
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 26 February 2025
Sec. Skin Cancer
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1466185
 Ainara Soria1
Ainara Soria1 Pedro Sanchez Mauriño2
Pedro Sanchez Mauriño2 Juan José Serrano Domingo1
Juan José Serrano Domingo1 Regina García Galindo3
Regina García Galindo3 Silvia Sequero4Lourdes Gutiérrez Sanz5Guillermo Crespo6Roberto Díaz-Beveridge7Teresa Puértolas8Pedro López9Joaquín Fra Rodríguez10Rafael López Castro11Cristina Aguayo12
Silvia Sequero4Lourdes Gutiérrez Sanz5Guillermo Crespo6Roberto Díaz-Beveridge7Teresa Puértolas8Pedro López9Joaquín Fra Rodríguez10Rafael López Castro11Cristina Aguayo12 Javier Valdivia13Alberto Jacobo Cunquero-Tomás14Gretel Benítez15
Javier Valdivia13Alberto Jacobo Cunquero-Tomás14Gretel Benítez15 Pablo Ayala de Miguel16
Pablo Ayala de Miguel16 Enrique Espinosa17
Enrique Espinosa17 Eva Muñoz-Couselo18Begoña Campos19Lourdes García Sánchez20
Eva Muñoz-Couselo18Begoña Campos19Lourdes García Sánchez20 Pablo Cerezuela-Fuentes21*
Pablo Cerezuela-Fuentes21*Purpose: Combined BRAF/MEK inhibition with encorafenib (E) plus binimetinib (B) has demonstrated efficacy and tolerability in phase III clinical trials, and is the standard of care for advanced/metastatic BRAFV600-mutant melanoma. However, real-life evidence is limited, particularly in patients pre-treated with immune checkpoint inhibitors (ICI).
Patients and methods: BECARE GEM 2002 was a retrospective, non-interventional study aimed at investigating the real-world effectiveness and tolerability of EB in patients with unresectable or metastatic BRAFV600-mutant melanoma conducted at 21 sites in Spain. The primary objective of this study was to characterise the population of patients receiving EB and assess the efficacy and tolerability of EB in real life. The study included patients treated according to standard clinical practice with EB as the 1st line or 2nd line after progression to ICI for an unresectable or metastatic stage. Patients who previously received treatment with BRAF and/or MEK inhibitor, other than as adjuvants, that ended ≥ 6 m before EB were not eligible
Results: From September 2021 to March 2023, 117 patients were included; 89 (76.1%) and 28 (23.9%) patients received EB as 1st line and 2nd line, respectively. The median follow-up was 13.8 months (95% CI: 12.0-17.4). In patients with EB as 1st line treatment, ORR and median PFS were 75% and 12 months (95% CI: 9.4-18.6), respectively. In patients with EB as 2nd line treatment after ICI, ORR and median PFS were 77.8% and 12.5 months (95% CI: 6.6-NA), respectively. In patients with brain metastasis ORR and median PFS were 70.8% and 6.3 months (95% CI: 6.1-10.3). Treatment-related adverse events of grade ≥3 were reported in 17 (14.5%) patients; transaminitis (9.4%) and diarrhoea (2.6%) were the most frequent adverse events.
Conclusion: In this real-world study, EB treatment demonstrated effectiveness and a consistent safety profile in patients with BRAFV600-mutant melanoma treated according to standard clinical practice, including in those with prior ICI treatment and of brain metastasis; therefore, EB is a feasible treatment option for unresectable and metastatic melanoma.
Clinical trial identification: REec: 0004-2021-OBS
Clinical trial identification: REec: 0004-2021-OBS.
In the last decade, BRAF- and MEK-targeted therapies (TT) and anti-CTLA4 and anti-PD1 immune checkpoint inhibitor antibodies (ICIs) (1) have been introduced to improve the prognosis of patients with advanced and metastatic melanoma. These therapies represent the current standard of care for patients with locally advanced, unresectable, or metastatic BRAFV600-mutant melanoma.
Anti-PD1 pembrolizumab therapy achieved a 5-year overall survival (OS) rate of 38.7% (2) and combined anti-PD1 and anti-CTLA4 treatment with nivolumab and ipilimumab resulted in 5-year OS and progression-free survival (PFS) rates of 44 and 29%, respectively (3). Additionally, three TT combinations of BRAF and MEK inhibitors are available: encorafenib plus binimetinib, dabrafenib plus trametinib and vemurafenib plus cobimetinib. Comparisons between these clinical trials are limited, and only vemurafenib monotherapy has been used as a comparator in different phase III studies (4–6), showing that the combination of encorafenib plus binimetinib has a comparable or improved efficacy. The 5-year OS rates were 35%, 34% and 31%, and the observed median OS was 33.6, 25.9 and 22.5 months for encorafenib plus binimetinib (7), dabrafenib plus trametinib (8) and vemurafenib plus cobimetinib (9), respectively. The safety profiles of the three combinations were similar, with a combination-specific increase in punctual and generally mild adverse events such as fever for dabrafenib plus trametinib; skin toxicity, vemurafenib plus cobimetinib; neuromonopathies, encorafenib plus binimetinib.
After marketing authorisation by the European Medicines Agency (EMA) for the treatment of adult patients with unresectable or metastatic melanoma with the BRAFV600 mutation, encorafenib plus binimetinib became the standard of care for patients, including those with diverse profiles and prognostic characteristics who were excluded from the phase III registration trial. For instance, less than 5% of patients in the COLUMBUS trial had received check-point inhibitors prior to study inclusion, and only nine patients (4.7%) had brain metastasis.
Real-life evidence of the efficacy and tolerability of encorafenib plus binimetinib is limited, particularly in patients pre-treated with immune checkpoint inhibitors.
This study investigated the real-world efficacy, safety and tolerability of encorafenib plus binimetinib in unresectable advanced or metastatic BRAFV600-mutant malignant melanoma in Spain, focusing on patients who were treated in the 1st line and in the 2nd line after receiving ICIs.
BECARE is a multicentre, retrospective, non-interventional, observational study of encorafenib plus binimetinib in patients diagnosed with unresectable or metastatic (TNM Classification, 8th edition) BRAFV600-mutant melanoma conducted at 21 sites in Spain. All data documented in the study were obtained from the patients’ medical history and the decision to treat the patients with a specific therapeutic strategy was made before and independently from inclusion in the study, following standard clinical practice. Data from patients’ clinical histories were collected retrospectively for at least 12 months. Survival follow-up was extended until at least 51% of the documented patients declared exitus to ensure sufficient data maturity for time-to-event endpoints. All patients with melanoma who met the eligibility criteria at the participating sites were included to mitigate the selection bias.
