 Jinqun Xu
Jinqun Xu Qing Zhang1
Qing Zhang1 Weiru Xu
Weiru Xu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 16 April 2025
Sec. Breast Cancer
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1500410
Introduction: Effective treatments for preventing and treating chemotherapy-induced peripheral neuropathy (CIPN) are still under exploration. Acupuncture in the treatment of CIPN requires more clinical trial data. This study aimed to evaluate the therapeutic effect of acupuncture on CIPN and explore its efficacy and safety in improving peripheral neuropathy.
Methods: A randomized controlled trial was conducted from May 2021 to June 2023. Eligible patients were randomly divided into a verum acupuncture group and a sham acupuncture group at a 1:1 ratio with sealed opaque envelopes. The patients of both the two groups took oral mecobalamin tablets, 0.5 mg, three times a day for 2 weeks. Participants received acupuncture treatment three times a week for 2 weeks. The primary outcome was evaluated using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) 3.0. The secondary outcomes were assessed using the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-CIPN twenty-item subscale (QLQ-CIPN20), Numerical Rating Scale (NRS), Traditional Chinese Medicine (TCM) syndrome score, and nerve conduction study (NCS) testing. Assessments were conducted at baseline, 1 week, and 2 weeks.
Results: All 70 participants were recruited and randomized. In the end, 68 patients were included in the datasets and received verum acupuncture (n = 34) or sham acupuncture (n = 34). After 2 weeks of treatment and follow-up, a statistically significant difference was found in the NCI-CTCAE scores between the two groups (p = 0.02). Baseline-to-2-week assessment scores improved significantly in the intervention group (vs. controls) on EORTC QLQ-CIPN20 (p = 0.02), NRS scores (p = 0.03), TCM syndrome scores (p = 0.04), and sensory nerve action potential (SNAP) of median and peroneal nerves, sensory nerve conduction velocity (SNCV) and motor nerve conduction velocity (MNCV) of peroneal nerves (p < 0.05). No serious adverse events were reported.
Conclusion: This study supports the feasibility of acupuncture combined with medication as an intervention for patients with CIPN and confirms its efficacy and safety in improving peripheral neuropathy.
Clinical Trial Registration: The Chinese Clinical Trial Registry, identifier ChiCTR2100045762.
Chemotherapy-induced peripheral neuropathy is a serious adverse effect and occurs after the usage of chemotherapeutic agents (1). Damage of peripheral neuropathy usually causes sensory and motor deficits, characterized by hyperpathia, tingling, numbness, and weakness in the hands and/or feet (2–4). The prevalence of CIPN was more than 68% (5–7). Platinum-based drugs have the highest incidence of peripheral neuropathy (70%–100%), and taxane-induced peripheral neuropathy ranks second (11%–87%) (8). Symptoms are dose dependent and would lead to discontinuation of treatment or reduction of treatment dose affecting the patient’s overall survival (9). Some patients could pursue CIPN for months after treatment discontinuation, which severely influences their quality of life physically and financially (10, 11). Therefore, it is extremely necessary to actively and effectively treat CIPN as early as possible to improve the quality of life and effectiveness of treatment for cancer patients.
Currently, treatment of CIPN includes nerve-protective therapy, ion channel-targeted therapy, anti-inflammatory therapy, neurotransmitter-based therapy, antioxidant, and non-drug treatment (12), whereas effective treatments for preventing and treating CIPN are still under exploration because of the varying pathophysiology of CIPN with different classes of chemotherapy drugs (5, 13),. According to the latest American Society of Clinical Oncology (ASCO) guidelines, duloxetine is the only drug with evidence to support its use in the treatment of painful CIPN (14). Duloxetine belongs to a class of medications called selective serotonin and norepinephrine reuptake inhibitors (SNRIs), it is likely to enhance analgesia but is not neuroprotective (15). Current clinical treatment recommendations for CIPN include analgesia and symptom management. Some studies have shown that acupuncture can effectively reduce chemotherapy-induced peripheral neuropathy in patients with hyperpathia and other various symptoms (16, 17). However, Traditional Chinese Medicine (TCM) syndromes have not yet been involved in current studies on acupuncture treatment of CIPN. Syndrome differentiation, as a fundamental approach in TCM diagnosis and treatment, can guide the selection of acupuncture points (18, 19). In this study, we aimed to explore the efficacy and safety of acupuncture combined with medication in the treatment of CIPN with the syndrome of qi deficiency and blood stasis and provide an alternative direction for the prevention and treatment of CIPN in the future. We believe that the effective rate of acupuncture for CIPN can be increased under the guidance of TCM evidence-based treatment. It will also help doctors to accurately treat the patients with the syndrome of qi deficiency and blood stasis. Besides, in this study, we used multi-scales to comprehensively analyze the effectiveness of acupuncture in treating CIPN, including patients’ subjective symptoms (NCI-CTCAE, EORTC QLQ-CIPN20, NRS), objective data (NCS), and the syndrome score of Traditional Chinese Medicine.
We conducted a single-center, randomized, controlled, single-blind clinical trial. The therapeutic verum acupuncture group was compared to the sham acupuncture group for patients with chemotherapy-induced peripheral neuropathy (CIPN). Patients were randomly divided into a verum acupuncture group and a sham acupuncture group. We observed both groups to evaluate the therapeutic effect of acupuncture combined with medication on CIPN and explored its efficacy and safety in improving peripheral neuropathy in patients. This study aimed to establish a treatment method that can be clinically applied and promoted.
We conducted the study at the Beijing Hospital of Traditional Chinese Medicine, Capital Medical University. Participants were recruited at the outpatient clinic and inpatient ward of the Oncology Department. The study coordinator explained the possible benefits and adverse reactions of the trial to the eligible patients, and all patients signed informed consent forms.
Inclusion criteria included the following:
1. All cases were confirmed as malignant tumors by histopathology or cytology.
2. Patients underwent chemotherapy with platinum-based or taxane agents and subsequently developed sensor neuropathy (numbness, sensory loss, pain, paresthesia in the extremities) and/or motor neuropathy (muscle cramps, muscle weakness, myalgia, paralysis).
3. Patients rated grade 2 or higher on the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) for sensory and motor neuropathy within 7 days to 2 years after cessation of chemotherapy.
4. Patients were diagnosed with qi deficiency and blood stasis as the primary syndrome according to Traditional Chinese Medicine (TCM) differentiation.
5. Patients with Eastern Cooperative Oncology Group (ECOG) performance status scores of 0–3.
6. Patients with an expected survival time of more than 3 months.
Exclusion criteria included the following:
1. Patients with peripheral neuropathy that were not caused by chemotherapy agents.
2. Patients were undergoing treatment with other medications that may cause neurotoxicity.
3. Patients who received any suspected effective medication, such as tricyclic antidepressants or anticonvulsants.
4. Patients with severe diseases involving the cardiovascular, hepatic, renal, immune, or hematopoietic systems.
5. Patients were pregnant or breastfeeding.
6. Patients cannot undergo acupuncture treatment, due to needle phobia or allergy to stainless steel needles, etc.
Eligible patients were randomly allocated to the verum acupuncture group or sham acupuncture group in a 1:1 ratio. An independent researcher at the Beijing Hospital of Traditional Chinese Medicine generated random numbers by a computer-generated randomization program. Random sequences were loaded into sealed opaque envelopes and kept by the study coordinator. All neuropathy evaluations were performed exclusively by a trained medical professional, who had underwent standardized training to ensure consistency and adherence to the NCI-CTCAE guidelines prior to patient enrollment. The acupuncturist did not participate in the patient’s inclusion. The study coordinator opened the envelope and informed the acupuncturist before the intervention. The study participants, assessor, and statistician were all blinded to the treatment assignments. Only the acupuncturist and study coordinator were aware of these details.
All acupuncture procedures were performed by the same licensed acupuncturist with over 5 years of experience. During the treatment, patients were asked to avoid medications that might alleviate CIPN (such as tricyclic antidepressants or antiepileptic drugs, Chinese herbal decoction, and patent Chinese medicine).
