 Sven E. Niklander
Sven E. Niklander
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oral. Health , 22 February 2021
Sec. Oral Cancers
Volume 2 - 2021 | https://doi.org/10.3389/froh.2021.642238
This article is part of the Research Topic The Translational and Therapeutic Potential of the Tumor Microenvironment in Oral Cancer View all 11 articles
Approximately 15% of cancers are attributable to the inflammatory process, and growing evidence supports an association between oral squamous cell carcinoma (OSCC) and chronic inflammation. Different oral inflammatory conditions, such as oral lichen planus (OLP), submucous fibrosis, and oral discoid lupus, are all predisposing for the development of OSCC. The microenvironment of these conditions contains various transcription factors and inflammatory mediators with the ability to induce proliferation, epithelial-to-mesenchymal transition (EMT), and invasion of genetically predisposed lesions, thereby promoting tumor development. In this review, we will focus on the main inflammatory molecules and transcription factors activated in OSCC, with emphasis on their translational potential.
The links between cancer and chronic inflammation are well-established. In this process, pro-inflammatory mediators act by stimulating inflammation to either abrogate tumor progression or facilitate tumor growth and metastasis [1, 2]. Approximately 15% of cancers are attributable to the inflammatory process [3]. Such cancers include lung, pancreatic, esophageal, bladder, gastric, cervical, colorectal, and prostate [4]. During the oral malignant transformation process [from non-dysplastic hyperkeratosis, through oral dysplasia to the development of oral squamous cell carcinoma (OSCC)], there is a progressive increase of the inflammatory infiltrate (quality and density) [5], and growing evidence supports an association between OSCC and chronic inflammation [6, 7]. Different oral inflammatory conditions, such as OLP, submucous fibrosis, and oral discoid lupus, are all predisposing for the development of OSCC [8]. The microenvironment of these conditions contains activated cytokines and chemokines, prostaglandins, reactive oxygen species, and various transcription factors. Some of these mediators have the ability to induce proliferation, epithelial-to-mesenchymal transition (EMT), and invasion [9] of genetically predisposed lesions (with mutations in tumor-suppressor genes and/or oncogenes), thereby promoting tumor development. In established OSCC, chronic inflammation is also a common feature, being involved in tumor progression, invasion, and metastasis [5, 6, 10]. Thus, many studies have assessed the utility of different inflammatory molecules as prognostic biomarkers and treatment targets for OSCC.
The aim of this review is to outline the main inflammatory molecules and transcription factors activated in OSCC, with special focus on their translational potential.
There are different inflammatory mediators reported to have a role in the development and progression of OSCC (Table 1). In this review, we will focus on the most commonly investigated.
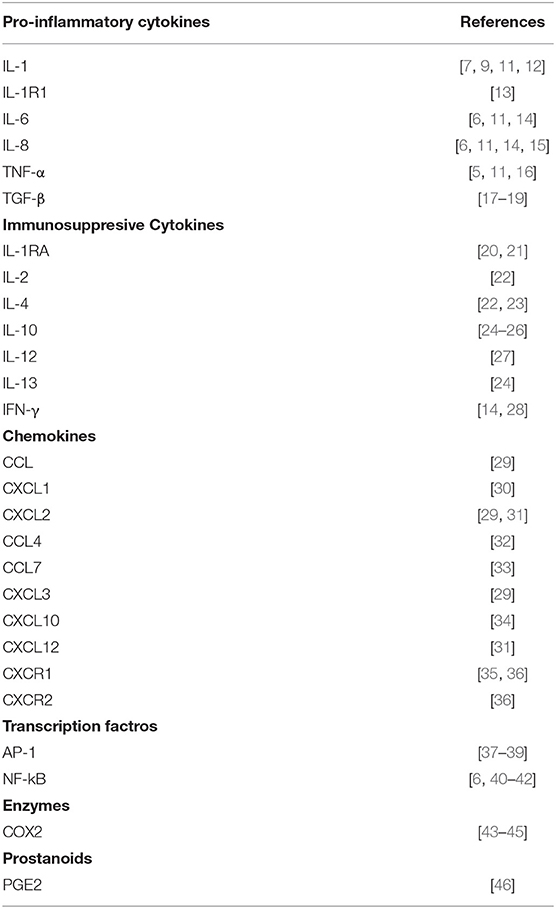
Table 1. Inflammatory pathways and mediators reported to have a role in oral carcinogenesis.
Nuclear factor kappa-beta (NF-κB) is a key inflammatory transcription factor frequently expressed in tumors that regulates the expression of a variety of genes involved in inflammation, proliferation, tumorigenesis, and cell survival [47–49]. NF-κB is canonically activated by tumor necrosis factor alpha (TNF-α), interleukin (IL)-1, and lipopolysaccharide (LPS) [48], and when activated, it enhances the expression of different cytokines, including IL-1, IL-6, and IL-8 [50]. Its aberrant expression is linked to carcinogenesis [51] and EMT induction [52] and is associated with worse survival in solid cancers [53]. In OSCC, NF-κB is constitutively activated and is associated with the upregulation of different inflammatory genes, including IL-6, IL-8, CCL5, and CXCL10 [6], and is considered a major factor responsible for the inflammatory infiltrate observed in the tumor microenvironment (TME) [54]. NF-κB has an important role in the malignant phenotype of oral cancers, as it participates in the modulation of bone invasion [48]; enhances angiogenesis [55], invasion [40, 56], and metastasis [40, 41]; and induces EMT [52]. The EMT process is a crucial step for the development of OSCC metastasis [57]. It involves the repression of E-cadherin (an important epithelial adhesion molecule) via Snail expression, which depends on NF-κB activation via AKT [52]. IL-8 and EGF are able to induce EMT via NF-κB activation, and IL-8- and EGF-induced EMT can be reversed by blocking AKT or NF-κB [58, 59]. NF-κB importance during OSCC development is well-exemplified by its inactivation, as this inhibits cell survival and growth; expressions of IL-1α, IL-6, and IL-8 [60]; and metastases [41]. Because of this, NF-κB inhibition has been proposed as a possible treatment for head and neck squamous cell carcinoma (HNSCC).
Activator protein 1 (AP-1) is a transcription factor complex composed of either homodimers of Jun protein or heterodimers of Jun and Fos proteins [61] that orchestrates the expression of different genes involved in inflammation, embryonic development, lymphoid proliferation, oncogenesis, and apoptosis [62] and is reported to be essential for DNA synthesis [63]. AP-1 activation seems to be of clinical significance in cancer, as high expression levels have been associated with drug resistance [64]. AP-1 is activated during oral keratinocyte carcinogenesis [37], and its expression increases with oral tumor progression [38]. Similar to NF-κB, it can also be activated by IL-1 [65], which induces IL-8 secretion and promotes the cell survival and growth of HNSCC cells [39]. A recent study suggested that AP-1 induces bcl-2 expression (a proto-oncogene related to apoptosis suppression implicated in resistance to chemoradiation therapy in OSCC) in recurrent chemo- and radioresistant oral tumors [38], which suggests that targeting the AP-1 pathway might contribute to overcome resistance to chemoradiation therapy in OSCC. As AP-1 can be activated by IL-1, targeting IL-1 could be beneficial for oral cancer treatment, as this could reduce the activation of NF-κB and AP-1 pathways with subsequent reduction of bcl-2, but this hypothesis needs to be corroborated.
TNF-α is a multifunctional cytokine identified as an important mediator of cancer development [66], as well as induces EMT [67] and enhances tumor angiogenesis [68] and invasion [56]. Therefore, it is considered an important regulator of proliferation, invasion, and metastasis of many cancers [69]. TNF-α is expressed in some oral potentially malignant disorders (OPMDs), such as OLP [70], and is endogenously expressed in oral carcinomas [71]. In OSCC, TNF-α promotes a pro-invasive and pro-inflammatory phenotype in a paracrine manner [5, 16] by upregulating genes that are associated with neutrophil recruitment, invadopodia, and invasion. The upregulation of these genes was also associated with reductions in both the overall survival and disease-free survival of patients with OSCC [5]. Elevated TNF-α receptor-1 (TNFR-1) signaling has also been associated with metastasis of OSCC [41, 72], attributable to the ability of TNF-α to stimulate the invasion of OSCC cells by enhancing matrix metalloproteinase (MMP)-2 and MMP-9 production [41, 56], which is regulated by the NF-κB, AKT, and PI3K signaling pathways [5, 41, 72]. It has been demonstrated that MMPs play critical roles in OSCC, as elevated expression of MMPs is associated with increased OSCC invasion, metastasis, and poor prognosis [73–75]. MMPs are also reported to have a prominent role in the EMT process [76], as MMP-2, MMP-9, and MMP-7 are able to enhance EMT [77–79]. NF-κB is an important regulator of MMPs [80], and TNF-α can activate NF-κB via TNFR1, which results in enhanced MMP secretion [81]. TNF-α is also able to induce EMT via p38 MAPK activation [82], and TNF-α-induced EMT has been related to the induction of cancer stem cells (CSCs) [67]. The presence of CSCs in OSCC is of importance as this has been linked to therapy resistance and worst prognosis. In OSCC, the expression of CD44 (a well-known CSC marker) has been associated with increased cell invasion, cell migration, and therapy resistance via a mechanism that includes the activation of PI3K/Akt/GSK3β and Raf-MEK-ERK signaling networks [83], and silencing CD47 (a molecule involved in the generation of CSCs in OSCC) has shown to reduce EMT and the presence of CSCs [84]. The activation of the PI3K/Akt/GSK3β signaling pathway has also been associated with increased proliferation, invasion [85], the development of EMT, and distant metastasis [86].
