
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 28 February 2025
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1482705
This article is part of the Research TopicImaging to Guide Treatment in Brain TumorsView all articles
 Artem Rafaelian1*
Artem Rafaelian1* Sae-Yeon Won1
Sae-Yeon Won1 Bedjan Behmanesh1
Bedjan Behmanesh1 Daniel Cantré2
Daniel Cantré2 Joshua D. Bernstock3
Joshua D. Bernstock3 Thomas M. Freiman1
Thomas M. Freiman1 Jakob Seidlitz4,5,6Peter Baumgarten7
Jakob Seidlitz4,5,6Peter Baumgarten7 Nazife Dinc8
Nazife Dinc8 Juergen Konczalla9
Juergen Konczalla9 Florian Gessler1
Florian Gessler1 Daniel Dubinski1
Daniel Dubinski1Purpose: Recently, the temporalis muscle thickness on cranial CT scan was proposed as a surrogate marker for patients’ baseline frailty that correlates with outcome in primary and metastatic brain tumor patients. In this study, we investigated whether the velocity of temporalis muscle atrophy (TMA) affects the outcome of patients with cerebral metastases.
Methods: We analyzed radiological and clinical data sets of 96 patients who received craniotomy for cerebral metastasis resection in our institution. We then correlated the radiological data with clinical course and outcome after stratification for the velocity of temporalis muscle atrophy.
Results: The median velocity of TMA was 0.0016 mm/day. In patients with a slow TMA rate, the median overall survival was significantly longer than in patients with a fast TMA rate (37.7 months versus 22.9, p = 0.0007). Furthermore, patients with slow TMA had longer progression-free survival postoperatively (7.6 versus 4.38 months, p <0.0001). The overall survival postoperatively (OS-PO) was also significantly longer in patients with slow TMA (8.9 months versus 5.1, p=0002).
Conclusion: Based on this study, the velocity of temporalis muscle atrophy may represent an objective and dynamic index with potential for survival prognostication for patients with cerebral metastases.
With advances in screening, imaging, and therapy, survival and the quality of life has improved annually in cancer patients. However, cerebral metastasis remains a major source of persistent neurological deficits, disability, and mortality, and 20% to 40% of all solid tumors metastasize to the brain at some point in time, changing the approach to cancer treatment and significantly limiting the ability to participate in clinical trials (1–3). The decision on further adjuvant treatment and its intensity largely depends on the prognosis of the underlying disease (4).
Currently, several approaches have been developed for prognostication of cancer progression both on the basis of mathematical analysis and on the basis of artificial intelligence (5, 6). Widely adopted scales in the assessment of patients’ frailty and therefore suitability of neo- and adjuvant therapy are the Karnofsky Performance Status (KPS) and the Eastern Cooperative Oncology Group (ECOG) Performance status. One of the disadvantages however is the subjective nature of these scales and the potential for biased reporting. On the other hand, scientific interest in the objective assessment of patient’s physiological reserve is growing and patient’s frailty estimation via the surrogate temporalis muscle thickness (TMT) measurement has gained increasing interest due to the ability to measure via non-invasive head imaging (7).
The pathobiology underlying sarcopenia and frailty in individuals with brain metastases is complex, with underlying factors such as chemo-radiation and immune therapy-induced hypodynamia, malnutrition and/or dietary factors, and tumor-induced inflammation fostering a pro-catabolic state characterized by heightened protein degradation relative to synthesis—all culminating in skeletal muscle tissue loss and autophagy. Klicken oder tippen Sie hier, um Text einzugeben (8, 9).Klicken oder tippen Sie hier, um Text einzugeben. On the other hand, the TMT measurement on MRI or CT scan is easy to obtain and recent studies showed a positive correlation between the thickness of temporalis muscle and patients’ outcome in neuro-trauma and oncological diseases. Klicken oder tippen Sie hier, um Text einzugeben (10–16).
In this study, we consistently moved away from the static TMT measurement at the beginning of the disease and investigated the influence of frailty dynamics on the clinical course and outcome. Therefore, the aim of this study was primarily to investigate the dynamics of frailty, measured by TMT, and its potential for predicting clinical outcomes in cancer patients with brain metastases. We chose temporalis muscle data because this muscle is almost always clearly depicted on MRI scans, which are used both preoperatively and for regular follow-up examinations. In particular, we aim to evaluate whether changes in TMT over time can serve as a more reliable marker of frailty compared with static preoperative measurements alone, as described by other authors. This dynamic approach is expected to more accurately predict clinical outcomes and response to treatment, given the variable nature of frailty in cancer patients. The dynamics of frailty, especially as reflected in the rate of change in TMT, may provide insights into how cancer progression, treatment interventions, and patient responses lead to changes in the patient’s physiological reserve.