Participants in the verum acupuncture (intervention) group received 2 weeks of acupuncture treatment. The principle of acupuncture treatment was activating meridians and collaterals, benefiting qi, and promoting blood circulation to remove blood stasis. The acupuncture prescription included bilateral ST36, SP10, LI4, LR3, LI11, EX-LE10, EX-UE9, and RN6. The location of the acupoints are illustrated in Figure 1. The acupuncturist followed the guidelines outlined in the Acupuncture and Moxibustion Medicine from the New Century Higher Medical Education Planning Textbook series (published by China Traditional Chinese Medicine Press). The acupuncturist used disposable sterile acupuncture needles (0.25 × 40 mm, 0.25 × 25 mm, Hwato, China), then disinfected the acupuncture points and their hands strictly with 75% alcohol before needle insertion.
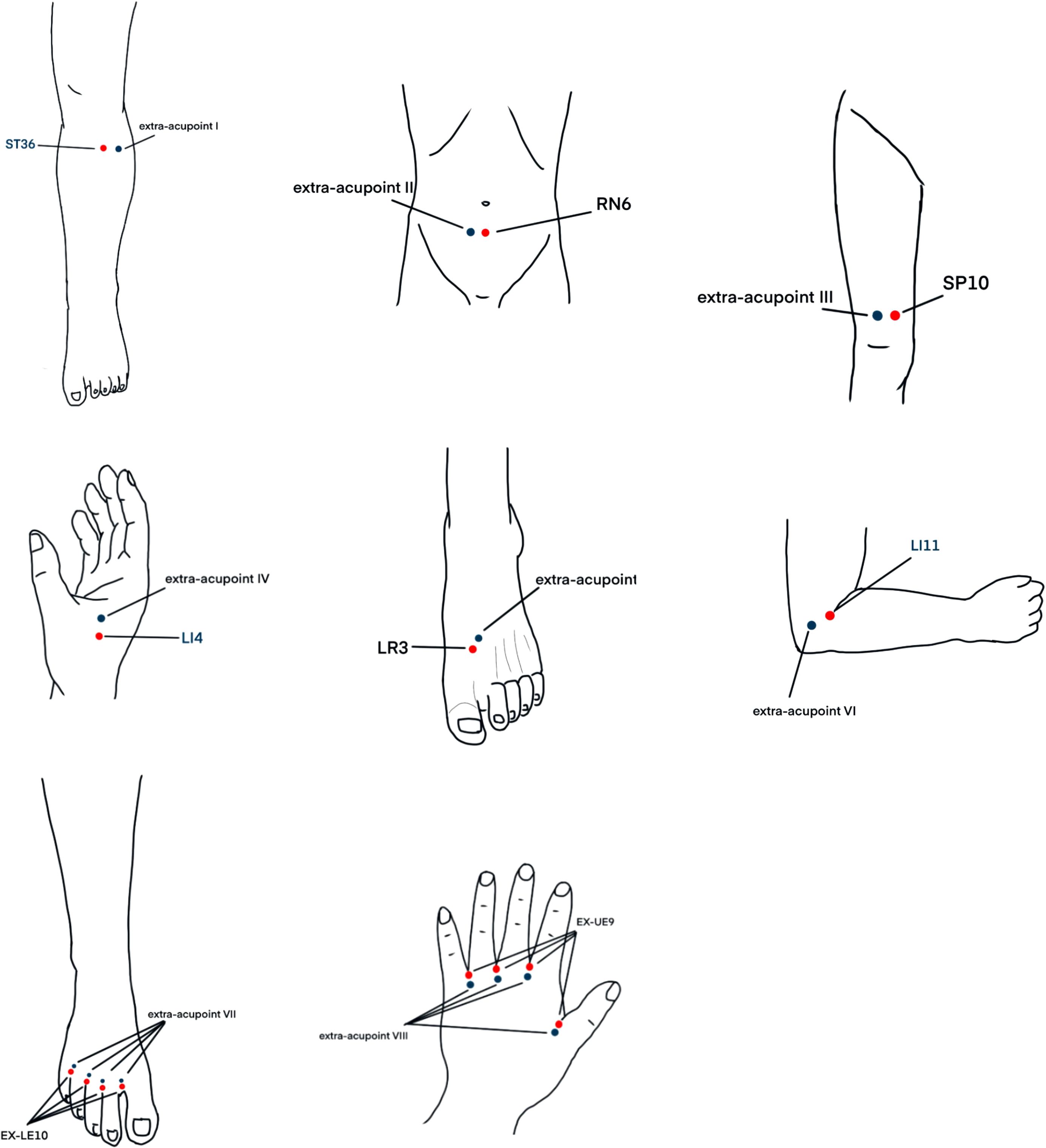
Figure 1. The acupoints of the verum acupuncture group and the sham acupuncture group.
After needle insertion, each acupoint was evenly lifted, thrust, and twirled three times to achieve a local sensation of soreness, numbness, distension, or heaviness indicating “de qi.” The needles were retained for 30 min, with one needle twisted and performed midway. Treatment frequency is three times per week, lasting for 2 weeks.
Participants in the sham acupuncture (control) group received 2 weeks of sham acupuncture treatment. This group used non-traditional acupoints located adjacent to the conventional acupoints. Extra-acupoint I was outwardly parallelled 1 cun with ST36, extra-acupoint II was outwardly parallelled 1 cun with RN6, extra-acupoint III was outwardly parallelled 1 cun with SP10, extra-acupoint IV was the midpoint between LI4 and EX-UE9, extra-acupoint V was the midpoint between LR3 and ST42, extra-acupoint V was the midpoint between TE10 and LI11, extra-acupoint VII was upward 0.25 cun from EX-LE10, and extra-acupoint VII was upward 0.25 cun from EX-UE9. The location of the acupoints are illustrated in Figure 1. The needles were inserted superficially and penetrated only the subcutaneous layer without manipulation to obtain qi. The acupuncture instruments, needle insertion frequency, and treatment duration were consistent with those of the verum acupuncture group.
The patients of both the two groups received medication treatment: oral mecobalamin tablets (Produced by Eisai China Pharmaceutical Co., Ltd., approval number: National Medicine Standard H20143107), 0.5 mg, three times a day, continuously for 2 weeks.
The patient’s general condition and tumor-related indicators were recorded before the time of random assignment, including age, sex, body mass index (BMI), employment status, education, diagnosis, cancer stage, adjuvant type, chemotherapy cycles, ECOG performance status, months after last chemotherapy. Outcomes related to preliminary efficacy included primary outcome indicators and secondary outcome indicators. The independent assessor recorded relevant outcomes at baseline, 1 week, and 2 weeks after initiation of the study intervention.
Peripheral neuropathy grading based on NCI-CTCAE scale V3.0 was used to evaluate the primary outcome.
Secondary outcomes were evaluated using the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-CIPN twenty-item subscale (QLQ-CIPN20), Numerical Rating Scale (NRS), Traditional Chinese Medicine(TCM) syndrome score, and nerve conduction study (NCS) testing.
The EORTC QLQ-CIPN20 evaluates the sensory, motor, and autonomic symptoms of peripheral nerves (20). The assessor scored according to the actual situation, with a four-point system for each item. The higher the total score, the worse the peripheral nerve function. The NRS was used to assess pain severity using numbers from 0 to 10, where 0 represents no pain and 10 represents the worst pain imaginable.
The TCM syndrome is qi deficiency and blood stasis syndrome. The respondents scored according to the actual situation, with a four-point method for each item. The higher the total score, the worse the symptoms related to the TCM syndrome. The diagnosis of this syndrome was based on the Guidelines for Clinical Research of New Traditional Chinese Medicine Drugs for Syndrome Patterns issued by the National Medical Products Administration (21). According to this guideline, a patient is diagnosed with “qi deficiency and blood stasis” syndrome if they meet one of the following criteria: 1. One primary symptom of qi deficiency plus one primary symptom of blood stasis. 2. One primary symptom of qi deficiency plus one secondary symptom of blood stasis. 3. One primary symptom of blood stasis plus one secondary symptom of qi deficiency. Additionally, the diagnosis requires specific tongue and pulse signs.
