 Grégoire B. Morand
Grégoire B. Morand Khalil Sultanem2
Khalil Sultanem2- 1Department of Otolaryngology Head and Neck Surgery, Centre Intégré Universitaire de Santé et de Services Sociaux West-Central Montreal-Jewish General Hospital, McGill University, Montreal, QC, Canada
- 2Department of Radiation Oncology, Centre Intégré Universitaire de Santé et de Services Sociaux West-Central Montreal-Jewish General Hospital, McGill University, Montreal, QC, Canada
The treatment of oropharyngeal cancer has undergone many paradigms shifts in recent decades. First considered a surgical disease, improvements in radiotherapy led to its popularization in the 1990s. Subsequently, the discovery of the human papillomavirus (HPV) in the pathogenesis of oropharyngeal cancer, as well as the increase in HPV-associated oropharynx cancer incidence, have prompted a reevaluation of its management. Its sensitivity to standard treatment with a favorable prognosis compared to non HPV-associated oropharyngeal cancer led to a focus on minimizing treatment toxicity. Advances in radiation and surgical techniques, including the use of transoral robotic surgery, gave the rationale to ongoing de-escalation clinical trials in HPV-associated oropharynx cancer.
Introduction
Similar to oral cavity cancer, oropharyngeal cancer has classically been addressed surgically with wide local excision of the tumor with margins and neck dissection to address the lymphatic drainage [1]. Unlike oral cavity cancer, some oropharyngeal tumors are difficult to access through the transoral route. These are approached using a mandibular swing, midline glossotomy, lateral pharyngotomy, or pull-through [2]. The morbidity and potential complications associated with these approaches are significant, resulting in swallowing difficulties, malocclusion following mandibular osteotomy, and wound complications. Additionally, the lower lip sometimes has to be split for access, leaving a visible scar on the face. Furthermore, damage to the hypoglossal, lingual, and superior laryngeal nerves is possible, which makes postoperative swallowing rehabilitation more challenging. In addition, depending on the extent of the resection, reconstruction with a vascularized free tissue flap is often necessary [2, 3].
The morbid surgical approach to oropharyngeal cancers led to the popularization of radiotherapy as the primary treatment modality [4]. With the exception of early-stage cancer (T1, small T2 with limited nodal disease), this is usually combined with concomitant chemotherapy [5]. Radiotherapy has several advantages: oropharynx tumors are generally radiosensitive and radiotherapy treats the primary tumor and the neck during the same setting [6]. In the case of larger tumors of the oropharynx that extend over several sub-regions and/or extend to neighboring areas, radiation therapy offers the advantage of treating and preserving the pharynx and larynx and potentially preserving swallowing function. Finally, advanced carcinomas of the tonsil or soft palate sometimes metastasize to the retropharyngeal lymph nodes (Rouvière), which is not so easily accessible surgically [7, 8].
Radiotherapy, however, also has treatment-related toxicities, such as xerostomia, dysphagia, changes in taste, and dental caries [9]. These effects are chronic and lifelong, which can have a major impact on the quality of life of patients who survive oropharyngeal cancer [9, 10]. Radiotherapy gained popularity during the 1990s as an alternative to surgery. The introduction of conformal radiotherapy (IMRT: intensity modulated radiotherapy), which minimizes radiation to surrounding normal tissue has decreased toxicity while maintaining treatment efficacy and further contributed to the standard use of this modality [11].
Discovery of The Role of The Human Papilloma Virus In Oropharyngeal Cancer
Oropharyngeal carcinoma, like most head and neck squamous cell carcinomas, are classically caused by chronic exposure to extrinsic carcinogens such as cigarette smoke and alcohol. Thus, a patient who regularly smokes cigarettes is exposed to a higher risk of cancer of the mouth, oropharynx, larynx, and hypopharynx. However, a proportion of head and neck cancers occur in people without a history of tobacco or alcohol consumption, which suggests the contribution of other etiologies. Some epidemiological studies from the 1990s have shown that the incidence of cancer of the oropharynx was higher in geographical areas with high rates of cancer of the cervix [12, 13]. Since cervical cancer is caused by the human papillomavirus (HPV), this led to the hypothesis that a proportion of oropharyngeal cancers could also be caused by HPV [14, 15]. Many subsequent studies were able to confirm this hypothesis and demonstrate the causal link between HPV and a proportion of oropharyngeal cancer [16, 17].
