 Maximilian Richter1*
Maximilian Richter1* Christian Doll1
Christian Doll1 Friedrich Mrosk1
Friedrich Mrosk1 Elena Hofmann1,2
Elena Hofmann1,2 Steffen Koerdt1
Steffen Koerdt1 Max Heiland1
Max Heiland1 Konrad Neumann3
Konrad Neumann3 Marcus Beck4
Marcus Beck4 Steffen Dommerich5
Steffen Dommerich5 Korinna Jöhrens6†
Korinna Jöhrens6† Jan-Dirk Raguse7†
Jan-Dirk Raguse7†- 1Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Department of Oral and Maxillofacial Surgery, Berlin, Germany
- 2Berlin Institute of Health at Charité – Universitätsmedizin Berlin, BIH Biomedical Innovation Academy, BIH Charité Junior Clinician Scientist Program, Berlin, Germany
- 3Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Institute of Biometry and Clinical Epidemiology, Berlin, Germany
- 4Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Department of Radiooncology and Radiotherapy, Berlin, Germany
- 5Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Department of Otorhinolaryngology, Berlin, Germany
- 6Institute of Pathology, Klinikum Chemnitz, Chemnitz, Germany
- 7Department of Oral and Maxillofacial Surgery, Fachklinik Hornheide, Münster, Germany
Objective: Despite numerous studies addressing the impact of p16INK4a in oral squamous cell carcinoma (OSCC), consistent data regarding survival and tumor proliferation behavior are lacking. Although some authors investigate both p16INK4a and Mib/Ki-67 in their cohorts, direct correlations are consistently missing. The aim of this study was to investigate the combined influence of p16INK4a and Mib/Ki-67 status on prognosis in OSCC.
Materials and methods: Clinical data of all patients diagnosed with OSCC and treated curatively between 2005 and 2011 were collected retrospectively. Tissue microarrays of formalin-fixed paraffin-embedded specimens were stained for p16INK4a and Mib/Ki-67 using the CINtec Histology V-Kit or MIB-1 antibody and correlated with the clinical outcome.
Results: A total of 316 patients, with a mean age of 61.7 years were included. Tumor tissues that were tested p16INK4a positive with low Mib/Ki-67 expression demonstrated a remarkable 5-year survival rate of 83% with an improved RFS compared to all other subgroups (p=0.034; p=0.017; p=0.026) and an improved OS compared to those with high Mib/Ki-67 expression (p=0.026; p=0.020). Cox regression identified the combined p16INK4a and Mib/Ki-67 status as a risk factor on OS (HR 6.25; CI1.26-31.0; p=0.025) and RFS (HR 5.88; CI1.19-29.20; p=0.030).
Conclusion: These results underscore the importance of a combined assessment of p16INK4a and Mib/Ki-67 in evaluating the prognosis of OSCC, leading to the identification of distinct subgroups that may serve as risk factors for treatment stratification.
Introduction
Oral squamous cell carcinoma (OSCC) is a form of epithelial cancer that originates from the mucosal surface of the mouth and represents the most prevalent type of oral cancer (1). Globally, 389,846 new cases of oral and lip carcinomas were diagnosed in 2022, accounting for approximately 2% of all malignant tumors (2). While developing countries such as India and Sri Lanka exhibit decreasing incidence rates, nations with historically low disease rates have observed an increase in incidence, placing significant strain on their healthcare systems (3).
In addition to well-established risk factors like tobacco use and alcohol consumption (4), the role of human papillomavirus (HPV) and/or p16INK4a status remains poorly understood and requires further investigation. A deeper understanding of these risk factors could potentially lead to optimized risk-adjusted treatments and improved outcomes.
Given the context of low survival rates, factors such as tumor size and depth of invasion are long known prognostic indicators (5, 6). Furthermore, the impact of cell proliferation has been studied extensively by various authors. Expression of Ki-67, a widely accepted and practical tool for assessing the proportion of proliferating cells, was initially described in 1983 (7). Located on Chromosome 10, Ki-67 plays a major role in mitosis and is present in all proliferating cells, while being absent in resting cells (8). A meta-analysis published in 2016 indicated an adverse impact on overall survival (OS) and disease-free survival in OSCC with high Ki-67 positivity (9). Given the limited sample sizes and heterogeneity of the included studies, particularly regarding the use of different antibodies/methods and encompassing diverse ethnicities, further investigations are needed (9).
In contrast, there is a discrepancy in data regarding the influence of p16INK4a positivity in OSCC. Acting as a cell cycle protein, increased expression of p16INK4a naturally inhibits cyclin-dependent kinases, thereby inducing cellular senescence (10). While a beneficial prognostic effect of increased p16INK4a has been demonstrated in oropharyngeal squamous cell carcinoma (OPSCC) (11), alongside an association with HPV status (12), this correlation does not seem to apply to OSCC, with most authors reported no influence of p16INK4a status on survival (13, 14).
The integration of a combined assessment of p16INK4a and Mib/Ki-67 status, known as dual-staining, has been implemented in the early detection of pathologies in cytological sections of the cervix uteri (15). The distinctive decoupling, which demonstrates a high proliferation rate despite increased p16INK4a expression, has led to an improved identification of cervical intraepithelial neoplasia (15). Similar findings have been observed in tumors of the head and neck region, suggesting an enhanced detection of the malignant transformation of oral submucous fibrosis (16). Nevertheless, a significant impact on survival has not been confirmed for OSCC (17).
The aim of this study was to evaluate the prognostic role of combined p16INK4a and Mib/Ki-67 assessment in a substantial cohort of patients with OSCC.
Patients and methods
Ethics statement
The Ethics Committee of the Faculty of Medicine Charité - Universitätsmedizin Berlin approved this study (EA2/028/15).
Data collection
Clinical data of all patients diagnosed with curatively treated OSCC between 2005 and 2011 were collected retrospectively including TNM stage, age, gender, survival time and treatment regime. In case of a surgical treatment further information especially the pathological TNM was recorded.