Primary symptoms: 1. Qi deficiency: shortness of breath, weakness, fatigue. 2. Blood stasis: stabbing pain, fixed pain, tenderness, vascular stasis, subcutaneous bruising, abdominal masses, or bleeding.
Secondary symptoms: 1. Qi deficiency: spontaneous sweating, lazy speech. 2. dry or scaly skin, limb numbness or paralysis, mental disorders, irritability, forgetfulness, localized sensory abnormalities, or a history of trauma, surgery, or abortion.
Tongue and pulse: purple and dark tongue or petechiae or ecchymosis, sublingual varices, or pale tongue; unsmooth pulse, no pulse, sinking and string pulse, string and slow pulse, or deficient pulse.
Patients underwent nerve conduction study (NCS) testing by independently trained neurologists before and after treatment. Skin surface electrodes were tested with Viking Quest, Nicolet EDX, EMG/NCS/EP/IOM System (Natus, America). We studied the motor conduction of the bilateral median and peroneal nerves by recording the motor conduction velocity and the amplitude. Sensory conduction was tested in the bilateral median and peroneal nerves by measuring the sensory conduction velocity and amplitude. The endpoint was the change in sensory nerve action potential (SNAP), sensory nerve conduction velocity (SNCV), motor nerve action potential (MNAP), and motor nerve conduction velocity (MNCV) in the median and peroneal nerves.
The study coordinator monitored treatment-related adverse events via standard adverse event (CTCAE v.5.0) reporting throughout the study. Included: 1. Patients underwent blood routine, urine routine, stool routine, liver and kidney functions, and electrocardiogram before and after treatment. 2. Patients were evaluated for acupuncture treatment safety (needle fainting, infection, bleeding, hematoma, needle breakage, and other injuries).
EpiData was used to establish the database. Two data managers were responsible for data entry and verification. The statistician performed data statistical analysis.
Statistical analysis was performed using the SAS 9.4 software. If the continuous outcomes obey the normal distribution, we described it as the mean values ± standard deviation. Otherwise, it was expressed as the median, interquartile range, and range. For comparison between the two groups, we used the independent samples t-test. For comparison before and after treatment, we used the paired t-test or the Wilcoxon signed-rank test. Categorical data are expressed as frequencies and percentages. We used the Pearson chi-square test or Fisher’s exact test. All statistical tests used two-sided tests unless otherwise stated, and the significance level was p-value <0.05.
All 70 participants were recruited at the Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, from January 2021 to June 2023. Thirty-five patients were assigned to the verum acupuncture group, and 35 patients were assigned to the sham acupuncture group. In the verum acupuncture group, one patient was lost to follow-up because of schedule conflicts. In the sham acupuncture group, one patient was excluded because of depression and received treatment that might alleviate CIPN. In our study, patients who missed two follow-up assessments were dropped and excluded from the final analysis. To ensure that patients took methylcobalamin on time and in the correct dosage, as well as to prevent unauthorized use of other medications, we implemented the following measures: 1. Patient and family education. 2. Medication record cards. 3. Monitoring and verification. Finally, 68 patients were included in the datasets. The study process is illustrated in Figure 2. We found no statistical differences between the intervention group and control group in the baseline characteristics or clinical characteristics, such as age, sex, BMI, employment status, education, diagnosis, cancer stage, adjuvant type, chemotherapy cycles, ECOG performance status, and months after last chemotherapy, as shown in Table 1.
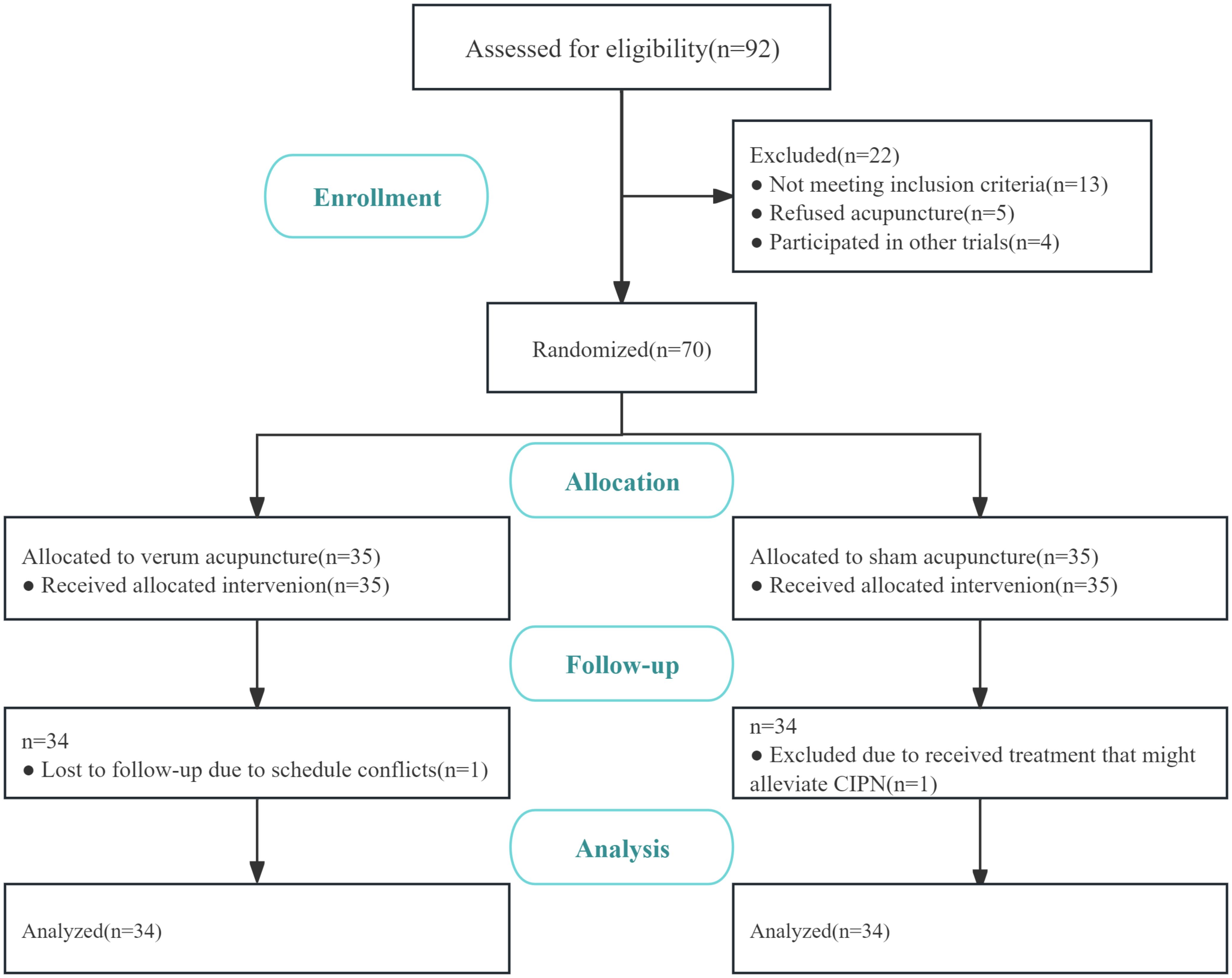
Figure 2. Flow diagram of the study participants.
