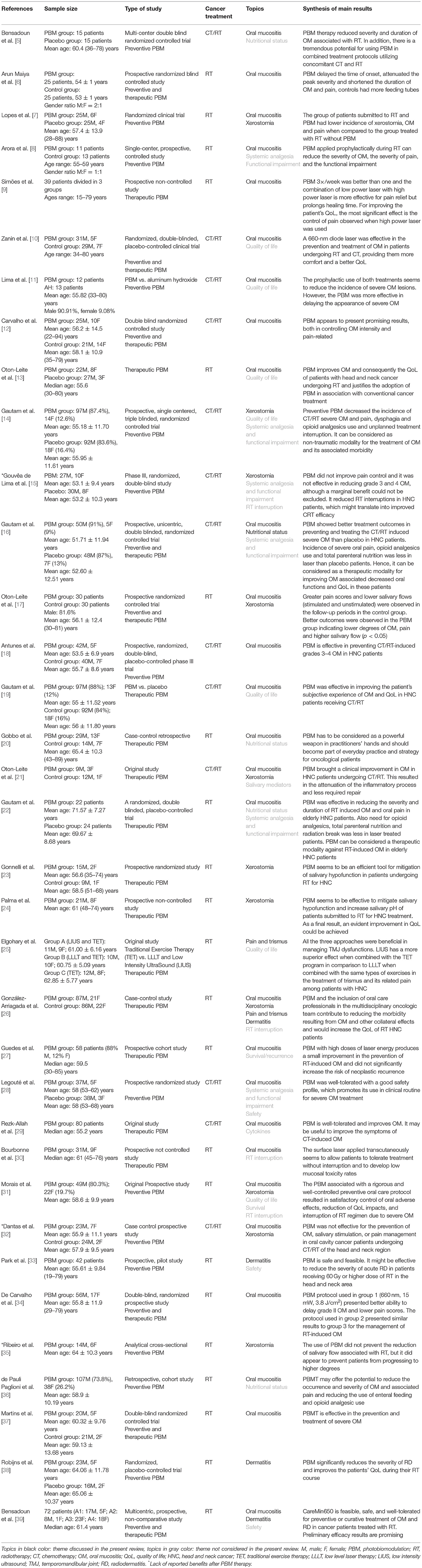
Table 1. Characteristics of studies included in the narrative review.
Light Parameters
Detailed characteristics of PBM protocols in included studies are outlined in Table 2. We noted considerable variations in the types of used lasers, mode of application, frequency of treatment, and treatment parameters. Our analysis precludes robust clinical guidelines. Nonetheless, an overview of the most relevant protocols for each category is outlined to assist clinical implementation.
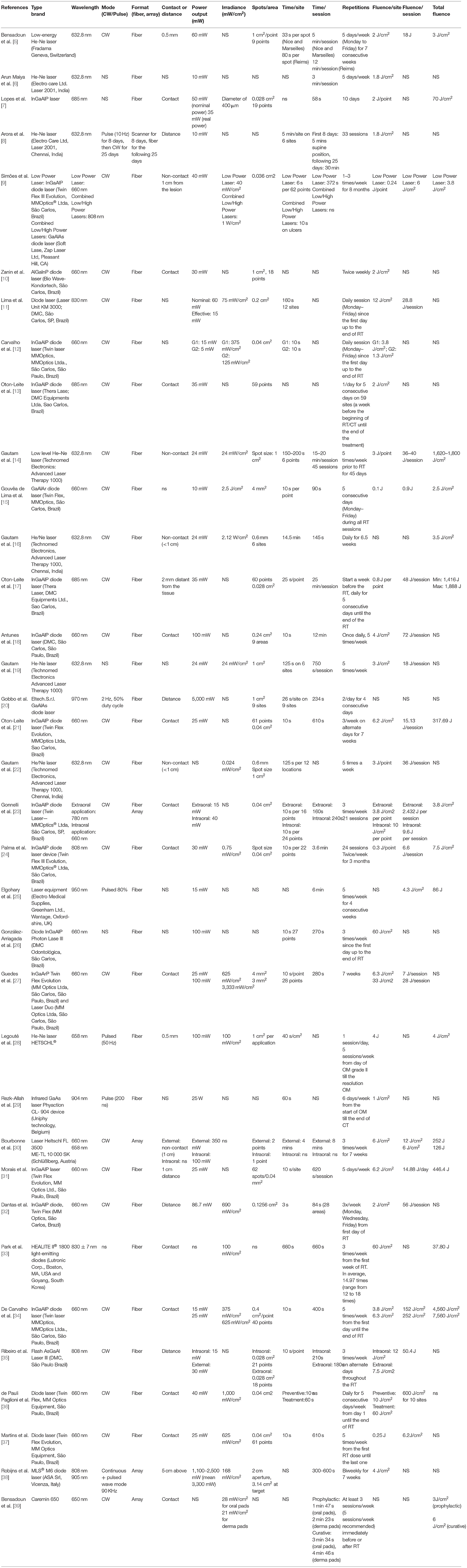
Table 2. Laser parameters of the studies included in the narrative review.
