 Denisse Castro-Uriol1,2*
Denisse Castro-Uriol1,2* Juana Vera3
Juana Vera3 Bryan Valcarcel4
Bryan Valcarcel4 Marco López-Ilasaca5
Marco López-Ilasaca5 Alejandro Yabar3
Alejandro Yabar3 Anaís Cámara1
Anaís Cámara1 Luis Malpica6
Luis Malpica6 Brady Beltrán1,2
Brady Beltrán1,2- 1Departamento de Oncología y Radioterapia, Hospital Nacional Edgardo Rebagliati Martins, EsSalud, Lima, Peru
- 2Centro de Investigación de Medicina de Precisión, Universidad de San Martin de Porres, Lima, Peru
- 3Departmento de Anatomía Patológica, Hospital Nacional Edgardo Rebagliati Martins, EsSalud, Lima, Peru
- 4Department of Epidemiology, Milken Institute School of Public Health, The George Washington University, Washington, DC, United States
- 5Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, United States
- 6Department of Lymphoma and Myeloma, The University of Texas MD Anderson Cancer Center, Houston, TX, United States
Introduction: Epstein-Barr virus (EBV) infection has been linked to cervical cancer (CC), but few have described the clinical and outcome features of patients with CC and EBV infection.
Methods: We conducted a single-center matched cohort study on 94 patients with CC. Real-time Polymerase chain reaction (RT-PCR) was used to detect EBNA-1 (Epstein-Barr nuclear antigen 1) and LMP-1 (Latent membrane protein 1). We used Kaplan-Meier and Cox regression analysis to evaluate the effect of EBV infection on overall survival (OS) and progression-free survival (PFS). Females with a positive EBV status were matched to those without infection using a propensity score.
Results: Of the 94 patients in our cohort, 21 (22%) had a positive EBV status. Before and after matching, there were no differences in baseline clinical and sociodemographic features between patients diagnosed with CC with and without EBV infection. Most patients received concurrent chemoradiotherapy (73%) as frontline treatment. With a median follow-up of 67 months, the 5-year OS was 42% (95% CI: 33–55%) and the 5-year PFS was 37% (95% CI: 37–49%) in the entire population. Patients with EBV-positive status had comparable 5-year OS (50% vs. 37%, p-value=0.490; Hazard Ratio [HR] 0.77, 95% CI 0.36-1.62) and 5-year PFS (44% vs. 37%, p-value=0.750; HR 0.89, 95% CI 0.43-1.83) to those with EBV-negative CC, respectively.
Conclusion: Females with CC and EBV infection have similar clinical features and outcomes compared to those without EBV infection.
1 Introduction
Cervical cancer (CC) is the fourth most common cause of cancer-related deaths among women and the fourth leading cause of death worldwide (1). Despite global advances, survival outcomes in Peru remain notably worse than those in Western countries (2–4). A previous Peruvian study found that locally advanced CC was the most common stage at presentation and was associated with poor outcomes, indicating that additional factors may be contributing to the unfavorable prognosis (4). This survival difference is generally associated with limited access to cancer care, resulting in a higher proportion of patients presenting with advanced-stage disease at diagnosis (4, 5). However, it is unclear whether other factors, such as environmental influences, including Epstein-Barr virus (EBV) infection, also contribute to these poor outcomes.
EBV-related cancers are more prevalent in Latin America than in other regions, with Peru showing one of the highest rates (6). EBV infection has been recognized as a prognostic factor in several cancers, though its impact on survival remains inconsistent across studies (7). In solid tumors, EBV-associated gastric carcinoma and nasopharyngeal carcinoma have generally been linked to favorable outcomes (8, 9). In contrast, EBV positivity in hematologic malignancies, such as diffuse large B-cell lymphoma treated with chemotherapy alone (10), natural killer/T-cell lymphomas (11), and EBV-positive recipients after allogeneic transplantation (12), have been associated with poorer survival. Our group recently reported the largest cohort of EBV-positive Diffuse large B-cell lymphoma in Latin America, demonstrating unfavorable clinical features but no significant survival differences when rituximab was incorporated into chemotherapy regimens (13). The influence of EBV on CC outcomes, however, remains largely unexplored.
Preclinical studies suggest that EBV may enhance and accelerate the integration of Human papillomavirus (HPV), thereby promoting tumor progression in cervical cancer and highlighting a possible synergistic interaction between these two oncogenic viruses (14). Yet, whether EBV infection leads to worse outcomes in locally advanced CC patients remains uncertain. A single-center study from China found no significant survival differences between EBV-positive and EBV-negative CC patients (15). However, this study focused predominantly on EBV prevalence, infection patterns, and certain pathological and immunological features without a detailed examination of key patient characteristics, treatment modalities, or comparative survival outcomes. Additionally, the study included a broader population, of which locally advanced cases were a minority. Herein, we aim to fill this gap by comprehensively characterizing the sociodemographic and clinical features, treatment approaches, and survival outcomes of CC patients with and without EBV infection in an endemic setting.