This observational study was conducted in compliance with the International Ethical Guidelines for Biomedical Research Involving Human Subjects, Good Clinical Practice guidelines, and the Declaration of Helsinki, 1964; local laws; SAS order 3470/2009; and, Organic Law 3/2018, of December 5, on the Protection of Personal Data and guarantee of digital rights. This study received an IEC approval by the Ethics Committee of Hospital Universitario Ramón y Cajal (25/03/2021 ACTA 410). The patients signed an informed consent form prior to data collection. Considering that the research could not be carried out without the omission of written consent patients who died to avoid bias, the local Ethics Committee waived the requirement of written authorisation (as established by local Spanish regulations: RD 957/2020) in these cases. This study was registered with the Spanish Registry of Clinical Studies (Ref: 0004-2021-OBS) in May 2021.
The study included adult patients treated with 450 mg of encorafenib once daily and 45 mg of binimetinib twice per day orally, according to the current summary of product characteristics (SmPC), in the 1st line or after progression to a 1st line with immune checkpoint inhibitors in the unresectable or metastatic setting, starting this treatment at least 6 months before the patient’s inclusion in the study. Previous BRAF and/or MEK inhibitors were prohibited, except in the adjuvant setting if it ended ≥6 months before the initiation of the studied line of treatment in advanced/metastatic setting. Patients with previous systemic treatments, including chemotherapy or other treatments, other than a single 1st line ICIs in an advanced setting were excluded. Patients with any contraindications to receiving encorafenib or binimetinib, those currently participating in interventional studies, and those having any tumour other than melanoma with active treatment were excluded.
This study aimed to determine the effectiveness and safety of encorafenib plus binimetinib administration in the treatment of unresectable or metastatic BRAFV600-mutant melanoma in the real-world. The objectives of this study were to describe the baseline demographic and pathological characteristics of the population of patients treated with encorafenib plus binimetinib in Spain, treatment compliance, effectiveness and safety, survival outcomes and the influence of prognostic factors and prior systemic treatments on effectiveness.
Efficacy endpoints included objective response rate (ORR), defined as the percentage of patients that achieve partial response (PR; >30% decrease in the sum of target lesions, considering the baseline sum diameter as reference) or complete response (CR; disappearance of all target lesions) as their best responses; duration of response (DoR), defined as the time elapsed from the first determination of response (PR or CR) to the progression of the disease or death, whichever occurs first, in patients with response; disease control rate (DCR), defined as the percentage of patients with CR, PR or stable disease (SD) as their best response; duration of disease control (DoDC), calculated among responders and stable patients from the date of the start of treatment until the documentation of progression or death; progression-free survival (PFS) rate at 12 months, defined as the percentage of patients alive and free of progression (increase of >20% in the sum of diameters of target lesions, considering the smallest sum on study as the reference) at 12 months after the start of treatment; median PFS, defined as the time elapsed from the start of treatment until progression or death, whichever occurs first; and, OS, calculated from the start of treatment until the date of death due to any cause. For PFS, patients who were lost to follow-up or had no event of progression or death by the time of the analysis were censored at the date of the last tumour assessment or last contact when there was no progression, whichever occurred last. For OS, patients who were alive at the time of analysis were censored at their last follow-up. Safety endpoints included adverse events classified according to severity, number of interruptions, dose adjustments, and permanent treatment discontinuation.
The initially planned sample size was at least 50 patients, assuming that it was adequate for a descriptive study. The number of participation sites was selected considering adequate geographic coverage and the involvement of different centre types. After achieving the expected sample size, the study was amended to include up to 100 patients. The study was descriptive and no formal assumptions on safety or efficacy endpoints were made for the sample size calculations.
Statistical analyses were performed using descriptive statistics for quantitative variables and frequency, percentages and confidence intervals for categorical variables. Time-to-event endpoints and survival analyses were performed using the Kaplan-Meier method and risk factor analyses were performed based on the Cox proportional hazard model. All statistical tests were two-tailed and results with p<0.05 were considered significant. All statistical analyses were performed using R (version 3.6.3 [2020-02-29] “Holding the Windsock” R Foundation for Statistical Computing, Vienna, Austria) and SPSS (IBM SPSS Statistics version 26, Armonk, NY, US). Figures and tables were generated using RStudio (version 1.2.5033 2009-2019 RStudio, Inc., Boston, MA, US).
Between September 2021 and March 2023, 117 patients with unresectable or metastatic BRAFV600-mutant melanoma were enrolled. The baseline characteristics of the enrolled patients are summarised in Table 1. The median age was 59 years (range, 23-89 years) and the histological subtypes were superficial extension (51 patients, 43.6%), nodular (42 patients, 35.9%), acral (three patients, 2.6%) and unknown (21 patients, 17.9%). Metastasis was present at treatment initiation in 116 (99.1%) patients, with more than three metastatic sites in 49 (41.9%) patients. The most frequent metastatic locations were nodes (59.0%), lungs (43.6%), and cutaneous (26.5%). Brain and liver metastases were observed in 25 (21.4%) and 24 (20.5%) patients, respectively. Lactate dehydrogenase (LDH) levels were increased in 35.9% of patients. Encorafenib plus binimetinib was the 1st line of treatment for 89 patients (76.1%) and 2nd line of treatment after previous treatment with ICI in 28 patients (23.9%). Among patients included in the second line treatment, 24 patients (85.7%) had progressed to ICI during treatment and 4 (14.3%) after discontinuation of ICI treatment. ICIs comprised treatment with a single ICI such as nivolumab (11 patients), or pembrolizumab (nine patients); dual ICIs such as nivolumab plus ipilimumab (4 patients); clinical trial-related ICI (three patients) and ICI treatment not specified (one patient) (Supplementary Figure 1).
