
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol., 24 February 2025
Sec. Cancer Immunity and Immunotherapy
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1525924
 Javier David Benitez Fuentes1*
Javier David Benitez Fuentes1* Jorge Bartolome Arcilla2,3
Jorge Bartolome Arcilla2,3 Antonio David Lazaro Sanchez4Alicia de Luna Aguilar5
Antonio David Lazaro Sanchez4Alicia de Luna Aguilar5 Kauzar Mohamed Mohamed6Kissy Guevara-Hoyer6,7
Kauzar Mohamed Mohamed6Kissy Guevara-Hoyer6,7 Pablo Ballestin Martinez8
Pablo Ballestin Martinez8 Miguel Borregon Rivilla1
Miguel Borregon Rivilla1 Asia Ferrandez Arias1
Asia Ferrandez Arias1 Silvia Sánchez-Ramon6,7
Silvia Sánchez-Ramon6,7 Alberto Ocaña2,3,9*
Alberto Ocaña2,3,9*Background: Immunotherapy has gained momentum with the discovery of novel antibodies targeting immunosuppressive proteins. HLA-E, a non-classical major histocompatibility complex class I (MHC-I) protein, exhibits immunosuppressive properties, potentially influencing tumor immune evasion mechanisms. The association between Human Leukocyte Antigen E (HLA-E) expression and outcomes in solid tumors remains unclear.
Methods: A systematic review of MEDLINE, Scopus, and the Cochrane Library up to March 15, 2024, was conducted following the PRISMA guidelines. Studies investigating HLA-E expression in solid tumors and its association with OS and DFS were included. Statistical analysis was performed using Comprehensive Meta-Analysis (version 3.0) with random-effects models.
Results: After screening 657 articles, 11 studies were included, comprising a total of 1781 patients. The studies encompassed a variety of cancer types, follow-up periods, and staging details, with the majority focusing on non-metastatic cases. Notably, three studies evaluated colorectal cancer, while others focused on pancreatic, esophageal, brain, renal cell, gastric, endometrial, cervical, and hepatocellular carcinomas. The mean age of the patients was 59.81 ± 2.01 years, and the median follow-up period was 57.45 ± 8.91 months. HLA-E expression demonstrated no statistically significant association with OS (HR 0.913, 95% CI = 0.567-1.469; P=0.707), with significant heterogeneity observed (I2 = 84%). However, HLA-E non-expression was significantly associated with improved DFS (HR 1.406, 95% CI = 1.027-1.930; P=0.03), with moderate heterogeneity (I2 = 45%).
Conclusion: This systematic review highlights that HLA-E expression in solid tumors could be a biomarker of better prognosis, measured by DFS. These findings align with the clinical benefit observed for agents targeting this pathway. However, further studies should be performed to confirm these preliminary observations.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024527598, identifier CRD42024527598.
In parallel with the development of personalized precision oncology treatments targeting key relevant genomic alterations, strategies acting on the immune system have demonstrated significant clinical activity (1). The approved therapies in this field target immunosuppressive proteins, therefore inducing the activation of the immune system (2). Among the different components of the immune system, human leukocyte antigen (HLA) proteins, including both class I and class II molecules, are key participants in immune regulation and immune escape in the cancer process (2, 3).
There are two major classes of HLA molecules: class I and class II. Class II HLA molecules, including HLA-DQ, HLA-DR, and HLA-DP, are primarily expressed on antigen-presenting cells (APCs) such as dendritic cells, macrophages, and B cells. These molecules play a critical role in presenting extracellular antigens to CD4+ T helper cells, thereby initiating and modulating adaptive immune responses. Dysregulation of HLA class II expression has been implicated in immune evasion by tumors, as reduced expression can impair the activation of CD4+ T cells and weaken antitumor immunity (3).
Class I HLA molecules are further divided into classical and non-classical subtypes (2). Classical type I HLA molecules (HLA-A, HLA-B, and HLA-C), are essential for immunosurveillance and cancer immunotherapy as T cells are presented with cellular antigens by this subtype (2, 4, 5). The non-classical HLA molecules, HLA-E, HLA-F, and HLA-G have immunosuppressive properties in contrast to traditional HLA-I molecules (2, 4, 5). HLA-E, found on chromosome 6, is formed by the association of a heavy chain and β2-microglobulin. This molecule presents peptides derived from the leader sequences of other MHC class I molecules, as well as potentially from pathogen-derived peptides (6). Its primary role is to enable Natural Killer (NK) cells to monitor the expression of the other class I HLA molecules, limiting NK action while also inhibiting T-cell cytotoxicity (6). Thus, HLA-E serves as a critical link between memory-driven adaptive immunity and the rapid response of innate immunity (5, 7–9).
Although it is frequently prevalent in trophoblast and tumor cells, HLA-E can be expressed at low levels in all nucleated cells (7, 10). Growing evidence indicates that tumors can use HLA-E expression to evade NK cell detection even in the absence of conventional class I HLA (8). A poor prognosis has been linked to HLA-E expression in various malignancies including colorectal cancer, gastric cancer, gynecological cancers, non-small cell lung cancer (NSCLC) and breast cancer (11–16).
Additionally, the tumor microenvironment (TME) is a dynamic ecosystem comprising immune cells, stromal components, and signaling molecules that collectively influence tumor progression and therapeutic responses (17–20). Within this setting, HLA-E can further facilitate immune evasion by engaging inhibitory receptors on NK and T cells, underscoring its relevance in shaping antitumor immunity and response to immunotherapies. In certain tumors, HLA-E expression can diminish the protective role of tumor-infiltrating lymphocytes, thus contributing to immune escape (20). Re-education strategies targeting the pro-tumor TME may help restore antitumor immune functions (17). This evolving understanding highlights HLA-E as a potential therapeutic target, particularly in combination with immunotherapies aimed at counteracting T cell exhaustion and enhancing treatment outcomes (18, 19).
HLA-E has shown significant therapeutic potential due to its expression in tumor cells compared to healthy tissues (21). By inhibiting cytotoxic NK cells and a subset of CD8 T lymphocytes through interaction with the NKG2A/CD94 heterodimer, it presents a promising target for novel therapeutic antibodies currently under evaluation in clinical studies (21). Targeting this pathway is vital because NK cells perform cytotoxic functions, facilitate antibody-mediated cellular cytotoxicity (ADCC), and recruit dendritic cells into tumors enhancing communication between the innate and adaptive immune systems (21).
Considering the importance of this family of proteins and particularly the relevant role of HLA-E for therapeutic purposes we conducted a systematic review and meta-analysis to investigate the predictive relationship between HLA-E and survival in solid tumors.
This systematic review and meta-analysis were performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) (22) and was registered in PROSPERO (CRD42024527598).
A comprehensive search was performed on MEDLINE, Scopus, and the Cochrane Library from inception till 15th March 2024. The following keywords were used in the search string, along with Boolean Operators “AND” and “OR” to design an encompassing search string: “human leukocyte antigen E” or “HLA-E”, “solid tumors”, “neoplasm”, “malignancy”, “cancer” and “clinical outcomes” or “prognosis.” Additionally, bibliometrics of published articles, conference abstracts and grey literature were reviewed to ensure there were no missing articles.
Articles were screened to identify and remove the duplicates. The remaining articles were then revised by independent reviewers (JDBF, JBA, ADLS, ALA, KMM), to ensure that the recruited articles met the defined eligibility criteria. The inclusion criteria used to shortlist studies were: (i) Studies published in English language, (ii) Observational, cross-sectional, cohort or randomized controlled trials, (iii) Studies involving human participants diagnosed with solid tumors, (iv) Studies reporting at least one of the outcomes of interest.