Due to all the beneficial effects of TNF-α during cancer development, targeting TNF-α might be a useful strategy for OSCC treatment. In vitro experiments have shown anti-TNF-α therapy to reduce growth and metastasis of OSCC cells [87], but this needs to be investigated further before it can be translated into the clinic.
Both IL-6 and IL-8 are considered “oncogenic cytokines,” as they are able to cause EMT [88], stimulate angiogenesis and tumor growth [89, 90], disrupt cell–cell communication, impede macrophage function, and promote epithelial and endothelial cell migration and invasion [91]. IL-6 and IL-8 levels are elevated in patients with OPMDs and OSCCs [6, 14, 92, 93], which is likely to be a consequence of aberrant NF-κB activation [94]. IL-6 and IL-8 can be produced by malignant oral keratinocytes themselves, or by other cells of the TME, such as tumor-associated macrophages (TAMs). TAMs are an important source of both of these cytokines, and thus many attempts have been done to target TAMs to restrict their secretion [95]. IL-8 is reported to act as an autocrine growth factor in HNSCC and other cancers [15] and has been proposed as a potential mediator of the development of OSCC. It is constitutively expressed in malignant oral keratinocytes, and its inhibition decreases viability, proliferation [6], and invasion of OSCC cells [16] and enhances the proliferation, angiogenesis, and survival rate of cancer cells [96]. Similarly, IL-6 overexpression in patients with HNSCC is associated with poor prognosis, probably by enabling an immunosuppressive TME by increasing the presence of myeloid-derived suppressor cells and PDL-1 expression, and is considered a significant predictor of treatment outcome [97]. In OSCC, the expressions of IL-6 and IL-8 are associated with a more invasive mode of growth [11].
IL-1 is the prototype of a pro-inflammatory cytokine and includes IL-1α and IL-1β. IL-1α and IL-1β are both constitutively expressed in OSCC [9, 12, 98, 99], can be found in the saliva of patients with OSCC [100, 101], and have been reported to have important functions in OSCC carcinogenesis and tumor progression [7, 10].
IL-1α expressed by OSCC promotes autocrine activation of NF-κB and AP-1 and upregulates the expression of IL-8 [39] and IL-6 [98]. OSCC cells produce IL-1α [12], which induces the proliferation and cytokine secretion by cancer-associated fibroblasts (CAFs) (CCL7, CXCL1, and IL-8), promoting tumor progression [33]. IL-1α seems to be important for the development of distant metastases, as IL-1α is highly expressed in metastatic HNSCC tumors compared to non-metastatic HNSCC tumors. This is probably achieved by the capability of IL-1α to induce transmigration of tumor cells across the endothelium and to enhance the expression of metastatic genes, such as MMP-9, PGE2, VEGF, and IL-8 [10]. It has also been reported that IL-1α can act as an oncoprotein by itself, as intranuclear IL-1α has been shown to induce malignant transformation of cells from the bone marrow and perivascular area [102].
IL-1β increases the levels of IL-6 and IL-8 expressed by OD and OSCC cells and promotes the invasiveness of OSCC by inducing EMT [9]. IL-1β has also been identified as a key node gene in the TME of OSCC in vivo [7]. The expression of precursor IL-1β mRNA is correlated with the presence of malignant changes (from normal, to mild, through severe dysplasia to OSCC) [9], and elevated IL-1β expression has been related to lymph node metastasis of OSCC [103]. IL-1 produced by HNSCC can also stimulate the production of different cytokines by CAFs and normal fibroblasts, such as CCL-7, CXCL1, IL-8, and CCL-5 [33, 104]. These findings strongly suggest a possible role of IL-1β in the oral carcinogenesis process, which is supported by the fact that IL-1β silencing can reduce tumor size in vivo [7].
The IL-1 agonist receptor, IL-1R1, is also overexpressed in OSCCs and, together with IL-1β, was shown to promote cancer growth and metastasis by upregulating CXCR4, which could be reversed by inhibiting IL-1R1 by overexpressing the interleukin 1 receptor antagonist (IL-1RA) [13]. Interestingly, IL-1RA has been reported to be downregulated in OD and in OSCC [20] and is reported to regulate IL-1-induced secretion of IL-6 and IL-8 by inhibiting the p38 MAPK and NF-κB pathways [50, 105].
Cyclooxygenase (COX)-2, an inflammation-induced enzyme that converts arachidonic acid into prostaglandins [e.g., prostaglandin E2 (PGE2)], is frequently expressed in many types of cancers. COX-2 is able to induce CSC-like activity and to promote angiogenesis, proliferation, apoptotic resistance, inflammation, invasion, and metastasis of cancer cells [106]. Importantly, COX-2 inhibition has been shown to reverse cancer progression [107, 108]. COX-2 is induced by a variety of molecules, including IL-1 [109], epithelial growth factor (EGF) [110], transforming growth factor-beta (TGF-β) [111, 112], and TNF-α. COX-2 expression is induced early in the process of oral carcinogenesis [43]. Its level is associated with the degree of dysplasia [44], is overexpressed in OSCC [113, 114], and is correlated with advanced tumor stage, high risk of distant metastasis [115], and worse prognosis in patients with OSCC [116]. In oral cancer, COX-2 is of importance for maintaining a chronic inflammatory state [117], influencing different processes, such as cell migration by upregulating the expression of intercellular adhesion molecule-1 (ICAM-1) via PGE2 [46], and lymphoangiogenesis by regulating VEGF production [45, 118, 119]. VEGF is commonly overexpressed in OSCC, and COX-2/VEGF-C co-expression is correlated with lymphoangiogenesis, lymph node metastasis, and TNM stage and is reported as an independent factor for survival [45]. Increased VEGF expression in oral cancer is also a consequence of tumor-associated hypoxia, as VEGF is upregulated in decreasing concentrations of oxygen [120, 121]. In reduced oxygen concentrations, hypoxia-inducible factor-1α (HIF-1α) binds to hypoxia response elements and upregulates VEGF, promoting angiogenesis [122]. In OSCC, HIF-1α and HIF-2α correlate positively with clinical–pathological parameters, such as tumor size and micro vessel density, and in vivo experiments have shown their knockdown to reduce tumor angiogenesis and tumor growth [123]. In addition, hypoxia will also promote an inflammatory state, as VEGF is able to induce COX-2 expression, which will result in the production of PGE2 and the activation of NF-κB [124].
TGF-β is a multifunctional pro-inflammatory cytokine that can either inhibit or promote tumor formation and progression of many cancers, whether by inducing apoptosis and growth arrest and by inhibiting proliferation or by stimulating angiogenesis, inflammation, EMT, and immune suppression, respectively [125]. If TGF-β acts as a tumor suppressor or tumor promoter depends on the regional and cellular context [126]. In OSCC, TGF-β is reported to promote tumorigenesis [17]. This is supported by the fact that OPMDs [18] and OSCC [19, 127] express higher levels of TGF-β than healthy controls and that high TGF-β levels are associated with disease recurrence and poor prognosis in patients with OSCC [19]. There are different mechanisms by which TGF-β could act as a tumor promoter in oral cancer. TGF-β is probably the most important factor involved in the differentiation of CAFs, and the accumulation of CAFs is reported as an independent prognostic factor in OSCC. CAFs are able to modulate the TME, facilitating cancer progression [128]. An in vivo mouse model in which TGF-β1 was transgenically induced revealed that TGF-β1 induced epithelia hyperproliferation, severe inflammation, and angiogenesis at similar levels to those observed in HNSCCs, suggesting that TGF-β1 provides a tumor-promoting microenvironment [17]. In OPMDs, TGF-β promotes a more malignant phenotype by increasing cell motility via the protein phosphatase 1 (PP-1) signaling pathway [129]. TGF-β seems to be important for EMT development, as TGF-β induces EMT in endothelial cells, and endothelial cells cultured with TGF-β are able to induce EMT in OSCC cells [130]. Also, TGF-β is able to induce EMT by stimulating the expression of ADAM12 (a desintegrin and metalloprotease associated with cancers) [131].
Anti-inflammatory cytokines also have a role in the oral carcinogenesis process. They can act as a double-edged sword, they can counteract the tumorigenic potential of their pro-inflammatory counterpart, and they can act as immunosuppressive molecules by decreasing the anti-tumor immune response [132]. Different immunosuppressive cytokines have been reported to have different roles in OSCC development (Table 1), with IL-1RA, IL-4, IL-10, and IL-13 being the most commonly investigated. IL-1RA decreases during the oral carcinogenesis process [20] and IL1RN (the gene that codes for IL-1RA) is downregulated in HNSCC [133, 134]. This in theory would allow higher IL-1 activity with the aforementioned effects. Nevertheless, high IL1-RA expression has been reported in advanced and poorly differentiated OSCCs [20, 24], suggesting that IL-1RA expression could increase tumor progression, but this needs further investigation. IL-4, IL-10, and IL-13 have also been reported to increase in OSCC patients compared to healthy controls [24, 25, 135], and high IL-10 expression has been associated with a more aggressive OSCC phenotype [136]. IL-4 induces immune deviation from TH1 to TH2 responses, which prevents tumor rejection [137]; IL-10 suppresses the anti-tumor immunity and contributes to tumor immune escape [135] and IL-13 compromises the anti-tumor response by inhibiting IFN-γ secretion and CD8+ T lymphocyte activity [138].