OS was defined as the time span between the date of initial diagnosis (or, if not available, the date of therapy initiation) and the date of death or was censored at the date of the last contact.
Recurrence-free survival (RFS) was described as the time span from the end of therapy until the occurrence of a recurrence or until the time of death. In contrast, tumors that recurred within the first six months after surgery with R1/Rx status or primary radio(chemo)therapy were classified as residual tumors and were excluded from RFS analysis.
Patients receiving palliative care, those who underwent only a single induction therapy, those who received no therapy, or those who discontinued radiochemotherapy were not considered.
Immunohistochemical staining
Immunohistochemical analyses were performed using tissue microarrays (TMAs). Initially, archived formalin-fixed paraffin-embedded specimens were retrieved and marked based on the hematoxylin-eosin-stained sections of the tumor. Representative sections were transferred using 1 or 2 punches (1.2 mm in diameter), depending on tumor size. In total, 15 TMAs were produced, each containing 66 punches. The subsequent evaluation of the immunohistochemical stainings, as described below, was carried out by two independent examiners.
p16INK4a analysis
The CINtec Histology V-Kit (Roche, Switzerland), an antibody against the E6H4 epitope, was used for immunohistochemical staining. The staining process was fully automated using the Ultraview DAB procedure of the VENTANA BenchMark ULTRA staining system (Roche, Switzerland). In accordance with Prigge et al., tumors were considered p16INK4a positive if at least 70% of tumor cells exhibit cytoplasmic and/or nuclear expression and demonstrate at least moderate staining intensity (18).
Mib/Ki-67 analysis
Following cell conditioning with ULTRA Cell Conditioning Solution (Ventana, USA; Roche, Switzerland), immunohistochemical staining was performed using the MIB-1 antibody (Agilent, USA), a monoclonal antibody for a 1002 bp fragment of the Ki-67 cDNA, at a ratio of 1:50. The staining process was fully automated using the Ultraview DAB procedure of the VENTANA BenchMark ULTRA staining system (Roche, Switzerland). Referring to the publication by Lange et al., a threshold value of ≥37% was defined as Mib/Ki-67 positive (19).
HPV DNA analysis
Samples defined p16INK4a positive were examined for the presence of HPV DNA. DNA extraction was performed on formalin-fixed samples using the Maxwell RSC DNA FFPE Kit (Promega, Germany). For DNA amplification, a polymerase chain reaction (PCR) was conducted (denaturation at 95°C for 5 minutes, amplification with a total of 45 cycles, and elongation at 72°C for 7 minutes). HPV typing was then carried out using the HPV 3.5 LCD-Array Kit (Chipron, Germany; TIB Molbiol, Germany) to detect specific regions of the L1 gene. This method allows for the identification of HPV types 6, 11, 16, 18, 31, 33, 35, 39, 42, 44, 45, 51, 52, 53, 54, 56, 58, 59, 61, 62, 66, 67, 68, 70, 72, 73, 81, 82, 83, 84, 90, and 91.
Statistical analysis
Data were collected using Microsoft Excel version 15 (Microsoft Corporation, Redmond, WA, USA) and analyzed with IBM SPSS Statistics version 27 and R version 4.0.3 (20). Categorical variables were presented as frequency and percentage, while continuous variables were expressed as mean values. Frequencies of categorical or ordinal variables were compared using the chi-square test, or Fisher’s exact test when expected frequencies were less than 5.
Overall survival (OS) and relapse-free survival (RFS) were analyzed using the Kaplan-Meier method and compared with the log-rank test. Multivariate Cox regression analysis was conducted to evaluate combined p16INK4a and Mib status as risk factors. All p-values are exploratory and have not been adjusted for multiple comparisons. Statistical significance was determined at a threshold of α=0.05, with p-values below this threshold considered significant.
Results
A total of 316 patients (female: 110 (34.8%), male: 206 (65.2%)) met the inclusion criteria with an average age of 61.7 years (SD ±12.0 years; range 27-96 years) at initial diagnosis. The therapies included surgery without an adjuvant therapy (n=201, 63.6%), followed by surgery with adjuvant therapy (n=75; 23.7%) and primary radio(chemo)therapy (n=40; 12.7%).
The mean OS in this cohort was 79.9 months (CI: 73.9-85.9 months), with a 5-year survival rate of 59%. RFS (as defined above) was 66.3 months (CI: 60.2-72.4 months).
p16INK4a analysis
Only 21 out of 316 tumors (6.6%) tested positive for p16INK4a. Patients with p16INK4a positive and p16INK4a negative tumors exhibited no differences in the clinical parameters examined (Table 1). Survival analysis revealed better OS for patients with p16INK4a positive tumors, with a 10-year survival rate of 60% (OS: 87.6 months; CI: 63.7-111.4), compared to patients with p16INK4a negative tumors, who demonstrated a 10-year survival rate of 39% (OS: 79.2 months; CI: 73.1-85.4). However, this difference was not statistically significant (p=0.359). Similarly, in terms of RFS, we observed comparable trends, with a better survival of 80.6 months in p16INK4a positive tumors (compared to 65.2 months in p16INK4a negative tumors, p=0.194).