Five independent reviewers (JDBF, JBA, ADLS, ALA, KMM) conducted the data extraction and verification process. Any disagreements were settled through discussion and the input of a third reviewer (AO). The data gathered from each study encompassed several variables: the study population and the year of publication, the sample size, basic patient demographics (age and gender), tumor type, median follow-up period in months, the method of HLA-E detection (in tissue versus plasma), the detection techniques employed (such as Immunohistochemistry [IHC], Enzyme-Linked Immunosorbent Assay [ELISA], or mRNA analysis), the specific antibody used for detection (when applicable), the percentage of patients exhibiting HLA-E expression, and the outcomes reported by the studies. The primary outcomes analyzed included Overall Survival (OS) and Disease-Free Survival (DFS).
Comprehensive Meta-Analysis (CMA) version 3.0 was used for all relevant meta-analyses of this study. A random-effects model was used due to variability in study populations, differences in study designs and methods, and unknown sources of heterogeneity. Publication bias was assessed by checking asymmetry in the funnel plots generated via CMA. A p-value <0.05 was considered statistically significant for all outcomes. Heterogeneity was assessed with Higgin’s I2 test. A value of I2 = 25%-50% was considered mild, 50%-75% as moderate, and >75% as significant heterogeneity.
A total of 657 articles were identified from the literature search (Figure 1). After removal of duplicates as well as reviews, abstracts, editorials, and case reports, 126 studies were given a full-text evaluation, and 11 were finally included in the meta-analysis (11–13, 23–30).
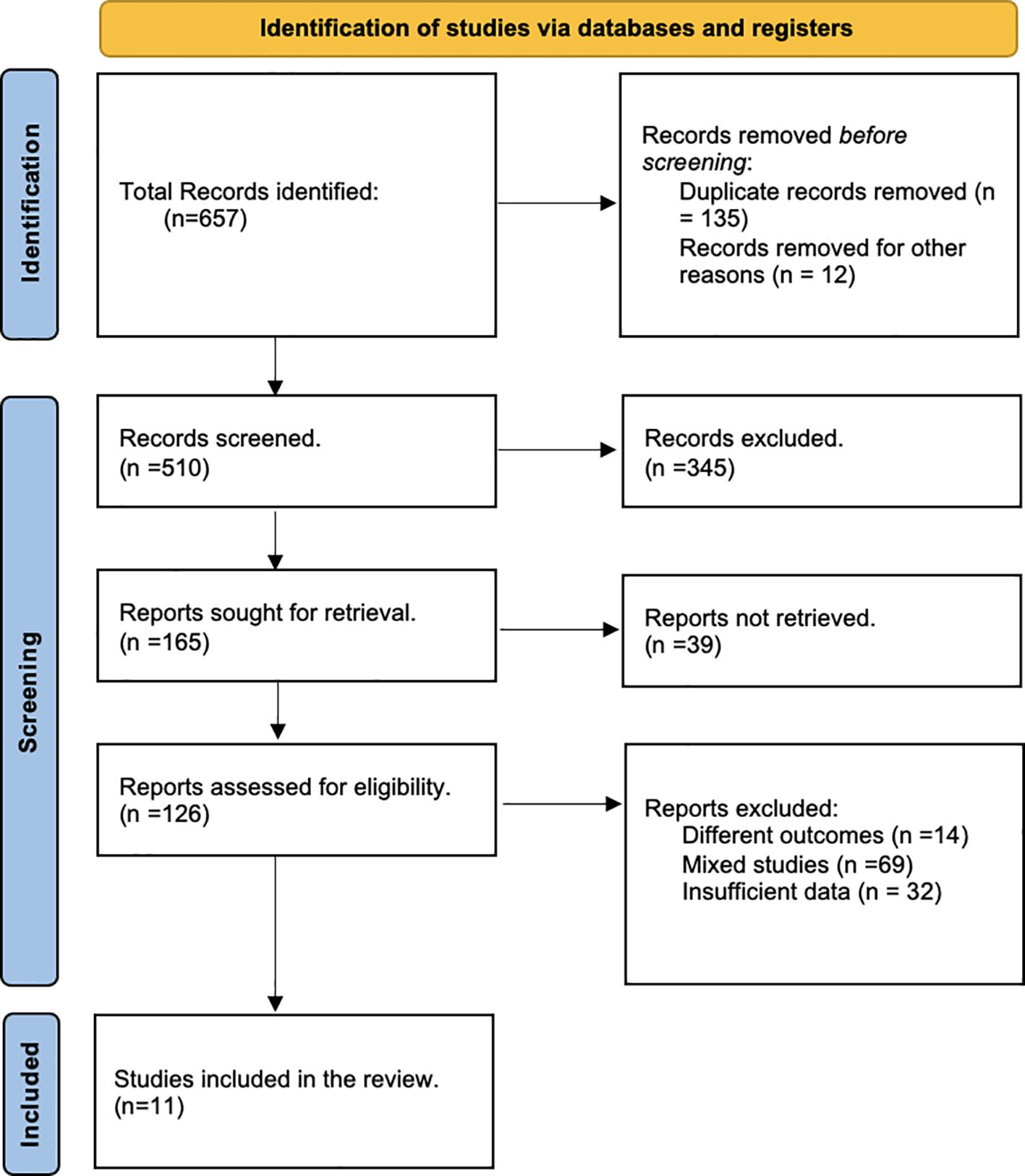
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart of literature search.
A total of 1781 patients were included across the 11 studies, with their characteristics summarized in Table 1. Three studies evaluated colorectal cancer (11, 26, 28), while others included pancreatic (23), esophageal (24), brain (25), renal cell (27), gastric (12), endometrial (29), cervical (13), and hepatocellular carcinoma (30). The mean age of the patients was 59.81 ± 2.01 years. The median follow-up for the studies was calculated to be 57.45 ± 8.91 months. Four of the studies were conducted in China (24–27), while three in Japan (12, 23, 30). Two studies were conducted in Italy (11, 28) as well as two in the Netherlands (13, 29). Staging information was heterogeneous across the studies with varying levels of detail provided. None of the studies offered a comprehensive account of any systemic therapies administered.
