
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 28 January 2025
Sec. Cancer Immunity and Immunotherapy
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1485532
 Shicheng Zheng1†
Shicheng Zheng1† Zhongqiao Lin2†
Zhongqiao Lin2† Ruibo Zhang1Zihang Cheng1Kaixin Li1Chenkai Gu1
Ruibo Zhang1Zihang Cheng1Kaixin Li1Chenkai Gu1 Yu Chen3,4*Jing Lin3,4*‡
Yu Chen3,4*Jing Lin3,4*‡Melanoma is highly aggressive, with brain metastasis being a significant contributor to poor outcomes. Immunotherapy has emerged as a crucial treatment modality for melanoma, particularly for addressing brain metastases. This review explores recent developments in immunotherapy for patients with melanoma brain metastasis, with such treatments encompassing immune checkpoint inhibitors and various immunotherapy combination approaches, such as dual immunotherapy, immunotherapy combined with chemotherapy, immunotherapy combined with targeted drugs, and immunotherapy combined with radiotherapy. This article also discusses existing treatment obstacles and potential future avenues for research and clinical practice.
A melanoma is a malignant tumor arising from melanocytes located in the skin, mucosa and other tissues. The disease is categorized into cutaneous, mucosal, arcal, and unknown primary types on the basis of the site of origin (1, 2). Melanoma exhibits a high degree of malignancy and aggressiveness and is susceptible to distant metastasis. Indeed, patients with melanoma have a greater prevalence of brain metastases than patients with other cancers (3), with an incidence of 28%-60% at diagnosis or during treatment and 73%~90% in postmortem (4–6). Melanoma brain metastases (MBMs) also have a poor prognosis in the past, with dismal patient survival durations of 3-6 months (4, 7–9). Early treatment of MBMs is particularly challenging because many therapeutic agents cannot penetrate the blood−brain barrier (BBB) to reach the brain (10). Chemotherapy, which commonly involves temozolomide and fotrmustine, has an intracranial objective response rate (ORR) of only 10%-14.3% (11, 12). Radiation therapy is typically indicated for patients presenting with meningeal or diffuse brain metastases; these patients have a median survival generally limited to approximately three months following localized interventions, including surgery and radiation therapy (10). In addition, patients with MBMs have often been excluded from clinical studies (13). Currently, the development of immunotherapies, such as immune checkpoint inhibitors, is crucial for the treatment of brain metastatic melanoma. Novel treatment approaches such as immunotherapy and combination immunotherapy have enabled clinicians to adopt more targeted and strategic approaches for the treatment of these patients. This article reviews the recent progress in immunotherapy and its combination with chemotherapy, radiotherapy, targeted drugs, as well as other immune therapeutic modalities in the treatment of MBMs.
Currently, immune checkpoint inhibitors such as CTLA-4, PD-1/PD-L1, LAG-3 monoclonal antibodies and TIGIT monoclonal antibodies are widely used for immunotherapy or during clinical trials and show desirable efficacy (14, 15). For melanoma patients with brain metastases, the common immune checkpoint inhibitors used for monotherapy are PD-1/PD-L1 and cytotoxic T lymphocyte-associated protein 4 (CTLA-4). CTLA-4 inhibitors, such as ipilimumab, can enhance and prolong the adaptive immune response to tumor cells by blocking the CTLA-4 molecule. In addition, ipilimumab is the first commercialized immune checkpoint inhibitor. A multicenter phase II study of ipilimumab in 2012 was the first to report the intracranial activity of an immune checkpoint inhibitor in patients with MBMs (16). However, only patients with asymptomatic brain metastases show greater benefit, with response rates of 16% and a median overall survival of 7.0 months (16). Therefore, the following studies of ipilimumab have focused more on combinations with PD-1 inhibitors (e.g., Checkmate 204). Other CTLA-4 inhibitors, such as tremelimumab, are currently unreported for the treatment of MBMs.