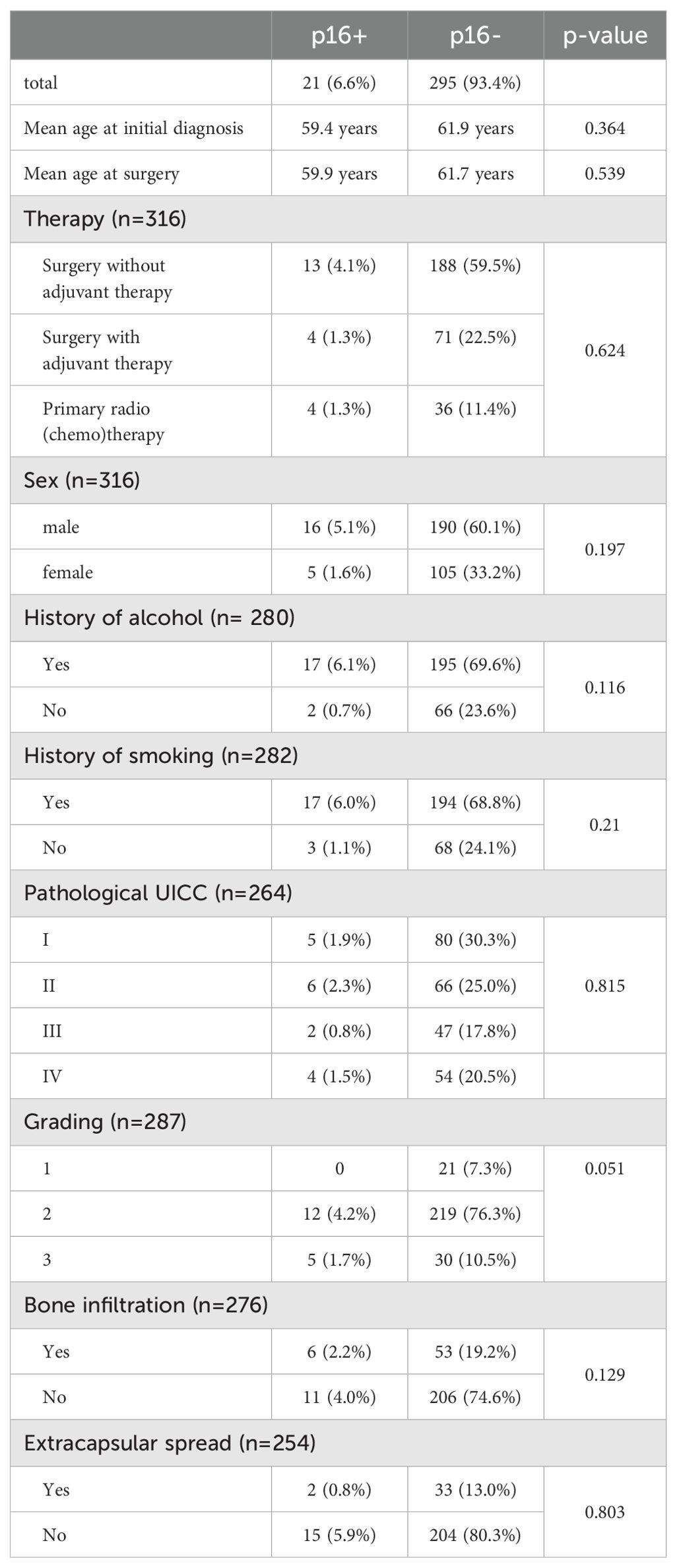
Table 1. Clinical characteristics in patients with p16INK4a positive and p16INK4a negative tumors.
For the analysis of HPV DNA, 18 of 21 p16INK4a positive samples were available. Amplification could not be detected in 4 cases. In 5 of the remaining 14 p16INK4a positive samples (35.7%), HPV was successfully detected (in all cases HPV 16 DNA).
When analyzing OS/RFS regarding type of therapy, we found no statistically significant differences between p16INK4a positive and p16INK4a negative tumors in patients who received surgery without adjuvant therapy (p=0.532/p=0.430), surgery with adjuvant therapy (p=0.198/0.152) or primary radio(chemo)therapy (p=0.544/p=0.433).
Mib/Ki-67 analysis
The mean Mib/Ki-67 expression was 28.3% (SD ±17.3%) tested in 316 tumors.
When analyzing the mean Mib/Ki-67 positivity depending on the grading we found significant differences between G1 (Mib/Ki-67 expression: 11.8%) and G2 tumors (Mib/Ki-67 expression: 29.0%, p<0.001) and between G1 and G3 tumors (Mib/Ki-67 expression: 33.0%, p<0.001).
However, in the entire cohort, no cut-off value could be identified that showed a significant influence on the OS or RFS. When performing survival analysis for respective therapy regiments with a cut-off value of 37%, we found no significant differences in OS or RFS between Mib/Ki-67 positive and negative tumors in patients who underwent surgery without adjuvant therapy (p=0.061/p=0.103), surgery with adjuvant therapy (p=0.857/p=0.944) or primary radio(chemo)therapy (p=0.471/p=0.311).
Combined assessment of p16INK4a and Mib/Ki-67
Next, subanalyses were conducted for the combined assessment of p16INK4a and Mib/Ki-67.
The mean Mib/Ki-67 positivity in the 21 patients that tested positive for p16INK4a was 32.5% (SD ±17.4%) compared to 28.0% (SD ±17.2%) in the 295 patients with p16INK4a negative tumors (p=0.240). No differences in proliferation rates were found between tumors with predominantly nuclear p16INK4a expression (n=11) and those with primarily cytoplasmic or balanced expression (n=10; p=0.194).
A cut-off value in the Mib/Ki-67 immunohistochemistry of 37% based on Lange et al. (19) was selected to divide the cohort into four subgroups: p16INK4a positive/Mib positive (p16+/Mib+), p16INK4a positive/Mib negative (p16+/Mib-), p16INK4a negative/Mib negative (p16-/Mib-) and p16INK4a negative/Mib positive (p16-/Mib+) tumors.
Regarding clinical characteristics or HPV DNA detection we found no significant differences between p16+/Mib+ and p16+/Mib- tumors (Table 2).
