
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 02 April 2025
Sec. Molecular and Cellular Oncology
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1556881
 Sanjib Saha1*
Sanjib Saha1* Ulf-Göran Gerdtham1,2
Ulf-Göran Gerdtham1,2 Gottfrid Sjödahl3,4Christel Häggström5,6James W. F. Catto7John D. Kelly8Anders Ullén9,10Lars Holmberg5,11Fredrik Liedberg3,4
Gottfrid Sjödahl3,4Christel Häggström5,6James W. F. Catto7John D. Kelly8Anders Ullén9,10Lars Holmberg5,11Fredrik Liedberg3,4Background: Guidelines recommend neoadjuvant chemotherapy (NAC) and radical cystectomy (RC) for muscle-invasive bladder cancer (MIBC). Current recommendations do not consider genomic profiles, although the Basal/Squamous (Ba/Sq) subtype is less likely to respond to NAC compared to Urothelial-like (Uro) and Genomically Unstable (GU) subtypes. The aim of this study is to perform cost-effectiveness analyses of a de-escalated use of NAC in patients with Ba/Sq tumors and MIBC.
Methods: A cost-effectiveness analysis was performed using a decision analytic Markov model using a healthcare provider perspective. Treatment and prognosis probabilities originated from the Bladder Cancer Data Base, Sweden (BladderBaSe) 2.0. Information on molecular subtype and outcomes was retrieved from published studies, and quality-adjusted life year (QALY) data were obtained from the iROC trial. Costs were collected from the regional healthcare registers in Sweden, utility values were obtained from the literature, and outcomes are presented as incremental cost-effectiveness ratio (ICER). Scenario analyses, along with several one-way and probabilistic sensitivity analyses were performed to capture uncertainties.
Results: At a 5-year time horizon, the model predicts that molecular subtype-based treatment has an ICER of 4,964 Euro/QALY (66,766 Swedish Krona/QALY), which is deemed cost-effective in the Swedish setting. At €7,427 (100,000 SEK) willingness-to-pay threshold, the molecular subtype-based treatment has a 65% probability of being cost-effective. The results were not sensitive to uncertainty analyses.
Conclusion: Molecular subtype-based treatment of MIBC, i.e., refraining from administering NAC to patients with Ba/Sq tumors, is cost-effective compared to the current treatment practices in Sweden.
With the advent of molecular classification based on transcriptomic profiling (1) and subsequent studies suggesting a role for molecular subtyping in predicting neoadjuvant chemotherapy (NAC) response (2–4), possibilities to individually tailor the use of NAC have emerged. By applying the Lund taxonomy (LundTax), we have shown that patients with the Basal/Squamous (Ba/Sq) subtype are less likely to benefit from three courses of cisplatin-based chemotherapy compared to those with Urothelial-like (Uro) or Genomically Unstable (GU) subtypes, both when evaluating the pathological response in the cystectomy specimen and the survival outcomes (3).
Today, the standard of care for all patients with muscle-invasive bladder cancer (MIBC) without metastases (T2-T4aN0M0) is cisplatin-based NAC followed by radical cystectomy (RC). The use of NAC gains a 5% absolute survival benefit at five years compared to RC only (5). In Sweden, 113 out of 152 (74%) patients under 76 years received such preoperative treatment in 2022 (6). For patients not receiving NAC, cisplatin-based chemotherapy can be considered in the adjuvant setting for selected patients with advanced disease (pT3/pT4 and/or N+) according to Swedish and EAU guidelines (7).
Applying a molecular subtype-based and de-escalated use of NAC to reduce overtreatment combined with offering adjuvant chemotherapy only to those with advanced disease in the cystectomy specimen may entail a better utilization of healthcare resources. It might also increase the uptake of NAC, which up to now have had a low utilization rate of only 17.2% according to a recent meta-analysis (8). This is particularly important considering that bladder cancer is one of the most expensive malignancies, with a total annual cost of around $7.93 billion in the USA (in 2015) and €5.24 billion in Europe (in 2019) (9).
To alter the current treatment practice, offering NAC to all eligible patients, and provide treatment according to molecular subtypes in line with the ideas behind precision medicine, a broad and comprehensive assessment including both effectiveness of treatment patterns as well as cost-effectiveness is needed. The objective of this study is to estimate whether molecular subtype-specific use of NAC in patients with MIBC is cost-effective compared to current practice in Sweden by applying a de-escalated use of NAC for the Ba/Sq subtype.
In the absence of a clinical trial, this cost-effectiveness analysis utilized a Markov decision analytic simulation model following the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) (10).
We used data from the Bladder Cancer Data Base Sweden (BladderBaSe 2.0), a research database including all patients in the Swedish National Register for Urinary Bladder Cancer (SNRUBC) diagnosed from the 1st of January 1997 through the 31st of December 2019, individually linked by using the unique Swedish personal identification number to several Swedish national data sources (11). BladderBaSe 2.0 includes information on tumor characteristics, treatments, and important confounding factors such as socioeconomic variables and comorbidity, and also with extensive follow-up. As a proxy for cisplatin-eligibility, we choose from this database all patients who were 76 years or younger at the time of RC as their main treatment for clinical stage T2-T4aN0M0 disease from 1999 to 2019. This is also in line with the Swedish national guidelines on urothelial carcinoma recommending that above 60% in this population should be offered NAC (12). We excluded patients who were treated with both NAC and adjuvant chemotherapy (AC), given that this is not recommended by EAU guidelines (7). The study population sample selection procedure is displayed in Figure 1.
