 Ye Han
Ye Han Hong Yu1
Hong Yu1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 15 April 2025
Sec. Surgical Oncology
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1550429
Study objective: Phyllodes tumors of the breast (PT) are rare fibroepithelial tumors with varied clinical and histopathological characteristics, and standardized with wide margins in surgery, a systemic retrospective study of PT could improve our understanding of prognosis.
Design: We conducted a retrospective study spanning 2008-2021, which included 333 cases of PT for chart review. We used logistic regression and comparison tests to evaluate the association between clinical features and local recurrence (LR), as well as to summarize overall survival (OS) and disease-free survival (DFS).
Setting: Phyllodes tumors of the breast exhibit a propensity for a higher recurrence rate. The surgical protocol advocates for achieving wide margins (>1 cm), which presents challenges in clinical practice due to the ambiguity in defining such margins.
Participants: A retrospective screening identified 333 cases of PT for inclusion in the study. Comprehensive data for this analysis was extracted from the clinical patient records.
Interventions: Post-operation, all cases were subjected to a standardized protocol of regular follow-up , with subsequent documentation of follow-up data.
Main outcome measures: At a median follow-up of 79 (inter-quartile range: 28-109) months, recurrence occurred in 9.7% (19/196) of benign, 18.4% (18/98) of borderline, and 28.2% (11/39) of malignant tumors. Local recurrence was not reduced with enlarged margin width (<1 cm vs. >1 cm: odds ratio (OR)=0.84; 95% CI, 0.48 to 1.47; p=0.53), but it was associated with age (<40 vs. >40: OR=2.04; 95% CI, 1.13 to 3.68; p=0.01). LR was significantly correlated with mitosis (<5/HFP vs. >=5/HFP: OR=0.56; 95% CI, 0.32 to 0.98; p=0.003), stromal overgrowth (yes vs. no: OR=0.43; 95% CI, 0.32 to 0.98; p=0.014), and stromal atypia (mild vs. marked: OR=0.59; 95% CI, 0.30 to 1.17; p=0.003).
Result and conclusion: This retrospective study confirmed that recurrence and prognosis were not associated with wide margins in the real world, as suggested by previous guidelines, possibly due to the influence of characteristics such as age, stromal overgrowth, stromal atypia, and mitosis.
Phyllodes tumors (PT) of the breast are rare fibroepithelial neoplasms that comprise approximately 1% of all breast tumors (1). They were named after their distinctive leaf-like histologic architectures, first described in 1838, and exhibit variant histological behaviors spanning from benign, borderline, to malignant subtypes, which are subclassified by the World Health Organization (WHO) since 1981 (2, 3). Histologically, morphological and biological features such as stromal overgrowth, stromal cellularity, stromal atypia, epithelial hyperplasia, tumor necrosis, tumor margins, and mitotic activity per 10 high power field (HPF) count are described to subclassify PT and evaluate the rate of local recurrence (4). The standardized treatment for PT involves surgical removal with wide margins ≥1cm and individually tailored adjuvant therapy, as per National Comprehensive Cancer Network (NCCN) guidelines (5). However, benign phyllodes tumors (BPT) is no longer required for wide margins (≥1cm) since 2022 NCCN guidelines.
The prognosis of PT is conceptually evaluated by local recurrence (LR), overall survival rate (OS) and disease-free survival (DFS) (6). The LR rate of PTs varies from 10% to 40% (average 15%) with distant metastasis reported in approximately 25% of malignant PTs. The 5-year DFS rate is around 80%, considering both LR and distant metastasis, and the 5-year estimated OS and DFS rates are reported to be approximately 85% and 77%, respectively (7, 8). Time to local recurrence has been identified as a predictor of survival in patients with soft tissue sarcoma (9). LR has been reported to be correlated with several independent factors, including positive margins, age, grade, tumor size, cellular atypia, stromal overgrowth, and mitoses (10, 11). However, despite the standardized recommendation for wide margins in surgery, recent debates have cast doubt on the significance of margin width in reducing LR. Some researchers have suggested that there is no significant difference in LR between surgery with narrow margins (<1cm) or wide margins (>1cm) (10).
The ongoing controversy regarding the recommended margins has created a dilemma in the treatment of PT, and further investigation is necessary. Therefore, we conducted a study to collect available data and review the prognosis of PT in our institution to clarify the optimal surgical approach and identify independent risk factors.
All the data analyzed in this study were collected from Asian patients treated at Shengjing Hospital of China Medical University between 2008 and 2021, as shown in Table 1. Patients who were diagnosed with phyllodes tumors were identified retrospectively from the Hospital Information System (HIS) and classified using the AJCC 8th Edition classification system (12). All clinical characteristics, including age, tumor size, clinical presentation, surgery methods, adjuvant therapy, local recurrences, and systemic metastases, were recorded and analyzed retrospectively. The histological features analyzed in this study included stromal cellularity, stromal overgrowth, cellular atypia, mitosis, borders, heterogeneous component, and focal infiltration.

Table 1. Clinicopathologic features of phyllodes tumors patient in the study.
Surgical treatment for PT included various procedures such as lumpectomy (LE), wide local excision (WLE), breast conserving surgery (BCS), and mastectomy. LE involved the removal of the tumor with a negative margin (width of margin <1cm) through an open incision entrance. On the other hand, WLE involved the removal of the tumor with adjacent tissue (width of margin >1cm). BCS, in contrast, involved the removal of the tumor with pathologic wide margins for malignant tumors. All surgical treatment data were collected according to the medical records.
Patients diagnosed with malignant PT were required to visit the hospital every 3 months after surgery. For benign and borderline PT, patients were advised to have a follow-up visit every 3 to 6 months after resection through outpatient visits or telephone interviews. Breast ultrasound and Mammogram were recommended during the follow-up visit. Follow-up results for all patients were collected through the HIS system and telephonic interviews over the past 13 years. The diagnosis of PT was histologically confirmed and recorded by the Pathologic Department of Shengjing Hospital of China Medical University, including any local recurrence and metastasis.
Raw data of clinical characteristics, surgical treatment, and pathological features were compared using the χ2 test or Fisher’s exact test. The 5-year DFS and OS were presented using Kaplan-Meier curves and analyzed using the log-rank test. Multivariate regression analysis was performed using the Cox proportional hazards model to determine the risk factors for LR. A p-value of <0.05 was considered statistically significant.
Between January 2008 and December 2021, a total of 333 cases of PT were screened at Shengjing Hospital of China Medical University. The median age of the patients was 44 years (inter-quartile range, IQR: 34-52 years). The median tumor size was 3cm (IQR:2-4) for benign PT, 4cm (IQR:3-6.75) for borderline PT, and 4cm (IQR:3-8) for malignant PT, with a range of 1cm to 22cm. Among all cases, 58.9% (N=196) were benign PT, 29.4% (N=98) were borderline PT, and 11.7% (N=39) were malignant PT. The median follow-up time was 89.7 months (range: 3-194 months), and all patients were female and diagnosed by the Pathology Department at Shengjing Hospital of China Medical University.
The clinical characteristics of the patients are presented in Table 1, stratified by benign PT, borderline PT, and malignant PT. Benign PTs were found to be significantly smaller in size compared to borderline and malignant PTs (p=0.013). The median age of the patients for the three subtypes was 40.5 years for benign PT, 45 years for borderline PT, and 47.8 years for malignant PT, with a significant difference observed (p<0.05). The majority of the PT cases were unilateral, with 54.7% (N=182) occurring in the left breast, 45.0% (N=150) occurring in the right breast, and only 0.3% (N=1) being bilateral.
In terms of primary management, the most common approach was lumpectomy (47.7%), followed by WLE (31.2%), mastectomy (15.6%), and breast-conserving surgery (5.4%). LE was the initial operative management for 63.3% of benign PT cases, 30.6% of borderline PT cases, and 12.8% of malignant PT cases. Borderline and malignant PT cases were more likely to undergo WLE (34.7% and 28.2%, respectively) and mastectomy (26.5% and 48.7%, respectively) than benign PT cases. Tumor size was classified as T1 in 76.3% of cases (<5cm), T2 in 18.3% of cases (≥5cm and <10cm), and T3 in 5.4% of cases (≥10cm).
Regarding surgical margins, in this study, lumpectomy (LE) was defined as a narrow margin (margin <1 cm), while wide local excision (WLE), breast-conserving surgery (BCS), and mastectomy were defined as wide margins (margin >1 cm). Among patients with benign phyllodes tumors (PT), 124 (63.3%) underwent LE, and 72 (36.7%) underwent surgery with wide margins. In the case of borderline PT, 30 (30.6%) cases underwent LE, and 68 (69.4%) cases were treated with wide margins. For malignant PT, 5 (12.8%) patients underwent LE, and 34 (87.2%) patients underwent surgery with wide margins. However, in this study, the disease-free survival (DFS) and local recurrence rates were not significantly correlated with wide margins, even for malignant PT.