PBM for Oral Mucositis
The results for OM management were consistent, and guidelines for both prevention and treatment could be outlined in the current narrative review (Supplementary Table 1). All Authors choose diode lasers, more often indium gallium aluminum phosphide (InGaAlP) diode laser, and Helium-Neon (He/Ne) laser. The most preferred wavelength was red (632–660 nm) for both prevention and treatment protocols in continuous wave (CW) mode using fiber in contact or reduced (<1 cm) distance. Power output reported varied (5–5,000 mW), but most papers did not discriminate between nominal and effective, resulting in overestimated values, especially in non-contact protocols. A suggestion could be between 10 and 100 mW effective power. While some Authors mention irradiance per treatment point, others suggest a defocused beam ranging between 0.024 and 150 mW/cm2. As per the new PBM dosing, the most effective preventive protocol would use a total dose of 1.2 Einstein (photon fluence at 650 nm = 5.7 p.J/cm2). The data suggests successive intraoral applications on single spots on the oral cavity, rather than a scanning motion over the entire mucosal surface, may offer the most predictable outcomes. Also, the time of application was very variable, ranging from sessions of 270 s to 25 min. A minimum of 30 s per point with three (up to 5) sessions a week is recommended in preventive and treatment protocols. Overall, preventive protocols need more repetitions per week than treatment protocols.
PBM for Xerostomia
All authors employed diode lasers, specifically indium gallium aluminum phosphide (InGaAlP) or Gallium Aluminum Arsenide (GaAlAs), preferring low power protocols (Supplementary Table 2). Both visible red (650–660 nm) and infrared (780–808 nm) wavelengths were used in CW mode. In two cases, the application was both intraoral and extraoral. Output power varied consistently, ranging from 10 to 100 mW for intraoral to 15–30 mW for extraoral applications. Also, time per site reported significantly gone from 3 to 400 s. Fluence went between 2 and 60 J/cm2, equating to 3.8–114 p.J/cm2 (photon fluence at 650 nm) or 0.8–25 Einstein. Sessions should be repeated at least twice a week but would be best effective if performed each day of RT (5-day per week), both in preventive and therapeutic protocols.
PBM for Radiodermatitis
Among the four papers dealing with PBM for dermatitis management, two proposed a red wavelength, while the other used infrared (Supplementary Table 3). All Authors employed very heterogeneous diode devices (e.g., He/Ne, InGaAlP). Only Robjins et al. studied dermatitis specifically, while other authors did not distinguish between prevention or treatment of specific side effects [38]. Outputs varied between 100 and 2,500 mW and irradiance between 100 and 168 mW/cm2 when mentioned. The fluence varied between 2 and 60 J/cm2, equating to 3.8 to 114 p.J/cm2 (photon fluence at 650 nm) or 0.8 to 25 Einstein. Treatment time per session varied from 270 to 720 s while repetitions varied between 2 and 5 times a week for the whole course of RT. Although the publications on this topic are scarce and heterogeneous, there is a feeling toward the appropriateness of 2 or 3-weekly applications instead of daily sessions, preferring a preventive or combined strategy rather than just using PBM in a curative way. DeLand et al. reported that LED treatments immediately after RT reduces dermatitis incidence in breast cancer patients. These findings may inspire a protocol for HNC subjects. Despite the variability of the parameters, a general recommendation can be hypothesized [40].
PBM for Pain and Trismus
PBM treatments for the management of pain and trismus induced by RT were assessed by two papers (Supplementary Table 4) [26]. While both protocols were focused on treatment, and the parameters were too heterogeneous for comparison, such as wavelength (660 red vs. 950 infrared), output powers (100 vs. 15 mW), and fluences (60 vs. 7.6 J/cm2 per session). Further, Elgohary et al. compared various techniques, including PBM, that were not the study's primary objective [25]. Based on our clinical experience, we recommend using a combination of 660 and 810 nm PBM devices, both intraoral and extraoral, at 50 mW/cm2 for 30 s per site, treating multiple areas in a scanning motion for a total fluence of 6 J/cm2 which equates to 9 p.J/cm2 at 810 nm or 2 Einstein. Treatments should be repeated up to 3 times per week for at least 3–4 weeks.