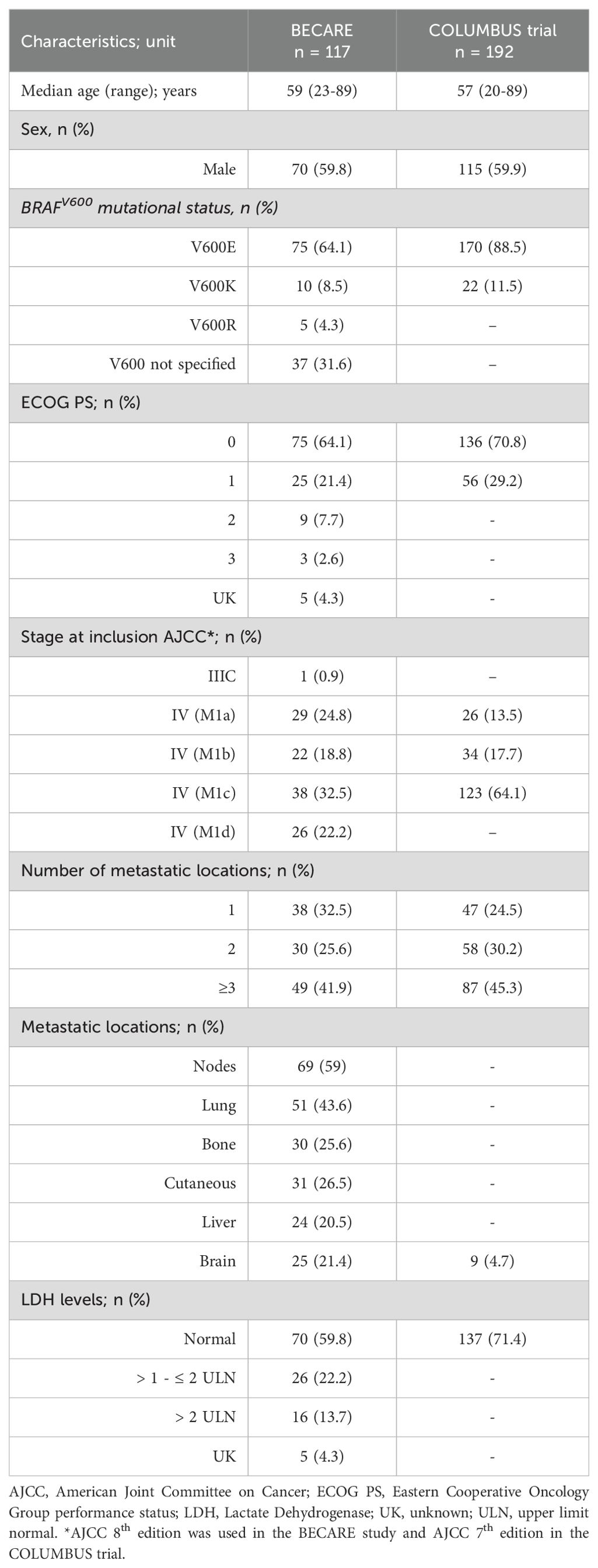
Table 1. Baseline patient characteristics for the patients enrolled in BECARE observational study, the COLUMBUS study, that led to approval of EB.
The median duration of treatment with encorafenib plus binimetinib was 11.5 months (95% CI, 8.5-13.5). At the data cut off date, 80 patients (68.4%) had permanently discontinued treatment owing to progression (58.1%), exitus (6.8%), unacceptable toxicity (6.8%), clinical deterioration (1.7%), loss to follow-up (1.7%), complete response (1.7%) and patient’s decision (0.9%). Encorafenib plus binimetinib treatment was temporarily discontinued in 37 (31.6%) patients, due to toxicity in 27 (23.1%); physician criteria, three (2.6%); requirement of radiotherapy, three (2.6%); management of coronavirus disease (COVID-19), three (2.6%); and, surgical intervention, 1 (0.9%). Dose reduction was required in 29 (24.8%) patients to manage treatment-related adverse events. The encorafenib dose was reduced to daily doses of 300 mg in 20 (17.1%) patients, 200 mg in six (5.1%), and 100 mg in one (0.9%). Binimetinib dose was reduced to two daily doses of 30 mg in 23 (19.7%) patients. Two and six patients did not report the details of dose reductions of encorafenib and binimetinib, respectively. Both treatment doses were reduced in 20 (17.1%) patients.
With a median follow-up of 13.8 months (95% CI, 12.0-17.4), the ORR was 75.7% and the DCR was 90.1% (Figure 1A). The median follow-up was 14.6 months (95% CI: 12.0-19.0) and 12.7 months (95% CI: 9.9, 17.3) for patients in the 1st and 2nd line treatment, respectively. The ORR and DCR for patients treated with encorafenib plus binimetinib as 1st line treatment were 75% and 90.5%, respectively, whereas the ORR and DCR for patients treated in the 2nd line were 77.8% and 88.9%, respectively (Figures 1B, C). The DoDC was 9.7 months (95% CI 6.9-16.9) for the overall population; 9.9 months (95% CI 7.8-18.3), patients treated with encorafenib plus binimetinib as 1st line treatment; and, 6.8 months (95% CI 3.3-not reached [NR]), patients treated after immune checkpoint inhibitors (Supplementary Figure 2). Patients with brain metastasis (n=25) showed ORR and DCR of 70.8% and 83.3%, respectively, and patients with M1a/b/c showed ORR and DCR of 74.2% and 87.6%, respectively (Figures 1D, F). Patients with liver metastasis had an ORR and DCR of 83.3% and 91.7% Figure 1E. The ORR was 81.9% and 56.5% in patients with ECOG 0 and ≥1, respectively.
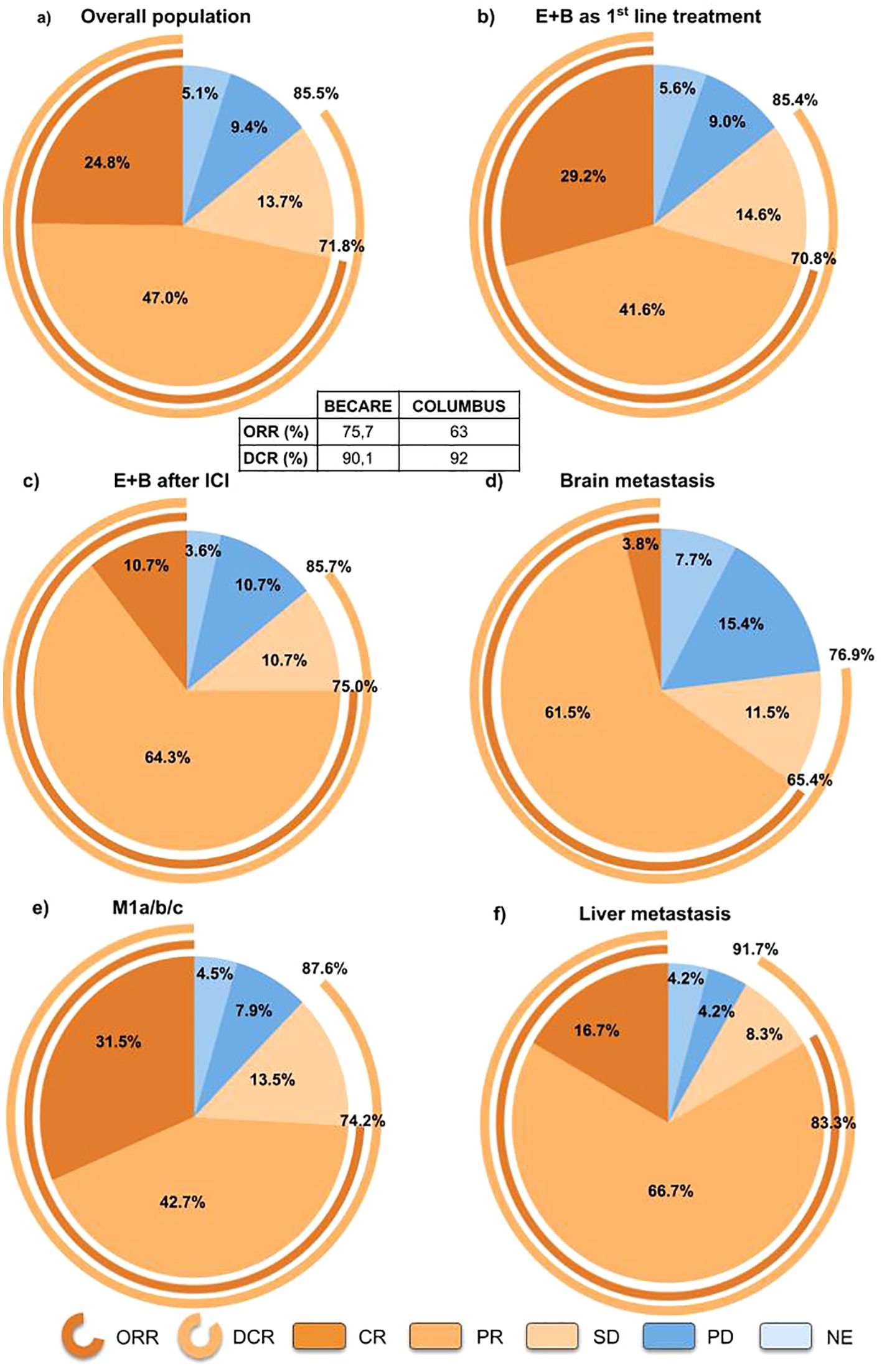
Figure 1. Best overall response for (A) overall population, (B) patients treated with encorafenib+binimetinib as 1st line, (C) patients treated with encorafenib+binimetinib as 2nd line, (D) patients with brain metastasis, (E) patients with liver metastasis, and (F) patients with M1a/b/c melanoma. DCR, disease control rate; E+B, encorafenib plus binimetinib; ICI, Immune checkpoint inhibitors; ORR, objective response rate; NE, not evaluable.