Regarding lymph node evaluation, 6.6% of patients underwent sentinel lymph node biopsy (SLNB), and 1.5% underwent axillary lymph node dissection (ALND), which revealed only one metastatic lymph node. A second operation was required in 1.0% of borderline PT cases and 10.3% of malignant PT cases, and all second operations involved mastectomy. While initial negative margin width was less than 1cm in 68.4% of benign PT cases, 36.7% of borderline PT cases, and 10.3% of malignant PT cases, only 1.5% of women expressed a willingness to undergo a second operation.
The study found that mild stromal cellularity was present in 31.6% (62/196) of benign PT, 45.9% (45/98) of borderline PT, and only 2.6% (1/39) of malignant PT. This difference was statistically significant (p<0.0001). Pushing borders were observed in 58.3% (194/333) of cases, while infiltrative borders were observed in only 5.4% (18/333) of cases. Stromal atypia, mitosis, intra-tumoral necrosis, and stromal overgrowth were significantly associated with histopathological grades (p<0.05). Malignant PT were more likely to exhibit marked stromal atypia and overgrowth, higher mitotic activity, and intra-tumoral necrosis compared to benign and borderline PT (Table 1).
Local recurrence (LR) occurred in 14.7% (n=49) of the entire cohort, with a median follow-up of 42 months. The LR rate was 10.2% (20/196) for benign, 18.4% (18/98) for borderline, and 28.2% (11/39) for malignant PT. LR rates were assessed based on age, tumor size, final closest margin, surgical management, PT grade, and histopathological features (Table 2). Logistic regression analysis revealed a significant correlation between LR and age [<40 vs. ≥40: odds ratio (OR)=2.04; 95%CI, 1.13 to 3.68; p=0.008]. Histologically, LR was associated with marked stromal atypia (mild vs. marked, odds ratio [OR] =0.43; 95%CI, 0.25 to 0.77; p=0.0031), stromal overgrowth (yes vs. no, odds ratio [OR] =0.56; 95%CI, 0.32 to 0.98; p=0.01), and active mitosis per 10 high power fields (HPF) (<5 vs. ≥5: OR=0.88; 95%CI, 0.49 to 1.59; p=0.03) (Figures 1–3).
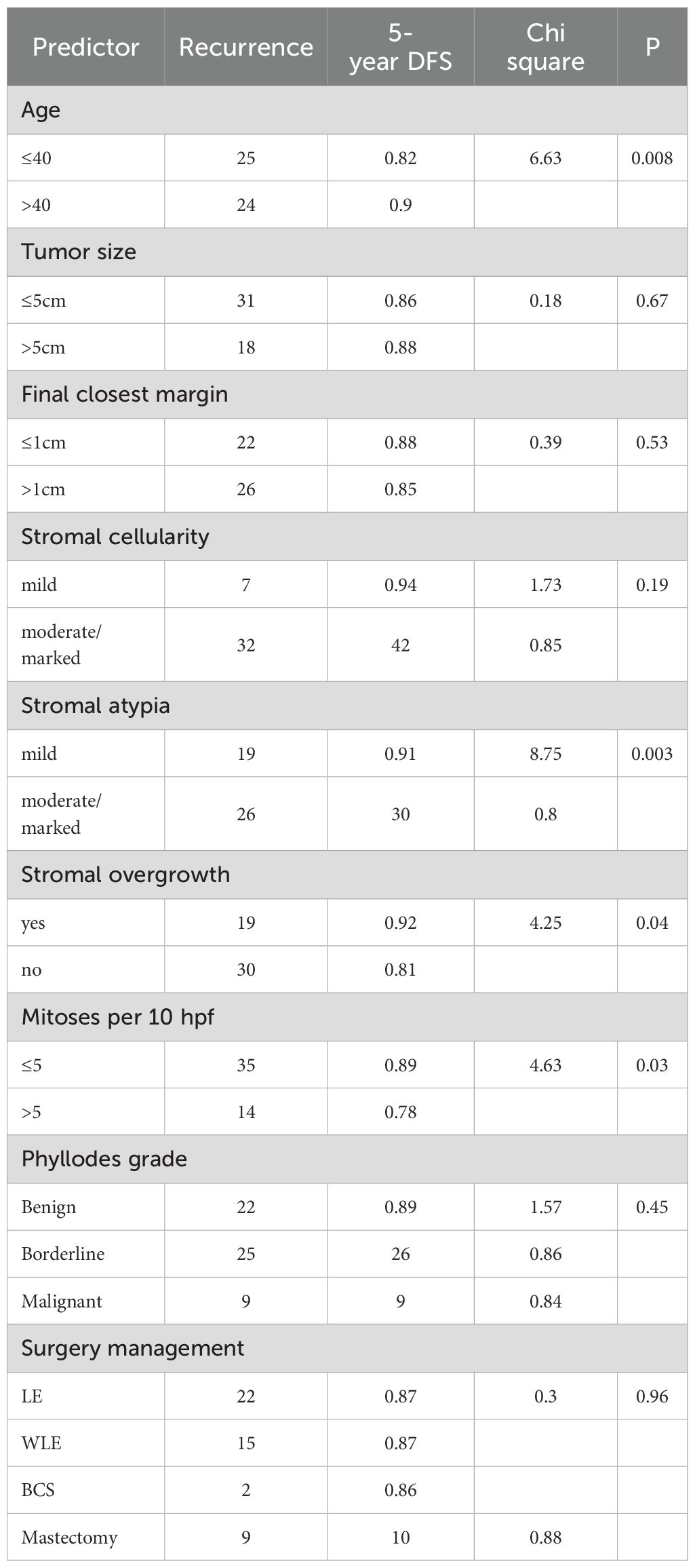
Table 2. Kaplan-Meirer model predicting 5-year DFS.
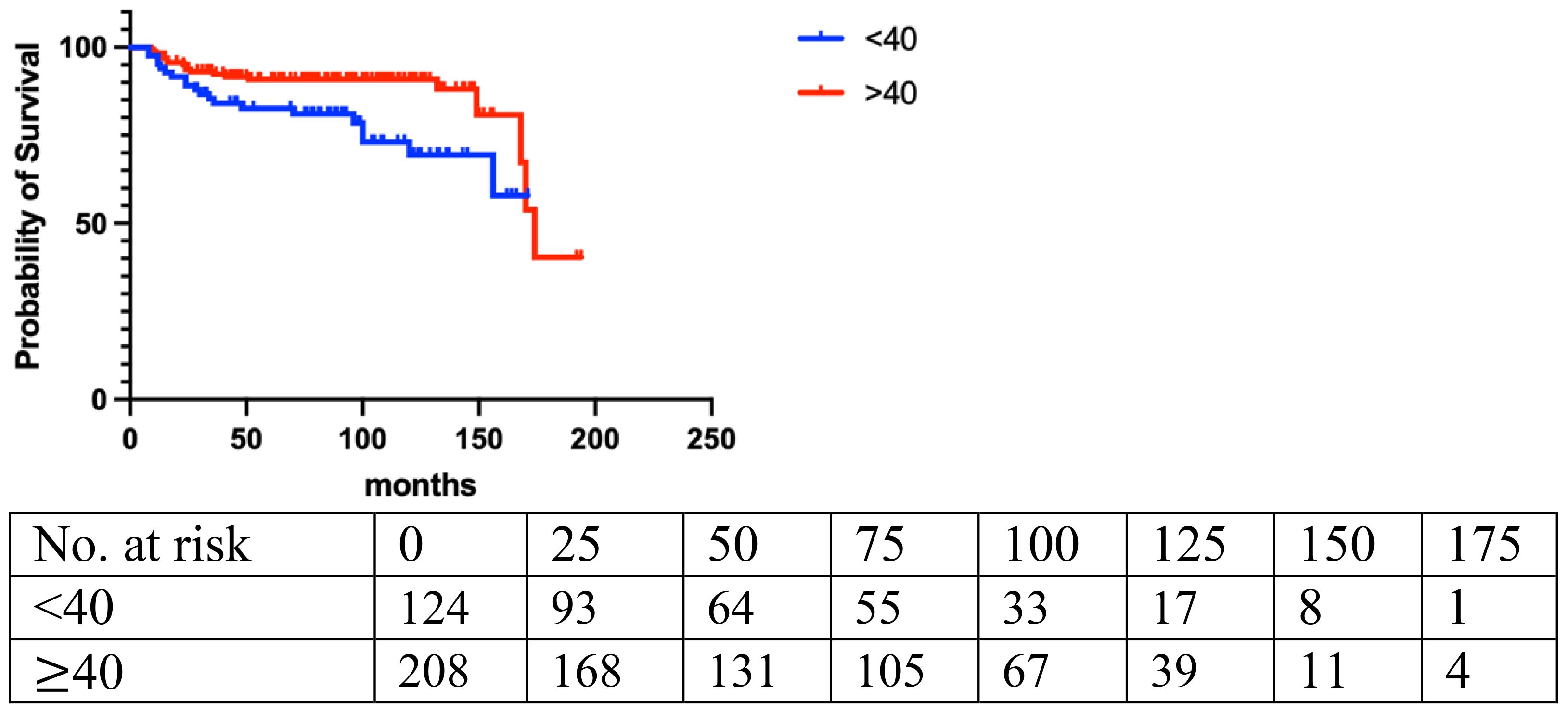
Figure 1. Age (p=0.008).
