 Jiawei Kang
Jiawei Kang Nan Jiang1
Nan Jiang1- 1Department of Clinical Medicine, Xinjiang Medical University, Ürümqi, Xinjiang, China
- 2Department of Histology and Embryology, Basic Medical College of Xinjiang Medical University, Ürümqi, Xinjiang, China
- 3Department of Pharmacy, Xinjiang Key Laboratory of Neurological Diseases, Xinjiang Clinical Research Center for Nervous System Diseases, Second Affiliated Hospital of Xinjiang Medical University, Ürümqi, Xinjiang, China
Purpose: This study seeks to systematically analyze the research literature pertaining to breast cancer surgery from 2010 to 2024, as indexed in the PubMed database, employing bibliometric methodologies.
Methods: Employing the “bibliometrix” package in the R software, this research conducted a comprehensive visual analysis of 1,195 publications. The analysis encompassed publication trends, collaborative networks, co-citation networks, co-occurrence networks, journal evaluation, prominent publications, author and institutional assessments, country-specific analyses, keyword exploration, and the identification of research hotspots.
Results: The study observed a rising trend in the number of publications related to breast cancer surgery. However, there was a concomitant decline in citation rates, potentially indicating either a saturation of the research field or a diminution in research quality. The United States, China, and Japan are the leading contributors to research output, with the United States showing the most extensive international collaboration. The University of California, University of Toronto, and University of Texas MD Anderson Cancer Center were the top institutions for the number of published papers. Through a comprehensive analysis of keywords, we have identified “breast cancer” “pain” “anxiety” “lymphedema” “mastectomy” and “surgery” as central research themes within this domain, the corresponding clusters were subjected to analysis.
Conclusion: This study provides a comprehensive review of breast cancer surgery research, emphasizing major research areas and proposing future research directions. This study provides a significant resource for researchers and clinicians in the field.
1 Introduction
Breast cancer (BC) is a leading malignancy among women globally and significantly contributes to cancer-related mortality in this group. Surgical intervention, a fundamental aspect of the comprehensive therapeutic approach to BC (1), plays an indispensable role. An examination of surgical trends from 2005 to 2017 indicates a decline in the preference for invasive surgical procedures, accompanied by an increase in breast-conserving surgery (BCS) and reconstructive surgery (2). Increasing evidence indicates that BCS, when combined with adjuvant therapy, not only preserves the efficacy of tumor treatment but also improves aesthetic outcomes and patient satisfaction (3). This advancement can be traced back to the pioneering work of Umberto Veronesi, whose dedicated research and clinical practice significantly enhanced patient treatment experiences and quality of life, while also establishing a robust foundation for future research and clinical applications (4, 5). BC surgery has significantly evolved since the mid-20th century, transitioning from radical mastectomy to more conservative techniques that emphasize patient quality of life. This transition is largely attributed to the pioneering research and clinical trials conducted by Dr. Bernard Fisher (6). Recent investigations have examined novel surgical methodologies, including opioid-free anesthesia, that enhance postoperative recovery while maintaining effective pain management (7).
Bibliometrics, a discipline dedicated to the quantitative analysis of scientific literature, has emerged as an invaluable instrument for uncovering research trends, identifying knowledge gaps within research domains, and evaluating the impact of scientific contributions (8). Through the visualization of research patterns and collaboration networks, bibliometrics offers a distinctive perspective on the dynamics of the scientific community (9). A comprehensive bibliometric analysis of literature pertaining to BC surgery can identify emerging research themes, landmark studies, and the geographical distribution of scientific contributions (10).
This study aims to perform a detailed bibliometric examination of publications on BC surgery from 2010 to 2024.Utilizing the PubMed database, this research seeks to elucidate trends, prominent topics, and their developmental trajectories within this domain. This analysis examines publication trends, collaboration patterns, and the principal contributors to the field, categorized by countries, institutions, journals, and authors. Furthermore, the study explores prominent research topics and developmental trends in BC surgery, with the objective of offering guidance and insights for future research directions and clinical practices.
2 Methods
2.1 Data sources and retrieval strategy
PubMed, an integral component of the NCBI’s Entrez search system, offers access to 38 distinct databases, thereby serving as a central repository for medical literature. As of December 2023, PubMed contains over 36 million publications, underscoring its extensive collection of medical research (11). Data for this study were sourced from the PubMed database. On August 7, 2024, we exported a dataset of literature, complete with metadata, utilizing the “PubMed export file” feature (12). Our retrieval strategy was based on a topic search:((Breast Cancer Surgery[title]) AND ((“2010/1/1”[Date - Publication]: “2024/8/7”[Date – Publication])).
2.2 Data analysis
The content should be changed to the following: This study predominantly utilizes the R package “bibliometrix” (version 4.2.3) (13) (accessible at https://www.bibliometrix.org) for conducting bibliometric analysis. Data analysis is performed using R code in conjunction with the Bibliometrix package (R version 4.2.0) (14, 15). The initial data interpretation is facilitated through the “biblioAnalysis()” command and the “summary()” function within the Bibliometrix package (16). Collaboration networks are examined using the “metaTagExtraction” and “Biblionetwork” commands, with subsequent graphical representation achieved via the “Networkplot” command. Furthermore, the “Biblioshiny()” command is employed for analyses pertaining to national scientific collaboration, institutional collaboration networks, keyword analysis, co-occurrence network synthesis, and thematic map analysis.
3 Results
3.1 Literature search and processing
A thorough literature review identified 1,195 articles. Figure 1 provides a comprehensive overview of the methodology.
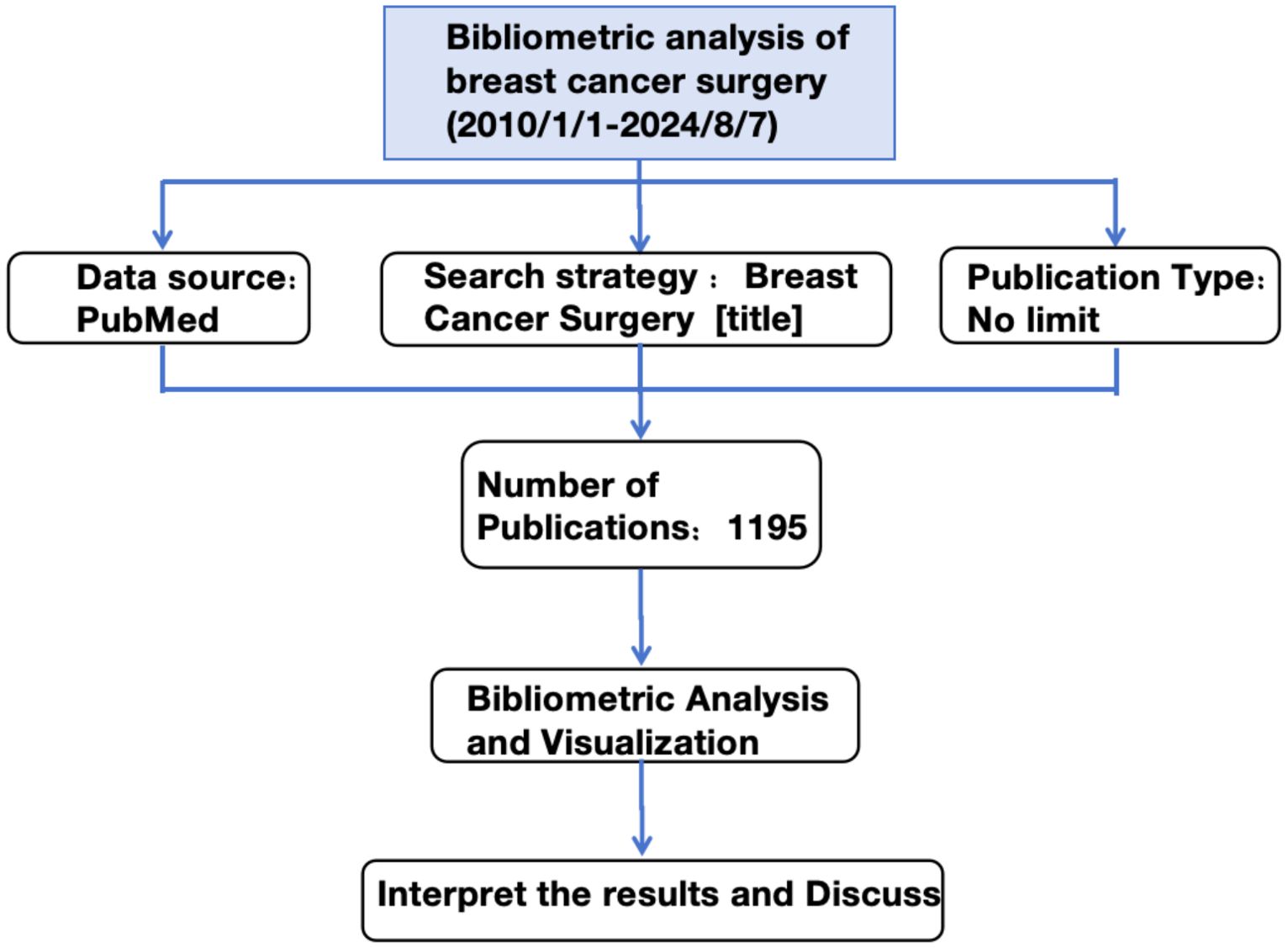
Figure 1. Workflow of the study.
3.2 Analysis of annual publishing trends and citation volume dynamics
Figure 2A presents the total number of relevant articles retrieved, which amounts to 1,195. The average annual publication rate is approximately 79 articles per year. In 2010, the scholarly output pertaining to the subject comprised 57 publications. Subsequently, a gradual increase was observed, culminating in a peak of 120 articles by 2020. However, a slight decline occurred in 2021, succeeded by a substantial rise in 2022 and 2023, with publication counts reaching 124 and 131 articles, respectively. Notably, in 2024, there was a pronounced decrease in the number of publications, with only 64 articles released. Furthermore, the trend in average annual citation counts demonstrates an inverse relationship with the trend in publication volume.
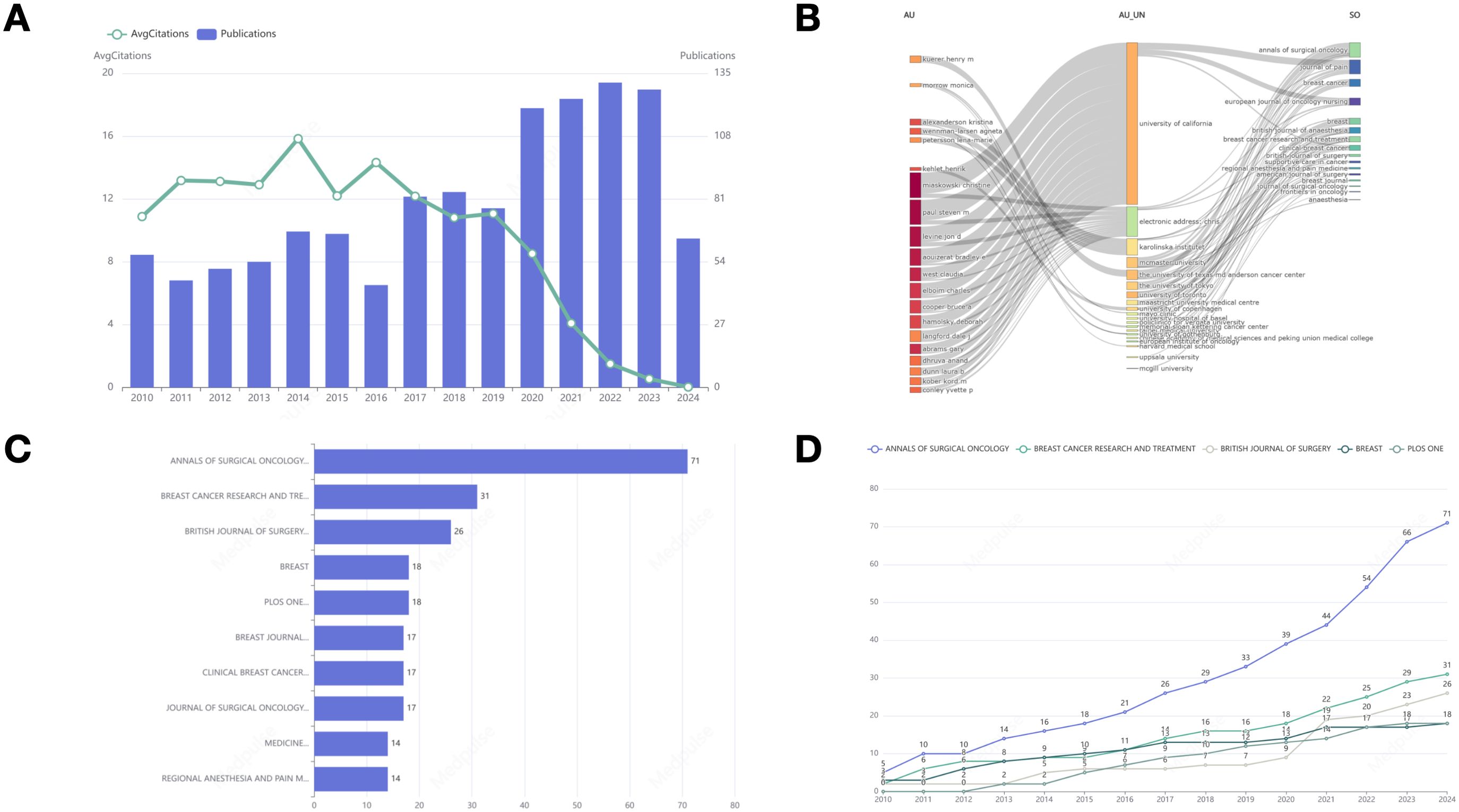
Figure 2. (A) Annual publication trends and average annual citations. (B) Three-field plot, Left field: Author; Middle field: Affiliation; Right field: Source. (C) Bar graph representing the distribution of literature sources. (D) The statistics of the top five journals in terms of cumulative publication volume in different years.
