 Ka Hey Agnes Fong
Ka Hey Agnes Fong Isaac Ho
Isaac Ho Tsz Him So
Tsz Him So
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol., 12 February 2025
Sec. Cancer Immunity and Immunotherapy
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1483117
Immunotherapy has been the mainstay of the initial systemic treatment for metastatic melanoma regardless of the tumor’s genetic mutation status (Atkins et al., 2022). It is known to offer long-term overall and treatment-free survival benefits, also with generally tolerable side effect profiles. However, upon disease progression on first- and second-line immunotherapy, further systemic treatment options are limited especially for cases without actionable molecular alterations. With emerging evidence suggesting that radiotherapy can enhance the efficacy of immunotherapy via various mechanisms, together with its potential abscopal effect, the possibility of overcoming immunotherapy resistance with radiotherapy is theoretically sound. We report a case of metastatic melanoma which demonstrated a reversal of immunotherapy resistance after the addition of low-dose radiotherapy to progressive tumor. Complete metabolic remission is achieved with durable response observed.
In patients with metastatic melanoma, genetic sequencing has been available in identifying actionable molecular alterations—most commonly mutation in the BRAF gene at V600 codon. Nonetheless, the combination of immune checkpoint inhibitor with anti-programmed cell death-1 protein (anti-PD1) and anti-cytotoxic T-lymphocyte-associated protein 4 (anti-CTLA4) remains the recommended choice of initial therapy in treatment-naïve, immunotherapy-eligible patients (1, 2), regardless of genetic mutation status (3).
Even though there are remarkable durability of disease control and survival benefits in melanoma patients treated with immunotherapy, there is still a substantial proportion of 40%–50% patients who showed a lack of response to this treatment (4–6). The development of immunotherapy resistance is also inevitable in the initially responding group. Subsequent treatment options are limited especially in patients who are not eligible for the targeted agents. The proposed immunomodulatory effect of low-dose radiotherapy (L-XRT) has shed lights of hope to these patients. The addition of radiotherapy to immunotherapy is increasingly recognized as a potential method to enhance the anti-tumor efficacy and overcome resistance (7, 8). This phenomenon is supported by various pre-clinical models and is also observed in some clinical trials. In addition to the localized effect of radiotherapy, the potential of radiation-induced abscopal effect and the generation of immune memory are also being explored with favorable observations by far. It is therefore plausible to postulate that L-XRT can improve both the local and systemic control of melanoma treated with immunotherapy.
Here we present a case of a patient with metastatic melanoma which demonstrated reversal of immunotherapy resistance, with subsequent exceptional treatment response to the combination of L-XRT and anti-PD1 therapy.
In January 2021, a 63-year-old man with a history of metabolic syndrome and deranged renal function presented with a left big toe mass underneath the nail. He was diagnosed with left big toe melanoma subsequently and underwent left big toe resection with left groin lymph node dissection in February 2021. The pathology results confirmed melanoma with lymph node metastases. BRAF mutation was negative.
He was put on adjuvant nivolumab (240 mg every 2 weeks) for 1 month after the operation. After 16 cycles of nivolumab in October 2021, tumor recurrence was noted with increasing cutaneous nodules over the left thigh and the groin region. The 18F-FDG PET/CT scan found no other metastases. The biopsy results of the left groin lymph node proved a BRAF-negative melanoma recurrence. A next-generation sequencing did not show any driver mutation.
He was started on ipilimumab (80 mg) and pembrolizumab (200 mg), given every 3 weeks, since November 2021. After 4 cycles of dual immunotherapy, the results of PET/CT in 1/2022 showed a mixed response with resolution of the known left groin and thigh lesions, but two new lesions were found over the left knee and the left groin, respectively. Resection of the new nodules was performed, and the pathology results confirmed theseto be metastatic melanoma. He was then continued on maintenance pembrolizumab every 3 weeks. Another PET/CT was performed in May 2022 after 5 more cycles, and it showed partial response with one residual left pelvic lesion. Stereotactic body radiation therapy (SBRT) of 40 Gy over five fractions on alternate days was given to the pelvic lymph node in May 2022. He received a total of 11 cycles of pembrolizumab and was put on drug holiday from June 13, 2022 due to tolerance from immune-related grade 2 skin rash and blisters over the bilateral lower limbs and difficult wound healing.
The interim PET/CT in September 2022 showed no recurrence of disease upon drug holiday. In March 2023, new masses over the small bowel and right peritoneum were noted on PET/CT. A small bowel excision was done on April 13, 2023. The pathology results showed recurrence of melanoma with a 6-cm-sized tumor, multiple mesenteric lymph nodes of 2 to 3 cm, and numerous metastatic nodules over the small bowel mesentery. Next-generation sequencing showed no driver mutations.