All patients admitted to the neurosurgical department at the University Hospital Rostock between 2018 and 2022 who underwent surgical resection for parenchymal brain metastases were included. Indication for craniotomy were neurological deficit, metastasis size unsuitable for radiotherapy, and/or tumor size >3 cm in diameter. The indication for surgical treatment was confirmed in advance at an interdisciplinary tumor conference for all cases. Exclusion methods were missing MR imaging before and/or after surgical intervention in the radiology facility of our university. A total of 96 patients were included in the study. Patient characteristics and medical data were collected via the institution’s electronic database. For this retrospective analysis, ethical approval was obtained from the Ethics Committee of the University Medicine Rostock, Germany (Identification number: A 2021-0112); as a non-interventional, retrospective study, patient consent was waived. The collected data included age at surgical examination, gender, BMI, the amount of dexamethasone received 2 weeks before and after surgery, the date of the first oncological diagnosis, histological and mutational tumor characteristics, the presence of metastasis in other organs, assessment of cerebral metastasis (size, quantity, cerebral edema) concomitant diseases, median TMT before surgery and in the last follow-up, perioperative complications, KPS prior to surgery, the presence of adjuvant and neoadjuvant treatment, the Graded Prognostic Assessment index, and the date of the last inspection, contact, or death. Due to the heterogeneity of the underlying oncological disease and the subject-specific definition of progression-free survival, we did not include the progression-free survival in our analysis and restricted this study to patients’ overall survival, progression-free survival, and overall survival postoperatively (OS, PFS-PO, and OS-PO, respectively).
TMT measurements were performed on contrast-enhanced T1-weighted MR images (T1-mprage with 1-mm isotropic voxel size), in standardized axial reconstructions, by a reader blinded to the outcome. For each patient, we performed these measurements in the preoperative staging MRI examination (TMT1), as well as follow-up MRI examinations until the last examination, last before lost to follow-up, or patients’ decease (TMT2). TMT was measured perpendicular to the long axis of the temporalis muscle at the level of the Sylvian fissure (anteroposterior landmark) and the roof of the orbit (craniocaudal landmark). If the axial plane was tilted from the desired plane during image registration, the image was aligned to the required plane using the 3D-MPR mode. The measurements were performed separately for both sides, and then the arithmetic mean was calculated, resulting in a mean TMT value for each patient and timepoint. If the craniotomy involved the temporal muscle (e.g., temporal approach or pterional approach), then the thickness of the temporal muscle was calculated both pre- and postoperatively on the “healthy” side only. The time interval between examination timepoints was also determined in numbers of days (n). Thus, the rate of temporalis muscle atrophy (TMA) was obtained according to the formula V = (mean TMT1 − mean TMT2)[mm]/n [day]. Preoperative and postoperative images and subsequent MRI scans were analyzed using PACS software JiveX® v5.2 (VISUS Technology Transfer GmbH, Bochum, Germany). Image analysis was performed independently by two neurosurgeons who was blinded to patients’ medical data, and the mean of both measurements was calculated. A representative analysis is displayed in Figure 1.
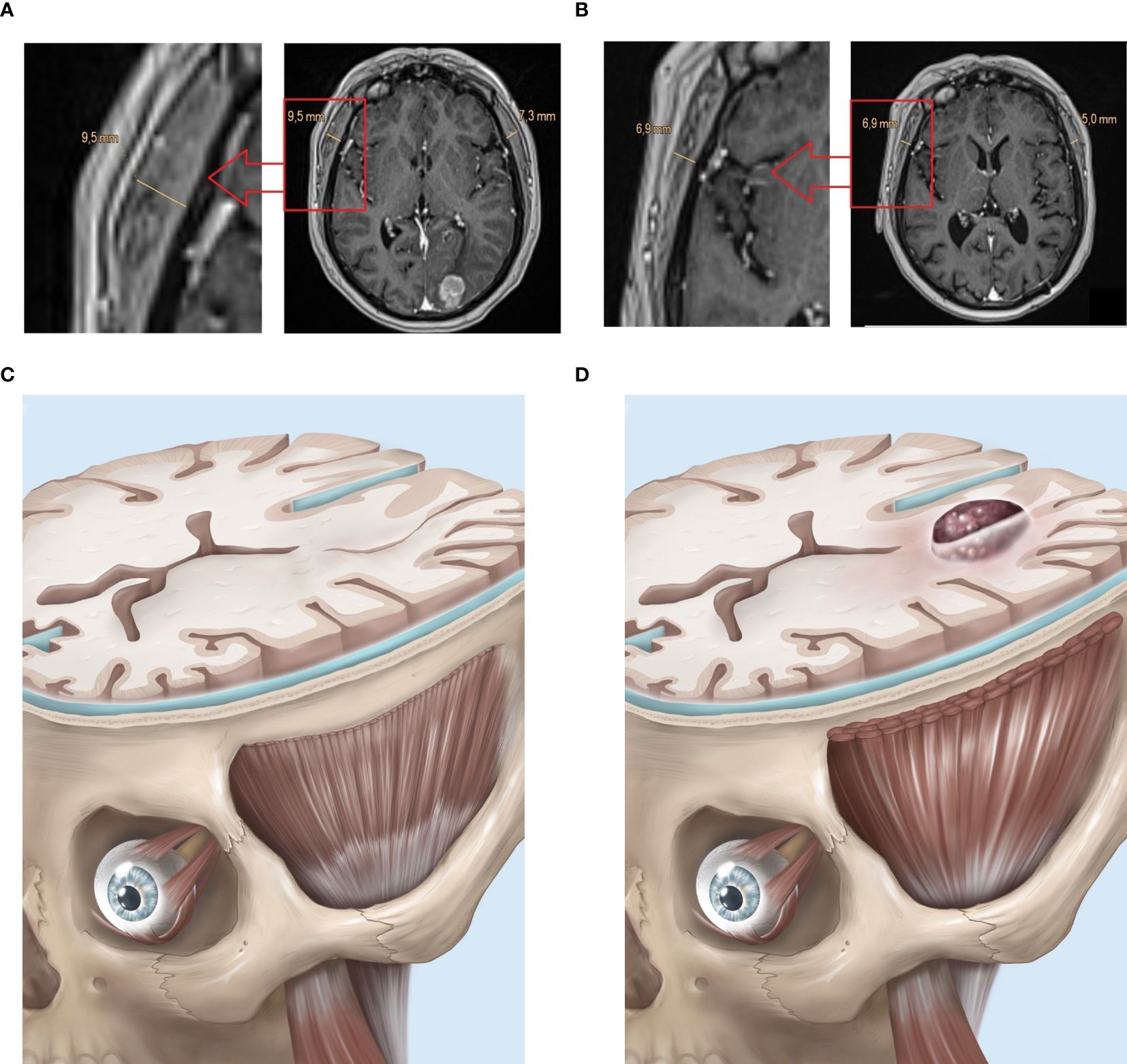
Figure 1. Exemplary case depicting temporalis muscle atrophy (TMA) in a case of NSCLC (EGFR, ALK: neg.) with singular cerebral metastasis, treated with metastasis resection and combined immune- and radiation therapy. TMT-Measurements assessed in axial reconstructions of contrast enhanced T1-weighted MRI sequences (A) in the preoperative staging MRI (resulting mean TMT1 = (9.5 mm + 7.3 mm)/2 = 8.4 mm) and (B) in the final follow-up MRI (TMT2 = 5.95 mm) after combined treatment with good response. The time interval between these MRIs was 421 days. The rate of TMA was V = (8.4–5.95)/421 = 0.00581 mm/day. (C) Illustrative model with occipital lobe metastasis at the beginning of the treatment with healthy TMT. D: Same model with TMA after treatment.