3.3 Three-field plot
Figure 2B illustrates a Sankey diagram that represents the interconnections among authors, their affiliations, and the sources of publication. A comprehensive analysis of the collaborative networks among these entities is undertaken, revealing the University of California as a pivotal institution within these partnerships.
3.4 Journal analysis
Figure 2C displays a ranking of the top ten journals based on publication volume. The ANNALS OF SURGICAL ONCOLOGY leads with 71 publications, followed by BREAST CANCER RESEARCH AND TREATMENT with 31, and the BRITISH JOURNAL OF SURGERY with 26. Figure 2D illustrates the annual publication counts for the top five journals in BC surgery. Recent years have seen an overall increase in publication numbers in prominent journals, with the ANNALS OF SURGICAL ONCOLOGY experiencing notable growth.
3.5 Author analysis
Figure 3A displays a ranking of the top ten authors based on their number of publications. MIASKOWSKI CHRISTINE is the leading author with 34 publications, followed by PAUL STEVEN M with 32 publications, and LEVINE JON D, who holds the third position with 26 publications. Figure 3B depicts the annual publication output of these authors, emphasizing the academic productivity of MIASKOWSKI CHRISTINE, PAUL STEVEN M, AOUIZERAT BRADLEY E, WEST CLAUDIA, ABRAMS GARY, HAMOLSKY DEBORAH, and LEVINE JON D in the years 2012 and 2014, as detailed in Table 1. Each of these authors demonstrated a remarkable scholarly output, publishing no fewer than 120 works annually over the two-year period. Furthermore, Elboim Charles and Cooper Bruce A also showed notable productivity in 2014. Figures 3C–E illustrate the collaborative network among the authors. In this network diagram, the connections between nodes signify collaborative efforts, underscoring that authors with the highest publication counts have increasingly engaged in collaborative endeavors with their peers in recent years. Notably, Miaskowski Christine emerges as the most interconnected author, with a betweenness centrality of 3.9754, a closeness centrality of 0.0556, and a PageRank of 0.0409, this suggests that his extensive collaborative efforts may position him as a pivotal researcher within the field.
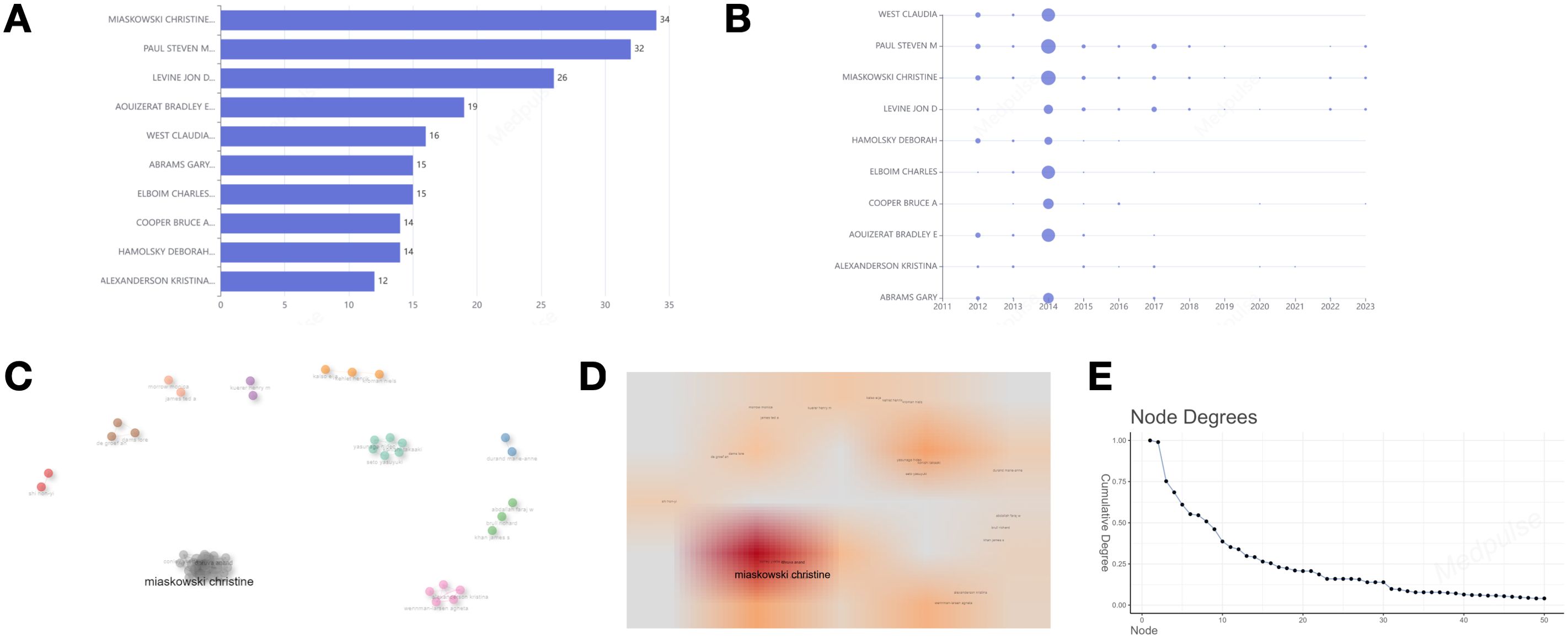
Figure 3. (A) Ten of the most relevant authors. (B) Top 10 authors’ production over time. (C–E) Collaboration network map and density map of the key authors analysis. (C) Collaboration network map. (D) Density map; (E) The number of connections per node in the network.
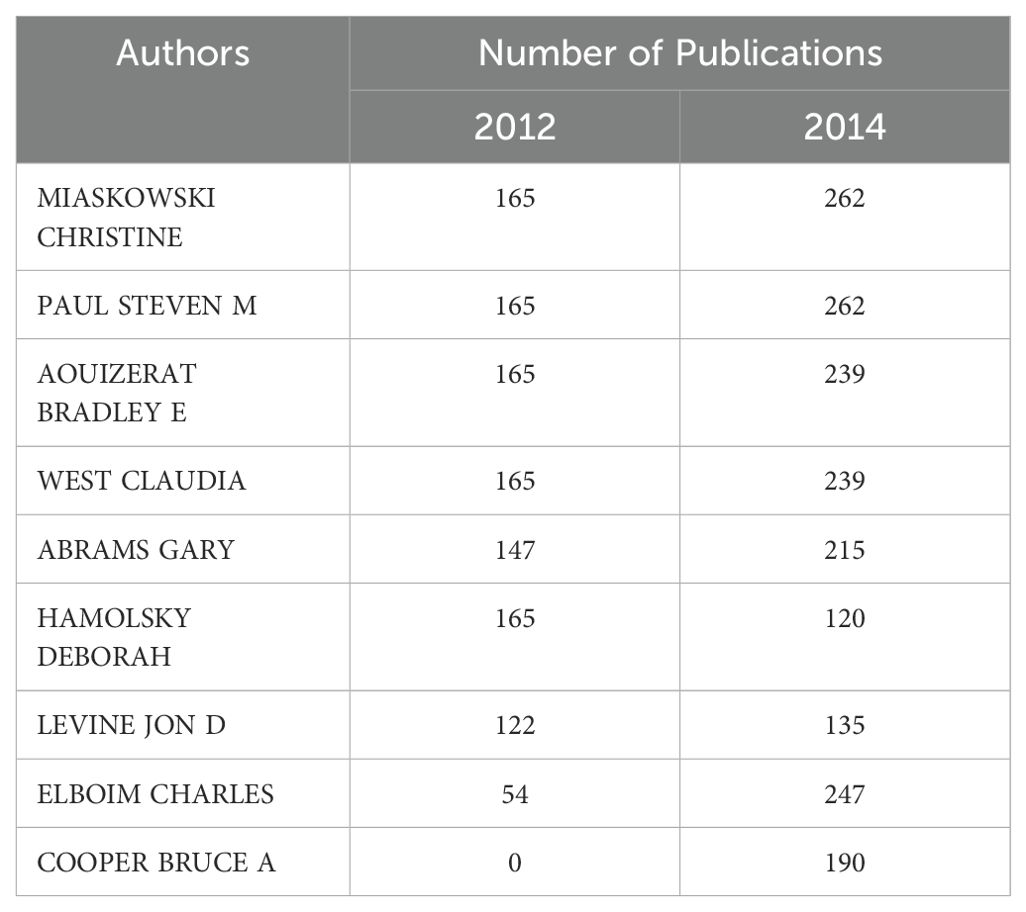
Table 1. The top 9 authors published the most in 2012 and 2014.
3.6 Institution analysis
Figure 4A shows that the University of California has the most publications (n=70). The University of Toronto ranks second with 49 publications, followed by The University of Texas MD Anderson Cancer Center in third place with 45 publications. Figure 4B depicts the publication trends over the years for the top five institutions, highlighting the University of California as the most consistent and significant contributor. Significant contributions to the field have been made by the University of Toronto, McMaster University, the University of Texas MD Anderson Cancer Center, and the University of Tokyo. An increasing trend in the number of publications is evident across all these institutions.
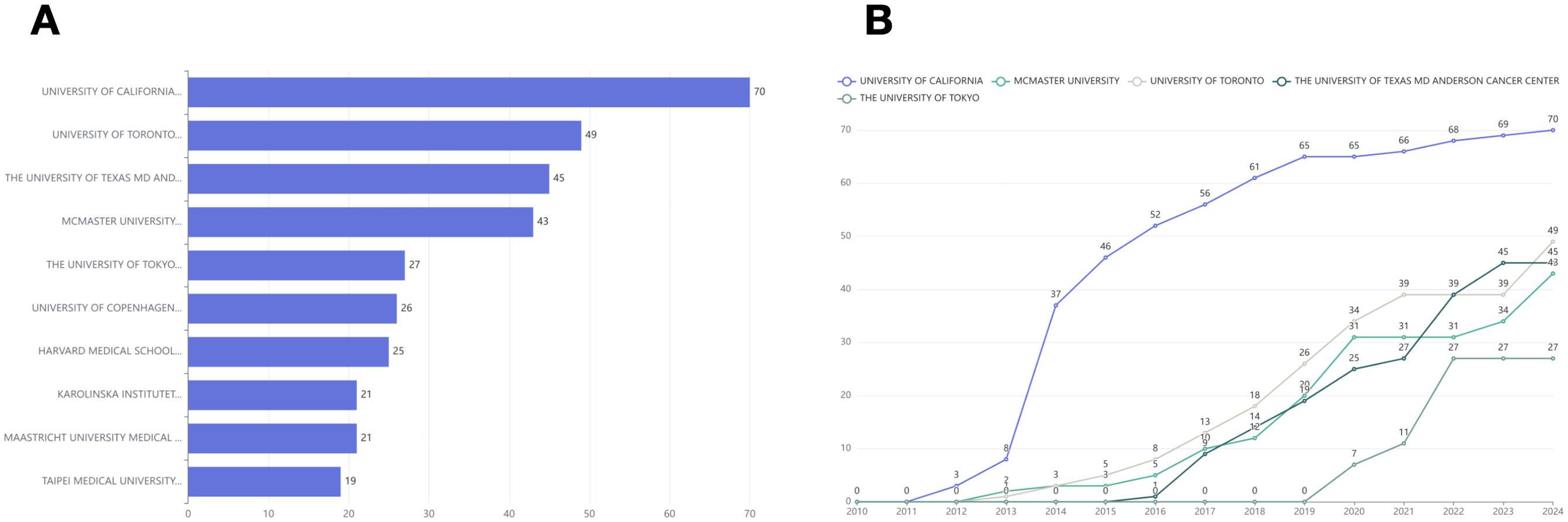
Figure 4. (A) Top 10 most relevant affiliations. (B) The top 5 affiliations’ production over time.