Human papillomaviruses (HPVs) are DNA viruses that infect cells of the mucosal epithelium and are subsequently integrated into the cellular genome [18]. There are many HPV virus subtypes, but HPV serotypes 16, 18, 31, and 33 are considered the main carcinogenic serotypes. Transmission of the virus occurs from human to human through direct sexual contact [18]. The presence of the virus in tumor cells can be confirmed by the presence of HPV DNA by PCR or by in situ hybridization. In routine clinical practice, the presence of the protein p16, which is produced by cancer cells infected with HPV but cancer cells induced by extrinsic carcinogen exposure is often used as a surrogate marker for infection with HPV [18].
HPV-associated oropharyngeal cancer most commonly arises in the palatine tonsils (about 70% of cases), followed by base of tongue tonsillar tissue. For the other sites of the oropharynx, and for the oral cavity, larynx and hypopharynx, the role of HPV in oncogenesis is disputed, with likely <5% of cases attributable to HPV [19]. The predilection of HPV for the palatine and tongue base tonsils is poorly understood, but HPV is thought to infect the tonsil crypts where it finds an epithelium more susceptible to the transformative effects of the virus. For cervical cancer, HPV attacks the transformation zone between the squamous epithelium of the vagina and the columnar epithelium of the uterus [20].
Implications of Human Papilloma Virus In The Treatment Of Oropharyngeal Cancer
During the 2000s, many studies showed an increase in the proportion of oropharyngeal cancers caused by HPV. The percentage of HPV-associated oropharyngeal cancer was around 15% in the 1990s. In 2020 this proportion was estimated to reach 80% in North America [21]. At the same time, it was also found that HPV-associated tumors had a better prognosis than non-HPV-associated tumors regardless of the treatment modality [22]. This means that if you irradiate or operate on a tumor of the oropharynx, the prognosis is better if it is positive for HPV [21].
HPV-associated oropharynx cancer usually occurs in younger and healthier patients, and has a very high probability of achieving a long term cure [21, 23]. Since the traditional treatments for oropharyngeal cancer are subject to substantial morbidity and side effects that can persist in the long term, clinicians have tried to de-intensify the treatment [24]. The objective is to achieve the same oncological outcome while diminishing the side effects of the treatment. The goal is to improve the long term quality of life and survivorship in patients with HPV-associated oropharynx cancer. It is important to emphasize that an attempt to de-escalate the treatment can only be made in the context of a clinical trial ensuring that the de-escalation of the treatment is not detrimental to oncological outcomes of the patients [25].
Robotic Transoral Surgery As A Surgical De-Escalation Tool
Patients with HPV-associated cancer do better regardless of treatment modality. Beyond strategies aimed at limiting the toxicities related to radiotherapy, the possibility of using surgery as a primary modality has also been explored. In the early 2000s, technological progress allowed the popularization of the Da Vinci robot (Intuitive Surgical ©), which, due to its configuration, allows the surgeon to access the base of the tongue and the tonsils via a transoral route, thus avoiding the more morbid traditional external approaches to the oropharynx [26].
It is very important to understand the difference between non-surgical and surgical robots. A surgical robot is generally defined as a master-slave system where the machine is capable of performing movements directed by the surgeon. For transoral robotic surgery (TORS), the robot is merely an instrument that affords better visualization and access to remote areas of the oropharynx but is controlled by the surgeon. Therefore, it is more accurately called robot-assisted surgery.
Recent data suggests that the oncological results of robotic surgery are comparable to those of open surgery and chemoradiotherapy [27]. The ORATOR 1 study compared radiation vs. TORS in the treatment of early oropharyngeal cancers. Both modalities seemed to result in similar oncological outcomes but somewhat different side effect profiles [24]. Recently, the Eastern Cooperative Oncology Group (ECOG) 3,311 showed that upfront TORS followed by reduced doses of adjuvant radiation allows for similar oncologic results to standard chemoradiation in patients with locoregionally advanced HPV-associated oropharynx cancer [28].