2 Materials and methods
2.1 Study design and population
We conducted a retrospective cohort study of adult females diagnosed with CC between December 2013 and June 2014, with follow-up through July 2019. The patients were identified using the Department of Oncology and Radiotherapy database of the Hospital Edgardo Rebagliati Martins in Lima, Peru. Medical records were manually reviewed, and data abstracted from August to September 2019 in a secured database. Inclusion criteria: females aged ≥18 years; cancer stage IIB, IIIA, or IIIB; and anatomopathological diagnosis of squamous cell carcinoma. We excluded those treated at outside healthcare centers, patients without medical records (lost or destroyed), patients with incomplete or insufficient data for pathological characterization, insufficient cervical tissue samples for real-time polymerase chain reaction (RT-PCR), and untreated patients or those who received non-platinum-based chemotherapy (n=95) with no intention to cure. The Institutional Review Board and Ethics Committee of the Hospital Edgardo Rebagliati Martins-EsSalud approved the conduction of this study.
2.2 Study variables
Baseline demographic and clinical features were abstracted at CC diagnosis. EBV positivity was defined as a positive result for the expression of Epstein-Barr nuclear antigen 1 (EBNA-1) (16) or latent membrane protein 1 (LMP-1) (17). Conversely, EBV negativity was defined as negative results for expressing EBNA-1 and LMP-1. We collected data regarding the following sociodemographic and clinical covariates: age; parity; performance status; complete blood cell count (i.e., absolute leukocyte count, neutrophils, lymphocytes, monocytes, and platelets); red blood cell distribution width coefficient of variations and red blood cell distribution width standard deviation; serum albumin; clinical stage of CC; and frontline treatment received such as chemoradiotherapy (CRT) or radiotherapy (RT) only. Parity was classified as nulliparous (never given birth), primiparous (given birth once), and multiparous (given birth two or more times). Performance status was measured using the Eastern Cooperative Oncology Group (ECOG) scale. For CC staging, we used the Fédération Internationale de Gynécologie et d’Obstétrique staging system (18).
2.3 EBV analysis
Tissue specimens were obtained through an incisional biopsy of the cervical tumor site. They were routinely fixed in formalin and embedded in paraffin. The samples were stored in the hospital archives until subsequent analysis. Genomic DNA was purified from paraffin-embedded tissue sections. The following primers were used for RT-PCR: EBNA-1 Forward 5'-TACAGGACCTGGAAATGGCC-3' and Reverse 5'-TCTTTGAGGT CCACT GC CG-3'; LMP-1 Forward 5'-CAGTCAGGCAAGCCTATGA-3' and Reverse 5'-CTGGTT CCGGTGG AGATGA-3'. Additionally, the human β-actin gene (Forward: 5'- ATCATGTTTGAGACCTTCAACAC-3' and Reverse: 5'- CATCTCTTGCTCGAAGTCCAG-3') was used as an internal control for the presence of intact genomic DNA. A sample was considered EBV-positive when the fluorescence amplification curves were recorded by the thermal cycler as positive against EBNA-1 and LMP-1.
2.4 Data analysis
Continuous variables were compared with a two-sample t-test or the Wilcoxon rank-sum test, as appropriate. We used the χ-squared test or Fisher’s exact test as appropriate for categorical variables. The median follow-up time was computed using the reverse Kaplan–Meier method. Our endpoints were overall survival (OS) and progression-free survival (PFS). OS was defined as the time (in months) from CC diagnosis until death from any cause, while PFS was determined from diagnosis until recurrence, death from any reason, or loss to follow-up, whichever comes first. Survival probabilities were estimated using the Kaplan-Meier method, and the curves were compared using the log-rank test.
The effect of EBV on OS and PFS was initially evaluated in multivariable Cox regression models, adjusting for age, parity, performance status, and cancer stage. To further reduce confounding, we matched females with EBV infection with those without infection using propensity score matching and a ratio of 2:1. We used the nearest neighborhood approach for the propensity score. The matched variables had an optimal standard mean difference: age (SMD=0.05), year of diagnosis (SMD=0.07), performance status (SMD=0.1), cancer stage (SMD=0.1), and frontline treatment (SMD=0.1). Subgroup analyses compared the effect of EBV on survival outcomes within the frontline treatment received (CRT or RT alone). Analyses are reported with hazard ratios (HRs) and 95% confidence intervals (CI). Analyses were performed in R using the packages “tidyverse,” “survival,” “survminer,” “MatchIt, “ and “ggplot2”.