PD-1 (Programmed cell death protein 1) and PD-L1 (Programmed death-ligand 1) inhibitors can reactivate the immune response of T cells to tumors by blocking the binding of PD-1 to PD-L1 (14, 17). In MBMs, PD-1/PD-L1 inhibitors such as pembrolizumab and nivolumab have demonstrated marked therapeutic efficacy (18). A phase II study initially demonstrated a response rate of 22% in 18 melanoma patients with asymptomatic brain metastases measuring <2 cm who received pembrolizumab, and their durations of brain metastasis response were all greater than 4 months (19). Patients with asymptomatic brain metastases benefitted more from nivolumab, with response rates of 20% and 18.5 months of median overall survival. This multicohort study revealed that patients with symptomatic brain metastases had a response rate of only 6% and a median overall survival of 5.1 months, regardless of the presence of BRAF mutations (20). Another retrospective study revealed that patients with symptomatic brain metastases had shorter PFS than did those without symptoms (2.7 vs. 7.4 months, P=0.035), as well as a lower ORR (21% vs. 56%), regardless of which anti-PD-1 therapy (pembrolizumab or nivolumab) was used (21). Thus, anti-PD-1 monotherapy may be suitable for patients with asymptomatic brain metastases. PD-L1 inhibitors such as atezolizumab, durvalumab, and avelumab have not been studied or reported to be effective for monotherapy in MBMs thus far.
ICI monotherapy has been shown to be effective in patients with symptomatic brain metastases. Several studies have demonstrated that the combination of ICIs yields a higher intracranial remission rate and greater efficacy than individual ICIs do (22). Nivolumab and ipilimumab stand out as the most frequently utilized combination among the various treatment options (23). The ABC study first assessed the effectiveness of nivolumab (anti-PD-1) combined with ipilimumab (anti-CTLA-4) in the treatment of MBMs. In the recent 5-year follow-up, the intracranial response (ICR) rates were 51% in patients in cohort A (nivolumab + ibritumomab, asymptomatic), 20% in cohort B (nivolumab, asymptomatic), and 6% in Cohort C (nivolumab; patients who failed local therapy or experienced neurologic symptoms). The 5-year intracranial PFS rates were 46% in cohort A, 15% in cohort B, and 6% in cohort C (24). Further research, such as the CheckMate 204 study, included long-term evaluations of the efficacy of nivolumab plus ipilimumab. The study revealed that 54% (54/101) of asymptomatic patients experienced clinical remission, and 33% of them achieved an intracranial complete response; the 36-month intracranial progression-free survival rate was 54.1%, and the overall survival rate was 71.9%. In contrast, among symptomatic patients, only 16.7% (3/18) had an intracranial complete response; the 36-month intracranial progression-free survival rate was 18.9%, and the overall survival rate was 36.6%. In addition, only 15% of patients in the CheckMate 204 study experienced grade 3–4 treatment-related adverse events (TRAEs), which were well tolerated (25). Compared with that of previous chemotherapy, which has achieved a 10%-14.3% remission rate for brain metastases (11, 12), the efficacy of ICI dual-immunotherapy has significantly improved. In the CheckMate 204 study, the NCCN, ESMO, EORTC, and CCA guidelines recommended nivolumab plus ipilimumab as the preferred initial treatment in untreated asymptomatic patients with MBM < 3 cm (26). Another retrospective study included patients with symptomatic MBMs and concurrent treatment with corticosteroids who were also receiving ipilimumab plus nivolumab. The researchers reported an objective response rate (ORR) of 28% (8/29) and a duration of response (DOR) of 7.85 months; however, the responding patients had a longer OS of 56.4 months (27). Patients with symptomatic MBMs only modestly benefit from ICI dual immunotherapy, possibly because steroids impair the efficacy of ICIs, which still need more evidences. Regarding other ICI combinations, a recent phase II study of relatlimab (LAG-3 monoclonal antibody) used in combination with nivolumab in patients with active MBMs is in progress (NCT05704647), and the results are keenly anticipated (28). Table 1 summarizes the ORR, intracranial PFS and OS of the mono-ICI and dual-ICI trials mentioned above.