Discussion
The present review offers an overview of the literature on PBM therapy in HNC patients with RT-related side effects, specifically OM, xerostomia, dermatitis, pain, and trismus. The most studied side effect of cancer treatments remains OM [41]. Literature has increased substantially, outlining preventive, therapeutic, or combined protocols [42]. The results section of our literature review has provided reliable suggestions for creating an effective protocol. PBM biological responses depend on the treatment parameters, delivery protocols, and redox state of the cells. It is well-established that PBM dosing is biphasic and relies on the underlying pathology and patient-associated factors that may affect individual outcomes. Further, inappropriate dosing may result in poor or adverse therapeutic effects. The PBM dose window is defined by correct treatment timing, the number of repetitions, and specific adaptation of protocols for each indication [43].
In general, PBM was noted to be effective in both the prevention and treatment of OM [27, 32]. It is almost universally accepted that the primary goal of treatment is reducing pain and improving QoL; most studies confirmed this regardless of the protocol. Even the low PBM efficacy papers noted reduced severity of OM grades (scores 3 and 4 according to the World Health Organization scale) and fewer treatment interruptions during RT. Most of the papers included in our systematic review used CW protocols. This contrasts with prior reports that pulsed, low-frequency (<100 Hz) may be superior for wound healing or the damage prevention. Moreover, while most studies used intraoral PBM treatments, there is evidence for extra-orally administered PBM that appears to be more effective for managing of OM of the buccal mucosa, vestibule, and inner lips when combined with an intraoral approach [44, 45].
The PBM studies on salivary glands after RT employed combined external and intraoral applications with both infrared and visible red wavelengths [17, 23]. There appears to be a dose-effect relationship for PBM on reduction of hyposalivation after RT, especially after 15 sessions with red or combined red and infra-red wavelengths [46]. For example, Ribeiro et al. conducted a cross-sectional study with a quantitative approach applying extraoral infrared PBM during the whole course of RT. They demonstrated unchanged unstimulated salivary flow during RT but decreased saliva quantity 1 month after the end of cancer treatment. Despite not corroborating the role of PBM in modulating hyposalivation and salivary gland damage, a concomitant intraoral, lower dose protocol was used for OM that was not the main objective of the study confounding the interpretations of their results [35]. Interestingly, the control of hyposalivation induced by RT seems to be positively affected by PBM treatment strategies [47]. On the contrary, the effect was not marked in preventive protocols. Three studies did not evidence a beneficial impact of PBM in reducing salivary flow connected to RT or combined CT/RT [15, 32, 35]. Note that only one of them is a randomized clinical trial and they all include a limited number of subjects. Moreover, there was no specific protocol for salivary complications that can be distinguished from other side effects, such as OM.
All the publications included in this narrative review suggest that PBM is a safe and valuable strategy for cutaneous complications in the HNR. Encouraging results were noted for PBM management or prevention of radiodermatitis. Many papers have been published regarding radiodermatitis in other body districts, breast in primis. However, little has been investigated in the cervical and facial sites, although it is associated with significant pain, disfigurement, risk of RT interruption, and poor cancer prognosis [38]. For cutaneous areas other than the HNR, the literature suggests that preventive PBM application, starting concomitantly or even before RT or combined CT/RT, may not only mitigate the severity of dermatitis but also positively impact the onset and severity of late complications, via the mechanisms of tissue repair and regeneration. For example, a study on pigs suggested that combined wavelengths positively influence the development of late radiation damage to the skin. This indicates that this approach may also be applied in the HNR [48]. The fact that all the included publications were very recent (2018–2022) indicates increased interest and recognition of the efficacy of this treatment, together with its proven safety, suggesting that a universal protocol may be feasible shortly.
Specific interest has emerged in this review in trismus management, which is not corroborated by previous literature work. HNC patients are often subdued to destructive surgery, which provokes muscle spasms and reduced mouth opening. The evidence that PBM reduces fibrosis and promotes muscle regeneration could be the primary rationale for the clinical benefit looked for by the Authors, even if it is evident that this topic needs further clinical research [45].