3 Results
3.1 Patient characteristics
A total of 189 patients were assessed for eligibility, of whom 94 (49.7%) met the inclusion criteria. Patient characteristics at diagnosis are summarized in Table 1. The median age was 55 years. Most patients had ECOG 0–1 (70%), were multiparous (74%), and had clinical stage IIB (64%). A total of 21 (22.3%) patients had an EBV-positive status at CC diagnosis. According to frontline treatment, the majority received concurrent CRT (73%) compared to RT alone (27%).

Table 1. Clinical and treatment characteristics of patients with CC by EBV status before and after matching.
3.2 Clinicopathological differences by EBV status
Before and after matching, there were no differences in baseline clinical and sociodemographic features between patients diagnosed with CC with and without EBV infection. CC patients with EBV infection tended to be younger (p-value=0.740), multiparous (p-value=0.3), exhibited ECOG scores of 2-3 (p-value=0.137), and were more likely to be in more advanced clinical stage (stages IIIA/B, p-value=0.469) compared to those without EBV infection (Table 1), but these findings were not statistically significant.
3.3 Survival outcomes
The median follow-up was 67 months (95% CI: 56.0-66.9) in the entire cohort. The 5-year OS was 42% (95% CI: 33–55%) and the 5-year PFS was 37% (95% CI: 27–49%). In the unmatched cohort, EBV positivity showed similar outcomes in OS (5-year OS: 47% vs. 40%, p-value=0.780; adjusted HR [aHR] 0.85, 95% CI: 0.43-1.69), and PFS (5-year PFS: 42% vs. 34%, p-value=0.720; aHR 0.83, 95% CI: 0.43-1.60) compared to EBV negativity. Likewise, in the matched cohort, we identified that patients with CC and EBV infection had similar OS (5-year OS: 50% vs. 37%, p-value=0.490; aHR 0.77, 95% CI: 0.36-1.62) and PFS (5-year PFS: 44% vs. 37%, p-value=0.750; aHR 0.89, 95% CI: 0.43-1.83) compared to those without a positive EBV status (Figure 1, Table 2).
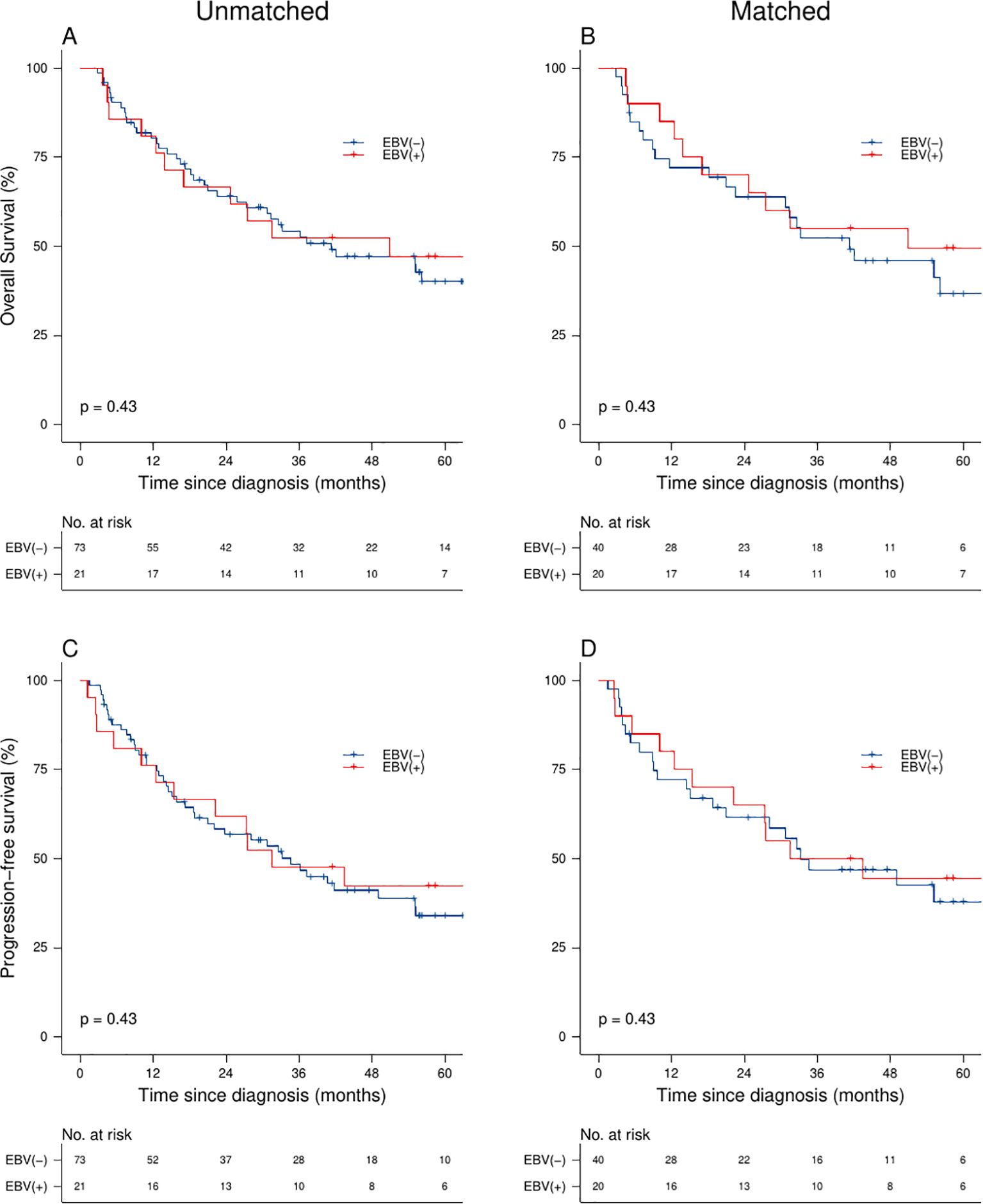
Figure 1. Survival analysis of CC patients: Overall survival (A, B) and progression-free survival (C, D) stratified by EBV status and matched cohort analysis.