We calculated overall survival (OS) using days from the first diagnosis to the death date and OS postoperative (OS-PO) using days from the operation to the death date. Kaplan–Meier survival curve analysis and the log-rank test were conducted to obtain the median OS of the groups. Univariate and multivariate analyses were performed using a Cox proportional regression model. To assess the impact of the variables, odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Results with a p-value of ≤0.05 were considered to be statistically relevant. All statistical analyses were conducted using the GraphPad Prism 10 (GraphPad Software, California, USA). For patient characteristics, descriptive statistics were used.
The study group consisted of 121 patients; in 25 patients (20.6%), medical datasets and/or follow-up data were incomplete, and therefore 96 patients remained in the study. The average age was 64 years old (IQR: 56.8–71.3), and 55 (57.3%) of the patients were men. In 34 (35.4%) cases, symptomatic cerebral metastases lead to the first oncological diagnosis. The median TMT at admission was 5.95 mm (IQR: 5.1–7.0). The median total dexamethasone doses that patients were administered (total count for 14 days) pre-OP and post-OP were 36 mg (IQR: 0–72) and 60 mg (IQR: 19.5–93.75), respectively. It is noteworthy that eight (8.3%) patients had an increase in muscle mass. Patient characteristics are shown in Table 1.
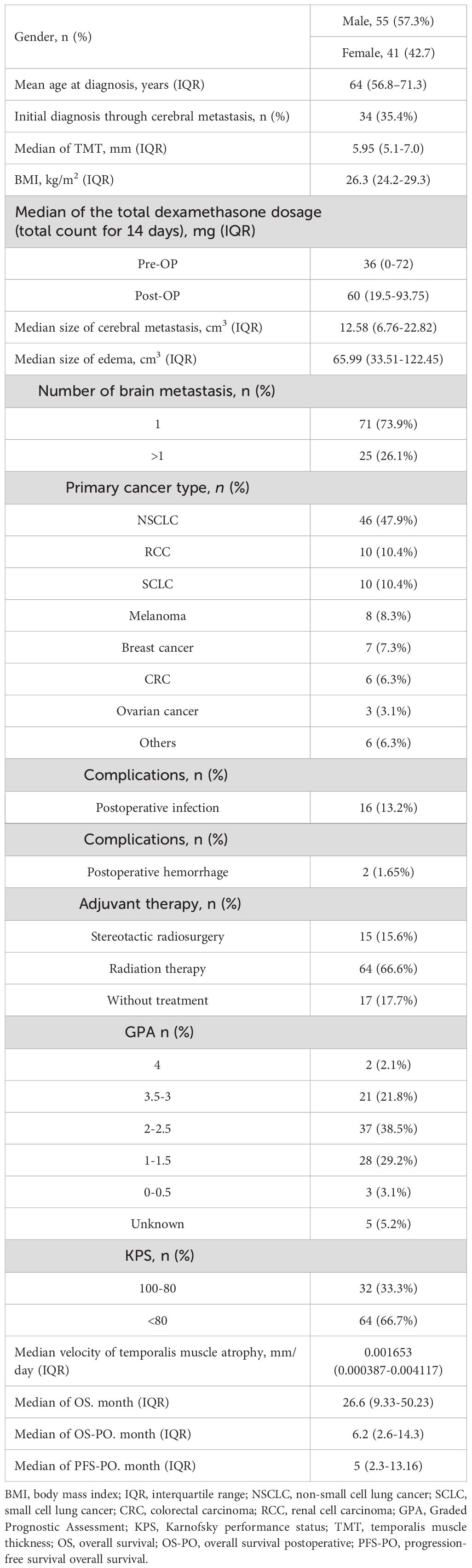
Table 1. Demographics.