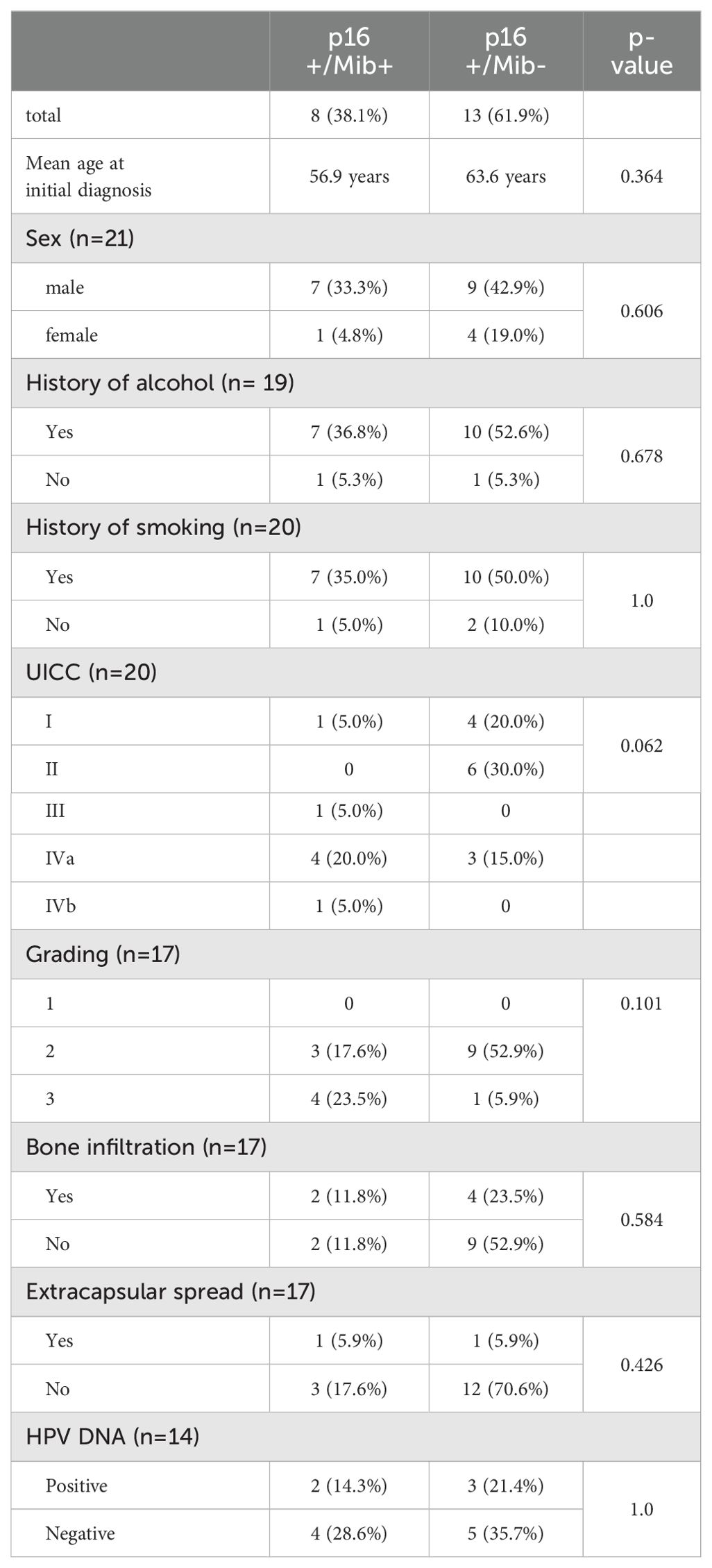
Table 2. Clinical characteristics in patients with p16+/Mib+ and p16+/Mib- tumors.
We observed a significant superiority of p16+/Mib- tumors compared to p16-/Mib+ (p=0.026) and p16+/Mib+ (p=0.020) leading to a 5-year survival rate of 83%. In contrast, p16+/Mib+ showed a 5-year survival rate of 25%, which was even lower than that of p16-/Mib- (59%) or p16-/Mib+ tumors (58%) (Figure 1; Table 3). The combined p16/Mib status emerged as a risk factor for OS in the Cox regression, with a hazard ratio (HR) of 6.25 (CI: 1.26-31.0) in the group of p16+/Mib+ tumors compared to p16+/Mib- tumors (p=0.025) (Table 4).
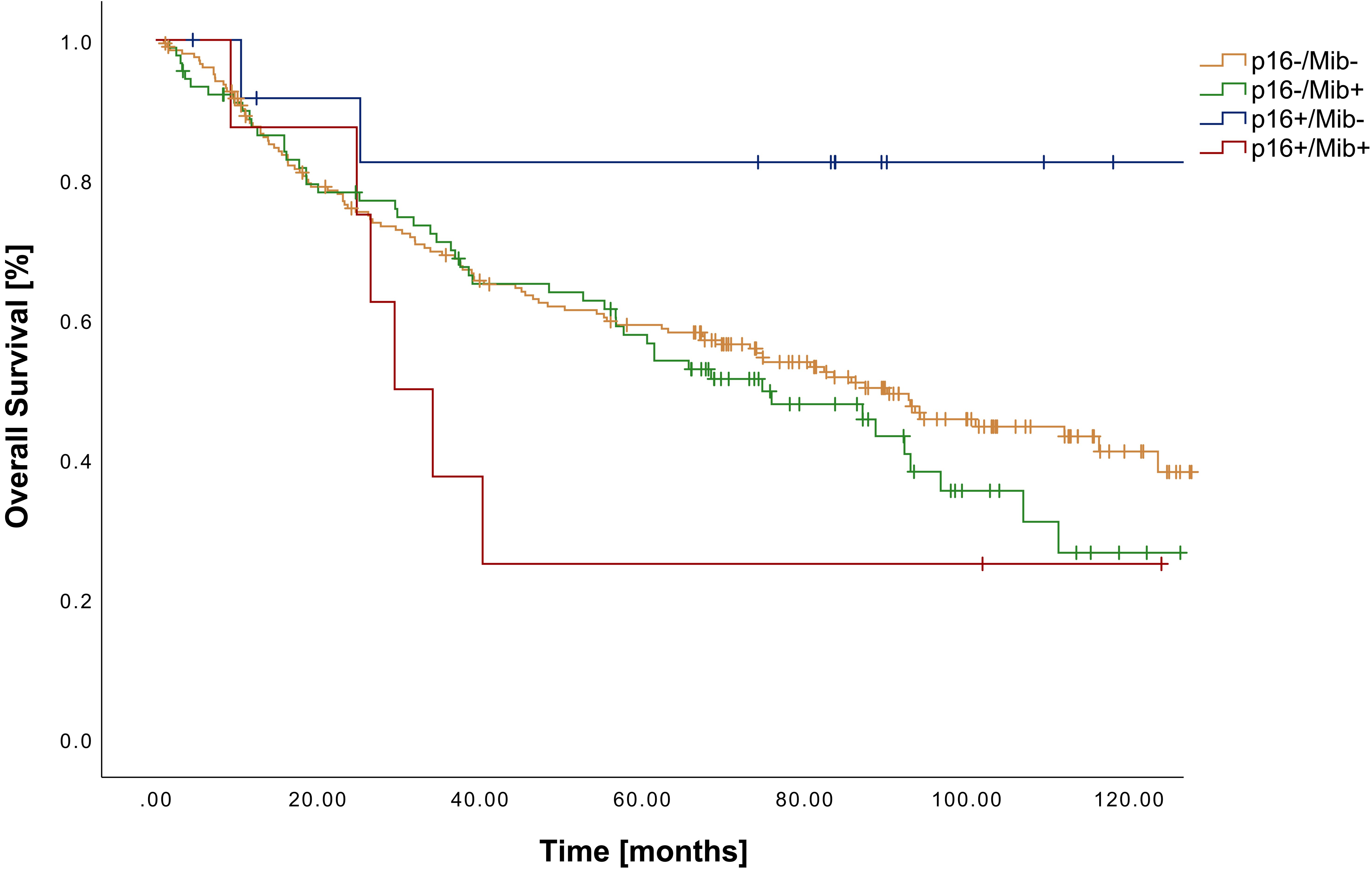
Figure 1. Kaplan-Meier curves showing OS of patients with OSCC in relation to the combined p16INK4a (cut-off ≥70%) and Mib/Ki-67 status (cut-off ≥37%).