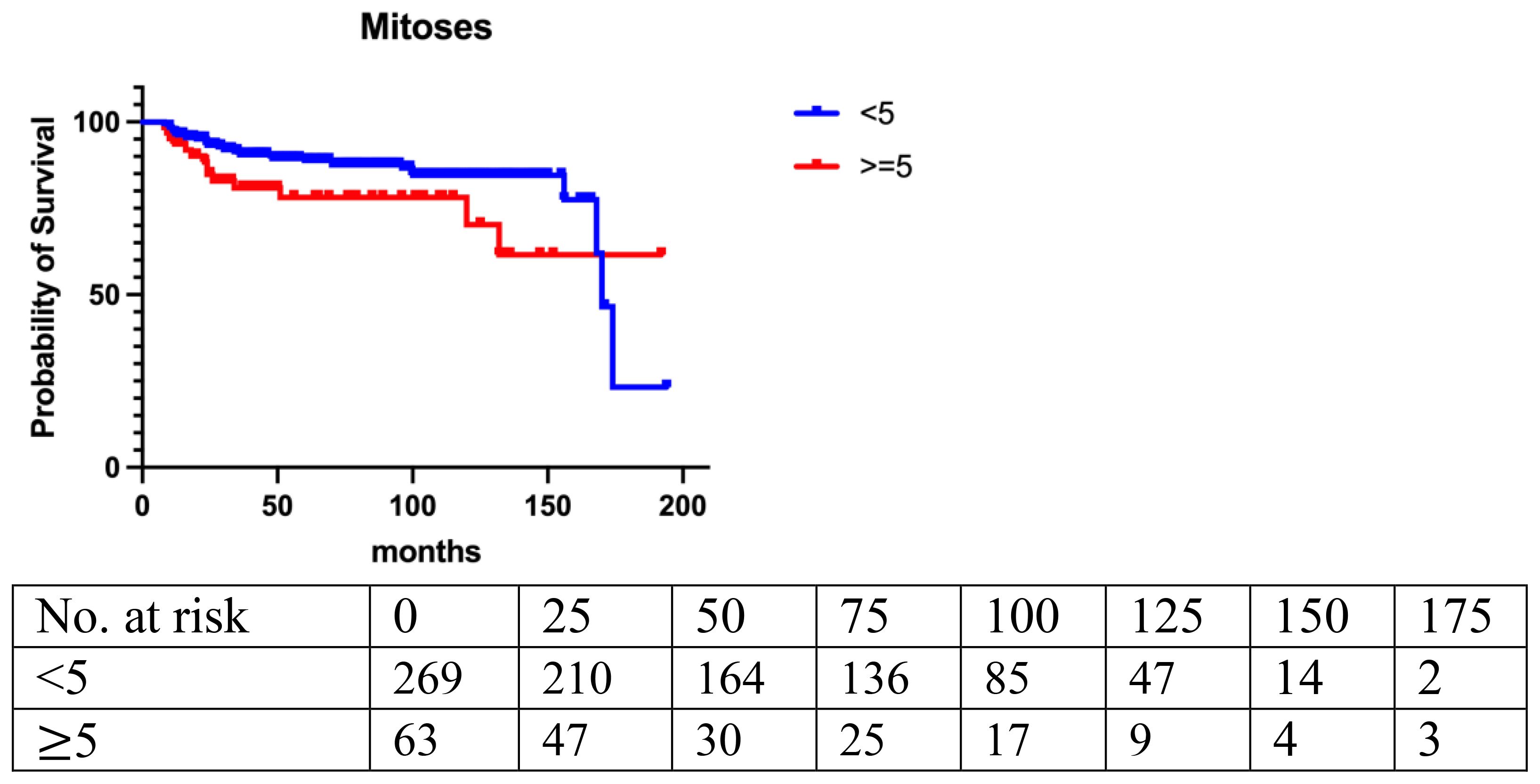
Figure 2. Mitoses (p=0.025).
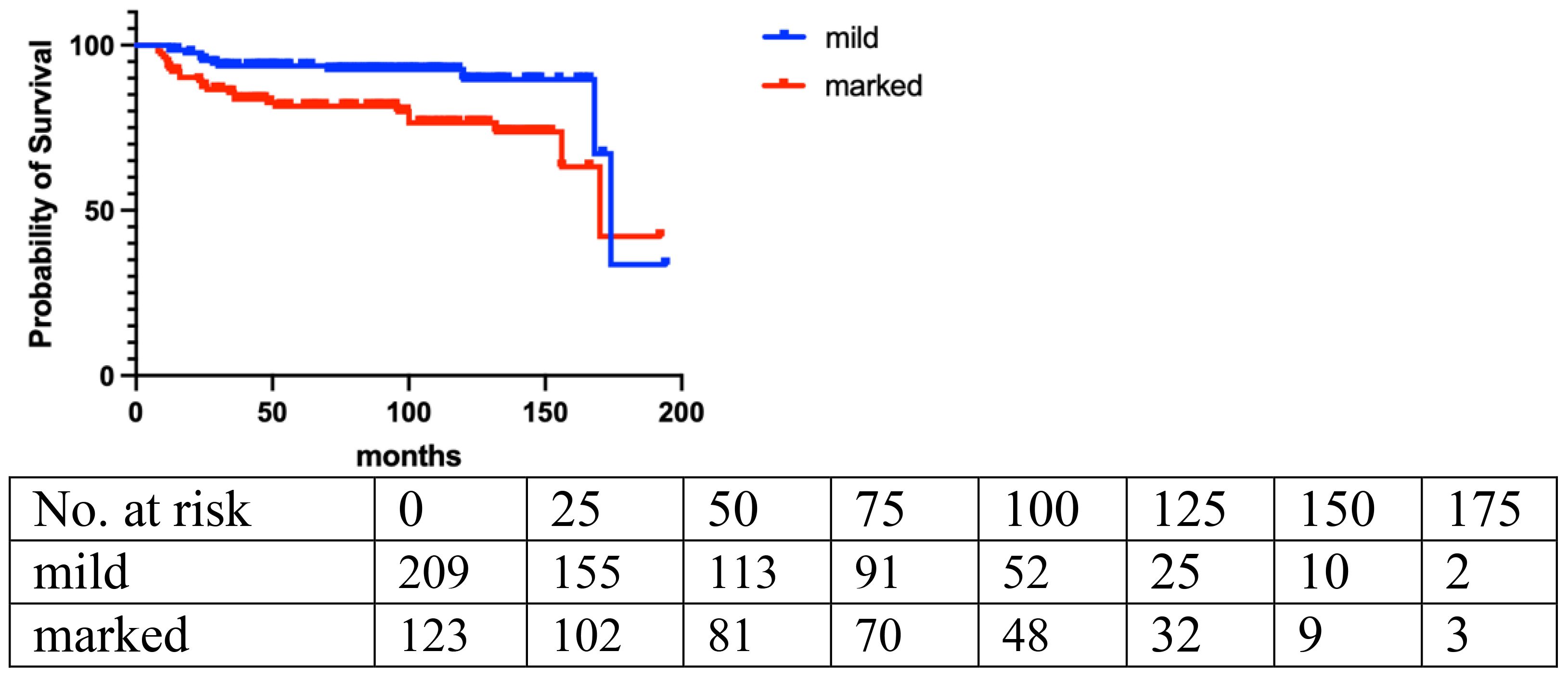
Figure 3. Stromal atypia (p=0.004).
Logistic regression analysis revealed no significant association between LR and surgical management (LE vs. wide margin: OR=0.89; 95% CI, 0.48 to 1.66; p=0.46), or tumor size (<5cm vs. >5cm: OR=0.88; 95% CI, 0.49 to 1.59; p=0.67). There was no significant association between LR and final margin, surgery management, stromal cellularity, histological border, and stromal overgrowth at diagnosis (Table 3, Figures 4, 5). The correlation between LR and various surgical management strategies was analyzed in each subgroup graded by histopathological diagnosis (p=0.09 in benign PT, p=0.3 in borderline PT, p=0.56 in malignant PT), and no significance was identified (Table 4).