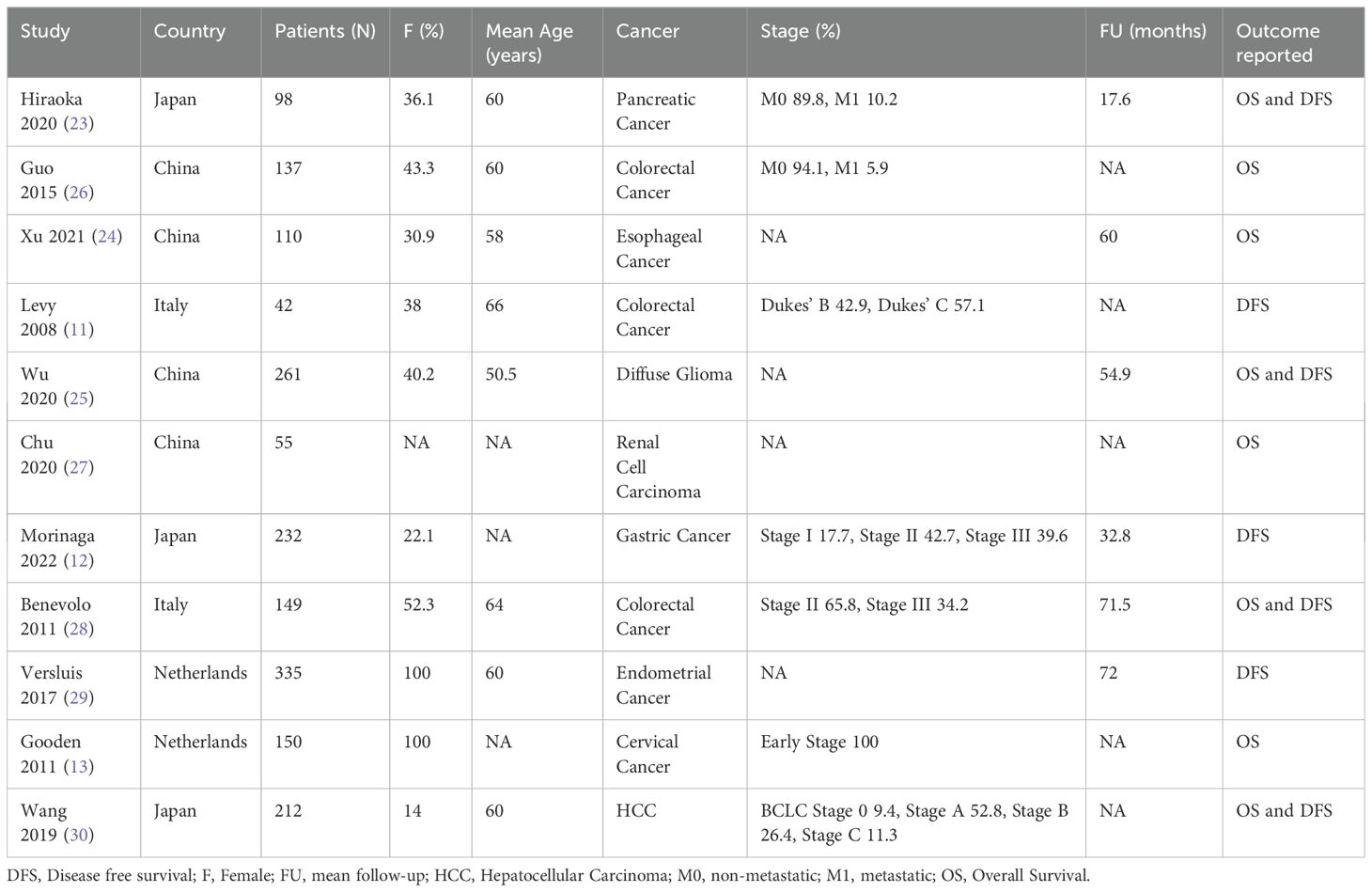
Table 1. Characteristics of included studies.
The HLA-E expression percentage was calculated to be approximately 70.23% across all reported studies. All articles used tissue samples for HLA-E detection, predominantly employing IHC as the 1 technique. Table 2 details the characteristics of antibodies and their detection methods used in each study. The MEM-E/02 antibody was consistently reported across most studies (11–13, 23, 24, 26, 28, 29) except for three studies that used mRNA-based detection methods (25, 27, 30).
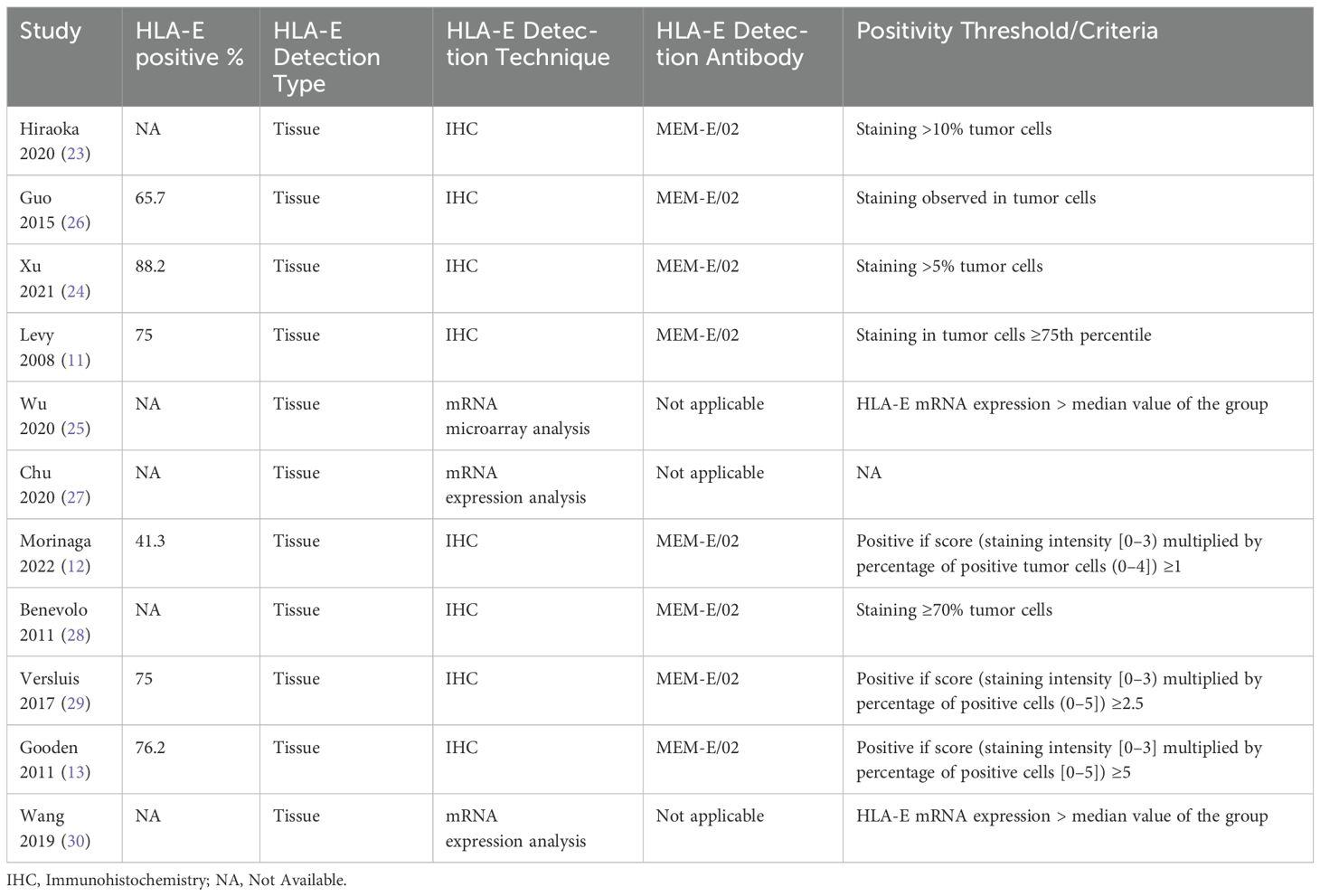
Table 2. Summary of the detection methods and HLA-E expression percentages in the included studies.
Seven studies (13, 23, 24, 26–28, 30) comprising 911 patients reported HRs for OS, the forest plot of the outcome is illustrated in Figure 2. Our combined analysis demonstrated that HLA-E expression had no statistically significant relationship with OS (HR 0.913, 95% CI = 0.567-1.469; P=0.707). Heterogeneity was calculated via a fixed-effect model and hence was demonstrated to be significant. (I2 = 84%).