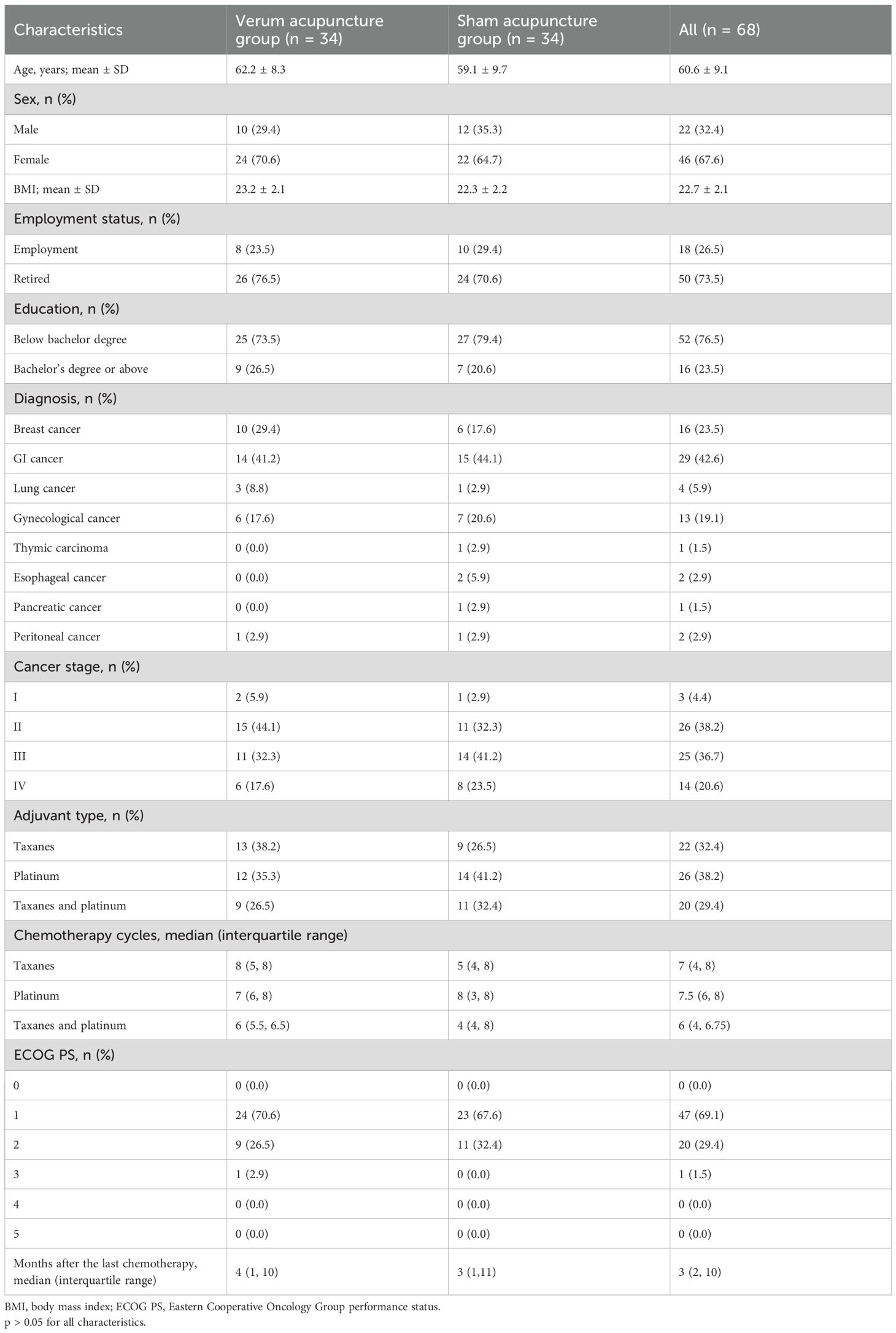
Table 1. Clinical characteristics of participants.
NCI-CTCAE peripheral neuropathy grade was the primary outcome measure of this study. We found no significant difference between the two groups about changes in NCI-CTCAE scores from baseline (p = 0.32), and 1 week (p = 0.53). Significant difference in between-group improvements was in favor of NCI-CTCAE scores from 2 weeks (p = 0.02). Data are summarized in Table 2.
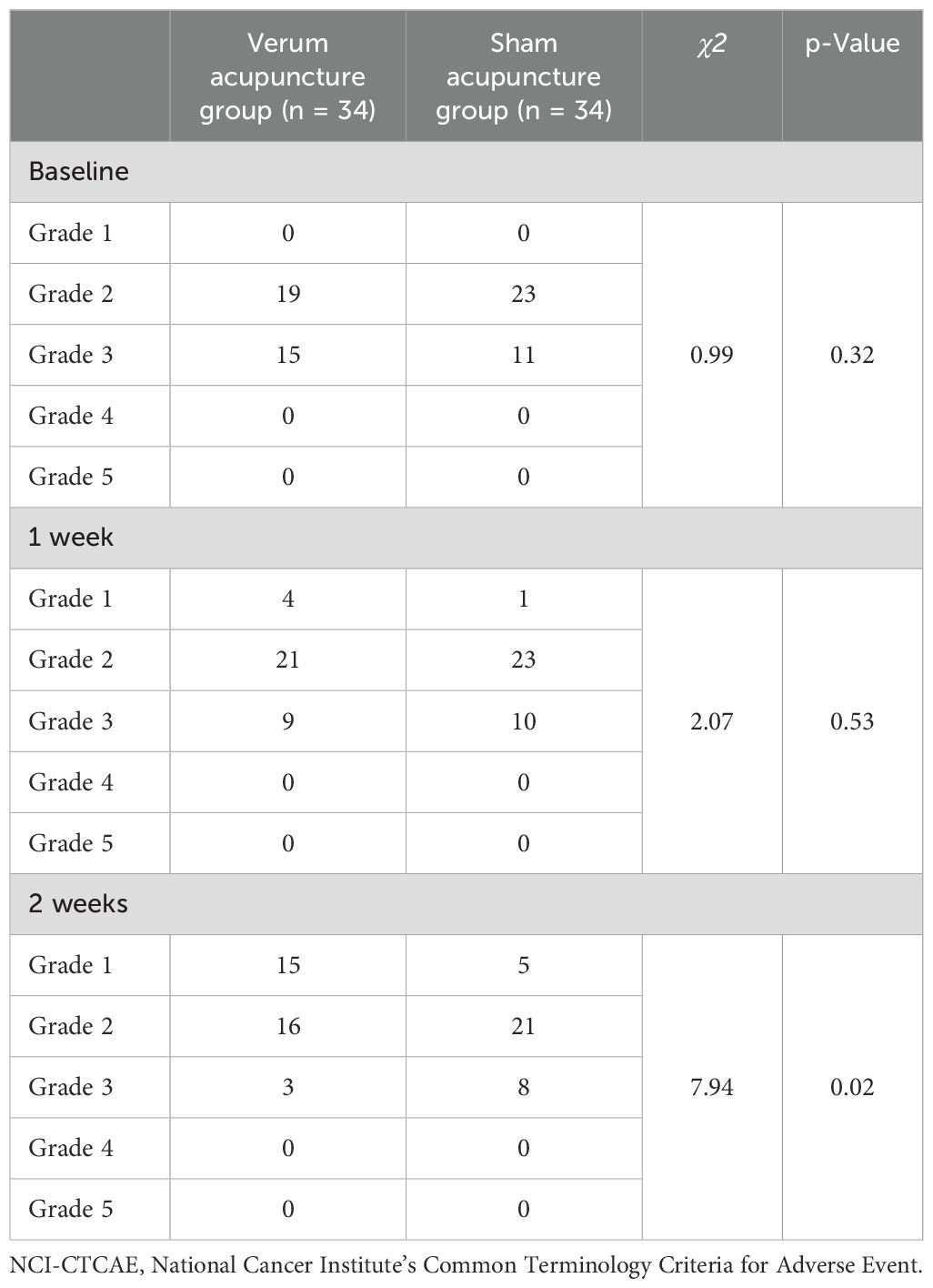
Table 2. NCI-CTCAE scores.
The result, as accessed by the EORTC QLQ-CIPN20, showed no significant differences between the two groups at baseline (p=0.14) and 1 week (p = 0.80), respectively. Significant differences were found between groups for improvements at 2 weeks (p = 0.02). Concurrently, we performed an ANCOVA evaluation, and significant differences were found within the verum acupuncture group (p < 0.001), but not within the sham acupuncture group (p = 0.17), as shown in Table 3.