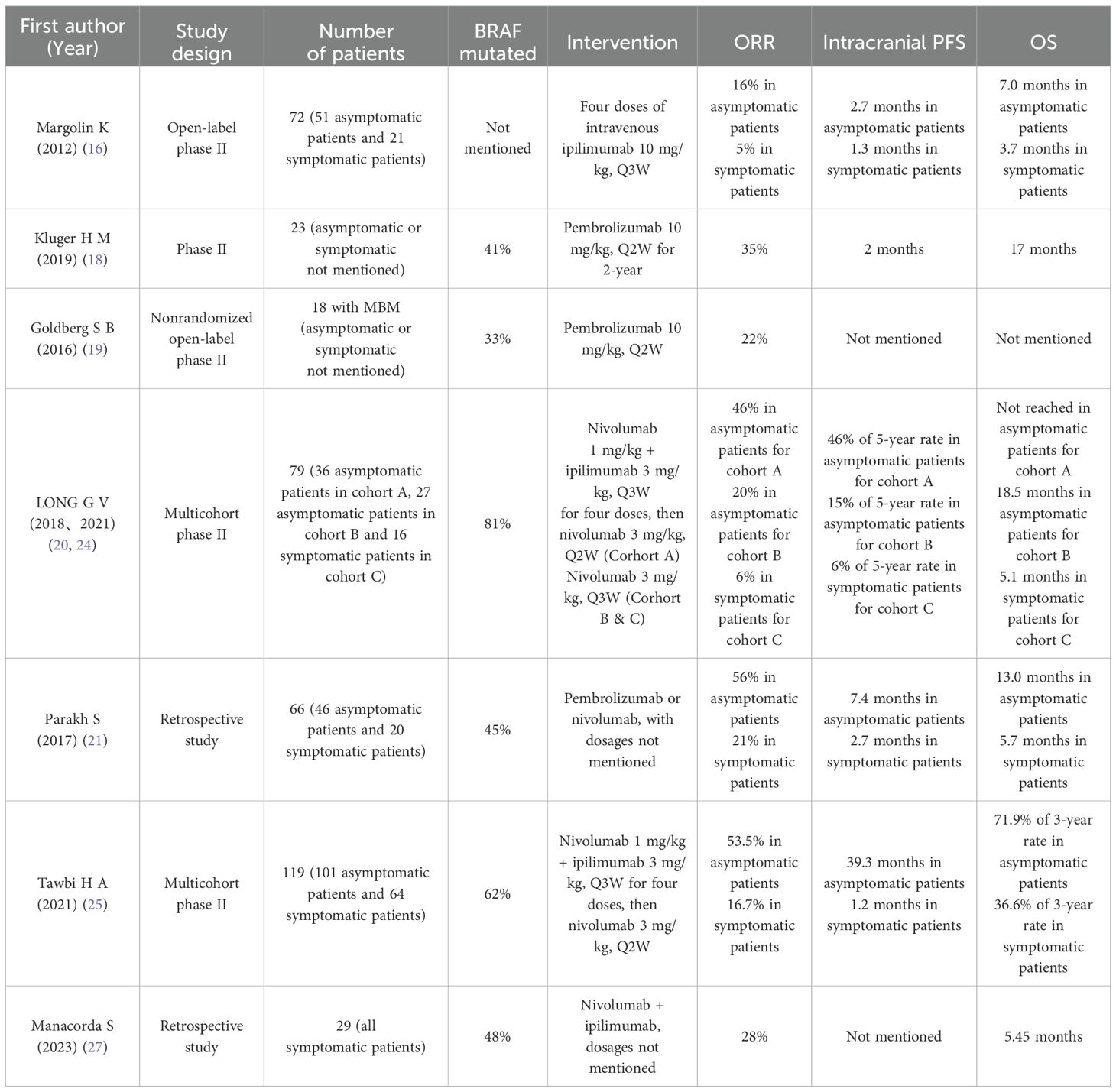
Table 1. Outcomes of patients with melanoma brain metastases treated with ICIs.