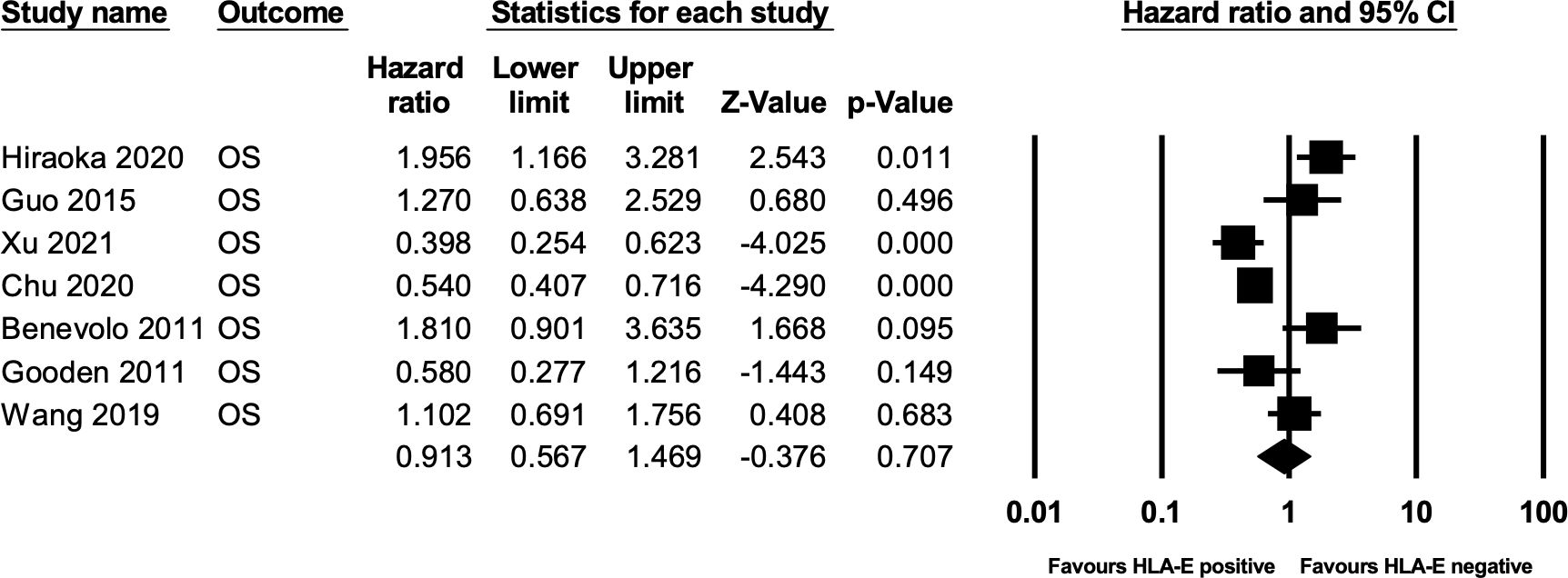
Figure 2. Forest plot of OS.
A total of six studies (11, 12, 23, 28–30) comprising 1068 patients reported HRs for DFS. The forest plot of the outcome is illustrated in Figure 3. On analysis via a random effect model, we determined that HLA-E non-expression was associated with disease-free survival, and it was statistically significant (HR 1.406, 95% CI = 1.027-1.930 9; P=0.03). Heterogeneity was moderate amongst the given studies (I2 = 45%).
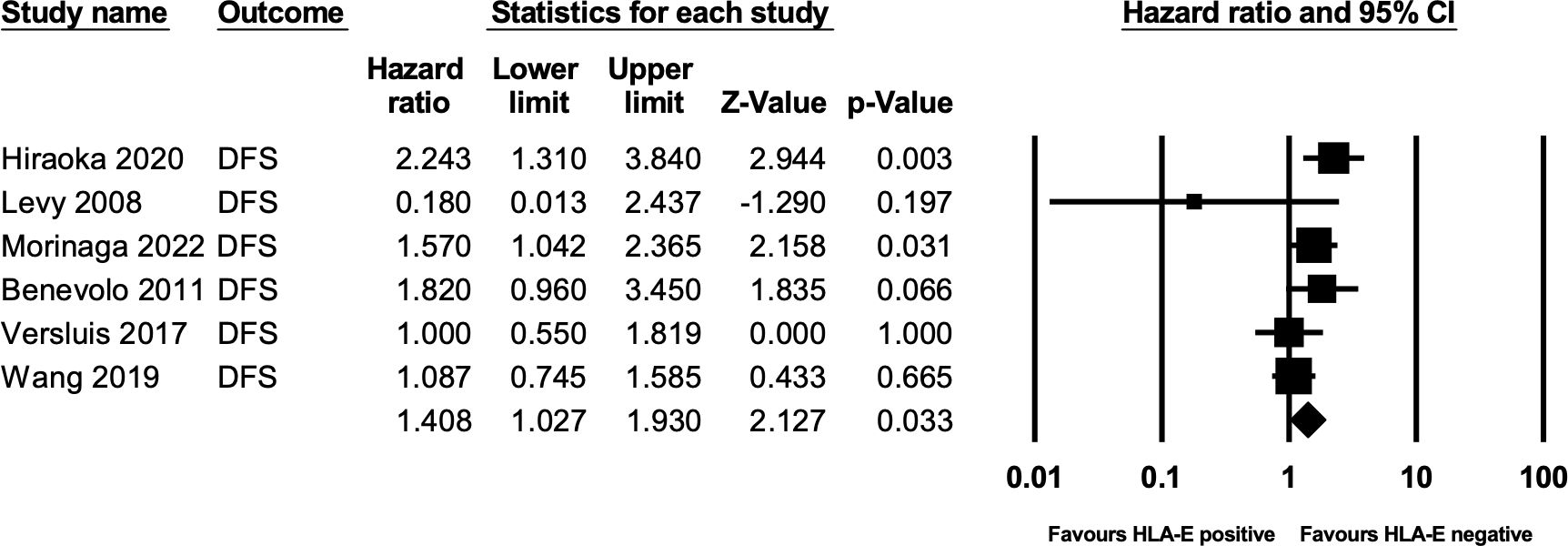
Figure 3. Forest plot of DFS.
HLA-E expression levels, typically elevated in tumor cells compared to healthy tissues, lead to the inhibition of cytotoxic NK cells and CD8 T lymphocytes through interaction with the NKG2A/CD94 heterodimer (2, 21, 31, 32). Consequently, tumor cells may evade NK cell action through HLA-E overexpression (21, 33). This immunosuppressive mechanism emphasizes the potential therapeutic importance of targeting the NKG2A/HLA-E axis (13, 15, 21, 34). This systematic review and meta-analysis investigated the relationship between HLA-E expression and survival in solid tumors. Our analysis revealed no statistically significant association between HLA-E expression and OS. However, HLA-E non-expression was significantly associated with improved DFS. The included studies encompassed a diverse range of solid tumors, with considerable variability in staging and follow-up periods.
HLA-E binding peptides are primarily responsible for controlling HLA-E expression (31, 32). Tumors may upregulate the expression of HLA-E by ensuring a sufficient supply of peptides that stabilize HLA-E, thereby engaging the inhibitory receptor NKG2A on NK cells and certain T cells to protect themselves from immune attack (35, 36). HLA-E can modulate CD8+ T cell responses, and under certain conditions, can induce a Th2-like cytokine profile and activate B cells (Figure 4) (37, 38).