Within the TME, cancer cells are not the only source of inflammatory molecules. Tumors are complex systems composed not only of neoplastic cells but also of stromal cells, which form the TME. These cells are not innocent bystanders and can interact with tumor cells and modify the extracellular matrix, facilitating and promoting proliferation, invasion, angiogenesis, and metastasis [49, 139]. Single cell profile of 5,578 samples obtained from 18 OSCCs revealed the presence of nine clusters of cells based on known marker genes, such as epithelial cells (malignant and non-malignant, based on CNV and their karyotypes), T cells (four sub-clusters), B/plasma cells, macrophages, dendritic cells, mast cells, endothelial cells, fibroblasts (three sub-clusters), and myocytes [140], which shows how heterogeneous tumors are.
As discussed previously, malignant oral keratinocytes (which are genetically unstable) activate different transcription factors, such as AP-1 and NF-κB, leading to the activation of oncogenes (which induces proliferation by the regulation of apoptosis, angiogenesis, and cell growth), and inflammatory genes [6]. The latter results in the constitutive production of different inflammatory factors, such as IL-1, IL-6, IL-8, TNF-α, and TGF-β [141], among many others, that can activate the same transcription factors, creating a positive feedback loop.
TAMs, T lymphocytes, neutrophils, and mast cells are also considered important sources of inflammatory mediators [5]. TAMs promote proliferation and invasion in OSCC [142, 143], and their presence correlates with disease progression and is considered an adverse prognostic factor [144]. They act as an important source of cytokines, metalloproteinases, and growth factors [95]. T lymphocytes are considered the most abundant inflammatory cells among the inflammatory infiltrate observed in OSCCs and can be beneficial or detrimental for oral carcinogenesis depending on their secretion profile [145]. They can secrete molecules that favor tumor progression (IL-6, IL-17, IL-23, TNF-α, and TGF-β) or molecules that exhibit an anti-tumor effect (IL-12 and IFN-γ) [49]. Neutrophil infiltration increases OSCC invasion by inducing matrix degradation and invadopodia formation through a paracrine TNF-α-induced mechanism [5, 16]. Mast cells have been associated with angiogenesis and are able to secrete numerous cytokines, chemokines, and angiogenic factors [146, 147], but their role in the development of OSCC is still debatable.
Cancer-associated fibroblasts, the most dominant components of the TME, are recipients of many of these factors (e.g., TGF-β), as well as directly contributing to tumor progression and an inflammatory TME via the secretion of VEGF, IL-6, IL-8, PGE2, TGF-β, and activation of NF-κB [148]. The presence and activity of CAFs are associated with poorer prognostic outcomes for OSCC [149] and are involved in bone invasion [150].
Senescent cells (which are more prevalent in older individuals, same as cancer) also contribute to chronic inflammation. When cells senesce, they develop an inflammatory secretory phenotype known as the senescent-associated secretory phenotype (SASP) [151], characterized by the secretion of high levels of “pro-oncogenic cytokines,” such as IL-1, IL-6, and IL-8 [152]. In fact, the SASP is currently recognized as a cancer promoter mechanism, as it can induce EMT, invasion, and metastasis [151, 153], and its regulation has been proposed as anti-cancer treatment [154, 155].
Due to the advantages of using saliva samples (non-invasive and cost-efficient) for diagnostic and disease screening purposes, different studies have explored the possibility of using salivary inflammatory factors as biomarkers for the development and progression of OSCC. The most studied inflammatory proteins are TNF-α [5, 14, 42, 141, 156–159], IL-1 [5, 14, 141, 160, 161], IL-6 [5, 14, 34, 42, 92, 141, 158, 159, 162–164], and IL-8 [2, 5, 14, 42, 141, 160, 161, 164] (NF-κB-dependent cytokines), which have been found to be increased in the saliva of patients with different OPMDs (including OLP, oral leukoplakia, verrucous proliferative leucoplakia, and oral submucous fibrosis) and OSCC in comparison to healthy controls. Other cytokines, such as MIP-1β and IFNγ [14], and the anti-inflammatory cytokines IL-10 and IL-13 [24] have also been found to be increased in the saliva of patients with OSCC.
Using an array that analyzed the expression of 50 cytokines present in the saliva of patients with stage I OSCC before and after surgical treatment, Kamatani et al. [101] showed a significant decrease in salivary IL-1β after surgical resection. Similar to this, higher salivary levels of IL-8, IL-6, IL-1β, MIP-1β, and IP-10 before surgical intervention in patients with stage I OSCC were recently reported [165]. These results suggest that salivary inflammatory cytokines might be useful to monitor disease relapse.
A proteomic analysis of 60 saliva samples from healthy individuals and patients with OPMD and OSCC detected 21 proteins differentially expressed in OSCC compared to those in the other groups. Among those, three proteins were selected for further validation using ELISA, which included the interleukin-1 receptor antagonist (IL-1RA). Salivary IL-1RA was significantly decreased in patients with OPMD and control individuals compared to that in patients with OSCC but, alone, was suboptimal for distinguishing patients with OPMDs and healthy controls from patients with OSCC. In combination with other biomarkers (SLC3A2 and S100A2), IL-1RA was able to distinguish patients with OSCC from both healthy individuals and patients with OPMD with a sensitivity and specificity of 83.33/83.33% and of 93.33/70%, respectively [21]. Salivary IL-1β and IL-8 have also been found to discriminate between healthy individuals and patients with OSCC [160, 166] and high sensitivity and specificity values have been reported (86/97% for IL-8 and 83/76% for IL-1β) [166, 167]. Nevertheless, a recent systematic review reported average sensitivity and specificity values of 41/69% for IL-8 and of 26/46% for IL-1β [94], which are suboptimal. Both cytokines performed better when used in combination with other markers [161, 166], so it is likely that their future use will be as part of a panel of salivary biomarkers, rather than as single markers.
IL-6 is also a promising biomarker for the development of OSCC. IL-6 salivary levels are reported to increase with the severity of oral dysplasia [34], to differentiate between OPMD and OSCC (sensitivity and specificity values of 96 and 99%, respectively) [163], and to predict treatment outcomes in patients with OSCC [11, 97]. High salivary expression of TNF-α, IL-1α, and IL-8 has also been associated with a decreased survival rate in tongue squamous cell carcinoma (TSCC) [11].
The understanding of the role and origin of the different inflammatory molecules involved during tumor initiation, promotion, and progression of oral cancers provides an opportunity to target inflammation to improve patient outcomes. This can be done by selectively targeting transcription pathways (e.g., NF-κB), cytokines (e.g., IL-1), or cell types known to contribute to the inflammatory secretome (e.g., CAFs and senescent cells). There are several research lines in this field, but little has been translated into the clinics, especially with regard to OSCC. Although all of the aforementioned reports are pointing in the direction that salivary cytokines could be used for diagnostic and prognostic aims in patients with oral cancer, more prospective studies are needed before they could be used in clinical settings.