He was rechallenged with ipilimumab (75 mg) and pembrolizumab from April 2023, switching to maintenance pembrolizumab alone upon the 5th cycle. The PET/CT results in July 2023 showed a rebound of the disease with a 2.2-cm mesenteric lesion in the peritoneum (Figure 1).
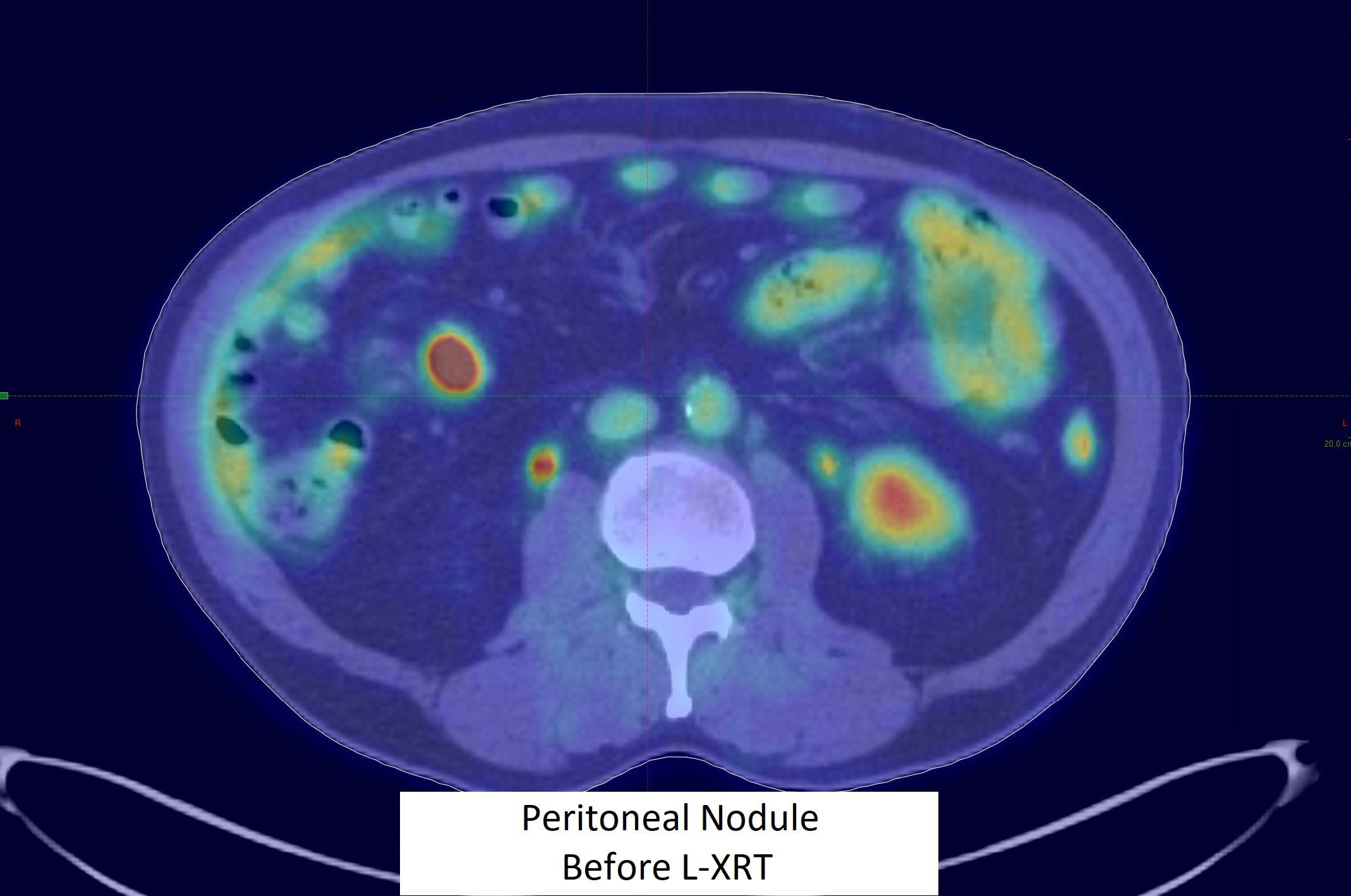
Figure 1. Peritoneal nodule before L-XRT.
A low-dose radiation of 10 Gy over five daily fractions to the mesenteric nodule with 2cm GTV-PTV margin (Figure 2) was given from July 21 to 26, 2023. The treatment was well tolerated, complicated only by self-resolving grade 2 diarrhea.