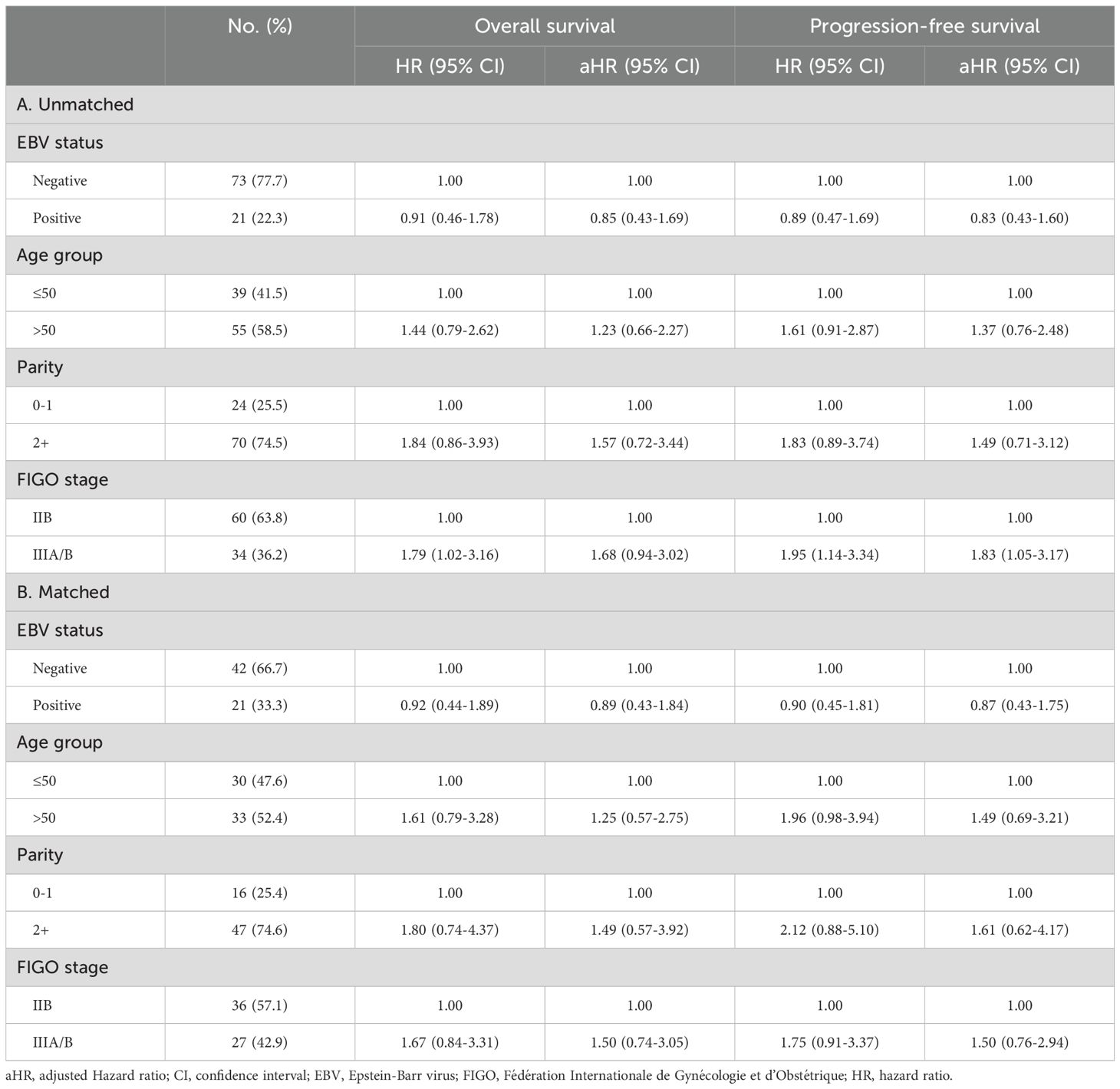
Table 2. Cox regression analyses of the effect of EBV status on the OS and PFS among patients with CC (A) before and (B) after matching.