SN performed the review and wrote the manuscript.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Voronov E, Dinarello CA, and Apte RN. Interleukin-1alpha as an intracellular alarmin in cancer biology. Semin Immunol. (2018) 38:3–14. doi: 10.1016/j.smim.2018.10.006
2. Portier M, Zhang XG, Ursule E, Lees D, Jourdan M, Bataille R, et al. Cytokine gene expression in human multiple myeloma. Br J Haematol. (1993) 85:514–20. doi: 10.1111/j.1365-2141.1993.tb03341.x
3. Kuper H, Adami HO, and Trichopoulos D. Infections as a major preventable cause of human cancer. J Intern Med. (2000) 248:171–83. doi: 10.1046/j.1365-2796.2000.00742.x
4. Apte RN, Dotan S, Elkabets M, White MR, Reich E, Carmi Y, et al. The involvement of IL-1 in tumorigenesis, tumor invasiveness, metastasis, and tumor-host interactions. Cancer Metastasis Rev. (2006) 25:387–408. doi: 10.1007/s10555-006-9004-4
5. Goertzen C, Mahdi H, Laliberte C, Meirson T, Eymael D, Gil-Henn H, et al. Oral inflammation promotes oral squamous cell carcinoma invasion. Oncotarget. (2018) 9:29047–63. doi: 10.18632/oncotarget.25540
6. Rao SK, Pavicevic Z, Du Z, Kim JG, Fan M, Jiao Y, et al. Pro-inflammatory genes as biomarkers and therapeutic targets in oral squamous cell carcinoma. J Biol Chem. (2010) 285:32512–21. doi: 10.1074/jbc.M110.150490
7. Wu T, Hong Y, Jia L, Wu J, Xia J, Wang J, et al. Modulation of IL-1beta reprogrammes the tumor microenvironment to interrupt oral carcinogenesis. Sci Rep. (2016) 6:20208. doi: 10.1038/srep20208
8. Speight PM, Khurram SA, and Kujan O. Oral potentially malignant disorders: risk of progression to malignancy. Oral Surg Oral Med Oral Pathol Oral Radiol. (2018) 125:612–27. doi: 10.1016/j.oooo.2017.12.011
9. Lee CH, Chang JS, Syu SH, Wong TS, Chan JY, Tang YC, et al. IL-1beta promotes malignant transformation and tumor aggressiveness in oral cancer. J Cell Physiol. (2015) 230:875–84. doi: 10.1002/jcp.24816
10. Leon X, Bothe C, Garcia J, Parreno M, Alcolea S, Quer M, et al. Expression of IL-1alpha correlates with distant metastasis in patients with head and neck squamous cell carcinoma. Oncotarget. (2015) 6:37398–409. doi: 10.18632/oncotarget.6054
11. Korostoff A, Reder L, Masood R, and Sinha UK. The role of salivary cytokine biomarkers in tongue cancer invasion and mortality. Oral Oncol. (2011) 47:282–7. doi: 10.1016/j.oraloncology.2011.02.006
12. Bates AM, Gomez Hernandez MP, Lanzel EA, Qian F, and Brogden KA. Matrix metalloproteinase (MMP) and immunosuppressive biomarker profiles of seven head and neck squamous cell carcinoma (HNSCC) cell lines. Transl Cancer Res. (2018) 7:533–42. doi: 10.21037/tcr.2018.05.09
13. Sun Y, Zhu D, Wang G, Wang D, Zhou H, Liu X, et al. Pro-inflammatory cytokine IL-1β up-regulates CXC chemokine receptor 4 via notch and ERK signaling pathways in tongue squamous cell carcinoma. PLoS ONE. (2015) 10:e0132677. doi: 10.1371/journal.pone.0132677
14. Lee LT, Wong YK, Hsiao HY, Wang YW, Chan MY, and Chang KW. Evaluation of saliva and plasma cytokine biomarkers in patients with oral squamous cell carcinoma. Int J Oral Maxillofac Surg. (2018) 47:699–707. doi: 10.1016/j.ijom.2017.09.016
15. Cohen RF, Contrino J, Spiro JD, Mann EA, Chen LL, and Kreutzer DL. Interleukin-8 expression by head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. (1995) 121:202–9. doi: 10.1001/archotol.1995.01890020064013
16. Glogauer JE, Sun CX, Bradley G, and Magalhaes MA. Neutrophils increase oral squamous cell carcinoma invasion through an invadopodia-dependent pathway. Cancer Immunol Res. (2015) 3:1218–26. doi: 10.1158/2326-6066.CIR-15-0017
17. Lu SL, Reh D, Li AG, Woods J, Corless CL, Kulesz-Martin M, et al. Overexpression of transforming growth factor beta1 in head and neck epithelia results in inflammation, angiogenesis, and epithelial hyperproliferation. Cancer Res. (2004) 64:4405–10. doi: 10.1158/0008-5472.CAN-04-1032
18. Gonçalves AS, Mosconi C, Jaeger F, Wastowski IJ, Aguiar MCF, Silva TA, et al. Overexpression of immunomodulatory mediators in oral precancerous lesions. Hum Immunol. (2017) 78:752–7. doi: 10.1016/j.humimm.2017.09.003
19. Lu Z, Ding L, Ding H, Hao F, Pu Y, Wang Y, et al. Tumor cell-derived TGF-β at tumor center independently predicts recurrence and poor survival in oral squamous cell carcinoma. J Oral Pathol Med. (2019) 48:696–704. doi: 10.1111/jop.12888
20. Shiiba M, Saito K, Yamagami H, Nakashima D, Higo M, Kasamatsu A, et al. Interleukin-1 receptor antagonist (IL1RN) is associated with suppression of early carcinogenic events in human oral malignancies. Int J Oncol. (2015) 46:1978–84. doi: 10.3892/ijo.2015.2917
21. Shan J, Sun Z, Yang J, Xu J, Shi W, Wu Y, et al. Discovery and preclinical validation of proteomic biomarkers in saliva for early detection of oral squamous cell carcinomas. Oral Dis. (2019) 25:97–107. doi: 10.1111/odi.12971
22. Manchanda P, Sharma SC, and Das SN. Differential regulation of IL-2 and IL-4 in patients with tobacco-related oral squamous cell carcinoma. Oral Dis. (2006) 12:455–62. doi: 10.1111/j.1601-0825.2005.01220.x
23. Beppu M, Ikebe T, and Shirasuna K. The inhibitory effects of immunosuppressive factors, dexamethasone and interleukin-4, on NF-kappaB-mediated protease production by oral cancer. Biochim Biophys Acta. (2002) 1586:11–22. doi: 10.1016/S0925-4439(01)00080-1
24. Aziz S, Ahmed SS, Ali A, Khan FA, Zulfiqar G, Iqbal J, et al. Salivary immunosuppressive cytokines IL-10 and IL-13 are significantly elevated in oral squamous cell carcinoma patients. Cancer Invest. (2015) 33:318–28. doi: 10.3109/07357907.2015.1041642
25. Alhamarneh O, Agada F, Madden L, Stafford N, and Greenman J. Serum IL10 and circulating CD4(+) CD25(high) regulatory T cell numbers as predictors of clinical outcome and survival in patients with head and neck squamous cell carcinoma. Head Neck. (2011) 33:415–23. doi: 10.1002/hed.21464
26. Arantes DA, Costa NL, Mendonça EF, Silva TA, and Batista AC. Overexpression of immunosuppressive cytokines is associated with poorer clinical stage of oral squamous cell carcinoma. Arch Oral Biol. (2016) 61:28–35. doi: 10.1016/j.archoralbio.2015.10.013
27. Adappa ND, Sung CK, Choi B, Huang TG, Genden EM, and Shin EJ. The administration of IL-12/GM-CSF and Ig-4-1BB ligand markedly decreases murine floor of mouth squamous cell cancer. Otolaryngol Head Neck Surg. (2008) 139:442–8. doi: 10.1016/j.otohns.2008.05.001
28. Tian S, Jiang C, Liu X, Xu S, Zhang Z, Chen H, et al. Hypermethylation of IFN-γ in oral cancer tissues. Clin Oral Investig. (2017) 21:2535–42. doi: 10.1007/s00784-017-2052-z
29. Peng X, Li W, Johnson WD, Torres KE, and McCormick DL. Overexpression of lipocalins and pro-inflammatory chemokines and altered methylation of PTGS2 and APC2 in oral squamous cell carcinomas induced in rats by 4-nitroquinoline-1-oxide. PLoS ONE. (2015) 10:e0116285. doi: 10.1371/journal.pone.0116285
30. Lee CH, Syu SH, Liu KJ, Chu PY, Yang WC, Lin P, et al. Interleukin-1 beta transactivates epidermal growth factor receptor via the CXCL1-CXCR2 axis in oral cancer. Oncotarget. (2015) 6:38866–80. doi: 10.18632/oncotarget.5640
31. Prasad G, and McCullough M. Chemokines and cytokines as salivary biomarkers for the early diagnosis of oral cancer. Int J Dent. (2013) 2013:813756. doi: 10.1155/2013/813756
32. Lien MY, Lin CW, Tsai HC, Chen YT, Tsai MH, Hua CH, et al. Impact of CCL4 gene polymorphisms and environmental factors on oral cancer development and clinical characteristics. Oncotarget. (2017) 8:31424–34. doi: 10.18632/oncotarget.15615
33. Bae JY, Kim EK, Yang DH, Zhang X, Park YJ, Lee DY, et al. Reciprocal interaction between carcinoma-associated fibroblasts and squamous carcinoma cells through interleukin-1alpha induces cancer progression. Neoplasia. (2014) 16:928–38. doi: 10.1016/j.neo.2014.09.003
34. Sharma M, Bairy I, Pai K, Satyamoorthy K, Prasad S, Berkovitz B, et al. Salivary IL-6 levels in oral leukoplakia with dysplasia and its clinical relevance to tobacco habits and periodontitis. Clin Oral Investig. (2011) 15:705–14. doi: 10.1007/s00784-010-0435-5
35. Abdullah Zubir AZ, Whawell SA, Wong TS, and Khurram SA. The chemokine lymphotactin and its recombinant variants in oral cancer cell regulation. Oral Dis. (2020) 26:1668–76. doi: 10.1111/odi.13500
36. Khurram SA, Bingle L, McCabe BM, Farthing PM, and Whawell SA. The chemokine receptors CXCR1 and CXCR2 regulate oral cancer cell behaviour. J Oral Pathol Med. (2014) 43:667–74. doi: 10.1111/jop.12191
37. Timmons SR, Nwankwo JO, and Domann FE. Acetaldehyde activates Jun/AP-1 expression and DNA binding activity in human oral keratinocytes. Oral Oncol. (2002) 38:281–90. doi: 10.1016/S1368-8375(01)00056-2
38. Alam M, Kashyap T, Pramanik KK, Singh AK, Nagini S, and Mishra R. The elevated activation of NFκB and AP-1 is correlated with differential regulation of Bcl-2 and associated with oral squamous cell carcinoma progression and resistance. Clin Oral Investig. (2017) 21:2721–31. doi: 10.1007/s00784-017-2074-6
39. Wolf JS, Chen Z, Dong G, Sunwoo JB, Bancroft CC, Capo DE, et al. IL (Interleukin)-1 promotes nuclear factor- B and AP-1-induced IL-8 expression, cell survival, and proliferation in head and neck squamous cell carcinomas. Clin Cancer Res. (2001) 7:1812–20.
