
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Ophthalmol., 27 February 2025
Sec. Inflammatory Eye Diseases
Volume 5 - 2025 | https://doi.org/10.3389/fopht.2025.1491981
This article is part of the Research TopicAdvancements in Non-Infectious Uveitis: Emerging Therapies and Novel Drug Administration RouteView all 4 articles
 Otto M. Olivas-Vergara1*
Otto M. Olivas-Vergara1* Inés Hernanz2Pablo E. Borges-Deniz1
Inés Hernanz2Pablo E. Borges-Deniz1 Fredeswinda Romero-Bueno1
Fredeswinda Romero-Bueno1 Olga Sanchez-Pernaute1
Olga Sanchez-Pernaute1 Ester Carreño2
Ester Carreño2Background: Secukinumab is a monoclonal antibody that selectively neutralizes interleukin-17A and has shown efficacy in the treatment of psoriatic arthritis, psoriasis, and axial spondyloarthritis. Its use in non-anterior non-infectious uveitis is controversial, with evidence generally not supporting its effectiveness in these conditions. However, the role of secukinumab in anterior non-infectious uveitis remains unclear.
Methods: Case series. Five patients with biological therapy-refractory non-infectious anterior uveitis who were treated with secukinumab were included.
Results: All 5 patients experienced a uveitis flare-up during treatment, and secukinumab failed to induce long-term remission in 2 of these patients, who also had uncontrolled systemic disease.
Conclusion: Secukinumab failed to prevent uveitis flare-up in these patients with biological therapy-refractory disease. Further studies are necessary to determine the potential role of secukinumab in the treatment of anterior uveitis.
Secukinumab is a fully human monoclonal antibody that binds to and neutralizes interleukin-17A (IL-17A) with high affinity. Its effectiveness has been established for the treatment of psoriatic arthritis (PsA), psoriasis, and radiographic axial spondyloarthritis (Ax-SpA) (1). Despite the fact that non-infectious uveitis shares the same cytokine pathway with these inflammatory diseases in terms of their immunopathogenesis (1, 2), clinical trials using subcutaneous doses of secukinumab for non-infectious non-anterior uveitis have not shown significant differences in clinical outcomes compared to placebo. This has been observed in three different clinical trials (SHIELD, INSURE, and ENDURE) (3). Although a small trial with a high intravenous dose of secukinumab has shown positive results, it has not yet been validated in a larger cohort (4).
On the other hand, the effectiveness of secukinumab has not been evaluated in randomized clinical trials for non-infectious anterior uveitis. To date, no monoclonal antibody has been approved specifically for isolated anterior uveitis, although there is evidence that adalimumab, when used for systemic indications, can help control flare-ups of anterior uveitis (5, 6). Long-term monitoring of patients treated with secukinumab, who were included in pivotal clinical trials for Ax-SpA and a Swedish national database, has shown a low incidence of anterior uveitis. However, this incidence is higher when compared to monoclonal tumor necrosis factor inhibitors (TNFi) (7, 8). In the absence of clinical trials, reports on the outcomes of secukinumab treatment for non-infectious anterior uveitis can assist clinicians in determining the potential usefulness of this monoclonal antibody for this indication. The aim of this study is to report the real-world experience of the use of secukinumab in anterior uveitis.
A retrospective review was conducted on the medical records of patients with anterior uveitis who were treated with secukinumab at Fundación Jiménez Díaz Hospital between 2017 and 2024. This study protocol was approved by the institutional review board of Fundacion Jimenez Diaz University Hospital (EOH018-20_FJD).
The decision of starting secukinumab was based in treating clinician’s criteria and the lack of response to conventional DMARDs (disease-modifying anti-rheumatic drugs) and at least one TNFi. Before starting secukinumab, there was not specific washout period. Secukinumab was started at the time of the next dose of the previous treatment. The patients with anterior uveitis were given secukinumab in the standard dose for PsA and Ax-SpA, which is 150mg subcutaneously every week for five weeks, followed by monthly maintenance dosing. If there was no clinical response based on the clinician’s criteria, the dose was increased to 300mg in accordance with the summary of product characteristics. Before administering the first dose of secukinumab, we followed national safety recommendations for the use of monoclonal antibodies and screened for active HIV, hepatitis B, hepatitis C, and tuberculosis (9).
For all patients, the following data were collected: age, gender, anatomical classification of the uveitis based on the criteria of the SUN working group (10), clinical phenotype, associated systemic disease, time from diagnosis to secukinumab treatment, previous treatment, treatment regimen at baseline, secukinumab dose, duration of treatment with secukinumab, and length of follow-up period. Systemic disease activity/control was based on treating-physician opinion.