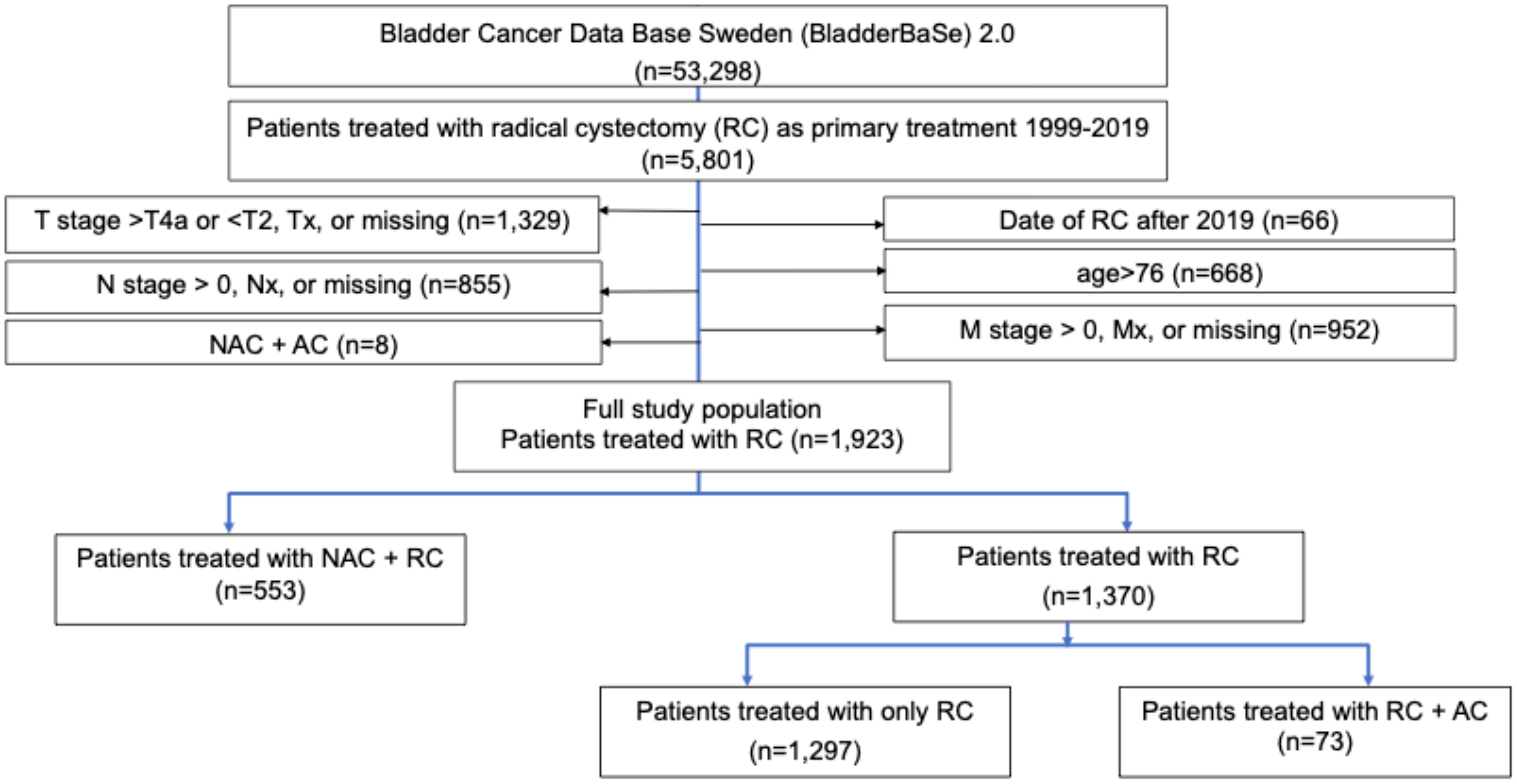
Figure 1. Study sample selection procedure from the BladderBase 2.0 database. RC, Radical Cystectomy; NAC, Neoadjuvant Chemotherapy; AC, Adjuvant Chemotherapy.
We created a Markov decision-analytic simulation model comparing current treatment practice when offering NAC to all cisplatin-eligible patients with MIBC to a de-escalated use of NAC based on molecular subtype. In the current treatment practice, patients receive either three courses of NAC, with ddMVAC (methotrexate, vinblastine, Adriamycin, and cisplatin), followed by RC (NAC+RC) or RC only. Those who received upfront RC without NAC optionally received four courses of AC (ddMVAC) in cases of non-organ-confined disease in the cystectomy specimen (i.e., pT3 or higher or pN+).
In the molecular subtype-based treatment option, patients with either Uro or GU tumors will receive NAC+RC, while those with the Ba/Sq subtype will receive upfront RC, but if the cystectomy specimen displays pT3 or higher or pN+, four courses of AC will be administered postoperatively according to guidelines. The Markov model is based on only three health states: survival after RC, death by bladder cancer, and death by other causes than bladder cancer, where patients transition into these health states are estimated in a yearly cycle. In Figure 2, the Markov model structure is described. The model is developed and analyzed using TreeAgePro Healthcare, v2023.
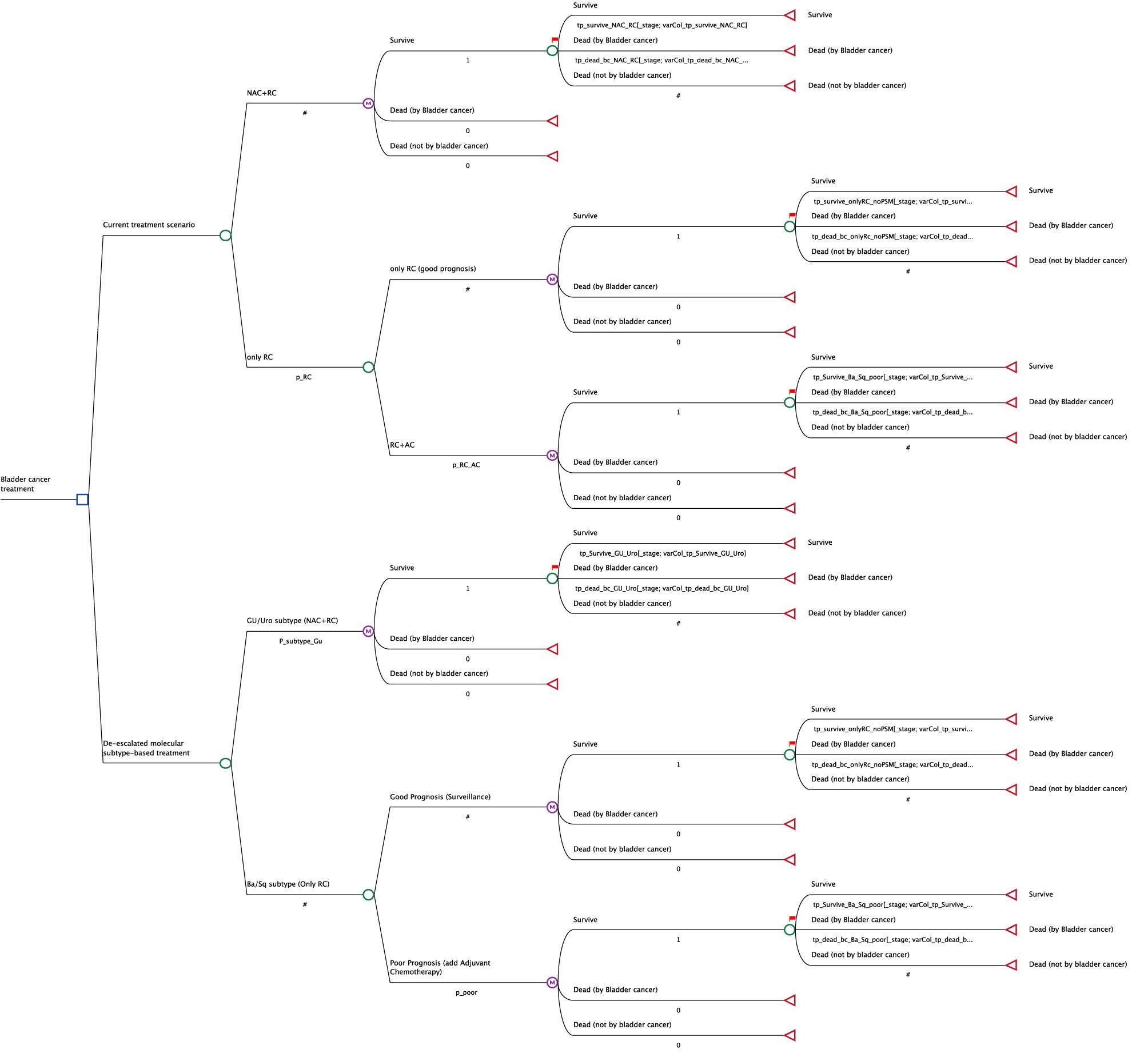
Figure 2. The Markov model structure.
