 Ejaz Ansari1,2*
Ejaz Ansari1,2*- 1Ophthalmology, Maidstone & Tunbridge Wells NHS Trust, Maidstone, United Kingdom
- 2Institute of Medical Sciences, Christ Church Canterbury University, Canterbury, United Kingdom
Most readers will be familiar with terminology (from meetings and conferences) that we, the editors, would deem to be incorrect or confusing. In general, we all tend to accept the information conveyed to us without really questioning what the terms truly mean. Therefore, the subsequent chapters discussing the IOLs in question should be studied with this in mind since a lot of familiar terminology will be used in those chapters, which, strictly speaking, may not be in line with the most accurate terminology and classification. The reader is encouraged to read this full article to be mindful of the current confusion surrounding IOL terminology and what the correct terminology should be. This is so that one is better prepared to understand and question the mechanism of action and side effects of IOLs that one is planning to use.
Introduction
When describing intraocular lenses (IOLs) that are used for the management of presbyopia, certain terms are repeated and become embedded, often without question or further enquiry by the listener. Phrases such as “premium IOL, EDoF (extended depth of focus), and “fewer dyspohotopsias” are well known by the cataract surgery fraternity. But what do these phrases mean and is it correct to use them?
Discussion
A premium is the cost of insurance, that is usually an amount paid annually. “At a premium” means scarce and in demand, or above the usual or nominal price, the latter meaning being most appropriate in this case. However, it does not indicate how the IOL functions for the patient’s benefit. Another phrase that is used interchangeably with premium is “presbyopia-correcting”. This is misleading since these IOLs do not correct presbyopia, but rather increase the range of focus (RoF). High- performance IOL (HPIOL) is a better descriptor.
What does EDoF mean? The acronym EDoF comes from photography, where it refers to the extended depth of field achieved by reducing either the aperture or the magnification of an optical system. EDoF is used liberally by manufacturers and surgeons who promote enhanced vision quality and range of focus compared to multifocal IOLs and monofocal IOLs respectively.
In actual fact, the only lenses that truly extend the depth of field are small-aperture (i.e., pinhole) lenses, e.g., the IC8 (AcuFocus) and XtraFocus Pinhole Implant (Morcher). The remainder are either extended range of focus (EROF) or increased range of focus (IROF) implants. Full range of focus (FROF) would apply to trifocals.
The American National Standards Institute (ANSI) (Z80.35-2018) standard for EDoF IOLs require implants to have intermediate vision (67 cm) of 20/30 in at least 50% of recipients. There is no mention of dyspohotopsias, but clinicians tend to associate EDoF IOLs with fewer dyspohotopsias! This misconception that EDoF equals fewer or no dyspohotopsias has stoked the flames of enthusiasm in many IOL manufacturers.
In actual fact, the mechanisms of action of some EDoF IOLs may result in halos, glare, starbursts, and unsharp focus. For example, the mechanism utilised to increase the range of focus may not follow the principle of elongating the conoid of Sturm. Instead, refractive, diffractive or a combination of mechanisms are used resulting in dyspohotopsias that are associated with bifocal and trifocal IOLs anyway. This can lead to dissatisfied patients who have been informed erroneously that they will not experience dyspohotopsias with an EDoF IOL.