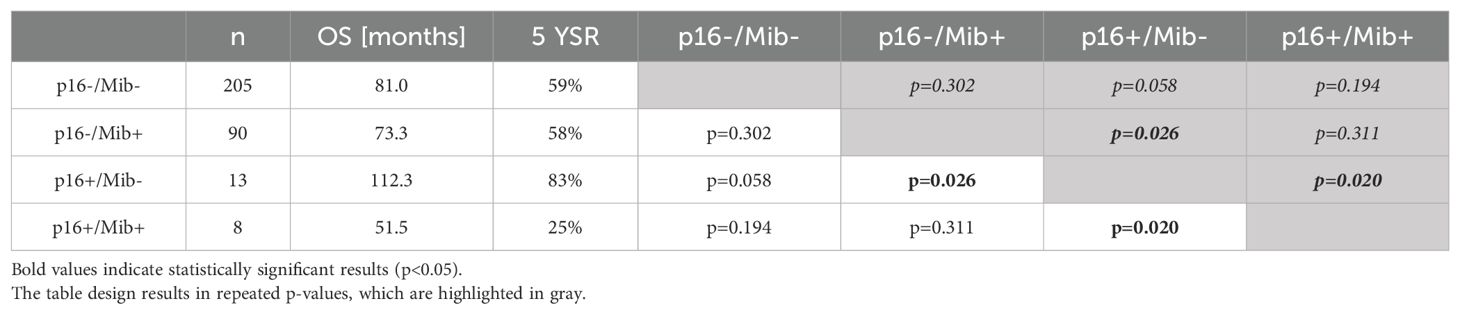
Table 3. OS in relation to the subgrouping of patients according to the combined assessment of p16INK4a and Mib/Ki-67.

Table 4. Cox regression for OS according to the combined assessment of p16INK4a and Mib/Ki-67.
Similar findings were evident in RFS with a statistically significant better outcome in patients with p16+/Mib- tumors compared to p16+/Mib+, p16-/Mib+ and p16-/Mib- tumors (p=0.026; p=0.017; p=0.034) (Figure 2). Mean RFS varied from 106.9 months (CI: 79.6-134.3 months) in p16+/Mib- to 41.7 months (CI: 15.2-68.3 months) in p16+/Mib+ tumors (Table 5). Cox regression showed a HR of 5.88 (CI: 1.19-29.20) in the group of p16+/Mib+ tumors compared to the p16+/Mib- tumors (p=0.030) (Table 6).