40. Nakayama H, Ikebe T, Beppu M, and Shirasuna K. High expression levels of nuclear factor kappaB, IkappaB kinase alpha and Akt kinase in squamous cell carcinoma of the oral cavity. Cancer. (2001) 92:3037–44. doi: 10.1002/1097-0142(20011215)92:12<3037::AID-CNCR10171>3.0.CO;2-#
41. Tanaka T, Nakayama H, Yoshitake Y, Irie A, Nagata M, Kawahara K, et al. Selective inhibition of nuclear factor-κB by nuclear factor-κB essential modulator-binding domain peptide suppresses the metastasis of highly metastatic oral squamous cell carcinoma. Cancer Sci. (2012) 103:455–63. doi: 10.1111/j.1349-7006.2011.02174.x
42. Zhang Y, Lin M, Zhang S, Wang Z, Jiang L, Shen J, et al. NF-kappaB-dependent cytokines in saliva and serum from patients with oral lichen planus: a study in an ethnic Chinese population. Cytokine. (2008) 41:144–9. doi: 10.1016/j.cyto.2007.11.004
43. Liu YC, Ho HC, Lee MR, Lai KC, Yeh CM, Lin YM, et al. Early induction of cytokines/cytokine receptors and Cox2, and activation of NF-κB in 4-nitroquinoline 1-oxide-induced murine oral cancer model. Toxicol Appl Pharmacol. (2012) 262:107–16. doi: 10.1016/j.taap.2012.04.023
44. Shibata M, Kodani I, Osaki M, Araki K, Adachi H, Ryoke K, et al. Cyclo-oxygenase-1 and−2 expression in human oral mucosa, dysplasias and squamous cell carcinomas and their pathological significance. Oral Oncol. (2005) 41:304–12. doi: 10.1016/j.oraloncology.2004.09.009
45. Morita Y, Morita N, Hata K, Nakanishi M, Kimoto N, Omata T, et al. Cyclooxygenase-2 expression is associated with vascular endothelial growth factor-c and lymph node metastasis in human oral tongue cancer. Oral Surg Oral Med Oral Pathol Oral Radiol. (2014) 117:502–10. doi: 10.1016/j.oooo.2013.12.410
46. Yang SF, Chen MK, Hsieh YS, Chung TT, Hsieh YH, Lin CW, et al. Prostaglandin E2/EP1 signaling pathway enhances intercellular adhesion molecule 1 (ICAM-1) expression and cell motility in oral cancer cells. J Biol Chem. (2010) 285:29808–16. doi: 10.1074/jbc.M110.108183
47. Postler TS, and Ghosh S. Bridging the gap: a regulator of NF-κB linking inflammation and cancer. J Oral Biosci. (2015) 57:143–7. doi: 10.1016/j.job.2015.05.001
48. Jimi E, Kokabu S, Matsubara T, Nakatomi C, Matsuo K, and Watanabe S. NF-κB acts as a multifunctional modulator in bone invasion by oral squamous cell carcinoma. Oral Sci Int. (2016) 13:1–6. doi: 10.1016/S1348-8643(15)00038-5
49. Tampa M, Mitran MI, Mitran CI, Sarbu MI, Matei C, Nicolae I, et al. Mediators of inflammation - a potential source of biomarkers in oral squamous cell carcinoma. J Immunol Res. (2018) 2018:1061780. doi: 10.1155/2018/1061780
50. Garat C, and Arend WP. Intracellular IL-1Ra type 1 inhibits IL-1-induced IL-6 and IL-8 production in Caco-2 intestinal epithelial cells through inhibition of p38 mitogen-activated protein kinase and NF-kappaB pathways. Cytokine. (2003) 23:31–40. doi: 10.1016/S1043-4666(03)00182-0
51. Papa S, Bubici C, Zazzeroni F, Pham CG, Kuntzen C, Knabb JR, et al. The NF-kappaB-mediated control of the JNK cascade in the antagonism of programmed cell death in health and disease. Cell Death Differ. (2006) 13:712–29. doi: 10.1038/sj.cdd.4401865
52. Julien S, Puig I, Caretti E, Bonaventure J, Nelles L, van Roy F, et al. Activation of NF-kappaB by Akt upregulates snail expression and induces epithelium mesenchyme transition. Oncogene(2007) 26:7445–56. doi: 10.1038/sj.onc.1210546
53. Wu D, Wu P, Zhao L, Huang L, Zhang Z, Zhao S, et al. NF-κB expression and outcomes in solid tumors: a systematic review and meta-analysis. Medicine. (2015) 94:e1687. doi: 10.1097/MD.0000000000001687
54. Yang X, Cheng H, Chen J, Wang R, Saleh A, Si H, et al. Head and neck cancers promote an inflammatory transcriptome through coactivation of classic and alternative NF-κB pathways. Cancer Immunol Res. (2019) 7:1760–74. doi: 10.1158/2326-6066.CIR-18-0832
55. Zhang J, and Peng B. NF-kappaB promotes iNOS and VEGF expression in salivary gland adenoid cystic carcinoma cells and enhances endothelial cell motility in vitro. Cell Prolif . (2009) 42:150–61. doi: 10.1111/j.1365-2184.2009.00588.x
56. Ikebe T, Takeuchi H, Jimi E, Beppu M, Shinohara M, and Shirasuna K. Involvement of proteasomes in migration and matrix metalloproteinase-9 production of oral squamous cell carcinoma. Int J Cancer. (1998) 77:578–85. doi: 10.1002/(SICI)1097-0215(19980812)77:4<578::AID-IJC18>3.0.CO;2-2
57. Lin Z, Sun L, Chen W, Liu B, Wang Y, Fan S, et al. miR-639 regulates transforming growth factor beta-induced epithelial-mesenchymal transition in human tongue cancer cells by targeting FOXC1. Cancer Sci. (2014) 105:1288–98. doi: 10.1111/cas.12499
58. Wang Y, Lin Z, Sun L, Fan S, Huang Z, Zhang D, et al. Akt/Ezrin Tyr353/NF-κB pathway regulates EGF-induced EMT and metastasis in tongue squamous cell carcinoma. Br J Cancer. (2014) 110:695–705. doi: 10.1038/bjc.2013.770
59. Ma T, Zhao Z, Wang Z, Wang C, and Zhang L. MiR-940 inhibits migration and invasion of tongue squamous cell carcinoma via regulatingCXCR2/NF-κB system-mediated epithelial-mesenchymal transition. Naunyn Schmiedebergs Arch Pharmacol. (2019) 392:1359–69. doi: 10.1007/s00210-019-01671-w
60. Duffey DC, Chen Z, Dong G, Ondrey FG, Wolf JS, Brown K, et al. Expression of a dominant-negative mutant inhibitor-kappaBalpha of nuclear factor-kappaB in human head and neck squamous cell carcinoma inhibits survival, proinflammatory cytokine expression, and tumor growth in vivo. Cancer Res. (1999) 59:3468–74.
61. Shaulian E, and Karin M. AP-1 as a regulator of cell life and death. Nat Cell Biol. (2002) 4:E131–6. doi: 10.1038/ncb0502-e131
62. Fujioka S, Niu J, Schmidt C, Sclabas GM, Peng B, Uwagawa T, et al. NF-kappaB and AP-1 connection: mechanism of NF-kappaB-dependent regulation of AP-1 activity. Mol Cell Biol. (2004) 24:7806–19. doi: 10.1128/MCB.24.17.7806-7819.2004
63. Riabowol K, Schiff J, and Gilman MZ. Transcription factor AP-1 activity is required for initiation of DNA synthesis and is lost during cellular aging. Proc Natl Acad Sci U S A. (1992) 89:157–61. doi: 10.1073/pnas.89.1.157
64. Bunjobpol W, Dulloo I, Igarashi K, Concin N, Matsuo K, and Sabapathy K. Suppression of acetylpolyamine oxidase by selected AP-1 members regulates DNp73 abundance: mechanistic insights for overcoming DNp73-mediated resistance to chemotherapeutic drugs. Cell Death Differ. (2014) 21:1240–9. doi: 10.1038/cdd.2014.41
65. Werman A, Werman-Venkert R, White R, Lee JK, Werman B, Krelin Y, et al. The precursor form of IL-1alpha is an intracrine proinflammatory activator of transcription. Proc Natl Acad Sci USA. (2004) 101:2434–9. doi: 10.1073/pnas.0308705101
66. Scott KA, Moore RJ, Arnott CH, East N, Thompson RG, Scallon BJ, et al. An anti-tumor necrosis factor-alpha antibody inhibits the development of experimental skin tumors. Mol Cancer Ther. (2003) 2:445–51.
67. Zhang L, Jiao M, Wu K, Li L, Zhu G, Wang X, et al. TNF-α induced epithelial mesenchymal transition increases stemness properties in renal cell carcinoma cells. Int J Clin Exp Med. (2014) 7:4951–8.