In summary, the available evidence shows that PBM was satisfactory in managing complications related to cancer therapies, both in the prevention of onset and in the reduction of severity and duration, especially for OM. Objective and subjective parameters were studied with comparable rates of success, and the favorable implications on QoL outcomes and wellbeing accounted for most of the positive results expressed by the authors [37]. PBM generates beneficial effects, including reducing of inflammation and pain [49], promoting tissue repair, reducing fibrosis, and favoring nerve regeneration. Therefore, it is clear why studies on PBM application cover a vast range of acute and chronic cancer-related complications in HNC patients.
Moreover, there is growing evidence that PBM is cost-effective both in preventing and treating cancer treatment-related toxicities, such as OM and breast cancer-related lymphedema. This scenario may provide a wider acceptance of PBM at cancer treatment centers, especially if fomented by additional clinical studies to validate cost-effectiveness for preventing and managing cancer treatment-related toxicities other than OM [50].
PBM dosimetry has raised significant interest in recent years, primarily due to its efficacy in a broad range of clinical applications, regardless of the underlying pathology and varying protocols. But since Mester's first description of its benefits, PBM has been used rather empirically as a magic wand, without actual knowledge of photobiological, molecular, and intercellular mechanisms of laser-tissue interaction that cannot be ignored [51]. The absence of clear guides for standardizing protocols description and data presentation remains an issue that can limit comparison among studies and the creation of coherent clinical practice guidelines. Inconsistencies in clinical outcomes are mainly due to problems in reporting PBM dosing and delivery. For the latter, using “treatment surface irradiance” rather than laser irradiance alone is expected to reduce confusion about power output, spot size, and distance, especially when using contact and defocused (distant) PBM treatments [24]. This should assist in significantly improving dose reproducibility. The availability of large arrays has encouraged defocused, large treatment areas that reduce treatment time and thermal damage in tissues. Eventually, disease-focused protocols could be created as specific wavelengths target biological chromophores at varying penetration depths and evoke discrete biological responses. Universal protocols may seem convenient and somewhat effective, they are likely to generate inconsistent or irreproducible results [52].
Even in the case of different protocols applied to the same condition, the evoked PBM responses may vary. The absorption of light by a chromophore depends on the affinity with the used wavelength. Even if the wavelength falls within the correct absorption spectrum, low doses of energy are insufficient to start the biological effect, and excessive dosages can result in inhibitory. Moreover, therapeutic responses are restricted to a limited therapeutic dose window termed the Arndt Schultz curve [53]. Recent papers emerged in the literature regarding the possibility of enabling comparisons between protocols, creating a system of “dosing consistency,” which is effective with multiple combined wavelengths. Young et al. suggested using the terms photonic fluence (p.J/cm2) and “Einstein” (photonic fluence at 810 nm as a reference wavelength) [51]. This enables easy, universal interoperability between dose recommendations with different wavelengths. This novel dose system has been recently applied to the dosing recommendations by the World Association for Photobiomodulation Therapy (WALT) to increase practical implementation irrespective of individual wavelengths or devices that are available globally while preventing overdosing and enabling dose combination with various wavelengths [51].
The similarities of the pathophysiology in different complications and the fact that the same patients may suffer from more than one side effect represent a clear clinical challenge. Moreover, based on the logical extension of acute complications as precursors for chronic ones, preventive (“pre-conditioning”) PBM protocols could effectively reduce early and late complications [54]. PBM should be applied using the optimal parameters based on the biological target, device parameters, and delivery technique. Therefore, it is rational to posit that optimal protocols could maximize clinical efficacy, creating a reproducible, and consistent treatment irrespective of the device being used. This work attempts to outlining some of these parameters to pave the way for universal PBM protocols.
Conclusion
PBM seems to be an efficacious intervention for several complications of cancer therapy. Robust evidence of the clinical benefit elicited by the correct biological and molecular patterns of light stimulation exists. There is a strong perception that multiple protocols may be applied to similar conditions but to maximize the effect on specific tissue targets, there is an urgent need for standardization and reproducibility of dosages. The increasing number of papers regarding the management of HNC complications via PBM witnesses a strong interest in the field. The very recent publications proposing dosage standardization indicate we are moving in the right direction.