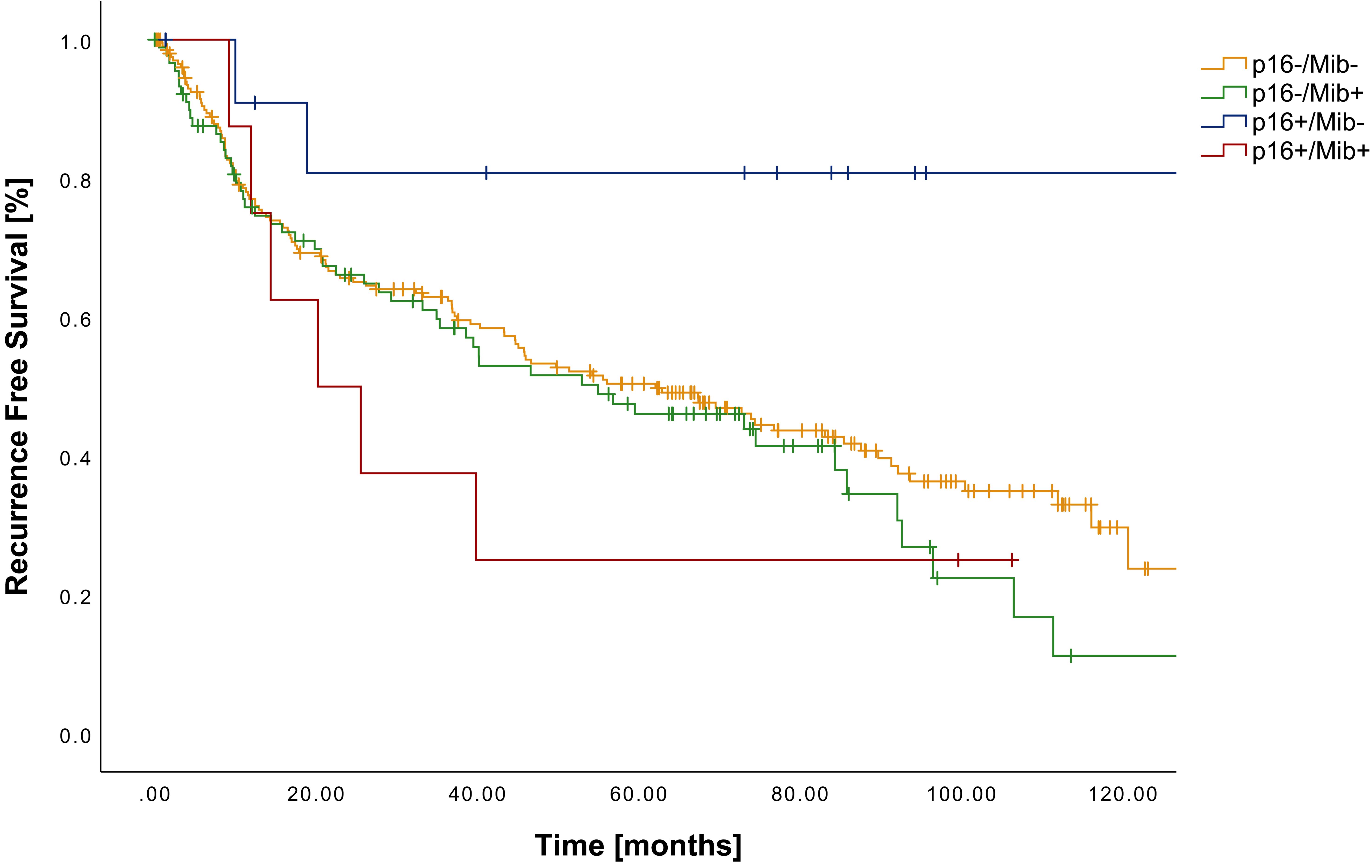
Figure 2. Kaplan-Meier curves showing RFS of patients with OSCC in relation to the combined p16INK4a (cut-off ≥70%) and Mib/Ki-67 status (cut-off ≥37%).
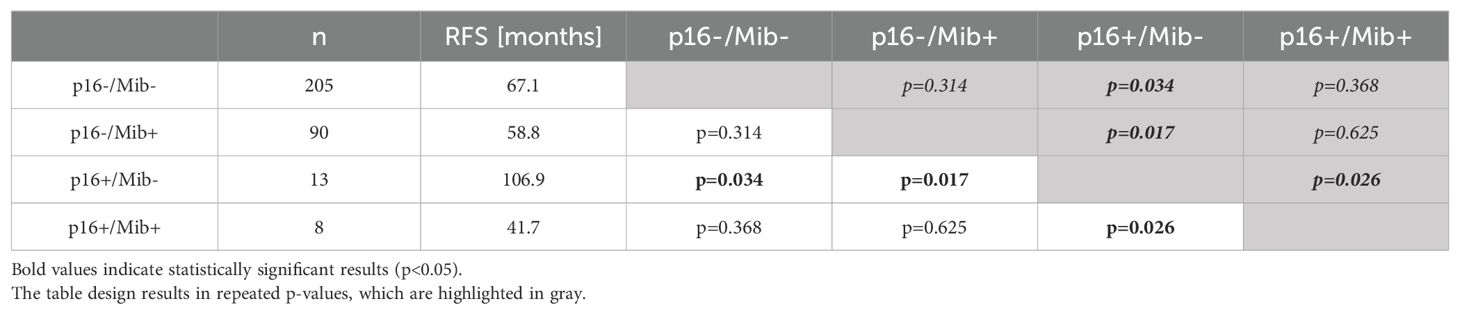
Table 5. RFS in relation to the subgrouping of patients according to the combined assessment of p16INK4a and Mib/Ki-67.

Table 6. Cox regression for RFS according to the combined assessment of p16INK4a and Mib/Ki-67.
Discussion
Nowadays, the role of p16INK4a as a predictor for prognosis in head and neck cancers, especially in OPSCC, is widely accepted (21, 22). However, in OSCC, its role remains unclear, leading to different approaches in implementing it into clinical routines.
Most studies report no significant influence of the p16INK4a status on OS or RFS in OSCC (13, 23). However, there is a divergence of study results, with some authors suggesting a negative (24) or positive (25) prognostic impact. Many authors attribute these discrepancies to varied definitions of p16INK4a positivity and small patient cohorts (26, 27). In our study, we applied a widely accepted definition in a large cohort of 316 patients with OSCC. Even within this sizable group, only 21 tumors (6.6%) tested positive for p16INK4a, demonstrating no significant influence on OS or RFS. In summary, our results concur with the reports that the singular p16INK4a status has a minimal or likely absent influence in OSCC.
Numerous studies have investigated the impact of Mib/Ki-67 in OSCC. Comparable to our results, studies have shown a correlation between the proliferation rate and tumor grading, with higher rates of Mib/Ki-67 positive cells in poorly differentiated carcinomas (28). Similar associations are also found in premalignant stages (29). Furthermore, the heightened responsiveness of proliferating cells to radiation and chemotherapy has been consistently observed, correlating with increased tumor survival rates in cases with elevated Mib/Ki-67 levels (9). Nonetheless, our analysis revealed no influence of the Mib/Ki-67 status on OS or RFS (cut off 37%). The absence of a universally accepted cut-off value necessitates ongoing research efforts to harmonize the interpretation of Mib/Ki-67 immunohistochemical staining results (9). The validation of a consistent cut-off could enhance the reliability of Mib/Ki-67 as a prognostic marker, offering valuable insights into treatment response and aiding clinicians in refining therapeutic strategies for patients with OSCC.