The proportion of patients receiving NAC+RC, upfront RC only, and RC+AC was estimated by use of BladderBaSe 2.0. Since BladderBaSe 2.0 does not have information on molecular subtype, the percentage of individuals with Uro/GU and Ba/Sq subtypes, respectively, was estimated using data from Sjödahl et al. (3) and Olah et al. (13). The proportion of patients with Ba/Sq subtypes who had poor prognosis (≥pT3 or pN+) based on inclusion criteria in adjuvant trials (14, 15) and the corresponding proportion of good prognosis (≤pT2N0) according to the pathological tumor stage in the cystectomy specimen after RC was also estimated from these two studies (3, 13). Assuming cisplatin eligibility before and after RC, the poor prognosis definition was applied to determine the proportion of patients treated with upfront RC who would be recommended for AC. The criteria for poor and good prognosis are presented in Table 1, and the parameters of the model are given in Table 2.
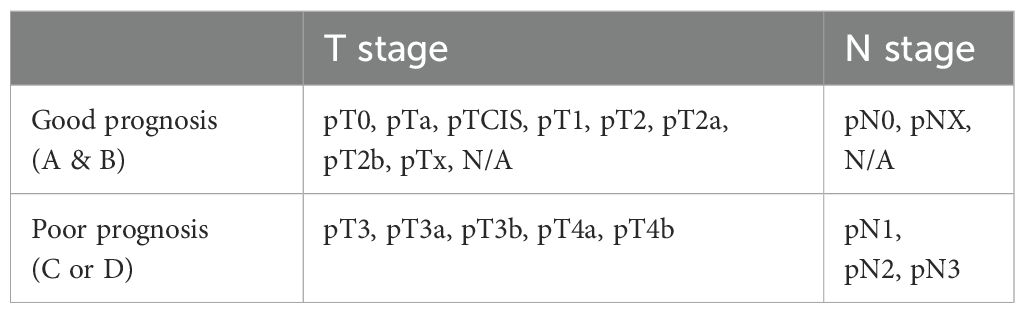
Table 1. The criteria for good and poor prognosis are based on the pathological tumour stage (pT-stage) and pathological nodal stage (pN-stage) in the radical cystectomy specimen.
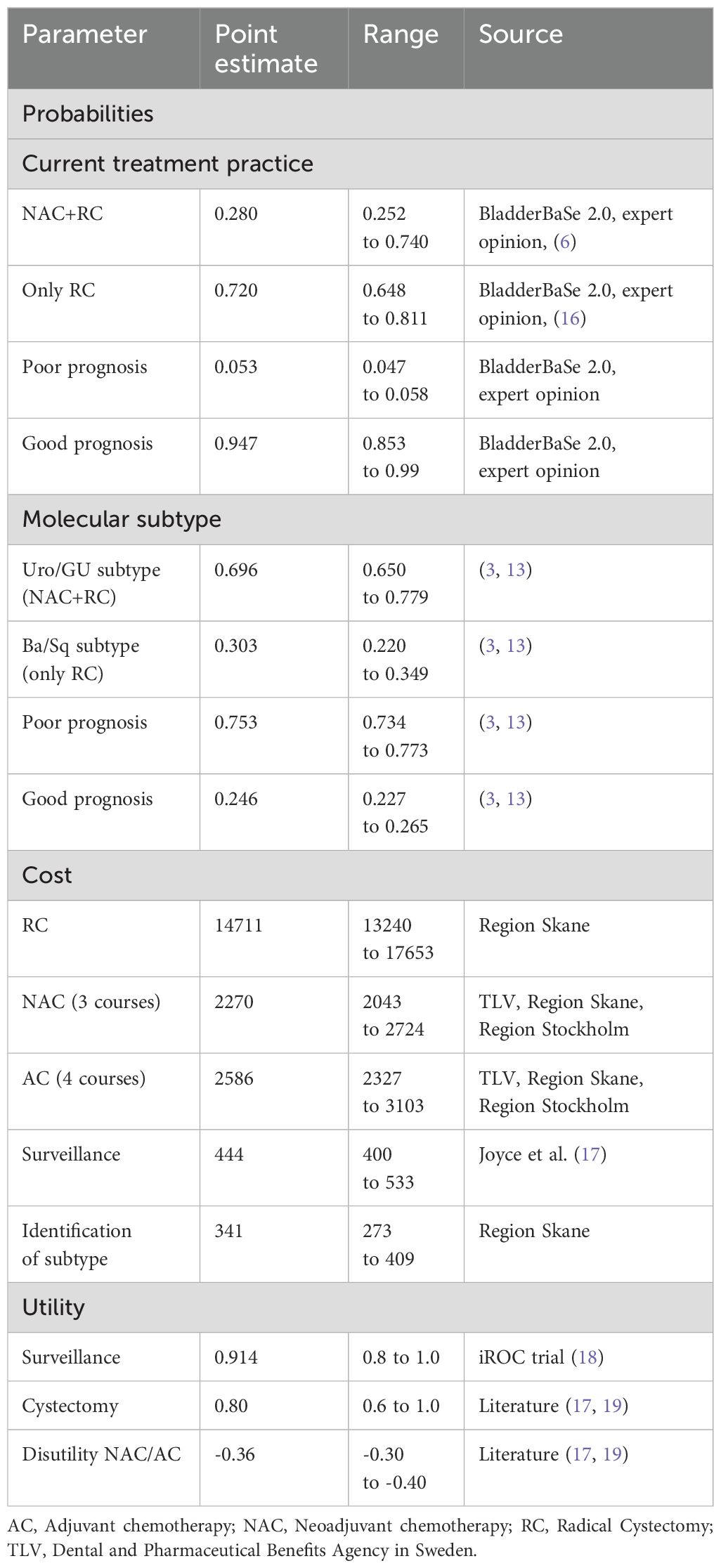
Table 2. Cost (in Euro (EU-27), 2022 price year) and utility parameters used in the model.
The yearly survival probabilities, including death due to bladder cancer or other causes, were retrieved from BladderBaSe 2.0 (n=1297). Additionally, we used data from Sjödahl et al. to estimate the survival for individuals with Uro/GU subtypes who received NAC+RC (n=77) (3). Due to a small sample size, survival probabilities for patients with Ba/Sq subtype in both the good and poor prognosis categories were uncertain. Instead, we used survival estimates from those treated with RC only (n=1297) and with RC+AC (n=73) in BladderBaSe 2.0, respectively (Figure 1). The yearly transition probabilities are presented in the Supplementary Materials (Section 1: Supplementary Tables S1-S6). The statistical analyses were conducted using STATA version 17.
This cost-effectiveness analysis was performed from a healthcare provider’s perspective. Costs due to RC, chemotherapy, and identification of molecular subtypes through RNA extraction and RNA-sequencing applying LundTax single sample classifiers (20) were estimated from the Skane Regional Council healthcare registers (Table 2). All healthcare services were valued by using diagnosis-related groups (DRG), a patient cost classification system (21). All costs were collected in Swedish kronor (SEK) and converted into Euro (27-EU) using purchasing power parity in the 2022 price year. (22). Utility values for the survival health states were obtained from the literature and expert opinion (Table 2). The utility values, toll, and time within each health condition, i.e., RC with three or four courses of chemotherapy, were used to calculate quality-adjusted life years (QALYs) with the area under the curve methodology (23). Baseline QALY, i.e., at the year of diagnosis, was obtained from the iROC trial (18). The assumptions behind the QALY estimations are presented in the Supplementary Materials (Section 2). Costs and QALYs were discounted at a rate of 3% annually following the guideline of the Dental and Pharmaceutical Benefits Agency (TLV) of Sweden (24).