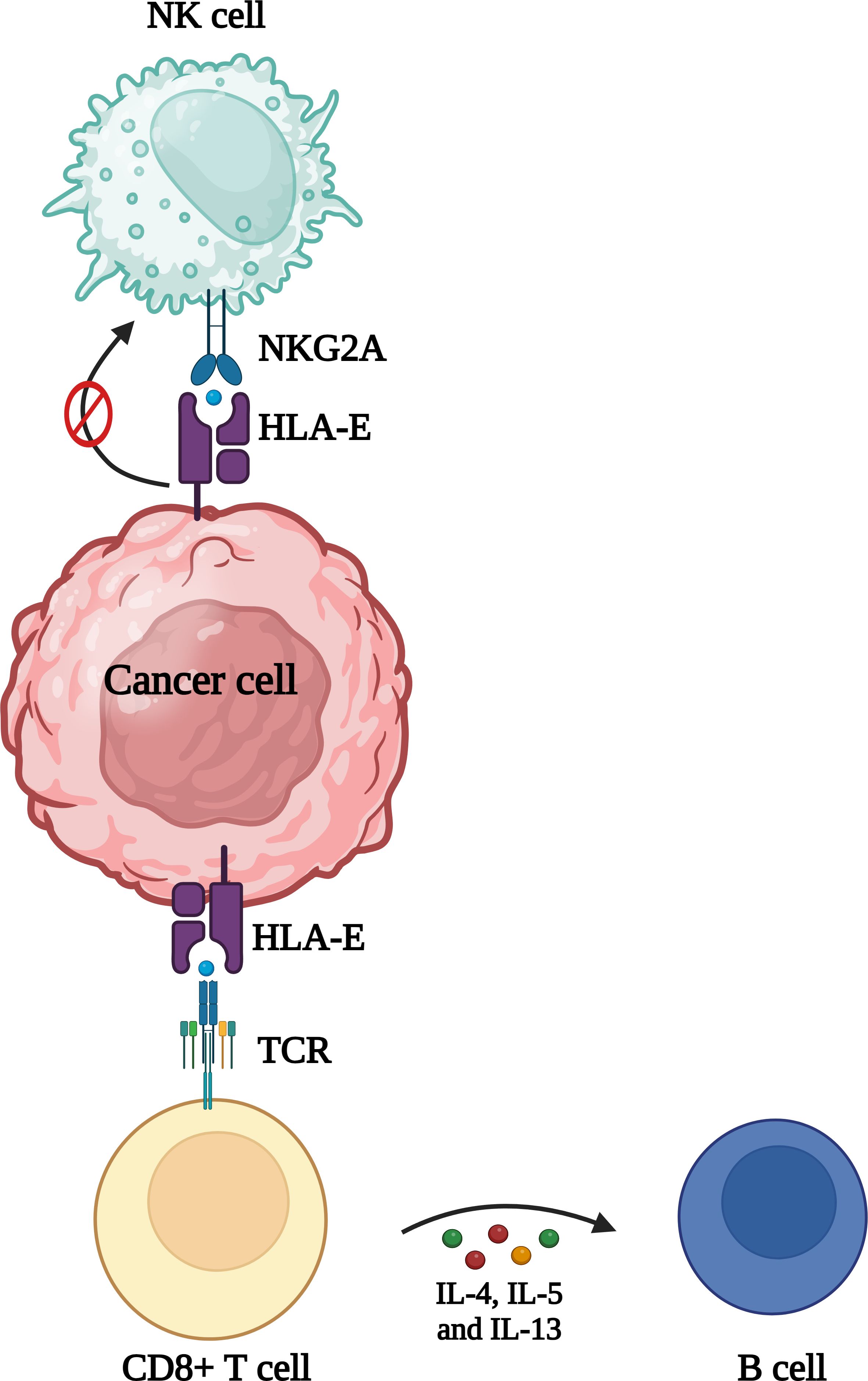
Figure 4. Role of HLA in cancer. Overexpression of HLA-E is frequently observed in cancer cells and can contribute to evasion of NK cell and CD8+ T cell mediated detection and lysis. Additionally, promoting a Th2 response might reduce the cytotoxic potential of CD8+ T cells, aiding in immune evasion.
HLA-E exists in different conformational forms, notably the peptide-bound form and the open conformer. The peptide-bound form, associated with β2-microglobulin and a peptide ligand, is the predominant form expressed on the cell surface and interacts with inhibitory receptors such as NKG2A/CD94 on NK cells and CD8+ T cells (36). In contrast, the open conformer lacks a bound peptide and may have altered stability and receptor interactions (39). The conformational state of HLA-E can influence its expression levels, immune recognition, and function in immune regulation (36, 39).
Depending on the receptor and the responding cell, HLA-E engagement can result in immune activation or suppression (31, 40). As a result, several studies have investigated the connection between HLA-E expression and tumors in recent years. Patients with melanoma (41), glioblastoma (42), gastric cancer (12), breast cancer (16), and ovarian cancer (32) were reported to have high expression of HLA-E and the expression level of HLA-E was linked to clinical outcomes. Another study reported a similar correlation between HLA-E expression and disease-free survival in bladder cancer patients (43).
In the current study, HLA-E made no difference in OS. The reasons for the disparity of the results could be due to different histologies as well as differences in methodology. Our results for DFS, however, showed that overexpression of HLA-E was associated with a poor DFS. Across the six studies included in our DFS analysis, a common theme emerged: HLA-E expression was linked to worse DFS outcomes, despite the variability in cancer types and methodologies. Levy et al. evaluated colorectal cancer patients using IHC, finding that high HLA-E expression was significantly associated with shorter DFS, especially in Dukes’ C patients (11). Levy et al. also highlighted the role of HLA-E in immune evasion through NK cell inhibition (11). Similarly, Morinaga et al. (12), Hiraoka et al. (23), Benevolo et al. (28), and Versluis et al. (29), found that higher HLA-E expression correlated with poorer DFS across esophageal squamous cell carcinoma, pancreatic ductal adenocarcinoma, cervical cancer, and endometrial cancer. Lastly, Wang et al. in their mRNA expression analysis in hepatocellular carcinoma patients showed that higher HLA-E mRNA levels were associated with worse DFS (30). In this context, in primary tumors, predominantly from early-stage disease, HLA-E could play a key immunosuppressive role (31) and therefore could be associated with a detrimental prognosis. In line with their potential role as a therapeutic target, treatments targeting their receptor, NKGD2, are currently under research (44).
Therapeutic strategies targeting the NKG2A/HLA-E axis include both monotherapies and combination therapies (21, 45). While direct inhibition of HLA-E could potentially prevent its interaction with the activating NKG2C receptor, the preferred approach has been to block NKG2A (46). Monalizumab, a first-in-class humanized IgG4 antibody targeting the NKG2A/CD94 receptor, has shown promise in preclinical studies by enhancing NK and CD8 T cell activity (44, 45). Monalizumab blocks the interaction of NKG2A/CD94 with HLA-E, thus promoting NK and CD8 T cell activation. This mechanism not only enhances cytotoxic activities but also augments antibody-dependent cellular cytotoxicity (ADCC), a crucial effector function for many anticancer antibodies (46, 47). Early clinical trials with Monalizumab alone or in combination with anti-PD-L1 antibodies like Durvalumab have demonstrated acceptable safety profiles and preliminary signs of immune activation, the COAST study reported improved overall response rates (ORR) and progression-free survival (PFS) with Monalizumab and Durvalumab in unresectable stage III NSCLC patients (48).
