 Wen-Wen Yang1,2
Wen-Wen Yang1,2 Xiong Zhou
Xiong Zhou Gan He
Gan He- 1Department of Ophthalmology, Chongqing University Center Hospital, Chongqing Emergency Medical Center, Chongqing Fourth People’s Hospital, Chongqing, China
- 2Department of Hepatobiliary Surgery, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, China
- 3Department of Gastrointestinal Surgery, Yongchuan Hospital of Chongqing Medical University, Chongqing, China
Purpose: The purpose of this current study was to find out whether human immunodeficiency virus (HIV) affected overall survival (OS) of colorectal cancer (CRC) patients after surgery.
Methods: PubMed, Embase, the Cochrane Library, and CNKI were searched from inception to March 27, 2023 to find eligible studies. Eligible studies included CRC patients grouped by HIV status (HIV-positive and HIV-negative). Stata SE 16 was used for data analysis.
Results: A total of eight studies involving 2180 patients were enrolled in this study. After data analysis, there were significant differences in sex (OR=0.69, 95% CI=0.49 to 0.98, I2 = 22.6%, P=0.04<0.1), tumor grade (OR=6.61, 95% CI=2.36 to 18.49, I2 = 0.00%, P=0.00<0.1), and tumor location (OR=2.19, 95% CI=1.74 to 2.77, I2 = 0.04%, P=0.00<0.1) between the HIV and non-HIV groups. Furthermore, we found that HIV was associated with worse OS in CRC patients after surgery (HR=3.12, 95% CI=2.07 to 4.69, I2 = 52.51%, P=0.00<0.1).
Conclusion: This study highlights that HIV is associated with significantly poorer OS in CRC patients after surgery, emphasizing the need for tailored postoperative management strategies for this vulnerable population. Future research should explore underlying mechanisms and potential interventions to improve outcomes for HIV-positive CRC patients.
1 Introduction
In recent years, with the use of highly active antiretroviral therapy (HAART), the survival of human immunodeficiency virus (HIV) -infected patients has been significantly increased (1–4). This has led to an increased chance of malignancy in HIV-infected people as well, especially in non-HIV related malignancy (5, 6).
Colorectal cancer (CRC) is one of the most common malignancies in the world and the second leading cause of cancer-related deaths (7, 8). Currently, there are approximately 185 million CRC patients worldwide (9). Surgical resection remains the cornerstone of colorectal cancer treatment (10, 11). Previous studies have shown that the incidence of CRC is higher in people with HIV compared to the general population (12–14). As the life expectancy of HIV patients increases, it is important to understand the epidemiology and natural course of CRC in HIV-infected patients and its treatment.
The impact of HIV on postoperative overall survival (OS) in CRC patients remained controversial in previous studies. Berretta M et al. (15) and Sigel C et al. (16) found that OS after surgery was worse in HIV-infected CRC patients than in general CRC patients. Other studies reported there was no significant difference of HIV on OS in CRC patients after surgery (17–21). Therefore, this study aimed to determine whether HIV affects the overall survival of CRC patients post-surgery and to identify factors contributing to worse outcomes.
2 Methods
This study was performed with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (22).
2.1 Search strategy
Four databases including PubMed, Embase, the Cochrane Library, and CNKI were searched from inception to March 27, 2023. Two key words were as follows: HIV and CRC. As for HIV, the search strategy was as follows: (HIV OR human immunodeficiency virus OR AIDS OR acquired immunodeficiency syndrome); in terms of CRC, we searched: (colorectal cancer OR colorectal neoplasm OR colorectal tumor OR colorectal carcinoma). Finally, we used “AND” to connect the key words. Titles and abstracts were limited. English and Chinese were the limited languages.
2.2 Inclusion and exclusion criteria
Inclusion and exclusion criteria were used to screen potential articles. The inclusion criteria were as follows: 1, all patients were diagnosed with CRC and underwent surgery; and 2, both the HIV group and the non-HIV group were reported. The exclusion criteria were as follows: 1, case reports, case series, comments, letters to the editor, conference abstracts and nonoriginal articles; 2, data were repeated or overlapped; and 3, incomplete data.
2.3 Study selection
Four databases were independently searched and screened for eligible studies by two researchers. First, duplicate studies were excluded. Then, the two researchers scanned the titles and abstracts to exclude ineligible studies according to the inclusion and exclusion criteria. Finally, full text would be read to identify studies that could be included. The group discussion resolved all differences.
2.4 Data collection
The information contained baseline characteristics of the included studies and patients. The studies’ characteristics included first author, published year, country, study date, study type, sample size, language of the studies, and Newcastle-Ottawa Scale (NOS) score. As for patients’ baseline information, age, sex, tumor stage, grade, and location were collected. As for prognosis, we included OS.
2.5 Quality assessment
NOS was used to assess the quality of included studies (23). Classification of eligible articles as high quality (9 points), medium quality (7-8 points), or low quality (less than 7 points) based on NOS score.
2.6 Statistical analysis
Dichotomous variables were described by odds ratios (ORs) and 95% confidence intervals (CIs). Mean differences (MDs) and 95% CIs were calculated for continuous variables. Hazard ratios (HRs) and 95% CIs were used to calculate prognosis of patients. To evaluate the statistical heterogeneity, the I2 value and the chi-squared test were used (24, 25). We used the random effects model only to deliver more conservative conclusions, and p<0.1 was considered statistically significant. Stata SE 16 was used for data analysis.