The median global PFS was 12.0 months (95% CI, 9.9-16.7) and the 12-month PFS rate was 50.7% (95% CI, 42.3-60.8) (Figure 2A). Efficacy was similar in 1st and 2nd line, with a median PFS and 12-month PFS of 12.0 months (95% CI, 9.4-18.6) and 50.3% (95% CI, 40.7-62.0) for 1st line treatment, and 12.5 months (95% CI, 6.6-NR) and 52% (95% CI, 36.1-74.8) for 2nd line treatment, respectively (Figure 2B, Supplementary Figure 3). The median PFS in patients with ECOG 0, 1 and ≥2 was 16.0 months (95% CI, 11.4-22.8), 7.7 months (95% CI, 5.1-29.6) and 6.6 months (95% CI, 6.3-NR), respectively (Supplementary Figure 4). For patients with M1a/b/c melanoma, the median PFS was 13.5 months (95% CI, 10.7-21.6).
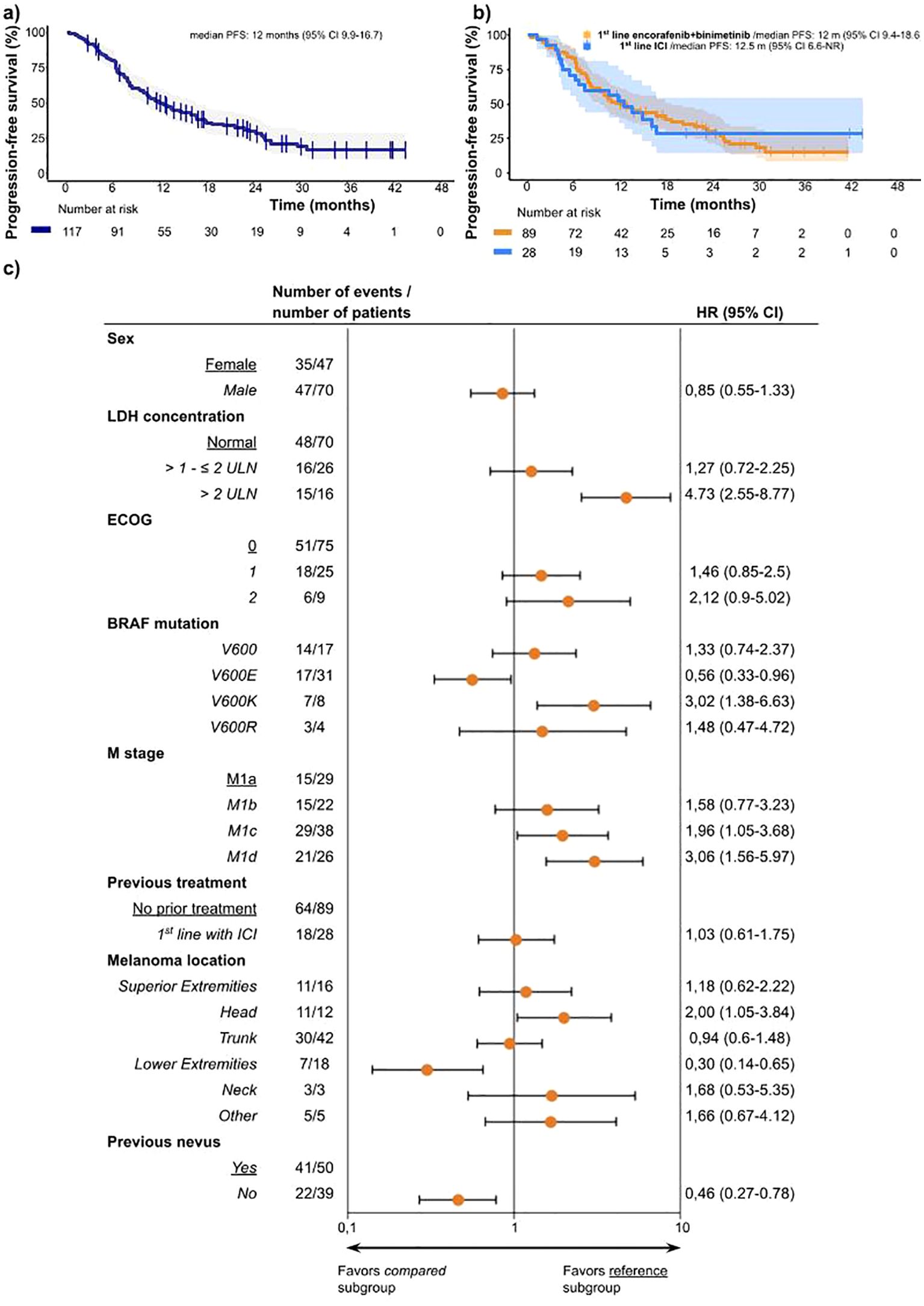
Figure 2. (A) Kaplan-Meier curves of progression-free survival for overall population and median PFS. (B) Kaplan-Meier curves of progression-free survival and median PFS for encorafenib plus binimetinib as 1st line treatment (orange) and encorafenib plus binimetinib after treatment with checkpoint inhibitors (blue). (C) Progression-free survival by subgroups according to baseline characteristics. For each characteristic, the subgroups are compared with other subgroup as reference. This reference is listed first and underlined and has no Hazard ratio calculated, except for BRAF mutation and Melanoma location, which were compared with the opposite option. As an example, BRAFV600E mutation was compared to population not having BRAF V600E mutation. Compared groups are written in italic. ECOG status 3, Melanoma location Hand and Melanoma location Feet are not included due to the very low number of cases and all this patient did not survive. ECOG PS, Eastern Cooperative Oncology Group performance status; LDH, Lactate Dehydrogenase; ULN, upper limit normal.