In a subgroup analysis, the 5-year OS rates were 34% (95% CI: 19-60%) for RT and 45% (95% CI: 34-60%) for CRT, with a p-value of 0.121. The 5-year PFS rates were 26% (95% CI: 13-52%) for RT and 40% (95% CI: 29-56%) for CRT, with a p-value of 0.069. We did not identify differences in OS and PFS between patients with CC with and without EBV infection who received either CRT (5-year OS: 61% vs. 39%, p-value=0.360; and 5-year PFS: 61% vs. 40%, p-value=0.390) or RT (5-year OS: 29% vs. 31%, p-value=0.760; and 5-year PFS: 14% vs. 31%, p-value=0.840) as a frontline treatment (Figure 2).
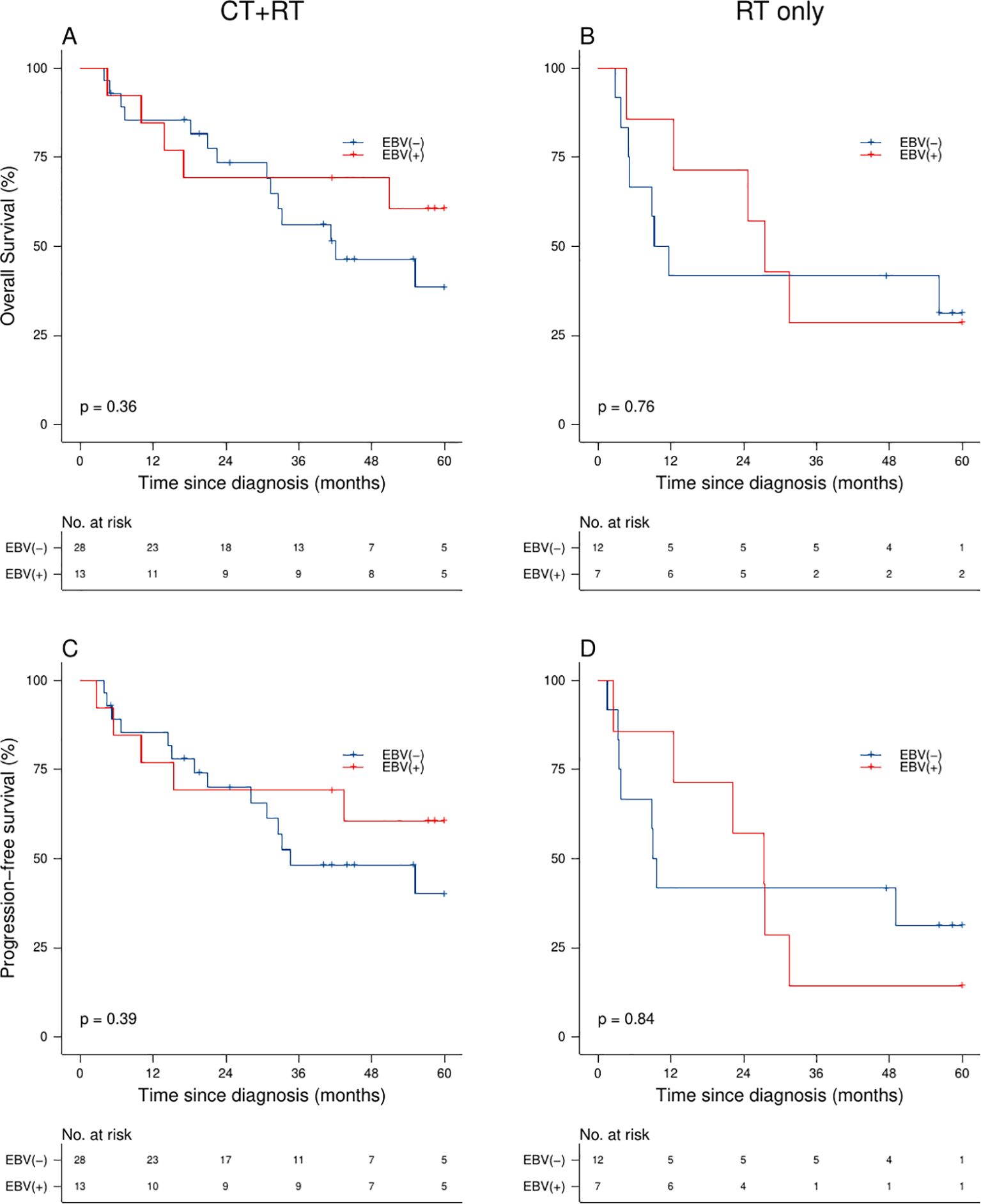
Figure 2. Survival analysis of CC patients: Overall survival (A, B) and progression-free survival (C, D) stratified by EBV status and frontline treatment modality.
