
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Ophthalmol. , 08 July 2024
Sec. Cornea and Refractive Surgery
Volume 4 - 2024 | https://doi.org/10.3389/fopht.2024.1408587
This article is part of the Research Topic Corneal diseases in children View all articles
 Anna M. Roszkowska1,2
Anna M. Roszkowska1,2 Rosaria Spinella3Alessandro Calderone1Marianna Sindoni1Bogumił H. Wowra4*Maciej Kozak2Katarzyna Sajak-Hydzik2
Rosaria Spinella3Alessandro Calderone1Marianna Sindoni1Bogumił H. Wowra4*Maciej Kozak2Katarzyna Sajak-Hydzik2 Jorge Aliò5
Jorge Aliò5Neurotrophic keratitis or keratopathy (NK) is a degenerative corneal disease induced by impairment of the trigeminal nerve function. This condition may lead to persistent epithelial defects, corneal ulceration, and perforation. The diagnosis of NK requires a careful investigation of any ocular and systemic condition associated with the disease and ocular surface and corneal sensitivity examinations. In the past, several medical and surgical procedures were used to treat this condition with different clinical effectiveness. Cenegermin is a recombinant human nerve growth factor (rh-NGF) that supports corneal reinnervation. Different clinical trials have demonstrated the safety and efficacy of topical cenegermin in patients with moderate to severe neurotrophic keratitis. In this review, we report the literature on clinical results regarding the treatment of NK with cenegermin since its approval by the European Medicines Agency (EMA) and the Food and Drug Administration (FDA) in 2017 and 2018, respectively.
The extremely rich corneal innervation originates from the ophthalmic branch of the trigeminal nerve and controls the maintenance of ocular surface homeostasis, ensuring proper functioning of the ocular surface unit and corneal transparency, mandatory for visual performance (1). This function is exerted by promoting the release of neurotrophic factors such as nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and neurotrophins 3 and 4 (NT-3 and NT-4) (2–6). NGF controls corneal healing and remodeling through the regulation of epithelial and stromal interaction (7, 8). A reduced level of NGF determines a nerve function impairment and altered corneal function with consequent visual loss (9, 10). Neurotrophic keratitis (NK) is a degenerative corneal disease resulting from severe impairment of the trigeminal nerve function, causing the deficiency of neural factors and the consequent loss of corneal tropism and impaired corneal healing (9). Nerve malfunction is the hallmark of NK, which manifests clinically in the early stage with epithelial defects that do not heal (10). Several factors have been identified as a possible cause of NK such as local or systemic diseases and surgeries, and traumatic, infective, and metabolic injuries affecting both the trigeminal and corneal nerves, with herpetic keratitis being the most frequently encountered (9, 11, 12). The disease may present with punctate epitheliopathy, persistent epithelial defects, corneal ulceration, and perforation and is accompanied by different grades of impaired corneal sensation (13). NK is classified as mild, involving only slight epithelial changes; moderate, with persisting epithelial defects (PEDs); and severe, with different grades of stromal involvement such as ulcer, corneal melting, and perforation (9, 13, 14). Recently, an additional classification based on Anterior Chamber Optical Coherence Tomography (AC-OCT) and in vivo confocal microscopy (IVCM) findings was proposed (15). The diagnosis of NK requires careful investigation of any ocular and systemic condition associated with corneal changes, and the testing of corneal sensitivity detecting hypoesthesia is considered as a main finding necessary to confirm diagnosis (13, 14). The therapy is challenging, and different therapeutic approaches, both medical and surgical, were adopted. In relation to NK severity, different therapies were used such as the therapeutic contact lens (CL), preservative-free artificial tears, topical autologous serum, Regenerating matrix agent (RGTA)—a matrix agent mimicking heparan sulfate, thyroxin beta-4, topical substance P, insulin-like GF1, amniotic membrane, conjunctival flap, tarsorrhaphy, and neurotization (16–18). Nevertheless, none of these therapeutic options provided satisfying results (14, 19, 20). Lambiase et al. demonstrated the effectiveness of murine NGF in promoting corneal healing and sensation recovery in patients with NK (21). Successively, the human recombinant NGF was used, and its efficacy in NK was demonstrated in the REPARO 1 and 2 studies (22, 23). The efficacy of rh-NGF was recently confirmed by Pflugfelder et al. in a multicenter randomized vehicle-controlled pivotal trial conducted in the United States (24). The rh-NGF 0.002% (cenegermin) was approved by the European Medicines Agency (EMA) in 2017 and the Food and Drug Administration (FDA) in 2018, and it actually represents the first-ever topical biologic drug for the first-line treatment of patients with NK stages 2 and 3 who do not respond to conventional treatment. In this review, we present the results of the clinical use of rh-NGF cenegermin (Oxervate; Dompé Farmaceutici SpA, Milan, Italy) in the treatment of moderate and severe NK.