3 Results
3.1 Study selection
A total of 2694 studies were searched from four databases (556 in PubMed, 884 in Embase, 373 in the Cochrane Library, 881 in CNKI) on March 27, 2023. 2284 records were left after duplicates removed. Then, 437 unqualified studies were excluded. After screening the titles and abstracts, 17 studies were left for full text accessed. Finally, eight eligible studies were enrolled in this study (15–21, 26) (Figure 1).
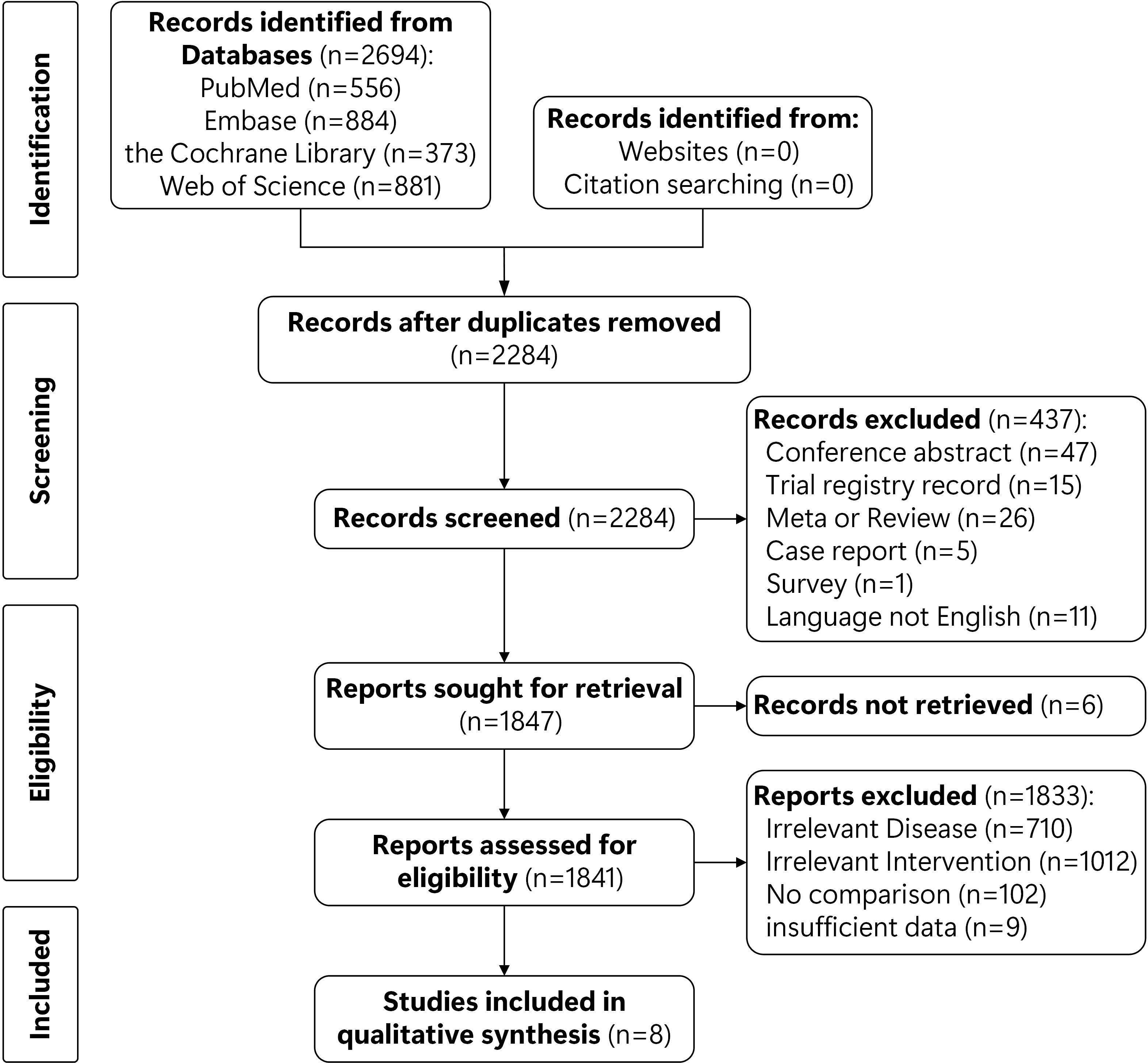
Figure 1. Flowchart of study selection.
3.2 Baseline characteristics of the included studies
There were eight studies involving 2180 patients enrolled, 493 patients in the HIV group and 1687 patients in the non-HIV group. These studies were firstly published in 2007 and most recently in 2022. The studies were published in Israel, the United States America (USA), Japan, South Africa, China, and some other Europe countries. The study date was from 1985 to 2019. All the studies were retrospective studies. More details (sample size, language of studies and NOS score) were shown in Table 1.