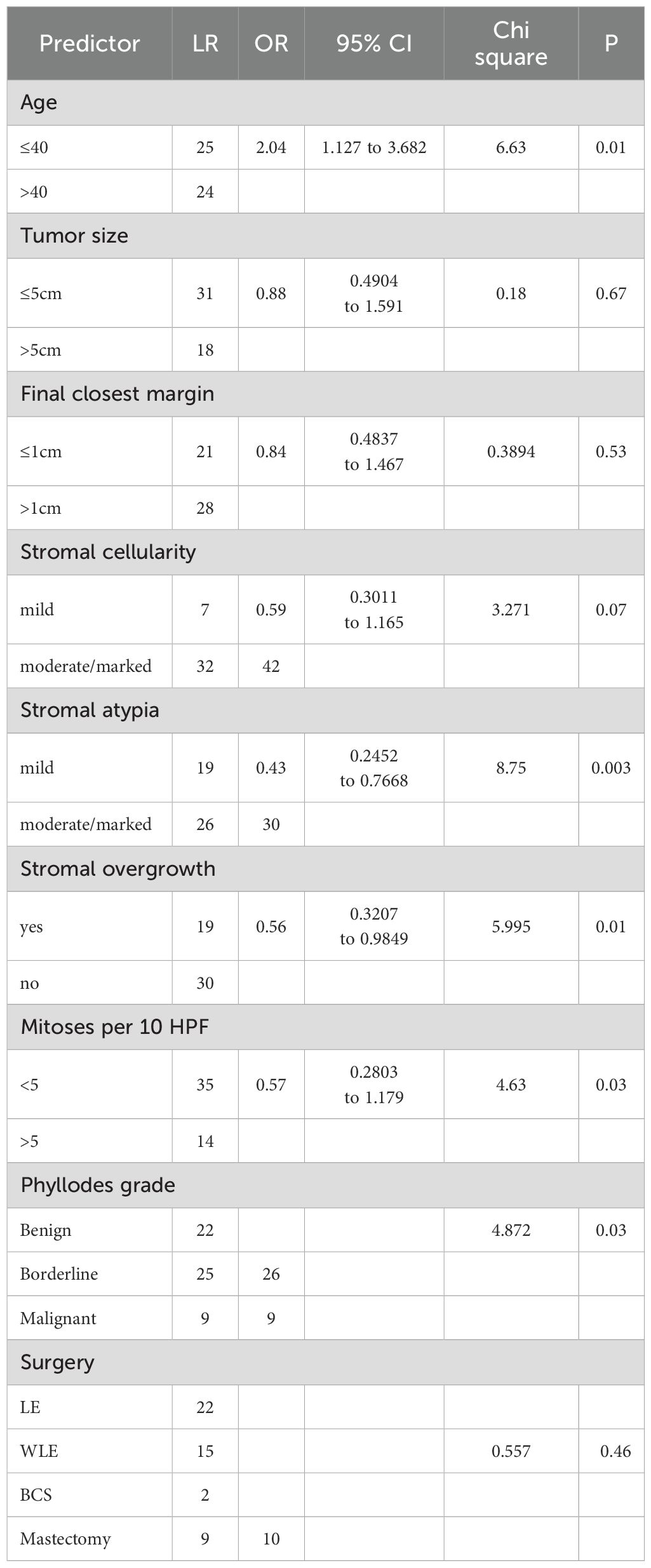
Table 3. Logistic regression models predicting likelihood of local recurrence.
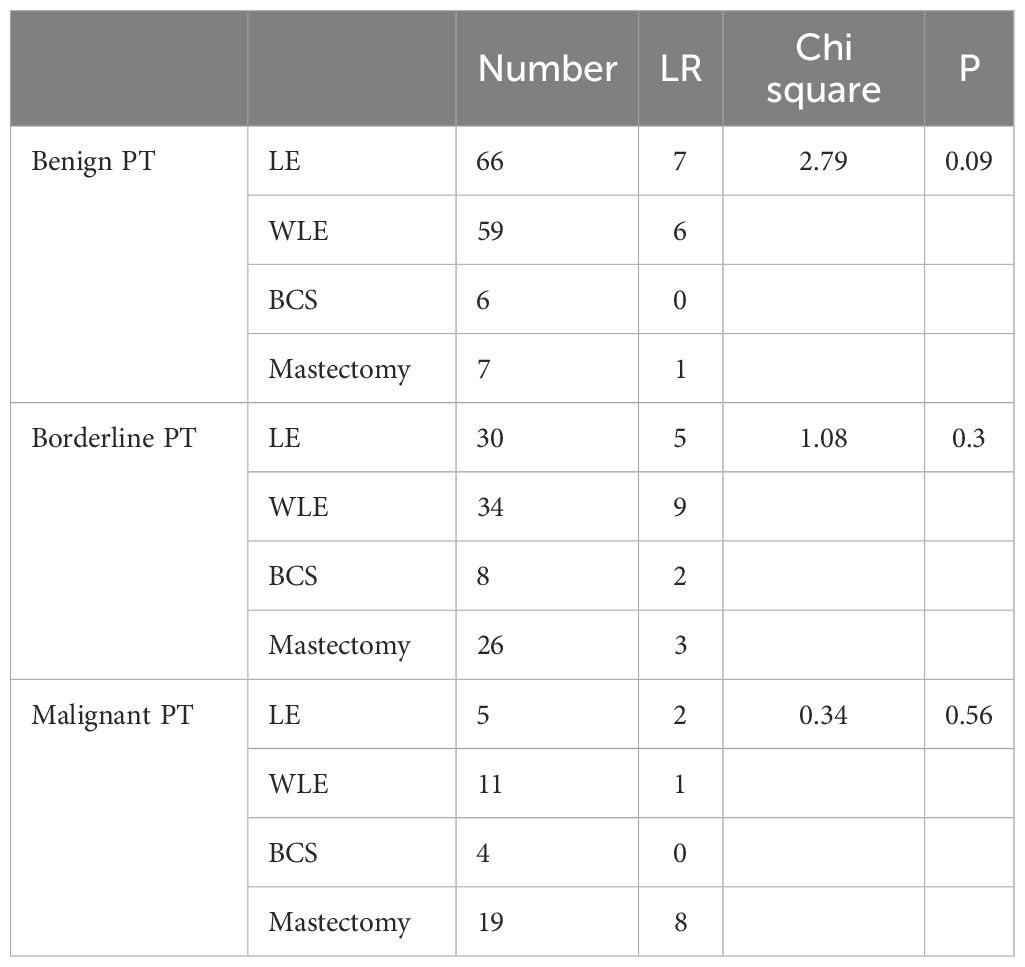
Table 4. The correlation between LR and surgical managements in subgroups by log-rank test.
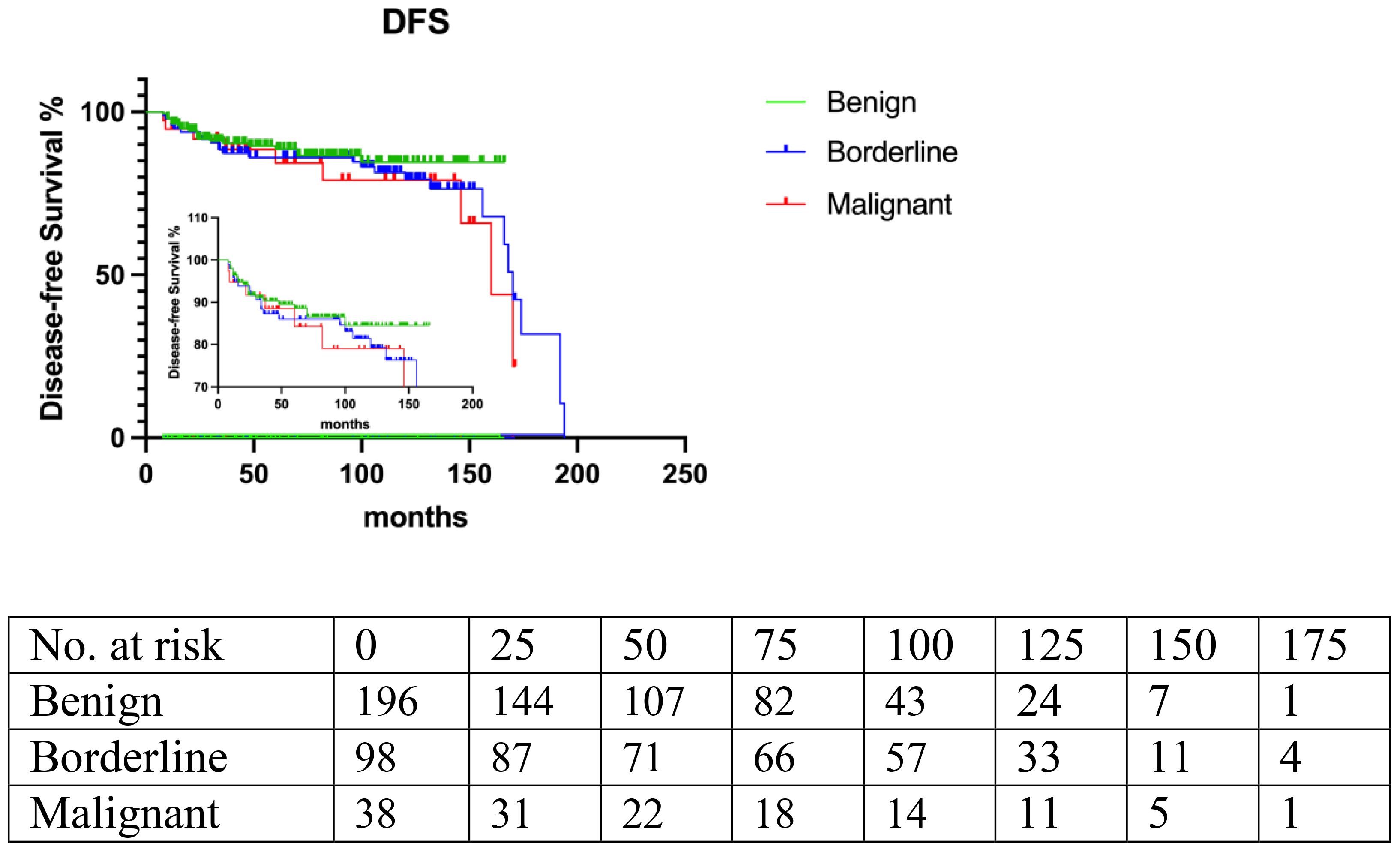
Figure 4. Histopathological grade: benign, borderline, malignant. (p=0.06).