The first recognizable alteration in the natural history of the pathology is the loss of corneal sensitivity. This factor generates a vicious cycle that induces and fuels the suffering of the cornea itself. The tear film is reduced in quantity and is unstable, the composition of its layers is altered, and the triggering stimulus mediates the production of proinflammatory cytokines and other harmful factors that change the homeostasis of the ocular surface and its ability to protect itself from external stimuli. The supply of growth factors and molecules useful to the limbal cells for the normal replacement of corneal cellular elements is greatly reduced, which remain senescent in the central portion of the cornea, thus worsening the quality of the eyelid redistribution mechanism. Inflammatory factors and aged dysfunctional cells accumulate, reducing the trophic and protective action of the tear film. As previously mentioned, the central lesion presents rolled borders consisting of elder cells that cannot link properly with their basal membrane, due to inflammation factors, mucin alterations, and the lack of proper tear film action. The chronicity of this process leads to the dysfunction of the intercellular junctions, worsening the corneal structural stability and inducing the risk of microbial overlap. The loss of stability of the tear film, the accumulation of inflammatory mediators, and the delay in the replacement of cellular elements establish the basis for the formation of the chronic epithelial defect. The stable epithelial defect leads to suffering of the stroma, exposed to the uncontrolled action of metalloproteinases, and therefore, to the possibility of melting and perforation, if the process is not promptly interrupted (25, 26).
The diagnostic moment for a presumed patient suffering from NK cannot ignore the evaluation of his clinical history and general anamnesis. The slit lamp biomicroscopic examination is accompanied by various tests that contribute to the formulation of a certain diagnosis and the recognition of the various etiological and developmental factors. The analysis of the symptomatic process reported by the patient must consider the possibility that the symptoms vary considerably during the natural history of the pathology. The severity of the symptoms often does not correspond precisely to the quantity and quality of the recognizable signs, and therefore, to the progress of the pathology.
The symptoms present in the early stages are mainly linked to alterations of the ocular surface and therefore mainly consist of dryness linked to changes in epithelial homeostasis. The patient may experience photophobia and worsening of visual quality especially in the morning, if subjected to trigger situations caused by air conditioning, the prolonged use of electronic devices, and staying in dry and heated environments. The symptoms may decrease as the patient’s clinical condition worsens due to the reduction in corneal sensitivity. However, as soon as the central portion of the cornea is significantly affected, the patient will complain of a sharp decline in visual quality. In the early phase, patients complain of dry eye symptoms detectable with a short break-up time, a narrowed tear meniscus, and often, a superficial punctate keratitis with epithelial irregularities; in particular, in post-refractive surgery patients, the epithelial defect is recognizable in the central portion of the cornea, gradually forming coalescing erosions due to the failure of tissue healing and turnover mechanisms. The repetition of the damage and healing phases over time leads to the development of a permanent epithelial defect with blunt edges and a weak bond with the underlying Bowman’s membrane, easily recognizable with fluorescein staining, which leaks under the epithelium. The underlying stroma is exposed to harmful inflammatory factors, and even if initially sterile, the lesion can develop a secondary infection and perforate. In this phase, evaluating the presence of signs of distress such as Descemet’s folds, corneal vascularization, and cellularity or signs of inflammation in AC is mandatory. The presence of accessory signs can help in recognizing the noxa that led to the development of the pathology; vice versa, classifying the patient by their anamnesis is useful to differentiate peculiar signs of the different presentations of the disease.
Underlying signs of pathologies, such as outcomes of uveitis or keratitis, dystrophies, or corneal scarring, can be differentiated by the signs that suggest a systemic condition.
Corneal sensitivity is assessed by estimating the response of the cornea to an external stimulus and comparing the reaction during stimulation of the two eyes. In patients with NK, the response to stimuli and blinking are significantly reduced, as confirmed by the Cochet–Bonnet esthesiometer.
As has been widely demonstrated, the latest generation of instruments in the possession of ophthalmologists is an obligatory step for the study and follow-up of patients suffering from the different corneal pathologies (27). AS-OCT is useful to study corneal thickness changes in stages 2–3 of NK and is used to measure the depth of corneal ulcerations and stromal thickness, facilitating the diagnosis and improving the follow-up analysis (27, 28).
Analysis of nerve fibers can be performed with IVCM that allows qualitative and quantitative assessment in terms of density, morphology, course, and dimensions of corneal nerves. It has recently been introduced in clinical examination to study the cornea at the cellular level (29). As the nerve’s examination permits the detection of early changes occurring in peripheral neuropathies, the IVCM becomes, over time, an important tool for their assessment and follow-up (29).
Typical NK alterations visible on confocal microscopy are a decrease in corneal subbasal nerve fiber number and density, increased tortuosity of corneal nerves, a decrease in corneal epithelial and endothelial cell density, and an increase in the number of hyper-reflective keratocytes. In NK, IVCM is an important instrument to help in the diagnosis and to find the etiology of the disease, thanks to the accurate qualitative and quantitative information about subbasal and stromal nerves.
Cenegermin is a recombinant form of human nerve growth factor (rh-NGF) produced in Escherichia coli; its molecule is identical to human NGF. A preclinical study on different doses of human rh-NGF eye drops demonstrated the good tolerability and safety of this drug. Clinical studies such as REPARO1 and 2 demonstrated the clinical efficacy and safety of human recombinant NGF (rh-NGF) at doses of 10 μg/mL and 20 μg/mL in promoting corneal healing in mild and severe NK with a clinically better outcome with the higher concentration formulation without changes in tolerability.