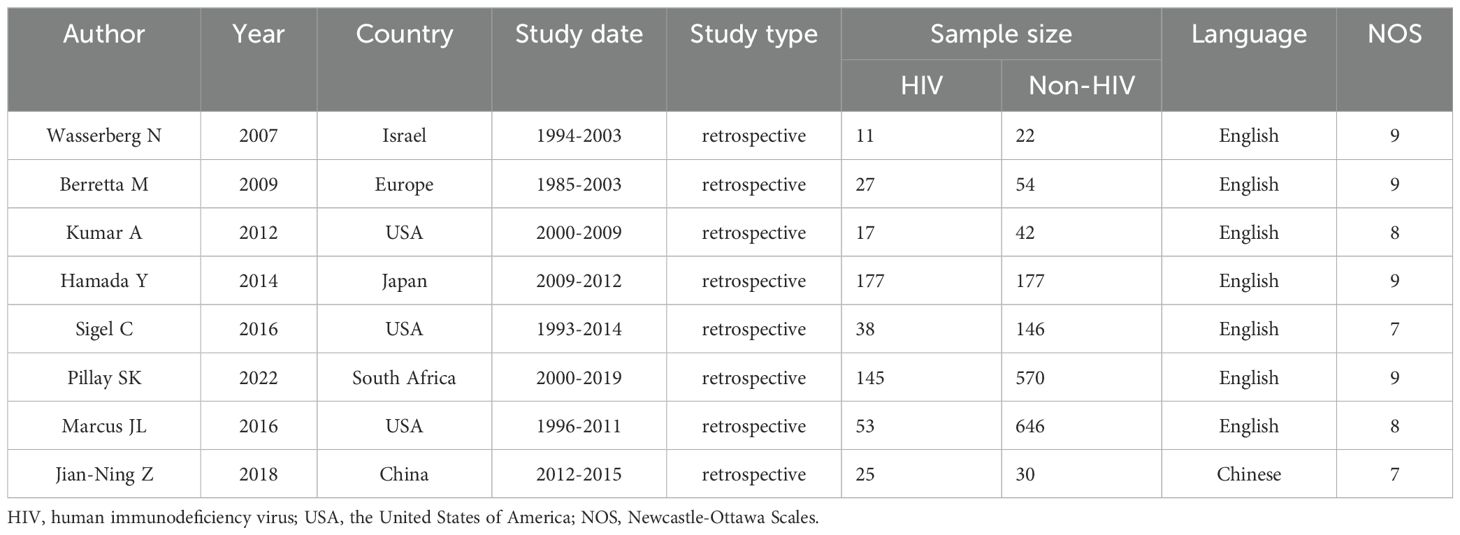
Table 1. Baseline characteristics of included studies.
3.3 Baseline characteristics of the included patients
In terms of the patients’ baseline characteristics, we pooled up age, sex, tumor stage, tumor grade, and tumor location. After data analysis, there were significant differences in sex (OR=0.69, 95% CI=0.49 to 0.98, I2 = 22.6%, P=0.04<0.1), tumor grade (OR=6.61, 95% CI=2.36 to 2.24, I2 = 0.00%, P=0.00<0.1), and tumor location (OR=2.19, 95% CI=1.74 to 2.77, I2 = 0.04%, P=0.00<0.1) between the HIV and non-HIV groups. Age (MD=-0.49, 95% CI=-1.43 to 0.69, I2 = 98.33%, P=0.49>0.1) and tumor stage (OR=1.23, 95% CI=0.68 to 2.24, I2 = 51.57%, P=0.49>0.1) were not statistically different between the two groups (Table 2).
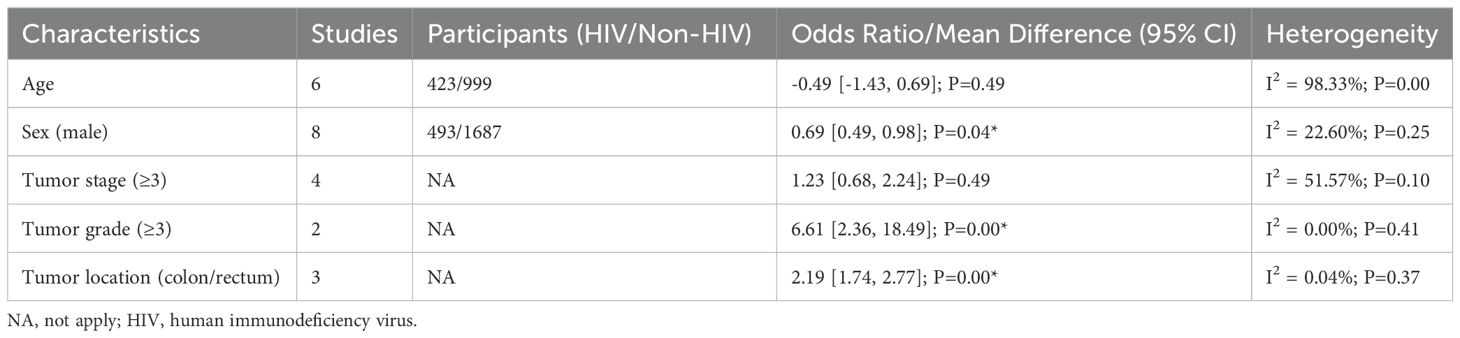
Table 2. Baseline information of the patients in the HIV and non-HIV groups.
3.4 OS of the patients
According to our data analysis, we found that HIV was associated with worse OS in CRC patients (HR=3.12, 95% CI=2.07 to 4.69, I2 = 52.51%, P=0.00<0.1) (Figure 2).