Receiving encorafenib plus binimetinib treatment as 1st or 2nd line treatment did not significantly affect the risk of progression or death (HR 1.03, 95% CI: 0.61-1.75; p=0.900) (Figure 2C). Male patients had a similar risk of progression as that of female patients (HR 0.85, 95% CI: 0.55-1.33; p=0.483). Analysis of histology and location as prognostic factors showed a lower risk of progression or death for melanoma located at lower extremities (HR 0.30; 95% CI: 0.14-0.65; p=0.002) and higher risk when located in the head (HR 2.00, 95%CI: 1.05-3.84; p=0.036) (Figure 2C). The univariate Cox analysis of baseline BRAFV600 mutations showed that the type of mutation correlates with the prognosis, showing a lower risk of progression or death for BRAFV600E (HR 0.56, 95%CI: 0.33-0.96; p=0.035) and higher risk for BRAFV600K mutation (HR 3.02, 95%CI: 1.38-6.63; p=0.006). The patients with normal levels of LDH and elevated >1 and ≤2 times above (upper limit of normal (ULN) had comparable PFS, but the risk was higher in patients with LDH levels elevated >2 times above ULN (HR 4.73, 95%CI: 2.55-8.77; p<0.001) (Figure 2C).
Subgroup analyses of the M subtypes showed a worse prognosis in subtypes M1d (HR 3.06, 95% CI: 1.56-5.97; p=0.001) and M1c (HR 1.96, 95% CI: 1.05-3.68; p=0.035) compared to those in M1a and M1b (HR 1.58, 95% CI: 0.77-3.23; p=0.214). The median PFS for the M1d subgroup was 6.3 (95% CI, 6.12-10.25) months and the 12-month PFS rate was 25.2% (Supplementary Figure 5). Patients with M1a/b/c had a median OS of 25.8 months (95% CI, 17.9-NR) (Supplementary Figure 6). Patients with liver metastasis had a median PFS of 11.4 (95% CI, 6.3-25) months and median OS of 14.8 (95% CI, 7.4-NR) months (Supplementary Figure 7). The OS rate at 12 months in patients with brain metastasis was 35.2% (95% CI, 20.4-60.7). Only one patient with brain metastasis was included after progression to ICI, reporting PR as the best response and being alive and free of progression 14 months after the initiation of encorafenib plus binimetinib treatment.
For patients receiving encorafenib plus binimetinib as 1st line and 2nd line treatment, the 12-month OS rates were 69.1% and 60.7%, respectively (Figure 3).
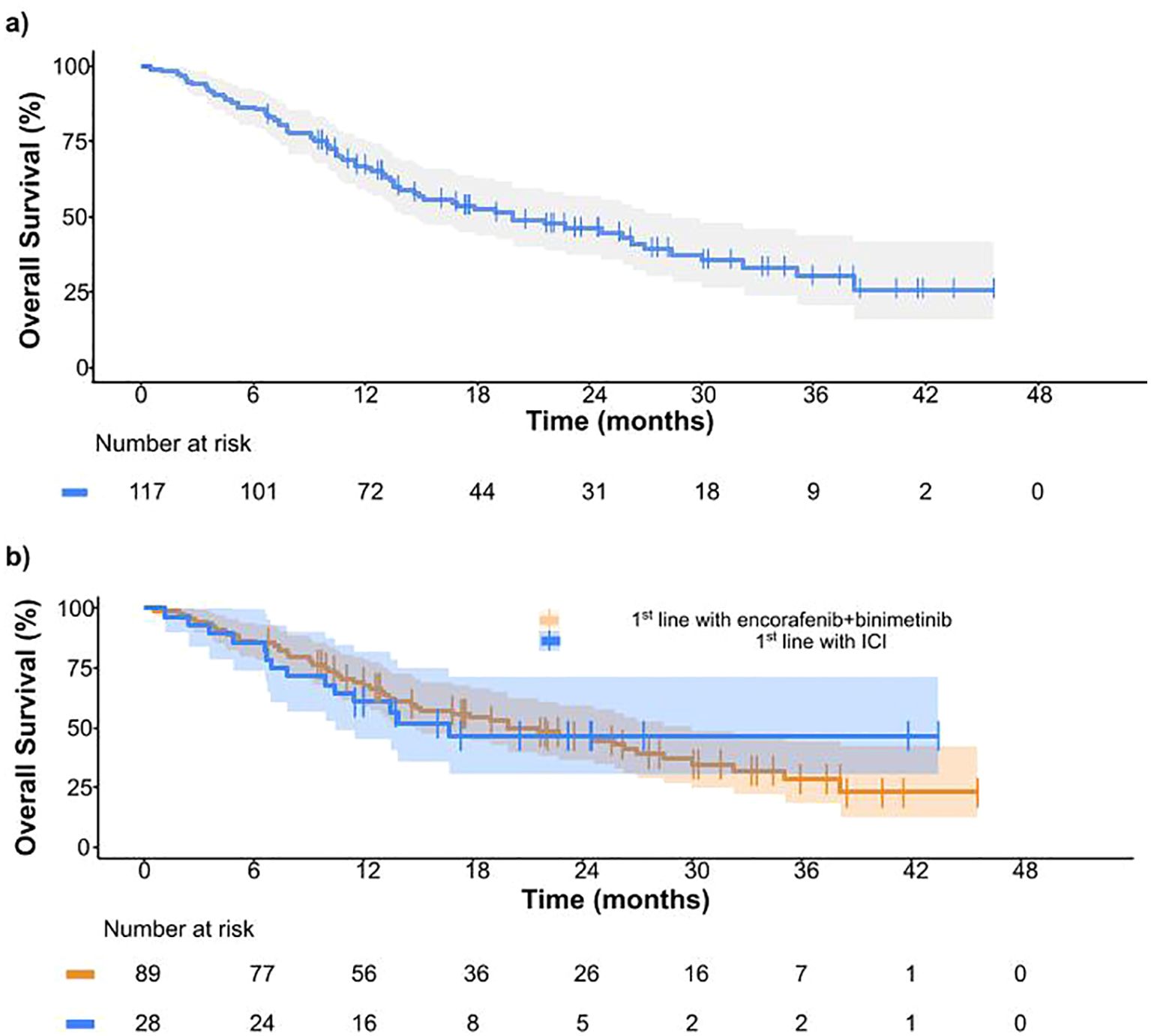
Figure 3. (A) Overall survival in all patients from BECARE study. (B) Overall survival for patients receiving encorafenib plus binimetinib as 1st line treatment (orange) and encorafenib plus binimetinib after treatment with checkpoint inhibitors (blue).