We used the median rate of TMA (0.001653 mm/day) to stratify the cohort. The cohort (n=96) was divided into groups with high and low rates of TMT atrophy based on this median value. A comparative analysis of the data of the two groups was carried out. We would like to point out that both groups in our study were quite homogeneous in terms of patient gender, whether the diagnosis of brain metastasis was the first oncologic diagnosis, and interestingly, both groups showed an almost equal number of patients who refused further adjuvant treatment.
The univariate analysis showed no significant association between patients’ sex (p = 0.84), BMI (p = 0.4872), or median TMT at admission (p = 0.77) and the velocity of temporalis muscle atrophy. Furthermore, there was no significant difference between the KPS (p =0.0668) or GPA (p = 0.17-0.99) and the velocity of temporalis muscle atrophy. Such an indicator as the age of patients showed a difference in the two groups, but in our sample of patients, it was statistically insignificant (63 versus 59.5; p = 0.15). The detailed results are presented in Table 2.
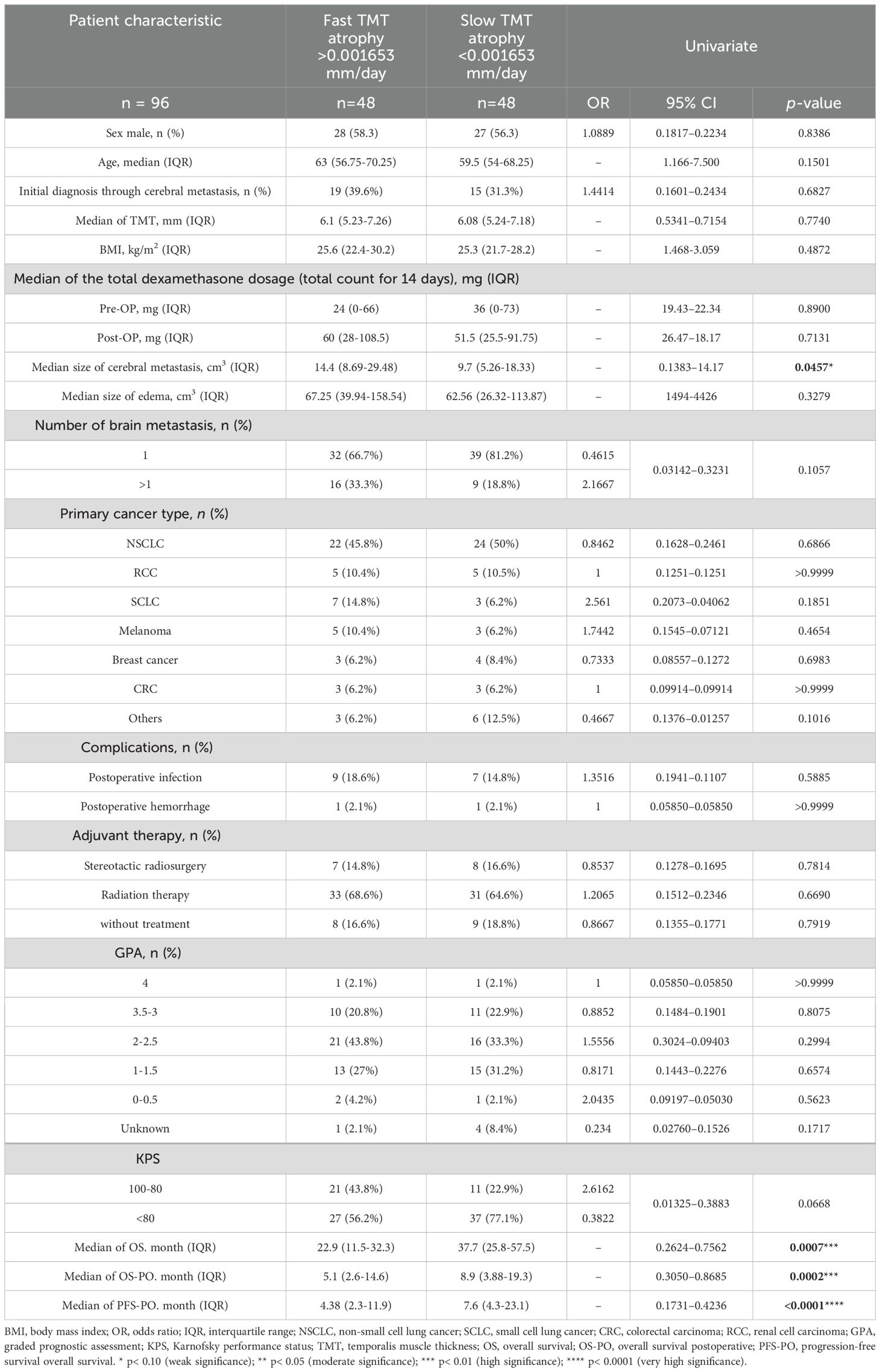
Table 2. Univariate analysis of juxtaposed characteristics according to the rate of TMT muscle atrophy.
The Kaplan–Meier overall survival, progression-free survival, and overall survival postoperatively each subgroup are presented in Figures 2, 3.