Author Contributions
GO and MG contributed to conception and design of the study. MG, EM, PA, R-JB, AS-S, LG, and GO performed the articles screening and data collection. MG wrote the first draft of the manuscript. EM, PA, R-JB, AS-S, LG, and GO wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
The authors gratefully acknowledge the support of Eltech K-Laser Company for the publication financial support. Eltech K-Laser Company was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2022.945718/full#supplementary-material
References
1. Brook I. Early side effects of radiation treatment for head and neck cancer. Cancer Radiother. (2021) 25:507–13. doi: 10.1016/j.canrad.2021.02.001
2. Khan I, Tang E, Arany P. Molecular pathway of near-infrared laser phototoxicity involves ATF-4 orchestrated ER stress. Sci Rep. (2015) 5:10581. doi: 10.1038/srep10581
3. Arany PR. Craniofacial wound healing with photobiomodulation therapy: new insights and current challenges. J Dent Res. (2016) 95:977–84. doi: 10.1177/0022034516648939
4. Worthington HV, Clarkson JE, Bryan G, Furness S, Glenny AM, Littlewood A, et al. Interventions for preventing oral mucositis for patients with cancer receiving treatment. Cochrane Database Syst Rev. (2011) 2011:CD000978. doi: 10.1002/14651858.CD000978.pub4
5. Bensadoun RJ, Franquin JC, Ciais G, Darcourt V, Schubert MM, Viot M, et al. Low-energy He/Ne laser in the prevention of radiation-induced mucositis. A multicenter phase III randomized study in patients with head and neck cancer. Support Care Cancer. (1999) 7:244–52. doi: 10.1007/s005200050256
6. Arun Maiya G, Sagar MS, Fernandes D. Effect of low level helium-neon (He-Ne) laser therapy in the prevention & treatment of radiation induced mucositis in head & neck cancer patients. Indian J Med Res. (2006) 124:399–402.
7. Lopes CO, Mas JR, Zangaro RA. Low level laser therapy in the prevention of radiotherapy-induced xerostomia and oral mucositis. Radiol Bras. (2006) 39:131–6. doi: 10.1590/S0100-39842006000200012
8. Arora H, Pai KM, Maiya A, Vidyasagar MS, Rajeev A. Efficacy of He-Ne Laser in the prevention and treatment of radiotherapy-induced oral mucositis in oral cancer patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2008) 105:180–6.e1. doi: 10.1016/j.tripleo.2007.07.043
9. Simões A, Eduardo FP, Luiz AC, Campos L, Sá PH, Cristófaro M, et al. Laser phototherapy as topical prophylaxis against head and neck cancer radiotherapy-induced oral mucositis: comparison between low and high/low power lasers. Lasers Surg Med. (2009) 41:264–70. doi: 10.1002/lsm.20758
10. Zanin T, Zanin F, Carvalhosa AA, Castro PH, Pacheco MT, Zanin IC, et al. Use of 660-nm diode laser in the prevention and treatment of human oral mucositis induced by radiotherapy and chemotherapy. Photomed Laser Surg. (2010) 28:233–7. doi: 10.1089/pho.2008.2242
11. Lima AG, Antequera R, Peres MP, Snitcosky IM, Federico MH, Villar RC. Efficacy of low-level laser therapy and aluminum hydroxide in patients with chemotherapy and radiotherapy-induced oral mucositis. Braz Dent J. (2010) 21:186–92. doi: 10.1590/S0103-64402010000300002
12. Carvalho PA, Jaguar GC, Pellizzon AC, Prado JD, Lopes RN, Alves FA. Evaluation of low-level laser therapy in the prevention and treatment of radiation-induced mucositis: a double-blind randomized study in head and neck cancer patients. Oral Oncol. (2011) 47:1176–81. doi: 10.1016/j.oraloncology.2011.08.021
13. Oton-Leite AF, Corrêa de Castro AC, Morais MO, Pinezi JC, Leles CR, Mendonça EF. Effect of intraoral low-level laser therapy on quality of life of patients with head and neck cancer undergoing radiotherapy. Head Neck. (2012) 34:398–404. doi: 10.1002/hed.21737