68. Johnston DA, Dong B, and Hughes CC. TNF induction of jagged-1 in endothelial cells is NFkappaB-dependent. Gene. (2009) 435:36–44. doi: 10.1016/j.gene.2009.01.003
69. Balkwill F. Tumour necrosis factor and cancer. Nat Rev Cancer. (2009) 9:361–71. doi: 10.1038/nrc2628
70. Mozaffari HR, Ramezani M, Mahmoudiahmadabadi M, Omidpanah N, and Sadeghi M. Salivary and serum levels of tumor necrosis factor-alpha in oral lichen planus: a systematic review and meta-analysis study. Oral Surg Oral Med Oral Pathol Oral Radiol. (2017) 124:e183–9. doi: 10.1016/j.oooo.2017.06.117
71. Scheff NN, Ye Y, Bhattacharya A, MacRae J, Hickman DN, Sharma AK, et al. Tumor necrosis factor alpha secreted from oral squamous cell carcinoma contributes to cancer pain and associated inflammation. Pain. (2017) 158:2396–409. doi: 10.1097/j.pain.0000000000001044
72. Tang D, Tao D, Fang Y, Deng C, Xu Q, and Zhou J. TNF-alpha promotes invasion and metastasis via NF-Kappa B pathway in oral squamous cell carcinoma. Med Sci Monit Basic Res. (2017) 23:141–9. doi: 10.12659/MSMBR.903910
73. Ren ZH, Wu K, Yang R, Liu ZQ, and Cao W. Differential expression of matrix metalloproteinases and miRNAs in the metastasis of oral squamous cell carcinoma. BMC Oral Health. (2020) 20:24. doi: 10.1186/s12903-020-1013-0
74. de Vicente JC, Fresno MF, Villalain L, Vega JA, and Hernández Vallejo G. Expression and clinical significance of matrix metalloproteinase-2 and matrix metalloproteinase-9 in oral squamous cell carcinoma. Oral Oncol. (2005) 41:283–93. doi: 10.1016/j.oraloncology.2004.08.013
75. Jimenez L, Jayakar SK, Ow TJ, and Segall JE. Mechanisms of invasion in head and neck cancer. Arch Pathol Lab Med. (2015) 139:1334–48. doi: 10.5858/arpa.2014-0498-RA
76. Ricci S, Pinto F, Auletta A, Giordano A, Giovane A, Settembre G, et al. The enigmatic role of matrix metalloproteinases in epithelial-to-mesenchymal transition of oral squamous cell carcinoma: implications and nutraceutical aspects. J Cell Biochem. (2019) 120:6813–9. doi: 10.1002/jcb.26905
77. Horejs CM. Basement membrane fragments in the context of the epithelial-to-mesenchymal transition. Eur J Cell Biol. (2016) 95:427–40. doi: 10.1016/j.ejcb.2016.06.002
78. Chen IC, Chiang WF, Huang HH, Chen PF, Shen YY, and Chiang HC. Role of SIRT1 in regulation of epithelial-to-mesenchymal transition in oral squamous cell carcinoma metastasis. Mol Cancer. (2014) 13:254. doi: 10.1186/1476-4598-13-254
79. Zhang S, Wang B, Zhou X, Yue K, and Wang X. The experimental study of CXC subfamily receptor 4 modulating oral squamous cell carcinoma epithelial-mesenchymal transition to influence lymphatic metastasis in vitro. Zhonghua Kou Qiang Yi Xue Za Zhi. (2014) 49:171–6.
80. Epanchintsev A, Shyamsunder P, Verma RS, and Lyakhovich A. IL-6, IL-8, MMP-2, MMP-9 are overexpressed in Fanconi anemia cells through a NF-κB/TNF-α dependent mechanism. Mol Carcinog. (2015) 54:1686–99. doi: 10.1002/mc.22240
81. Tanaka T, Imamura T, Yoneda M, Irie A, Ogi H, Nagata M, et al. Enhancement of active MMP release and invasive activity of lymph node metastatic tongue cancer cells by elevated signaling via the TNF-α-TNFR1-NF-κB pathway and a possible involvement of angiopoietin-like 4 in lung metastasis. Int J Oncol. (2016) 49:1377–84. doi: 10.3892/ijo.2016.3653
82. Bates RC, and Mercurio AM. Tumor necrosis factor-alpha stimulates the epithelial-to-mesenchymal transition of human colonic organoids. Mol Biol Cell. (2003) 14:1790–800. doi: 10.1091/mbc.e02-09-0583
83. Kashyap T, Pramanik KK, Nath N, Mishra P, Singh AK, Nagini S, et al. Crosstalk between Raf-MEK-ERK and PI3K-Akt-GSK3β signaling networks promotes chemoresistance, invasion/migration and stemness via expression of CD44 variants (v4 and v6) in oral cancer. Oral Oncol. (2018) 86:234–43. doi: 10.1016/j.oraloncology.2018.09.028
84. Pai S, Bamodu OA, Lin YK, Lin CS, Chu PY, Chien MH, et al. CD47-SIRPα signaling induces epithelial-mesenchymal transition and cancer stemness and links to a poor prognosis in patients with oral squamous cell carcinoma. Cells. (2019) 8:1658. doi: 10.3390/cells8121658
85. Liu M, Gao X, and Liu CL. Increased expression of lncRNA FTH1P3 promotes oral squamous cell carcinoma cells migration and invasion by enhancing PI3K/Akt/GSK3b/ Wnt/β-catenin signaling. Eur Rev Med Pharmacol Sci. (2018) 22:8306–14. doi: 10.26355/eurrev_201812_16528
86. Wang H, Deng X, Zhang J, Ou Z, Mai J, Ding S, et al. Elevated expression of zinc finger protein 703 promotes cell proliferation and metastasis through PI3K/AKT/GSK-3β signalling in oral squamous cell carcinoma. Cell Physiol Biochem. (2017) 44:920–34. doi: 10.1159/000485360
87. Lai KC, Liu CJ, Lin TJ, Mar AC, Wang HH, Chen CW, et al. Blocking TNF-α inhibits angiogenesis and growth of IFIT2-depleted metastatic oral squamous cell carcinoma cells. Cancer Lett. (2016) 370:207–15. doi: 10.1016/j.canlet.2015.10.016
88. Coppe JP, Patil CK, Rodier F, Sun Y, Munoz DP, Goldstein J, et al. Senescence-associated secretory phenotypes reveal cell-nonautonomous functions of oncogenic RAS and the p53 tumor suppressor. PLoS Biol. (2008) 6:2853–68. doi: 10.1371/journal.pbio.0060301
89. Sparmann A, and Bar-Sagi D. Ras-induced interleukin-8 expression plays a critical role in tumor growth and angiogenesis. Cancer Cell. (2004) 6:447–58. doi: 10.1016/j.ccr.2004.09.028
90. Ancrile B, Lim KH, and Counter CM. Oncogenic ras-induced secretion of IL6 is required for tumorigenesis. Genes Dev. (2007) 21:1714–9. doi: 10.1101/gad.1549407
91. Loaiza N, and Demaria M. Cellular senescence and tumor promotion: is aging the key? Biochim Biophys Acta. (2016) 1865:155–67. doi: 10.1016/j.bbcan.2016.01.007
92. Panneer Selvam N, and Sadaksharam J. Salivary interleukin-6 in the detection of oral cancer and precancer. Asia Pac J Clin Oncol. (2015) 11:236–41. doi: 10.1111/ajco.12330
93. Dikova VR, Principe S, and Bagan JV. Salivary inflammatory proteins in patients with oral potentially malignant disorders. J Clin Exp Dent. (2019) 11:e659–64. doi: 10.4317/jced.55917
94. Gaba FI, Sheth CC, and Veses V. Salivary biomarkers and their efficacies as diagnostic tools for oral squamous cell carcinoma: systematic review and meta-analysis. J Oral Pathol Med. (2018) 1–9. doi: 10.1111/jop.12791. [Epub ahead of print].
95. Zhou J, Tang Z, Gao S, Li C, Feng Y, and Zhou X. Tumor-associated macrophages: recent insights and therapies. Front Oncol. (2020) 10:188. doi: 10.3389/fonc.2020.00188
96. Waugh DJ, and Wilson C. The interleukin-8 pathway in cancer. Clin Cancer Res. (2008) 14:6735–41. doi: 10.1158/1078-0432.CCR-07-4843
97. Tsai MS, Chen WC, Lu CH, and Chen MF. The prognosis of head and neck squamous cell carcinoma related to immunosuppressive tumor microenvironment regulated by IL-6 signaling. Oral Oncol. (2019) 91:47–55. doi: 10.1016/j.oraloncology.2019.02.027
98. Woods RV, Adler-Storthz K, Dayman GL, Francis GM, and Grimm EA. Interleukin-1 regulates interleukin-6 secretion in human oral squamous cell carcinoma in vitro: possible influence of p53 but not human papillomavirus E6/E. Cancer Res. (1998) 58:3142–9.
99. von Biberstein SE, Spiro JD, Lindquist R, Kreutzer DL. Interleukin-1 receptor antagonist in head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. (1996) 122:751–9. doi: 10.1001/archotol.1996.01890190047012
100. SahebJamee M, Eslami M, AtarbashiMoghadam F, and Sarafnejad A. Salivary concentration of TNFα, IL1α, IL6, and IL8 in oral squamous cell carcinoma. Med Oral Patol Oral Cir Bucal. (2008) 13:E292–5.