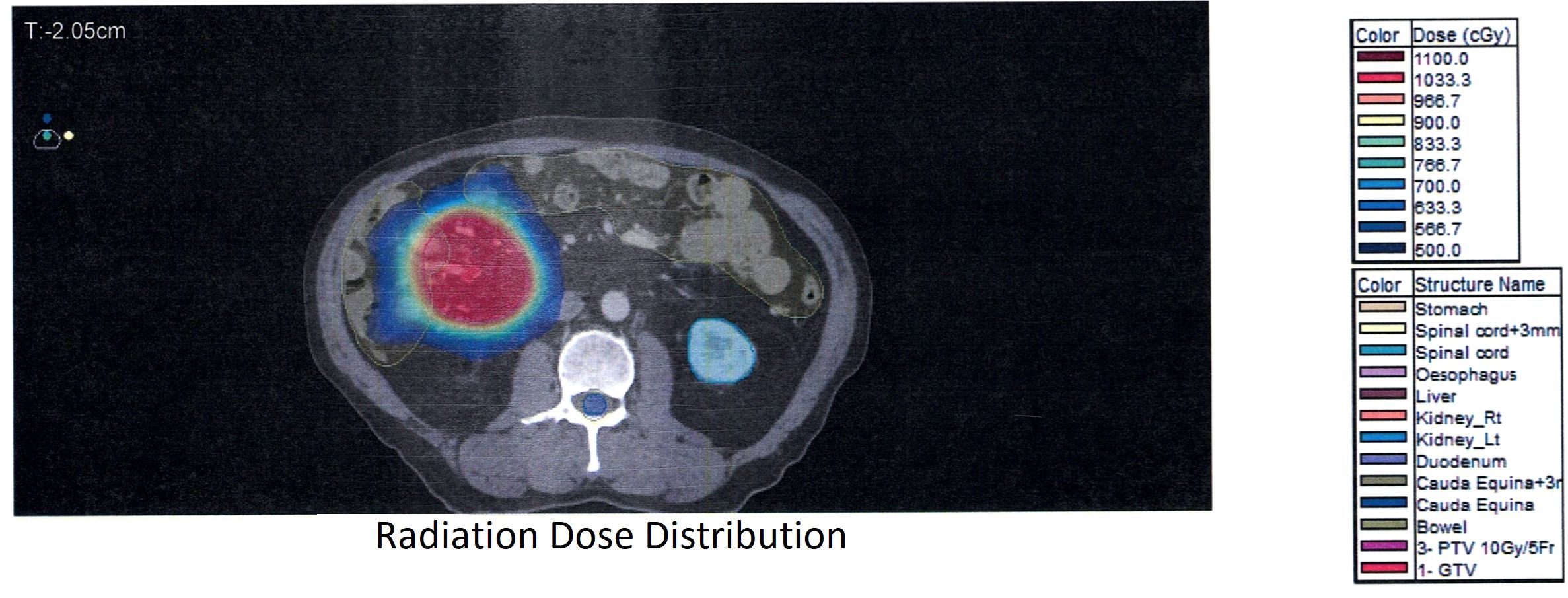
Figure 2. Radiation dose distribution.
He continued with maintenance pembrolizumab. The progress CT done 2 months after low-dose RT showed shrinking of the mesenteric nodule from 2.2 to 1.4 cm; no new lesions were identified. The subsequent CT in December 2023 and PET/CT in April 2024 showed complete remission of disease (Figure 3).
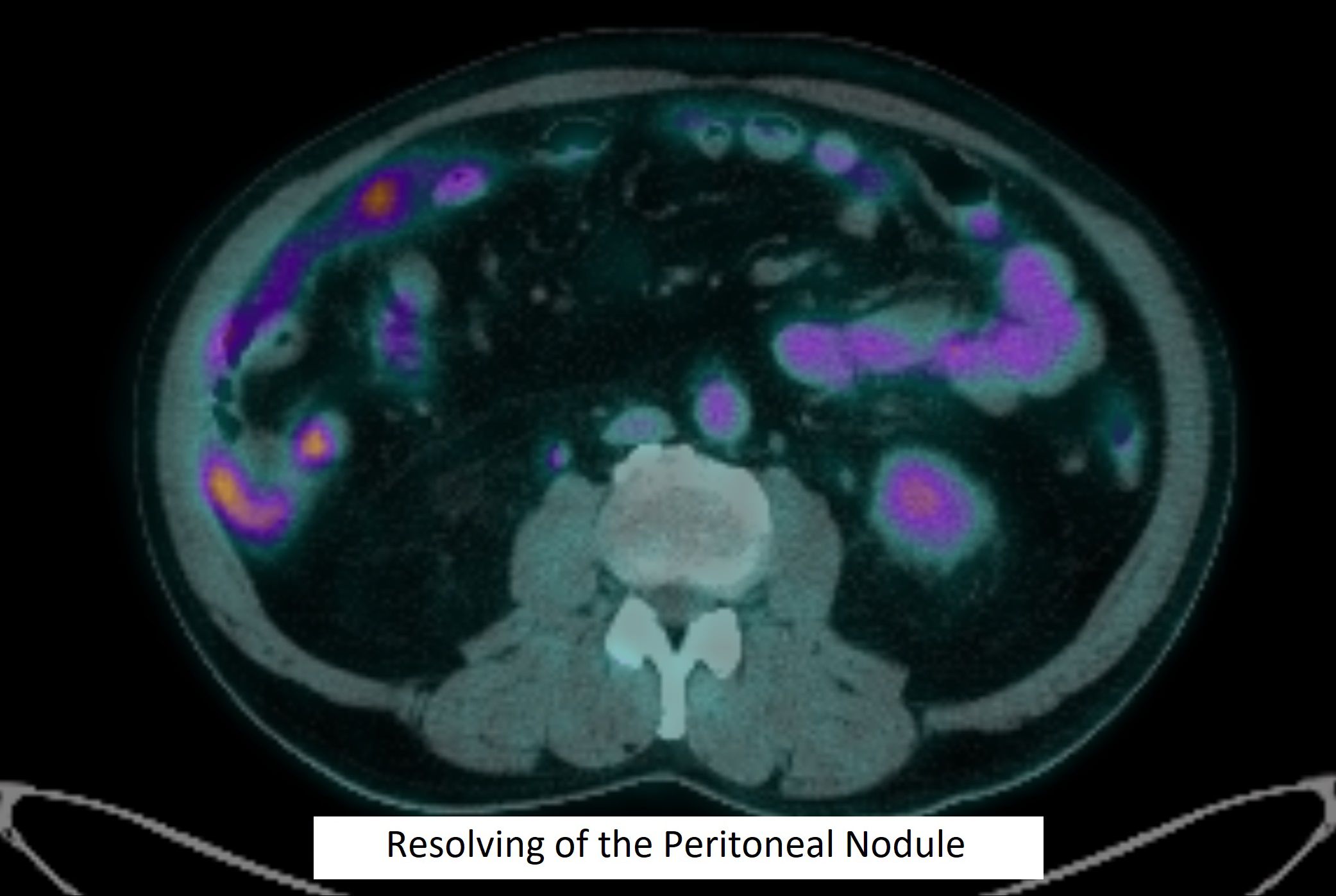
Figure 3. Resolving of the peritoneal nodule.
This patient continued to receive pembrolizumab and finished cycle 19 in June 2024. He tolerated the immunotherapy well and did not have any long-term side effects from the radiation.
Table 1 below shows a brief description of major events occurred to our patient listed in temporal sequence.
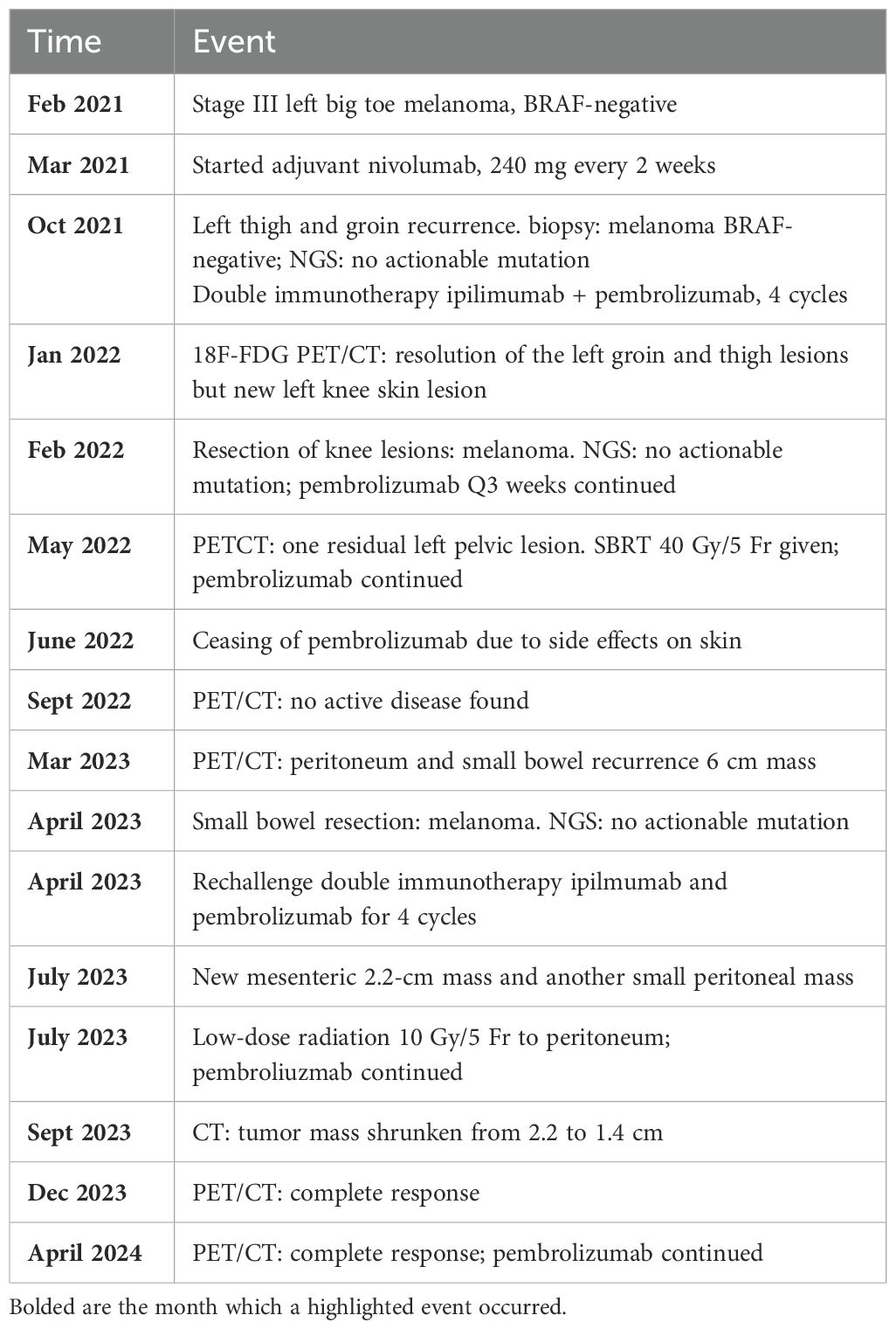
Table 1. Highlighted events occurred to our patient in temporal sequence.
PETCT scan has been used as imaging modality for follow-up diagnostic assessment. Pathological diagnoses were provided on the surgical specimens. Therapeutic intervention included immunotherapy drugs (ipilimumab, pembrolizumab, nivolumab) and radiation (stereotactic body radiation and low-dose radiation). Outcome was complete resolution of the abdominal tumor. No significant side effects or adverse outcomes were found.