14. Gautam AP, Fernandes DJ, Vidyasagar MS, Maiya AG, Vadhiraja BM. Low level laser therapy for concurrent chemoradiotherapy induced oral mucositis in head and neck cancer patients - a triple blinded randomized controlled trial. Radiother Oncol. (2012) 104:349–54. doi: 10.1016/j.radonc.2012.06.011
15. Gouvêa de Lima A, Villar RC, de Castro G Jr, Antequera R, Gil E, Rosalmeida MC, et al. Oral mucositis prevention by low-level laser therapy in head-and-neck cancer patients undergoing concurrent chemoradiotherapy: a phase III randomized study. Int J Radiat Oncol Biol Phys. (2012) 82:270–5. doi: 10.1016/j.ijrobp.2010.10.012
16. Gautam AP, Fernandes DJ, Vidyasagar MS, Maiya GA. Low level helium neon laser therapy for chemoradiotherapy induced oral mucositis in oral cancer patients - a randomized controlled trial. Oral Oncol. (2012) 48:893–7. doi: 10.1016/j.oraloncology.2012.03.008
17. Oton-Leite AF, Elias LS, Morais MO, Pinezi JC, Leles CR, Silva MA, et al. Effect of low level laser therapy in the reduction of oral complications in patients with cancer of the head and neck submitted to radiotherapy. Spec Care Dentist. (2013) 33:294–300. doi: 10.1111/j.1754-4505.2012.00303.x
18. Antunes HS, Herchenhorn D, Small IA, Araújo CM, Viégas CM, Cabral E, et al. Phase III trial of low-level laser therapy to prevent oral mucositis in head and neck cancer patients treated with concurrent chemoradiation. Radiother Oncol. (2013) 109:297–302. doi: 10.1016/j.radonc.2013.08.010
19. Gautam AP, Fernandes DJ, Vidyasagar MS, Maiya AG, Nigudgi S. Effect of low-level laser therapy on patient reported measures of oral mucositis and quality of life in head and neck cancer patients receiving chemoradiotherapy–a randomized controlled trial. Support Care Cancer. (2013) 21:1421–8. doi: 10.1007/s00520-012-1684-4
20. Gobbo M, Ottaviani G, Perinetti G, Ciriello F, Beorchia A, Giacca M, et al. Evaluation of nutritional status in head and neck radio-treated patients affected by oral mucositis: efficacy of class IV laser therapy. Support Care Cancer. (2014) 22:1851–6. doi: 10.1007/s00520-014-2155-x
21. Oton-Leite AF, Silva GB, Morais MO, Silva TA, Leles CR, Valadares MC, et al. Effect of low-level laser therapy on chemoradiotherapy-induced oral mucositis and salivary inflammatory mediators in head and neck cancer patients. Lasers Surg Med. (2015) 47:296–305. doi: 10.1002/lsm.22349
22. Gautam AP, Fernandes DJ, Vidyasagar MS, Maiya AG, Guddattu V. Low level laser therapy against radiation induced oral mucositis in elderly head and neck cancer patients-a randomized placebo controlled trial. J Photochem Photobiol B. (2015) 144:51–6. doi: 10.1016/j.jphotobiol.2015.01.011
23. Gonnelli FA, Palma LF, Giordani AJ, Deboni AL, Dias RS, Segreto RA, et al. Low-Level laser for mitigation of low salivary flow rate in head and neck cancer patients undergoing radiochemotherapy: a prospective longitudinal study. Photomed Laser Surg. (2016) 34:326–30. doi: 10.1089/pho.2016.4104
24. Palma LF, Gonnelli FAS, Marcucci M, Dias RS, Giordani AJ, Segreto RA, et al. Impact of low-level laser therapy on hyposalivation, salivary pH, and quality of life in head and neck cancer patients post-radiotherapy. Lasers Med Sci. (2017) 32:827–32. doi: 10.1007/s10103-017-2180-3
25. Elgohary HM, Eladl HM, Soliman AH, Soliman ES. Effects of ultrasound, laser and exercises on temporomandibular joint pain and trismus following head and neck cancer. Ann Rehabil Med. (2018) 42:846–53. doi: 10.5535/arm.2018.42.6.846
26. González-Arriagada WA, Ramos LMA, Andrade MAC, Lopes MA. Efficacy of low-level laser therapy as an auxiliary tool for management of acute side effects of head and neck radiotherapy. J Cosmet Laser Ther. (2018) 20:117–22. doi: 10.1080/14764172.2017.1376097
27. Guedes CDCFV, de Freitas Filho SAJ, de Faria PR, Loyola AM, Sabino-Silva R, Cardoso SV. Variation of energy in photobiomodulation for the control of radiotherapy-induced oral mucositis: a clinical study in head and neck cancer patients. Int J Dent. (2018) 2018:4579279. doi: 10.1155/2018/4579279