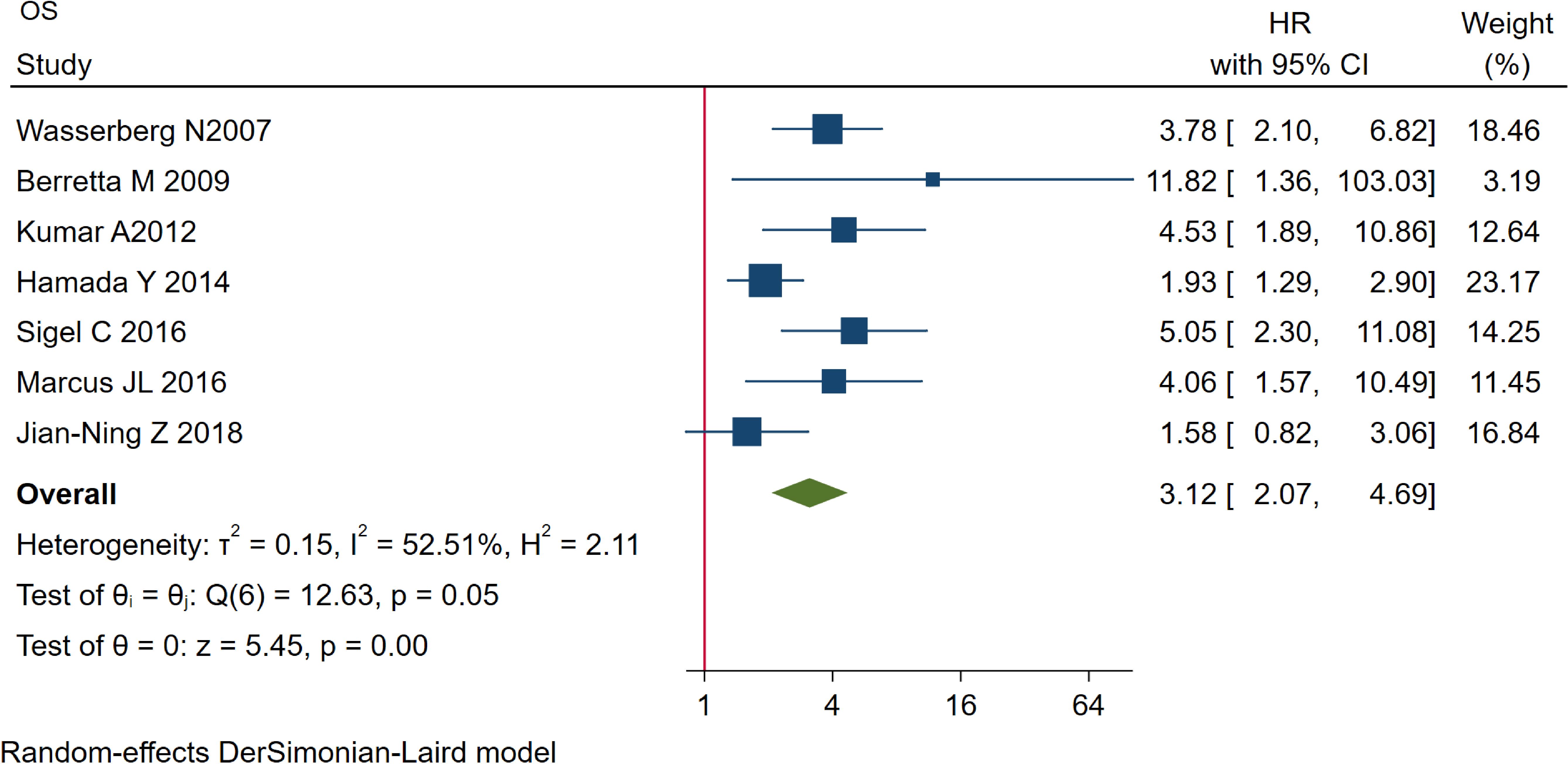
Figure 2. Comparison of OS between the two groups. OS, overall survival.
3.5 Funnel plot
Funnel plot was used to assess publication bias. According to the funnel plot, which showed symmetry, suggesting that there was no significant publication bias in the included studies. Symmetry in the plot typically indicated that the studies were evenly distributed around the effect