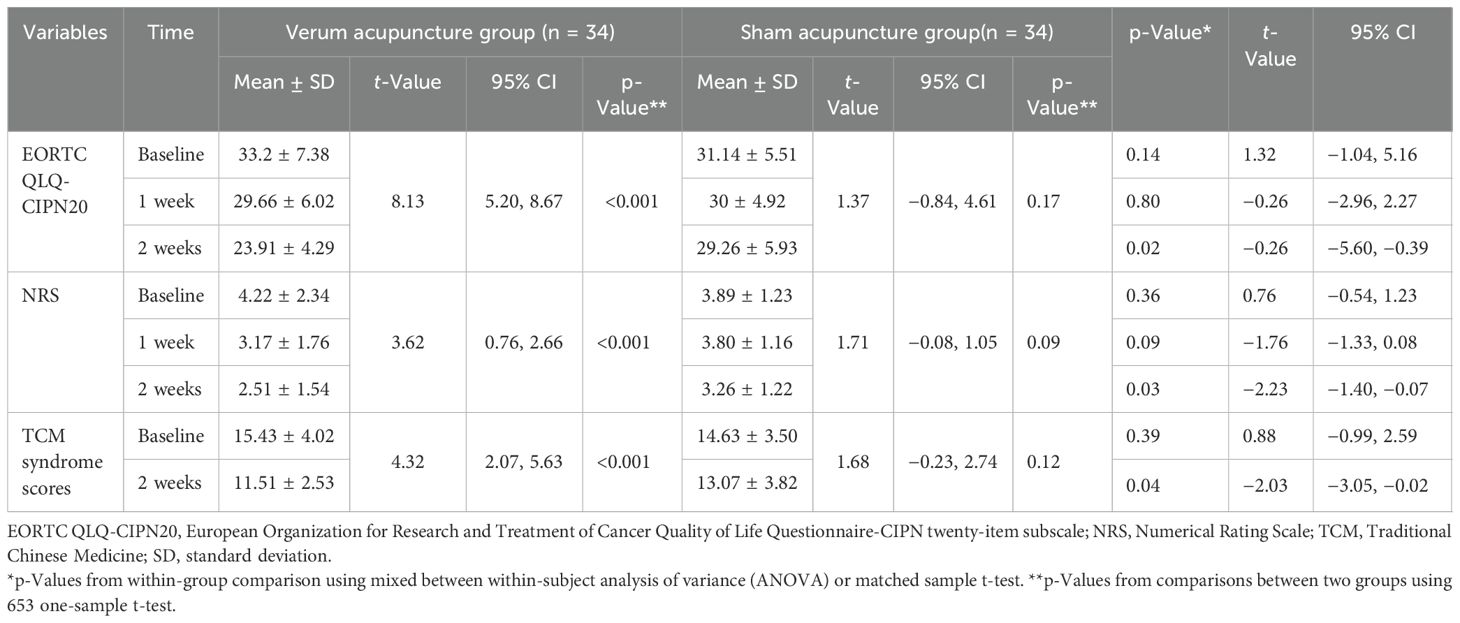
Table 3. Symptom scores of secondary outcomes.
Symptoms of pain in NRS were not statistically different between groups at baseline (p = 0.36) and 1 week (p = 0.09), respectively. Significant between-group alleviations in favor of pain reduction were found in NRS at 2 weeks (p = 0.03). Significant differences were found within the verum acupuncture group (p < 0.001), but not within the sham acupuncture group (p = 0.09), as shown in Table 3.
We found that there were no significant differences between the changes in the two groups in TCM syndrome scores at baseline (p = 0.39). There were significant differences between the improvements of the two groups at 2 weeks (p = 0.04). Significant differences were found within the verum acupuncture group (p < 0.001), but not within the sham acupuncture group (p = 0.12), as shown in Table 3.
The result of statistics showed that the nerve conduction velocity (NCV) (except the median motor NCV) in the verum acupuncture group improved significantly (p < 0.05), while improvement in the sham acupuncture group was not observed (p > 0.05). The SNAP of both median and peroneal nerves improved significantly in the intervention group (p < 0.05), while the MNAP did not (p > 0.05). The difference in nerve action potential (NAP) was not statistically significant in the sham acupuncture group (p > 0.05). There were significant differences between the two groups in the SNAP of the median and peroneal nerves after 2 weeks of treatment (p < 0.05). In contrast, there were no significant differences between the two groups in the MNAP of the median and peroneal nerves after treatment (p > 0.05). The changes in peroneal nerve SNCV and MACV showed statistical significance in comparison to those of the control group (p < 0.05), while the changes in the median nerve SNCV and MNCV showed no statistical significance (p > 0.05), as shown in Table 4.
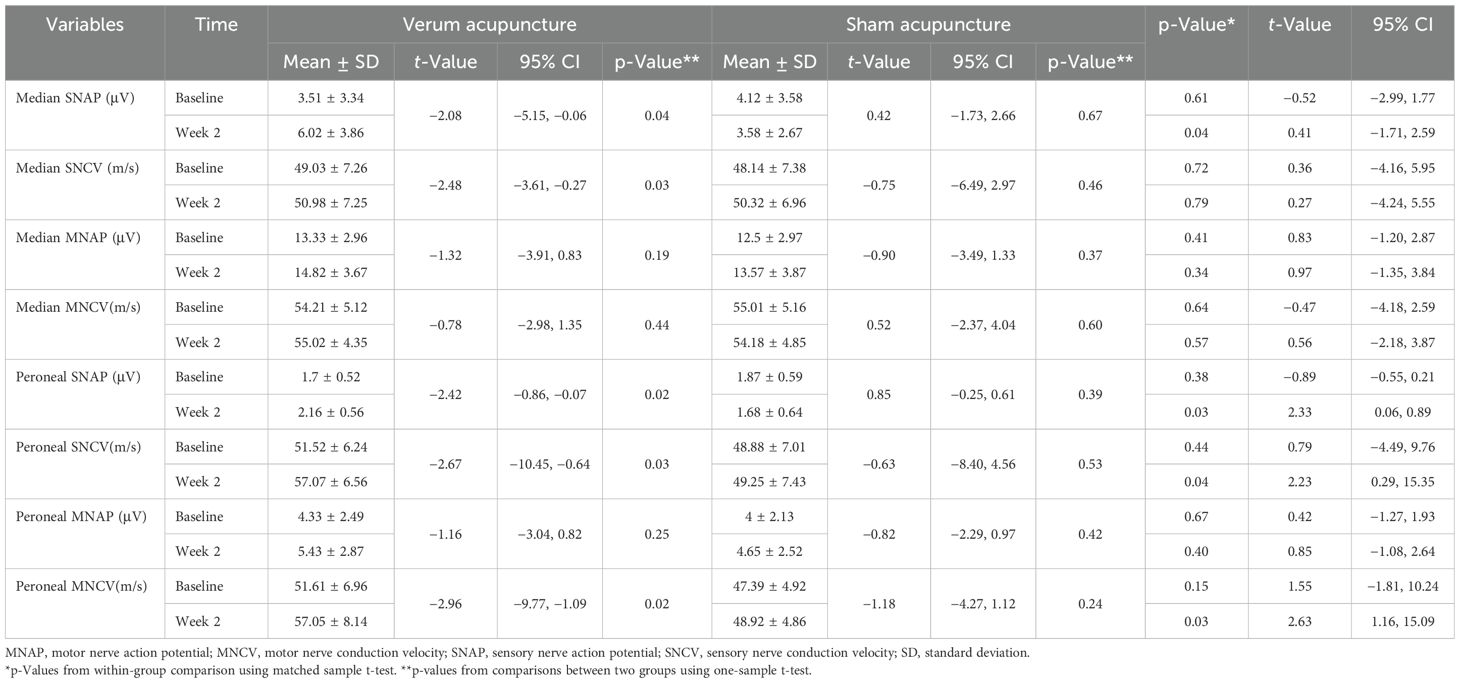
Table 4. Changes in nerve conduction velocity.