An alternative classification of this category of IOLs has been suggested by the American European Congress of Ophthalmic Surgery (AECOS) (1). A committee of four surgeons set about to demystify the myth that EDoF IOLs leading to fewer dyspohotopsias and the confusion arising from the variety of IOLs in this category (Table 1). They subdivided the concept of lens performance into three main components:
1. Range of focus
2. Mechanisms of action
3. Dyspohotopsias (1)
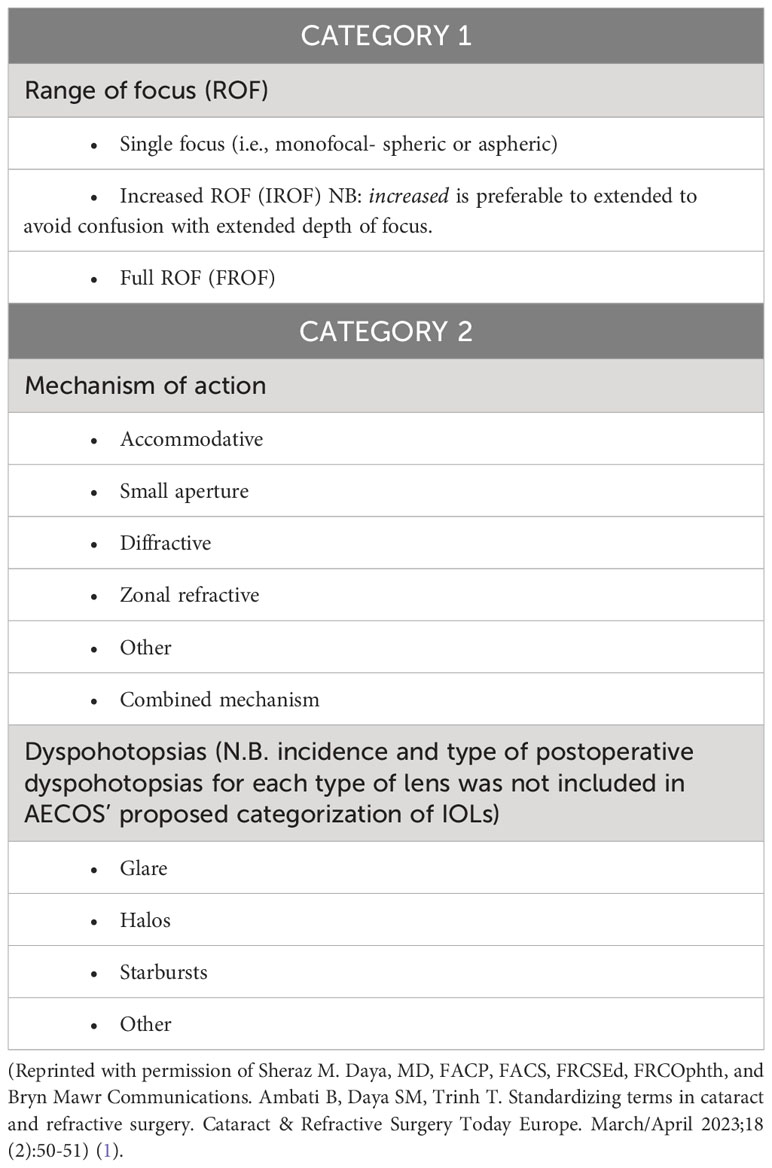
Table 1 AECOS classification of IOLs: terminology separates lens performance (i.e., ROF) from mechanism of action.
It is true that other variables such as neuroadaptation, expectations, corneal optics, post-operative pupil size and axial length have a part to play in final lens performance, however these were not included in the classification to avoid too much complexity.
Another consideration when selecting IROF IOLs is their dependence on good centration along the visual axis. This is described in the fourth column of the Table 2.