101. Kamatani T, Shiogama S, Yoshihama Y, Kondo S, Shirota T, and Shintani S. Interleukin-1 beta in unstimulated whole saliva is a potential biomarker for oral squamous cell carcinoma. Cytokine. (2013) 64:497–502. doi: 10.1016/j.cyto.2013.08.011
102. Stevenson FT, Turck J, Locksley RM, and Lovett DH. The N-terminal propiece of interleukin 1 is a transforming nuclear oncoprotein. Cell Biol. (1997) 94:508–13. doi: 10.1073/pnas.94.2.508
103. Lee CH, Wong TS, Chan JY, Lu SC, Lin P, Cheng AJ, et al. Epigenetic regulation of the X-linked tumour suppressors BEX1 and LDOC1 in oral squamous cell carcinoma. J Pathol. (2013) 230:298–309. doi: 10.1002/path.4173
104. Al-Sahaf S, Hunter KD, Bolt R, Ottewell PD, and Murdoch C. The IL-1/IL-1R axis induces greater fibroblast-derived chemokine release in human papillomavirus-negative compared to positive oropharyngeal cancer. Int J Cancer. (2019) 144:334–44. doi: 10.1002/ijc.31852
105. Banda NK, Guthridge C, Sheppard D, Cairns KS, Muggli M, Bech-Otschir D, et al. Intracellular IL-1 receptor antagonist type 1 inhibits IL-1-induced cytokine production in keratinocytes through binding to the third component of the COP9 signalosome. J Immunol. (2005) 174:3608–16. doi: 10.4049/jimmunol.174.6.3608
106. Hashemi Goradel N, Najafi M, Salehi E, Farhood B, and Mortezaee K. Cyclooxygenase-2 in cancer: a review. J Cell Physiol. (2019) 234:5683–99. doi: 10.1002/jcp.27411
107. Schellhorn M, Haustein M, Frank M, Linnebacher M, and Hinz B. Celecoxib increases lung cancer cell lysis by lymphokine-activated killer cells via upregulation of ICAM-1. Oncotarget. (2015) 6:39342–56. doi: 10.18632/oncotarget.5745
108. Chu TH, Chan HH, Kuo HM, Liu LF, Hu TH, Sun CK, et al. Celecoxib suppresses hepatoma stemness and progression by up-regulating PTEN. Oncotarget. (2014) 5:1475–90. doi: 10.18632/oncotarget.1745
109. Choi YH, Back KO, Kim HJ, Lee SY, and Kook KH. Pirfenidone attenuates IL-1β-induced COX-2 and PGE2 production in orbital fibroblasts through suppression of NF-κB activity. Exp Eye Res. (2013) 113:1–8. doi: 10.1016/j.exer.2013.05.001
110. Konstantinopoulos PA, Vandoros GP, Karamouzis MV, Gkermpesi M, Sotiropoulou-Bonikou G, and Papavassiliou AG. EGF-R is expressed and AP-1 and NF-kappaB are activated in stromal myofibroblasts surrounding colon adenocarcinomas paralleling expression of COX-2 and VEGF. Cell Oncol. (2007) 29:477–82. doi: 10.1155/2007/831416
111. Fang L, Chang HM, Cheng JC, Leung PC, and Sun YP. TGF-β1 induces COX-2 expression and PGE2 production in human granulosa cells through Smad signaling pathways. J Clin Endocrinol Metab. (2014) 99:E1217–26. doi: 10.1210/jc.2013-4100
112. Nakao S, Ogtata Y, Shimizu E, Yamazaki M, Furuyama S, and Sugiya H. Tumor necrosis factor alpha (TNF-alpha)-induced prostaglandin E2 release is mediated by the activation of cyclooxygenase-2 (COX-2) transcription via NFkappaB in human gingival fibroblasts. Mol Cell Biochem. (2002) 238:11–8. doi: 10.1023/A:1019927616000
113. Amirchaghmaghi M, Mohtasham N, and Mozaffari PM. Comparison of COX2 expression between oral squamous cell carcinoma, leukoplakia and normal mucosa. J Contemp Dent Pract. (2012) 13:205–9. doi: 10.5005/jp-journals-10024-1122
114. Chan G, Boyle JO, Yang EK, Zhang F, Sacks PG, Shah JP, et al. Cyclooxygenase-2 expression is up-regulated in squamous cell carcinoma of the head and neck. Cancer Res. (1999) 59:991–4.
115. Yang B, Jia L, Guo Q, Ren H, Hu Y, and Xie T. Clinicopathological and prognostic significance of cyclooxygenase-2 expression in head and neck cancer: a meta-analysis. Oncotarget. (2016) 7:47265–77. doi: 10.18632/oncotarget.10059
116. Sano Y, Kogashiwa Y, Araki R, Enoki Y, Ikeda T, Yoda T, et al. Correlation of inflammatory markers, survival, and COX2 expression in oral cancer and implications for prognosis. Otolaryngol Head Neck Surg. (2018) 158:667–76. doi: 10.1177/0194599817745284
117. Nasry WHS, Rodriguez-Lecompte JC, and Martin CK. Role of COX-2/PGE2 mediated inflammation in oral squamous cell carcinoma. Cancers. (2018) 10:348. doi: 10.3390/cancers10100348
118. Wang YH, Wu MW, Yang AK, Zhang WD, Sun J, Liu TR, et al. COX-2 gene increases tongue cancer cell proliferation and invasion through VEGF-C pathway. Med Oncol. (2011) 28(Suppl. 1):S360–6. doi: 10.1007/s12032-010-9737-3
119. Kono M, Watanabe M, Abukawa H, Hasegawa O, Satomi T, and Chikazu D. Cyclo-oxygenase-2 expression is associated with vascular endothelial growth factor C expression and lymph node metastasis in oral squamous cell carcinoma. J Oral Maxillofac Surg. (2013) 71:1694–702. doi: 10.1016/j.joms.2013.04.015
120. Shang ZJ, Li ZB, and Li JR. VEGF is up-regulated by hypoxic stimulation and related to tumour angiogenesis and severity of disease in oral squamous cell carcinoma: in vitro and in vivo studies. Int J Oral Maxillofac Surg. (2006) 35:533–8. doi: 10.1016/j.ijom.2005.09.006
121. Lee LT, Wong YK, Chan MY, Chang KW, Chen SC, Chang CT, et al. The correlation between HIF-1 alpha and VEGF in oral squamous cell carcinomas: expression patterns and quantitative immunohistochemical analysis. J Chin Med Assoc. (2018) 81:370–5. doi: 10.1016/j.jcma.2017.06.025
122. Pouysségur J, Dayan F, and Mazure NM. Hypoxia signalling in cancer and approaches to enforce tumour regression. Nature. (2006) 441:437–43. doi: 10.1038/nature04871
123. Zhu GQ, Tang YL, Li L, Zheng M, Jiang J, Li XY, et al. Hypoxia inducible factor 1α and hypoxia inducible factor 2α play distinct and functionally overlapping roles in oral squamous cell carcinoma. Clin Cancer Res. (2010) 16:4732–41. doi: 10.1158/1078-0432.CCR-10-1408
124. Aguilar-Cazares D, Chavez-Dominguez R, Carlos-Reyes A, Lopez-Camarillo C, Hernadez de la Cruz ON, and Lopez-Gonzalez JS. Contribution of angiogenesis to inflammation and cancer. Front Oncol. (2019) 9:1399. doi: 10.3389/fonc.2019.01399
125. Wu F, Weigel KJ, Zhou H, and Wang XJ. Paradoxical roles of TGF-β signaling in suppressing and promoting squamous cell carcinoma. Acta Biochim Biophys Sin. (2018) 50:98–105. doi: 10.1093/abbs/gmx127
126. Massagué J. TGFβ signalling in context. Nat Rev Mol Cell Biol. (2012) 13:616–30. doi: 10.1038/nrm3434
127. Taghavi N, Bagheri S, and Akbarzadeh A. Prognostic implication of CD57, CD16, and TGF-β expression in oral squamous cell carcinoma. J Oral Pathol Med. (2016) 45:58–62. doi: 10.1111/jop.12320
128. Takahashi H, Sakakura K, Kudo T, Toyoda M, Kaira K, Oyama T, et al. Cancer-associated fibroblasts promote an immunosuppressive microenvironment through the induction and accumulation of protumoral macrophages. Oncotarget. (2017) 8:8633–47. doi: 10.18632/oncotarget.14374
129. Walsh JE, and Young MR. TGF-beta regulation of focal adhesion proteins and motility of premalignant oral lesions via protein phosphatase 1. Anticancer Res. (2011) 31:3159–64.