The results were expressed as incremental cost-effectiveness ratio (ICER), where ICER is defined as the difference in costs divided by the differences in QALYs between groups. According to the Swedish National Board of Health and Welfare, cost per QALY gained below 100,000 SEK (7,427 Euro/QALY) is considered low cost-effective (25) and used as the willingness-to-pay (WTP) threshold in this study. The analysis applied a base case time horizon of two years, three years, and five years from the time of RC (Table 3).
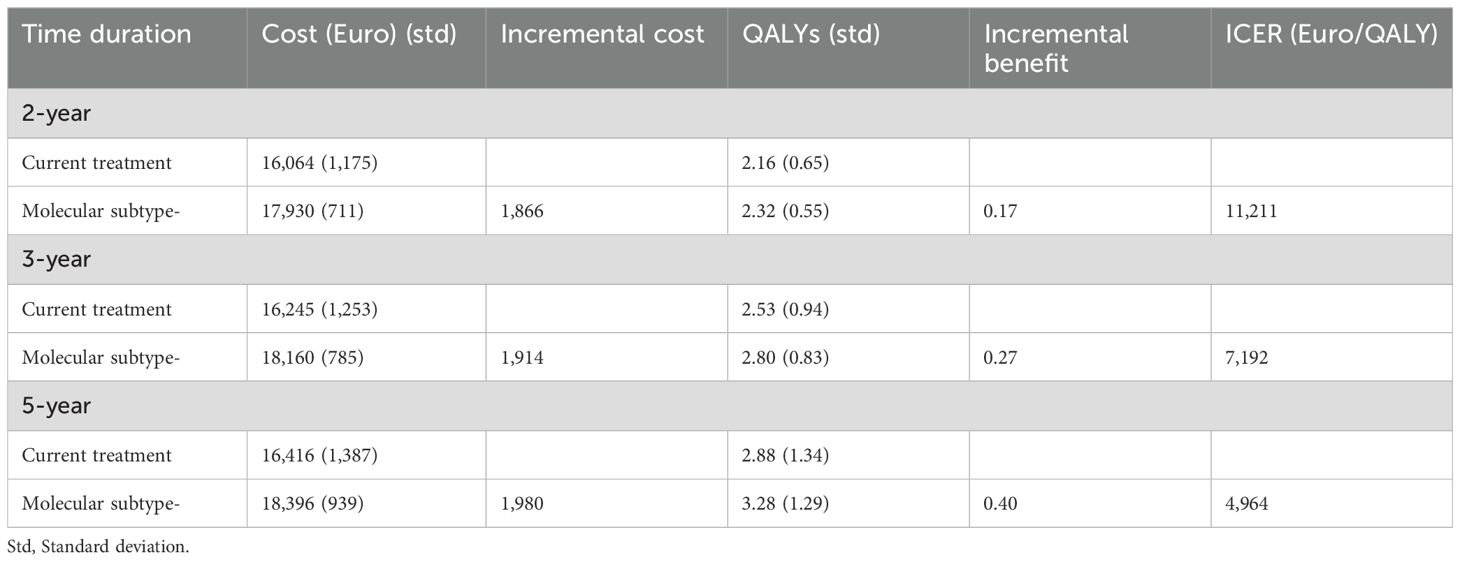
Table 3. Incremental cost-effectiveness ratio (ICER) at 2-year, 3-year and 5-year by current treatment practice and de-escalated molecular subtype-based use of perioperative chemotherapy, respectively.
Several one-way and probabilistic sensitivity analyses, together with three scenario analyses, were performed to estimate the uncertainty around the base case result. Sensitivity analyses were performed for the estimate using a 5-year time horizon. Most of the parameters in the model were varied over plausible ranges, and the outcomes were presented as a tornado diagram. For example, the proportion of patients receiving NAC in Sweden has increased over the years; thus, we used the most recent value from 2022 (74%) (6). Furthermore, we used the data from a recent German study on the proportion of upfront RC in a context where NAC, by tradition, is less frequently applied (16). For probabilistic sensitivity, Monte Carlo simulations with 10,000 iterations were employed and portrayed as Cost-Effectiveness Acceptability Curve (CEAC), which shows the probability of the intervention being cost-effective across a spectrum of WTP thresholds. The three scenario analyses are presented in the Supplementary Materials (Section 3).
In the base case analyses, the de-escalated molecular subtype-based treatment was associated with a 0.40 QALY increase compared to the current treatment practice with an additional cost of €1,980 at the 5-year time horizon. This yielded an ICER of €4,964/QALY, which is deemed cost-effective in the Swedish setting. With a WTP of 7,427 Euro, a de-escalated use of NAC was deemed cost-effective beyond a 2-year time horizon (Table 2).
In the tornado diagram, while the base case result showed stability, the ICER demonstrated variability across parameters (Figure 3). The CEAC (Figure 4) showed that at €10,000 WTP, the molecular subtype-based treatment has a 90% probability of being cost-effective. The probability of being cost-effective increases with increasing WTP. The ICERs for the scenario analyses also fell below the WTP threshold except the third scenario (Supplementary Materials: Section 3 and Supplementary Tables S8-S10).