3.7 National analysis
In our analysis of national contributions, corresponding authors originate from 19 different countries. Figure 5A presents a ranking of these countries based on their publication output, with China at the forefront (P=121; SCP=113; MCP=8), followed by the United States (P=120; SCP=108; MCP=12), and Japan in third place (P=47; SCP=46; MCP=1). The majority of publications originating from these countries are characterized by multinational collaborations. In contrast, Spain exhibits a multinational publication ratio of 0%, indicating a notable absence of international cooperation. China and the United States demonstrate multinational publication ratios of 6.81% and 10%, respectively, suggesting that China’s level of international collaboration is comparatively lower than that of the United States.
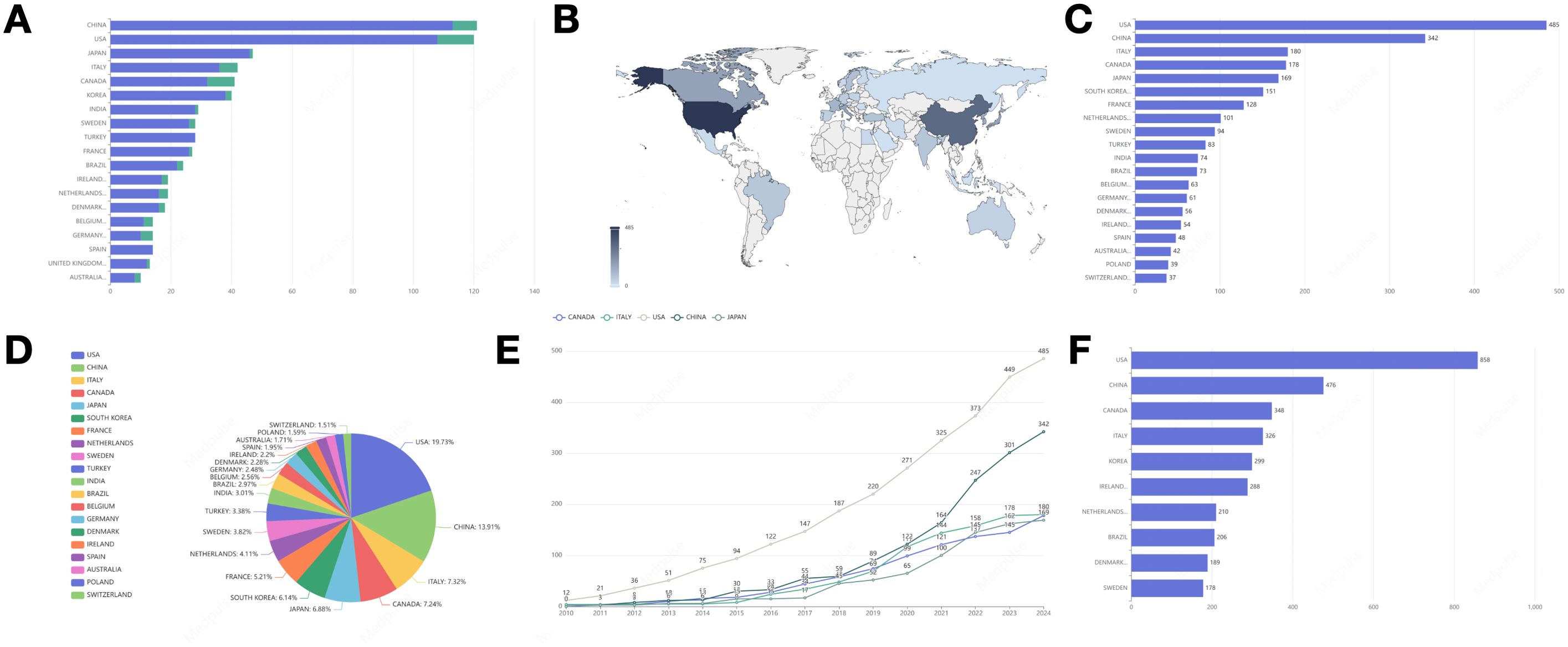
Figure 5. (A) Ranking of publications in the countries where the corresponding authors are located and the proportion of international cooperation (blue for single-country publications, green for multi-country publications). (B) Country scientific production. (C) Distribution of publications in the top 20 countries. (D) Percentage distribution of publications in the top 20 countries. (E) The number of publications in the top 5 countries by volume and their growth trend. (F) The most influential country in terms of number of citations to its articles.
The academic publications analyzed in this study are distributed across 60 countries and regions worldwide, as depicted in Figure 5B. We have mapped the geographical distribution of these publications, with a particular focus on the top 20 countries, as illustrated in Figures 5C, D. Among these, 12 countries are from Europe, along with several from North America, South America, Asia, and Oceania. The United States ranks first in publications with 485 entries (19.73%), followed by China with 342 entries (13.91%). Italy ranks third in publication output (n=180, p=7.32%).
Upon analyzing the trends in publication growth across various countries, it is evident that the top five nations, in terms of publication volume, exhibit a consistent annual increase, as illustrated in Figure 5E. The United States leads in contributions with the most publications, followed by China, Italy, Canada, and Japan. It is noteworthy that China has experienced a marked upward trajectory in publication output since 2021.
Figure 5F illustrates the citation impact of the top ten countries by total citations (TC). The top three countries include the United States, China, and Canada. The United States exhibits a notably higher total number of citations (TC=858) compared to other nations, being approximately 1.8 times greater than China (TC=476) and 2.5 times greater than Canada (TC=348).
3.8 Countries’ collaboration world map
Figure 6 depicts the international research collaboration network encompassing 38 countries and regions. Within this network, Australia and Belgium are particularly prominent, having established cooperative relationships with over ten different countries each. Furthermore, Brazil, France, and Germany emerge as significant contributors to the network, actively participating in frequent scientific research collaborations with numerous countries.
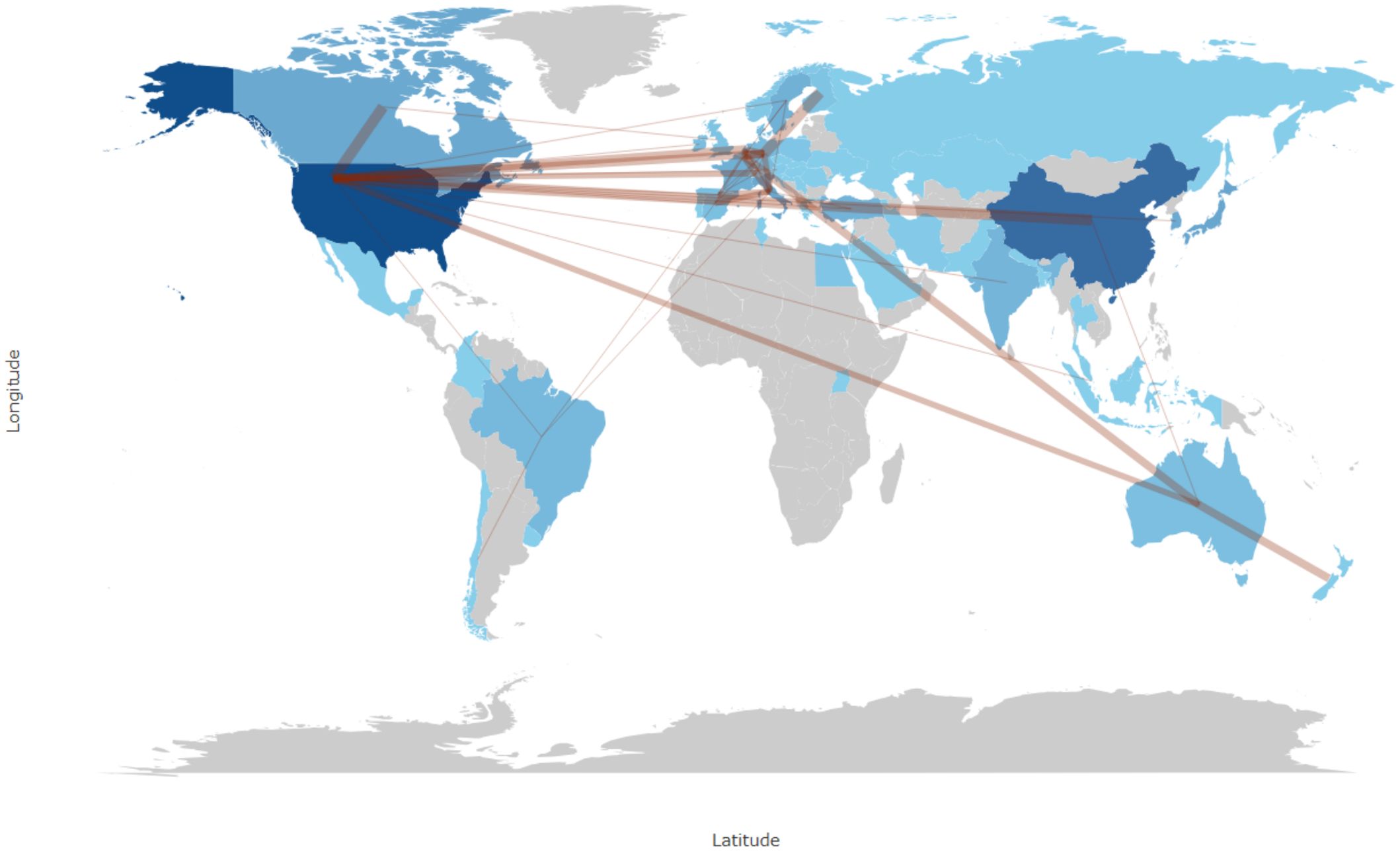
Figure 6. World map of collaboration between countries.
3.9 Analysis of prominent publications
Within the domain of BC surgery, we have highlighted the top ten papers from two distinct perspectives: international citation rankings (Figure 7A) (Table 2) and impact factor rankings (Table 3). The paper “Locoregional Recurrence After Breast Cancer Surgery: A Systematic Review by Receptor Phenotype” is the most cited, with 154 citations. “Perioperative Management May Lead to Less Pain After Breast Cancer Surgery” ranks highest in impact factor, achieving a notable score of 503.1.
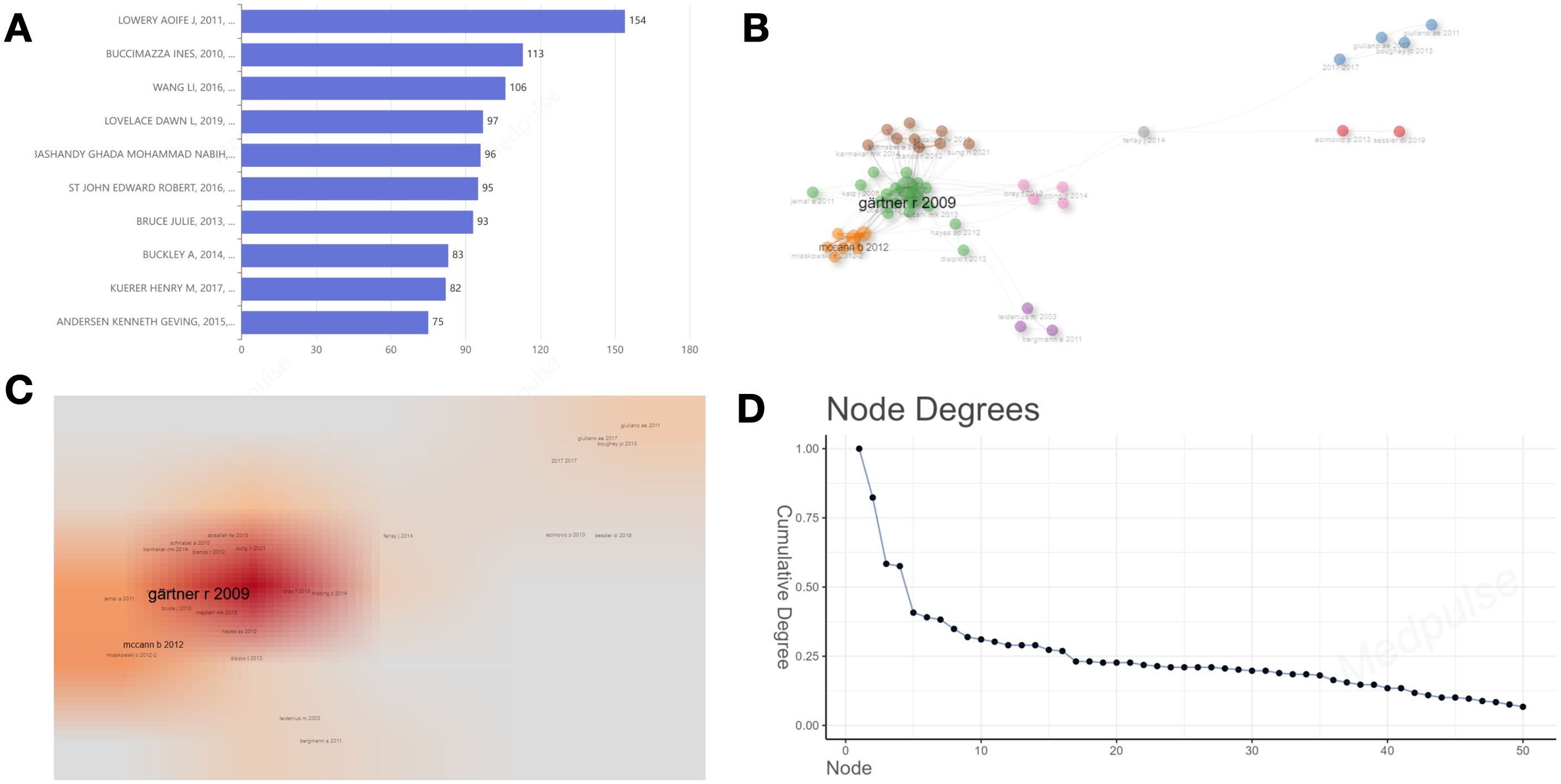
Figure 7. (A) The top 10 most globally cited documents. (B) Literature co-citation network visualization. (C) Literature co-citation density visualization. (D) The number of connections per node in the network.