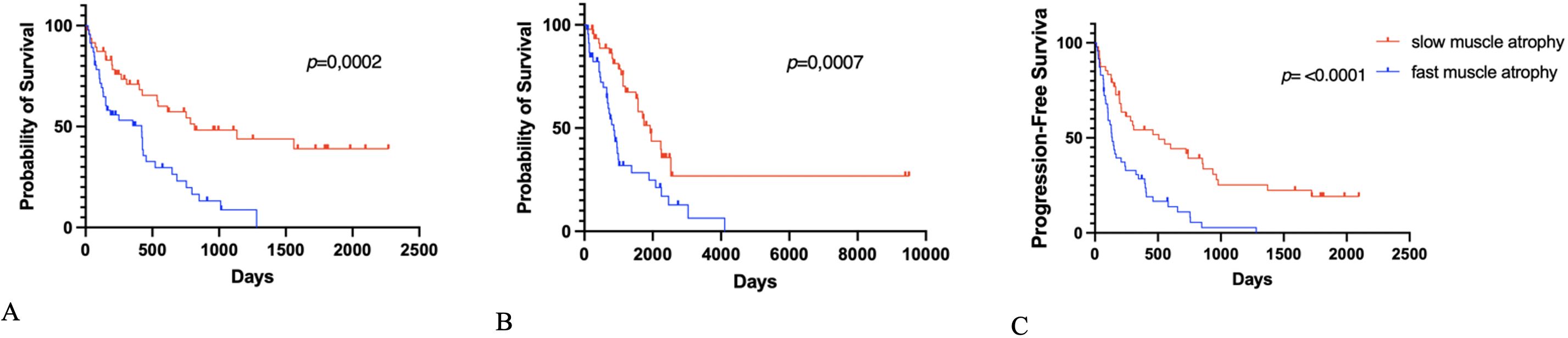
Figure 2. Kaplan–Meier survival graphs of (A) overall survival, (B) overall survival postoperatively (OS-PO), and (C) progression-free survival postoperatively (PFS-PO) stratified according to fast und slow TMT atrophy.
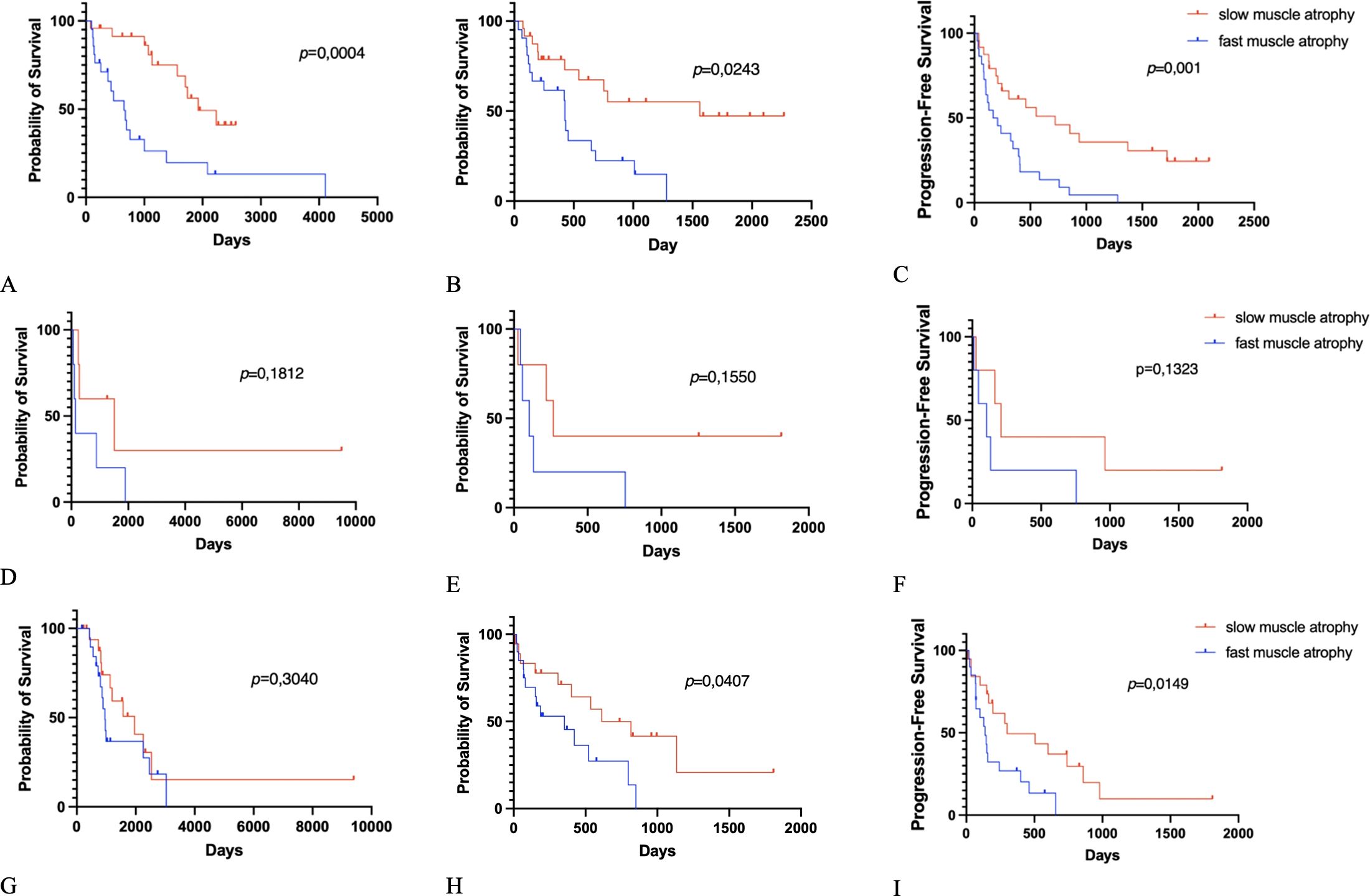
Figure 3. Kaplan–Meier survival graphs: (A) Overall survival (OS), (B) OS-postoperative (OS-PO), (C) progression-free survival postoperative (PFS-PO) for fast and slow muscle degeneration and non-small cell lung cancer. (D) OS, (E) OS-PO, (F) PFS-PO for fast and slow muscle degeneration and renal cell carcinoma. (G) OS, (H) OS-PO, (I) PFS-PO for fast and slow muscle degeneration and all other tumors.