Eventhou the benefits of TORS vs. radiotherapy are still controversial in early stage HPV-positive cancer [4], TORS seems to be a valid alternative to radiation therapy with similar oncologic outcomes and represents a de-escalation when compared to traditional surgical approaches. The most significant complication of robotic surgery is postoperative hemorrhage with an incidence rate ranging from 3 to 8% [24]. Although exceedingly rare, this complication can be fatal. The risk and amount of postoperative bleeding can be reduced by ligating branches of the external carotid artery [29].
A further disadvantage of TORS is the fact that postoperative radiation may be necessary is a significant proportion of cases, for which safe margins could not be achieved by surgery only [24]. Furthermore, postoperative radiation to the neck is often considered necessary for 2 or more positive nodes. In case of positive microscopic margins and/or extranodal extension, adjuvant chemoradiation is needed [30].
Future Directions
There are several de-escalation strategies that have been performed for HPV-associated oropharynx cancers (Table 1). In 2019, two large randomized clinical trials evaluated a less toxic concomitant chemotherapy (cetuximab) demonstrated that standard therapy with concomitant high-dose cisplatin had a better cure rate and therefore remained the standard of care [36, 37]. However, interest in de-escalation has not waned and many more studies are underway.
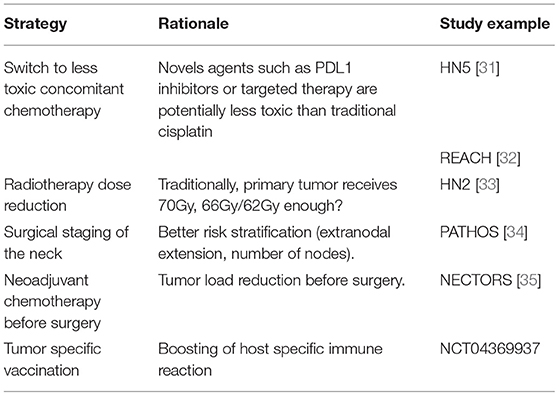
Table 1. Deintensification strategies in HPV-positive oropharyngeal cancer.
After several trials have shown the superiority of check-point inhibitors over standard chemotherapy in the recurrent and metastatic setting [38], numerous studies have tried to imitate those success in the definitive setting and to potentially deescalate the treatment for patients. Among the first studies with check point inhibitors in the definitive setting, the JAVELIN 100 study was negative as it failed to show a survival advantage in patients receiving avelumab compared to placebo in addition to standard chemoradiation [39, 40]. The interest for immunotherapy has however not faded. Trials similar to JAVELIN 100 in lung and esophageal cancer showed that the addition of check-point inhibitor in the adjuvant rather than concomitant setting let to survival improvement, suggesting that timing of stimulation of the immune system is critical to the oncologic outcome [39].
Given that standard chemoradiation treatment for patients with locoregionally advanced HPV-associated oropharynx cancer often leads to lifelong treatment-related toxicities and about 20% failure rate alternative treatment strategies are being sought. Our group has been evaluating the use of neoadjuvant platinum-based chemotherapy followed by robotic surgery for locoregionally advanced HPV-associated oropharyngeal cancer [American Joint Commission on Cancer version-7 (AJCC-7) Stage III (T1N1, T2N1, T3N0, T3N1) and stage IVa (T1N2, T2N2, T3N2)]. The Neoadjuvant Chemotherapy and Transoral Robotic Surgery for Oropharyngeal Cancer (NECTORS) study hypothesizes that treatment with neoadjuvant chemotherapy followed by transoral surgery and neck dissection is highly effective treatment allowing competitive cure rate compared to concurrent chemoradiotherapy with <10% failure rate, while avoiding radiotherapy in majority of cases. It is also hypothesized that better functional and quality of life outcome can achieved with this approach [41].
Conclusion And Outlook
In conclusion, this review presents a brief history of oropharyngeal cancer treatment. Traditionally approached by morbid surgeries, advances in radiotherapy and the good response of oropharyngeal cancer to this treatment modality led to a paradigm shift. Subsequently, the discovery of the role of HPV in the oncogenesis of oropharyngeal carcinoma and the favorable prognosis associated with younger age at diagnosis have provided the rationale for de-escalation therapy for which many approaches are being evaluated. Among those, transoral robotic surgery (TORS) is a validated approach with similar outcomes to conformational radiotherapy in terms of tumor control and quality of life. Many trials are on-going to determine the effectiveness and side effects of different de-escalation strategies.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
Study idea by AM. Manuscript drafting, literature review, and table by GM. All authors reviewed, amended, and approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors of the study would like to thank Isabel Cardona and Lisa Antonanzas.