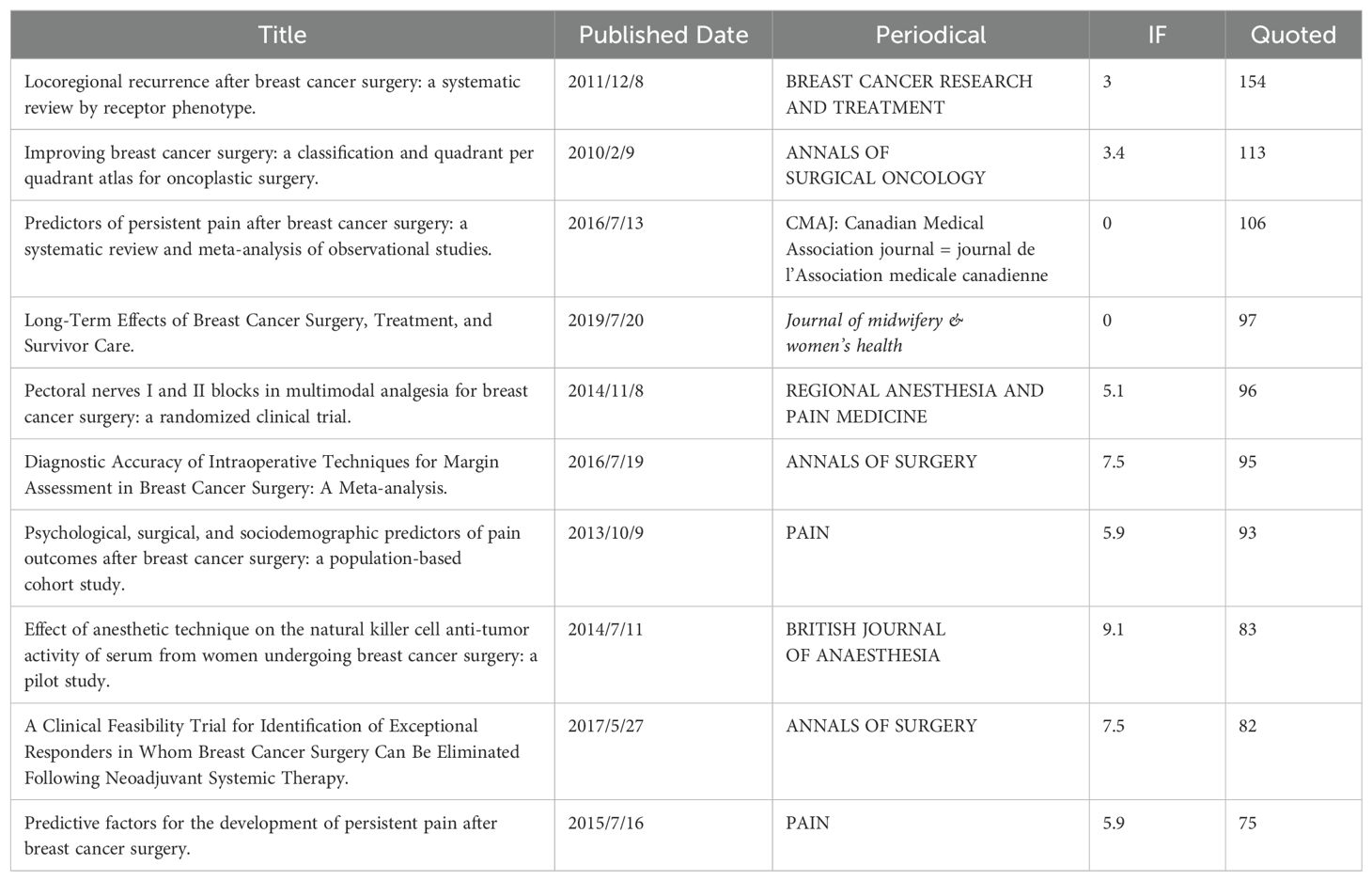
Table 2. Highly cited literature.
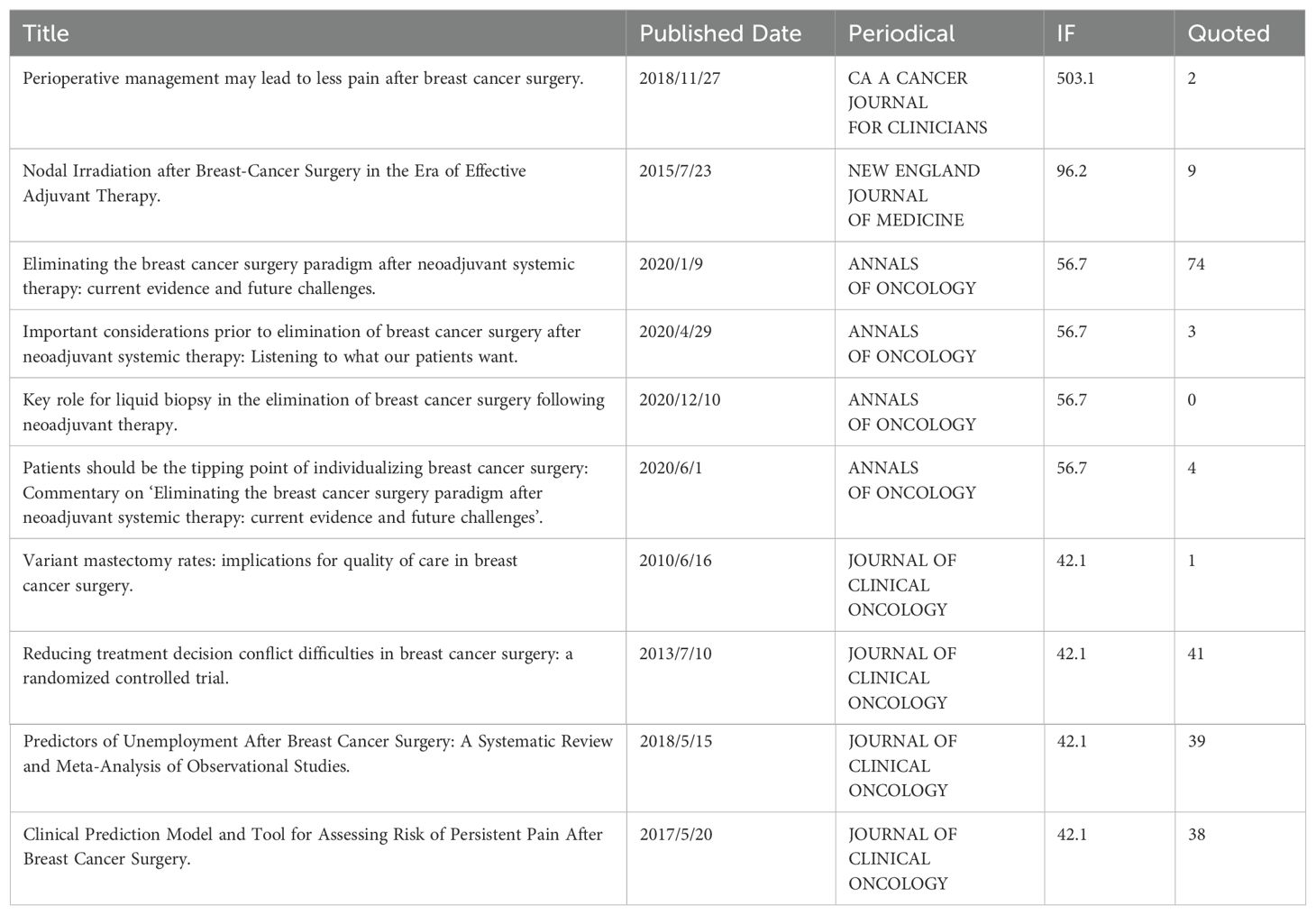
Table 3. High-scoring literature.
3.10 Co-citation network
Figures 7B–D depict the co-citation network within the literature. Co-citation is the simultaneous citation of two references within a single article. In this network, nodes and links represent the citation relationships between referenced works and their co-citation connections. The most significant contribution is attributed to the work of Gärtner (2009), with metrics of Betweenness=294.5934, Closeness=0.0068, and PageRank=0.0654. This is followed by McCann (2012), with Betweenness=93.5772, Closeness=0.0066, and PageRank=0.0333.
3.11 Keywords analysis
Figures 8A, B depict the high-frequency keywords prevalent in the literature of this field, while Figure 8C presents the ten most frequently occurring keywords. “Breast cancer” emerges as the most prevalent keyword (frequency = 275), followed by “breast cancer surgery” (frequency = 69), “mastectomy” (frequency = 64), and “surgery” (frequency = 60). These findings align with the results derived from the word cloud analysis. Figure 8D illustrates the temporal trends of the top ten keywords based on frequency, highlighting that “breast cancer” consistently remains the most frequent keyword and exhibits the most significant growth trend over time. Since 2022, the term “breastcancer” has gained prominence, demonstrating an increasing trend in annual frequency.