In addition to well-known immune checkpoint inhibitors, oncolytic virus immunotherapy, tumor-infiltrating lymphocyte (TIL) therapy and TCR-T-cell therapy are novel individualized immunotherapies. The oncolytic virus T-VEC has shown good efficacy in the treatment of extracranial lesions and has been approved by the FDA for clinical treatment. It is also considered useful in brain metastasis patients because it is capable of crossing the BBB, but few data on its use combined with ICIs in clinical trials are available at present. There are only two clinical cases showing that T-VEC has a certain effect on brain metastatic lesions, and its specific efficacy still needs to be further explored in trials (29, 30). TIL therapy attacks tumor cells by extracting and modifying T cells from the patient’s own tumor tissue and then reinjecting them into the patient’s body. In a clinical trial, Lifileucel, a novel TIL therapy, was used to treat refractory melanoma. The study, which included 153 patients, including those with brain metastases, demonstrated an objective remission rate (ORR) of 31.4%, a median survival (OS) of 13.9 months, and a 12-month OS incidence of 54.0% (31). Lifileucel initially showed good antitumor activity in patients with advanced brain metastatic melanoma and was also effective in patients who had failed PD-1 therapy, with a long-lasting clinical benefit as well as a high ORR (31). T-cell receptor–engineered T (TCR-T) cell therapy has several advantages, such as a large repertoire of targetable antigens, lower epitope density, increased sensitivity and greater avidity, which have revolutionized the immunotherapy of cancers (32). However, TCR-T-cell therapy for MBMs is still in its infancy. There is only one case report, which describes a mucosal melanoma patient with brain metastases who received MAGE-A4-targeted TCR-T-cell therapy in combination with low-dose radiotherapy and experienced durable remission (33). Cytologic therapy has initially shown notable efficacy in the treatment of MBM, but its effectiveness and safety need to be fully explored.
Chemotherapy, such as temozolomide or fotemustine, is less effective in controlling MBM, with an intracranial ORR of 10%-14.3% (11, 12). Chemotherapy combined with immunotherapy for MBM is less studied. Fotemustine is a chemotherapeutic drug commonly used for patients with MBM, and the overall remission rate was found to be 17% in patients receiving monotherapy (12). A multicenter phase III NIBIT-M2 trial explored the efficacy of the combination of fotemustine with ipilimumab in MBM. The last 7-year follow-up study reported a 7-year intracranial ORR of 19.2% for fotemustine plus ipilimumab, 11.5% for the 7-year intracranial PFS rate and 13.8 months for the median intracranial DOR (34). Although the NIBIT-M2 trial did not demonstrate favorable outcomes of ORR and PFS with ipilimumab + fotemustine compared with ipilimumab + nivolumab, Grade 3~4 immune-related AEs were observed in 38% (10) of patients receiving ipilimumab plus fotemustine (34), similar to the 33% (9) receiving ipilimumab + nivolumab. Unlike the NIBIT-M2 trial (anti-CTLA-4 combination with chemotherapy), anti-PD-1/PD-L1 combination with chemotherapy has been less explored in MBM but has shown efficacy in advanced nonsquamous NSCLC patients with brain metastases, with a confirmed intracranial ORR of 46.7% and an intracranial PFS of 7.6 months (CAP-BRAIN trial) (35). Future studies may focus on this combination and explore the efficacy of MBM.