Of the 117 patients, 50 (42.7%) experienced adverse events, 47 (40.2%) of which had AE related to encorafenib and binimetinib. The most frequent treatment-related adverse events were diarrhoea (n=16, 13.7%), fatigue (n=12, 10.3%) and transaminitis (n=10, 8.5%) (Supplementary Tables 1, 2). Grade 3-4 treatment-related adverse events were reported in 17 patients (14.5%), and the most frequent were transaminitis in seven (6%) patients; diarrhoea, three (2.6%); and, fatigue, three (2.6%) (Figure 4). No grade 5 toxicities were observed. The safety profile was not significantly different between patients receiving encorafenib plus binimetinib as 1st line and those treated after ICI.
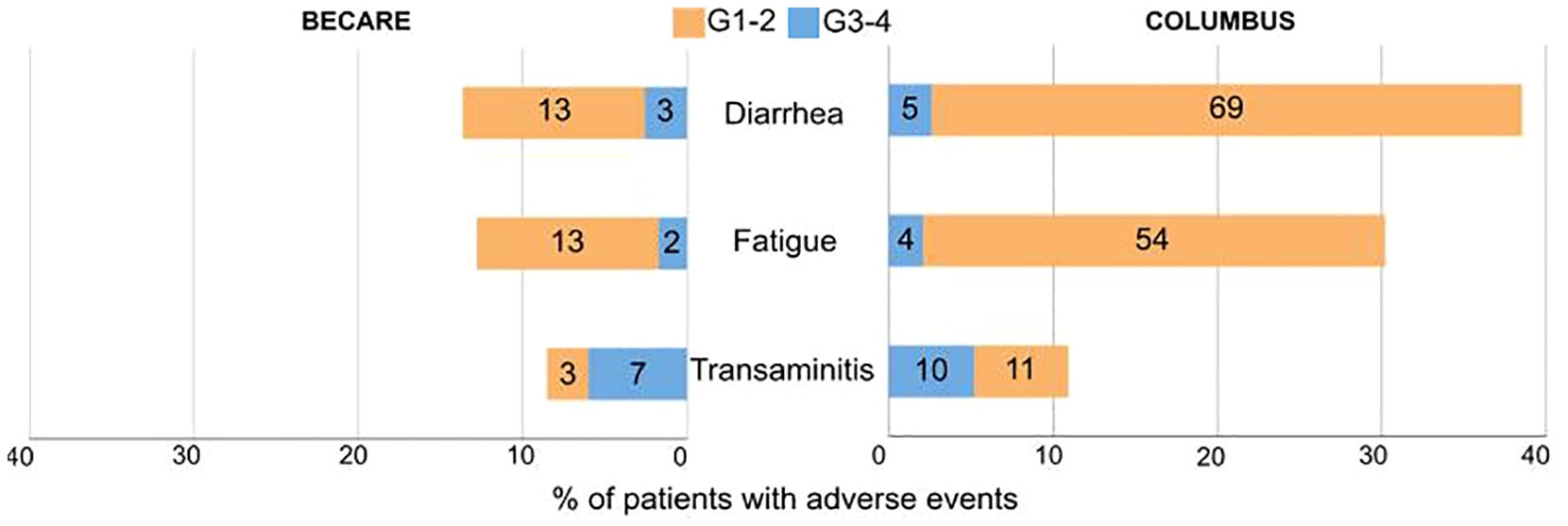
Figure 4. Bar chart of most frequent adverse events with 5% threshold in BECARE (left) and COLUMBUS (right) study. The number of patients with the AE are indicated in each bar.
BECARE is the 1st observational study to report the real-world effectiveness and safety of encorafenib plus binimetinib for the treatment of unresectable or metastatic BRAFV600-mutant malignant melanoma in Spain.
The PFS reported in the BECARE trial was equivalent to the reported in the phase III registration study COLUMBUS, reaching a median PFS of 12 vs 14.9 months and a 12-month PFS rate of 50.7% vs. 56.2% for BECARE and COLUMBUS, respectively. The PFS values were slightly lower in the BECARE study, which was potentially influenced by the fact that the real-world population had worse prognostic factors (i.e. older population [59 vs 57], higher rate of brain metastasis [21.4% vs 4.7%], or a higher % of patients with LDH above the ULN [47.7% vs 28.6%]). This finding is consistent with those of previous reports, suggesting that patients with brain metastasis or high LDH levels are underrepresented in phase III clinical trials. The median PFS was similar to that reported for dabrafenib plus trametinib (11.4 months, COMBI-v study) (10) and higher than that for cobimetinib plus vemurafenib (9.9 months) (4) in phase III clinical trials. The DCR was similar for all TKIs, and the ORR reported in the BECARE trial (75.7%) was higher than that in the COLUMBUS study (63%) and phase III trials with other BRAF/MEK inhibitors such as dabrafenib plus trametinib or cobimetinib plus vemurafenib (5, 11).
A subgroup analysis was performed to better understand the efficacy of encorafenib plus binimetinib in specific populations. Consistent with previous reports (12), our data showed that patients with M1c metastasis (distant metastasis to non-CNS visceral sites) had a higher risk of disease progression or death (HR, 1.96) than those with M1a metastasis. Additionally, our study included 26 (22.2%) patients with M1d (distant metastasis in the CNS) and had an even worse prognosis, with an HR of 3.06 compared to M1a. The COLUMBUS study only included nine (4.7%) patients, and the coBRIM study only included one (0.4%) patient with brain metastasis. These patients had a slightly lower response rate and the median PFS was nearly half that of the overall population. However, the median PFS in patients with brain metastasis was higher than that in previous reports (12–14), suggesting that encorafenib plus binimetinib is a feasible option for these patients.
With regard to patients receiving encorafenib plus binimetinib as 2nd line after ICI, in the BECARE study, the ORR, DCR, and PFS outcomes were similar to those in patients treated with the combination in the 1st line. Although the numerical 12-month OS rate was slightly lower than that in the 1st line, the difference was not statistically significant. Previous real-world studies with other TKIs have also shown similar trends (15). Thus, our results show that encorafenib plus binimetinib is a feasible treatment option even after progression to ICI. Regarding this observation, early evidence on sequentiality indicated that ICI first could reach better outcomes than BRAF/MEK inhibitors in advanced melanoma (16). However, the study was not designed to compare encorafenib plus binimetinib with ICI, and therefore we could not provide recommendations on sequentiality, which may require further evidence from randomized trials or real world evidence using propensity score in bigger patient datasets.
The toxicity profile in the real world is manageable and validated the results of the phase III clinical trial. According to our results, in the real world, treatment-related adverse events were lower than those in the registration phase III COLUMBUS clinical trial, which led to the approval of encorafenib plus binimetinib treatment by the FDA and EMA. The number of AEs was lower in our study. Most common G3-4 AE proportions were similar between the BECARE and COLUMBUS studies, with proportions of 2.6% vs. 2.6%, 1.7% vs. 2.1%, and 4.3% vs. 5.2% for diarrhoea, fatigue, and transaminitis respectively.