4 Discussion
This study is among the first to comprehensively explore the impact of EBV infection on survival in women with CC living in an endemic Latin American country like Peru. We observed no significant differences in clinical features or survival outcomes between patients diagnosed with CC with and without EBV infection.
Although we were unable to find a prognostic role for EBV, existing evidence supports that EBV plays an important role in tumor progression in HPV-related CC (14). A meta-analysis of retrospective studies from Asia, Europe, Africa, and Latin America found differences in the rates of EBV infection among cervical lesions. The highest prevalence was observed in carcinoma cases (43.6%), compared to preinvasive disease (cervical intraepithelial neoplasia grade 1: 23%, and cervical intraepithelial neoplasia grade 2 and 3: 34%) and normal cervical samples (19%) (19). Notably, Latin America had the highest EBV prevalence among carcinoma cases (62%) (19). The most representative study from the meta-analysis was conducted in Brazil, where 169 CC cases were examined. They found that EBV was higher in CC (64.2%) compared to high-grade lesions (21.1%) and normal cervical samples (8.9%) (20). Similarly, a recent study of Chinese women with CC reported an EBV prevalence of 20.2% (15). These findings indicate that patients with EBV infection have a higher frequency of carcinoma than those without EBV infection and likely suggest that the prevalence of EBV may differ by region, with Latin America exhibiting one of the highest percentages.
Our study did not show significant differences in clinical features or frontline treatment approaches between patients with and without EBV infection. Interestingly, although our population differed from that of Zuo et al., who included a broad range of patients with both early and advanced clinical stages of CC, their findings showed that patients with EBV infection and CC had significantly more advanced clinical stages (≥ IIB) (52.4% vs. 10.8%, p-value <0.01), a higher rate of tumor‐positive lymph nodes (61.9% vs. 26.5%, p-value=0.02), neural invasion (38.1% vs. 14.5%, p-value =0.014), and increased infiltration depth (1.2 vs. 0.9 cm, p-value=0.031) compared to patients without EBV infection (15). Additionally, a significant increase in immunosuppressive cells such as FoxP3+, CTL4+, ratio of Tregs cells to CD8+ tumor-infiltrating lymphocytes, PDL-1, and PD-1 expression was observed in EBV-positive than EBV‐negative squamous CC cases (15), indicating that EBV-positive tissue may be more susceptible to immunotherapy (21).
To date, only one study evaluated the impact of EBV on survival outcomes in CC. Similar to our findings, Zuo et al. found no significant association between EBV positivity in OS (p-value=0.212) or PFS (p-value=0.667) in patients with CC (15). One possible explanation for both our findings and those of Zuo et al. is that EBV may serve only as an enhancer of HPV, facilitating the transition from normal tissue to invasive cancer rather than serving as a prognostic factor, as observed in other malignancies (14, 22). Our results may have been influenced by delays in treatment initiation at our institution, obscuring differences between groups, as not all patients received timely and appropriate frontline treatment. This effect likely explains the inferior survival outcomes in our cohort compared to previous reports, where survival rates ranged from 60-80% in developed countries (2, 15) and 50-60% in developing countries (2). These results may be attributed to barriers to access treatment that affect up to 66% of the population in Peru (5).
Our study has limitations. First, the retrospective design restricted the availability of complete clinical and pathological data, likely introducing bias and confounding factors and limiting the strength of the associations observed. Second, we excluded 95 patients due to tissue deterioration, which may have affected the generalizability of our results; however, we do not expect to be differential based on EBV status. Third, this study was conducted in a single center that primarily serves the insured working population through the Social Security System in Peru, limiting the extrapolation of our findings to this specific demographic. Additionally, HPV status was not directly assessed; however, given the nearly universal presence of HPV in squamous cell carcinoma histology (23), it is likely that all patients with squamous cell carcinoma were HPV-positive. Despite these limitations, the main strength of our study lies in the use of RT-PCR, a highly sensitive technique for detecting EBV in the tissues of seropositive individuals (24). While the gold standard for EBV detection (EBER study) is effective for identifying latent infections, it has limitations in detecting cases where the virus is in the lytic phase, resulting in lower sensitivity and a higher rate of false-negative results compared to RT-PCR (25).