In acral melanoma with brain metastases, heterogeneous tumor interactions within the brain microenvironment drive resistance to ICIs and target drugs (36). Under such circumstances, chemotherapy may remain important as standard therapy. In a recent CAP-03 trial, camrelizumab + apatinib + temozolomide triple therapy showed primary efficacy in advanced acral melanoma without brain metastases (37). The ORR was 64.0%, the DOR was 17.5 months, and the median PFS was 18.4 months (37). Although grade 3 or 4 treatment-related AEs (TRAEs) have been reported in 66% of patients, they can be effectively alleviated by dosage adjustments and symptomatic treatments (37). Although the CAP-03 trial did not include patients with brain metastases, this triplet combination may provide new insights into the treatment of acral melanoma with brain metastases.
Furthermore, for patients with symptomatic MBM, who may receive steroids to temporarily alleviate symptoms of increased intracranial pressure and cerebral edema, immunotherapy combined with chemotherapy may be advantageous, as chemotherapy can help control cerebral lesions before the addition of immunotherapy for a synergistic effect. However, no retrospective or prospective studies on immunotherapy combined with chemotherapy in patients with symptomatic MBM have been conducted, and further research in such patients is needed.
The classical COMBI-MB study demonstrated promising treatment efficacy of dabrafenib + trametinib (D+T) in patients with BRAF V600-mutated MBM, with an intracranial ORR of up to 58% and a median PFS of up to 5.6 months (38). However, evidence for the combination of immunotherapy and targeted therapy for MBM patients with BRAF mutations is lacking. Although of three large randomized controlled studies, KEYNOTE-022, IMspire150, and COMBI-I for the triplet regimen of immunotherapy combined with targeted drugs in advanced melanoma patients with BRAF V600 mutations, none demonstrated meaningful improvements in OS, and all three trials reported increases in adverse events in the triple therapy group (39–41). However, IMspire150 likely presented a longer median PFS (15.1 vs. 10.6 months) and median DOR (21.0 vs. 12.6 months) and a 23% reduction in disease progression and a 21% reduction in death risk in the triple therapy group than in the dual therapy group (42). A retrospective analysis revealed that patients who undergo at least six months of targeted therapy without disease progression tend to experience better remission rates when subsequent immunotherapy is administered than do those who experience rapid relapse (43). For MBM patients, an important study of immunotherapy combined with targeted drugs was performed in the TRICOTEL trial, which showed that the addition of atezolizumab (anti-PD-L1) to vemurafenib (BRAFi) or cobimetinib (MEKi) provided promising intracranial activity in patients with BRAF V600-mutated melanoma with CNS metastases, the intracranial ORR was 42% in the BRAF V600 mutation-positive cohort and 27% in the BRAF V600 wild-type cohort (44). In patients with BRAF V600 mutations, the intracranial ORR was 35% in symptomatic patients, which was lower than the 46% reported in asymptomatic patients. The intracranial DOR was 7.4 months and the PFS was 4.5 months in symptomatic patients, whereas the intracranial DOR was 7.6 months and the PFS was 5.5 months in asymptomatic patients, but the difference was not statistically significant (44). Treatment-related serious adverse events (grade ≥3) occurred in 16 (21%) of 75 patients who received triplet therapy, and no treatment-related deaths occurred, which initially indicated favorable safety (44). The ongoing phase II SWOG S2000 trial is aimed to explore a triplet regimen of BRAF/MEK inhibitors with anti-PD-1 therapy (encorafenib + binimetinib + nivolumab) versus anti-PD-1+CTLA-4 therapy (nivolumab + ipilimumab) in patients with symptomatic BRAF-mutant MBM; these results are also highly anticipated (45).