Clinical trials have also explored various combinations of Monalizumab with other therapeutic agents in the recurrent or metastatic setting (46, 49, 50). Other monoclonal antibodies like S095029 and HY-0102 are in clinical development (51, 52). However, tumors may compensate for NKG2A/HLA-E blockade by upregulating other immunosuppressive molecules like PD-L1 or IDO, thereby preserving an immune-evasive niche (18, 20).
To the best of our knowledge, our study is the first meta-analysis to discuss HLA-E and its role in the outcomes of solid cancer patients, including OS and DFS. It offers valuable insights into the prognostic significance of HLA-E expression in various solid tumors. However, to contextualize the interpretation of our findings, it is important to highlight several limitations. A significant limitation is the pronounced heterogeneity among the included studies, encompassing diverse tumor types (e.g., colorectal, pancreatic, esophageal, brain, renal cell, gastric, endometrial, cervical, and hepatocellular carcinomas) and varying disease stages. Each of these cancer types possesses unique biological behaviors, prognostic factors, treatment modalities and responses to treatment. The variability in cancer stages across studies further compounds this issue. This heterogeneity in tumor types and stages may confound the relationship between HLA-E expression and survival outcomes, thereby limiting the ability to generalize our findings. There was substantial variation in the methods used to quantify HLA-E expression. While the majority of studies employed IHC to detect HLA-E levels in tissue samples, others utilized mRNA expression analyses, and the positivity thresholds can varied widely. Importantly, the specificity of the MEM-E/02 antibody for HLA-E detection warrants consideration, as potential cross-reactivity with other HLA class I molecules or recognition of different conformational forms of HLA-E could impact the accuracy of HLA-E expression assessment (53). Such discrepancies in detection techniques, antibody specificity, and positivity criteria can lead to inconsistencies in categorizing patients as HLA-E positive or negative, potentially impacting the results. Moreover, our study did not correlate HLA-E expression with T cell and NK cell infiltration or the expression of HLA-E-specific receptors on immune cells, which limits our understanding of the immunological context and mechanisms of immune evasion (31). Furthermore, HLA-E expression can be influenced by underlying polymorphisms, such as the commonly studied HLA-E01:01 and HLA-E01:03 alleles, which differ in expression levels and surface stability (8, 35, 43). These variations may modulate immune recognition and the extent of immune evasion within the TME, further highlighting the complexity of HLA-E’s prognostic and therapeutic role. Much of the research that comprises our analysis is retrospective, which brings with it inherent limitations including selection bias, dependence on pre-existing data sources and confounding variables. Additionally, relying solely on published literature could introduce publication bias. These limitations could affect the validity of our findings. Although the results of our meta-analysis shed light on the predictive importance of HLA-E expression in solid tumors, they do not clarify the underlying mechanisms responsible for these correlations. To shed light on the causative pathways and biological significance of our findings, further research is necessary to fully understand the intricate interactions between HLA-E expression, tumor biology, immune microenvironment, and treatment modalities.
Our systematic review and meta-analysis provide comprehensive insights into the prognostic significance of HLA-E expression in solid tumors. Despite the lack of statistical significance in the relationship between HLA-E expression and OS, our results point to a possible predictive role for HLA-E non-expression for improved DFS suggesting that targeting the NKG2A/HLA-E axis could be a valuable strategy in enhancing antitumor immune responses, which could be particularly beneficial for early-stage diseases. However, several challenges remain. The variability in clinical outcomes highlights the need for more research to optimize treatment combinations and identify the patient populations that would benefit most from NKG2A/HLA-E axis inhibition. In particular, prospective studies and clinical trials evaluating HLA-E as a therapeutic target will be instrumental. Moreover, understanding the underlying mechanisms of immune evasion and the role of HLA-E in different tumor microenvironments is crucial for developing effective treatments. Further investigation is essential to develop these approaches, optimize combination strategies, and elucidate the mechanisms driving the variable clinical outcomes across different cancer types and stages.
The datasets generated during the current study are not publicly available due to local research institute and department regulations. Requests to access these datasets will be made available by the corresponding author upon reasonable request.
JBF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JBA: Data curation, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. ALS: Data curation, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. ALA: Data curation, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. KM: Data curation, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. KG-H: Methodology, Writing – original draft, Writing – review & editing. PB: Methodology, Writing – original draft, Writing – review & editing. MB: Methodology, Writing – original draft, Writing – review & editing. AF: Methodology, Writing – original draft, Writing – review & editing. SS-R: Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. AO: Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. KG-H is supported by a Juan Rodés Grant from the Instituto de Salud Carlos III (JR22/00018).
AO is a former employee of Symphogen. AO reports personal fees from Servier, CancerAppy, Entrechem and Worldwide Clinical Trials. PB reports speaker/advisory grants from GlaxoSmithKline, Merck and MSD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. McKean WB, Moser JC, Rimm D, Hu-Lieskovan S. Biomarkers in precision cancer immunotherapy: promise and challenges. Am Soc Clin Oncol Educ Book. (2020) 40:e275–91. doi: 10.1200/EDBK_280571
2. Bukur J, Jasinski S, Seliger B. The role of classical and non-classical HLA class I antigens in human tumors. Semin Cancer Biol. (2012) 22:350–8. doi: 10.1016/j.semcancer.2012.03.003