A decrease in the number of adverse events resulted in fewer dose reductions (24.8% vs. 48%) and lower discontinuation rates (6.0% vs. 8.3%). These results are consistent with previous observational studies (17) and support the idea that the implemented management strategies in clinical practice and the experience of handling treatment-related adverse events contributed to reducing the number of discontinuations due to toxicity (18). The low discontinuation rates observed might respond to a less stringent discontinuation criteria in the real-world than in clinical trials, and the potential bias due to the inherently less stringent monitoring of adverse events in observational studies can not be discarded.
Discontinuation rates due to toxicity after treatment with other TKIs were 14% for cobimetinib plus vemurafenib (4), 7% for vemurafenib (4) and 13% for dabrafenib plus trametinib (10). For immunotherapy, toxicity-related discontinuation in a real-world context has been reported to range from 22 to 32% (19, 20). Discontinuation of melanoma treatment due to toxicity in a real-world context has been reported to range from 4 to 10% for targeted therapies (14, 15, 18, 21). Consistent with our results, toxicities appear to be better managed in clinical practice leading to fewer toxicity-related discontinuations.
The limitations of this study are those inherent to retrospective observational studies, such as limited follow-up, a higher missing data rate, lack of standardised tumour assessment criteria (i.e. RECIST) and small subgroups. Nevertheless, most data was available to ensure reliable conclusions. This study also had no control arm to contextualise the results. Although follow-up was acceptable to address the proposed survival outcomes, further follow-up after long term will help to confirm the benefit of E+B on survival.
In conclusion, encorafenib plus binimetinib showed comparable efficacy than that in the phase III registration trial and good tolerability, despite worse prognosis in the real-world population studied, which comprised more cases of brain and liver metastases. Encorafenib plus binimetinib is a feasible treatment option for unresectable and metastatic melanoma in the real-world, with similar outcomes as 1st line treatment or after treatment with ICI, including in patients with brain metastasis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee from Hospital Universitario Ramón y Cajal (25/03/2021 ACTA 410). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AS: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. PS: Investigation, Resources, Visualization, Writing – review & editing. JS: Investigation, Resources, Visualization, Writing – review & editing. RG: Investigation, Resources, Visualization, Writing – review & editing. SS: Investigation, Resources, Visualization, Writing – review & editing. LG (6th author): Investigation, Resources, Visualization, Writing – review & editing. GC: Investigation, Resources, Visualization, Writing – review & editing. RD: Investigation, Resources, Visualization, Writing – review & editing. TP: Investigation, Resources, Visualization, Writing – review & editing. PL: Investigation, Resources, Visualization, Writing – review & editing. JF: Investigation, Resources, Visualization, Writing – review & editing. RL: Investigation, Resources, Visualization, Writing – review & editing. CA: Investigation, Resources, Visualization, Writing – review & editing. JV: Investigation, Resources, Visualization, Writing – review & editing. AC: Investigation, Resources, Visualization, Writing – review & editing. GB: Investigation, Resources, Visualization, Writing – review & editing. PA: Investigation, Resources, Visualization, Writing – review & editing. EE: Investigation, Resources, Visualization, Writing – review & editing. EM: Investigation, Resources, Visualization, Writing – review & editing. BC: Investigation, Resources, Visualization, Writing – review & editing. LG (21st author): Investigation, Resources, Visualization, Writing – review & editing. PC: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was sponsored by the Grupo Español Multidisciplinar Melanoma (GEM) with Industry partner Pierre-Fabre Ibérica. The funder did not have a role in designing or conducting the study.
The authors thank all patients and families, investigators and study staff involved in the BECARE study; the MFAR Clinical Research team for regulatory, monitoring, and quality assurance activities; Guillem Marco Ph.D and Pau Doñate Ph.D. for manuscript and language editing; and Emilio Pecharroman MsC. for statistical support. This study was previously presented at the ESMO Congress 2022 and the ESMO Congress 2023.
EM: received honoraria for speaker, consultancy or advisory role from Novartis, BMS, MSD, Pierre Fabre, Roche, Sanofi and SunPharma, Sanofi and Regeneron, and aid for attendance at conferences from Novartis, MSD and Pierre Fabre. EE: received honoraria for speakers from BMS, MSD, Novartis and Pierre Fabre. PC: received honoraria for speaker, consultancy or advisory role from Novartis, BMS, MSD, Pierre Fabre, Roche, Sanofi and SunPharma, and aid for attendance at conferences from Novartis, MSD and Pierre Fabre. GC: received honoraria for speaker, consultancy or advisory role from Novartis, BMS, MSD, Pierre Fabre and Roche, and aid for attendance at conferences from BMS, MSD and Pierre Fabre. RL: Received honoraria for speaker, consultancy or advisory role from Novartis, BMS, MSD, Pierre Fabre, Roche and Aristo and aid for attendance at conferences from Roche, MSD, Takeda and Pierre Fabre. PA: Received honoraria for speaker from MSD, Novartis, Pierre Fabre and Sanofi. CA: Received honoraria for advisory board from Pierre Fabre and for continuous medical education from Pfizer, Novartis, MSD, Pierre Fabre, BMS and Roche. JF: received honoraria for speaker, consultancy or advisory role from Pierrre-Fabre, Novartis-ADVANCED ACCELERATOR APPLICATIONS IBÉRICA, Merck, Astra-Zeneca and Roche; and aid for attendance at conferences from MSD, Roche and Pierre Fabre. AC: received honoraria for speaker from BMS and Gilead, and aid for attendance at conferences from MSD. SS: Received honoraria for speaker or advisory from MSD, Novartis, Pierre Fabre, Roche, Sanofi, Regeneron, Gilead, Incyte, AstraZeneca, Pfizer and aid for attendance at conferences from Novartis, Roche, MSD and Pierre Fabre. BC: received honoraria for speaker, consultancy or advisory role from Novartis, BMS, MSD, Pierre Fabre, Roche, SunPharma, Sanofi and Regeneron, and aid for attendance at conferences from Novartis, BMS and Pierre Fabre. AS: received honoraria for speaker, consultancy or advisory role from BMS, Merck, Sharp&Dohme, Novartis, Sanofi and Pierre Fabre, and aid for attendance at conferences from Pierre Fabre, Merck and Sharp&Dohme. TP: received honoraria for presentations from BMS, Immunocore, Novartis, Pierre-Fabre, SunPharma and MSD, Advisory Board from BMS, Immunocore, Novartis, Pierre-Fabre, Seagen and SunPharma.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1466185/full#supplementary-material