estimate, supporting the reliability and generalizability of the results (Figure 3).
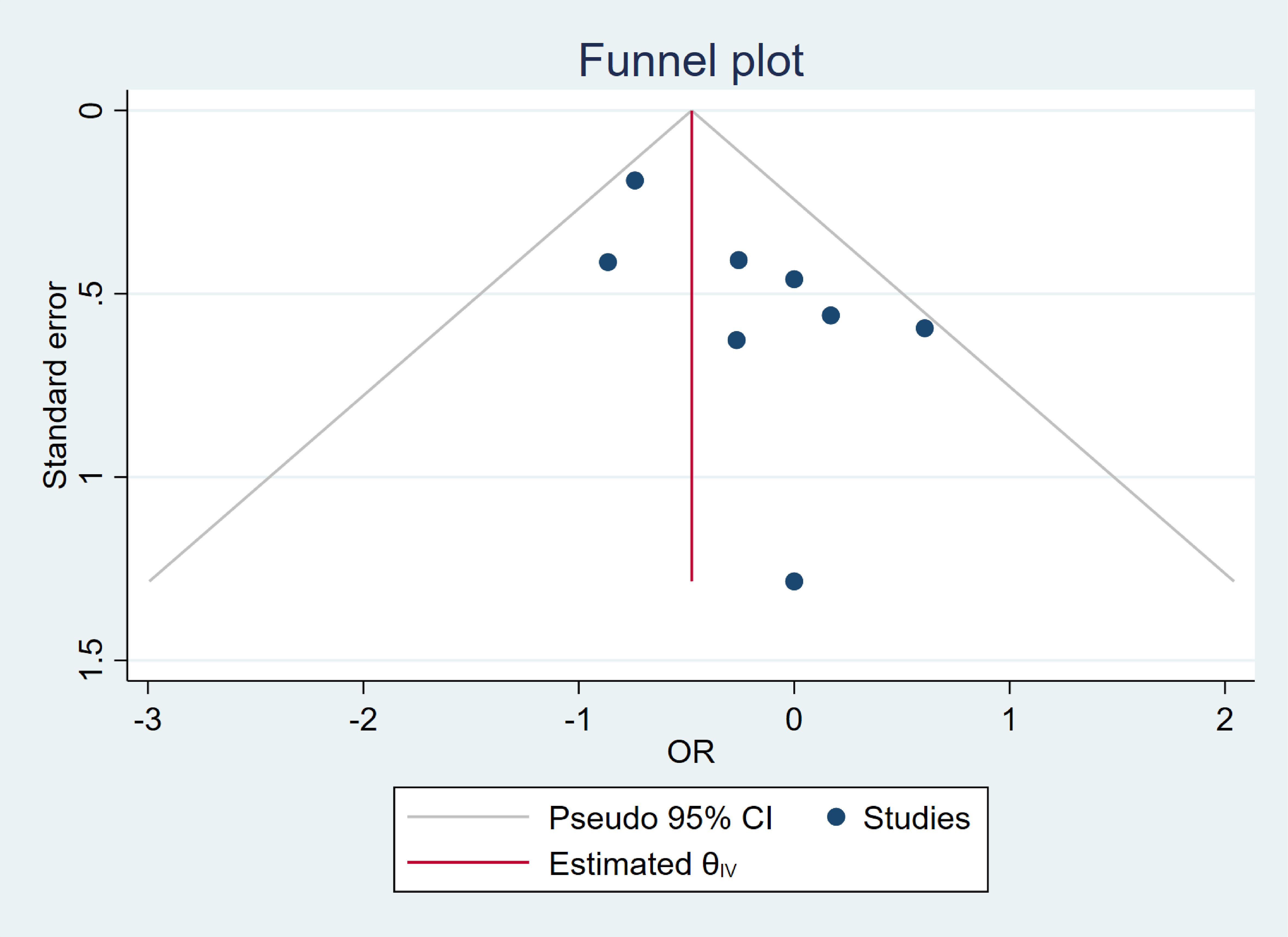
Figure 3. Funnel plot of overall complications.
3.6 Sensitivity analysis
We analyzed sensitivity by excluding each study one at a time. There were no significant differences in the results after each analysis was performed (Figure 4).
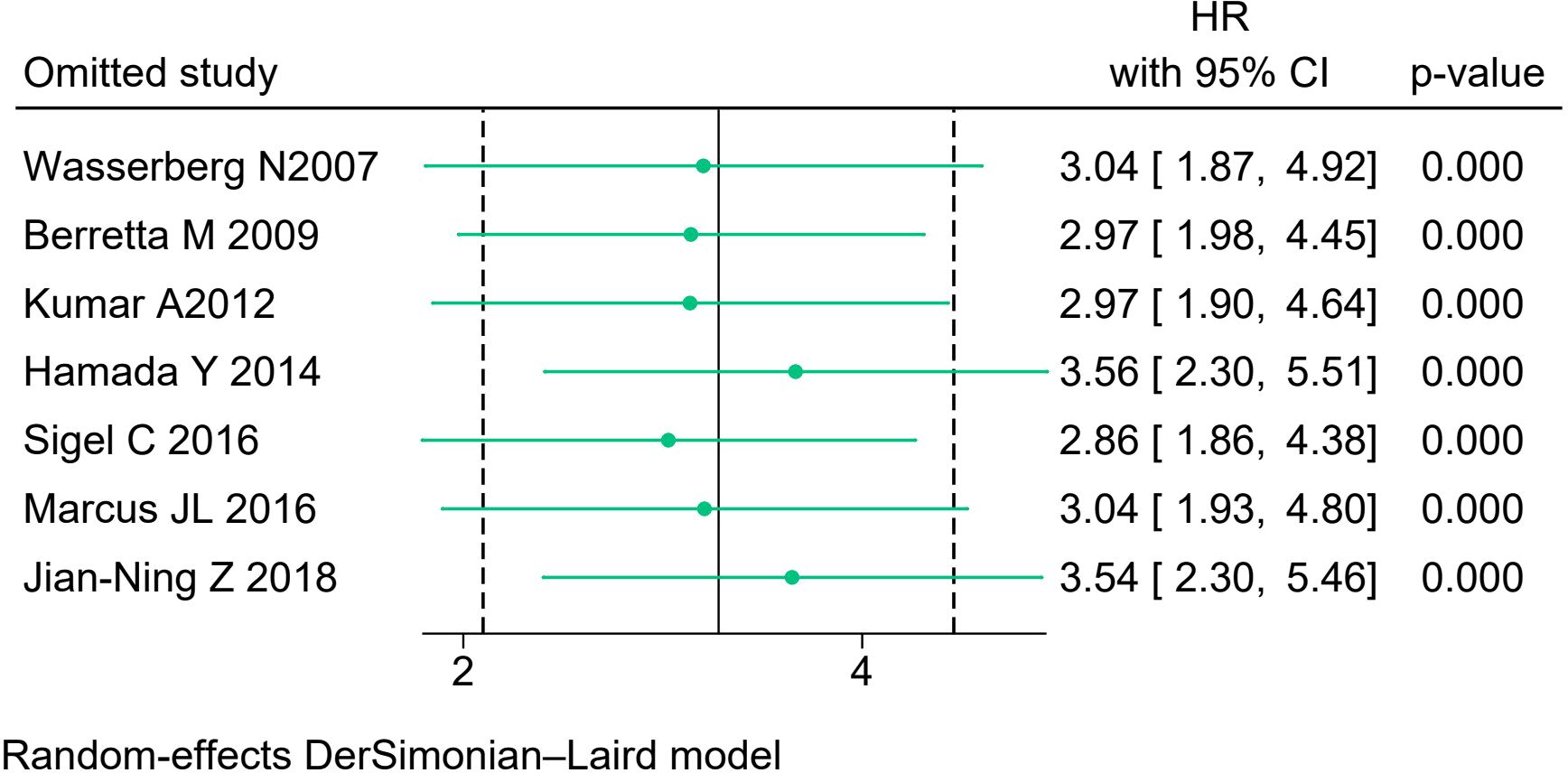
Figure 4. Sensitivity analysis.