A significant association between the velocity of TMA and the median size of cerebral metastasis was observed (median size of cerebral metastasis of 14.4 cm3 (IQR: 8.69–29.48) in the fast TMT atrophy cohort vs. 9.7 cm3 (IQR: 5.26–18.33) in the Slow TMT atrophy cohort; p = 0.0457).
In the group with a slow TMT atrophy rate, median OS was significantly longer than in the group with a fast TMT atrophy rate (37.7 (IQR: 25.8-57.5) versus 22.9 (IQR: 11.5-32.3) months, p = 0.0007). The group with a slow TMT atrophy rate had longer progression-free survival postoperative (PFS-PO) (7.6 (IQR: 4.3-23.1) versus 4.38 (IQR: 2.3-11.9) months, p <0.0001). In the group with a slow TMT atrophy rate, median OS-PO was significant longer than in the group with fast TMT atrophy (8.9 (IQR: 3.88-19.3) versus 5.1 (2.6-14.6) months, p = 0.0002).
In this study, we hypothesized that time-dependent TMA could be used as a dynamic index to objectify patients’ frailty throw-out adjuvant treatment. We used the median rate of TMA (0.001653 mm/day) for cohort stratification. The survival analysis showed a statistically highly significant difference in all three key oncologic indicators OS, OS-PO, and PFS-PO (p=0.0007; p=0.0002; p<0.0001). Unfortunately, we have no data on the change in BMI in patients during treatment, as the study is retrospective and not all patients had this index recorded at control MRI. We recognize that this index would be interesting for comparison. However, it did not show a statistically significant difference in the fast and slow temporal muscle atrophy groups at the onset of the disease.
Surprisingly, our analysis revealed no statistically significant difference in patient age (p=0.150) and sex distribution (p=0.838), variables recognized in various studies as prognostic factors. This underscores the importance of incorporating dynamic indicators (such as fitness level, weight loss, or quality of nutrition) that may evolve during the course of treatment (17). The question of finding direct correlations between a patient’s “biological age” and the presence of objective biomarkers is becoming increasingly common (18).
Sarcopenia, meanwhile, finds itself trapped in a cycle where aggressive adjuvant and neoadjuvant therapies contribute to its development, and its progression, in turn, leads to poorer treatment outcomes. As highlighted in Bozzetti’s article, various mechanisms of sarcopenia pathogenesis are discussed (19). There are various studies linking sarcopenia to muscle protein catabolism, which intensifies as tumor growth progresses (20, 21). Some side effects of chemotherapy, such as fatigue, loss of appetite, nausea, vomiting, and diarrhea, can negatively affect food intake and physical activity (22). Chemotherapy may suppress anabolic processes through the IGF-1/PI3K/Akt/mTOR pathway, which also contributes to muscle loss (23). Chemotherapy and radiation can also reduce microvessels in muscle through anti-angiogenesis and cause localized muscle tissue damage, inflammation, and fibrosis, reducing its functionality (24).
While numerous publications have previously elucidated the deleterious impact of sarcopenia on cancer prognosis, our objective is to underscore the rate of sarcopenia index development within this context. Panje et al.’s (25) research indicates that sarcopenia’s onset during treatment may not only prognosticate outcomes but also elevate the risk of severe complications during adjuvant radiochemotherapy. Furthermore, the noteworthy study by Jang et al. suggests that diverse neoadjuvant therapies for breast cancer patients may variably influence sarcopenia progression, reinforcing the pertinence of this field and the necessity for further prospective investigations. Consequently, interventions aimed at preserving muscle mass, such as exercise regimens and resistance training, alongside nutritional support throughout various disease stages—including adjuvant, surgical, and neoadjuvant treatments—may prove pivotal in enhancing disease prognosis (26, 27).
Given the heterogeneous treatment response and survival outcomes among patients with cerebral metastases, numerous studies have sought to forecast prognosis through classification scoring systems (4). Among these is the Graded Prognostic Assessment (GPA), introduced by Sperduto et al., which stands out as a widely utilized metric in the field. Specifically designed for disease-specific evaluation, the GPA scale furnishes a prognostic index adapted to the diverse manifestations of brain metastasis across various primary cancers (28). However, a significant limitation of this method lies in its predominantly subjective nature, thus prompting consideration for the inclusion of more objective parameters of frailty, such as TMT atrophy (29).
Our colleagues have previously demonstrated a significant correlation between overall life expectancy in malignant brain tumors and TMT. Subsequently, Furtner et al. conducted a comprehensive retrospective study involving 755 glioblastoma patients, stratifying them into two groups based on TMT measurements. Sarcopenia risk was defined as TMT values ≤6.3 mm for men and ≤5.2 mm for women. Results revealed that patients exhibiting sarcopenia at baseline displayed a markedly elevated risk for disease progression and mortality compared with those with normal muscle status (30).