28. Legouté F, Bensadoun RJ, Seegers V, Pointreau Y, Caron D, Lang P, et al. Low-level laser therapy in treatment of chemoradiotherapy-induced mucositis in head and neck cancer: results of a randomised, triple blind, multicentre phase III trial. Radiat Oncol. (2019) 14:83. doi: 10.1186/s13014-019-1292-2
29. Rezk-Allah SS, Abd Elshaf HM, Farid RJ, Hassan MAE, Alsirafy SA. Effect of low-level laser therapy in treatment of chemotherapy induced oral mucositis. J Lasers Med Sci. (2019) 10:125–30. doi: 10.15171/jlms.2019.20
30. Bourbonne V, Otz J, Bensadoun RJ, Dissaux G, Lucia F, Leclere JC, et al. Radiotherapy mucositis in head and neck cancer: prevention by low-energy surface laser. BMJ Support Palliat Care. (2019). doi: 10.1136/bmjspcare-2019-001851
31. Morais MO, Martins AFL, de Jesus APG, de Sousa Neto SS, da Costa AWF, Pereira CH, et al. A prospective study on oral adverse effects in head and neck cancer patients submitted to a preventive oral care protocol. Support Care Cancer. (2020) 28:4263–73. doi: 10.1007/s00520-019-05283-1
32. Dantas JBL, Martins GB, Lima HR, Carrera M, Reis SRA, Medrado ARAP. Evaluation of preventive laser photobiomodulation in patients with head and neck cancer undergoing radiochemotherapy: laser in patients with head and neck cancer. Spec Care Dentist. (2020) 40:364–73. doi: 10.1111/scd.12486
33. Park JH, Byun HJ, Lee JH, Kim H, Noh JM, Kim CR, et al. Feasibility of photobiomodulation therapy for the prevention of radiodermatitis: a single-institution pilot study. Lasers Med Sci. (2020) 35:1119–27. doi: 10.1007/s10103-019-02930-1
34. de Carvalho PAG, Lessa RC, Carraro DM, Assis Pellizzon AC, Jaguar GC, Alves FA. Three photobiomodulation protocols in the prevention/treatment of radiotherapy-induced oral mucositis. Photodiagnosis Photodyn Ther. (2020) 31:101906. doi: 10.1016/j.pdpdt.2020.101906
35. Ribeiro LN, Lima MH, Carvalho AT, Albuquerque RF, Leão JC, Silva IH. Evaluation of the salivary function of patients in treatment with radiotherapy for head and neck cancer submitted to photobiomodulation. Med Oral Patol Oral Cir Bucal. (2021) 26:e14–20. doi: 10.4317/medoral.23912
36. de Pauli Paglioni M, Faria KM, Palmier NR, Prado-Ribeiro AC, E Dias RB, da Graça Pinto H, et al. Patterns of oral mucositis in advanced oral squamous cell carcinoma patients managed with prophylactic photobiomodulation therapy-insights for future protocol development. Lasers Med Sci. (2021) 36:429–36. doi: 10.1007/s10103-020-03091-2
37. Martins AFL, Morais MO, de Sousa-Neto SS, de Jesus APG, Nogueira TE, Valadares MC, et al. Photobiomodulation reduces the impact of radiotherapy on oral health-related quality of life due to mucositis-related symptoms in head and neck cancer patients. Lasers Med Sci. (2021) 36:903–12. doi: 10.1007/s10103-020-03167-z
38. Robijns J, Lodewijckx J, Claes S, Van Bever L, Pannekoeke L, Censabella S, et al. Photobiomodulation therapy for the prevention of acute radiation dermatitis in head and neck cancer patients (DERMISHEAD trial). Radiother Oncol. (2021) 158:268–75. doi: 10.1016/j.radonc.2021.03.002
39. Bensadoun RJ, Bollet MA, Liem X, Cao K, Magné N. New photobiomodulation device for prevention and cure of radiotherapy-induced oral mucositis and dermatitis: results of the prospective safe PBM study. Support Care Cancer. (2022) 30:1569–77. doi: 10.1007/s00520-021-06574-2
40. DeLand MM, Weiss RA, McDaniel DH, Geronemus RG. Treatment of radiation-induced dermatitis with light-emitting diode (LED) photomodulation. Lasers Surg Med. (2007) 39:164–8. doi: 10.1002/lsm.20455
41. Cronshaw M, Parker S, Anagnostaki E, Mylona V, Lynch E, Grootveld M. Photobiomodulation and oral mucositis: a systematic review. Dent J. (2020) 8:87. doi: 10.3390/dj8030087