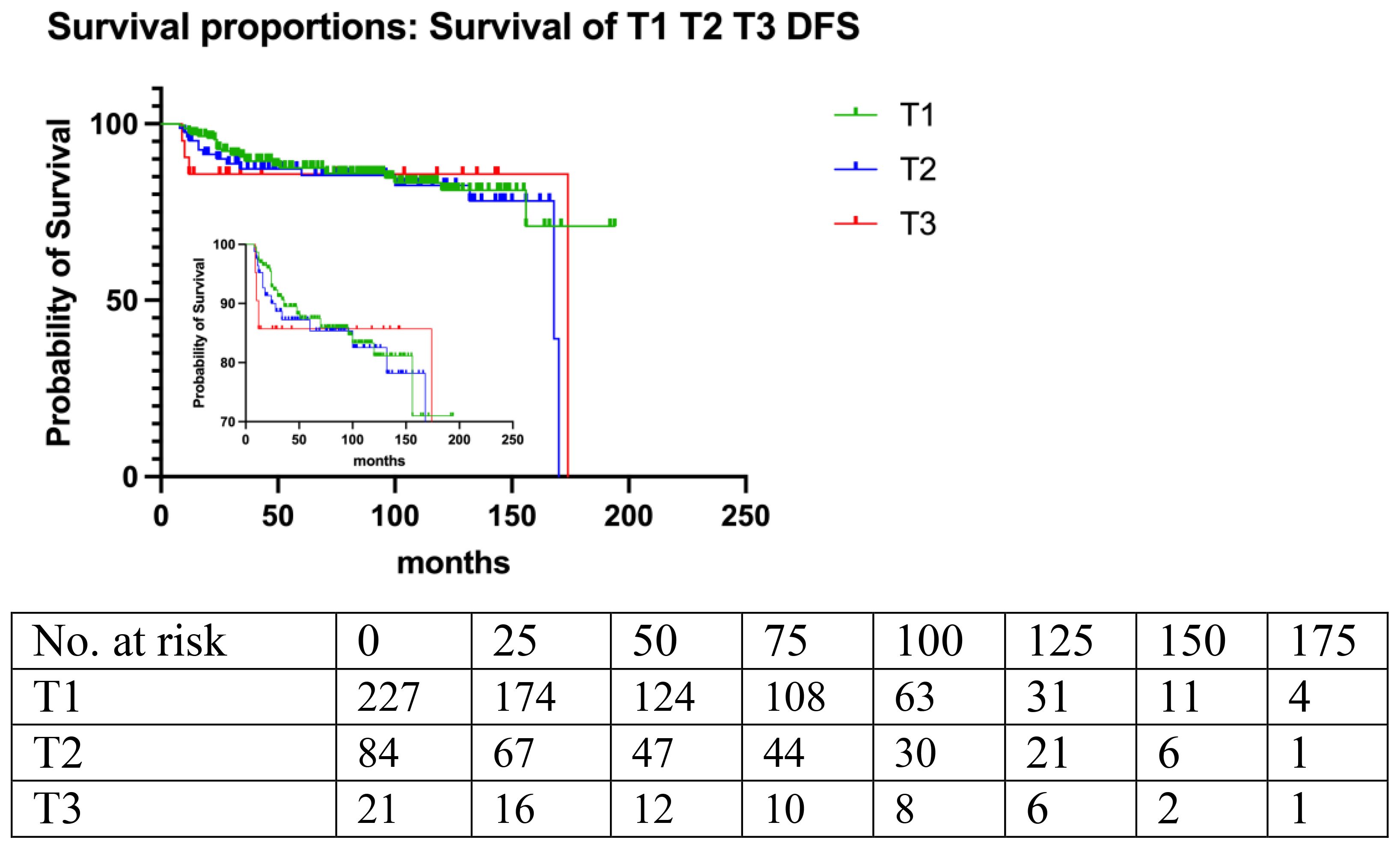
Figure 5. Tumor size (p=0.41).
All cases of local recurrence were managed with secondary surgical interventions. Specifically, for benign phyllodes tumors (PTs), 13 recurrent cases underwent local excision with wide margins. In the case of borderline PTs, 2 recurrent cases were treated with local excision and wide margins, and one of these cases received adjuvant radiotherapy (RT). The remaining 17 cases of recurrence were managed with mastectomy. For malignant PTs, 3 cases were treated with mastectomy, and 8 cases underwent local removal of the recurrent tumors. This approach reflects the complexity of managing recurrent PTs, particularly in the context of their variable biological behavior and the need to balance surgical margins with the potential benefits of adjuvant therapy.
A limited number of patients underwent adjuvant radiotherapy (n=3, 0.9%) or chemotherapy (n=2, 0.6%), therefore, the evaluation of the effectiveness of adjuvant therapy was limited.
Kaplan-Meier regression analysis showed that the 5-year disease-free survival (DFS) rates were 86.6% for benign PT, 86.3% for borderline PT, and 83.5% for malignant PT according to histological grade. The DFS rates tended to decrease from benign to malignant subtype, although this trend did not reach statistical significance (p=0.06).
Multivariate COX proportional hazards model analysis revealed that significant risk factors for local recurrence (LR) and DFS included stromal atypia (HR=1.96, 95% CI, 1.38 to 2.798; p<0.001), stromal overgrowth (HR=1.96, 95% CI, 1.03 to 2.8; p<0.05), and mastectomy (HR=0.34, 95% CI, 0.13 to 0.84; p<0.05) (Table 3, Figure 6).
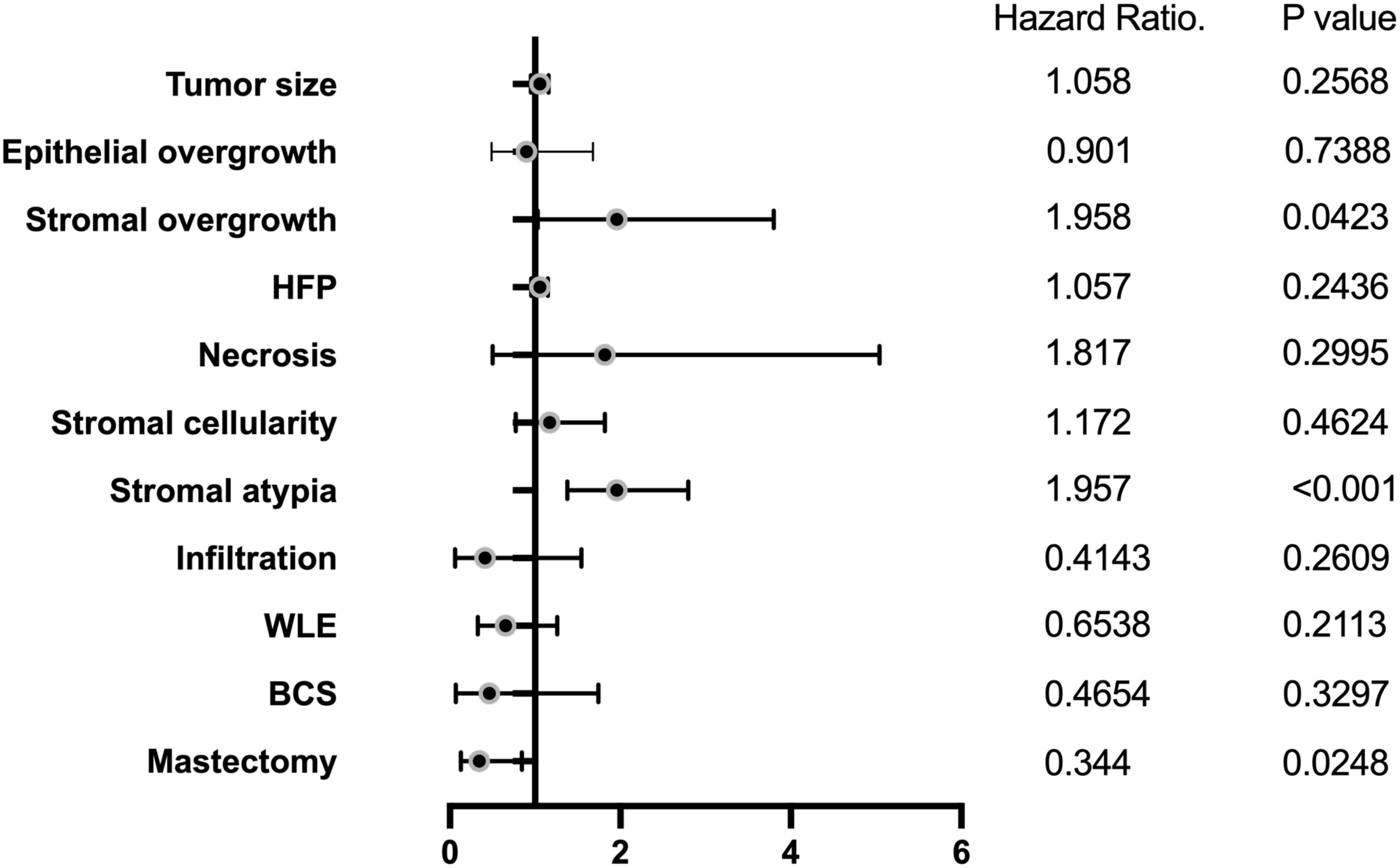
Figure 6. Multiple predictors of local recurrence.