The combined assessment of p16INK4a and Mib/Ki-67, known as dual-staining, has been described already for pathologies of the cervix uteri. A large study by Schmidt et al. showed a significant superiority of the dual-staining compared to HPV testing alone in detection of cervical intraepithelial neoplasia (15). Furthermore, the authors delineated advantages in comparison to singular p16INK4a staining, admitting benefits to the morphology independence of the dual-staining (15). Ziemke and Marquardt found a better specificity and positive predictive value of the dual-staining concerning the presence of intraepithelial neoplasia compared to cytology and HPV testing in low grade dysplasia of the cervix (30).
In neoplasm of the oral cavity there are only a few studies which examine dual-staining.
Bazarsad et al. highlighted the combined assessment of p16INK4a and Mib/Ki-67 as a predictor for the malignant transformation of oral submucous fibrosis in a small collective of 36 patients (16). In context of OSCC, Reuschenbach et al. reported a slightly better survival in p16+/Mib- tumors; however, this finding did not reach statistical significance (17). As in our cohort, no association with HPV could be demonstrated (17). When comparing these results with our data, variations in the definitions of p16INK4a or Mib/Ki-67 positivity must be acknowledged. However, there is a lack of other publications that include the combined assessment of p16INK4a and Mib/Ki-67 regarding the prognosis of OSCC.
Our findings suggest that the role of p16INK4a should be evaluated in the context of Mib/Ki-67 status, leading to entirely different subgroups of OSCC. We hypothesize that a combined assessment of p16INK4a and Mib/Ki-67 could provide an explanation for the observed lack of influence when considering p16INK4a status alone. Nevertheless, it is important to note the reduced statistical power of the analyses due to the small sample size of p16INK4a positive tumors and the need for further investigations to understand the specific biological relationship between p16INK4a and Mib/Ki-67 in OSCC.
In conclusion, the relation between p16INK4a and Mib/Ki-67 must be reevaluated in other cohorts, particularly in those with a higher p16INK4a prevalence, to potentially implement these findings into clinical practice.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by Ethikkommission der Charité – Universitätsmedizin Berlin. The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from primarily isolated as part of your previous study for which ethical approval was obtained. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
MR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft. CD: Conceptualization, Supervision, Validation, Writing – review & editing. FM: Validation, Visualization, Writing – review & editing. EH: Formal analysis, Validation, Writing – review & editing, Visualization. SK: Conceptualization, Supervision, Validation, Writing – review & editing. MH: Project administration, Resources, Supervision, Writing – review & editing. KN: Data curation, Formal analysis, Investigation, Validation, Writing – review & editing. MB: Supervision, Validation, Visualization, Writing – review & editing. SD: Formal analysis, Supervision, Writing – review & editing. KJ: Conceptualization, Formal analysis, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing. JR: Conceptualization, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
This study is part of the doctoral thesis of MR. We thank Birgit Milluks for the great support. During the preparation of this work the author(s) used Chat GPT-4 architecture in order to improve language style and translation. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. El-Naggar AK, Chan JKC, Rubin Grandis J, Takata T, Slootweg PJ, International Agency for Research on Cancer. WHO classification of head and neck tumours. In: World Health Organization classification of tumours, 4th edition. International Agency for Research on Cancer, Lyon (2017). p. 347.
2. Ferlay J, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, et al. Global Cancer Observatory: Cancer Today (2024). Lyon, France: International Agency for Research on Cancer. Available online at: https://gco.iarc.who.int/today (Accessed 18.05.2024).
3. McGuire S. World cancer report 2014. Geneva, Switzerland: world health organization, international agency for research on cancer, WHO press, 2015. Adv Nutr. (2016) 7:418–9. doi: 10.3945/an.116.012211
4. Blot WJ, McLaughlin JK, Winn DM, Austin DF, Greenberg RS, Preston-Martin S, et al. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res. (1988) 48:3282–7.
5. Mucke T, Kanatas A, Ritschl LM, Koerdt S, Tannapfel A, Wolff KD, et al. Tumor thickness and risk of lymph node metastasis in patients with squamous cell carcinoma of the tongue. Oral Oncol. (2016) 53:80–4. doi: 10.1016/j.oraloncology.2015.11.010
6. Pinto FR, de Matos LL, Palermo FC, Kulcsar MA, Cavalheiro BG, de Mello ES, et al. Tumor thickness as an independent risk factor of early recurrence in oral cavity squamous cell carcinoma. Eur Arch Otorhinolaryngol. (2014) 271:1747–54. doi: 10.1007/s00405-013-2704-9
7. Gerdes J, Schwab U, Lemke H, Stein H. Production of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferation. Int J Cancer. (1983) 31:13–20. doi: 10.1002/ijc.2910310104
8. Scholzen T, Gerdes J. The Ki-67 protein: from the known and the unknown. J Cell Physiol. (2000) 182:311–22. doi: 10.1002/(SICI)1097-4652(200003)182:3<311::AID-JCP1>3.0.CO;2-9
9. Xie S, Liu Y, Qiao X, Hua RX, Wang K, Shan XF, et al. What is the prognostic significance of ki-67 positivity in oral squamous cell carcinoma? J Cancer. (2016) 7:758–67. doi: 10.7150/jca.14214