The outcome measures of this study included the time to the first uveitis flare-up, time to the second uveitis flare-up, total number of uveitis flare-ups, and systemic disease control. The response to the treatment was evaluated on an individual basis. All the data collected were compiled into a database designed in Microsoft Excel 365 for retrospective analysis.
The SUN working group grading for anterior chamber inflammation (AC) was used (10). A flare-up of anterior uveitis was defined as the presence of at least 1+ AC cells in a previously quiet eye (≤0.5 + AC cells). All the anterior uveitis flare-ups were treated with a tapering regimen of topical dexamethasone or prednisolone acetate, starting with administration every 2 hours, as per local protocols. In case of macular edema associated to the anterior uveitis flare-up every 6 hours topical ketorolac (5mg/ml) was added to the topical steroids.
Five patients were identified (3 females and 2 male) with a mean age of 43 years (range 35-53 years) at the time of starting secukinumab treatment. The mean time of treatment duration after the first dose of secukinumab was 12.6 months (range 6-33 months).
All patients were diagnosed with non-infectious anterior uveitis and psoriasis or spondyloarthropathy-spectrum disease (PsA/Ax-SpA) as a systemic disease. Prior to receiving secukinumab, they had all been treated with at least one biologic DMARDs. Three out of 5 patients also used at least two conventional synthetic DMARDs previously. The decision to initiate secukinumab was based on active ocular or systemic disease and a lack of response or intolerance to biological therapy (TNFi or anti IL23, see Table 1). It is also noteworthy that Patient 1 was HIV positive and receiving antiretroviral therapy with an undetectable viral load and normal CD4 count. No other signs of advanced disease were detected during follow-up in this patient. We do not consider the anterior uveitis as infectious in this patient by its clinical characteristics (bilateral and non-hypertensive).
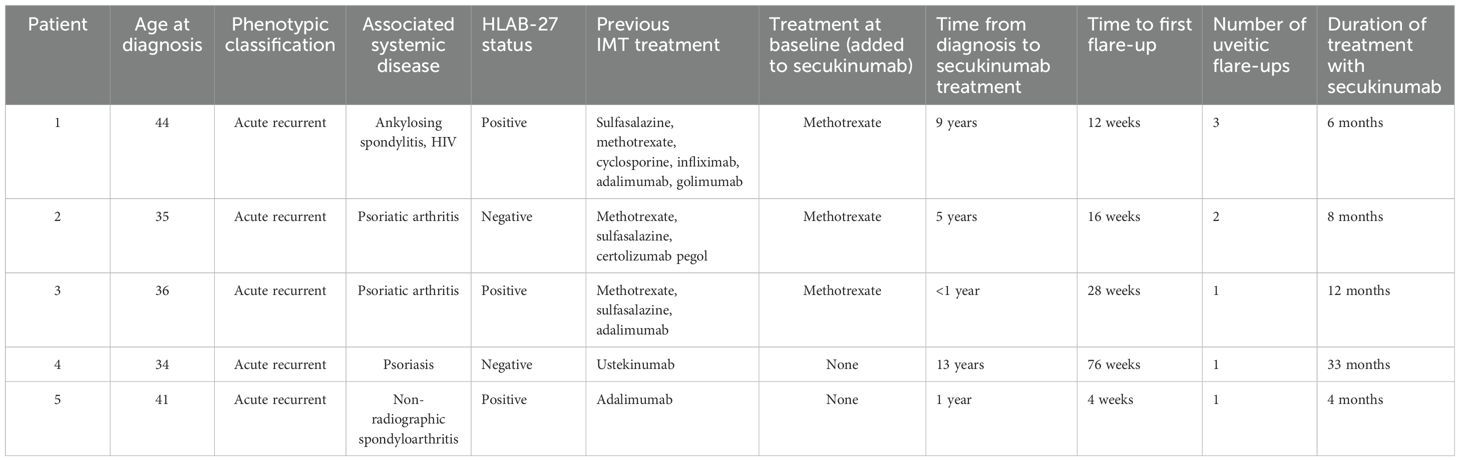
Table 1. Clinical characteristics and outcomes of patients with non-infectious anterior uveitis treated with secukinumab.
Patients 1, 2 and 5 had their secukinumab dose increased to 300mg after 3, 8 and 4 months of treatment, respectively. Patient 3, on the other hand, increased to the 300mg dose due to uncontrolled systemic disease prior to experiencing the first episode of anterior uveitis. Patient 4 started with a dose of 300mg because of severe plaque psoriasis.