This is an intriguing case of metastatic melanoma which demonstrated a promising result of achieving complete tumor resolution with the addition of low-dose radiation therapy (L-XRT) despite its initial resistance to anti-PD1 immunotherapy. This outcome aligns with the emerging evidence which suggests that combining radiotherapy with immunotherapy can enhance antitumor responses and overcome resistance (7, 8).
Radiotherapy has long been recognized for its ability to induce direct cytotoxic effects on tumor cells through DNA damage and subsequent immunogenic cell death (9). However, recent studies have highlighted its potential to modulate the tumor microenvironment (TME) and enhance systemic antitumor immunity. Low-dose radiation, defined as 0.5–2 Gy per fraction for up to 1–10 Gy total, has been shown to overcome the inhibitory stroma within the TME, facilitating better immune cell infiltration and activation (10). This mechanism likely played a crucial role in the observed clinical outcome of our patient.
The RadScopal technique, which involves the strategic use of both high-dose and low-dose radiation, has demonstrated significant potential of RT in enhancing the efficacy of immunotherapy (10). In our patient’s case, the use of L-XRT has likely contributed to the reactivation of the immune response against the tumor. This is supported by findings from various studies where L-XRT was shown to enhance systemic anti-tumor immune responses via multiple mechanisms. Some showed that L-XRT increases the proportion of effector immune cells and reduces inhibitory regulatory T cells in tumors (10–12), while some showed improved T-cell trafficking and infiltration from peritumoral stroma to the intraepithelial tumor compartment after L-XRT (13–17). Notably, it is known that the presence of T-lymphocyte infiltration into melanoma lesions is associated with better prognosis (18). The abovementioned findings are some plausible explanations to the observed reversal of immunotherapy resistance in our patient’s case.
Lattice radiotherapy (LRT) (19) and the Radscopal technique share similarities in their use of spatially modulated radiation to stimulate anti-tumor immune responses while minimizing toxicity to healthy tissues. Both approaches deliver high doses to specific tumor subvolumes, releasing tumor antigens and priming the immune system. However, they differ in application and goals. LRT uses alternating high-dose (peaks) and low-dose (valleys) patterns within bulky tumors, such as large breast cancers (19), to achieve local tumor downsizing and symptom palliation without exceeding organ-at-risk (OAR) tolerance. In contrast, the Radscopal technique combines localized high-dose radiation with systemic immunotherapy, targeting metastatic cancers to enhance systemic immune responses and abscopal effects. While LRT focuses on local control, the Radscopal technique emphasizes systemic tumor control through immune modulation, making them distinct yet complementary strategies in radiation oncology.