Minor hematomas following needle acupuncture were observed in 2 of 68 patients (2.9%) without requiring medical intervention. All events were classified as mild via standard adverse event.
The findings of this study support the feasibility and safety of acupuncture as an intervention for patients with CIPN. After 2 weeks of treatment and follow-up, statistically significant difference was found in NCI-CTCAE scores between the two groups (p = 0.02). This is further supported by the QLQ-CIPN20 where significant improvements were also seen (23.91 ± 4.29 vs. 29.26 ± 5.93). The QLQ-CIPN20, while having many similar questions as the FACT/GOG-NTX, was used in clinical practice and research to measure CIPN. The 20-item scale reflecting three subscales, including sensory, motor, and autonomic symptoms, and functioning were internally consistent (22, 23). Moreover, the NRS was improved best in the verum acupuncture group before and after treatment. We recruited patients with qi deficiency and blood stasis syndrome (24). The verum acupuncture group showed a significant improvement in the TCM syndrome scores. The NCS could more objectively evaluate the nerve fibers’ repair and structural regeneration (25, 26). The results showed that the NCS (SNAP of median and peroneal nerves, SNCV and MACV of peroneal nerve) testing was improved best in the verum acupuncture group. The results of this study showed that acupuncture treatment effectively reduced the neuropathy grade of CIPN, improved symptoms associated with peripheral neuropathy, relieved pain and improved physical fitness for patients, alleviated the TCM symptoms of patients with qi deficiency and blood stasis syndrome, and increased peripheral nerve conduction study.
We conducted a single-center, randomized, controlled, single-blind clinical trial. This trial was well implemented following its study design in terms of randomization, allocation concealment, and blinding of outcome assessors. Several previous studies lacked sham- or attention-control methods (27–29). The influence of placebo effect could interfere with the results. We tried to minimize the risk of bias by using sham acupuncture in the control group. The acupuncturist was aware of group allocation and was asked to talk less with the patients. We hope that these methods could reduce the potential bias to some extent. Moreover, based on ethical and patient considerations, patients in both the two groups took oral mecobalamin tablets.
Acupuncture treatment of CIPN in animal models has some possible mechanisms, including peripheral and spinal levels, but the available evidence is limited. Studies have shown that the mechanism of acupuncture treatment for CIPN may be related to the activation or inhibition of receptors such as spinal opioid receptors (μ, δ, and κ) (30), α2- and β-adrenoceptors (31), 5-hydroxytryptamine 1A (5-HT1A) receptors (32), cannabinoid receptor, and specific ligand-gated ion channels (33). Zhao et al. (34) showed that electroacupuncture alleviates paclitaxel-neuropathic pain via increased mechanical and thermal sensitivity, and this was accompanied by impaired Nrf2-antioxidant response element (Nrf2-ARE) and upregulation of oxidative signals in the dorsal root ganglion (DRG) of rats. According to current studies, acupuncture can be used to increase peripheral microcirculation and skin blood perfusion (35–37), and may contribute to nerve repair with measurable improvement of the axons or myelin sheaths (38).
There is no record of CIPN in the ancient Chinese medical books. According to its typical symptoms, such as numbness, pain, and muscle weakness, we attribute it to the category of “Bi disease” and “impotence.” According to our preliminary study and references, the syndrome of qi deficiency and blood stasis is the main syndrome of CIPN (39–44). Chemotherapeutic drugs are very toxic products, injuring people’s qi. Qi deficiency is unable to promote the circulation of blood leading to blood stasis and internal obstruction. Then, the skin does not get warmth and moistening from the qi and blood. The appearance of numbness, limb sensory loss, movement disorders and muscle atrophy, and other symptoms, can be attributed to the Chinese medicine range of “Bi disease and impotence.” The ancient Chinese medical text “Treatment of Bi Disease, Classical Evidence Treatment and Cure” says: “The stasis of qi and blood for a long time leads to Bi disease,” suggesting that the pathogenesis of Bi disease is stagnation of qi and blood. The Bi disease will eventually turn into impotence after a long time, which means that the qi and blood become seriously stagnated.
The “Yellow Emperor’s Classic of Internal Medicine” has the following words: “Treat impotence by taking Yangming meridian,” “Stabbing Yangming meridian produces qi and blood,” and the Yangming meridian is the meridian with a high level of qi and blood, which has the effect of warming the yang and dredging the collaterals, tonifying qi and blood. So acupoints on treating impotence are mostly based on the Yangming meridian. The ST36 point is the lower He-sea point of the stomach meridian of Yangming. According to the “Yellow Emperor’s Classic of Internal Medicine”: “If you have got Bi disease or cold for a long time, Sanli point must be taken.” Therefore, Zusanli (ST36) is the important acupoint for the treatment of CIPN combined with Quchi (LI11) and Hegu (LI4), the combined acupoints of hand Yangming meridian, which plays an important role in benefiting qi and warming yang. Taichong (LR3) and Hegu (LI4), the combination of Yangming meridian and Jueyin meridian, one yin and one yang, one zang and one fu, reconcile the yin yang and qi and blood in the upper and lower parts of the body, so that the yin and yang are reconciled, and the meridians are unobstructed. The RN6 of the Ren meridian is the sea of qi, which has the effect of reinforcing yuan qi, tonifying kidney and consolidating essence. So, RN6 can help the acupoints of Yangming meridian to benefit qi. The Xuehai (SP10) is the acupoint of the spleen meridian of the foot Taiyin, which has the effect of invigorating blood circulation and unblocking blood flow. A-B Classic of Acupuncture and Moxibustion mentioned that “if the blood is obstructed…… Xuehai (SP10) will be taken.” The EX-LE10 and the EX-UE9 belongs to the extraordinary acupoints that have a strong effect of regulating local qi and blood and activating meridians and collaterals. In general, the principle of acupuncture treatment involves activating meridians and collaterals, benefiting qi, and promoting blood circulation to remove blood stasis.
A meta-analysis of 19 studies with 1,108 patients found that acupuncture for CIPN had a significant advantage in terms of overall efficacy (45) and that ST36, LI4, LI11, and LR3 were the most frequently used acupoints in terms of selection. Although there are many similarities in the selection of acupoints in these studies, there is no uniformity of criteria. The selection of acupoints for our study was guided by syndrome differentiation. According to this differentiation, the patients with a syndrome of qi deficiency and blood stasis were enrolled. The principle of acupuncture treatment involves activating meridians and collaterals, benefiting qi, and promoting blood circulation to remove blood stasis, which makes our treatment of CIPN patients more targeted and effective. Based on clinical findings in existence (27, 46–51), acupuncture is estimated to have potential therapeutic effect in treating symptoms of CIPN with particular advantages of relieving pain and improving the quality of life. Some studies are single-arm trials and deficient in randomization and control (49–51). Some studies used a blank control rather than a sham acupuncture group control (27). The results of this study also showed that acupuncture treatment effectively relieved pain and improved physical fitness for patients. To eliminate the potential placebo effect caused by the acupuncture itself, we created the sham acupuncture group. In addition, the verum acupuncture could alleviate TCM symptoms of patients with the syndrome of qi deficiency and blood stasis.
There are several important areas for improvement as follows. 1. The most significant limitation of the trial was the short intervention time, although our findings suggest certain effects after 2 weeks of treatment in the verum acupuncture group. We followed up the patients who had completed the treatment. Some patients chose to continue acupuncture treatment, and as the treatment time prolonged, the patients’ peripheral nerve-related symptoms were relieved more significantly. Based on this trial’s result and the overall positive trend, future studies may consider including longer treatment and follow-up phases. 2. This study was a small-sample single-center trial, and only patients from China were observed. We look forward to a larger multi-center trial to further verify our results.