The rh-NGF cenegermin was approved by the FDA at a concentration of 0.002%; Oxervate™ (Dompé Farmaceutici SpA, Milan, Italy), which is an ophthalmic solution of rh-NGF, is the first-ever topical biologic drug approved in the field of ophthalmology and the first drug approved for treatment of NK (30).
It was demonstrated that the drug has high specificity for the anterior segment of the eye, playing an important role in supporting corneal healing and maintaining corneal integrity with the posology of one drop × six times/day × 8 weeks.
The studies and trials recorded so far have highlighted that most adults affected by moderate or severe NK experienced complete corneal healing after up to 8 weeks of topical cenegermin therapy (31).
In this review, we analyze the results of 15 studies presented in the literature database, reporting the clinical outcome of the therapy of NK with rh-NGF. Eight papers report results in adult patients and seven papers report results in a pediatric population.
Tables 1, 2 show the studies on adults and pediatric patients, respectively.
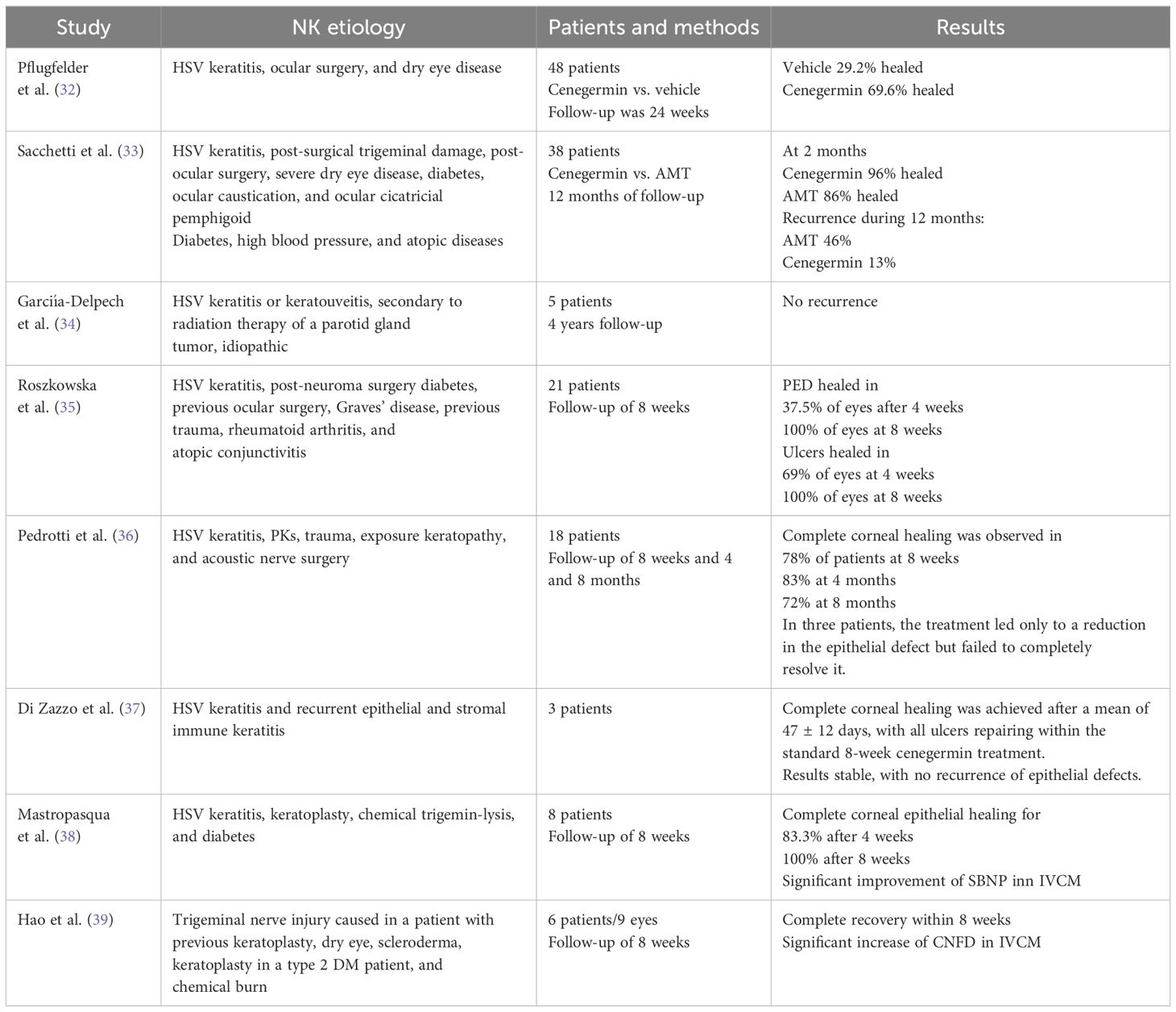
Table 1 Clinical outcomes in adult patients with NK treated with cenegermin.