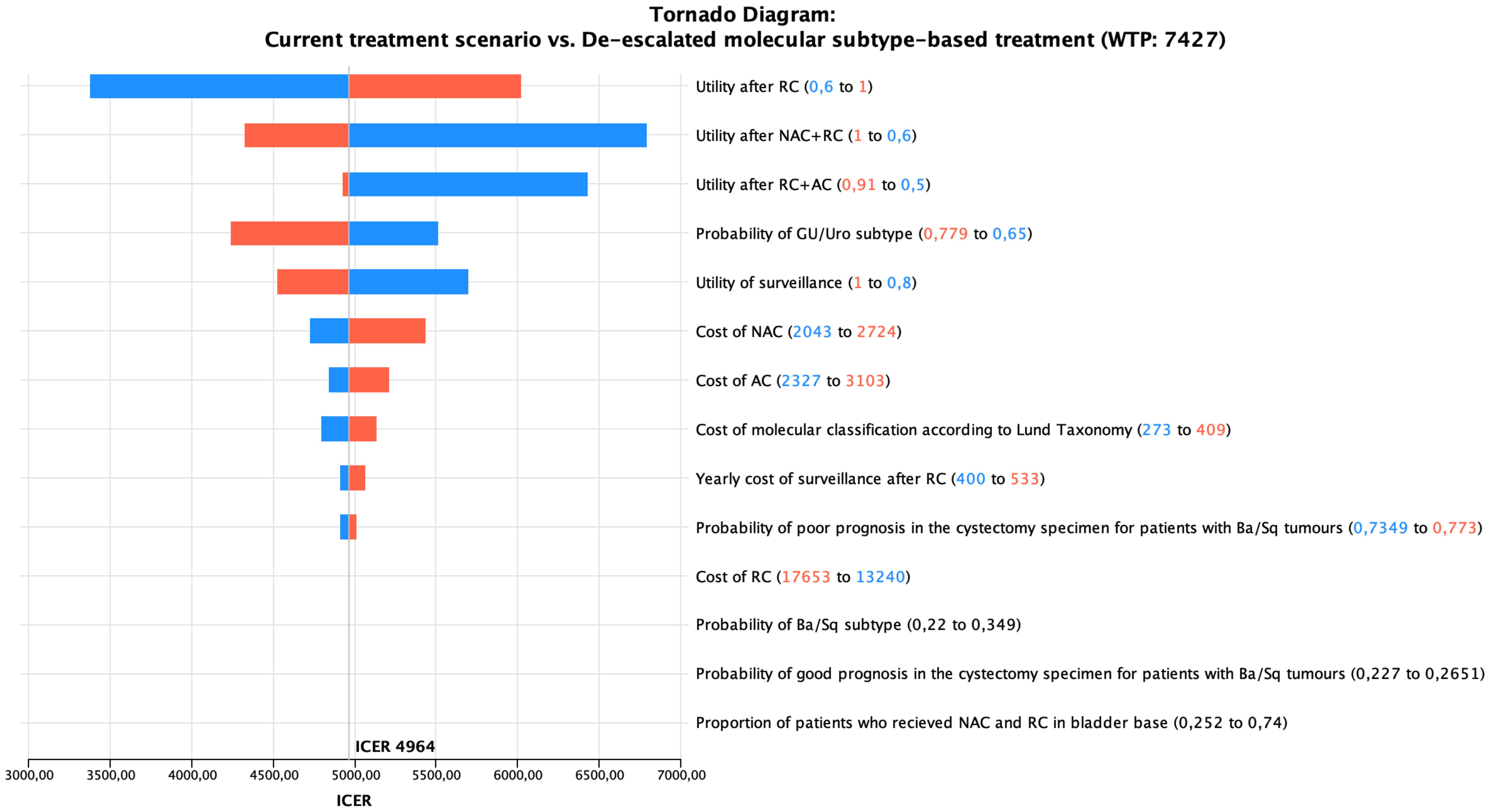
Figure 3. The Tornado diagram for one-way sensitivity analyses.
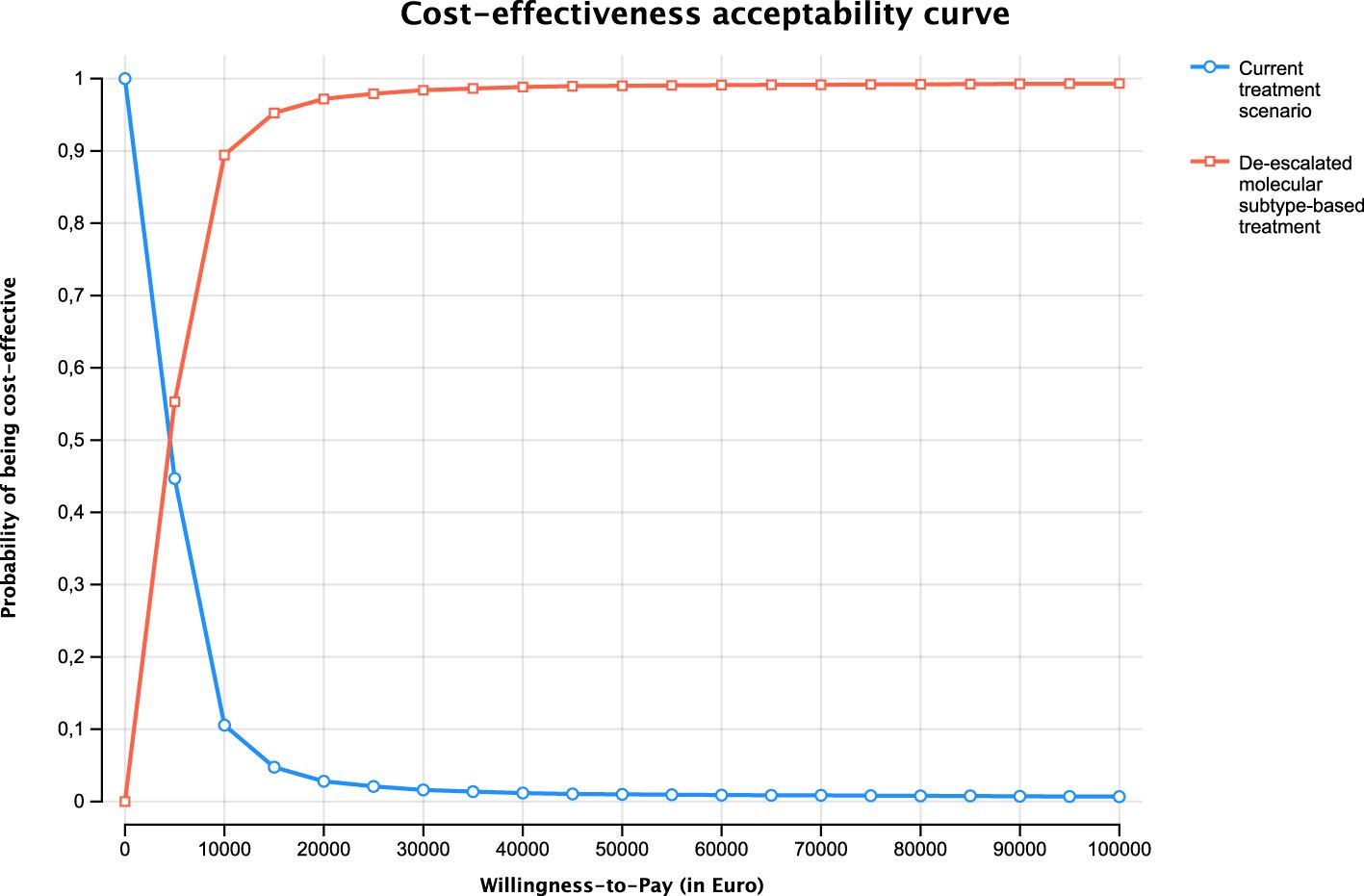
Figure 4. The cost-effectiveness acceptibility curve.
We estimated the cost-effectiveness of molecular subtype-based use of NAC compared to the current treatment practice using population-based real-world data. We found that refraining from NAC in patients with Ba/Sq tumors and instead directly proceeding to upfront RC was cost-effective in base case, sensitivity, and scenario analyses.
To our knowledge, this is the first cost-effectiveness analysis using molecular subtype-based treatment for patients with MIBC. Thus, any comparisons with similar studies in bladder cancer were not possible. However, a de-escalated use of AC in breast cancer based on gene expression profiling has been reported as cost-effective (26), and so has molecular classification-based treatment in endometrial cancer (27).