Low-dose radiation (L-XRT) plays a crucial role in overcoming the inhibitory tumor stroma, which is a significant barrier to effective immune responses against cancer. The tumor stroma, composed of various cellular and extracellular components, often creates an immunosuppressive environment that hinders the infiltration and function of effector immune cells. L-XRT has been shown to modulate this inhibitory stroma by several mechanisms. Firstly, it reduces the levels of transforming growth factor β (TGF-β), an inhibitory cytokine associated with the protumor M2 phenotype of tumor-associated macrophages (TAMs). By decreasing TGF-β, L-XRT helps to reprogram TAMs from the M2 phenotype to the antitumor M1 phenotype, which supports immune activation and tumor destruction. Additionally, L-XRT enhances the infiltration of effector T cells and natural killer (NK) cells into the tumor microenvironment (TME), thereby promoting a more robust antitumor immune response. This reprogramming of the TME not only facilitates better immune cell trafficking but also creates a cytokine and chemokine gradient that attracts these effector cells to the tumor site. Collectively, these effects of L-XRT help to dismantle the immunosuppressive barriers within the TME, making it more conducive to effective immune-mediated tumor eradication (10, 13).
Apart from the immunomodulatory effect of RT to irradiated tumor, the potential of radiation-induced abscopal effect has been increasingly recognized in recent years as well. The systemic anti-tumor effect is observed to be immune-mediated (20–22). There have also been multiple case reports and trials proving the synergistic phenomenon of RT and immunotherapy in achieving abscopal effect (23–28). The combination of L-XRT with anti-PD1 therapy has been explored in preclinical and clinical settings with encouraging results. This suggests that radiation can potentiate the effects of immune checkpoint inhibitors not only in terms of local control of the irradiated tumor but also leading to regression over distant non-irradiated sites.
Our patient’s complete tumor resolution following the combination of L-XRT and continued anti-PD1 therapy underscores the potential of this approach to overcome immunotherapy resistance. This aligns with the concept that radiation can induce immunogenic cell death, thereby enhancing the visibility of tumor antigens to the immune system and promoting a more robust and sustained antitumor response (29).
Furthermore, the generation of long-term immune memory, as observed in preclinical models with similar combinatorial approaches, suggests that this strategy does not only address the existing tumors but may also provide protection against future recurrences (30). This is particularly relevant for melanoma, a cancer known for its high mutational burden and potential for immune evasion. Nevertheless, the innovative approach of combining immunotherapy with radiation requires careful consideration. This area of research presents certain challenges, as this therapeutic strategy may lead to uncommon adverse effects—for example, cases of bone erosion (31) and neuritis symptoms (32) have been reported.
There are several limitations to our presented case. Firstly, we utilized the higher end dose (10 Gy in 5 Fr) of L-XRT to treat the mesenteric tumor. It remains uncertain whether a lower dose of L-XRT could achieve the same therapeutic effect while reducing the side effect of diarrhea. Secondly, we did not conduct serum tests for immune markers such as TGF-β. Thirdly, a biopsy of the recurrent mesenteric tumor was not performed due to its location, which would necessitate laparoscopy. The patient declined another laparoscopy following a recent bowel resection surgery. Obtaining a tumor sample would have been valuable for studying the tumor microenvironment. These limitations can be addressed in a future prospective study.
In conclusion, the successful treatment of our melanoma patient with peritoneal metastases using L-XRT in conjunction with anti-PD1 therapy highlights the potential of integrating radiotherapy with immunotherapy to overcome resistance and achieve durable responses. This case adds to the growing body of evidence supporting the synergistic effects of these modalities and underscores the need for further research to optimize combination strategies for cancer treatment.