This study supports the feasibility of acupuncture combined with medication as an intervention for patients with CIPN and determines its efficacy and safety in improving peripheral neuropathy. As there are no known effective treatments to prevent or reverse CIPN, the potential symptom management benefit of acupuncture in CIPN deserves further study in a large-sample multi-center trial with a long-term follow-up. Furthermore, exploring the predictive genetic risk markers associated with the development of CIPN may be crucial to improve the design of future clinical trials to test neuroprotective strategies targeting CIPN.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Medical Ethics Committee of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JX: Data curation, Methodology, Writing – original draft, Writing – review & editing. QZ: Methodology, Writing – review & editing. NX: Methodology, Writing – review & editing. CZ: Supervision, Writing – review & editing. WX: Methodology, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by grants from the Beijing Municipal Administration of Hospitals Incubating Program (grant number: PZ2020019) and the Beijing Municipal Administration of Hospitals’ Youth Programme (grant number: QML20161001).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cavaletti G, Marmiroli P. Chemotherapy-induced peripheral neurotoxicity. Nat Rev Neurol. (2010) 6:657–66. doi: 10.1038/nrneurol.2010.160
2. Brown TJ, Sedhom R, Gupta A. Chemotherapy-induced peripheral neuropathy. JAMA Oncol. (2019) 5:750. doi: 10.1001/jamaoncol.2018.6771
3. Li X, Wu L, Bai D, Li J. Peripheral neurotoxicity induced by albumin-bound paclitaxel: a case report. Front Oncol. (2024) 14:1440205. doi: 10.3389/fonc.2024.1440205
4. Stubblefield MD, Burstein HJ, Burton AW, Custodio CM, Deng GE, Ho M, et al. NCCN task force report: management of neuropathy in cancer. J Natl Compr Canc Netw. (2009) 7:S1–S28. doi: 10.6004/jnccn.2009.0078
5. Seretny M, Currie GL, Sena ES, Ramnarine S, Grant R, MacLeod MR, et al. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain. (2014) 155:2461–70. doi: 10.1016/j.pain.2014.09.020
6. Staff NP, Grisold A, Grisold W, Windebank AJ. Chemotherapy-induced peripheral neuropathy: A current review. Ann Neurol. (2017) 81:772–81. doi: 10.1002/ana.24951
7. Knoerl R. CE: chemotherapy-induced peripheral neuropathy. Am J Nurs. (2021) 121:26–30. doi: 10.1097/01.NAJ.0000742060.56042.e7
8. Banach M, Juranek JK, Zygulska AL. Chemotherapy-induced neuropathies-a growing problem for patients and health care providers. Brain Behav. (2016) 7::e00558. doi: 10.1002/brb3.558
9. Hershman DL, Lacchetti C, Loprinzi CL. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. (2014) 32:1941–67. doi: 10.1200/JOP.2014.001776
10. Schwab L, Visovsky C. Psychological distress and quality of life in breast cancer survivors with taxane-induced peripheral neuropathy: A scoping review. Front Oncol. (2023) 12:1005083. doi: 10.3389/fonc.2022.1005083
11. Pike CT, Birnbaum HG, Muehlenbein CE, Pohl GM, Natale RB. Healthcare costs and workloss burden of patients with chemotherapy-associated peripheral neuropathy in breast, ovarian, head and neck, and nonsmall cell lung cancer. Chemother Res Pract. (2012) 2012:913848. doi: 10.1155/2012/913848
12. Desforges AD, Hebert CM, Spence AL, Reid B, Dhaibar HA, Cruz-Topete D, et al. Treatment and diagnosis of chemotherapy-induced peripheral neuropathy: An update. BioMed Pharmacother. (2022) 147:112671. doi: 10.1016/j.biopha.2022.112671
13. Stillman M, Cata JP. Management of chemotherapy-induced peripheral neuropathy. Curr Pain Headache Rep. (2006) 10:279–87. doi: 10.1007/s11916-006-0033-z
14. Loprinzi CL, Lacchetti C, Bleeker J, Cavaletti G, Chauhan C, Hertz DL, et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. J Clin Oncol. (2020) 38:3325–48. doi: 10.1200/JCO.20.01399
15. Bae EH, Greenwald MK, Schwartz AG. Chemotherapy-induced peripheral neuropathy: mechanisms and therapeutic avenues. Neurother. (2021) 18:2384–96. doi: 10.1007/s13311-021-01142-2
16. Kutcher AM, LeBaron VT. Evaluating acupuncture for the treatment of chemotherapy-induced peripheral neuropathy: an integrative review. West J Nurs Res. (2022) 44:169–79. doi: 10.1177/0193945921992538
17. Lu W, Giobbie-Hurder A, Freedman RA, Shin IH, Lin NU, Partridge AH, et al. Acupuncture for chemotherapy-induced peripheral neuropathy in breast cancer survivors: A randomized controlled pilot trial. Oncol. (2020) 25:310–8. doi: 10.1634/theoncologist.2019-0489
18. Pu T, Liu Y, Wang J, Zhang J, Zhang J, Ran Z, et al. Acupuncture and other traditional Chinese medicine therapies in the treatment of children’s tic syndrome: A network meta-analysis. Front Neurosci. (2023) 17:1156308. doi: 10.3389/fnins.2023.1156308
19. Cao L, Zhu G, Wang X, Kuang Z, Song X, Ma X, et al. Yiqi Wenyang Jiedu prescription for preventing and treating postoperative recurrence and metastasis of gastric cancer: a randomized controlled trial protocol. Front Oncol. (2024) 14:1326970. doi: 10.3389/fonc.2024.1326970
20. Cavaletti G, Cornblath DR, Merkies ISJ, Postma TJ, Rossi E, Frigeni B, et al. The chemotherapy-induced pe-ripheral neuropathy outcome measures standardization study:from consen-sus to the first validity and reliability findings. Ann Oncol. (2013) 24:454–62. doi: 10.1093/annonc/mds329
21. National Medical Products Administration. Guidelines for clinical research of new traditional chinese medicine drugs for syndrome patterns. Available online at: https://www.nmpa.gov.cn/xxgk/ggtg/qtggtg/20181106155701473.html. (2018-11-06). (Accessed February, 2021)
22. Rattanakrong N, Thipprasopchock S, Siriphorn A, Boonyong S. Reliability and validity of the EORTC QLQ-CIPN20 (European organization for research and treatment of cancer quality of life questionnaire-chemotherapy-induced peripheral neuropathy 20-item scale) among thai women with breast cancer undergoing taxane-based chemotherapy. Asian Pac J Cancer Prev. (2022) 23:1547–53. doi: 10.31557/APJCP.2022.23.5.1547
23. Abu Sharour L. Psychometric evaluation of the arabic version the european organization for research and treatment of cancer quality of life questionnaire for chemotherapy-induced peripheral neuropathy questionnaire (EORTC QLQ-CIPN20). Appl Neuropsychol Adult. (2021) 28:614–8. doi: 10.1080/23279095.2019.1677232
24. Xu WR, Hua BJ, Hou W, Bao YJ. Clinical randomized controlled study on acupuncture for treatment of peripheral neuropathy induced by chemotherapeutic drugs. Zhongguo Zhen Jiu. (2010) 30:457–60. doi: 10.13703/j.0255-2930.2010.06.011
25. Donofrio PD, Albers JW. AAEM minimonograph 34: polyneuropathy: classification by nerve conduction studies and electromyography. Muscle Nerve. (1990) 13:889–903. doi: 10.1002/mus.880131002
26. Litscher G, Wang L, Schwarz G, Schikora D. Increases of intracranial pressure and changes of blood flow velocity due to acupressure, needle and laser needle acupuncture? Forsch Komplementarmed Klass Naturheilkd. (2005) 12:190–5. doi: 10.1159/000087044