Patient 1 experienced a flare-up of uveitis 12 weeks after starting treatment with the 150mg dose of secukinumab and had a total of three flare-ups during follow-up. Despite increasing the dose to 300mg and continuing concomitant methotrexate therapy, active arthritis persisted, prompting the addition of off-label tofacitinib after six months of secukinumab treatment.
Patient 2 had a longer time to first flare-up, at 16 weeks after starting the 150mg dose of secukinumab but had two flare-ups during follow-up. Despite increasing the dose to 300mg and continuing concomitant methotrexate therapy, active arthritis persisted, and the patient refused further changes in therapy, including intraarticular steroid injections.
Patient 3 was diagnosed of non-infectious anterior uveitis after 28 weeks of starting treatment with secukinumab, but not presented new flares during the follow-up. In the same way, patient 4 presented a flare after 76 weeks of treatment.
Patient 5 experienced a flare after 4 weeks of treatment and the dose was increased from 150mg to 300mg monthly, but until last visit she still continued with inflammatory back pain without new flares.
No adverse events were recorded during treatment in our patients.
In this study, the clinical response to secukinumab was evaluated in five patients with anterior non-infectious uveitis refractory to biological therapy. Despite receiving the maximum dose of 300mg per month, all five patients experienced uveitis flare-ups during treatment. Three of the patients also had a clinically uncontrolled systemic disease (PsA/Ax-SpA), and secukinumab failed to induce a long-lasting remission in these cases, even though there has not been a specific washout period for the previous biological therapy. The study’s findings are in line with previous clinical trials that evaluated the use of secukinumab for non-anterior uveitis and found it to be ineffective. We acknowledge that our study has several limitations: small sample, different systemic diseases, systemic disease control based on treating-physician opinion and not in a specific disease index, and lack of specific washout period. Despite these limitations, our study resembles a real-life scenario where there is no data from clinical trials.
The study by Miserocchi et al. showed a positive response to secukinumab in patients with HLA-B27 associated uveitis, which is a more homogeneous sample than the patients in our study (11). It is important to note that the patients in both studies were refractory to conventional immunosuppressors and TNFi, making them a difficult-to-treat subset. Additionally, the sample size was small. It is possible that refractory patients may benefit from intravenous administration of secukinumab, although this approach has not been tested in isolated non-infectious anterior uveitis and remains speculative.
The attempt to develop secukinumab for non-anterior uveitis parallels its unsuccessful trials in rheumatoid arthritis (RA). In RA, IL-17 is overexpressed in animal models and in patient samples, but clinical trials, including those that tested intravenous secukinumab, failed to show significant clinical benefit (12). This may be due to the highly variable expression of IL-17A, IL-17F, and their receptors among individual patients at the tissue level (13). Identifying patients who are more likely to respond to anti-IL 17 treatment based on tissular IL-17 expression may be possible, but it is not yet feasible in ophthalmological clinical practice due to the associated risk of obtaining intraocular samples.
A recent approved drug for axial spondyloarthritis, bimekizumab, a monoclonal antibody that selectively inhibits IL-17A and IL-17F, has showed a lower incidence rate of uveitis among patients randomized to this drug in a pooled analysis from phase 2b/3 trials (14). Although these results should be taken with caution because of the limitations of this study (low overall rate of events, short duration of treatment period, events not assessed by an ophthalmologist), this clinical data suggests that inhibition of IL-17A and IL-17F may be effective for the prevention of non-infectious anterior uveitis in this scenario (14).
In conclusion, secukinumab failed to prevent uveitis flare-up in these patients with biological therapy-refractory disease. Further research is needed to understand the role of IL-17 inhibitors in anterior and non-anterior uveitis.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Comite de Etica de la Investigación Fundación Jiménez Díaz. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because retrospective pseudoanonymized data.