This study aimed to assess the management and prognosis of patients diagnosed with PT in a single institution over a 13-year period. A total of 333 patients were included in the analysis, and the study evaluated various clinical and histological factors to predict the recurrence rate. Most cases underwent lumpectomy, widely lumpectomy, breast conserving surgery, or mastectomy, despite the NCCN guideline recommending wide margin (>1cm) as the standard management for borderline PT and MPT. Surprisingly, the study found that wide margin was not significantly associated with local recurrence or DFS. Instead, age, stromal overgrowth, stromal atypia, and mitosis were identified as independent risk factors for recurrence, rather than surgical margin.
The diagnosis of PT relies on mammography, ultrasound, MRI and pathology (13). However, these imaging techniques often yield nonspecific results, which can complicate decision-making regarding surgical management (14). In this study, we found that the age of patients and tumor size increased gradually according to the pathological classification of benign, borderline, and malignant PT (p<0.05). Although the concordant diagnostic frequency of PT was found to be about 73.3% in previous reviews by comparing intraoperative frozen sections to permanent histology (15), this dilemma still undermines the value of intraoperative frozen section in the diagnosis of PT, as well as the wide excisional rate of borderline or malignant PT. Moreover, up to 20% of positive margins are identified in postoperative histological examination, which may require additional re-excision according to guidelines (16). The rate of re-excision ranges from 10% to 50% due to variable reasons (17). In our study, most cases of benign PT (93.4%, 183/196) underwent surgical lumpectomy with negative margins due to uncertainty in the rapid frozen section or core needle biopsy (CNB) results. On the other hand, 65.3% (64/98) of borderline PT and 41.0% (16/39) of malignant PT underwent lumpectomy with negative margins. The surgical margin was less than 1 cm in 68.4% of benign PT, 36.7% of borderline PT, and 10.3% of malignant PT, which significantly reduced after comparing with the final histopathology results (p<0.0001). With sufficient tissue for standard and immunological pathology examinations for borderline and malignant PT, we were able to verify the pathologic diagnosis and recommend a second resection with a wider margin in accordance with the NCCN guidelines.
In our study, we found that over half (54.7%) of cases underwent LE, which is contrary to current guidelines. However, only a small percentage of patients were willing to undergo re-excision or mastectomy, with most opting for observation due to uncertain oncologic benefit, low rates of residual PT, and cosmetic concerns (18). Despite this deviation from guidelines, there was no significant difference in local recurrence rates between the surgical treatment cohorts, indicating that recurrence was not a result of surgical management. These findings align with a recent study published in the Journal of Clinical Oncology, which found that wide margins were not an independent risk factor for local recurrence (18). Another study of 246 cases reported that 44% of benign PT underwent re-excision, but only 9% were found to have residual PT in the margins (19). In our study, we found no significant difference in LR rate between patients with benign PT who underwent re-excision and those who underwent observation alone (p=0.7 vs. 0.2). Even all risk factors are considered, there was no difference in the local recurrence of benign PT between open surgery and ultrasound-guided vacuum-assisted biopsy, suggesting that tumor margins may not be a significant factor in predicting recurrence (20). Therefore, there is an urgent need to determine the appropriate management strategies, including surgical margins and prognostic risk factors, for patients with PT.
Benign PT accounts for a significant proportion of PT (60-75%), with a reported lower LR rate of 10-20% when treated with WLE (21). Several investigations have shown no difference in LR between LE and WLE, potentially minimizing the risk of surgical margins (22, 23). Our study found that 11.22% of benign PT recurred, with no significant difference among various surgical management approaches (p=0.09), which is consistent with previous reports. However, the confusing and rapidly frozen pathological outcomes in real-world practice have hindered the WLE rate for borderline PT, which accounts for 10-20% of PT and has been identified with an LR rate of 14-30% by previous studies (24, 25). In a cohort of 90 cases of PT, 52 exhibited positive surgical margins. However, there was no significant difference observed between those who underwent re-excision and those who did not. The current literature provides limited and inconclusive evidence that broad margins in surgical management definitively minimize recurrence (23). In addition, it is noteworthy that the LR rate of borderline PT after WLE has been reported as high as 25% (26). Continuing with our investigation, in our sample, the LR rate of borderline PT was found to be 19.4%. Of the patients, 30.6% underwent lumpectomy (LE), while 34.7% underwent WLE. However, our retrospective investigation did not reveal a significant difference between the four surgical care techniques (p=0.30), thus supporting previous conclusions. For malignant PT cases, surgical management with wide margins or mastectomy was recommended, followed by adjuvant radiotherapy or chemotherapy as necessary (27, 28). It is interesting to note that Spanheimer et al. reported a relatively low LR rate of 12% in 71 patients with borderline or malignant PT, which is comparable to the rate seen in benign PT cases (29). In our study, the LR rate of malignant PT was found to be 28.2%, with most patients undergoing mastectomy (48.7%) or WLE (28.2%) and a median survival time of 160 months. Our results also showed no significant difference in recurrence between different surgical managements or margins, as determined by log-rank testing. However, we acknowledge that a larger, multicenter investigation is needed to confirm the effectiveness of surgical margins in reducing local recurrence in PT cases. Such research could help to guide optimal surgical management and improve patient outcomes.
As surgical margins or different surgical managements were found to be not significant predicting factors of local recurrence (LR) in our retrospective investigation, we further explored other potential factors. Our series revealed a relatively low LR rate of 15.6% (n=52) over a 13-year follow-up period, which is consistent with a recent report of an LR rate of 6.3% during an 8-year follow-up (30). Our analytic results show slightly higher local recurrence (LR) rates compared to a previous large series of 546 cases, which reported a 2.7% LR rate in a 10-year follow-up. In our retrospective study, the 5-year disease-free survival (DFS) rate was found to be 86.6% for benign PT, 86.3% for borderline PT, and 83.5% for malignant PT, but the decline was not statistically significant (p=0.06). The 5-year DFS rates for subgroups classified by margins (<1cm and ≥1cm) were relatively high at 87.8% and 86.6%, respectively, with no significant difference observed (p=0.70), consistent with recent reports. One such study reported a 5-year DFS rate of 87.8% for margin-negative patients and 85.1% for margin-involved patients, concluding that margin status was not significantly associated with recurrence (31). Thind et al. conducted a meta-analysis of 10 retrospective studies based on MEDLINE and Embase (1990 to 2019) to investigate whether margins <1cm are sufficient for excision to prevent local recurrence (LR) in PT cases. Their study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (32). The meta-analysis concluded that margins <1cm may provide adequate excision to prevent LR in PT cases. In another meta-analysis, it was concluded that different surgical management strategies with margins <1cm were not significantly associated with the risk of local recurrence (LR) in all grades of PT. The meta-analysis systematically analyzed 34 articles with Newcastle-Ottawa Scale (NOS) scores above 5 using RevMan5.3 software (33). These findings support the importance of individualized surgical management plans for PT cases based on the tumor’s characteristics and patient factors. Numerous large series around the world demonstrated that positive margins were not significantly associated with LR, including Bedi D. (N=270) (34), Belkacemi et al. (N=443) (35), Cheng et al. (N=182) (36), Tan et al. (N=605) (37), and Co et al. (N=465) (38); Increasing data has shown that negative margins are not necessarily relevant to LR and disease-free survival (DFS). However, the margins issue remains challenging to draw a conclusion due to the lack of supporting data. The rarity of PT and the limited availability of high-quality data from multiple institutions and prospective studies makes it difficult to draw definitive conclusions about the optimal management of surgical margins.