The general lack of cost-effectiveness studies evaluating precision medicine in cancer was highlighted in a recent review, where the authors argued that the lack of clinical trials to estimate the effectiveness is a significant barrier to the implementation of targeted therapies (28). In the setting of de-escalating cancer treatment based on gene expression profiling, such lack of evidence is even more pronounced except for one large non-inferiority breast cancer RCT (n=10,273) (29). Due to the sample-size requirement, it is unlikely that an adequately designed non-inferiority RCT based on the 5% absolute survival benefit from NAC (5) investigating molecular subtype-dependent de-escalated use of NAC in bladder cancer will be performed in the foreseeable future. Simulation models are particularly helpful in this case to predict the long-term impact of interventions over time, account for uncertainties in real-world settings, and test various scenarios that may not be feasible to evaluate in traditional studies. By simulating different outcomes, we can provide more accurate predictions of both the health and economic benefits of interventions, offering valuable insights for decision-makers.
There is also a lack of research on the estimation of QALYs in bladder cancer. For example, the disutilities of both AC and NAC were not available from validated sources, such as RCTs. In the absence of reliable data, we used information about utilities from observational studies (9, 30, 31) and expert opinion (the information presented in Supplementary Materials). In addition to QALY at one-year follow-up, side effects emerging at even longer follow-up from cisplatin, an essential component in NAC, such as long-term renal impairment (32, 33), sensory neuropathy, tinnitus, and hearing loss (34) are well known and can also be taken into account. Thus, if a patient can be spared NAC based on molecular information, avoiding long-term side effects, there is another well-founded argument to implement this practice.
There are several limitations to be acknowledged in this study. First, our estimates of molecular subtype proportions, including the distribution of pathological outcomes in the cystectomy specimens stratifying patients into good and poor prognosis after RC, were derived from two small cohorts (3, 13). Due to the scarcity of sufficiently large cohorts with both molecular subtyping and clinical outcomes, our survival estimates for individuals with Ba/Sq tumors were retrieved in BladderBaSe 2.0, lacking subtype information (Section 1: Supplementary Tables S1-S6), although being a population-based source with real world data. The rationale for applying these data was based on similar survival outcomes reported for LundTax subtypes in patients treated with upfront RC in a Swedish population-based series (35) and in an observational multicenter study (36). Although our QALY estimates were based mainly on observational data and expert opinion, which might introduce bias, the baseline QALY estimation came from an RCT (18) and was based on Swedish tariff data. Thus, we have little reason to expect that this would introduce a bias when comparing NAC and AC. Another limitation was the use of only one classification system when assessing cost-effectiveness. Although the LundTax is well conformed with the MIBC consensus classification (37), several other molecular subtyping systems exist. Nonetheless, the Ba/Sq subtype defined by the MIBC consensus-classification system is also associated with chemoresistance in a recent RCT (4). Cross-comparison of various subtyping systems by clustering identified the Ba/Sq subtype as the only highly concordant across all systems, indicating that the choice of MIBC classifier matters less for the identification of this subtype. It is also likely that our outcomes are generalizable to gemcitabine-cisplatin as NAC regimen, as this cisplatin-based combination also was used in studies investigating the use of molecular subtypes as a measure to stratify the use of NAC (2–4). A limitation of our model is that adjuvant immune checkpoint inhibitors are not considered (38), even though a subtype dependent response to adjuvant checkpoint inhibitors has been suggested (39). This is beyond the scope of current study but highlights the need for future research when response probabilities on such therapy are available.
The reliability of a simulation model is contingent on the quality of the data and assumptions incorporated. Our cost data, sourced from Swedish registers, contributes to the internal validity of our findings. Nevertheless, external validity and cross-validity of a simulation model can be subject to scrutiny, although we conducted a range of sensitivity analyses to enhance the robustness of our results.
The low cost per QALY gained (€4,964/QALY) motivates the introduction of this strategy in Sweden and similar healthcare settings. This is also supported by the survival benefit from AC in patients with Ba/Sq tumors (40). In fact, a real-time population-based pipeline with prospective RNA-sequencing and molecular subtyping according to LundTax is already operating in several healthcare regions in Sweden (UROSCANSEQ, ISRCTN 15459149) (41), and a versatile and upgraded version of the LundTax classification algorithm applicable to different gene expression platforms and less sensitive to variations in sample purity is available (42). Furthermore, LundTax molecular subtyping can also be performed by immunohistochemistry on formalin-fixed specimens, further increasing the applicability of molecular classification in other healthcare contexts (43). A de-escalated subtype-based use of NAC might even increase the incentive to apply NAC in populations and countries where such preoperative treatment today is only used for a minority of patients, where overtreatment is the main objective against applying NAC. For example, only 21% of patients below 60 years of age received NAC in 2017 in Germany (44), and an even lower proportion in a report from the SEER data from the USA (17%) (45), despite being recommended to all eligible patients based on level 1a evidence (7).
Applying a de-escalated use of NAC in patients with MIBC with the Ba/Sq molecular subtype according to LundTax is cost-effective, and implementation in clinical practice can be considered.
The data analyzed in this study is subject to the following licenses/restrictions: Data used for modeling is available upon request to the corresponding author (SS) and project leader (FL). Requests to access these datasets should be directed to c2FuamliLnNhaGFAbWVkLmx1LnNl.
This is a simulation model-based study where the parameters are derived from the BladderBase 2.0 and several published articles. The Bladderbase 2.0 database has ethical approval from the Research Ethics Board at Uppsala University, Sweden (Dnr 2015-277, 2019-03574, 2020-05123, and 2022-01747-02). The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from primarily isolated as part of previous studies for which ethical approval was obtained. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
SS: Conceptualization, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. UG: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. GS: Data curation, Writing – original draft, Writing – review & editing. CH: Data curation, Writing – original draft, Writing – review & editing. JC: Data curation, Writing – original draft, Writing – review & editing. JK: Data curation, Writing – original draft, Writing – review & editing. AU: Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. LH: Resources, Supervision, Writing – original draft, Writing – review & editing. FL: Conceptualization, Data curation, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Swedish Cancer Society (grant numbers CAN 2020/0710, CAN 2020/0709, CAN 2022/2021, CAN 2022/1971 and CAN 2023/2807), Swedish Research Council (2021-00859), Lund Medical Faculty (ALF), Skåne University Hospital Research Funds (Gerdtham), The Cancer Research Fund at Malmö General Hospital, Skåne County Council’s Research and Development Foundation (REGSKANE-622351), The Hjelm Family Foundation for Medical research, Gösta Jönsson Research Foundation, the Foundation of Urological Research (Ove and Carin Carlsson bladder cancer donation), and Hillevi Fries Research Foundation and FORTE (grant number 2023-01128). Gerdtham wants to thank STIAS (Stellenbosch Institute for Advanced Study) for providing him with the ideal conditions to complete this paper. The funding sources had no role in the study design, data analyses, interpretation of the results, or writing of the manuscript.