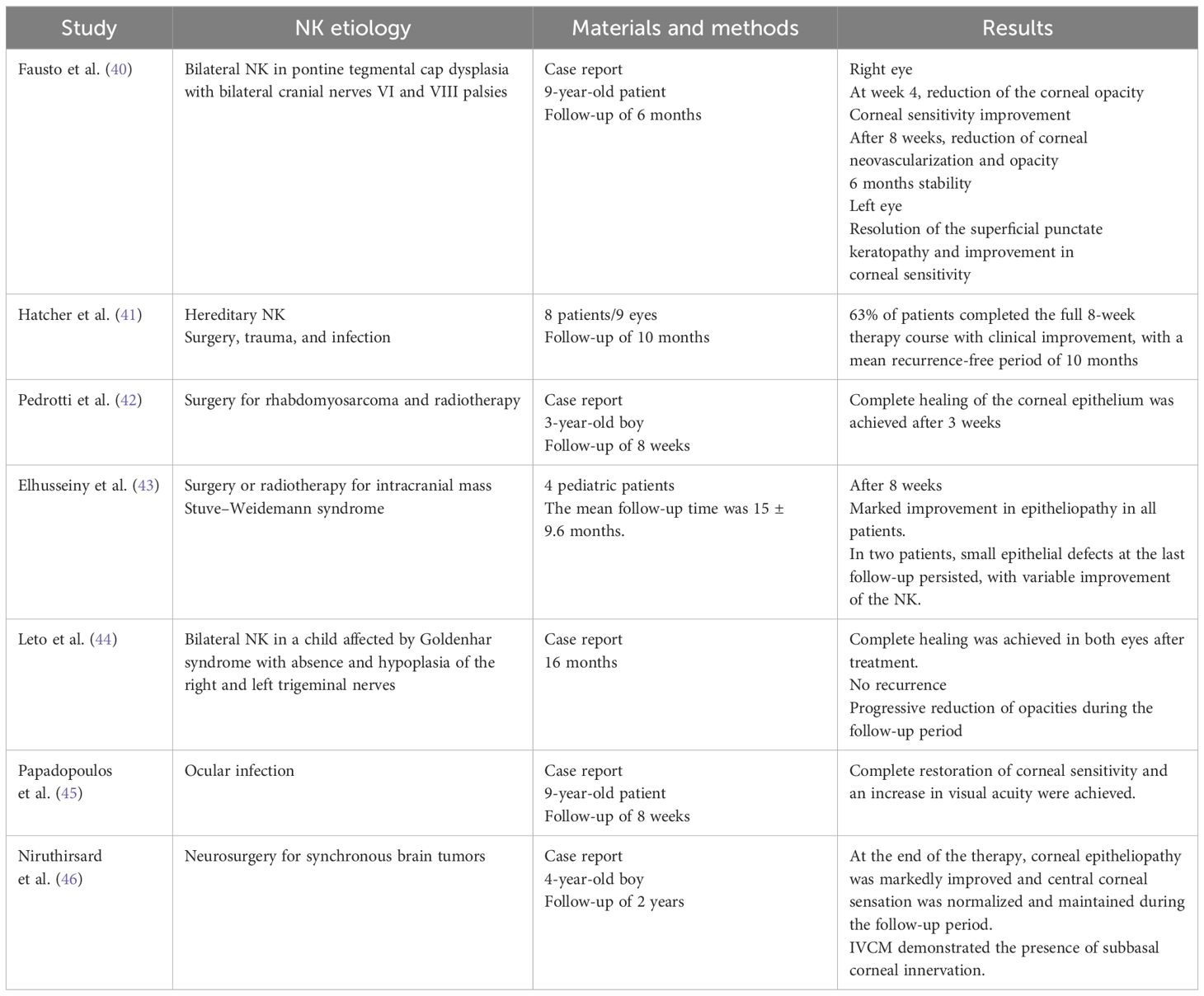
Table 2 Clinical outcomes in pediatric patients with NK treated with cenegermin.
A multicenter randomized double-masked study by Pflugferlder et al. on 48 patients with NK that compared cenegermin 0.002% to vehicle eye drops showed significantly higher healing rate in the rh-NGF group. The authors demonstrated that cenegermin-treated patients showed statistically significant reductions in lesion size and disease progression rates during masked treatment, and no severe adverse effects were experienced (32).
Sacchetti et al. compared the outcomes of 38 patients with NK treated with amniotic membrane transplantation (AMT) to those treated with cenegermin eye drops. At the end of treatment (2 months), a complete healing was observed in 86% of AMT-treated patients and in 96% of cenegermin-treated patients. During 12 months of follow-up, recurrence occurred in 46% of patients treated with AMT and in 13% of patients treated with cenegermin. The study confirmed the effectiveness of both AMT and cenegermin in stages 2 and 3 of NK; however, the last one was associated with minor frequency of recurrences and a high satisfaction of patients (33).
In a case series study, Garcia-Delpech et al. demonstrated the effectiveness of cenegermin eye drops in five adult patients affected by severe and moderate NK at stage 2 or 3 after showing poor results of the conventional therapy. Treatment was well tolerated by patients, and a complete corneal healing with a trend improvement in visual acuity (VA) and sensitivity was observed. In this study, during 4 years of follow-up, no recurrence of NK was observed (34).