Radiotherapy (RT) is a crucial local treatment for tumor brain metastases, and common radiation strategies include whole-brain radiotherapy (WBRT) and stereotactic radiosurgery (SRS) (46). Whole-brain radiation therapy (WBRT) offers a robust solution for managing both multiple and solitary lesions and is used in patients with multiple MBMs but has a limited effect on median survival (26). Stereotactic radiosurgery (SRS) delivers a high dose of radiation and can focus on certain areas with high three-dimensional conformality, which is effective in controlling a small number (< 4) of MBM lesions (with a total cerebral tumor volume of < 5 cm3) (26). Radiotherapy has been proven to improve immunosuppression in the tumor microenvironment, increase the permeability of the blood–brain barrier, promote T-cell activation by stimulating IFN-γ production and increasing MHC Class I, promote tumor antigen presentation, upregulate PD-L1 expression on the surface of tumor cells, and increase the efficacy of immune checkpoint inhibitors (47–51). Currently, RT combined with ICI therapy holds tremendous promise for controlling MBM. Potential sympathetic effects of immunotherapy combined with radiotherapy in the treatment of MBMs have been reported in several studies. A large meta-analysis including 44 studies indicated better survival outcomes in the ICI + RT group than in the RT alone or ICI alone groups (52). In addition, there were no marked increases in Grade 3~4 neurologic adverse events (NAEs) or Grade ≥ 3 radiation necrosis (52) in the ICI + RT group. A real-world study revealed that WBRT combined with ICIs significantly increased the median overall survival to 4.89 months compared with 3.12 months for WBRT alone, but Cox regression revealed that WBRT + ICI was associated with an increased risk of death (53). As WBRT poses a risk of cognitive impairment, three studies comparing SRS to WBRT in patients with 1-3 brain metastases revealed that SRS not only mitigated the detrimental effects of radiotherapy on cognitive function but also increased patient survival rates (54–56). A retrospective analysis included 160 patients with MBMs treated with SRS in combination with nivolumab, which demonstrated local control rates of 91% and 85% at 6 months and 12 months, respectively, along with OS rates of 11.8 and 12.0 months, respectively, which were significantly greater than those of patients treated with nivolumab or SRS alone (57). No treatment-related neurologic toxicities (such as nausea, vision changes, or focal weakness) or scalp reactions were reported during or after radiation (57).
For asymptomatic patients with MBMs, the dose−size response relationship of SRS with ICIs showed that the 12-month local control rate for a 7.5 mm lesion subjected to SRS (18 Gy) with ICIs was 87.8%, which was noticeably higher than the 79.8% reported without ICIs (58). Further studies compared the efficacy of SRS + nivolumab and SRS + ipilimumab in patients with either asymptomatic or symptomatic MBMs. SRS + nivolumab resulted in meaningful intracranial remission, resulting in 6-month and 12-month intracranial PFS rates of 69% and 42%, respectively, compared with 48% and 17%, respectively, for SRS + ipilimumab (59). Furthermore, the extracranial PFS and OS rates were 37% and 78% in the SRS + nivolumab group, respectively (59). Another notable finding in this study was that patients receiving multifraction SRS (3×9 Gy) compared with those receiving single-fraction SRS had better intracranial PFS (70% versus 46% at 6 months, p = 0.01), especially in combination with nivolumab (59). Moreover, Grade 3 AEs (e.g., diarrhea and fatigue) occurred in 11% of SRS + ipilimumab patients and in 6% of SRS + nivolumab patients, and radiation-induced brain necrosis occurred in 15% of all patients (59). SRS combined with dual-ICI immunotherapy was also explored. One study evaluated the clinical outcomes of patients with MBM treated with SRS within 3 months of receiving anti-PD-1+CTLA-4 therapy, anti-PD-1 therapy, or anti-CTLA-4 therapy; however, the 12-month OS rate and PFS rate for patients receiving SRS + anti-PD-1 + CTLA-4 therapy (68%, 57%) were higher than those for patients receiving SRS + anti-PD-1 therapy (59%, 53%) and SRS + anti-CTLA-4 therapy (45%, 42%), and the local control rates did not differ between the groups, with adverse effects on the rates of radiation necrosis (lower than 7%) (60). However, grade 1–2 toxicity was noted to be highest in patients treated with SRS+anti-PD-1+CTLA-4 therapy (45%) (60). Treatment with ICIs combined with SRS enhances the control of MBM and prolongs OS, and anti-PD-1 therapy combined with SRS is more recommended.