While our analysis underscores the importance of TMT atrophy velocity throughout the course of oncological disease and treatment in a substantial cohort of brain metastasis patients, our study is subject to certain constraints. The retrospective design of our TMT analysis precluded the evaluation of anatomical-functional correlations. Furthermore, given the observational nature of our study, potential confounding variables (such as comorbidities, refusal of treatment and therapy, accidents) and uncontrolled statistical errors cannot be excluded. Thus, future prospective randomized investigations involving larger cohorts are warranted to confirm our findings. Unfortunately due to the limited number of patients, multivariate analysis did not show significant differences in this regard; we will continue our study with a further prospective phase.
Based on our analysis, we propose monitoring the TMA dynamics longitudinally to facilitate the identification of suitable candidates for intensive therapeutic interventions or enrollment in clinical trials.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University Medicine Rostock (Identification number: A 2021-0112). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because it is a non-interventional, retrospective study.
AR: Conceptualization, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. S-YW: Writing – review & editing. BB: Writing – review & editing. DC: Formal analysis, Methodology, Writing – review & editing. JB: Writing – review & editing. TF: Writing – review & editing. JS: Writing – review & editing. PB: Writing – review & editing. ND: Writing – review & editing. JK: Writing – review & editing. FG: Conceptualization, Writing – review & editing. DD: Conceptualization, Formal analysis, Methodology, Resources, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors would like to thank Irina Pollenskaia for preparing the illustration in Figures 1C, D.
FG received honoraria from AstraZeneca. DD received honoraria from Novartis, Fresenius, Novocure, and Medtronic. JB and JS are co-founders and hold equity in Centile Bioscience. None of these entities were involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lamba N, Wen PY, Aizer AA. Epidemiology of brain metastases and leptomeningeal disease. Neuro Oncol. (2021) 23:1447–56. doi: 10.1093/neuonc/noab101
2. Lamba N, Mehanna E, Kearney RB, Catalano PJ, Haas-Kogan DA, Alexander BM, et al. Racial disparities in supportive medication use among older patients with brain metastases: a population-based analysis. Neuro Oncol. (2020) 22:1339–47. doi: 10.1093/neuonc/noaa054
3. Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. (2012) 14:48–54. doi: 10.1007/s11912-011-0203-y
4. Gaspar L, Scott C, Rotman M, Asbell S, Phillips T, Wasserman T, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Clinical Investigation Int J Radiation Oncology Biol Phys (1997) 37:745–51.
5. Sperduto PW, Mesko S, Li J, Cagney D, Aizer A, Lin NU, et al. Survival in patients with brain metastases: summary report on the updated diagnosis-specific graded prognostic assessment and definition of the eligibility quotient. J Clin Oncol. (2020) 38:3773–84. doi: 10.1200/JCO.20.01255
6. Bice N, Kirby N, Bahr T, Rasmussen K, Saenz D, Wagner T, et al. Deep learning-based survival analysis for brain metastasis patients with the national cancer database. J Appl Clin Med Phys. (2020) 21:187–92. doi: 10.1002/acm2.12995
7. Dodds RA, Aihie Sayer AB. Sarcopenia and frailty: new challenges for clinical practice. Clinical Medicine (2016) 16:455–63. doi: 10.7861/clinmedicine.16-5-455
8. Jiao J, Demontis F. Skeletal muscle autophagy and its role in sarcopenia and organismal aging. Curr Opin Pharmacol. (2017) 34:1–6. doi: 10.1016/j.coph.2017.03.009
9. Granic A, Suetterlin K, Shavlakadze T, Grounds MD, Sayer AA. Hallmarks of ageing in human skeletal muscle and implications for understanding the pathophysiology of sarcopenia in women and men. Clin Sci. (2023) 137:1721–51. doi: 10.1042/CS20230319
10. Beaudart C, McCloskey E, Bruyère O, Cesari M, Rolland Y, Rizzoli R, et al. Sarcopenia in daily practice: assessment and management. BMC Geriatr. (2016) 16:1–10. doi: 10.1186/s12877-016-0349-4
11. Dubinski D, Won SY, Mattes I, Trnovec S, Behmanesh B, Cantré D, et al. Frailty in cerebellar ischemic stroke—The significance of temporal muscle thickness. Front Neurol. (2023) 14:1193685. doi: 10.3389/fneur.2023.1193685
12. Dubinski D, Won SY, Meyer-Wilmes J, Trnovec S, Rafaelian A, Behmanesh B, et al. Frailty in traumatic brain injury—The significance of temporal muscle thickness. J Clin Med. (2023) 12(24):7625. doi: 10.3390/jcm12247625
13. Ilic I, Faron A, Heimann M, Potthoff AL, Schäfer N, Bode C, et al. Combined assessment of preoperative frailty and sarcopenia allows the prediction of overall survival in patients with lung cancer (Nsclc) and surgically treated brain metastasis. Cancers (Basel). (2021) 13(13):3353. doi: 10.3390/cancers13133353