Roszkowska et al. examined 21 patients affected by moderate and severe NK treated with cenegermin. Participants were evaluated at baseline and after 4 and 8 weeks of protocol therapy. In the moderate NK group at 4 weeks, PEDs healed in 37.5% of eyes, and at 8 weeks, a complete recovery was registered in 100% of eyes. In contrast, in the severe NK group, at 4 weeks of treatment, 69% of ulcers were closed, while at 8 weeks, 100% of eyes were completely healed.
This study showed that eyes affected by severe NK had better healing than eyes with moderate NK, but such finding needs to be further investigated (35).
Pedrotti et al. made an 8-month follow-up of NK that correlated with various systemic diseases (such as burns or acoustic nerve surgery with trigeminal damage) after treatment with cenegermin eye drops. Eighteen eyes of 18 patients were studied at baseline at 8 weeks (end of therapy) and at 2, 4, and 8 months after treatment (follow-up) (35). At 8 weeks in 78% of patients, complete healing was observed, and in 78%, 83%, and 72% of patients, respectively, at 2, 4, and 8 months of follow-up, resolution of signs and symptoms was observed (36).
Di Zazzo et al. studied three patients affected by NK stage 2 or stage 3 with a unilateral lesion not responding to classic medical therapies. Patients were evaluated at baseline, then weekly for 8 weeks and monthly thereafter. Complete corneal healing was achieved after a mean of 47 ± 12 days, with all ulcers repaired within the standard 8-week cenegermin treatment. The three eyes maintained a stable, healed corneal epithelium during the follow-up period with no recurrence of epithelial defects (37).
Mastropasqua et al. examined 18 patients affected by various NK etiologies who were treated with topical antibiotics, lubricants, and therapeutic CLs before enrolling in the study. After 4 weeks of cenegermin eye drops, 83.3% of patients showed complete corneal healing. The Schirmer I test showed a significant increase in tear film secretion after 8 weeks of treatment compared to baseline, and the Cochet–Bonnet esthesiometry demonstrated an increase in corneal sensation as compared to baseline. Additionally, the IVCM evaluation of the subbasal nerve fibers showed an increase in the diameter and number of nerve fibers as compared to the baseline values (38).
Hao et al. evaluated nine eyes of six patients with NK at stages 2–3 not responding to previous medical therapy. After 8 weeks of cenegermin treatment, there was a significant difference in corneal fluorescence staining scores, and the epithelial defects recovered completely. Based on confocal microscopy findings, the corneal subbasal nerve fiber density and number increased (39).
In a pediatric population, cenegermin was administrated in persistent visually threatening cases that did not respond to conventional treatments. In the literature, only two articles report a case series of four and eight patients, with the other articles being single case reports with severe underlying diseases.
Fausto et al. reported a case of a 9-year-old patient affected by a pontine tegmental cap dysplasia with bilateral cranial nerves VI and VIII palsies that caused a stage 2 NK in the right eye and a stage 1 NK in the left eye. Cenegermin was administered in both eyes according to the therapy protocol. At week 4, the corneal opacity of the right eye was reduced, and sensitivity was improved. At week 8, the corneal neovascularization was markedly reduced, and the epithelium seemed normal. Over the next 6 months, the opacity decreased in size and density and only a fine neovascularization remained. In the left eye, there was a complete resolution of the superficial punctate keratopathy and an improvement of sensitivity (40). Topical cenegermin was well tolerated and no side effects were reported.
Hatcher et al., in a retrospective case series on eight pediatric patients with acquired and hereditary NK, showed a clinical improvement of corneal defects and best-corrected visual acuity in five patients. These improvements persisted through the 10 months of follow-up. Side effects reported during therapy were ocular pain, difficulty sleeping, and persistent corneal thinning. Results of this study permitted us to understand that cenegermin gives a modest support for NK in the pediatric population and that the primary benefit was an improvement in corneal epithelial stability (41).
Pedrotti et al. reported the use of cenegermin in a 3-year-old child with NK after surgery for rhabdomyosarcoma of the jaw. A gradual improvement of corneal signs was noted after 2 weeks, and on the third week, the corneal epithelium was reestablished (42).
Elhusseiny et al. evaluated the efficacy of cenegermin drops in a retrospective study on four pediatric patients after failure of the classic medical therapy. In all cases, at the end of treatment, a marked improvement of the epitheliopathy was demonstrated with a general improvement of corneal signs and symptoms (43).
Leto et al. evaluated a bilateral NK in a pediatric patient with Goldenhar syndrome associated with hypoplasia of both trigeminal nerves. After 8 weeks of therapy, a complete healing in both eyes was achieved, and during the 16 months of follow-up, no complications or regression of the disease was detected, whereas corneal opacity became clearer, and there was no significant improvement of corneal sensation (44).
Papadopoulos et al. showed a complete restoration of the corneal surface and an increase in visual acuity after cenegermin administration in a 9-year-old child with NK refractory to usual therapy (45).
Niruthisard et al. reported a case of a 4-year-old child affected by severe NK, lagophthalmos, and facial palsy following neurosurgery for synchronous brain tumors initially treated with topical antibiotics, topical steroids, artificial tears, and lateral tarsorrhaphy with a transient result. After cenegermin treatment, the central corneal sensitivity recovered and the corneal epitheliopathy was significantly improved with a positive outcome lasting for 2 years after therapy (46).