1. Ugurel S, Röhmel J, Ascierto PA, Flaherty KT, Grob JJ, Hauschild A, et al. Survival of patients with advanced metastatic melanoma: the impact of novel therapies-update 2017. Eur J Cancer Oxf Engl 1990. (2017) 83:247–57. doi: 10.1016/j.ejca.2017.06.028
2. Robert C, Ribas A, Schachter J, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. (2019) 20:1239–51. doi: 10.1016/S1470-2045(19)30388-2
3. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. (2019) 381:1535–46. doi: 10.1056/NEJMoa1910836
4. Ascierto PA, McArthur GA, Dréno B, Atkinson V, Liszkay G, Di Giacomo AM, et al. Cobimetinib combined with vemurafenib in advanced BRAF(V600)-mutant melanoma (coBRIM): updated efficacy results from a randomised, double-blind, phase 3 trial. Lancet Oncol. (2016) 17:1248–60. doi: 10.1016/S1470-2045(16)30122-X
5. Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, Stroiakovski D, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. (2015) 372:30–9. doi: 10.1056/NEJMoa1412690
6. Dummer R, Ascierto PA, Gogas HJ, Arance A, Mandala M, Liszkay G, et al. Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. (2018) 19:603–15. doi: 10.1016/S1470-2045(18)30142-6
7. Dummer R, Flaherty KT, Robert C, Arance A, de Groot JWB, Garbe C, et al. COLUMBUS 5-year update: A randomized, open-label, phase III trial of encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF V600–mutant melanoma. J Clin Oncol. (2022) 40:4178–88. doi: 10.1200/JCO.21.02659
8. Robert C, Grob JJ, Stroyakovskiy D, Karaszewska B, Hauschild A, Levchenko E, et al. Five-year outcomes with dabrafenib plus trametinib in metastatic melanoma. N Engl J Med. (2019) 381:626–36. doi: 10.1056/NEJMoa1904059
9. Ascierto PA, Dréno B, Larkin J, Ribas A, Liszkay G, Maio M, et al. 5-Year Outcomes with Cobimetinib plus Vemurafenib in BRAFV600 Mutation-Positive Advanced Melanoma: Extended Follow-up of the coBRIM Study. Clin Cancer Res Off J Am Assoc Cancer Res. (2021) 27:5225–35. doi: 10.1158/1078-0432.CCR-21-0809
10. Long GV, Hauschild A, Santinami M, Atkinson V, Mandalà M, Chiarion-Sileni V, et al. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. N Engl J Med. (2017) 377:1813–23. doi: 10.1056/NEJMoa1708539
11. Larkin J, Ascierto PA, Dréno B, Atkinson V, Liszkay G, Maio M, et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N Engl J Med. (2014) 371:1867–76. doi: 10.1056/NEJMoa1408868
12. Aglietta M, Chiarion-Sileni V, Fava P, Guidoboni M, Depenni R, Minisini A, et al. Outcomes in patients with BRAFV600-mutated melanoma and brain metastases at baseline treated with dabrafenib plus trametinib. Tumori. (2023) 109:537–45. doi: 10.1177/03008916231179251
13. Davies MA, Liu P, McIntyre S, Kim KB, Papadopoulos N, Hwu WJ, et al. Prognostic factors for survival in melanoma patients with brain metastases. Cancer. (2011) 117:1687–96. doi: 10.1002/cncr.v117.8
14. Kähler KC, Debus D, Schley G, Göppner D, Hassel JC, Meier F, et al. Effectiveness, safety and utilization of cobimetinib and vemurafenib in patients with BRAF V600 mutant melanoma with and without cerebral metastasis under real-world conditions in Germany: the non-interventional study coveNIS. Melanoma Res. (2024) 34:44–53. doi: 10.1097/CMR.0000000000000908
15. Richtig E, Nguyen VA, Koelblinger P, Wolf I, Kehrer H, Saxinger W, et al. Dabrafenib plus trametinib in unselected advanced BRAF V600–mut melanoma: a non-interventional, multicenter, prospective trial. Melanoma Res. (2024) 34(2):142–151. doi: 10.1097/CMR.0000000000000948
16. Atkins MB, Lee SJ, Chmielowski B, Tarhini AA, Cohen GI, Truong TG, et al. Combination dabrafenib and trametinib versus combination nivolumab and ipilimumab for patients with advanced BRAF-mutant melanoma: the DREAMseq trial—ECOG-ACRIN EA6134. J Clin Oncol. (2023) 41:186–97. doi: 10.1200/JCO.22.01763
17. Rauwerdink DJW, Molina G, Frederick DT, Sharova T, Carmichael H, Boland GM. Adjuvant therapy failure patterns in the modern era of melanoma management. Ann Surg Oncol. (2020) 27:5128–36. doi: 10.1245/s10434-020-08631-2
18. Manzano JL, Martin-Liberal J, Fernández-Morales LA, Benítez G, Medina Martínez J, Quindós M, et al. Adjuvant dabrafenib and trametinib for patients with resected BRAF -mutated melanoma: DESCRIBE-AD real-world retrospective observational study. Melanoma Res. (2023) 33:388–97. doi: 10.1097/CMR.0000000000000888
19. Koelblinger P, Hoellwerth M, Dernoscheg MT, Koch L, Richtig E, Wanner M, et al. Adjuvant anti-PD-1 antibody treatment in stage III/IV melanoma: real-world experience and health economic considerations. J Dtsch Dermatol Ges J Ger Soc Dermatol JDDG. (2021) 19:1186–98. doi: 10.1111/ddg.14511
20. Mangana J, Dimitriou F, Braun R, Ludwig S, Dummer R, Barysch MJ. Single-center real-life experience with low-dose ipilimumab monotherapy in adjuvant setting for patients with stage III melanoma. Melanoma Res. (2019) 29:648–54. doi: 10.1097/CMR.0000000000000593
Keywords: melanoma, molecular targeted therapy, mutation, retrospective studies, immune checkpoint inhibitors
Citation: Soria A, Sanchez Mauriño P, Serrano Domingo JJ, García Galindo R, Sequero S, Gutiérrez Sanz L, Crespo G, Díaz-Beveridge R, Puértolas T, López P, Fra Rodríguez J, López Castro R, Aguayo C, Valdivia J, Cunquero-Tomás AJ, Benítez G, Ayala de Miguel P, Espinosa E, Muñoz-Couselo E, Campos B, García Sánchez L and Cerezuela-Fuentes P (2025) Real-life evidence of encorafenib plus binimetinib in patients with unresectable advanced or metastatic BRAFV600-mutant melanoma in Spain: the BECARE (GEM-2002) trial. Front. Oncol. 15:1466185. doi: 10.3389/fonc.2025.1466185
Received: 17 July 2024; Accepted: 17 January 2025;
Published: 26 February 2025.
Edited by:
Nikhil I. Khushalani, Moffitt Cancer Center, United StatesCopyright © 2025 Soria, Sanchez Mauriño, Serrano Domingo, García Galindo, Sequero, Gutiérrez Sanz, Crespo, Díaz-Beveridge, Puértolas, López, Fra Rodríguez, López Castro, Aguayo, Valdivia, Cunquero-Tomás, Benítez, Ayala de Miguel, Espinosa, Muñoz-Couselo, Campos, García Sánchez and Cerezuela-Fuentes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Cerezuela-Fuentes, cGNlcmV6dWVsYWZAc2VvbS5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.