From my own perspective, undergoing this innovative treatment has truly been a life-changing experience. At first, I was a bit concerned about the idea of receiving low-dose radiation, but the process turned out to be manageable. I experienced mild diarrhea during the treatment, but these were small inconveniences compared to the benefits I gained. Now, I am thrilled to be living a normal, active life—I can go about my daily routines and enjoy time with my family without constantly worrying about my cancer. It is incredible to me that such a simple and relatively low-cost treatment has made such a profound difference in reversing the resistance to my previous immunotherapy. I am genuinely amazed by the results and hopeful that this approach can help others facing similar health challenges. This journey has renewed my enthusiasm for exploring new treatment options and has given me a fresh perspective on the possibilities in cancer care.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
KF: Validation, Writing – original draft, Writing – review & editing. IH: Validation, Writing – original draft, Writing – review & editing, Resources. TS: Resources, Validation, Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Supervision, Visualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. New Engl J Med. (2019) 381:1535–46. doi: 10.1056/NEJMoa1910836
2. Wolchok JD, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J Clin Oncol. (2022) 40:127–37. doi: 10.1200/JCO.21.02229
3. Atkins MB, Lee SJ, Chmielowski B, Tarhini AA, Cohen GI, Truong TG, et al. Combination dabrafenib and trametinib versus combination nivolumab and ipilimumab for patients with advanced BRAF-mutant melanoma: the DREAMseq trial-ECOG-ACRIN EA6134. J Clin Oncol. (2023) 41:186–97. doi: 10.1200/JCO.22.01763
4. Ribas A, Hamid O, Daud A, Hodi FS, Wolchok JD, Kefford R, et al. Association of pembrolizumab with tumor response and survival among patients with advanced melanoma. JAMA. (2016) 315:1600–9. doi: 10.1001/jama.2016.4059
5. Wolchok JD, Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ, Cowey CL, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. New Engl J Med. (2017) 377:1345–56. doi: 10.1056/NEJMoa1709684
6. Hodi FS, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Cowey CL, et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. (2018) 19:1480–92. doi: 10.1016/S1470-2045(18)30700-9
7. Ferini G, Zagardo V, Critelli P, Santacaterina A, Sava S, Harikar MM, et al. Introducing radiotherapy in metastatic Merkel cell carcinoma patients with limited progression on avelumab: An effective step against primary and secondary immune resistance? J Personalized Med. (2023) 13:841. doi: 10.3390/jpm13050841
8. Zagardo V, Martorana E, Harikar M, Pergolizzi S, Ferini G. Effectiveness of radiotherapy in delaying treatment changes in primary or secondary immunorefractory oligoprogressive patients: Preliminary results from a single-center study. Discover Oncol. (2024) 15:531. doi: 10.1007/s12672-024-01360-y
9. Zagardo V, Harikar M, Ferini G. Is an immune-oriented use of radiation therapy possible? An increasingly open question under the spotlight of immunotherapy. Oncologie. (2024) 26:487–91. doi: 10.1515/oncologie-2024-0040
10. Barsoumian HB, Ramapriyan R, Younes AI, Caetano MS, Menon H, Comeaux NI, et al. Low-dose radiation treatment enhances systemic antitumor immune responses by overcoming the inhibitory stroma. J Immunother Cancer. (2020) 8:e000537. doi: 10.1136/jitc-2020-000537
11. Demaria S, Golden EB, Formenti SC. Role of local radiation therapy in cancer immunotherapy. JAMA Oncol. (2015) 1:1325–32. doi: 10.1001/jamaoncol.2015.2756
12. Liu R, Xiong S, Zhang L, Chu Y. Enhancement of antitumor immunity by low-dose total body irradiation is associated with selectively decreasing the proportion and number of T regulatory cells. Cell Mol Immunol. (2010) 7:157–62. doi: 10.1038/cmi.2009.117
13. He K, Barsoumian HB, Bertolet G, Verma V, Leuschner C, Koay EJ, et al. Novel use of low-dose radiotherapy to modulate the tumor microenvironment of liver metastases. Front Immunol. (2021) 12:812210. doi: 10.3389/fimmu.2021.812210
14. Patel RR, Barsoumian HB, Verma V, Cortez MA, Welsh JW. Low-dose radiation decreases cancer-associated fibroblasts and may increase T-cell trafficking into tumors. Int J Radiat Oncol Biol Phys. (2020) 108:e530–1. doi: 10.1016/j.ijrobp.2020.07.1660
15. Herrera FG, Ronet C, Ochoa de Olza M, Barras D, Crespo I, Andreatta M, et al. Low-dose radiotherapy reverses tumor immune desertification and resistance to immunotherapy. Cancer Discovery. (2022) 12:108–33. doi: 10.1158/2159-8290.CD-21-0003
16. Dovedi SJ, Cheadle EJ, Popple AL, Poon E, Morrow M, Stewart R, et al. Fractionated radiation therapy stimulates antitumor immunity mediated by both resident and infiltrating polyclonal T-cell populations when combined with PD-1 blockade. Clin Cancer Res. (2017) 23:5514–26. doi: 10.1158/1078-0432.CCR-16-1673