27. Molassiotis A, Suen LKP, Cheng HL, Mok TSK, Lee SCY, Wang CH, et al. A randomized assessor-blinded wait-list-controlled trial to assess the effectiveness of acupuncture in the management of chemotherapy-induced peripheral neuropathy. Integr Cancer Ther. (2019) 18:1534735419836501. doi: 10.1177/1534735419836501
28. Iravani S, Kazemi Motlagh AH, Emami Razavi SZ, Shahi F, Wang J, Hou L, et al. Effectiveness of acupuncture treatment on chemotherapy-induced peripheral neuropathy: A pilot, randomized, assessor-blinded, controlled trial. Pain Res Manage. (2020) 2020:2504674. doi: 10.1155/2020/2504674
29. Cai Y, Zhang CS, Zhang AL, Da Costa C, Xue CC, Wen Z. Electroacupuncture for poststroke spasticity: results of a pilot pragmatic randomized controlled trial. J Pain Symptom Manage. (2021) 61:305–14. doi: 10.1016/j.jpainsymman.2020.07.034
30. Meng X, Zhang Y, Li A, Xin J, Lao L, Ren K, et al. The effects of opioid receptor antagonists on electroacupuncture-produced anti-allodynia/hyperalgesia in rats with paclitaxel-evoked peripheral neuropathy. Brain Res. (2011) 1414:58–65. doi: 10.1016/j.brainres.2011.08.004
31. Choi JW, Kang SY, Choi JG, Kang DW, Kim SJ, Lee SD, et al. Analgesic effect of electroacupuncture on paclitaxel-induced neuropathic pain via spinal opioidergic and adrenergic mechanisms in mice. Am J Chin Med. (2015) 43:57–70. doi: 10.1142/S0192415X15500044
32. Zhang Y, Li A, Xin J, Ren K, Berman BM, Lao L, et al. Electroacupuncture alleviates chemotherapy-induced pain through inhibiting phosphorylation of spinal CaMKII in rats. Eur J Pain. (2018) 22:679–90. doi: 10.1002/ejp.1132
33. Li Y, Yin C, Li X, Liu B, Wang J, Zheng X, et al. Electroacupuncture alleviates paclitaxel-induced peripheral neuropathic pain in rats via suppressing TLR4 signaling and TRPV1 upregulation in sensory neurons. Int J Mol Sci. (2019) 20:E5917. doi: 10.3390/ijms20235917
34. Zhao X, Liu L, Wang Y, Wang G, Zhao Y, Zhang Y. Electroacupuncture enhances antioxidative signal pathway and attenuates neuropathic pain induced by chemotherapeutic paclitaxel. Physiol Res. (2019) 68:501–10. doi: 10.33549/physiolres.934084
35. Valentini J, Sigl M, Dunckel C, Krisam J, Amendt K, Greten HJ. Can acupuncture increase microcirculation in peripheral artery disease and diabetic foot syndrome? - a pilot study. Front Med (Lausanne). (2024) 11:1371056. doi: 10.3389/fmed.2024.1371056
36. VVickers AJ, Vertosick EA, Lewith G, MacPherson H, Foster NE, Sherman KJ, et al. Acupuncture for chronic pain: update of an individual patient data meta-analysis. J Pain. (2018) 19:455–74. doi: 10.1016/j.jpain.2017.11.005
37. Zhao L, Chen J, Li Y, Sun X, Chang X, Zheng H, et al. The long-term effect of acupuncture for migraine prophylaxis: A randomized clinical trial. JAMA Intern Med. (2017) 177:508–15. doi: 10.1001/jamainternmed.2016.9378
38. Litscher G, Wang L, Huber E, Nilsson G. Changed skin blood perfusion in the fingertip following acupuncture needle introduction as evaluated by laser Doppler perfusion imaging. Lasers Med Sci. (2002) 17:19–25. doi: 10.1007/s10103-002-8262-9
39. Xu WR, Hua BJ, Hou W, Bao YJ. Clinical randomized controlled study on acupuncture for treatment of peripheral neuropathy induced by chemotherapeutic drugs. Chinese Acupuncture Moxibustion. (2010) 30:457–60. doi: 10.13703/j.0255-2930.2010.06.011
40. Weiru XU, Mingwei YU, Qi FU. A retrospective study on the treatment of oxaliplatin-induced peripheral neuropathy by adding and subtracting Huangqi Guizhi Wu Wu Wu Tang. J Guangzhou Univ Traditional Chin Med. (2022) 39:24–30. doi: 10.13359/j.cnki.gzxbtcm.2022.01.005
41. Linbo L, Xiaofei G, Dan L. Research advancements in the traditional Chinese medicine treatment of taxane-induced peripheral neuropathy. Chin J Clin Oncol Rehabil. (2024) 31:561–70. doi: 10.13455/j.cnki.cjcor.113494-2024-2024-0167
42. Yuan YU, Lijuan CHEN, Jinfang SUN. Research progress on chinese and western medicine in the clinical treatment of chemotherapy-induced peripheral neuropathy. World Chin Med. (2024) 19:1348–54. doi: 10.3969/j.issn.1673-7202.2024.09.023
43. World Federation of Chinese Medicine Societies Tumor Precision Medicine Professional Committee, Jiege HUO. Expert consensus on the prevention and treatment of chemotherapy-induced peripheral neuropathy by integrated Chinese and Western medicine. Chin J Surg Oncol. (2023) 15:521–30. doi: 10.3969/j.issn.1674-4136.2023.06.001
44. Taxane-related peripheral neuropathy standardized management group. Expert consensus on standardized management of taxane-related peripheral neuropathy. Chin J Front Med Sci. (2020) 12:41–51. doi: 10.12037/YXQY.2020.03-07
45. Dai L. Acupuncture treatment for chemotherapy-induced peripheral neuropathy: meta-analysis. Guangzhou Univ Chin Med. (2019). doi: 10.27044/d.cnki.ggzzu.2019.000473
46. Schroeder S, Meyer-Hamme G, Epplée S. Acupuncture for chemotherapy-induced peripheral neuropathy (CIPN): a pilot study using neurography. Acupunct Med. (2012) 30:4–7. doi: 10.1136/acupmed-2011-010034
47. Lu W, Matulonis UA, Dunn JE, Lee H, Doherty-Gilman A, Dean-Clower E, et al. The feasibility and effects of acupuncture on quality of life scores during chemotherapy in ovarian cancer: results from a pilot, randomized sham-controlled trial. Med Acupunct. (2012) 24:233–40. doi: 10.1089/acu.2012.0904
48. Greenlee H, Crew KD, Capodice J, Awad D, Buono D, Shi Z, et al. Randomized sham-controlled pilot trial of weekly electro-acupuncture for the prevention of taxane-induced peripheral neuropathy in women with early stage breast cancer. Breast Cancer Res Treat. (2016) 156:453–64. doi: 10.1007/s10549-016-3759-2
49. Ben-Horin I, Kahan P, Ryvo L, Inbar M, Lev-Ari S, Geva R. Acupuncture and reflexology for chemotherapy-induced peripheral neuropathy in breast cancer. Integr Cancer Ther. (2017) 16:258–62. doi: 10.1177/1534735417690254
50. Bao T, Seidman AD, Piulson L, Vertosick E, Chen X, Vickers AJ, et al. A phase IIA trial of acupuncture to reduce chemotherapy-induced peripheral neuropathy severity during neoadjuvant or adjuvant weekly paclitaxel chemotherapy in breast cancer patients. Eur J Cancer. (2018) 101:12–9. doi: 10.1016/j.ejca.2018.06.008
Keywords: acupuncture, chemotherapy, peripheral neuropathy, therapeutic, randomized controlled trial
Citation: Xu J, Zhang Q, Xue N, Zhang C and Xu W (2025) The therapeutic effect of acupuncture in the treatment of chemotherapy-induced peripheral neuropathy: a randomized controlled trial. Front. Oncol. 15:1500410. doi: 10.3389/fonc.2025.1500410
Received: 23 September 2024; Accepted: 24 March 2025;
Published: 16 April 2025.
Edited by:
Yi-Hung Chen, China Medical University, TaiwanReviewed by:
Chien-Chen Huang, China Medical University, TaiwanCopyright © 2025 Xu, Zhang, Xue, Zhang and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weiru Xu, eHV3ZWlydUBianpob25neWkuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.