42. Mobadder ME, Farhat F, Mobadder WE, Nammour S. Photobiomodulation therapy in the treatment of oral mucositis, dysgeusia and oral dryness as side-effects of head and neck radiotherapy in a cancer patient: a case report. Dent J. (2018) 6:64. doi: 10.3390/dj6040064
43. Zecha JA, Raber-Durlacher JE, Nair RG, Epstein JB, Sonis ST, Elad S, et al. Low level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: part 1: mechanisms of action, dosimetric, and safety considerations. Support Care Cancer. (2016) 24:2781–92. doi: 10.1007/s00520-016-3152-z
44. Kauark-Fontes E, Migliorati CA, Epstein JB, Treister NS, Alves CGB, Faria KM, et al. Extraoral photobiomodulation for prevention of oral and oropharyngeal mucositis in head and neck cancer patients: interim analysis of a randomized, double-blind, clinical trial. Support Care Cancer. (2022) 30:2225–36. doi: 10.1007/s00520-021-06625-8
45. Zecha JA, Raber-Durlacher JE, Nair RG, Epstein JB, Elad S, Hamblin MR, et al. Low-level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: part 2: proposed applications and treatment protocols. Support Care Cancer. (2016) 24:2793–805. doi: 10.1007/s00520-016-3153-y
46. Brzak BL, Cigić L, Baričević M, Sabol I, Mravak-Stipetić M, Risović D. Different protocols of photobiomodulation therapy of hyposalivation. Photomed Laser Surg. (2018) 36:78–82. doi: 10.1089/pho.2017.4325
47. Sousa AS, Silva JF, Pavesi VCS, Carvalho NA, Ribeiro-Júnior O, Varellis MLZ, et al. Photobiomodulation and salivary glands: a systematic review. Lasers Med Sci. (2020) 35:777–88. doi: 10.1007/s10103-019-02914-1
48. Rezvani M, Robbins ME, Hopewell JW, Whitehouse EM. Modification of late dermal necrosis in the pig by treatment with multi-wavelength light. Br J Radiol. (1993) 66:145–9. doi: 10.1259/0007-1285-66-782-145
49. de Pauli Paglioni M, Alves CGB, Fontes EK, Lopes MA, Ribeiro ACP, Brandão TB, et al. Is photobiomodulation therapy effective in reducing pain caused by toxicities related to head and neck cancer treatment? A systematic review. Support Care Cancer. (2019) 27:4043–54. doi: 10.1007/s00520-019-04939-2
50. Kauark-Fontes E, Rodrigues-Oliveira L, Epstein JB, Faria KM, Araújo ALD, Gueiros LAM, et al. Cost-effectiveness of photobiomodulation therapy for the prevention and management of cancer treatment toxicities: a systematic review. Support Care Cancer. (2021) 29:2875–84. doi: 10.1007/s00520-020-05949-1
51. Young NC, Maximiano V, Arany PR. Thermodynamic basis for comparative photobiomodulation dosing with multiple wavelengths to direct odontoblast differentiation. J Biophotonics. (2022) 15:e202100398. doi: 10.1002/jbio.202100398
52. Khan I, Arany PR. Dosimetry for photobiomodulation therapy: response to Sommers et al. Ann Transl Med. (2016) 4:208. doi: 10.21037/atm.2016.05.34
53. Louzeiro GC, Teixeira DDS, Cherubini K, de Figueiredo MAZ, Salum FG. Does laser photobiomodulation prevent hyposalivation in patients undergoing head and neck radiotherapy? A systematic review and meta-analysis of controlled trials. Crit Rev Oncol Hematol. (2020) 156:103115. doi: 10.1016/j.critrevonc.2020.103115
Keywords: oral cancer, photobiomodulation, oral mucositis, dysgeusia, xerostomia, dermatitis, trismus, oedema
Citation: Gobbo M, Merigo E, Arany PR, Bensadoun R-J, Santos-Silva AR, Gueiros LA and Ottaviani G (2022) Quality Assessment of PBM Protocols for Oral Complications in Head and Neck Cancer Patients: Part 1. Front. Oral. Health 3:945718. doi: 10.3389/froh.2022.945718
Received: 16 May 2022; Accepted: 03 June 2022;
Published: 07 July 2022.
Edited by:
Paulo Bonan, Federal University of Paraíba, BrazilReviewed by:
Gabriela Botelho Martins, Federal University of Bahia, BrazilCopyright © 2022 Gobbo, Merigo, Arany, Bensadoun, Santos-Silva, Gueiros and Ottaviani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giulia Ottaviani, Z290dGF2aWFuaUB1bml0cy5pdA==