References
1. Morand GB, Diaconescu A, Ibrahim I, Lamarche G, Ruas JS, Dalfen J, et al. Molecular prognostic indicators in HPV-positive oropharyngeal cancer: an updated review. Clin Exp Metastasis. (2022) 1–10. doi: 10.1007/s10585-022-10148-9
2. Trivedi N Tumors Tumors of the Oropharynx Atlas Atlas of Head and Neck Cancer Surgery. New Delhi: Springer (2015). p. 143–55.
3. Seikaly H, Rieger J, Wolfaardt J, Moysa G, Harris J, Jha N. Functional outcomes after primary oropharyngeal cancer resection and reconstruction with the radial forearm free flap. The Laryngoscope. (2003) 113:897–5904. doi: 10.1097/00005537-200305000-00023
4. Monnier Y, Simon C. Surgery vs. radiotherapy for early oropharyngeal tumors: a never-ending debate. Current treatment options in oncology. (2015) 16:1–513. doi: 10.1007/s11864-015-0362-4
5. Calais G, Alfonsi M, Bardet E, Sire C, Germain T, Bergerot P, et al. Randomized trial of radiation therapy vs. concomitant chemotherapy and radiation therapy for advanced-stage oropharynx carcinoma. JCNI. (1999) 91:2081–6. doi: 10.1093/jnci/91.24.2081
6. Lekanne dit Deprez Morand GB, Thüring C, Pazahr S, Hüllner MW, Broglie MA. UV max for predicting regional control in oropharyngeal cancer. Eur Arch Oto-Rhino-L. (2021) 1–11. doi: 10.1007/s00405-021-07169-7
7. Spencer CR, Gay HA, Haughey BH, Nussenbaum B, Adkins DR, Wildes TM, et al. Eliminating radiotherapy to the contralateral retropharyngeal and high level iI lymph nodes in head and neck squamous cell carcinoma is safe and improves quality of life. Cancer. (2014) 120:3994–4002. doi: 10.1002/cncr.28938
8. Ludwig R, Hoffmann JM, Pouymayou B, Dappen MB, Morand GB, Guckenberger M, et al. Detailed patient-individual reporting of lymph node involvement in oropharyngeal squamous cell carcinoma with an online interface. Radiother Oncol. (2022) 169:1–7. doi: 10.1016/j.radonc.2022.01.035
9. Morand GB, Madana J, Da Silva SD, Roskies M, Sultanem K, Black MJ, et al. Survival and quality of life in oropharyngeal cancer patients treated with primary chemoradiation after salivary gland transfer. J Laryngol Otol. (2016) 130:755–62. doi: 10.1017/S0022215116008100
10. Nutting CM, Morden JP, Harrington KJ, Urbano TG, Bhide SA, Clark C, et al. Parotid-sparing intensity modulated vs. conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol. (2011) 12:127–36. doi: 10.1016/S1470-2045(10)70290-4
11. Nutting C, A'Hern R, Rogers M, Sydenham M, Adab F, Harrington K, et al. First results of a phase iII multicenter randomized controlled trial of intensity modulated (IMRT) vs. conventional radiotherapy (RT) in head and neck cancer (PARSPORT: iSRCTN48243537; cRUK/03/005). J Clin Oncol. (2009) 23:518–9. doi: 10.1016/j.clon.2010.08.021
12. Rabkin CS, Biggar RJ, Melbye M, Curtis RE. Second primary cancers following anal and cervical carcinoma: evidence of shared etiologic factors. American Journal of Epidemiology. (1992) 136:54–58. doi: 10.1093/oxfordjournals.aje.a116420
13. Hemminki K, Dong C, Frisch M. Tonsillar and other upper aerodigestive tract cancers among cervical cancer patients and their husbands. Eur J Cancer Prev. (2000) 9:433–7. doi: 10.1097/00008469-200012000-00010
14. Dürst M, Gissmann L H. Ikenberg, and h. zur Hausen, A papillomavirus DNA from a cervical carcinoma and its prevalence in cancer biopsy samples from different geographic regions. Proc Natl Acad Sci U S A. (1983) 80:3812–5. doi: 10.1073/pnas.80.12.3812
15. Boice JD, Jr Day NE, Andersen A, Brinton LA, Brown R, Choi NW, et al. Second cancers following radiation treatment for cervical cancer. an international collaboration among cancer registries. JNCI. (1985) 74:955–75. doi: 10.1093/jnci/74.5.955
16. Schwartz SM, Daling JR, Doody DR, Wipf GC, Carter JJ, Madeleine MM, et al. Oral cancer risk in relation to sexual history and evidence of human papillomavirus infection. JNCI. (1998) 90:1626–36. doi: 10.1093/jnci/90.21.1626
17. Andl T, Kahn T, Pfuhl A, Nicola T, Erber R, Conradt C, et al. Etiological involvement of oncogenic human papillomavirus in tonsillar squamous cell carcinomas lacking retinoblastoma cell cycle control. Cancer Res. (1998) 58:5–13.