NK is a sight-threatening condition due to the pathology of the trigeminal nerve and its ophthalmic branch terminations. Corneal alterations characterize the moderate and severe forms with significant reduction of the corneal sensation and loss of corneal trophism. Cenegermin is the first topical biologic drug for first-line treatment in patients with NK stages 2 and 3. The data presented in the literature demonstrate the clinical efficacy and safety of the treatment. Correct indications and prompt treatment with rh-NGF promote healing of persistent epithelial defects and induce healing of ulcers and recovery of the corneal sensitivity. The restoration of the corneal thickness and the healing of PED and ulcers after the treatment of rh-NGF confirm the crucial role of NGF in promoting the release of factors involved in the maintenance of the integrity of the corneal epithelium and ocular surface hemostasis. The overall reported results might consider the use of cenegermin eye drops in all cases of severe and moderate NK if the conventional therapy proved to be ineffective. In addition, unlike surgical treatments, cenegermin did not cause relevant side effects, thus having no impact on the patient’s quality of life.
The analyzed studies show the safety and prolonged effect of cenegermin in the treatment of both adult and pediatric NK with recovery in almost all patients. Nevertheless, the efficacy of the treatment and its stability have been proven in pediatric cases; such data need further investigation using prospective, randomized clinical trials with standardization of evaluation procedures and assessment on corneal sensitivity and IVCM.
The high cost of the drug and the need for cold chain storage and delivery limit its wide use.
AR: Conceptualization, Writing – review & editing. RS: Writing – review & editing. AA: Writing – review & editing. MS: Writing – review & editing. BW: Formal analysis, Writing – review & editing. MK: Writing – review & editing. KS-H: Writing – review & editing. JA: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer IA declared a past co-authorship with the author JA to the handling editor.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Marfurt CF, Cox J, Deek S, Dvorscak L. Anatomy of the human corneal innervation. Exp Eye Res. (2010) 90:478–92. doi: 10.1016/j.exer.2009.12.010
2. Labetoulle M, Baudouin C, Calonge M, Merayo-Lloves J, Boboridis KG, Akova YA, et al. Role of corneal nerves in ocular surface homeostasis and disease. Acta Ophthalmol. (2019) 97:137–45. doi: 10.1111/aos.13844
3. Müller LJ, Marfurt CF, Kruse F, Tervo TM. Corneal nerves: struc- ture, contents and function. Exp Eye Res. (2003) 76:521–42. doi: 10.1016/s0014-4835(03)00050-2
4. Al-Aqaba MA, Anis FS, Mohammed I, Dua HS. Nerve terminals at the human corneoscleral limbus. Br J Ophthalmol. (2018) 102:556–61. doi: 10.1136/bjophthalmol-2017-311146
5. Shaheen BS, Bakir M and Jain S. Corneal nerves in health and disease. Surv Ophthalmol. (2014) 59:263–85. doi: 10.1016/j.survophthal.2013.09.002
6. You L, Kruse FE, Voülcker HE. Neurotrophic factors in the human cornea. Invest Ophthalmol Vis Sci. (2000) 41:692–702.10711683.
7. Chen L, Wei RH, Tan DT, Beuerman RW, Li W, Zhao S. Nerve growth factor expression and nerve regeneration in monkey corneas after LASIK. J Refract Surg. (2014) 30:134–9. doi: 10.3928/1081597X-20140120-10
8. Di G, Qi X, Zhao X, Zhang S, Danielson P, Zhou Q. Corneal epithelium-derived neurotrophic factors promote nerve regeneration. Invest Ophthalmol Vis Sci. (2017) 58:4695–702. doi: 10.1167/iovs.16-21372
9. Bonini S, Rama P, Olzi D, Lambiase A. Neurotrophic keratitis. Eye (Lond). (2003) 17:989–95. doi: 10.1038/sj.eye.6700616
10. Araki K, Ohashi Y, Kinoshita S, Hayashi K, Kuwayama Y, Tano Y. Epithelial wound healing in the denervated cornea. Curr Eye Res. (1994) 13:203–11. doi: 10.3109/02713689408995778
11. Semeraro F, Forbice E, Braga O, Bova A, Di Salvatore A, Azzolini C. Evaluation of the efficacy of 50% autologous serum eye drops in different ocular surface pathologies. BioMed Res Int. (2014) 2014:826970.25136628. doi: 10.1016/s0014-4835(03)00050-2
12. Meduri A, Oliverio GW, Valastro A, Azzaro C, Camellin U, FranChina F, et al. Neurotrophic keratopathy in systemic diseases: A case series on patients treated with rh-NGF. Front Med (Lausanne). (2022) 9:920688. doi: 10.3389/fmed.2022.920688
13. Dua HS, Said DG, Messmer EM, Rolando M, Benitez-Del-Castillo JM, Hossain PN, et al. Neurotrophic kerato- pathy. Prog Retin Eye Res. (2018) 66:107–31. doi: 10.1016/j.preteyeres.2018.04.003
14. Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. (2014) 8:571–579.24672223.