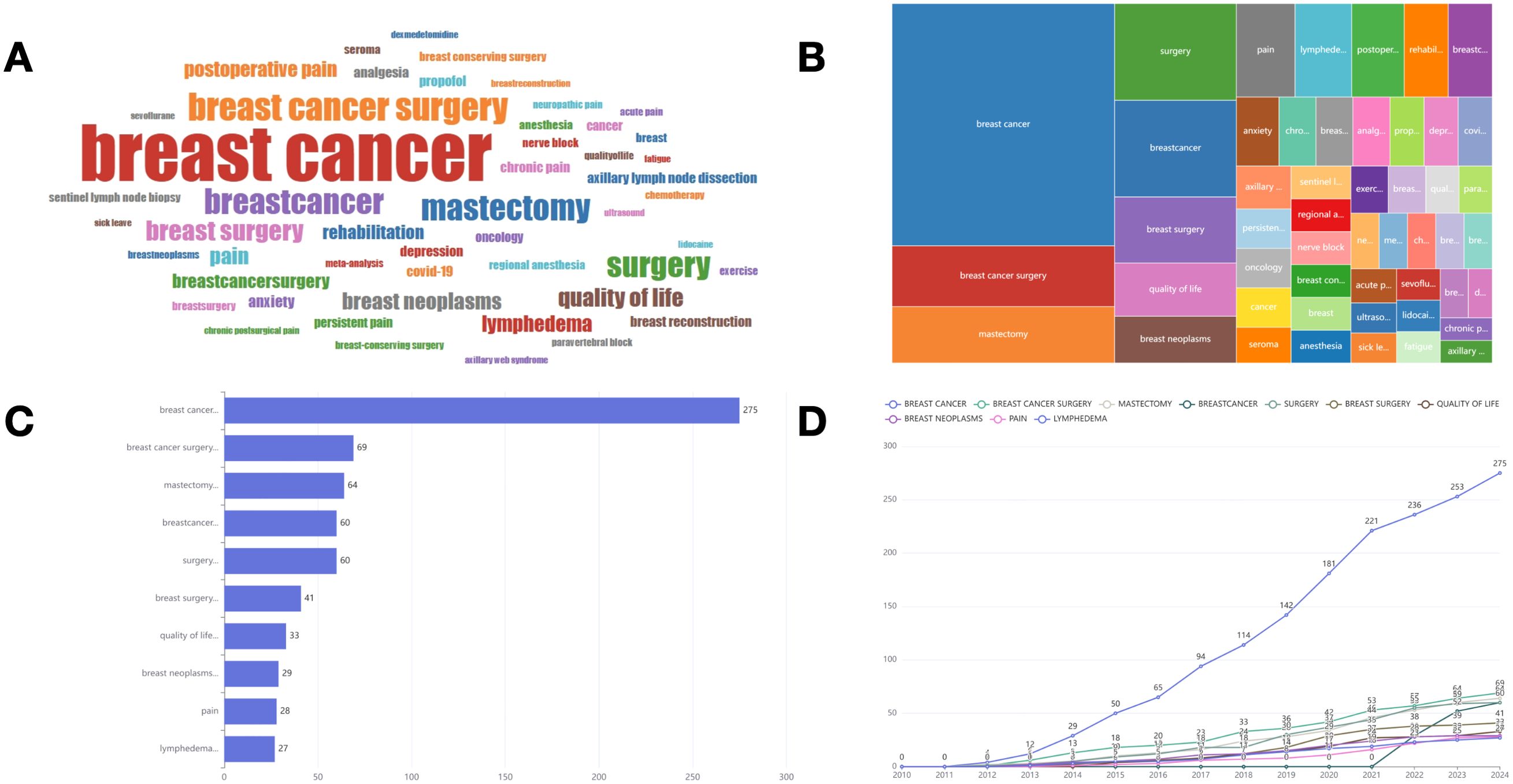
Figure 8. (A) World-Cloud for the relevant words. (B) Tree map for the relevant words. (C) Top 10 most frequent words. (D) Change in the frequency of the top 10 keywords over time.
3.12 Co-occurrence network
We conducted a co-occurrence network analysis of keywords (Figure 9A), which illustrates the interconnections among keywords in this domain. The density plot analysis (Figure 9B) provides a visualization based on the frequency of keyword occurrences, with “breast cancer” emerging as the most prominent term. Simultaneously, the degree distribution analysis (Figure 9C) underscores the particularly significant presence of “breast cancer,” reflecting its central position within the network diagram. Table 4 presents thematic descriptions and total link strength of keywords, organized into nine clusters: Pain Management Following BC Surgery, Management of Postoperative Pain and Regional Anesthesia (RA), Treatment and Rehabilitation of BC, Surgical Interventions for BC, Quality of Life Among BC Patients in Relation to Breast Reconstruction, Management of Lymphedema and Lymph Node Surgery Following BC Treatment, Anesthesia Management During BC Surgery, Use of Lidocaine in BC Surgery, and Incidence of Chronic Postsurgical Pain Following BC Surgery.
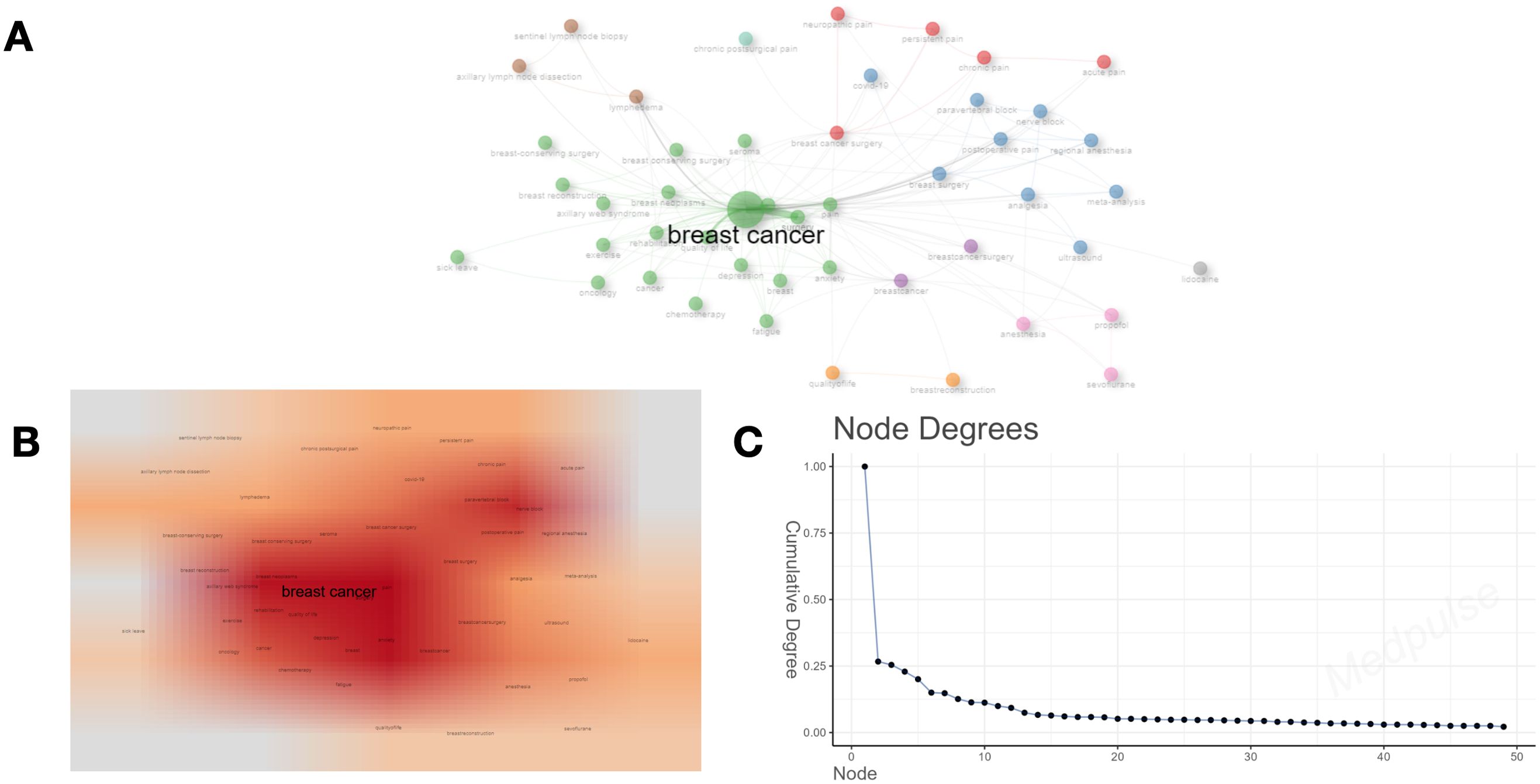
Figure 9. (A) Clustering diagram based on keyword analysis. The size of the circle indicates the number of occurrences of the keyword, and the different colors indicate the diversity of the clusters. (B) Darker areas indicate higher co-occurrence frequencies or stronger relationship densities. (C) The number of connections per node in the network.
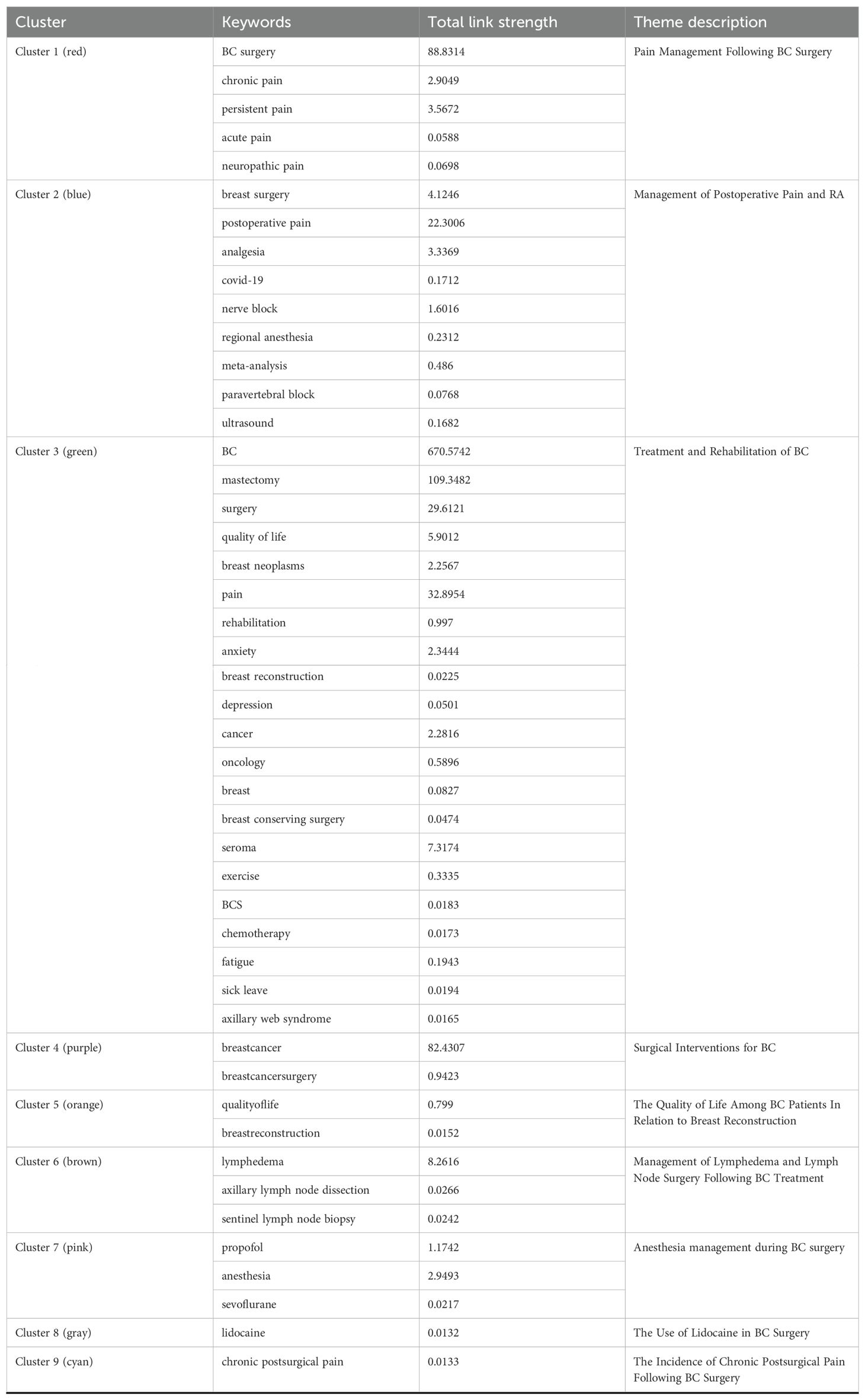
Table 4. Thematic co-occurrence clustering.
3.13 Analysis of trend themes and topic mapping
We employed the “bibliomtrix” software package to more accurately identify research hotspots within the field. Figure 10 delineates several prominent research themes. In 2019, the primary focal areas included “breast cancer” (frequency=275), “breast cancer surgery” (frequency=69), “breast neoplasms” (frequency=29), and “lymphedema” (frequency=27), corresponding to clusters 1, 3, and 6. In 2020, scholarly investigations predominantly addressed the topics of “mastectomy” (frequency=64), “surgery” (frequency=60), “breast surgery” (frequency=41), “quality of life” (frequency=33), “postoperative pain” (frequency=25), “rehabilitation” (frequency=21), “chronic pain” (frequency=13), and “COVID-19” (frequency=12), aligning with clusters 1, 2, and 3. The emergence of “COVID-19” underscores the critical need to examine the pandemic’s impact on the accessibility and continuity of BC treatment. In 2021, research efforts shifted to focus on “pain” (frequency=28), “anxiety” (frequency=15), and “analgesia” (frequency=13), corresponding to clusters 2 and 3. In 2023, the primary research focal points remained centered on “breastcancer” (frequency = 60) and “breastcancersurgery” (frequency = 21), both of which are associated with cluster 4.By employing co-occurrence network analysis, we can discern the overarching categories of research themes within this domain. Nevertheless, identifying future research trajectories continues to pose significant challenges. We employed the thematic mapping module (Figure 11) to analyze current research themes and identify potential future directions in BC surgery. The first quadrant includes key and established themes such as “breast cancer surgery,” “propofol,” “anesthesia,” “sevoflurane,” “postoperative pain,” “analgesia,” and “quality of life.” In contrast, the second quadrant comprises themes such as “dexmedetomidine,” “general anesthesia,” “growth mixture modeling,” “thoracic paravertebral block,” “chemotherapy,” “physical therapy,” and “radiotherapy,” which, although gaining popularity, are of comparatively lesser relevance to the field. The third quadrant encompasses themes such as “sick leave,” “lidocaine,” and “breast-conserving surgery,” which are characterized as underdeveloped, emerging, or declining. The fourth quadrant includes themes like ‘breast cancer’ ‘pain’ ‘anxiety’ ‘persistent pain’ ‘lymphedema’ ‘neuropathic pain’ ‘axillary lymph node dissection’ and ‘sentinel lymph node biopsy. ‘These themes are considered fundamental and significant to the field, yet they remain in a nascent stage of development. The terms “mastectomy” and “surgery” appear in both the first and fourth quadrants, indicating their significance as central development hotspots. Notably, all keywords located in the fourth quadrant are associated with clusters 1, 3, 4, and 6.Based on this integration of findings, it can be inferred that “breast cancer,” “pain,” “anxiety,” “lymphedema,” “mastectomy,” and “surgery” potentially represent the research frontier in this field.