18. Lee JO, Russo AA, Pavletich NP. Structure of the retinoblastoma tumour-suppressor pocket domain bound to a peptide from hPV e7. Nature. (1998) 391:85–65. doi: 10.1038/36038
19. Combes JD, Franceschi S. Role of human papillomavirus in non-oropharyngeal head and neck cancers. Oral Oncol. (2014) 50:370–9. doi: 10.1016/j.oraloncology.2013.11.004
20. Gillison ML, Koch WM, Shah KV. Human papillomavirus in head and neck squamous cell carcinoma: are some head and neck cancers a sexually transmitted disease? Curr Opin Oncol. (1999) 11:191–9. doi: 10.1097/00001622-199905000-00010
21. Nichols AC, Palma DA, Dhaliwal SS, Tan S, Theuer J, Chow W, et al. The epidemic of human papillomavirus and oropharyngeal cancer in a canadian population. Curr Oncol. (2013) 20:212–9. doi: 10.3747/co.20.1375
22. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tân PF, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J. (2010) 363:24–35. doi: 10.1056/NEJMoa0912217
23. Henry M, Arnovitz E, Frenkiel S, Hier M, Zeitouni A, Kost K, et al. Psychosocial outcomes of human papillomavirus (HPV)- and non-HPV-related head and neck cancers: a longitudinal study. Psycho-Oncology. (2022) 31:185–197.
24. Nichols AC, Theurer J, Prisman E, Read N, Berthelet E, Tran EK, et al. Radiotherapy vs. transoral robotic surgery and neck dissection for oropharyngeal squamous cell carcinoma (ORATOR): an open-label, phase. 2, randomised trial. Lancet Oncol. (2019) 20:1349–59. doi: 10.1016/S1470-2045(19)30410-3
25. Golusinski P, Corry J, Vander Poorten V, Simo R, Sjögren E, Mäkitie A, et al. De-escalation studies in hPV-positive oropharyngeal cancer: how should we proceed? Oral oncology. (2021) 123:105620. doi: 10.1016/j.oraloncology.2021.105620
26. Morand GBR, Angeregg N, Kleinjung T, Bohlender JE, Veraguth D, Broglie M, et al. Assessment of surgical complications respecting the surgical indication: proposal for an novel index. Frontiers in surgery. (2021) 8:9. doi: 10.3389/fsurg.2021.638057
27. De Almeida Byrd JK, Wu R, Stucken CL, Duvvuri U, Goldstein DP, Miles BA, et al. A systematic review of transoral robotic surgery and radiotherapy for early oropharynx cancer: a systematic review. The Laryngoscope. (2014) 124:2096–102. doi: 10.1002/lary.24712
28. Ferris RL, Flamand Y, Weinstein GS, Li S, Quon H, Mehra R, et al. Transoral robotic surgical resection followed by randomization to low-or standard-dose IMRT in resectable p16+ locally advanced oropharynx cancer: a trial of the ECOG-ACRIN Cancer Research Group (E3311). Am J Clin Oncol. (2020) 6500. doi: 10.1200/JCO.2020.38.15_suppl.6500
29. Gleysteen J, Troob S, Light T, Brickman D, Clayburgh D, Andersen P, et al. The impact of prophylactic external carotid artery ligation on postoperative bleeding after transoral robotic surgery (TORS) for oropharyngeal squamous cell carcinoma. Oral Oncology. (2017) 70:1–6. doi: 10.1016/j.oraloncology.2017.04.014
30. Bernier J, Cooper JS, Pajak T, Van Glabbeke M, Bourhis J, Forastiere A, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the eORTC (# 22931) and rTOG (# 9501). Head Neck. (2005) 27:843–50. doi: 10.1002/hed.20279