In conclusion, patients with CC and EBV infection in our Peruvian cohort demonstrated clinical features and survival outcomes comparable to those without EBV infection. Consequently, the routine screening for EBV in CC remains uncertain and requires further investigation. Future multicenter prospective studies are essential to clarify the prognostic significance of EBV infection in CC and determine its potential role in guiding clinical management.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The Institutional Review Board and Ethics Committee of the Hospital Edgardo Rebagliati Martins-EsSalud. The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from a by- product of routine care or industry. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
DC: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JV: Data curation, Investigation, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. BV: Conceptualization, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. ML: Investigation, Resources, Writing – original draft, Writing – review & editing. AY: Investigation, Writing – original draft, Writing – review & editing. AC: Data curation, Investigation, Writing – original draft, Writing – review & editing. LM: Investigation, Writing – original draft, Writing – review & editing. BB: Conceptualization, Funding acquisition, Investigation, Resources, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by the ‘Universidad de San Martin de Porres, which’ provided support for the RT-PCR platform used for all cervical samples included in the analysis.
Acknowledgments
We thank Dr. Ana Fernandez for her help in data collection and the CDX Molecular company (309 Javier Prado Avenue, San Isidro district, Lima-Peru) for providing the RT-PCR platform.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
EBNA-1, Epstein-Barr nuclear antigen 1; LMP-1, Latent membrane protein 1; RT-PCR, real-time polymerase chain reaction; CRT, chemoradiotherapy; RT, radiotherapy; ECOG, Eastern Cooperative Oncology Group scale.
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
2. Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. (2018) 391:1023–75. doi: 10.1016/S0140-6736(17)33326-3
3. Torres-Roman JS, Ronceros-Cardenas L, Valcarcel B, Arce-Huamani MA, Bazalar-Palacios J, Ybaseta-Medina J, et al. Cervical cancer mortality in Peru: regional trend analysis from 2008–2017. BMC Public Health. (2021) 21:1–10. doi: 10.1186/s12889-021-10274-1
4. Ruiz R, Serrano M, Ruiz EF, Mantilla R, Valdivieso N, Olivera M, et al. Características clínico-patológicas y sobrevida en mujeres jóvenes con cáncer cervical: análisis retrospectivo del Instituto Nacional de Enfermedades Neoplásicas. Rev Peru Med Exp Salud Publica. (2017) 34:218–27. doi: 10.17843/rpmesp.2017.342.2653
5. Barrios CH, Werutsky G, Mohar A, Ferrigno AS, Müller BG, Bychkovsky BL, et al. Cancer control in Latin America and the Caribbean: recent advances and opportunities to move forward. Lancet Oncol. (2021) 22:e474–87. doi: 10.1016/S1470-2045(21)00492-7
6. Chabay P, Lens D, Hassan R, Pinilla SMR, Gamboa FV, Rivera I, et al. Lymphotropic viruses EBV, KSHV and HTLV in latin america: epidemiology and associated Malignancies. A literature-based study by the RIAL-CYTED. Cancers (Basel). (2020) 12:1–58. doi: 10.3390/cancers12082166
7. Wong Y, Meehan MT, Burrows SR, Doolan DL, Miles JJ. Estimating the global burden of Epstein–Barr virus-related cancers. J Cancer Res Clin Oncol. (2021) 148:31–46. doi: 10.1007/s00432-021-03824-
8. Pyo JS, Kim NY, Kang DW. Prognostic implication of EBV infection in gastric carcinomas: A systematic review and meta-analysis. Medicina. (2023) 59(5):834. doi: 10.3390/medicina59050834
9. Ruuskanen M, Irjala H, Minn H, Vahlberg T, Randen-Brady R, Hagström J, et al. Epstein-Barr virus and human papillomaviruses as favorable prognostic factors in nasopharyngeal carcinoma: A nationwide study in Finland. Head Neck. (2019) 41:349–57. doi: 10.1002/hed.25450
10. Malpica L, Marques-Piubelli ML, Beltran BE, Chavez JC, Miranda RN, Castillo JJ. EBV-positive diffuse large B-cell lymphoma, not otherwise specified: 2024 update on the diagnosis, risk-stratification, and management. Am J Hematol. (2024) 99(10):2002–15. doi: 10.1002/ajh.27430