15. Mastropasqua L, Nubile M, Lanzini M, Calienno R, Dua HS. In vivo micro- scopic and optical coherence tomography classification of neurotrophic keratopathy. J Cell Physiol. (2019) 234:6108–6115. doi: 10.1002/jcp.27345
16. Donnerer J, Schuligoi R and Stein C. Increased content and transport of substance P and calcitonin gene-related peptide in sensory nerves innervating inflamed tissue: evidence for a regulatory function of nerve growth factor in vivo. Neuroscience. (1992) 49:693–8. doi: 10.1016/0306-4522(92)90237-V
17. Brown SM, Lamberts DW, Reid TW, Nishida T, Murphy CJ. Neurotrophic and anhidrotic keratopathy treated with substance P and insulin- like growth factor 1. Arch Ophthalmol. (1997) 115:926–7. doi: 10.1001/archopht.1997.01100160096021
18. Tripathi BJ, Kwait PS and Tripathi RC. Corneal growth factors: a new generation of ophthalmic pharmaceuticals. Cornea. (1990) 9:doi: 10.1097/00003226-199001000-00002
19. Di Zazzo A, Varacalli G, Mori T, Coassin M. Long-termrestoration of corneal sensitivity in neurotrophic keratopathy after rhNGF treatment. Eur J Ophthalmol. (2020) 27:1120672120953343. doi: 10.1177/1120672120953343
20. Versura P, Giannaccare G, Pellegrini M, Sebastiani S, Campos EC. Neurotrophic keratitis: current challenges and future prospects. Eye Brain. (2018) 10:37–45. doi: 10.2147/EB
21. Lambiase A, Rama P, Bonini S, Caprioglio G, Aloe L. Topical treatment with nerve growth factor for corneal neurotrophic ulcers. N Engl J Med. (1998) 338:1174–80. doi: 10.1056/NEJM199804233381702
22. Bonini S, Lambiase A, Rama P, Filatori I, Allegretti M, Chao W, et al. REPARO study group. Phase I trial recombinant Hum Nerve Growth factor neurotrophic keratitis. Ophthalmol. (2018) 125:1468–1471. doi: 10.1016/j.ophtha.2018.03.004
23. Bonini S, Lambiase A, Rama P, Sinigaglia F, Allegretti M, Chao W, et al. REPARO study group. Phase II randomized, double-masked, vehicle-controlled trial of recombinant human nerve growth factor for neurotrophic keratitis. Ophthalmology. (2018) 125:1332–43. doi: 10.1016/j.ophtha.2018.02.022
24. Pflugfelder SC, Massaro-Giordano M, Perez VL, Hamrah P, Deng SX, Espandar L, et al. Topical recombinant human nerve growth factor (Cenegermin) for neurotrophic keratopathy: a multicenter randomized vehicle-controlled pivotal trial. Ophthalmology. (2020) 127:14–26. doi: 10.1016/j.ophtha.2019.08.020
25. Pflugfelder SC, Farley W, Luo L, Chen LZ, de Paiva CS, Olmos LC, et al. Matrix metalloproteinase-9 knockout confers resistance to corneal epithelial barrier disruption in experimental dry eye. Am J Pathol. (2005) 166:61–71. doi: 10.1016/S0002-9440(10)62232-8
26. Chotikavanich S, de Paiva CS, Li de Q, Chen JJ, Bian F, Farley WJ, et al. Production and activity of matrix metalloproteinase-9 on the ocular surface increase in dysfunctional tear syndrome. Invest Ophthalmol Vis Sci. (2009) 50:3203–9. doi: 10.1167/iovs.08-2476
27. Inferrera L, Aragona E, Wylęgała A, Valastro A, Latino G, Postorino EI, et al. The role of hi-tech devices in assessment of corneal healing in patients with neurotrophic keratopathy. J Clin Med. (2022) 11:1602. doi: 10.3390/jcm11061602
28. Bonzano C, Olivari S, Cutolo CA, Macrì A, Sindaco D, Borroni D, et al. Recombinant human nerve growth factor (Cenegermin)-driven corneal wound healing process: an evidence-based analysis. Front Pharmacol. (2022) 12:760507. doi: 10.3389/fphar.2021.760507
29. Roszkowska AM, Licitra C, Tumminello G, Postorino EI, Colonna MR, Aragona P. Corneal nerves in diabetes-The role of the in vivo corneal confocal microscopy of the subbasal nerve plexus in the assessment of peripheral small fiber neuropathy. Surv Ophthalmol. (2021) 66:493–513. doi: 10.1016/j.survophthal.2020.09.003
30. Adams BS, Patel AR. Cenegermin. In: StatPearls, vol. 2023. StatPearls Publishing, Treasure Island (FL (2023). p. 34424642.