31. Wu SY, Yom SS. Current standards for organ preservation in locoregionally advanced non-nasopharyngeal head and neck cancer and evolving strategies for favorable-Risk and platinum-Ineligible populations. Curr Treat Options Oncol. (2019) 20:89. doi: 10.1007/s11864-019-0688-4
32. Tao Y, Aupérin A, Sun X, Sire C, Martin L, Coutte A, et al. Avelumab-cetuximab-radiotherapy vs. standards of care in locally advanced squamous-cell carcinoma of the head and neck: the safety phase of a randomised phase iII trial gORTEC 2017-01 (REACH). Eur J Cancer. (2020) 141:21–9. doi: 10.1016/j.ejca.2020.09.008
33. Yom SS, Torres-Saavedra P, Caudell JJ, Waldron JN, Gillison ML, Xia P, et al. Reduced-Dose radiation therapy for hPV-Associated oropharyngeal carcinoma (NRG oncology hN002). J Clin Oncol. (2021) 39:956–65. doi: 10.1200/JCO.20.03128
34. Owadally W, Hurt C, Timmins H, Parsons E, Townsend S, Patterson J, et al. PATHOS: a phase iI/III trial of risk-stratified, reduced intensity adjuvant treatment in patients undergoing transoral surgery for human papillomavirus (HPV) positive oropharyngeal cancer. BMC cancer. (2015) 15:1–10. doi: 10.1186/s12885-015-1598-x
35. Sadeghi N, Li NW, Taheri MR, Easley S, Siegel RS. Neoadjuvant chemotherapy and transoral surgery as a definitive treatment for oropharyngeal cancer: a feasible novel approach. Head neck. (2016) 38:1837–46. doi: 10.1002/hed.24526
36. Mehanna H, Robinson M, Hartley A, Kong A, Foran B, Fulton-Lieuw T, et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE hPV): an open-label randomised controlled phase 3 trial. Lancet. (2019) 393:51–60. doi: 10.1016/S0140-6736(18)32752-1
37. Gillison ML, Trotti AM, Harris J, Eisbruch A, Harari PM, Adelstein DJ, et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG oncology rTOG 1016): a randomised, multicentre, non-inferiority trial. Lancet. (2019). 393:40–50. doi: 10.1016/S0140-6736(18)32779-X
38. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M G., De Castro JR, et al. Pembrolizumab alone or with chemotherapy vs. cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. (2019) 394:191–28. doi: 10.1016/S0140-6736(19)32591-7
39. Yu Y, Zakeri K, Lee N. Javelin head neck 100: should we combine immunotherapy with radiation therapy? Oncotarget. (2021) 12:2223–6. doi: 10.18632/oncotarget.27987
40. Lee NY, Ferris RL, Psyrri A, Haddad RI, Tahara M, Bourhis J, et al. Avelumab plus standard-of-care chemoradiotherapy vs. chemoradiotherapy alone in patients with locally advanced squamous cell carcinoma of the head and neck: a randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. Lancet Oncol. (2021) 22:450–62. doi: 10.1016/S1470-2045(20)30737-3
Keywords: radiotherapy, intensity-modulated, quality of life, oropharyngeal neoplasms, xerostomia
Citation: Morand GB, Sultanem K, Mascarella MA, Hier MP and Mlynarek AM (2022) Historical Perspective: How the Discovery of HPV Virus Led to the Utilization of a Robot. Front. Oral. Health 3:912861. doi: 10.3389/froh.2022.912861
Received: 05 April 2022; Accepted: 20 April 2022;
Published: 06 May 2022.
Edited by:
Ronell Bologna-Molina, Universidad de la República, UruguayReviewed by:
Wei-fa Yang, The University of Hong Kong, Hong Kong SAR, ChinaCopyright © 2022 Morand, Sultanem, Mascarella, Hier and Mlynarek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alex M. Mlynarek, YWxleC5tbHluYXJla0BtY2dpbGwuY2E=