OO-V: Writing – original draft, Writing – review & editing. IH: Conceptualization, Writing – review & editing. PB-D: Writing – review & editing. FR-B: Writing – review & editing. OS-P: Writing – review & editing. EC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. McGonagle DG, McInnes IB, Kirkham BW, Sherlock J, Moots R. The role of IL-17A in axial spondyloarthritis and psoriatic arthritis: recent advances and controversies. Ann Rheum Dis. (2019) 78:1167–78. doi: 10.1136/annrheumdis-2019-215356
2. Weinstein JE, Pepple KL. Cytokines in uveitis. Curr Opin Ophthalmol. (2018) 29:267–74. doi: 10.1097/ICU.0000000000000466
3. Dick AD, Tugal-Tutkun I, Foster S, Zierhut M, Melissa Liew SH, Bezlyak V, et al. Secukinumab in the treatment of noninfectious uveitis: results of three randomized, controlled clinical trials. Ophthalmology. (2013) 120:777–87. doi: 10.1016/j.ophtha.2012.09.040
4. Letko E, Yeh S, Foster CS, Pleyer U, Brigell M, Grosskreutz CL, et al. Efficacy and safety of intravenous secukinumab in noninfectious uveitis requiring steroid-sparing immunosuppressive therapy. Ophthalmology. (2015) 122:939–48. doi: 10.1016/j.ophtha.2014.12.033
5. Lie E, Lindström U, Zverkova-Sandström T, Olsen IC, Forsblad-d’Elia H, Askling J, et al. Tumour necrosis factor inhibitor treatment and occurrence of anterior uveitis in ankylosing spondylitis: results from the Swedish biologics register. Ann Rheum Dis. (2017) 76:1515–21. doi: 10.1136/annrheumdis-2016-210931
6. Fabiani C, Vitale A, Rigante D, Emmi G, Lopalco G, Sota J, et al. Efficacy of anti-tumour necrosis factor-α monoclonal antibodies in patients with non-infectious anterior uveitis. Clin Exp Rheumatol. (2019) 37:301–5.
7. Deodhar A, Miceli-Richard C, Baraliakos X, Marzo-Ortega H, Gladman DD, Martin R, et al. SAT0270 Low incidence of both new-onset and flares of uveitis in secukinumab-treated patients with ankylosing spondylitis: clinical trial and post-marketing safety analysis. Ann Rheumatic Dis. (2018) 77:999–. doi: 10.1136/annrheumdis-2018-eular.4474
8. Lindström U, Bengtsson K, Olofsson T, Di Giuseppe D, Glintborg B, Forsblad-d’Elia H, et al. Anterior uveitis in patients with spondyloarthritis treated with secukinumab or tumour necrosis factor inhibitors in routine care: does the choice of biological therapy matter? Ann Rheum Dis. (2021) 80:1445–52. doi: 10.1136/annrheumdis-2021-220420
9. Reino JG, Loza E, Andreu JL, Balsa A, Batlle E, Cañete JD, et al. Consenso SER sobre la gestión de riesgo del tratamiento con terapias biológicas en pacientes con enfermedades reumáticas. Reumatol Clín. (2011) 7:284–98. doi: 10.1016/j.reuma.2011.05.002
10. Jabs DA, Nussenblatt RB, Rosenbaum JT, Group SoUNSW. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. (2005) 140:509–16. doi: 10.1016/j.ajo.2005.03.057
11. Miserocchi E, Giuffre C, Caporali R, Favalli EG. Secukinumab in HLA-B27 associated uveitis. Clin Exp Ophthalmol. (2021) 49:388–9. doi: 10.1111/ceo.13922
12. Fragoulis GE, Siebert S, McInnes IB. Therapeutic targeting of IL-17 and IL-23 cytokines in immune-mediated diseases. Annu Rev Med. (2016) 67:337–53. doi: 10.1146/annurev-med-051914-021944
13. van Baarsen LG, Lebre MC, van der Coelen D, Aarrass S, Tang MW, Ramwadhdoebe TH, et al. Heterogeneous expression pattern of interleukin 17A (IL-17A), IL-17F and their receptors in synovium of rheumatoid arthritis, psoriatic arthritis and osteoarthritis: possible explanation for nonresponse to anti-IL-17 therapy? Arthritis Res Ther. (2014) 16:426. doi: 10.1186/s13075-014-0426-z
Keywords: secukinumab, anterior uveitis, uveitis, spondyloarthritis, psoriatic arthritis
Citation: Olivas-Vergara OM, Hernanz I, Borges-Deniz PE, Romero-Bueno F, Sanchez-Pernaute O and Carreño E (2025) Secukinumab in refractory non-infectious anterior uveitis. Front. Ophthalmol. 5:1491981. doi: 10.3389/fopht.2025.1491981
Received: 05 September 2024; Accepted: 06 February 2025;
Published: 27 February 2025.
Edited by:
Cheng-Rong Yu, National Eye Institute (NIH), United StatesReviewed by:
Smitha Jasper, Christian Medical College and Hospital, IndiaCopyright © 2025 Olivas-Vergara, Hernanz, Borges-Deniz, Romero-Bueno, Sanchez-Pernaute and Carreño. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Otto M. Olivas-Vergara, b3R0by5vbGl2YXNAcXVpcm9uc2FsdWQuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.