17. Lugade AA, Moran JP, Gerber SA, Rose RC, Frelinger JG, Lord EM. Local radiation therapy of B16 melanoma tumors increases the generation of tumor antigen-specific effector cells that traffic to the tumor. J Immunol. (2005) 174:7516–23. doi: 10.4049/jimmunol.174.12.7516
18. Clemente CG, Mihm MC Jr, Bufalino R, Zurrida S, Collini P, Cascinelli N. Prognostic value of tumor infiltrating lymphocytes in the vertical growth phase of primary cutaneous melanoma. Cancer. (1996) 77:1303–10. doi: 10.1002/(SICI)1097-0142(19960401)77:7<1303::AID-CNCR12>3.0.CO;2-5
19. Ferini G, Zagardo V, Viola A, Patanè D, Parisi S, Cuccia F, et al. The promising effects of lattice radiotherapy for large, fungating, or ulcerating breast cancers: A prospective single-center study. In Vivo. (2024) 38:2484–93. doi: 10.21873/invivo.13719
20. Rodríguez-Ruiz ME, Vanpouille-Box C, Melero I, Formenti SC, Demaria S. Immunological mechanisms responsible for radiation-induced abscopal effect. Trends Immunol. (2018) 39:644–55. doi: 10.1016/j.it.2018.06.001
21. Poleszczuk JT, Luddy KA, Prokopiou S, Robertson-Tessi M, Moros EG, Fishman M, et al. Abscopal benefits of localized radiotherapy depend on activated T-cell trafficking and distribution between metastatic lesions. Cancer Res. (2016) 76:1009–18. doi: 10.1158/0008-5472.CAN-15-1423
22. Stamell EF, Wolchok JD, Gnjatic S, Lee NY, Brownell I. The abscopal effect associated with a systemic anti-melanoma immune response. Int J Radiat Oncol Biol Phys. (2013) 85:293–5. doi: 10.1016/j.ijrobp.2012.03.017
23. Postow MA, Callahan MK, Barker CA, Yamada Y, Yuan J, Kitano S, et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N Engl J Med. (2012) 366:925–31. doi: 10.1056/NEJMoa1112824
24. Grimaldi AM, Simeone E, Giannarelli D, Muto P, Falivene S, Borzillo V, et al. Abscopal effects of radiotherapy on advanced melanoma patients who progressed after ipilimumab immunotherapy. Oncoimmunology. (2014) 3:e28780. doi: 10.4161/onci.28780
25. Reynders K, Illidge T, Siva S, Chang JY, De Ruysscher D. The abscopal effect of local radiotherapy: using immunotherapy to make a rare event clinically relevant. Cancer Treat Rev. (2015) 41:503–10. doi: 10.1016/j.ctrv.2015.03.011
26. Aboudaram A, Modesto A, Chaltiel L, Gomez-Roca C, Boulinguez S, Sibaud V, et al. Concurrent radiotherapy for patients with metastatic melanoma and receiving anti-programmed-death 1 therapy: a safe and effective combination. Melanoma Res. (2017) 27:485–91. doi: 10.1097/CMR.0000000000000386
27. Roger A, Finet A, Boru B, Beauchet A, Mazeron JJ, Otzmeguine Y, et al. Efficacy of combined hypo-fractionated radiotherapy and anti-PD-1 monotherapy in difficult-to-treat advanced melanoma patients. Oncoimmunology. (2017) 7:e1442166. doi: 10.1080/2162402X.2018.1442166
28. Welsh JW, Tang C, de Groot P, Naing A, Hess KR, Heymach JV, et al. Phase II trial of ipilimumab with stereotactic radiation therapy for metastatic disease: outcomes, toxicities, and low-dose radiation-related abscopal responses. Cancer Immunol Res. (2019) 7:1903–9. doi: 10.1158/2326-6066.CIR-18-0793
29. Vanpouille-Box C, Alard A, Aryankalayil MJ, Sarfraz Y, Diamond JM, Schneider RJ, et al. DNA exonuclease Trex1 regulates radiotherapy-induced tumour immunogenicity. Nat Commun. (2017) 8:15618. doi: 10.1038/ncomms15618
30. Caetano MS, Younes AI, Barsoumian HB, Quigley M, Menon H, Gao C, et al. Triple therapy with merTK and PD1 inhibition plus radiotherapy promotes abscopal antitumor immune responses. Clin Cancer Res. (2019) 25:7576–84. doi: 10.1158/1078-0432.CCR-19-0795
31. Parisi S, Napoli I, Lillo S, Cacciola A, Ferini G, Iatì G, et al. Spine eburnation in a metastatic lung cancer patient treated with immunotherapy and radiotherapy. the first case report of bystander effect on Bone. J Oncol Pharm Pract. (2021) 28:237–41. doi: 10.1177/10781552211027348
32. Ferini G, Zagardo V, Boncoraglio A, Aiello MM, Pontoriero A. Leptomeningeal tumor spread or immune checkpoint inhibitor-related c/(poli-)neuritis? an unsolved dilemma in a patient on pembrolizumab for a history of brain metastases from lung adenocarcinoma. Acta Neurologica Belgica. (2024) 113:3. doi: 10.1007/s13760-023-02462-0
Keywords: melanoma, low dose radiation (LDR), immunotherapy, pembrolizumab, radiation
Citation: Fong KHA, Ho I and So TH (2025) Case report: Low-dose radiation reverses pembrolizumab resistance in melanoma. Front. Oncol. 15:1483117. doi: 10.3389/fonc.2025.1483117
Received: 19 August 2024; Accepted: 13 January 2025;
Published: 12 February 2025.
Edited by:
Domenico Mallardo, G. Pascale National Cancer Institute Foundation (IRCCS), ItalyReviewed by:
John E. Mignano, Tufts University, United StatesCopyright © 2025 Fong, Ho and So. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tsz Him So, c3RoNDk1QGhrdS5oaw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.