3. Campoli M, Ferrone S. HLA antigen changes in Malignant cells: epigenetic mechanisms and biologic significance. Oncogene. (2008) 27:5869–85. doi: 10.1038/onc.2008.273
4. Cornel AM, Mimpen IL, Nierkens S. MHC class I downregulation in cancer: underlying mechanisms and potential targets for cancer immunotherapy. Cancers (Basel). (2020) 12:1760. doi: 10.3390/cancers12071760
5. Hazini A, Fisher K, Seymour L. Deregulation of HLA-I in cancer and its central importance for immunotherapy. J Immunother Cancer. (2021) 9:e002899. doi: 10.1136/jitc-2021-002899
6. Wyatt RC, Lanzoni G, Russell MA, Gerling I, Richardson SJ. What the HLA-I!-classical and non-classical HLA class I and their potential roles in type 1 diabetes, Curr. Diab Rep. (2019) 19:159. doi: 10.1007/s11892-019-1245-z
7. Sharpe HR, Bowyer G, Brackenridge S, Lambe T. HLA-E: exploiting pathogen-host interactions for vaccine development. Clin Exp Immunol. (2019) 196:167–77. doi: 10.1111/cei.13292
8. Zhen ZJ, Ling JY, Cai Y, Luo WB, He YJ. Impact of HLA-E gene polymorphism on HLA-E expression in tumor cells and prognosis in patients with stage III colorectal cancer. Med Oncol. (2013) 30:482. doi: 10.1007/s12032-013-0482-2
9. Derré L, Corvaisier M, Charreau B, Moreau A, Godefroy E, Moreau-Aubry A, et al. Expression and release of HLA-E by melanoma cells and melanocytes: potential impact on the response of cytotoxic effector cells. J Immunol. (2006) 177:3100–7. doi: 10.4049/jimmunol.177.5.3100
10. Llano M, Lee N, Navarro F, García P, Albar JP, Geraghty DE, et al. HLA-E-bound peptides influence recognition by inhibitory and triggering CD94/NKG2 receptors: preferential response to an HLA-G-derived nonamer. Eur J Immunol. (1998) 28:2854–63. doi: 10.1002/(SICI)1521-4141(199809)28:09<2854::AID-IMMU2854>3.0.CO;2-W
11. Levy EM, Bianchini M, Von Euw EM, Barrio MM, Bravo AI, Furman D, et al. Human leukocyte antigen-E protein is overexpressed in primary human colorectal cancer. Int J Oncol. (2008) 32:633–41. doi: 10.3892/ijo.32.3.633
12. Morinaga T, Iwatsuki M, Yamashita K, Matsumoto C, Harada K, Kurashige J, et al. Evaluation of HLA-E expression combined with natural killer cell status as a prognostic factor for advanced gastric cancer. Ann Surg Oncol. (2022) 29:4951–60. doi: 10.1245/s10434-022-11665-3
13. Gooden M, Lampen M, Jordanova ES, Leffers N, Trimbos JB, van der Burg SH, et al. HLA-E expression by gynecological cancers restrains tumor-infiltrating CD8+ T lymphocytes. Proc Natl Acad Sci U S A. (2011) 108:10656–61. doi: 10.1073/pnas.1100354108
14. Andersson E, Poschke I, Villabona L, Carlson JW, Lundqvist A, Kiessling R, et al. Non-classical HLA-class I expression in serous ovarian carcinoma: Correlation with the HLA-genotype, tumor infiltrating immune cells and prognosis. Oncoimmunology. (2015) 5:e1052213. doi: 10.1080/2162402X.2015.1052213
15. Yazdi MT, van Riet S, van SChadewijk A, Fiocco M, van Hall T, Taube C, et al. The positive prognostic effect of stromal CD8+ tumor-infiltrating T cells is restrained by the expression of HLA-E in non-small cell lung carcinoma. Oncotarget. (2016) 7:3477–88. doi: 10.18632/oncotarget.6506
16. de Kruijf EM, Sajet A, van Nes JG, Natanov R, Putter H, Smit VT, et al. HLA-E and HLA-G expression in classical HLA class I-negative tumors is of prognostic value for clinical outcome of early breast cancer patients. J Immunol. (2010) 185:7452–9. doi: 10.4049/jimmunol.1002629
17. Quail DF, Joyce JA. Microenvironmental regulation of tumor progression and metastasis. Nat Med. (2013) 19:1423–37. doi: 10.1038/nm.3394
18. Liu X, Xi X, Xu S, Chu H, Hu P, Li D, et al. Targeting T cell exhaustion: emerging strategies in non-small cell lung cancer. Front Immunol. (2024) 15:1507501. doi: 10.3389/fimmu.2024.1507501
19. Xu S, Chen X, Ying H, Chen J, Ye M, Lin Z, et al. Multi−omics identification of a signature based on Malignant cell-associated ligand-receptor genes for lung adenocarcinoma. BMC Cancer. (2024) 24:1138. doi: 10.1186/s12885-024-12911-5
20. Benitez Fuentes JD, Bartolome Arcilla J, Mohamed Mohamed K, Lopez de Sa A, de Luna Aguilar A, Guevara-Hoyer K, et al. Targeting of non-classical human leukocyte antigens as novel therapeutic strategies in cancer. Cancers (Basel). (2024) 16:4266. doi: 10.3390/cancers16244266
21. van Hall T, André P, Horowitz A, Ruan DF, Borst L, Zerbib R, et al. Monalizumab: inhibiting the novel immune checkpoint NKG2A. J Immunother Cancer. (2019) 7:263. doi: 10.1186/s40425-019-0761-3
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
23. Hiraoka N, Ino Y, Hori S, Yamazaki-Itoh R, Naito C, Shimasaki M, et al. Expression of classical human leukocyte antigen class I antigens, HLA-E and HLA-G, is adversely prognostic in pancreatic cancer patients. Cancer Sci. (2020) 111:3057–70. doi: 10.1111/cas.14514
24. Xu YF, Du XF, Li ZY, Fang ZP, Zhang FB. Lesion human leukocyte antigen-E is associated with favourable prognosis for patients with oesophageal squamous cell carcinoma. J Int Med Res. (2021) 49:3000605211047278. doi: 10.1177/03000605211047278
25. Wu Z, Liang J, Wang Z, Li A, Fan X, Jiang T. HLA-E expression in diffuse glioma: relationship with clinicopathological features and patient survival. BMC Neurol. (2020) 20:59. doi: 10.1186/s12883-020-01640-4
26. Guo ZY, Lv YG, Wang L, Shi S-J, Yang F, Zheng G-X, et al. Predictive value of HLA-G and HLA-E in the prognosis of colorectal cancer patients. Cell Immunol. (2015) 293:10–6. doi: 10.1016/j.cellimm.2014.10.003
27. Chu G, Jiao W, Yang X, Liang Y, Li Z, Niu H. C3, C3AR1, HLA-DRA, and HLA-E as potential prognostic biomarkers for renal clear cell carcinoma. Transl Androl Urol. (2020) 9:2640–56. doi: 10.21037/tau-20-699
28. Benevolo M, Mottolese M, Tremante E, Rollo F, Diodoro MG, Ercolani C, et al. High expression of HLA-E in colorectal carcinoma is associated with a favorable prognosis. J Transl Med. (2011) 9:184. doi: 10.1186/1479-5876-9-184
29. Versluis MAC, Marchal S, Plat A, de Bock GH, van Hall T, de Bruyn M, et al. The prognostic benefit of tumour-infiltrating Natural Killer cells in endometrial cancer is dependent on concurrent overexpression of Human Leucocyte Antigen-E in the tumour microenvironment. Eur J Cancer. (2017) 86:285–95. doi: 10.1016/j.ejca.2017.09.008
30. Wang XK, Liao XW, Yang CK, Yu TD, Liu ZQ, Gong YZ, et al. Diagnostic and prognostic biomarkers of Human Leukocyte Antigen complex for hepatitis B virus-related hepatocellular carcinoma. J Cancer. (2019) 10:5173–90. doi: 10.7150/jca.29655
31. Wieten L, Mahaweni NM, Voorter CEM, Bos GMJ, Tilanus MGJ. Clinical and immunological significance of HLA -E in stem cell transplantation and cancer. Tissue Antigens. (2014) 84:523–35. doi: 10.1111/tan.12478
32. Zheng H, Guan X, Meng X, Tong Y, Wang Y, Xie S, et al. IFN-γ in ovarian tumor microenvironment upregulates HLA-E expression and predicts a poor prognosis. J Ovarian Res. (2023) 16:229. doi: 10.1186/s13048-023-01286-z