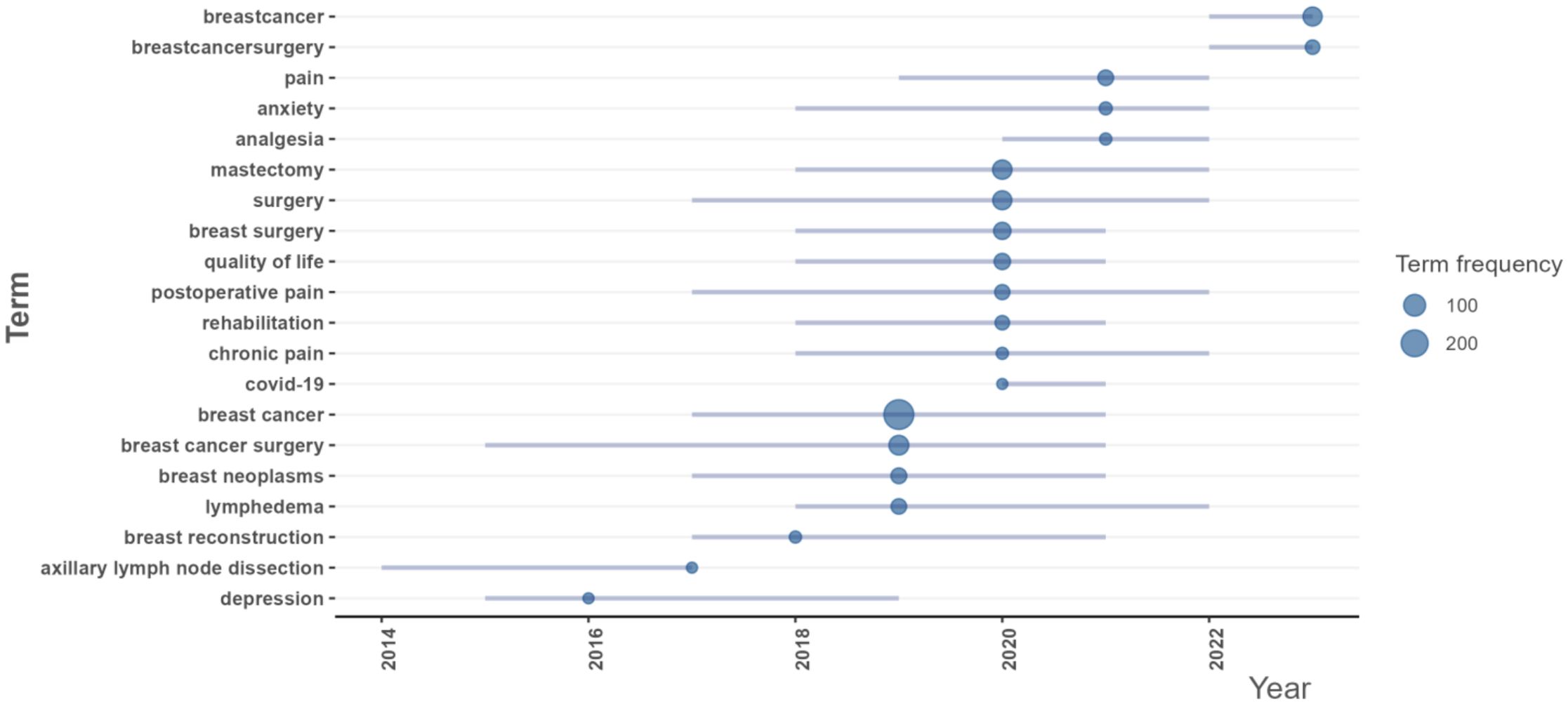
Figure 10. Trend topics authors’ keywords.
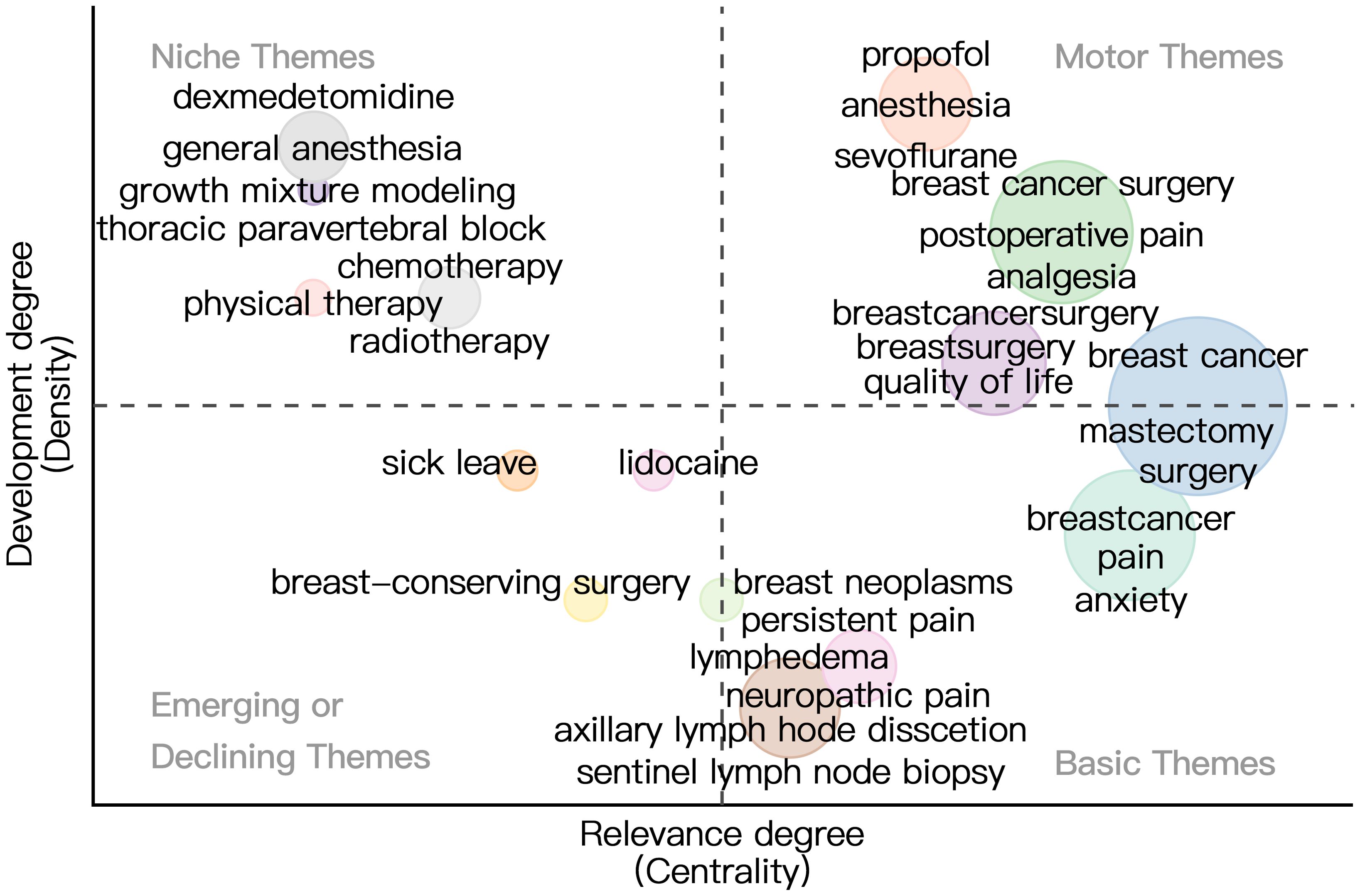
Figure 11. Thematic map. The horizontal axis represents centrality and indicates how relevant the topic is to the field. The vertical axis represents density, which indicates how developed the topic in the field is. Four quadrants are plotted accordingly: Motor Themes, Niche Themes, Emerging or Declining Themes, Basic Themes.
4 Discussion
4.1 Research status
This study employed “bibliometrix” package to perform a comprehensive visual analysis of 1,195 scholarly articles related to BC surgery, sourced from the PubMed database spanning the years 2010 to 2024. The analysis encompassed various dimensions such as publication and citation metrics, collaboration network analysis, journal evaluation, author and institutional profiling, country-specific contributions, identification of seminal literature, keyword examination, and the exploration of research hotspots within the field.
The total number of publications in this field is increasing, but citation frequency is declining. This pattern implies an increasing research interest in the area, which may also reflect a potential decline in the quality of papers or a saturation of the research domain, thereby hindering the ability of new studies to achieve significant breakthroughs. The observed decline in both publications and citations in 2024 could be attributed to the temporal limitations of the dataset, as the data collection was concluded on August 7th. China, the United States, and Japan are the leading publishing countries, with the United States showing the most frequent international collaborations. Conversely, Spain requires enhancement in its international cooperative efforts. Furthermore, an analysis of the national cooperation network indicates that Australia and Belgium maintain the most robust cooperative relationships. Christine Miaskowski, Steven M. Paul, and Jon D. Levine are among the authors with the highest publication output, with significant contributions in 2012 and 2014. This prominence may be attributed to advancements in research methodologies or techniques that enhanced research efficiency. The journals *Annals of Surgical Oncology*, *Breast Cancer Research and Treatment*, and the *British Journal of Surgery* have the highest publication counts, with each showing a trend of rising annual publication rates. The article “Locoregional Recurrence After Breast Cancer Surgery: A Systematic Review by Receptor Phenotype” (17) has been cited 154 times, whereas “Perioperative Management May Lead to Less Pain After Breast Cancer Surgery” (18) has an impact factor of 503.1.Both studies provide fresh insights into BC surgery and propose directions for future research. The placement of the two documents, Gärtner R (2009) (19) and McCann B (2012) (20), within the co-citation network suggests that they possess substantial influence and centrality within the scholarly discourse on BC surgery. These works have significantly contributed to the advancement of the field. The aforementioned studies demonstrate a consistent trajectory of progress in BC surgery research.
4.2 Research hotspots and trends
Keywords serve as concise representations of the central themes within the literature. An analysis of these keywords revealed that “breast cancer surgery,” “mastectomy,” and “surgery” were among the most frequently occurring terms. By integrating this analysis with studies on theme co-occurrence, thematic trends, and thematic mapping, we have identified “breast cancer,” “pain,” “anxiety,” “lymphedema,” “mastectomy,” and “surgery” as the principal research domains in this field. In the following sections, we will explore the research hotspots and trends associated with each of these five thematic clusters.
4.3 Cluster one: pain management following BC surgery
Effective pain management following BC surgery constitutes a critical component of patient care, given the prevalence of pain experienced by patients postoperatively. Post-surgical pain can be classified into acute pain, which generally arises immediately after the procedure, and chronic pain, which may develop progressively over time. Chronic pain post-BC surgery is characterized by its persistence and affects approximately 30% of patients, frequently exhibiting neuropathic features (21). The progression from acute to chronic pain represents a critical concern, given its potential to result in prolonged suffering and a diminished quality of life. Research suggests that between 10% and 50% of patients may experience chronic post-surgical pain, with contributory factors including nerve damage and inflammation being pivotal in its development (22). A thorough grasp of the mechanisms driving this transition is crucial for developing effective pain management strategies.
Effective pain management includes both pharmacological and non-pharmacological approaches. Opioids are commonly used for acute pain management, but extended use can lead to negative effects such as opioid-induced hyperalgesia (23). As a result, there is a growing emphasis on opioid-sparing pain management strategies, including the use of non-pharmacological methods like mindfulness-based stress reduction and acupuncture (22).