However, whether concurrent radiotherapy with ICIs or subsequent radiotherapy with ICIs is more effective and safer needs to be considered. Concurrent therapy was predominantly defined as the interval between the administration of an ICI and SRS within 4 weeks, and subsequent therapy was defined as the initiation of ICI treatment either >4 weeks before or after SRS (61). An international meta-analysis including 17 individual studies demonstrated that concurrent therapy yielded a higher 1-year OS rate (64.6%) than did subsequent therapy (51.6%), but the local control rate at 1 year did not significantly differ (89.2% vs. 67.8%, p = 0.09) (62). Thus, concurrent therapy may lead to better long-term outcomes. However, in the context of concurrent therapy, whether it is more appropriate to start with RT or ICI therapy still unclear. An exploratory phase II trial revealed that when MBM patients received RT (SRS or WBRT depending on the number of MBMs) followed by ipilimumab (ipi) ± nivolumab (nivo) at 3 weeks, after RT plus two cycles of ipi-based ICI, increased frequencies of activated CD4+ and CD8+ T cells and an increase in melanoma-specific T-cell responses were observed in the peripheral blood, suggesting that sequencing RT followed by ICI treatment may yield better outcomes in MBM patients (63). Thus, although immunotherapy combined with radiotherapy has been proven effective against MBMs, its treatment dosage and sequence require further study.
Malignant MBMs have a high incidence and poor prognosis. In the past, neurosurgery and radiotherapy were the primary treatments for patients with brain metastases. Since then, the emergence of immunotherapy has led to new treatment options for melanoma brain metastasis. Drugs targeting PD-1/PD-L1 and CTLA-4 have demonstrated efficacy in treating brain metastases. Newly marketed TIL cell therapies in recent years have also demonstrated notable efficacy, and many novel immunotherapies, such as CDR1as, novel TCR-T cells, and novel oncolytic viruses, have shown greater promise in the treatment of brain metastases. Clinical trials have shown that immunotherapy combined with other treatments can improve the treatment efficacy in MBM patients. However, the adverse reactions caused by combination therapy cannot be ignored, as these adverse reactions have a higher incidence rate and a significantly higher degree and the discontinuation of drug therapy caused by these adverse reactions is extremely unfavorable for the treatment of brain metastases. These advancements underscore the evolving landscape of treatment for MBMs, offering new hope and options for patients.
SZ: Writing – original draft, Writing – review & editing, Funding acquisition. ZL: Writing – review & editing, Project administration, Funding acquisition. RZ: Writing – original draft. ZC: Writing – review & editing. KL: Writing – review & editing. CG: Writing – review & editing. YC: Writing – review & editing, Project administration, Funding acquisition. JL: Project administration, Supervision, Writing – review & editing, Investigation, Methodology, Funding acquisition.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by Joint Funds for the Innovation of Science and Technology, Fujian Province, China (Grant No. 2021Y9227, Grant No. 2023Y9412); the Natural Science Foundation of Fujian Province, China (Grant No. 2023J011254); The Science Foundation for The Excellent Youth Scholars of Fujian Provincial Health Commission, China (Grant No. 2022ZQNZD009); The Special Research Funds for Local Science and Technology Development Guided by the Central Government, Fujian Province, China (Grant No. 2023L3020); the Fujian Medical University Startup Fund for Scientific Research (Grant No. 2023QH1173); and the Fujian Medical University Student Innovation and Entrepreneurship Training Project, China (Grant No. 202410392008).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor SL declared a past collaboration with the author YC.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rastrelli M, Tropea S, Rossi CR, Alaibac M. Melanoma: epidemiology, risk factors, pathogenesis, diagnosis and classification. In Vivo. (2014) 28:1005–11.