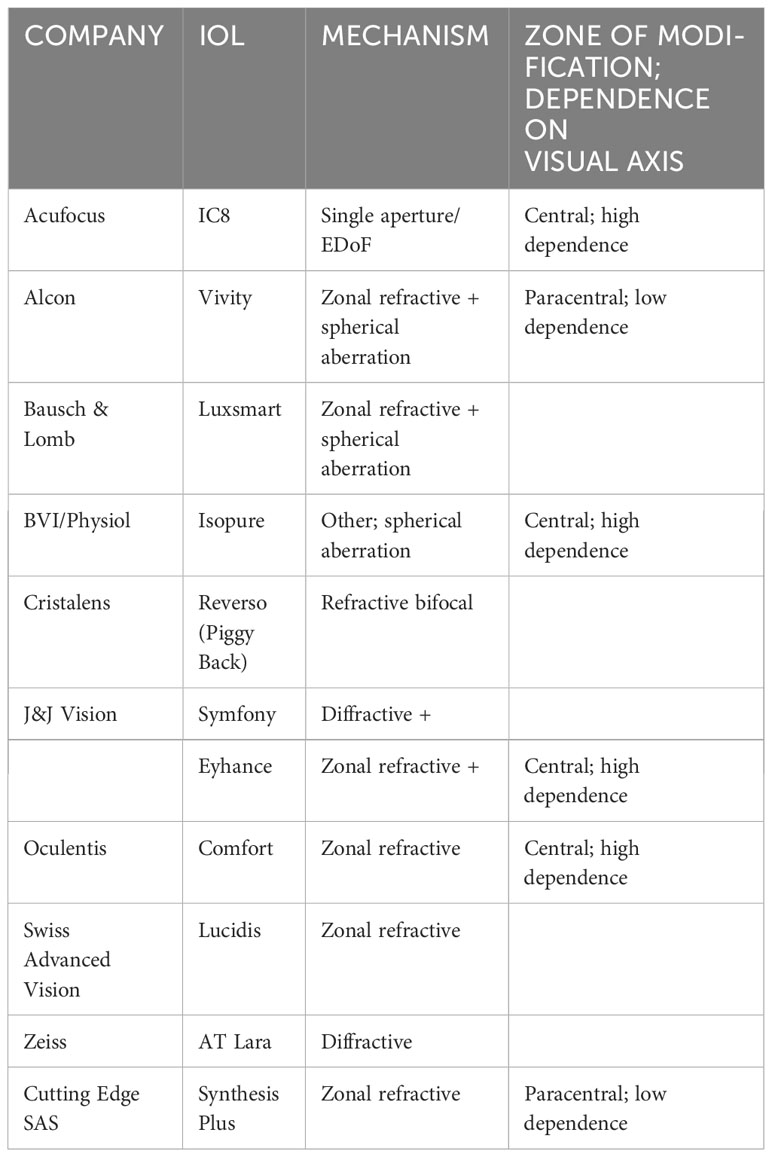
Table 2 Increased range of focus IOLs (2).
The + suffix refers to more than one mechanism of action (3, 4).
Conclusion
It is important to categorize IOLs in clear and simple language for the benefit of patients and surgeons alike. Obviously, clear, and simple language assists the surgeon in making sense of all the variety of options available and what would suit individual patients. Similarly, it helps patients to be more well informed of the IOL that suits their needs. Collaboration between stakeholders is essential to produce terminology that is clearer to everyone.
Falsehood flies, and the truth comes limping after it; so that when men become undeceived, it’s too late; the jest is over, and the tale has had its effect. Jonathan Swift 1710
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
The author confirms being the sole contributor of this work and has approved it for publication.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Daya SM, MD, FACP, FACS, FRCSEd, FRCOphth, and Bryn Mawr Communications, Ambati B, Daya SM, Trinh T. Standardizing terms in cataract and refractive surgery. Cataract & Refractive Surgery Today. (2023) 18(2):50–1.
3. Song X, Liu X, Wang W, Zhu Y, Qin Z, Lyu D, et al. Visual outcome and optical quality after implantation of zonal refractive multifocal and extended-range-of-vision IOLs: a prospective comparison. J Cataract Refract Surg (2020) 46(4):540–8. doi: 10.1097/j.jcrs.0000000000000088
Keywords: presbyopia-correcting, EDoF lenses, increased range of focus, dysphotopsias, depth of field
Citation: Ansari E (2023) Terminology - clarifying the current confusion and presenting the correct terminology. Front. Ophthalmol. 3:1249557. doi: 10.3389/fopht.2023.1249557
Received: 28 June 2023; Accepted: 26 October 2023;
Published: 14 November 2023.
Edited by:
Yongwei Guo, Zhejiang University Eye Hospital, ChinaReviewed by:
Senmao Li, University of Cologne, GermanyWanlin Fan, University Hospital of Cologne, Germany
Copyright © 2023 Ansari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ejaz Ansari, ZS5hbnNhcmlAbmhzLm5ldA==