10. Serrano M, Hannon GJ, Beach D. A new regulatory motif in cell-cycle control causing specific inhibition of cyclin D/CDK4. Nature. (1993) 366:704–7. doi: 10.1038/366704a0
11. Fischer CA, Kampmann M, Zlobec I, Green E, Tornillo L, Lugli A, et al. p16 expression in oropharyngeal cancer: its impact on staging and prognosis compared with the conventional clinical staging parameters. Ann Oncol. (2010) 21:1961–6. doi: 10.1093/annonc/mdq210
12. Klussmann JP, Gultekin E, Weissenborn SJ, Wieland U, Dries V, Dienes HP, et al. Expression of p16 protein identifies a distinct entity of tonsillar carcinomas associated with human papillomavirus. Am J Pathol. (2003) 162:747–53. doi: 10.1016/S0002-9440(10)63871-0
13. Nauta IH, Heideman DAM, Brink A, van der Steen B, Bloemena E, Koljenovic S, et al. The unveiled reality of human papillomavirus as risk factor for oral cavity squamous cell carcinoma. Int J Cancer. (2021) 149:420–30. doi: 10.1002/ijc.v149.2
14. Doll C, Steffen C, Beck-Broichsitter B, Richter M, Neumann K, Pohrt A, et al. The prognostic significance of p16 and its role as a surrogate marker for human papilloma virus in oral squamous cell carcinoma: an analysis of 281 cases. Anticancer Res. (2022) 42:2405–13. doi: 10.21873/anticanres.15719
15. Schmidt D, Bergeron C, Denton KJ, Ridder R, European CCSG. p16/ki-67 dual-stain cytology in the triage of ASCUS and LSIL papanicolaou cytology: results from the European equivocal or mildly abnormal Papanicolaou cytology study. Cancer Cytopathol. (2011) 119:158–66. doi: 10.1002/cncy.v119.3
16. Bazarsad S, Zhang X, Kim KY, Illeperuma R, Jayasinghe RD, Tilakaratne WM, et al. Identification of a combined biomarker for Malignant transformation in oral submucous fibrosis. J Oral Pathol Med. (2017) 46:431–8. doi: 10.1111/jop.2017.46.issue-6
17. Reuschenbach M, Kansy K, Garbe K, Vinokurova S, Flechtenmacher C, Toth C, et al. Lack of evidence of human papillomavirus-induced squamous cell carcinomas of the oral cavity in southern Germany. Oral Oncol. (2013) 49:937–42. doi: 10.1016/j.oraloncology.2013.03.451
18. Prigge ES, Arbyn M, von Knebel Doeberitz M, Reuschenbach M. Diagnostic accuracy of p16(INK4a) immunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Int J Cancer. (2017) 140:1186–98. doi: 10.1002/ijc.v140.5
19. Lange D, Heyden A, Lie E, Brandtzaeg P, Boysen M, Clausen O. Lack of prognostic significance for p53-overexpression and Ki-67-immunoreactivity in oral T1-2 squamous cell carcinomas. Oncol Rep. (1997) 4:737–42. doi: 10.3892/or.4.4.737
20. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2020). Available at: https://www.R-project.org/.
21. Liang C, Marsit CJ, McClean MD, Nelson HH, Christensen BC, Haddad RI, et al. Biomarkers of HPV in head and neck squamous cell carcinoma. Cancer Res. (2012) 72:5004–13. doi: 10.1158/0008-5472.CAN-11-3277
22. Ragin CC, Taioli E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: review and meta-analysis. Int J Cancer. (2007) 121:1813–20. doi: 10.1002/ijc.v121:8
23. Ni Y, Zhang X, Wan Y, Dun Tang K, Xiao Y, Jing Y, et al. Relationship between p16 expression and prognosis in different anatomic subsites of OSCC. Cancer biomark. (2019) 26:375–83. doi: 10.3233/CBM-192402
24. Malerova S, Kalfert D, Grega M, Tachezy R, Klozar J, et al. The significance of p16 protein expression in oral squamous cell carcinoma. Epidemiol Mikrobiol Imunol. (2020) 69:64–72.
25. Ghantous Y, Akrish S, Leiser Y, Abu El-Naaj I. The possible role of human papillomavirus infection in the prognosis of oral squamous cell carcinoma in a northern Israel population. Isr Med Assoc J. (2018) 20:155–60.
26. Blahak J, Zelinka J, Gumulec J, Machacek C, Danek Z, Bulik O. HPV, protein p16 and squamous cell carcinoma of the oral cavity. BioMed Pap Med Fac Univ Palacky Olomouc Czech Repub. (2019) 164(3):292-299. doi: 10.5507/bp.2019.026
27. Wang F, Zhang H, Xue Y, Wen J, Zhou J, Yang X, et al. A systematic investigation of the association between HPV and the clinicopathological parameters and prognosis of oral and oropharyngeal squamous cell carcinomas. Cancer Med. (2017) 6:910–7. doi: 10.1002/cam4.2017.6.issue-5
28. Dragomir LP, Simionescu C, Margaritescu C, Stepan A, Dragomir IM, Popescu MR, et al. P53, p16 and Ki67 immunoexpression in oral squamous carcinomas. Rom J Morphol Embryol. (2012) 53:89–93.
29. Takkem A, Barakat C, Zakaraia S, Zaid K, Najmeh J, Ayoub M. Ki-67 prognostic value in different histological grades of oral epithelial dysplasia and oral squamous cell carcinoma. Asian Pac J Cancer Prev. (2018) 19:3279–86. doi: 10.31557/APJCP.2018.19.11.3279
Keywords: oral squamous cell carcinoma, OSCC, prognostic marker, p16, Ki-67, MIB
Citation: Richter M, Doll C, Mrosk F, Hofmann E, Koerdt S, Heiland M, Neumann K, Beck M, Dommerich S, Jöhrens K and Raguse J-D (2024) The combined assessment of p16INK4a and Mib/Ki-67 in oral squamous cell carcinoma. Front. Oncol. 14:1493281. doi: 10.3389/fonc.2024.1493281
Received: 08 September 2024; Accepted: 01 November 2024;
Published: 27 November 2024.
Edited by:
Alberto Rodriguez-Archilla, University of Granada, SpainReviewed by:
William J. Magner, University at Buffalo, United StatesMing Zheng, Academy of Military Medical Sciences (AMMS), China
Alexander Gröbe, DIAKOVERE Henriettenstift gGmbH, Germany
Copyright © 2024 Richter, Doll, Mrosk, Hofmann, Koerdt, Heiland, Neumann, Beck, Dommerich, Jöhrens and Raguse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maximilian Richter, bWF4aW1pbGlhbi5yaWNodGVyQGNoYXJpdGUuZGU=
†These authors have contributed equally to this work and share last authorship