11. Tse E, Zhao WL, Xiong J, Kwong YL. How we treat NK/T-cell lymphomas. J Hematol Oncol. (2022) 15:1–13. doi: 10.1186/s13045-022-01293-5
12. Kołodziejczak M, Gil L, de la Camara R, Styczyński J. Impact of donor and recipient Epstein-Barr Virus serostatus on outcomes of allogeneic hematopoietic cell transplantation: a systematic review and meta-analysis. Ann Hematol. (2021) 100:763–77. doi: 10.1007/s00277-021-04428-9
13. Castro D, Beltran BE, Villela L, Montaño Figueroa E, Ramirez-Ibarguen AF, Candelaria M, et al. Clinicopathological features and outcomes of EBV positive and negative DLBCL: A study from the grupo de estudio latinoamericano de linfoproliferativos (GELL). Blood. (2021) 138:1442. doi: 10.1182/blood-2021-152340
14. Cyprian FS, Al-Farsi HF, Vranic S, Akhtar S, Al Moustafa AE. Epstein-Barr virus and human papillomaviruses interactions and their roles in the initiation of epithelial-mesenchymal transition and cancer progression. Front Oncol. (2018) 8:111. doi: 10.3389/fonc.2018.00111
15. Zuo Y, Xiao H, Lv D, Huang M, Wang L, Liu J, et al. Infection pattern and immunological characteristics of Epstein-Barr virus latent infection in cervical squamous cell carcinoma. J Med Virol. (2023) 95:e28717. doi: 10.1002/jmv.28717
16. Kahla S, Oueslati S, Achour M, Kochbati L, Chanoufi MB, Maalej M, et al. Correlation between EBV co-infection and HPV16 genome integrity in Tunisian cervical cancer patients. Braz J Microbiol. (2012) 43:744–53. doi: 10.1590/S1517-83822012000200039
17. Sasagawa T, Shimakage M, Nakamura M, Sakaike J, Ishikawa H, Inoue M. Epstein-Barr virus (EBV) genes expression in cervical intraepithelial neoplasia and invasive cervical cancer: A comparative study with human papillomavirus (HPV) infection. Hum Pathol. (2000) 31:318–26. doi: 10.1016/s0046-8177(00)80245-2
18. Bhatla N, Berek JS, Cuello Fredes M, Denny LA, Grenman S, Karunaratne K, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynecol Obstetrics. (2019) 145:129–35. doi: 10.1002/ijgo.12749
19. de Lima MAP, Neto PJN, Lima LPM, Gonçalves Júnior J, Teixeira Junior AG, Teodoro IPP, et al. Association between Epstein-Barr virus (EBV) and cervical carcinoma: A meta-analysis. Gynecol Oncol. (2018) 148:317–28. doi: 10.1016/j.ygyno.2017.10.005
20. Santos NBM, Villanova FE, Andrade PM, Ribalta J, Focchi J, Otsuka AY, et al. Epstein-Barr virus detection in invasive and pre-invasive lesions of the uterine cervix. Oncol Rep. (2009) 21:403–5. doi: 10.3892/or_00000236
21. Zheng X, Huang Y, Li K, Luo R, Cai M, Yun J. Immunosuppressive tumor microenvironment and immunotherapy of epstein–barr virus-associated Malignancies. Viruses. (2022) 14(5):1017. doi: 10.3390/v14051017
22. Vranic S, Cyprian FS, Akhtar S, Al Moustafa AE. The role of Epstein-Barr virus in cervical cancer: A brief update. Front Oncol. (2018) 8:113. doi: 10.3389/fonc.2018.00113
23. Pirog EC. Cervical adenocarcinoma diagnosis of human papillomavirus-positive and human papillomavirus-negative tumors. Arch Pathol Lab Med. (2017) 141:1653–67. doi: 10.5858/arpa.2016-0356-RA
24. Ryan JL, Fan H, Glaser SL, Schichman SA, Raab-Traub N, Gulley ML. Epstein-Barr Virus quantitation by real-time PCR targeting multiple gene segments: A novel approach to screen for the virus in paraffin-embedded tissue and plasma. J Mol Diagnostics. (2004) 6:378–85. doi: 10.1016/S1525-1578(10)60535-1
Keywords: Epstein-Barr virus, cervical cancer, clinical features, prognosis, survival
Citation: Castro-Uriol D, Vera J, Valcarcel B, López-Ilasaca M, Yabar A, Cámara A, Malpica L and Beltrán B (2024) Exploring the role of Epstein-Barr virus infection on the clinical features and survival in locally advanced cervical cancer: a retrospective cohort study. Front. Oncol. 14:1522244. doi: 10.3389/fonc.2024.1522244
Received: 04 November 2024; Accepted: 09 December 2024;
Published: 24 December 2024.
Edited by:
Kai Ding, University of Oklahoma Health Sciences Center, United StatesReviewed by:
Olugbenga Akindele Silas, University of Jos, NigeriaZeming Mo, Second Affiliated Hospital of Zunyi Medical University, China
Copyright © 2024 Castro-Uriol, Vera, Valcarcel, López-Ilasaca, Yabar, Cámara, Malpica and Beltrán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Denisse Castro-Uriol, ZGVuaXNzZWFuZ2VsaWNhY3VAZ21haWwuY29t