33. Pereira BI, Devine OP, Vukmanovic-Stejic M, Chambers ES, Subramanian P, Patel N, et al. Senescent cells evade immune clearance via HLA-E-mediated NK and CD8+ T cell inhibition. Nat Commun. (2019) 10:2387. doi: 10.1038/s41467-019-10335-5
34. van Esch EMG, Tummers B, Baartmans V, Osse EM, Ter Haar N, Trietsch MD, et al. Alterations in classical and nonclassical HLA expression in recurrent and progressive HPV-induced usual vulvar intraepithelial neoplasia and implications for immunotherapy. Int J Cancer. (2014) 135:830–42. doi: 10.1002/ijc.28713
35. van Hall T, Oliveira CC, Joosten SA, Ottenhoff THM. The other Janus face of Qa-1 and HLA-E: diverse peptide repertoires in times of stress. Microbes Infect. (2010) 12:910–8. doi: 10.1016/j.micinf.2010.07.011
36. Sullivan LC, Clements CS, Rossjohn J, Brooks AG. The major histocompatibility complex class Ib molecule HLA-E at the interface between innate and adaptive immunity. Tissue Antigens. (2008) 72:415–24. doi: 10.1111/j.1399-0039.2008.01138.x
37. van Meijgaarden KE, Haks MC, Caccamo N, Dieli F, Ottenhoff TH, Joosten SA. Human CD8+ T-cells recognizing peptides from Mycobacterium tuberculosis (Mtb) presented by HLA-E have an unorthodox Th2-like, multifunctional, Mtb inhibitory phenotype and represent a novel human T-cell subset. PloS Pathog. (2015) 11:e1004671. doi: 10.1371/journal.ppat.1004671
38. Bansal A, Gehre MN, Qin K, Sterrett S, Ali A, Dang Y, et al. HLA-E-restricted HIV-1-specific CD8+ T cell responses in natural infection. J Clin Invest. (2021) 131:e148979. doi: 10.1172/JCI148979
39. Hoare HL, Sullivan LC, Clements CS, Ely LK, Beddoe T, Henderson KN, et al. Subtle changes in peptide conformation profoundly affect recognition of the non-classical MHC class I molecule HLA-E by the CD94-NKG2 natural killer cell receptors. J Mol Biol. (2008) 377:1297–303. doi: 10.1016/j.jmb.2008.01.098
40. Guberina H, Rebmann V, Wagner B, da Silva Nardi F, Dziallas P, Dolff S, et al. Association of high HLA-E expression during acute cellular rejection and numbers of HLA class I leader peptide mismatches with reduced renal allograft survival. Immunobiology. (2017) 222:536–43. doi: 10.1016/j.imbio.2016.10.021
41. Allard M, Oger R, Vignard V, Percier JM, Fregni G, Périer A, et al. Serum soluble HLA-E in melanoma: A new potential immune-related marker in cancer. PloS One. (2011) 6:e21118. doi: 10.1371/journal.pone.0021118
42. Kren L, Slaby O, Muckova K, Lzicarova E, Sova M, Vybihal V, et al. Expression of immune-modulatory molecules HLA-G and HLA-E by tumor cells in glioblastomas: an unexpected prognostic significance? Neuropathology. (2011) 31:129–34. doi: 10.1111/j.1440-1789.2010.01149.x
43. Veiga-Castelli LC, de Paula Cruz AS, Inácio MM, Mendes-Junior CT, Vianello-Brondani R, Moreau P, et al. Lack of association between HLA-E polymorphisms and transitional cell carcinoma of the bladder. Tissue Antigens. (2013) 82:197–200. doi: 10.1111/tan.12159
44. Sætersmoen M, Kotchetkov I, Torralba-Raga L, Mansilla-Soto J, Sohlberg E, Krokeide SZ, et al. 512 Targeting HLA-E positive cancers with a novel NKG2A/C switch receptor. J Immunother Cancer. (2023) 11. doi: 10.1136/jitc-2023-SITC2023.0512
45. Borgeaud M, Sandoval J, Obeid M, Banna G, Michielin O, Addeo A, et al. Novel targets for immune-checkpoint inhibition in cancer. Cancer Treat Rev. (2023) 120:102614. doi: 10.1016/j.ctrv.2023.102614
46. André P, Denis C, Soulas C, Bourbon-Caillet C, Lopez J, Arnoux T, et al. Anti-NKG2A mAb is a checkpoint inhibitor that promotes anti-tumor immunity by unleashing both T and NK cells. Cell. (2018) 175:1731–1743.e13. doi: 10.1016/j.cell.2018.10.014
47. Kyrysyuk O, Wucherpfennig KW. Designing cancer immunotherapies that engage T cells and NK cells. Annu Rev Immunol. (2023) 41:17–38. doi: 10.1146/annurev-immunol-101921-044122
48. Herbst RS, Majem M, Barlesi F, Carcereny E, Chu Q, Monnet I, et al. COAST: an open-label, phase II, multidrug platform study of durvalumab alone or in combination with oleclumab or monalizumab in patients with unresectable, stage III non–small-cell lung cancer. J Clin Oncol. (2022) 40:3383–93. doi: 10.1200/JCO.22.00227
49. Fayette J, Licitra LFL, Harrington KJ, Haddad R, Siu LL, Liu YC, et al. 854O INTERLINK-1: Phase III study of cetuximab (CTX) ± monalizumab (M) in participants (pts) with recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC) with disease progression on/after platinum chemotherapy (CT) and previously treated with an immune checkpoint inhibitor (ICI). Ann Oncol. (2023) 34:S554–5. doi: 10.1016/j.annonc.2023.09.2000
50. Geurts VCM, Voorwerk L, Balduzzi S, Salgado R, Van de Vijver K, van Dongen MGJ, et al. Unleashing NK- and CD8 T cells by combining monalizumab and trastuzumab for metastatic HER2-positive breast cancer: Results of the MIMOSA trial. Breast. (2023) 70:76–81. doi: 10.1016/j.breast.2023.06.007
51. A Phase 1a/1b, Open-label, Multicenter Trial Investigating the Safety, Tolerability, and Preliminary Anti-neoplastic Activity of S095029 (Anti-NKG2A) as Monotherapy and in Combination With Sym021 (Anti-PD-1) in Patients With Advanced Solid Tumor Malignancies Followed by an Expansion Part With Triplet Combinations of S095029 and Sym021 and an Anti-HER2 mAb or Anti-EGFR mAbs (Futuximab/Modotuximab) in Patients With Metastatic Gastric or Colorectal Cancers (Accessed July 5, 2024).
52. A Study of HY-0102 in Patients With Advanced Solid Tumors . Available online at: https://clinicaltrials.gov/study/ (Accessed July 5, 2024).
Keywords: human leukocyte antigen, HLA-E, cancer, solid tumors, survival, immunotherapy
Citation: Benitez Fuentes JD, Bartolome Arcilla J, Lazaro Sanchez AD, de Luna Aguilar A, Mohamed Mohamed K, Guevara-Hoyer K, Ballestin Martinez P, Borregon Rivilla M, Ferrandez Arias A, Sánchez-Ramon S and Ocaña A (2025) Association between human leukocyte antigen E expression and outcomes in solid tumors: a systematic review and meta-analysis. Front. Oncol. 15:1525924. doi: 10.3389/fonc.2025.1525924
Received: 10 November 2024; Accepted: 03 February 2025;
Published: 24 February 2025.
Edited by:
Marco Bregni, San Raffaele Hospital (IRCCS), ItalyReviewed by:
Roberto Crocchiolo, Niguarda Ca’ Granda Hospital, ItalyCopyright © 2025 Benitez Fuentes, Bartolome Arcilla, Lazaro Sanchez, de Luna Aguilar, Mohamed Mohamed, Guevara-Hoyer, Ballestin Martinez, Borregon Rivilla, Ferrandez Arias, Sánchez-Ramon and Ocaña. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Javier David Benitez Fuentes, amF2aWVyZGF2aWRiZW5pdGV6ZnVlbnRlc0BnbWFpbC5jb20=; Alberto Ocaña, YWxiZXJ0by5vY2FuYUBzYWx1ZC5tYWRyaWQub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.