4 Discussion
A total of eight studies including 2180 patients were enrolled in this current study. We pooled up baseline information and prognosis of the included patients. After pooling up the data, we found the HIV group had less males, a higher tumor grade and a higher proportion of colon cancer. Moreover, the HIV group had a worse OS than the non-HIV group, however, the heterogeneity was not low and which needed to be considered.
The survival of HIV-infected patients was prolonged in the HAART era, and many HIV-positive CRC patients required radical surgery (27–30). Clinical practice shown that surgical trauma or stress response could affect the immune function of the patient’s body, stimulate the immune system in mild cases and strengthen the immunity of the body, but produce immunosuppression in severe cases and trigger the development of opportunistic infections such as bacteria, tuberculosis, fungi, and viruses. The higher HIV-RNA, the higher infectiousness, and the lower CD4+ count, the higher the risk of opportunistic infection (31). This could increase the incidence of postoperative complications and morbidity and mortality to some extent.
The researchers focused on finding out the impact of HIV on CRC patients after surgery. However, there was still a controversy. Some studies did not find a significant impact of HIV on OS in CRC patients (17–21). In their respective studies, Berretta M and Sigel C et al. showed that patients with HIV-infected CRC had a worse OS after surgery than the general CRC patients (15, 16). Previous studies have reported the survival in HIV-positive CRC patients, however, this meta-analysis is the first to specifically focus on CRC.
In this current study, the outcome revealed that HIV-infected patients had a worse OS in CRC patients after surgery, however, the heterogeneity of the results was not low and needs to be taken into consideration. Similarly, previous studies found a reduction in OS in HIV-associated cancers, such as malignant melanoma, other skin cancers, head and neck tumors, and lung cancer (32–35). The mechanisms of HIV altered clinical course of these malignancies were unclear. In acquired immunodeficiency syndrome (AIDS)-associated cancers (so-called AIDS-defining malignancies), most of the pathogenesis was virus-related, with impaired viral immunity being the cause of persistent viral pathogens. In the case of non-AIDS-defining malignancies, aggressive tumor behavior might be associated with an altered host immune response in immunosuppressed patients. Two epidemiological studies shown an association between advanced immunosuppression associated with HIV disease progression and non-AIDS-defining malignancies (36, 37).
Moreover, a study found low CD4 counts were associated with early recurrence in HIV-positive malignant melanoma patients (38). In contrast, when comparing AIDS to cancer registries, Mbretier et al. did not find an association between CD4 counts and non-AIDS defining cancers in over 82,000 patients (39). CD4 T cells were central to antitumor immunity, as they regulate immune surveillance and coordinate the cytotoxic response against malignant cells. Chronic immune suppression, as seen in HIV-positive individuals, could potentially compromise these mechanisms, leading to worse outcomes in certain cancers. At present, the current study found no correlation between CD4 counts and CRC occurrence, as all patients had relatively high CD4 counts at the time of CRC diagnosis (17). This finding may reflect effective antiretroviral therapy (ART) in maintaining immune function, which could mitigate the impact of CD4 count depletion. However, it is worth exploring whether variations in CD4 counts, particularly during different stages of HIV infection or treatment, might influence CRC prognosis or response to therapy. Future research could focus on longitudinal studies to better elucidate the dynamic interplay between immune status and CRC outcomes in HIV-positive populations.
We also found that the HIV group had more colon cancer. This was consistent with previous study (40). The HIV group had a higher tumor grade than the non-HIV group. High tumor grade might mean high aggressiveness and greater potential for metastasis. This could also be one of the reasons why the HIV group had a worse OS, but more studies were needed to prove this.
To our best knowledge, this study was the first study to pool up the prognosis in HIV-infected CRC patients in previous studies. However, there were some limitations of this pooling up analysis. First, most of these studies focused on Europe, which might cause selection bias; Second, insufficiency of the patient’s baseline information; Third, missing other factors on OS; Fourth, the results was moderate heterogeneity with no clear source of heterogeneity, however, there was insufficient data to perform a subgroup analysis. Therefore, more and more detailed research on this is needed in the future.