JC has received consulting fees from AstraZeneca, Ferring, Ipsen, Roche, and Janssen; has received speaker fees from Bristol Myers Squibb, Pfizer, Merck Sharp & Dohme, Janssen, Astellas, Nucleix, and Roche; has received honoraria for membership in advisory boards from Ferring, Roche, Gilead, Photocure, Pfizer, Bristol Myers Squibb, QED Therapeutics, and Janssen; and has received research funding from Roche. AU has research funding from Bayer, the healthcare business of Merck KGaA, Darmstadt, Germany, Pierre Fabre. AU also received consulting or advisory role form Astellas Pharma, Janssen-Cilag, Merck & Co., Kenilworth, NJ, Pierre Fabre, Pfizer, Roche, and the healthcare business of Merck KGaA, Darmstadt, Germany.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1556881/full#supplementary-material
1. Sjödahl G, Lauss M, Lövgren K, Chebil G, Gudjonsson S, Veerla S, et al. A molecular taxonomy for urothelial carcinoma. Clin Cancer Res. (2012) 18:3377–86. doi: 10.1158/1078-0432.CCR-12-0077-T
2. Taber A, Christensen E, Lamy P, Nordentoft I, Prip F, Lindskrog SV, et al. Molecular correlates of cisplatin-based chemotherapy response in muscle invasive bladder cancer by integrated multi-omics analysis. Nat Commun. (2020) 11:4858. doi: 10.1038/s41467-020-18640-0
3. Sjödahl G, Abrahamsson J, Holmsten K, Bernardo C, Chebil G, Eriksson P, et al. Different responses to neoadjuvant chemotherapy in urothelial carcinoma molecular subtypes. Eur Urol. (2022) 81:523–32. doi: 10.1016/j.eururo.2021.10.035
4. Groeneveld CS, Pfister C, Culine S, Harter V, Krucker C, Fontugne J, et al. Basal/squamous and Mixed subtype bladder cancers present poor outcomes after neoadjuvant chemotherapy in the VESPER trial. Ann Oncol. (2024) 36(1):89–98. doi: 10.1016/j.annonc.2024.09.008
5. Vale JA. Neoadjuvant chemotherapy in invasive bladder cancer: update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur Urol. (2005) 48:202–205; discussion 205-206. doi: 10.1016/j.eururo.2005.04.006
6. SNRUBC. Svenska nationella kvalitetsregistret för Urinblåse- och urinvägscancer (SNRUBC). Umea: The Swedish National Quality Register for Bladder and Urinary Tract Cancer (2022). Available at: https://statistik.incanet.se/Urinblasecancer/ (Accessed May 7, 2024).
7. Alfred Witjes J, Max Bruins H, Carrión A, Cathomas R, Compérat E, Efstathiou JA, et al. European association of urology guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2023 guidelines. Eur Urol. (2024) 85:17–31. doi: 10.1016/j.eururo.2023.08.016
8. Liu W, Tian J, Zhang S, Yang E, Shen H, Li F, et al. The utilization status of neoadjuvant chemotherapy in muscle-invasive bladder cancer: a systematic review and meta-analysis. Minerva Urol Nephrol. (2021) 73:144–53. doi: 10.23736/S2724-6051.19.03648-8
9. Joyce DD, Sharma V, Williams SB. Cost-effectiveness and economic impact of bladder cancer management: an updated review of the literature. Pharmacoeconomics. (2023) 41(7):751–69. doi: 10.1007/s40273-023-01273-8
10. Husereau D, Drummond M, Augustovski F, de-Bekker-Grob E, Briggs AH, Carswell C, et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. BMJ. (2022) 376:e067975. doi: 10.1016/j.jval.2021.11.1351
11. Häggström C, Hagberg O, Gårdmark T, Aljabery F, Ströck V, Hosseini A, et al. Cohort profile: bladder cancer data base Sweden (BladderBaSe) 2.0. BMJ Open. (2022) 12:e064898. doi: 10.1136/bmjopen-2022-064898
12. Ullén A, Aljabery F, Dahlman P, Falkman K, Gårdmark T, Jerlström T, et al. Swedish national guidelines on advanced and metastatic urothelial carcinoma: 2024 update. Scandinavian J Urol press. (2025).
13. Olah C, Reis H, Hoffmann MJ, Mairinger F, Ting S, Hadaschik B, et al. Predictive value of molecular subtypes and APOBEC3G for adjuvant chemotherapy in urothelial bladder cancer. Cancer Med. (2023) 12:5222–32. doi: 10.1002/cam4.v12.5
14. Sternberg CN, Skoneczna I, Kerst JM, Albers P, Fossa SD, Agerbaek M, et al. Immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-pT4 or N+ M0 urothelial carcinoma of the bladder (EORTC 30994): an intergroup, open-label, randomised phase 3 trial. Lancet Oncol. (2015) 16:76–86. doi: 10.1016/S1470-2045(14)71160-X
15. Bajorin DF, Witjes JA, Gschwend JE, Schenker M, Valderrama BP, Tomita Y, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. (2021) 384:2102–14. doi: 10.1056/NEJMoa2034442
16. Dumont C, Aregui A, Hauchecorne M, Lefèvre M, Aussedat Q, Reignier PL, et al. Safety and efficacy of preoperative chemotherapy for muscle-invasive bladder cancer in elderly patients. World J Urol. (2023) 41:2715–22. doi: 10.1007/s00345-023-04561-2
17. Joyce DD, Wymer KM, Sharma V, Moriarty JP, Borah BJ, Geynisman DM, et al. Comparative cost-effectiveness of neoadjuvant chemotherapy regimens for muscle-invasive bladder cancer: Results according to VESPER data. Cancer. (2022) 128:4194–202. doi: 10.1002/cncr.v128.24
18. Catto JWF, Khetrapal P, Ricciardi F, Ambler G, Williams NR, Al-Hammouri T, et al. Effect of robot-assisted radical cystectomy with intracorporeal urinary diversion vs open radical cystectomy on 90-day morbidity and mortality among patients with bladder cancer: A randomized clinical trial. JAMA. (2022) 327:2092–103. doi: 10.1001/jama.2022.7393
19. Kulkarni GS, Alibhai SM, Finelli A, Fleshner NE, Jewett MA, Lopushinsky SR, et al. Cost-effectiveness analysis of immediate radical cystectomy versus intravesical Bacillus Calmette-Guerin therapy for high-risk, high-grade (T1G3) bladder cancer. Cancer. (2009) 115:5450–9. doi: 10.1002/cncr.v115:23
20. Eriksson P, Marzouka NA, Sjödahl G, Bernardo C, Liedberg F, Höglund M. A comparison of rule-based and centroid single-sample multiclass predictors for transcriptomic classification. Bioinformatics. (2022) 38:1022–9. doi: 10.1093/bioinformatics/btab763
21. Diagnosis Related Group (DRG) (2020). Available online at: https://hmsa.com/portal/PROVIDER/zav_pel.fh.DIA.650.htm (Accessed May 7, 2024).
22. Data and Statistics. International monetary fund . Available online at: http://www.imf.org/external/pubs/ft/weo/2009/01/weodata/weoselser.aspx?c=144&t=1 (Accessed 2nd May).
23. Whitehead SJ, Ali S. Health outcomes in economic evaluation: the QALY and utilities. Br Med Bull. (2010) 96:5–21. doi: 10.1093/bmb/ldq033
24. TLV. Hur ska vi utvärdera och hur ska vi betala? Hälsoekonomiska bedömningar och betalningsmodeller för precisionsmedicin och ATMP. (2021). Available at: https://www.tlv.se/download/18.6dab39ff179179457163977e/1619976447278/Sammanfattning_Rapport_atmp_20210430.pdf (Accessed May 7, 2024).
25. SBU. SBU (Statens Beredning för medicinsk och social utvärdering). Stockholm: Swedish Agency for Health Technology Assessment and Assessment of Scoial Services (2017).