14. ten Cate C, Huijs SMH, Willemsen ACH, Pasmans RCOS, Eekers DBP, Zegers CML, et al. Correlation of reduced temporal muscle thickness and systemic muscle loss in newly diagnosed glioblastoma patients. J Neurooncol. (2022) 160:611–8. doi: 10.1007/s11060-022-04180-8
15. Tang J, Dong Z, Sheng J, Yang P, Zhao W, Xue J, et al. Advances in the relationship between temporal muscle thickness and prognosis of patients with glioblastoma: a narrative review. Front Oncol. (2023) 13:1251662. doi: 10.3389/fonc.2023.1251662
16. Kim Y, Shin JY, Yang SH, Kim HH, Shim BY, Ahn S. Association between temporal muscle thickness and overall survival in non-small cell lung cancer patients with brain metastasis. Curr Oncol. (2022) 29:6463–71. doi: 10.3390/curroncol29090508
17. Sperduto PW, Chao ST, Sneed PK, Luo X, Suh J, Roberge D, et al. Diagnosis-specific prognostic factors, indexes, and treatment outcomes for patients with newly diagnosed brain metastases: A multi-institutional analysis of 4,259 patients. Int J Radiat Oncol Biol Phys. (2010) 77:655–61. doi: 10.1016/j.ijrobp.2009.08.025
18. Diebel LWM, Rockwood K. Determination of biological age: geriatric assessment vs biological biomarkers. Curr Oncol Rep. (2021) 23(9):104. doi: 10.1007/s11912-021-01097-9
19. Bozzetti F. Chemotherapy-induced sarcopenia. Curr Treat Opt Oncol. (2020) 21(1):7. doi: 10.1007/s11864-019-0691-9
20. Lieffers JR, Mourtzakis M, Hall KD, McCargar LJ, Prado CMM, Baracos VE. A viscerally driven cachexia syndrome in patients with advanced colorectal cancer: Contributions of organ and tumor mass to whole-body energy demands. Am J Clin Nutr. (2009) 89:1173–9. doi: 10.3945/ajcn.2008.27273
21. Martin L, Birdsell L, MacDonald N, Reiman T, Clandinin MT, McCargar LJ, et al. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol. (2013) 31:1539–47. doi: 10.1200/JCO.2012.45.2722
22. Kakinuma K, Tsuruoka H, Morikawa K, Furuya N, Inoue T, Miyazawa T, et al. Differences in skeletal muscle loss caused by cytotoxic chemotherapy and molecular targeted therapy in patients with advanced non-small cell lung cancer. Thorac Cancer. (2018) 9:99–104. doi: 10.1111/1759-7714.12545
23. Moreira-Pais A, Ferreira R, Gil da Costa R. Platinum-induced muscle wasting in cancer chemotherapy: Mechanisms and potential targets for therapeutic intervention. Life Sci. (2018) 208:1–9. doi: 10.1016/j.lfs.2018.07.010
24. Barreto R, Waning DL, Gao H, Liu Y, Zimmers TA, Bonetto A. Chemotherapy-related cachexia is associated with mitochondrial depletion and the activation of ERK1/2 and P38 MAPKs. Oncotarget. (2016) 7(28):43442–60. doi: 10.18632/oncotarget.9779
25. Panje CM, Höng L, Hayoz S, Baracos VE, Herrmann E, Garcia Schüler H, et al. Skeletal muscle mass correlates with increased toxicity during neoadjuvant radiochemotherapy in locally advanced esophageal cancer: A SAKK 75/08 substudy. Radiat Oncol. (2019) 14(1):166. doi: 10.1186/s13014-019-1372-3
26. Dent E, Morley J, Cruz-jentoft A, Woodhouse L, Rodríguez-mañas L, Fried L, et al. Physical frailty: ICFSR international clinical practice guidelines for identification and management. J Nutr Health Aging. (2019) 10(9):771–87. doi: 10.1007/s12603-019-1273-z
27. Parahiba SM, Ribeiro ÉCT, Corrêa C, Bieger P, Perry IS, Souza GC. Effect of testosterone supplementation on sarcopenic components in middle-aged and elderly men: A systematic review and meta-analysis. Exp Gerontol. (2020) 142:111106. doi: 10.1016/j.exger.2020.111106
28. Sperduto PW, Kased N, Roberge D, Xu Z, Shanley R, Luo X, et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol. (2012) 30:419–25. doi: 10.1200/JCO.2011.38.0527
29. Kelly CM, Shahrokni A. Moving beyond karnofsky and ECOG performance status assessments with new technologies. J Oncol. (2016) 2016:6186543. doi: 10.1155/2016/6186543
30. Furtner J, Weller M, Weber M, Gorlia T, Nabors B, Reardon DA, et al. Temporal muscle thickness as a prognostic marker in patients with newly diagnosed glioblastoma: translational imaging analysis of the CENTRIC EORTC 26071-22072 and CORE trials. Clin Cancer Res. (2022) 28:129–36. doi: 10.1158/1078-0432.CCR-21-1987
Keywords: sarcopenia, cerebral metastases, survival analysis, frailty, temporal muscle
Citation: Rafaelian A, Won S-Y, Behmanesh B, Cantré D, Bernstock JD, Freiman TM, Seidlitz J, Baumgarten P, Dinc N, Konczalla J, Gessler F and Dubinski D (2025) The velocity of temporalis muscle wasting in cerebral metastasis is prognostic for poor survival. Front. Oncol. 15:1482705. doi: 10.3389/fonc.2025.1482705
Received: 18 August 2024; Accepted: 11 February 2025;
Published: 28 February 2025.
Edited by:
Steffi Thust, University of Nottingham, United KingdomReviewed by:
Atsuto Katano, The University of Tokyo Hospital, JapanCopyright © 2025 Rafaelian, Won, Behmanesh, Cantré, Bernstock, Freiman, Seidlitz, Baumgarten, Dinc, Konczalla, Gessler and Dubinski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Artem Rafaelian, YXJ0ZW0ucmFmYWVsaWFuQG1lZC51bmktcm9zdG9jay5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.