In our investigation, we examined several clinical and histological parameters, including age, tumor size, surgical margins, surgical procedure, stromal atypia, stromal overgrowth, and mitoses, to explore the underlying predicting factors of LR. Our results showed that age, stromal overgrowth, stromal atypia, and mitoses were significant risk factors for LR, as identified by logistic regression analysis. Specifically, age (<40 vs. ≥40), stromal atypia (mild vs. marked), stromal overgrowth (yes vs. no), and mitoses (<5 vs. ≥5) were found to be independent prognostic indicators for LR by log-rank regression analysis. Interestingly, our analysis showed that tumor size and surgical managements were not associated with DFS. However, other studies have reported different findings. For instance, Olaya J reported a LR rate of 14.8% with high-grade and mastectomy as high-risk factors, while a single center covering 192 cases revealed LR of 16.1% and distant metastasis of 6.3% in the 10-year follow-up (39). We came to the conclusion that tumor size, hemorrhage and margin status were independent predictors of LR and OS (40). A Canadian retrospective study examining 150 PT found that the overall LR was 7.3%, with 45% of benign, 27% of borderline, and 27% of malignant lesions (41). It is important to note that the need for wide margins to reduce LR varies based on the histopathologic type of PT. Borderline and malignant PT require a wide margin to reduce the risk of LR, while benign PT has no significance regarding margins. Recent research has also shown that negative margins may not be significant when LR reduction surgery is performed, particularly in the case of benign PT.
The NCCN guidelines suggest that radiotherapy should be considered for malignant PT when the risk of LR is high, which occurs in around 10-15% of cases (42, 43). Several studies have recommended adjuvant radiation for malignant PT to reduce the risk of LR, but its effect on overall survival has been found to be minimal (44, 45). A multivariate study of 1353 MPT patients with a follow-up of up to 331 months using Kaplan-Meier curves and Cox proportional hazards analysis found that adjuvant radiation did not improve overall survival (46). Another retrospective study of 108 PT patients with a follow-up of 56 months found no significant difference in the LR rate between borderline and malignant PT patients who did or did not receive adjuvant radiotherapy (47). The 5-year overall survival rates were 52% and 45% in the radiation and non-radiation groups, respectively (p=0.54). In our series, only 8.6% and 2.9% of malignant PT cases underwent adjuvant radiotherapy and chemotherapy, respectively. Adjuvant radiotherapy is not recommended for benign PT patients to prevent LR due to the potential risk of radiation-induced second malignancy (48). Therefore, adjuvant radiotherapy is controversial and supported mainly for large and high-grade phyllodes tumors (2, 35, 49).
There are several limitations to our study, which was a single-center and retrospective analysis, potentially introducing bias. The clinical characteristics of patients with benign, borderline, and malignant PT were not well-balanced, which may have impacted the statistical analyses. Additionally, larger studies are needed to further explore optimal surgical margins and prognostic indicators for PT.
Despite these limitations, our study contributes to the long-term prognosis of PT by providing a relatively long median follow-up period. Our findings suggest that wider surgical margins may not be necessary for all types of PT, as we found no significant difference in LR rate or DFS among different surgical managements. We also identified age, stromal overgrowth, stromal atypia, and mitotic rate as important risk factors for prognosis using multivariate COX proportional hazards analysis.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethics Community of Shengjing Hospital with No. 2020PS071K. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
YH: Validation, Funding acquisition, Writing – original draft, Writing – review & editing. WJ: Resources, Validation, Investigation, Supervision, Writing – original draft. HY: Data curation, Methodology, Writing – original draft. HS: Conceptualization, Formal analysis, Supervision, Visualization, Writing – review & editing. CL: Data curation, Writing – original draft.
The author(s) declare that financial support was received for the research and/or publication of this article. The project is supported by the following fundings: National Natural Science Foundation of China, No. 82002807; Applied Basic Programs of Science and Technology Commission Foundation of Liaoning Province, No. 2022JH2/101500002; 345 Talent Project of Shengjing Hospital of China Medical University, Grant Number: M0721.
All the colleagues contributed to the treatment of the patients. Thanks for their professional treatment.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Pitsinis V, Moussa O, Hogg F, McCaskill J. Reconstructive and oncoplastic surgery for giant phyllodes tumors: A single center’s experience. World J Plast Surg (2017) 6(2):233–7.
2. Bogach J, Shakeel S, Wright FC, Hong NJL. Phyllodes tumors: A scoping review of the literature. Ann Surg Oncol (2022) 29(1):446–59. doi: 10.1245/s10434-021-10468-2
3. Bevers TB, Helvie M, Bonaccio E, Calhoun KE, Daly MB, Farrar WB, et al. Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw (2018) 16(11):1362–89. doi: 10.6004/jnccn.2018.0083
4. Lissidini G, Mulè A, Santoro A, Papa G, Nicosia L, Cassano E, et al. Malignant phyllodes tumor of the breast: a systematic review. Pathologica (2022) 114(2):111–20. doi: 10.32074/1591-951X-754
5. Ji Y, Zhong Y, Zheng Y, Hu H, Min N, Wei Y, et al. Surgical management and prognosis of phyllodes tumors of the breast. Gland Surg (2022) 11(6):981–91. doi: 10.21037/gs-21-877
6. Park HJ, Ryu HS, Kim K, Shin KH, Han W, Noh DY. Risk factors for recurrence of Malignant phyllodes tumors of the breast. In Vivo (2019) 33(1):263–9. doi: 10.21873/invivo.11470
7. Lin CC, Chang HW, Lin CY, Chiu CF, Yeh SP. The clinical features and prognosis of phyllodes tumors: a single institution experience in Taiwan. Int J Clin Oncol (2013) 18(4):614–20. doi: 10.1007/s10147-012-0442-4
8. Mallick S, Joshi NP, Roy S, Gandhi AK, Pandit S, Sharma D, et al. Malignant and borderline phyllodes tumor of breast treated with a multi-modality approach in a tertiary cancer care center in North India. South Asian J Cancer (2016) 5(1):1–3. doi: 10.4103/2278-330X.179696
9. Liang Y, Guo T, Hong D, Xiao W, Zhou Z, Zhang X. Time to Local recurrence as a predictor of survival in patients with soft tissue sarcoma of the extremity and abdominothoracic wall. Front Oncol (2020) 10:599097. doi: 10.3389/fonc.2020.599097
10. Yu CY, Huang TW, Tam KW. Management of phyllodes tumor: A systematic review and meta-analysis of real-world evidence. Int J Surg (2022) 107:106969. doi: 10.1016/j.ijsu.2022.106969
11. Lu Y, Chen Y, Zhu L, Papa G, Nicosia L, Cassano E, et al. Local recurrence of benign, borderline, and Malignant phyllodes tumors of the breast: A systematic review and meta-analysis. Ann Surg Oncol (2019) 26(5):1263–75. doi: 10.1245/s10434-018-07134-5
12. Giuliano AE, Edge SB, Hortobagyi GN. Eighth edition of the AJCC cancer staging manual: Breast cancer. Ann Surg Oncol (2018) 25(7):1783–5. doi: 10.1245/s10434-018-6486-6
13. Panda KM. Naik r. a clinicopathological study of benign phyllodes tumour of breast with emphasis on unusual features. J Clin Diagn Research: JCDR (2016) 10(7):EC14–7. doi: 10.7860/JCDR/2016/18025.8184
14. Efared B, Ebang GA, Tahiri L, Sidibé IS, Erregad F, Hammas N, et al. Phyllodes tumors of the breast: Clinicopathological analysis of 106 cases from a single institution. Breast Disease (2018) 37(3):139–45. doi: 10.3233/BD-170297
15. Abdelkrim SB, Trabelsi A, Bouzrara M, Boudagga MZ, Memmi A, Bakir DA, et al. Phyllodes tumors of the breast: A review of 26 cases. World J Oncol (2010) 1(3):129–34. doi: 10.4021/wjon2010.06.220w