26. Harnan S, Tappenden P, Cooper K, Stevens J, Bessey A, Rafia R, et al. Tumour profiling tests to guide adjuvant chemotherapy decisions in early breast cancer: a systematic review and economic analysis. Health Technol Assess. (2019) 23:1–328. doi: 10.3310/hta23300
27. Orellana TJ, Kim H, Beriwal S, Bhargava R, Berger J, Buckanovich RJ, et al. Cost-effectiveness analysis of tumor molecular classification in high-risk early-stage endometrial cancer. Gynecol Oncol. (2022) 164:129–35. doi: 10.1016/j.ygyno.2021.10.071
28. Christofyllakis K, Bittenbring JT, Thurner L, Ahlgrimm M, Stilgenbauer S, Bewarder M, et al. Cost-effectiveness of precision cancer medicine-current challenges in the use of next generation sequencing for comprehensive tumour genomic profiling and the role of clinical utility frameworks (Review). Mol Clin Oncol. (2022) 16:21. doi: 10.3892/mco.2021.2453
29. Sparano JA, Gray RJ, Makower DF, Pritchard KI, Albain KS, Hayes DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med. (2018) 379:111–21. doi: 10.1056/NEJMoa1804710
30. Kukreja JB, Metcalfe MJ, Qiao W, Kamat AM, Dinney CPN, Navai N. Cost-effectiveness of robot-assisted radical cystectomy using a propensity-matched cohort. Eur Urol Focus. (2020) 6:88–94. doi: 10.1016/j.euf.2018.07.001
31. Machleid F, Ho-Wrigley J, Chowdhury A, Paliah A, Poon HL, Pizzo E. Cost-utility analysis of robotic-assisted radical cystectomy for bladder cancer compared to open radical cystectomy in the United Kingdom. PloS One. (2022) 17:e0270368. doi: 10.1371/journal.pone.0270368
32. Hemenway G, Lewis B, Ghatalia P, Anari F, Plimack ER, Kokate R, et al. Neoadjuvant chemotherapy with accelerated methotrexate, vinblastine, doxorubicin, and cisplatin in patients with muscle-invasive bladder cancer: A retrospective age-stratified analysis on safety and efficacy. Eur Urol Oncol. (2023) 6:431–6. doi: 10.1016/j.euo.2022.06.005
33. Ho MD, Black AJ, Zargar H, Fairey AS, Mertens LS, Dinney CP, et al. The effect of cisplatin-based neoadjuvant chemotherapy on the renal function of patients undergoing radical cystectomy. Can Urol Assoc J. (2023) 17:301–9. doi: 10.5489/cuaj.8570
34. Fosså SD, Haugnes HS, Dahl AA, Kiserud CE, Fosså A, Skalleberg J, et al. Adverse Health Outcomes and Global Quality of Life in Long-term Testicular Cancer Survivors: A longitudinal 30-year perspective. Ann Oncol. (2023) 32(12):1165–74. doi: 10.1016/j.annonc.2023.09.3101
35. Kollberg P, Chebil G, Eriksson P, Sjödahl G, Liedberg F. Molecular subtypes applied to a population-based modern cystectomy series do not predict cancer-specific survival. Urol Oncol. (2019) 37:791–9. doi: 10.1016/j.urolonc.2019.04.010
36. Morera DS, Hasanali SL, Belew D, Ghosh S, Klaassen Z, Jordan AR, et al. Clinical parameters outperform molecular subtypes for predicting outcome in bladder cancer: results from multiple cohorts, including TCGA. J Urol. (2020) 203:62–72. doi: 10.1097/JU.0000000000000351
37. Kamoun A, de Reyniès A, Allory Y, Sjödahl G, Robertson AG, Seiler R, et al. A consensus molecular classification of muscle-invasive bladder cancer. Eur Urol. (2020) 77:420–33. doi: 10.1016/j.eururo.2019.09.006
38. Sayyid RK, Bernardino R, Al-Daqqaq Z, Tiwari R, Al-Rumayyan M, Sildva T, et al. Association of extended core sampling with delayed intervention and pathologic outcomes for active surveillance patients A population-based analysis. Can Urol Assoc J. (2024) 18:E142–e151. doi: 10.5489/cuaj.8563
39. Hamidi H, Senbabaoglu Y, Beig N, Roels J, Manuel C, Guan X, et al. Molecular heterogeneity in urothelial carcinoma and determinants of clinical benefit to PD-L1 blockade. Cancer Cell. (2024) 42:2098–112.e2094. doi: 10.1016/j.ccell.2024.10.016
40. Koll FJ, Döring C, Herwig L, Hoeh B, Wenzel M, Cano Garcia C, et al. Impact of consensus molecular subtypes on survival with and without adjuvant chemotherapy in muscle-invasive urothelial bladder cancer. J Clin Pathol. (2023) 78(1):19–27. doi: 10.1136/jcp-2023-208973
41. Liedberg F, Abrahamsson J, Bernardo C, Bläckberg M, Edsjö A, Heidenblad M, et al. UROSCAN and UROSCANSEQ: a large-scale multicenter effort towards translation of molecular bladder cancer subtypes into clinical practice - from biobank to RNA-sequencing in real time. Scand J Urol. (2023) 57:2–9. doi: 10.1080/21681805.2022.2159519
42. Cotillas EA, Bernardo C, Veerla S, Liedberg F, Sjödahl G, Eriksson P. A versatile and upgraded version of the lundTax classification algorithm applied to independent cohorts. J Mol Diagnostics. (2024) 26:1081–101. doi: 10.1016/j.jmoldx.2024.08.005
43. Höglund M, Bernardo C, Sjödahl G, Eriksson P, Axelson H, Liedberg F. The Lund taxonomy for bladder cancer classification - from gene expression clustering to cancer cell molecular phenotypes, and back again. J Pathol. (2023) 259:369–75. doi: 10.1002/path.6062
44. Flegar L, Kraywinkel K, Zacharis A, Aksoy C, Koch R, Eisenmenger N, et al. Treatment trends for muscle-invasive bladder cancer in Germany from 2006 to 2019. World J Urol. (2022) 40:1715–21. doi: 10.1007/s00345-022-04017-z
Keywords: cost-effectiveness analysis, muscle invasive bladder cancer, molecular subtype, neoadjuvant chemotherapy, radical cystectomy
Citation: Saha S, Gerdtham U-G, Sjödahl G, Häggström C, Catto JWF, Kelly JD, Ullén A, Holmberg L and Liedberg F (2025) Cost-effectiveness of de-escalated molecular subtype dependent use of neoadjuvant chemotherapy in patients with muscle-invasive bladder cancer in a Swedish setting. Front. Oncol. 15:1556881. doi: 10.3389/fonc.2025.1556881
Received: 07 January 2025; Accepted: 07 March 2025;
Published: 02 April 2025.
Edited by:
Bartosz Malkiewicz, Wroclaw Medical University, PolandReviewed by:
Sara Mucherino, University of Naples Federico II, ItalyCopyright © 2025 Saha, Gerdtham, Sjödahl, Häggström, Catto, Kelly, Ullén, Holmberg and Liedberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sanjib Saha, c2FuamliLnNhaGFAbWVkLmx1LnNl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.