Furthermore, the identification of predictors for persistent postoperative pain is of paramount importance. Existing research indicates that factors such as chronic preoperative pain, psychological resilience, and the surgical techniques employed can substantially affect pain outcomes following surgery (24, 25). For example, individuals experiencing chronic pain prior to surgery are at an increased risk of moderate to severe postoperative pain, underscoring the necessity for comprehensive preoperative assessments and the implementation of targeted intervention strategies (25).
In conclusion, effective pain management following BC surgery necessitates a holistic approach that addresses both acute and chronic pain. By comprehensively understanding the associated risk factors and underlying mechanisms, healthcare providers can develop and implement individualized strategies aimed at enhancing patient treatment outcomes and mitigating the prevalence of persistent pain.
4.4 Cluster two: management of postoperative pain and RA
Effective postoperative pain management is a critical component of patient care, especially in the context of breast surgery, where moderate to severe pain can significantly impact patient recovery and overall satisfaction. Pectoral nerve blocks and erector spinae plane blocks are effective RA techniques for analgesia in breast surgery patients. Systematic reviews and network meta-analyses have indicated that these RA techniques are superior to traditional local anesthetic infiltration in managing early postoperative resting pain (26).
Moreover, the integration of RA into a multimodal analgesia regimen can substantially decrease reliance on opioids, a critical consideration given the increased awareness of opioid-related complications and the current opioid crisis. RA techniques not only alleviate pain but also facilitate faster recovery and shorter discharge times, aligning with Enhanced Recovery After Surgery protocols. These protocols underscore the significance of minimizing perioperative stress and optimizing pain management to enhance patient outcomes (27).
Amidst the ongoing challenges of the COVID-19 pandemic, integrating RA into postoperative pain management is essential for healthcare systems. This method addresses the immediate requirements of patients undergoing breast surgery while simultaneously enhancing surgical care pathways and optimizing overall patient outcomes within a swiftly evolving healthcare landscape (28). A systematic review indicates that paravertebral blocks significantly reduce both postoperative analgesic requirements and the incidence of postoperative nausea and vomiting compared to general anesthesia (29).
Furthermore, the implementation of ultrasound-guided paravertebral blocks has been shown to enhance the success rate of the procedure, resulting in improved analgesic outcomes and diminished opioid consumption (30). In a randomized controlled trial, ultrasound-guided paravertebral blocks demonstrated superior anesthetic and perioperative analgesic efficacy compared to traditional anatomical landmark techniques (31). This technological advancement enhances patient comfort and facilitates expedited recovery and discharge (32). Research suggests that managing postoperative pain with paravertebral blocks can reduce the occurrence of persistent post-surgical pain syndrome (33). The results underscore the significance of integrating RA techniques, particularly ultrasound-guided paravertebral blocks, into multimodal analgesia regimens to optimize postoperative pain management and enhance the overall recovery experience for patients undergoing diverse surgical procedures (34).
In general, the incorporation of RA and multimodal analgesia into postoperative pain management protocols can enhance patient comfort, contribute to improved surgical outcomes, and mitigate opioid-related complications.
4.5 Cluster three: treatment and rehabilitation of BC
The management and rehabilitation of BC involve a comprehensive array of surgical and non-surgical interventions designed to enhance treatment outcomes and patient quality of life. Mastectomy, a principal surgical intervention, entails the excision of one or both breasts, primarily to eradicate malignant tissue. The decision between undergoing a mastectomy and opting for BCS can profoundly influence the patient’s quality of life following treatment. Research indicates that although both surgical interventions can produce satisfactory outcomes, patients undergoing BCS frequently report superior quality of life metrics, especially concerning body image and emotional well-being (35, 40).
Conversely, post-mastectomy patients may encounter several complications, such as seroma formation, characterized by fluid accumulation at the surgical site. This condition can lead to discomfort and may necessitate further medical intervention, thereby impacting the overall recovery process and quality of life (38). Comprehending the implications of surgical complications, such as seroma, is essential for both patients and healthcare providers in the formulation of treatment plans. Research indicates that although mastectomy may be linked to specific complications, the overall effect on quality of life is contingent upon individual factors, including the type of reconstruction undertaken and the patient’s psychological resilience (36, 41).
Furthermore, the psychosocial dimensions of BC treatment warrant significant consideration. The decision to pursue mastectomy or breast reconstruction is frequently shaped by variables including patient age, individual preferences, and the risk-benefit profile of each surgical intervention. Notably, in older patients, the option of breast reconstruction post-mastectomy can substantially enhance quality of life, notwithstanding initial reluctance from both patients and surgeons (36, 37).
In conclusion, the interplay between BC treatment, surgical procedures like mastectomy, and subsequent rehabilitation is complex. It is imperative for healthcare professionals to thoroughly discuss with patients the available treatment options, potential complications such as seroma, and the anticipated effects on quality of life. This comprehensive approach facilitates informed decision-making by patients, ensuring alignment with their personal values and health objectives (39, 42).
4.6 Cluster four: surgical interventions for BC
Surgical management of BC primarily focuses on techniques such as BCS and mastectomy. BCS commonly known as lumpectomy, is the standard procedure for early-stage BC, allowing tumor removal while preserving as much breast tissue as possible (43). This approach significantly improves cosmetic outcomes and patient quality of life (45). Accurate localization of tumors during BCS continues to present significant challenges, particularly in cases involving small or non-palpable lesions. This difficulty can result in incomplete tumor excision and elevated rates of re-excision (43).
Recent advancements in surgical methodologies and technologies have been directed toward improving the precision of BC surgeries. Notably, the integration of fiber-optic photoacoustic guidance with augmented reality has demonstrated potential in enhancing tumor localization accuracy during surgical procedures, thereby potentially decreasing the necessity for re-excision (43). Advanced imaging techniques, such as quantitative micro-elastography and Cerenkov luminescence imaging, are being explored for their ability to identify residual cancer in the surgical cavity in real-time, potentially improving surgical results (47, 49).
In parallel, the management of axillary lymph nodes is undergoing significant transformation, with a discernible trend toward minimally invasive surgical approaches. The transition from routine axillary clearance to SLNB marks a pivotal shift, contributing to reduced morbidity and improved patient quality of life (45). This is particularly significant as a growing number of early-stage BC patients benefit from personalized treatment strategies that reduce invasiveness while ensuring effective cancer management (45).
The approach to treating ductal carcinoma in situ (DCIS) is undergoing changes. Studies indicate that many patients undergoing BCS for DCIS may face a second breast event, necessitating further surgical procedures (44). Comprehending the patterns of care and treatment modalities for SBE is essential for optimizing patient outcomes and informing future clinical practices (44).
The surgical management of BC is undergoing constant evolution, driven by ongoing research and technological advancements that seek to enhance precision, minimize complications, and improve the overall patient experience (46, 48, 50).
4.7 Cluster six: management of lymphedema and lymph node surgery following BC treatment
The management of lymphedema and the surgical treatment of lymph nodes are essential aspects of patient care following BC therapy. Surgical procedures for axillary lymph nodes include axillary lymph node dissection (ALND) and Sentinel lymph node biopsy (SLNB). ALND has traditionally been the standard surgical approach for patients with node-positive BC. However, recent research indicates that SLNB may provide a less invasive option with a reduced risk of complications, including lymphedema (51).
Lymphedema is a common complication of axillary surgery that can significantly impact patients’ quality of life. Research indicates that SLNB is associated with a lower incidence of lymphedema than ALND (52). This finding is especially pertinent for women with node-negative BC, as SLNB provides an effective method for axillary staging while concurrently minimizing the risk of developing lymphedema (53).
The management of postoperative lymphedema generally encompasses a multifaceted approach, including physical therapy, the use of compression garments, and instruction in patient self-care methodologies. Furthermore, current clinical trials are investigating the potential of axillary radiation therapy as an alternative to surgical clearance in specific patient cohorts, which may contribute to a decreased incidence of lymphedema (54).
A thorough grasp of lymph node surgery and lymphedema treatment impacts is crucial for enhancing therapeutic results and quality of life in BC survivors. As the field progresses, it is imperative to develop individualized treatment plans that take into account the specific circumstances and preferences of patients in order to effectively address the complexities associated with BC care (55, 56).
4.8 Limitations
This study is constrained by its reliance on the PubMed database, which may introduce potential publication bias. Furthermore, the cutoff date for the statistics is August 7, 2024, potentially leading to incomplete publication data for the year 2024 and consequently impacting the reliability of the reported findings. Moreover, this study sought to incorporate literature of high relevance to BC surgery to enhance the credibility of the research findings. However, this focus may have resulted in the exclusion of other pertinent literature related to BC surgery. We recognize this limitation and commit to examining a more comprehensive array of literature in future research endeavors.
5 Conclusion
This study utilized “bibliometrix” package for a visual analysis of literature on BC surgery. This approach provided a comprehensive overview of the research landscape, highlighting key themes and emerging trends in the field over the past 25 years. The analysis revealed that China, the United States, the University of California, author Christine Miaskowski, the journal *Annals of Surgical Oncology*, and two seminal papers have significantly influenced the field’s development. We identified key thematic areas, namely “BC,” “pain,” “anxiety,” “lymphedema,” “mastectomy,” and “surgery,” and analyzed the five clusters associated with these themes, offering novel insights for research in this domain. This study is timely in guiding future research trajectories in the field, although it is not without limitations. Future investigations should broaden the range of databases consulted, incorporate a greater number of high-quality articles, and enhance the data support for research pertaining to BC surgery.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The patient data used in this study came from datasets that were made publically available and included complete patient informed consent.