31. Deeks ED, Lamb YN. Cenegermin: A review in neurotrophic keratitis. Drugs. (2020) 80:489–94. doi: 10.1007/s40265-020-01289-w
32. Pflugfelder SC, Massaro-Giordano M, Perez VL, Hamrah P, Deng SX, Espandar L, et al. Topical recombinant human nerve growth factor (Cenegermin) for neurotrophic keratopathy: A multicenter randomized vehicle-controlled pivotal trial. Ophthalmology. (2020) 127:14–26. doi: 10.1016/j.ophtha.2019.08.020
33. Sacchetti M, Komaiha C, Bruscolini A, Albanese GM, Marenco M, Colabelli Gisoldi RAM, et al. Long-term clinical outcome and satisfaction survey in patients with neurotrophic keratopathy after treatment with cenegermin eye drops or amniotic membrane transplantation. Graefes Arch Clin Exp Ophthalmol. (2022) 260:917–25. doi: 10.1007/s00417-021-05431-6
34. García-Delpech S, Udaondo P, Fernández-Santodomingo AS, García-Teillard D. Neurotrophic keratopathy treated with topical recombinant human nerve growth factor (Cenegermin): case series study with long-term follow-up. Case Rep Ophthalmol. (2022) 13:663–70. doi: 10.1159/000525923
35. Roszkowska AM, Inferrera L, Aragona E, Gargano R, Postorino EI, Aragona P. Clinical and instrumental assessment of the corneal healing in moderate and severe neurotrophic keratopathy treated with rh-NGF (Cenegermin). Eur J Ophthalmol. (2022) 32:3402–10. doi: 10.1177/11206721221097584
36. Pedrotti E, Bonacci E, Chierego C, De Gregorio A, Cozzini T, Brighenti T, et al. Eight months follow-up of corneal nerves and sensitivity after treatment with cenegermin for neurotrophic keratopathy. Orphanet J Rare Dis. (2022) 17:63. doi: 10.1186/s13023-022-02237-5
37. Di Zazzo A, Varacalli G, Mori T, Coassin M. Long-term restoration of corneal sensitivity in neurotrophic keratopathy after rhNGF treatment. Eur J Ophthalmol. (2022) 32:NP15–8. doi: 10.1177/1120672120953343
38. Mastropasqua L, Lanzini M, Dua HS, D’ Uffizi A, Di Nicola M, Calienno R, et al. In vivo evaluation of corneal nerves and epithelial healing after treatment with recombinant nerve growth factor for neurotrophic keratopathy. Am J Ophthalmol. (2020), 217:278–286. doi: 10.1016/j.ajo.2020.04.036
39. Hao M, Cheng Y, Wu J, Cheng Y, Wang J. Clinical observation of recombinant human nerve growth factor in the treatment of neurotrophic keratitis. Int J Ophthalmol. (2023) 16:60–6. doi: 10.18240/ijo.2023.01.09
40. Fausto R, Ceccuzzi R, Micheletti E, Clerici R, Riva I, Katsanos A, et al. A case report of pediatric neurotrophic keratopathy in pontine tegmental cap dysplasia treated with cenegermin eye drops. Med (Baltimore). (2020) 99:e20816. doi: 10.1097/MD.0000000000020816
41. Hatcher JB, Soifer M, Morales NG, Farooq AV, Perez VL, Shieh C. Aftermarket effects of cenegermin for neurotrophic keratopathy in pediatric patients. Ocul Surf. (2021) 21:52–7. doi: 10.1016/j.jtos.2021.04.003
42. Pedrotti E, Bonetto J, Cozzini T, Fasolo A, Marchini G. Cenegermin in pediatric neurotrophic keratopathy. Cornea. (2019) 38:1450–2. doi: 10.1097/ICO.0000000000002112
43. Elhusseiny AM, Traish AS, Saeed HN, Mantagos IS. Topical cenegermin 0.002% for pediatric neurotrophic keratopathy. Eur J Ophthalmol. (2022) 32:3420–4. doi: 10.1177/11206721221094783
44. Leto MG, Toro ME, Indemini PE, Fruttero C, Denina M, Dalmazzo C, et al. Pediatric use of recombinant human nerve growth factor 20 μg/mL eye drops (Cenegermin) for bilateral neurotrophic keratopathy in congenital corneal anesthesia. Cornea. (2021) 40:228–31. doi: 10.1097/ICO.0000000000002612
45. Papadopoulos K, Besgen V, Sekundo W. Successful treatment of a pediatric neurotrophic keratopathy with cenegermin. Cornea. (2021) 40:516–8. doi: 10.1177/11206721221094
Keywords: rh-NGF, cenegermin, neurotrophic keratitis, persistent epithelial defects, nerve growth factors, corneal sensitivity
Citation: Roszkowska AM, Spinella R, Calderone A, Sindoni M, Wowra BH, Kozak M, Sajak-Hydzik K and Aliò J (2024) The use of rh-NGF in the management of neurotrophic keratopathy. Front. Ophthalmol. 4:1408587. doi: 10.3389/fopht.2024.1408587
Received: 28 March 2024; Accepted: 04 June 2024;
Published: 08 July 2024.
Edited by:
Sudi Patel, Svjetlost Clinic, CroatiaReviewed by:
Davide Borroni, Riga Stradiņš University, LatviaCopyright © 2024 Roszkowska, Spinella, Calderone, Sindoni, Wowra, Kozak, Sajak-Hydzik and Aliò. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bogumił H. Wowra, Ym9ndW1pbHdvd3JhQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.