5 Conclusion
Patients with HIV-infected CRC have a worse prognosis than the general CRC patient. As people living with HIV live longer, these patients should also receive more attention.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
W-WY: Conceptualization, Writing – original draft. XZ: Data curation, Methodology, Software, Writing – review & editing. GH: Data curation, Methodology, Software, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We acknowledged to all the authors in this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found onlineat: https://www.frontiersin.org/articles/10.3389/fonc.2025.1440105/full#supplementary-material
References
1. Siripurapu R, Ota Y. Human immunodeficiency virus: opportunistic infections and beyond. Neuroimaging Clin N Am. (2023) 33:147–65. doi: 10.1016/j.nic.2022.07.014
2. Onwumeh J, Okwundu CI, Kredo T. Interleukin-2 as an adjunct to antiretroviral therapy for HIV-positive adults. Cochrane Database Syst Rev. (2017) 5:CD009818. doi: 10.1002/14651858.CD009818.pub2
3. Zhao Y, Wu Z, McGoogan JM, Shi CX, Li A, Dou Z, et al. Immediate antiretroviral therapy decreases mortality among patients with high CD4 counts in China: A nationwide, retrospective cohort study. Clin Infect Dis. (2018) 66:727–34. doi: 10.1093/cid/cix878
4. Trickey A, McGinnis K, Gill MJ, Abgrall S, Berenguer J, Wyen C, et al. Longitudinal trends in causes of death among adults with HIV on antiretroviral therapy in Europe and North America from 1996 to 2020: a collaboration of cohort studies. Lancet HIV. (2024) 11:e176–85. doi: 10.1016/S2352-3018(23)00272-2
5. Rudek MA, Flexner C, Ambinder RF. Use of antineoplastic agents in patients with cancer who have HIV/AIDS. Lancet Oncol. (2011) 12:905–12. doi: 10.1016/S1470-2045(11)70056-0
6. Patel P, Hanson DL, Sullivan PS, Novak RM, Moorman AC, Tong TC, et al. Adult and Adolescent Spectrum of Disease Project and HIV Outpatient Study Investigators. Incidence of types of cancer among HIV-infected persons compared with the general population in the United States, 1992-2003. Ann Intern Med. (2008) 148:728–36. doi: 10.7326/0003-4819-148-10-200805200-00005
7. Liu F, Peng D, Liu XY, Liu XR, Li ZW, Wei ZQ, et al. The effect of carbon nanoparticles staining on lymph node tracking in colorectal cancer: A propensity score matching analysis. Front Surg. (2023) 10:1113659. doi: 10.3389/fsurg.2023.1113659
8. Liu XY, Kang B, Cheng YX, Yuan C, Tao W, Zhang B, et al. Higher body mass index was associated with better prognosis in diabetic patients with stage II colorectal cancer. BMC Cancer. (2022) 22:596. doi: 10.1186/s12885-022-09691-1
9. Cheng Y, Cheng YX, Liu XY, Kang B, Tao W, Peng D. The effect of type 2 diabetes mellitus on the short-term outcomes and prognosis of stage I-III colorectal cancer: A propensity score matching analysis. Cancer Manag Res. (2022) 14:205–14. doi: 10.2147/CMAR.S347242
10. Cheng YX, Tao W, Liu XY, Yuan C, Zhang B, Wei ZQ, et al. Hypertension remission after colorectal cancer surgery: A single-center retrospective study. Nutr Cancer. (2022) 74:2789–95. doi: 10.1080/01635581.2021.2025256
11. Liu XY, Kang B, Cheng YX, Yuan C, Tao W, Zhang B, et al. The short-term and oncologic outcomes of younger VS older colorectal cancer patients undergoing primary surgery: a propensity score matching analysis. BMC Cancer. (2022) 22:153. doi: 10.1186/s12885-022-09246-4
12. Pambou HOT, Gagneux-Brunon A, Fossi BT, Roche F, Guyot J, Botelho-Nevers E, et al. Assessment of cardiovascular risk factors among HIV-infected patients aged 50 years and older in Cameroon. AIMS Public Health. (2022) 9:490–505. doi: 10.3934/publichealth.2022034
13. Bini EJ, Green B, Poles MA. Screening colonoscopy for the detection of neoplastic lesions in asymptomatic HIV-infected subjects. Gut. (2009) 58:1129–34. doi: 10.1136/gut.2008.165985
14. Kothari ND, Engelson ES, Drake V, Mehdi A, Ionescu G, Kotler DP. Effect of HIV infection on the prevalence of colorectal adenomas during screening colonoscopy. J Clin Gastroenterol. (2010) 44:77–8. doi: 10.1097/MCG.0b013e3181a1f5b5
15. Berretta M, Cappellani A, Di Benedetto F, Lleshi A, Talamini R, Canzonieri V, et al. Clinical presentation and outcome of colorectal cancer in HIV-positive patients: a clinical case-control study. Onkologie. (2009) 32:319–24. doi: 10.1159/000215719
16. Sigel C, Cavalcanti MS, Daniel T, Vakiani E, Shia J, Sigel K. Clinicopathologic features of colorectal carcinoma in HIV-positive patients. Cancer Epidemiol Biomarkers Prev. (2016) 25:1098–104. doi: 10.1158/1055-9965.EPI-15-1179
17. Wasserberg N, Nunoo-Mensah JW, Gonzalez-Ruiz C, Beart RW Jr, Kaiser AM. Colorectal cancer in HIV-infected patients: a case control study. Int J Colorectal Dis. (2007) 22:1217–21. doi: 10.1007/s00384-007-0285-z
18. Kumar A, Shah N, Modi Y, Shaaban HS, DePasquale J, DeBari VA, et al. Characteristics of colorectal cancer in the human immunodeficiency virus-infected African American population. Med Oncol. (2012) 29:1773–9. doi: 10.1007/s12032-011-0015-9
19. Hamada Y, Nagata N, Nishijima T, Shimbo T, Asayama N, Kishida Y, et al. Impact of HIV infection on colorectal tumors: a prospective colonoscopic study of Asian patients. J Acquir Immune Defic Syndr. (2014) 65:312–7. doi: 10.1097/QAI.0000000000000016
20. Marcus JL, Chao C, Leyden WA, Xu L, Yu J, Horberg MA, et al. Survival among HIV-infected and HIV-uninfected individuals with common non-AIDS-defining cancers. Cancer Epidemiol Biomarkers Prev. (2015) 24:1167–73. doi: 10.1158/1055-9965.EPI-14-1079
21. Deng JN, Deng SH, Li ZW, Wu JW. Feasibility analysis of laparoscopic total rectal mesorectal resection for the treatment of AIDS combined with low-grade rectal cancer. Infection International(Electronic Edition). (2018) 7:1–3.