Author contributions
JK: Data curation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. NJ: Data curation, Validation, Writing – original draft. MS: Data curation, Writing – original draft. TT: Funding acquisition, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The research was supported by Natural Science Foundation of Xinjiang Uyghur Autonomous Region - Youth Science Foundation, (2022D01C277), China.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
BC, Breast cancer; BCS, Breast-conserving surgery; SLNB, Sentinel lymph node biopsy; ALND, Axillary lymph node dissection; RA, Regional Anesthesia; DCIS, Ductal carcinoma in situ.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA: Cancer J Clin. (2020) 70:7–30. doi: 10.3322/caac.21590
2. Nelson JA, Rubenstein RN, Haglich K, Chu JJ, Yin S, Stern CS, et al. Analysis of a trend reversal in US lumpectomy rates from 2005 through 2017 using 3 nationwide data sets. JAMA Surg. (2022) 157:702–11. doi: 10.1001/jamasurg.2022.2065
3. Franceschini G, Scardina L, Visconti G, Hayashi A, Masetti R. Editorial: update of current evidences in breast cancer surgery. Front Oncol. (2022) 12:928467. doi: 10.3389/fonc.2022.928467
4. Mazzocco K, Marzorati C, Pravettoni G. Professor Umberto Veronesi: a physician, a researcher, a brilliant man. Ecancermedicalscience. (2017) 11:742. doi: 10.3332/ecancer.2017.742
5. Duma MN. An update on regional nodal irradiation: indication, target volume delineation, and radiotherapy techniques. Breast Care (Basel Switzerland). (2020) 15:128–35. doi: 10.1159/000507040
6. Westcott LZ, Jones RC, Fleshman JW Jr. Development of the breast surgical oncology fellowship in the United States. Breast J. (2022) 2022:3342910. doi: 10.1155/2022/3342910
7. Zhang Q, Wu Y, An H, Feng Y. Postoperative recovery after breast cancer surgery: A randomised controlled trial of opioid-based versus opioid-free anaesthesia with thoracic paravertebral block. Eur J anaesthesiology. (2023) 40:552–9. doi: 10.1097/EJA.0000000000001856
8. Bornmann L, Mutz R. Growth rates of modern science: A bibliometric analysis based on the number of publications and cited references. J Assoc Inf Sci Technol. (2015) 66:2215–22. doi: 10.1002/asi.23256
9. Bornmann L, Daniel HD. Mapping scientific collaborations: A bibliometric analysis of Erasmus Mundus joint doctorate theses. J Informetrics. (2013) 7:281–93. doi: 10.1016/j.joi.2013.01.002
10. Hossain L, Ahmed SA. A bibliometric analysis of research trends, collaboration, and research output in the field of information systems. J Informetrics. (2017) 11:949–69. doi: 10.1016/j.joi.2017.08.006
11. Hamad AA, Jaradat JH, Alsalhi HK, Alkhawaldeh IM. Medical research production in native languages: A descriptive analysis of PubMed database. Qatar Med J. (2024) 54:21. doi: 10.5339/qmj.2024.21
12. D'Souza J, Ng V. Classifying temporal relations in clinical data: A hybrid, knowledge-rich approach. J Biomed Inf. (2013) 46:S29–39. doi: 10.1016/j.jbi.2013.08.003
13. Aria M, Cuccurullo C. Bibliometrix: An R-tool for comprehensive science mapping analysis. J Informetrics. (2017) 11:959–75. doi: 10.1016/j.joi.2017.04.002
14. Ogunsakin RE, Ebenezer O, Ginindza TG. A bibliometric analysis of the literature on Norovirus disease from 1991-2021. Int J Environ Res Public Health. (2022) 19(5):2508. doi: 10.3390/ijerph19052508
15. Musa HH, Musa TH. A systematic and thematic analysis of the top 100 cited articles on mRNA vaccine indexed in Scopus database. Hum Vaccin Immunother. (2022) 18(6):2135927. doi: 10.1080/21645515.2022.2135927
16. Volpe S, Mastroleo F, Krengli M, Jereczek-Fossa BA. Quo vadis radiomics? Bibliometric analysis of 10-year Radiomics journey. Eur Radiol. (2023) 33(10):6736–45. doi: 10.1007/s00330-023-09645-6
17. Lowery AJ, Kell MR, Glynn RW, Kerin MJ, Sweeney KJ. Locoregional recurrence after breast cancer surgery: a systematic review by receptor phenotype. Breast Cancer Res Treat. (2012) 133:831–41. doi: 10.1007/s10549-011-1891-6
18. Fillon M. Perioperative management may lead to less pain after breast cancer surgery. CA: Cancer J Clin. (2019) 69:5–6. doi: 10.3322/caac.21465
19. Gärtner R, Jensen MB, Nielsen J, Ewertz M, Kroman N, Kehlet H. Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA. (2009) 302:1985–92. doi: 10.1001/jama.2009.1568
20. McCann B, Miaskowski C, Koetters T, Baggott C, West C, Levine JD, et al. Associations between pro- and anti-inflammatory cytokine genes and breast pain in women prior to breast cancer surgery. J Pain. (2012) 13:425–37. doi: 10.1016/j.jpain.2011.02.358
21. Khan JS, Ladha KS, Abdallah F, Clarke H. Treating persistent pain after breast cancer surgery. Drugs. (2020) 80:23–31. doi: 10.1007/s40265-019-01227-5
22. Wylde V, Dennis J, Beswick AD, Bruce J, Eccleston C, Howells N, et al. Systematic review of management of chronic pain after surgery. Br J Surg. (2017) 104:1293–306. doi: 10.1002/bjs.10601
23. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet (London England). (2019) 393:1537–46. doi: 10.1016/S0140-6736(19)30352-6
24. Bruce J, Thornton AJ, Scott NW, Marfizo S, Powell R, Johnston M, et al. Chronic preoperative pain and psychological robustness predict acute postoperative pain outcomes after surgery for breast cancer. Br J Cancer. (2012) 107:937–46. doi: 10.1038/bjc.2012.341
25. Andersen KG, Duriaud HM, Jensen HE, Kroman N, Kehlet H. Predictive factors for the development of persistent pain after breast cancer surgery. Pain. (2015) 156:2413–22. doi: 10.1097/j.pain.0000000000000298
26. Wong HY, Pilling R, Young BWM, Owolabi AA, Onwochei DN, Desai N. Comparison of local and regional anesthesia modalities in breast surgery: A systematic review and network meta-analysis. J Clin Anesth. (2021) 72:110274. doi: 10.1016/j.jclinane.2021.110274
27. Carli F, Kehlet H, Baldini G, Steel A, McRae K, Slinger P, et al. Evidence basis for regional anesthesia in multidisciplinary fast-track surgical care pathways. Regional Anesth Pain Med. (2011) 36:63–72. doi: 10.1097/AAP.0b013e31820307f7
28. Katsnelson G, Brenna CTA, Girón-Arango L, Abdallah YM, Brull R. Analgesic benefits of regional anesthesia in the perioperative management of transition-related surgery: a systematic review. Regional Anesth Pain Med. (2024), rapm–2024-105479. doi: 10.1136/rapm-2024-105479
29. Chhabra A, Roy Chowdhury A, Prabhakar H, Subramaniam R, Arora MK, Srivastava A, et al. Paravertebral anaesthesia with or without sedation versus general anaesthesia for women undergoing breast cancer surgery. Cochrane Database systematic Rev. (2021) 2:CD012968. doi: 10.1002/14651858.CD012968.pub2
30. Patnaik R, Chhabra A, Subramaniam R, Arora MK, Goswami D, Srivastava A, et al. Comparison of paravertebral block by anatomic landmark technique to ultrasound-guided paravertebral block for breast surgery anesthesia: A randomized controlled trial. Regional Anesth Pain Med. (2018) 43:385–90. doi: 10.1097/AAP.0000000000000746
31. Uppal V, Sondekoppam RV, Sodhi P, Johnston D, Ganapathy S. Single-injection versus multiple-injection technique of ultrasound-guided paravertebral blocks: A randomized controlled study comparing dermatomal spread. Regional Anesth Pain Med. (2017) 42:575–81. doi: 10.1097/AAP.0000000000000631
32. Abdallah FW, Morgan PJ, Cil T, McNaught A, Escallon JM, Semple JL, et al. Ultrasound-guided multilevel paravertebral blocks and total intravenous anesthesia improve the quality of recovery after ambulatory breast tumor resection. Anesthesiology. (2014) 120:703–13. doi: 10.1097/ALN.0000436117.52143.bc
33. Heesen M, Klimek M, Rossaint R, Imberger G, Straube S. Paravertebral block and persistent postoperative pain after breast surgery: meta-analysis and trial sequential analysis. Anaesthesia. (2016) 71:1471–81. doi: 10.1111/anae.13649
34. Jin Z, Durrands T, Li R, Gan TJ, Lin J. Pectoral block versus paravertebral block: a systematic review, meta-analysis and trial sequential analysis. Regional Anesth Pain Med. (2020) 45:727–32. doi: 10.1136/rapm-2020-101512
35. Hanson SE, Lei X, Roubaud MS, DeSnyder SM, Caudle AS, Shaitelman SF, et al. Long-term quality of life in patients with breast cancer after breast conservation vs mastectomy and reconstruction. JAMA Surg. (2022) 157:e220631. doi: 10.1001/jamasurg.2022.0631
36. Walton L, Ommen K, Audisio RA. Breast reconstruction in elderly women breast cancer: a review. Cancer Treat Rev. (2011) 37:353–7. doi: 10.1016/j.ctrv.2011.02.001
37. Santosa KB, Qi J, Kim HM, Hamill JB, Pusic AL, Chun YS, et al. Comparing nipple-sparing mastectomy to secondary nipple reconstruction: A multi-institutional study. Ann Surg. (2021) 274:390–5. doi: 10.1097/SLA.0000000000003577
38. Browne JP, Jeevan R, Gulliver-Clarke C, Pereira J, Caddy CM, van der Meulen JHP. The association between complications and quality of life after mastectomy and breast reconstruction for breast cancer. Cancer. (2017) 123:3460–7. doi: 10.1002/cncr.30788
39. Garcia-Etienne CA, Forcellini D, Sagona A, Caviggioli F, Barbieri E, Cornegliani G, et al. Breast reconstruction: a quality measure for breast cancer care? Breast (Edinburgh Scotland). (2012) 21:105–6. doi: 10.1016/j.breast.2011.08.133
40. Ng ET, Ang RZ, Tran BX, Ho CS, Zhang Z, Tan W, et al. Comparing quality of life in breast cancer patients who underwent mastectomy versus breast-conserving surgery: A meta-analysis. Int J Environ Res Public Health. (2019) 16:4970. doi: 10.3390/ijerph16244970
41. Aygin D, Cengiz H. Life quality of patients who underwent breast reconstruction after prophylactic mastectomy: systematic review. Breast Cancer (Tokyo Japan). (2018) 25:497–505. doi: 10.1007/s12282-018-0862-8
42. Oei SL, Thronicke A, Grieb G, SChad F, Groß J. Evaluation of quality of life in breast cancer patients who underwent breast-conserving surgery or mastectomy using real-world data. Breast Cancer (Tokyo Japan). (2023) 30:1008–17. doi: 10.1007/s12282-023-01494-x
43. Lan L, Xia Y, Li R, Liu K, Mai J, Medley JA, et al. A fiber optoacoustic guide with augmented reality for precision breast-conserving surgery. Light Sci Appl. (2018) 7:2. doi: 10.1038/s41377-018-0006-0
44. Hassett MJ, Jiang W, Hughes ME, Edge S, Javid SH, Niland JC, et al. Treating second breast events after breast-conserving surgery for ductal carcinoma in situ. J Natl Compr Cancer Network: JNCCN. (2018) 16:387–94. doi: 10.6004/jnccn.2018.7003
45. Cyr A. Toward less-invasive management of early-stage breast cancer. J Natl Compr Cancer Network: JNCCN. (2015) 13:646–8. doi: 10.6004/jnccn.2015.0192
46. Zhang YQ, Liu WL, Luo XJ, Shi JP, Zeng YZ, Chen WL, et al. Novel self-assembled multifunctional nanoprobes for second-near-infrared-fluorescence-image-guided breast cancer surgery and enhanced radiotherapy efficacy. Advanced Sci (Weinheim Baden-Wurttemberg Germany). (2023) 10:e2205294. doi: 10.1002/advs.202205294
47. Gong P, Chin SL, Allen WM, Ballal H, Anstie JD, Chin L, et al. Quantitative micro-elastography enables in vivo detection of residual cancer in the surgical cavity during breast-conserving surgery. Cancer Res. (2022) 82:4093–104. doi: 10.1158/0008-5472.CAN-22-0578
48. Wilson KE, Bachawal SV, Willmann JK. Intraoperative resection guidance with photoacoustic and fluorescence molecular imaging using an anti-B7-H3 antibody-indocyanine green dual contrast agent. Clin Cancer research: an Off J Am Assoc Cancer Res. (2018) 24:3572–82. doi: 10.1158/1078-0432.CCR-18-0417
49. Grootendorst MR, Cariati M, Pinder SE, Kothari A, Douek M, Kovacs T, et al. Intraoperative assessment of tumor resection margins in breast-conserving surgery using 18F-FDG cerenkov luminescence imaging: A first-in-human feasibility study. J Nucl medicine: Off publication Soc Nucl Med. (2017) 58:891–8. doi: 10.2967/jnumed.116.181032
50. Tosello G, Torloni MR, Mota BS, Neeman T, Riera R. Breast surgery for metastatic breast cancer. Cochrane Database systematic Rev. (2018) 3:CD011276. doi: 10.1002/14651858.CD011276.pub2
51. Bundred NJ, Barnes NL, Rutgers E, Donker M. Is axillary lymph node clearance required in node-positive breast cancer? Nat Rev Clin Oncol. (2015) 12:55–61. doi: 10.1038/nrclinonc.2014.188
52. Sackey H, Magnuson A, Sandelin K, Liljegren G, Bergkvist L, Fülep Z, et al. Arm lymphoedema after axillary surgery in women with invasive breast cancer. Br J Surg. (2014) 101:390–7. doi: 10.1002/bjs.9401
53. Black DM, Jiang J, Kuerer HM, Buchholz TA, Smith BD. Racial disparities in adoption of axillary sentinel lymph node biopsy and lymphedema risk in women with breast cancer. JAMA Surg. (2014) 149:788–96. doi: 10.1001/jamasurg.2014.23
54. Naoum GE, Roberts S, Brunelle CL, Shui AM, Salama L, Daniell K, et al. Quantifying the impact of axillary surgery and nodal irradiation on breast cancer-related lymphedema and local tumor control: long-term results from a prospective screening trial. J Clin oncology: Off J Am Soc Clin Oncol. (2020) 38:3430–8. doi: 10.1200/JCO.20.00459
55. Voutsadakis IA, Spadafora S. Recommendation for omitting axillary lymph node dissection should be individualized in patients with breast cancer with one or two positive sentinel lymph nodes. J Clin oncology: Off J Am Soc Clin Oncol. (2014) 32:3901–2. doi: 10.1200/JCO.2014.57.1190
Keywords: breast cancer surgery, bibliometric analysis, research hotspots, international collaboration, publication patterns
Citation: Kang J, Jiang N, Shataer M and Tuersong T (2024) Research progress of breast cancer surgery during 2010–2024: a bibliometric analysis. Front. Oncol. 14:1508568. doi: 10.3389/fonc.2024.1508568
Received: 09 October 2024; Accepted: 22 November 2024;
Published: 09 December 2024.
Edited by:
Isabella Castellano, University of Turin, ItalyReviewed by:
Francesca Combi, University of Modena and Reggio Emilia, ItalyMatteo Ghilli, Pisana University Hospital, Italy
Copyright © 2024 Kang, Jiang, Shataer and Tuersong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tayier Tuersong, dGF5aWVydHVlcnNvbmdAMTYzLmNvbQ==