130. Yoshimatsu Y, Wakabayashi I, Kimuro S, Takahashi N, Takahashi K, Kobayashi M, et al. TNF-α enhances TGF-β-induced endothelial-to-mesenchymal transition via TGF-β signal augmentation. Cancer Sci. (2020) 111:2385–99. doi: 10.1111/cas.14455
131. Ruff M, Leyme A, Le Cann F, Bonnier D, Le Seyec J, Chesnel F, et al. The disintegrin and metalloprotease ADAM12 is associated with TGF-β-induced epithelial to mesenchymal transition. PLoS ONE. (2015) 10:e0139179. doi: 10.1371/journal.pone.0139179
132. Terabe M, Park JM, and Berzofsky JA. Role of IL-13 in regulation of anti-tumor immunity and tumor growth. Cancer Immunol Immunother. (2004) 53:79–85. doi: 10.1007/s00262-003-0445-0
133. Lallemant B, Evrard A, Combescure C, Chapuis H, Chambon G, Raynal C, et al. Clinical relevance of nine transcriptional molecular markers for the diagnosis of head and neck squamous cell carcinoma in tissue and saliva rinse. BMC Cancer. (2009) 9:370. doi: 10.1186/1471-2407-9-370
134. Koike H, Uzawa K, Nakashima D, Shimada K, Kato Y, Higo M, et al. Identification of differentially expressed proteins in oral squamous cell carcinoma using a global proteomic approach. Int J Oncol. (2005) 27:59–67. doi: 10.3892/ijo.27.1.59
135. Sun Y, Liu N, Guan X, Wu H, Sun Z, and Zeng H. Immunosuppression Induced by Chronic Inflammation and the Progression to Oral Squamous Cell Carcinoma. Mediators Inflamm. (2016) 2016:5715719. doi: 10.1155/2016/5715719
136. Chen CJ, Sung WW, Su TC, Chen MK, Wu PR, Yeh KT, et al. High expression of interleukin 10 might predict poor prognosis in early stage oral squamous cell carcinoma patients. Clin Chim Acta. (2013) 415:25–30. doi: 10.1016/j.cca.2012.09.009
137. Fallon PG, Jolin HE, Smith P, Emson CL, Townsend MJ, Fallon R, et al. IL-4 induces characteristic Th2 responses even in the combined absence of IL-5, IL-9, and IL-13. Immunity. (2002) 17:7–17. doi: 10.1016/S1074-7613(02)00332-1
138. Terabe M, Matsui S, Noben-Trauth N, Chen H, Watson C, Donaldson DD, et al. NKT cell-mediated repression of tumor immunosurveillance by IL-13 and the IL-4R-STAT6 pathway. Nat Immunol. (2000) 1:515–20. doi: 10.1038/82771
139. D'Arcangelo E, Wu NC, Cadavid JL, and McGuigan AP. The life cycle of cancer-associated fibroblasts within the tumour stroma and its importance in disease outcome. Br J Cancer. (2020) 122:931–42. doi: 10.1038/s41416-019-0705-1
140. Puram SV, Tirosh I, Parikh AS, Patel AP, Yizhak K, Gillespie S, et al. Single-cell transcriptomic analysis of primary and metastatic tumor ecosystems in head and neck cancer. Cell. (2017) 171:1611–24.e1624. doi: 10.1016/j.cell.2017.10.044
141. Rhodus NL, Ho V, Miller CS, Myers S, and Ondrey F. NF-kappaB dependent cytokine levels in saliva of patients with oral preneoplastic lesions and oral squamous cell carcinoma. Cancer Detect Prev. (2005) 29:42–5. doi: 10.1016/j.cdp.2004.10.003
142. Haque A, Moriyama M, Kubota K, Ishiguro N, Sakamoto M, Chinju A, et al. CD206(+) tumor-associated macrophages promote proliferation and invasion in oral squamous cell carcinoma via EGF production. Sci Rep. (2019) 9:14611. doi: 10.1038/s41598-019-51149-1
143. Lee CH, Liu SY, Chou KC, Yeh CT, Shiah SG, Huang RY, et al. Tumor-associated macrophages promote oral cancer progression through activation of the Axl signaling pathway. Ann Surg Oncol. (2014) 21:1031–7. doi: 10.1245/s10434-013-3400-0
144. Hu Y, He MY, Zhu LF, Yang CC, Zhou ML, Wang Q, et al. Tumor-associated macrophages correlate with the clinicopathological features and poor outcomes via inducing epithelial to mesenchymal transition in oral squamous cell carcinoma. J Exp Clin Cancer Res. (2016) 35:12. doi: 10.1186/s13046-015-0281-z
145. Greten FR, and Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. (2019) 51:27–41. doi: 10.1016/j.immuni.2019.06.025
146. Michailidou EZ, Markopoulos AK, and Antoniades DZ. VEGF expression from human dysplastic or malignant oral epithelium may be related to mast cell density and the subsequent angiogenetic phenomena. Int J Oral Maxillofac Surg. (2012) 41:1467–73. doi: 10.1016/j.ijom.2011.12.038
147. López de Cicco R, Watson JC, Bassi DE, Litwin S, and Klein-Szanto AJ. Simultaneous expression of furin and vascular endothelial growth factor in human oral tongue squamous cell carcinoma progression. Clin Cancer Res. (2004) 10:4480–8. doi: 10.1158/1078-0432.CCR-03-0670
148. Prime SS, Cirillo N, Hassona Y, Lambert DW, Paterson IC, Mellone M, et al. Fibroblast activation and senescence in oral cancer. J Oral Pathol Med. (2017) 46:82–8. doi: 10.1111/jop.12456
149. Dourado MR, Guerra ENS, Salo T, Lambert DW, and Coletta RD. Prognostic value of the immunohistochemical detection of cancer-associated fibroblasts in oral cancer: a systematic review and meta-analysis. J Oral Pathol Med. (2018) 47:443–53. doi: 10.1111/jop.12623
150. Elmusrati AA, Pilborough AE, Khurram SA, and Lambert DW. Cancer-associated fibroblasts promote bone invasion in oral squamous cell carcinoma. Br J Cancer. (2017) 117:867–75. doi: 10.1038/bjc.2017.239
151. Davalos AR, Coppe JP, Campisi J, and Desprez PY. Senescent cells as a source of inflammatory factors for tumor progression. Cancer Metastasis Rev. (2010) 29:273–83. doi: 10.1007/s10555-010-9220-9
152. Niklander S, Bandaru D, Lambert DW, and Hunter KD. ROCK inhibition modulates the senescence-associated secretory phenotype (SASP) in oral keratinocytes. FEBS Open Bio. (2020) 10:2740–9. doi: 10.1002/2211-5463.13012
153. Faget DV, Ren Q, and Stewart SA. Unmasking senescence: context-dependent effects of SASP in cancer. Nat Rev Cancer. (2019) 19:439–53. doi: 10.1038/s41568-019-0156-2
154. Lau L, Porciuncula A, Yu A, Iwakura Y, and David G. Uncoupling the senescence-associated secretory phenotype from cell cycle exit via interleukin-1 inactivation unveils its protumorigenic role. Mol Cell Biol. (2019) 39:e00586. doi: 10.1128/MCB.00586-18
155. Velarde MC, Demaria M, and Campisi J. Senescent cells and their secretory phenotype as targets for cancer therapy. Interdiscip Top Gerontol. (2013) 38:17–27. doi: 10.1159/000343572
156. Pezelj-Ribaric S, Prso IB, Abram M, Glazar I, Brumini G, and Simunovic-Soskic M. Salivary levels of tumor necrosis factor-alpha in oral lichen planus. Mediators Inflamm. (2004) 13:131–3. doi: 10.1080/09629350410001688530
157. Ghallab NA, el-Wakeel N, and Shaker OG. Levels of salivary IFN-gamma, TNF-alfa, and TNF receptor-2 as prognostic markers in (erosive) oral lichen planus. Mediators Inflamm. (2010) 2010:847632. doi: 10.1155/2010/847632
158. Kaur J, and Jacobs R. Proinflammatory cytokine levels in oral lichen planus, oral leukoplakia, and oral submucous fibrosis. J Korean Assoc Oral Maxillofac Surg. (2015) 41:171–5. doi: 10.5125/jkaoms.2015.41.4.171
159. Juretić M, Cerović R, Belušić-Gobić M, Brekalo Pršo I, Kqiku L, Špalj S, et al. Salivary levels of TNF-α and IL-6 in patients with oral premalignant and malignant lesions. Folia Biol. (2013) 59:99–102.
160. Singh P, Verma JK, and Singh JK. Validation of salivary markers, IL-1β, IL-8 and Lgals3bp for detection of oral squamous cell carcinoma in an Indian population. Sci Rep. (2020) 10:7365. doi: 10.1038/s41598-020-64494-3
161. Li Y, St John MA, Zhou X, Kim Y, Sinha U, Jordan RC, et al. Salivary transcriptome diagnostics for oral cancer detection. Clin Cancer Res. (2004) 10:8442–50. doi: 10.1158/1078-0432.CCR-04-1167
162. Bagan L, Sáez GT, Tormos MC, Labaig-Rueda C, Murillo-Cortes J, and Bagan JV. Salivary and serum interleukin-6 levels in proliferative verrucous leukoplakia. Clin Oral Investig. (2016) 20:737–43. doi: 10.1007/s00784-015-1551-z
163. Dineshkumar T, Ashwini BK, Rameshkumar A, Rajashree P, Ramya R, and Rajkumar K. Salivary and serum interleukin-6 levels in oral premalignant disorders and squamous cell carcinoma: diagnostic value and clinicopathologic correlations. Asian Pac J Cancer Prev. (2016) 17:4899–906. doi: 10.22034/APJCP.2016.17.11.4899
164. Khyani IAM, Qureshi MA, Mirza T, Farooq MU. Detection of interleukins-6 and 8 in saliva as potential biomarkers of oral pre-malignant lesion and oral carcinoma: a breakthrough in salivary diagnostics in Pakistan. Pak J Pharm Sci. (2017) 30:817–23.
165. Val M, Sidoti Pinto GA, Manini L, Gandolfo S, and Pentenero M. Variations of salivary concentration of cytokines and chemokines in presence of oral squamous cell carcinoma. A case-crossover longitudinal prospective study. Cytokine. (2019) 120:62–5. doi: 10.1016/j.cyto.2019.04.009
166. Brinkmann O, Kastratovic DA, Dimitrijevic MV, Konstantinovic VS, Jelovac DB, Antic J, et al. Oral squamous cell carcinoma detection by salivary biomarkers in a Serbian population. Oral Oncol. (2011) 47:51–5. doi: 10.1016/j.oraloncology.2010.10.009
Keywords: oral cancer, inflammation, oral carcinogenesis, biomarker, OPMD
Citation: Niklander SE (2021) Inflammatory Mediators in Oral Cancer: Pathogenic Mechanisms and Diagnostic Potential. Front. Oral. Health 2:642238. doi: 10.3389/froh.2021.642238
Received: 15 December 2020; Accepted: 13 January 2021;
Published: 22 February 2021.
Edited by:
Ricardo D. Coletta, Campinas State University, BrazilReviewed by:
Rogelio González-González, Juárez University of the State of Durango, MexicoCopyright © 2021 Niklander. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sven E. Niklander, c3Zlbi5uaWtsYW5kZXJAdW5hYi5jbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.