16. Landercasper J, Whitacre E, Degnim AC, Al-Hamadani M. Reasons for re-excision after lumpectomy for breast cancer: insight from the American Society of Breast Surgeons Mastery (SM) database. Ann Surg Oncol (2014) 21(10):3185–91. doi: 10.1245/s10434-014-3905-1
17. Reyna C, DeSnyder SM. Intraoperative margin assessment in breast cancer management. Surg Oncol Clin N Am (2018) 27(1):155–65. doi: 10.1016/j.soc.2017.08.006
18. Rosenberger LH, Thomas SM, Nimbkar SN, Hieken TJ, Ludwig KK, Jacobs LK, et al. Contemporary multi-institutional cohort of 550 cases of phyllodes tumors (2007-2017) demonstrates a need for more individualized margin guidelines. J Clin Oncol (2021) 39(3):178–89. doi: 10.1200/JCO.20.02647
19. Moo TA, Alabdulkareem H, Tam A, Fontanet C, Lu Y, Landers A, et al. Association between recurrence and re-excision for close and positive margins versus observation in patients with benign phyllodes tumors. Ann Surg Oncol (2017) 24(10):3088–92. doi: 10.1245/s10434-017-5955-7
20. Chao X, Jin X, Tan C, Sun P, Cui J, Hu H, et al. Re-excision or “wait and watch”-a prediction model in breast phyllodes tumors after surgery. Ann Transl Med (2020) 8(6):371. doi: 10.21037/atm.2020.02.26
21. Jabeen D, Vohra LM, Siddiqui T, Raza AUN. Recurrent phyllodes tumour of the breast transforming to a fibrosarcoma. Cureus (2020) 12(3):e7457. doi: 10.7759/cureus.7457
22. Cowan ML, Argani P, Cimino-Mathews A. Benign and low-grade fibroepithelial neoplasms of the breast have low recurrence rate after positive surgical margins. Mod Pathol (2016) 29(3):259–65. doi: 10.1038/modpathol.2015.157
23. Ogunbiyi S, Perry A, Jakate K, Simpson J, George R. Phyllodes tumour of the breast and margins: How much is enough. Can J Surg (2019) 62(1):E19–21. doi: 10.1503/cjs.005718
24. Zelek L, Llombart-Cussac A, Terrier P, Pivot X, Guinebretiere JM, Le Pechoux C, et al. Prognostic factors in primary breast sarcomas: A series of patients with long-term follow-up. JCO (2003) 21(13):2583–8. doi: 10.1200/JCO.2003.06.080
25. Garlet BB, Zogbi L, de LJP, Favalli PP de S, Krahe FD. Recurrent borderline phyllodes tumor of the breast submitted to mastectomy and immediate reconstruction: Case report. Int J Surg Case Rep (2019) 60:25–9. doi: 10.1016/j.ijscr.2019.05.032
26. Barth RJ. Borderline and Malignant Phyllodes Tumors: How Often do They Locally Recur and is There Anything we can do About it? Ann Surg Oncol (2019) 26(7):1973–5. doi: 10.1245/s10434-019-07278-y
27. Wang F, Jia Y, Tong Z. Comparison of the clinical and prognostic features of primary breast sarcomas and Malignant phyllodes tumor. Japanese J Clin Oncol (2015) 45(2):146–52. doi: 10.1093/jjco/hyu177
28. Strode M, Khoury T, Mangieri C, Takabe K. Update on the diagnosis and management of Malignant phyllodes tumors of the breast. Breast (2017) 33:91–6. doi: 10.1016/j.breast.2017.03.001
29. Spanheimer PM, Murray MP, Zabor EC, Stempel M, Morrow M, Van Zee KJ, et al. Long-term outcomes after surgical treatment of Malignant/Borderline phyllodes tumors of the breast. Ann Surg Oncol (2019) 26(7):2136–43. doi: 10.1245/s10434-019-07210-4
30. Borhani-Khomani K, Talman MLM, Kroman N, Tvedskov TF. Risk of local recurrence of benign and borderline phyllodes tumors: A danish population-based retrospective study. Ann Surg Oncol (2016) 23(5):1543–8. doi: 10.1245/s10434-015-5041-y
31. Yoon KH, Kang E, Kim EK, Park SY, Shin HC. Recurrence is not associated with margin status in phyllodes tumor. Ann Surg Oncol (2023) 30(4):2154–61. doi: 10.1245/s10434-022-12997-w
32. Thind A, Patel B, Thind K, Isherwood J, Phillips B, Dhaliwal K, et al. Surgical margins for borderline and Malignant phyllodes tumours. Ann R Coll Surgeons England (2020) 102(3):165–73. doi: 10.1308/rcsann.2019.0140
33. Wei Y, Yu Y, Ji Y, Zhong Y, Min N, Hu H, et al. Surgical management in phyllodes tumors of the breast: a systematic review and meta-analysis. Gland Surg (2022) 11(3):513–23. doi: 10.21037/gs-21-789
34. Bedi D, Clark BZ, Carter GJ, Yu J, Fine JL, Villatoro TM, et al. Prognostic significance of three-tiered world health organization classification of phyllodes tumor and correlation to singapore general hospital nomogram. Am J Clin Pathol (2022) 158(3):362–71. doi: 10.1093/ajcp/aqac055
35. Belkacémi Y, Bousquet G, Marsiglia H, Ray-Coquard I, Magné N, Malard Y, et al. Phyllodes tumor of the breast. Int J Radiat Oncology Biology Physics (2008) 70(2):492–500. doi: 10.1016/J.IJROBP.2007.06.059
36. Cheng SP, Chang YC, Liu TP, Lee JJ, Tzen CY, Liu CL. Phyllodes tumor of the breast: the challenge persists. World J Surg (2006) 30(8):1414–21. doi: 10.1007/s00268-005-0786-2
37. Tan PH, Thike AA, Tan WJ, Thu MM, Busmanis I, Li H, et al. Predicting clinical behaviour of breast phyllodes tumours: a nomogram based on histological criteria and surgical margins. J Clin Pathol (2012) 65(1):69–76. doi: 10.1136/jclinpath-2011-200368
38. Co M, Chen C, Tsang JY, Tse G, Kwong A. Mammary phyllodes tumour: a 15-year multicentre clinical review. J Clin Pathol (2018) 71(6):493–7. doi: 10.1136/jclinpath-2017-204827
39. Olaya J, Sanjuan J, Luna RL, Casanova L. Risk factors for disease recurrence in women with phyllodes tumors of the breast in southern colombia: A nine-year cohort study. Cureus (2020) 12(5):e7951. doi: 10.7759/cureus.7951
40. Wei J, Tan YT, Cai YC, Yuan ZY, Yang D, Wang SS, et al. Predictive factors for the local recurrence and distant metastasis of phyllodes tumors of the breast: a retrospective analysis of 192 cases at a single center. Chin J Cancer (2014) 33(10):492–500. doi: 10.5732/cjc.014.10048
41. Lim RS, Cordeiro E, Lau J, Lim A, Roberts A, Seely J. Phyllodes tumors-the predictors and detection of recurrence. Can Assoc Radiol J (2021) 72(2):251–7. doi: 10.1177/0846537119899553
42. Kim YJ, Kim K. Radiation therapy for Malignant phyllodes tumor of the breast: An analysis of SEER data. Breast (Edinburgh Scotland) (2017) 32:26–32. doi: 10.1016/J.BREAST.2016.12.006
43. Gnerlich JL, Williams RT, Yao K, Jaskowiak N, Kulkarni SA. Utilization of radiotherapy for Malignant phyllodes tumors: analysis of the National Cancer Data Base, 1998-2009. Ann Surg Oncol (2014) 21(4):1222–30. doi: 10.1245/s10434-013-3395-6
44. Li J, Tsang JY, Chen C, Chan SK, Cheung SY, Wu C, et al. Predicting outcome in mammary phyllodes tumors: Relevance of clinicopathological features. Ann Surg Oncol (2019) 26(9):2747–58. doi: 10.1245/s10434-019-07445-1
45. Zeng S, Zhang X, Yang D, Wang X, Ren G. Effects of adjuvant radiotherapy on borderline and Malignant phyllodes tumors: A systematic review and meta-analysis. Mol Clin Oncol (2015) 3(3):663–71. doi: 10.3892/mco.2015.503
46. Zhao W, Tian Q, Zhao A, Wang B, Yang J, Wang L, et al. The role of adjuvant radiotherapy in patients with Malignant phyllodes tumor of the breast: a propensity-score matching analysis. Breast Cancer (Tokyo Japan) (2021) 28(1):110–8. doi: 10.1007/S12282-020-01135-7
47. Barth RJ, Wells WA, Mitchell SE, Cole BF. A prospective, multi-institutional study of adjuvant radiotherapy after resection of Malignant phyllodes tumors. Ann Surg Oncol (2009) 16(8):2288–94. doi: 10.1245/s10434-009-0489-2
48. Birch JM, Alston RD, McNally RJ, Evans DG, Kelsey AM, Harris M, et al. Relative frequency and morphology of cancers in carriers of germline TP53 mutations. Oncogene (2001) 20(34):4621–8. doi: 10.1038/sj.onc.1204621
Keywords: wide margin, phyllodes tumor, histology, prognosis, local recurrence
Citation: Han Y, Yu H, Li C, Jiang W and Shan H (2025) Exploring the clinical and histopathological characteristics on breast phyllodes tumors predictors and prognosis in a real world. Front. Oncol. 15:1550429. doi: 10.3389/fonc.2025.1550429
Received: 23 December 2024; Accepted: 11 February 2025;
Published: 15 April 2025.
Edited by:
Alejandro Martin Sanchez, Multidisciplinary Breast Center - Fondazione Policlinico Universitario A. Gemelli IRCCS, ItalyReviewed by:
Giovanni Tazzioli, University of Modena and Reggio Emilia, ItalyCopyright © 2025 Han, Yu, Li, Jiang and Shan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Jiang, MTg5NDAyNTU1MTJAMTYzLmNvbQ==; Huilian Shan, c2FuaGxAc2otaG9zcGl0YWwub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.