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffman TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J Clin Epidemiol. (2021) 134:178–89. doi: 10.1016/j.jclinepi.2021.03.001
23. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
24. Ioannidis JP. Interpretation of tests of heterogeneity and bias in meta-analysis. J Eval Clin Pract. (2008) 14:951–7. doi: 10.1111/j.1365-2753.2008.00986.x
25. Siddaway AP, Wood AM, Hedges LV. How to do a systematic review: A best practice guide for conducting and reporting narrative reviews, meta-analyses, and meta-syntheses. Annu Rev Psychol. (2019) 70:747–70. doi: 10.1146/annurev-psych-010418-102803
26. Pillay SK, Moolla Z, Moodley Y, Madiba TE. Quantifying the relationship of HIV infection with clinicopathological spectrum and outcome among patients with colorectal cancer in a South African population. Afr Health Sci. (2022) 22:27–36. doi: 10.4314/ahs.v22i2.4
27. Pinzone MR, Fiorica F, Di Rosa M, Malaguarnera G, Malaguarnera L, Cacopardo B, et al. Non-AIDS-defining cancers among HIV-infected people. Eur Rev Med Pharmacol Sci. (2012) 16:1377–88.
28. Ke S, Fang Q, Lan J, Qiao N, Zhang X, Xie C, et al. Survival times of HIV/AIDS in different AIDS Diagnostic and Treatment Guidelines from 2006 to 2020 in Liuzhou, China. BMC Public Health. (2023) 23:1745. doi: 10.1186/s12889-023-15662-3
29. Gao TY, Zhao LK, Liu X, Li HY, Ma YT, Fang W, et al. Disease burden of AIDS in last 30-year period and its predicted level in next 25-years based on the global burden disease 2019. BMC Public Health. (2024) 24:2384. doi: 10.1186/s12889-024-19934-4
30. Poorolajal J, Hooshmand E, Mahjub H, Esmailnasab N, Jenabi E. Survival rate of AIDS disease and mortality in HIV-infected patients: a meta-analysis. Public Health. (2016) 139:3–12. doi: 10.1016/j.puhe.2016.05.004
31. Lam JO, Hurley LB, Udaltsova N, Alexeeff SE, Klein DB, Corley DA, et al. Colorectal cancer screening in people with and without HIV in an integrated health care setting. J Acquir Immune Defic Syndr. (2019) 81:284–91. doi: 10.1097/QAI.0000000000002024
32. Facciolà A, Venanzi Rullo E, Ceccarelli M, D'Andrea F, Coco M, Micali C, et al. Malignant melanoma in HIV: Epidemiology, pathogenesis, and management. Dermatol Ther. (2020) 33:e13180. doi: 10.1111/dth.13180
33. Shields CL, Ramasubramanian A, Mellen PL, Shields JA. Conjunctival squamous cell carcinoma arising in immunosuppressed patients (organ transplant, human immunodeficiency virus infection). Ophthalmology. (2011) 118:2133–2137.e1. doi: 10.1016/j.ophtha.2011.04.001
34. Borsetto D, Fussey J, Fabris L, Bandolin L, Gaudioso P, Phillips V, et al. HCV infection and the risk of head and neck cancer: A meta-analysis. Oral Oncol. (2020) 109:104869. doi: 10.1016/j.oraloncology.2020.104869
35. Mani D, Haigentz M Jr, Aboulafia DM. Lung cancer in HIV infection. Clin Lung Cancer. (2012) 13:6–13. doi: 10.1016/j.cllc.2011.05.005
36. Zhou Z, Liu H, Yang Y, Zhou J, Zhao L, Chen H, et al. The five major autoimmune diseases increase the risk of cancer: epidemiological data from a large-scale cohort study in China. Cancer Commun (Lond). (2022) 42:435–46. doi: 10.1002/cac2.12283
37. Tuano KS, Seth N, Chinen J. Secondary immunodeficiencies: An overview. Ann Allergy Asthma Immunol. (2021) 127:617–26. doi: 10.1016/j.anai.2021.08.413
38. Carpenter EL, Mick R, Rech AJ, Beatty GL, Colligon TA, Rosenfeld MR, et al. Collapse of the CD27+ B-cell compartment associated with systemic plasmacytosis in patients with advanced melanoma and other cancers. Clin Cancer Res. (2009) 15:4277–87. doi: 10.1158/1078-0432.CCR-09-0537
39. Chammartin F, Mocroft A, Egle A, Zangerle R, Smith C, Mussini C, et al. Measures of longitudinal immune dysfunction and risk of AIDS and non-AIDS defining Malignancies in antiretroviral-treated people with human immunodeficiency virus. Clin Infect Dis. (2024) 78:995–1004. doi: 10.1093/cid/ciad671
Keywords: HIV, colorectal cancer, surgery, overall survival, infection
Citation: Yang W-W, Zhou X and He G (2025) Patients with colorectal cancer combined with HIV had a worse overall survival after surgery: a meta-analysis. Front. Oncol. 15:1440105. doi: 10.3389/fonc.2025.1440105
Received: 29 May 2024; Accepted: 10 January 2025;
Published: 29 January 2025.
Edited by:
DeGaulle I. Chigbu, Salus at Drexel University, United StatesReviewed by:
Bhargavi Posinasetty, Prometrika, LLC, United StatesMiriam Onwuliri, NHS England, United Kingdom
Copyright © 2025 Yang, Zhou and He. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gan He, aGVnYW41MjcyNUAxNjMuY29t