2. Elder DE, Bastian BC, Cree IA, Massi D, Scolyer RA. The 2018 world health organization classification of cutaneous, mucosal, and uveal melanoma: detailed analysis of 9 distinct subtypes defined by their evolutionary pathway. Arch Pathol Lab Med. (2020) 144:500–22. doi: 10.5858/arpa.2019-0561-RA
3. Chukwueke UN, Brastianos PK. Precision medical approaches to the diagnoses and management of brain metastases. Curr Treat Options Oncol. (2019) 20:49. doi: 10.1007/s11864-019-0649-y
4. Davies MA, Liu P, Mcintyre S, Kim KB, Papadopoulos N, Hwu WJ, et al. Prognostic factors for survival in melanoma patients with brain metastases. Cancer. (2011) 117:1687–96. doi: 10.1002/cncr.v117.8
5. Cagney DN, Martin AM, Catalano PJ, Redig AJ, Lin NU, Lee EQ, et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic Malignancy: a population-based study. Neuro Oncol. (2017) 19:1511–21. doi: 10.1093/neuonc/nox077
6. Nieder C, Adam M, Astner ST. Disease presentation and outcome in young patients (<40 years) with brain metastases from Malignant melanoma. Anticancer Res. (2008) 28:1325–7.
7. Zheng R, Zhang S, Zeng H, Wang S, Sun K, Chen R, et al. Cancer incidence and mortality in China, 2016. J Natl Cancer Center. (2022) 2:1–9. doi: 10.1016/j.jncc.2022.02.002
8. Sloan AE, Nock CJ, Einstein DB. Diagnosis and treatment of melanoma brain metastasis: a literature review. Cancer Control. (2009) 16:248–55. doi: 10.1177/107327480901600307
9. Kohler BA, Ward E, McCarthy BJ, Schymura MJ, Ries LA, Eheman C, et al. Annual report to the nation on the status of cancer, 1975-2007, featuring tumors of the brain and other nervous system. J Natl Cancer Inst. (2011) 103:714–36. doi: 10.1093/jnci/djr077
10. Abate-Daga D, Ramello MC, Smalley I, Forsyth PA, Smalley KSM. The biology and therapeutic management of melanoma brain metastases. Biochem Pharmacol. (2018) 153:35–45. doi: 10.1016/j.bcp.2017.12.019
11. Agarwala SS, Kirkwood JM, Gore M, Dreno B, Thatcher N, Czarnetski B, et al. Temozolomide for the treatment of brain metastases associated with metastatic melanoma: a phase II study. J Clin Oncol. (2004) 22:2101–7. doi: 10.1200/JCO.2004.11.044
12. Addeo R, Zappavigna S, Luce A, Facchini S, Caraglia M. Chemotherapy in the management of brain metastases: the emerging role of fotemustine for patients with melanoma and NSCLC. Expert Opin Drug Saf. (2013) 12:729–40. doi: 10.1517/14740338.2013.789017
13. Maria DGA, Michele M. Nivolumab plus ipilimumab in melanoma brain metastases. Lancet Oncol. (2022) 23:e53–e. doi: 10.1016/S1470-2045(22)00001-8
14. Matteo SC, James L, Georgina VL. Immune checkpoint inhibitors in melanoma. Lancet. (2021) 398:1002–14. doi: 10.1016/S0140-6736(21)01206-X
15. Shi A-P, Tang X-Y, Xiong Y-L, Zheng KF, Liu YJ, Shi XG, et al. Immune checkpoint LAG3 and its ligand FGL1 in cancer. Front Immunol. (2022) 12:785091. doi: 10.3389/fimmu.2021.785091
16. Margolin K, Ernstoff MS, Hamid O, Lawrence D, Mcdermott D, Puzanov I, et al. Ipilimumab in patients with melanoma and brain metastases: an open-label, phase 2 trial. Lancet Oncol. (2012) 13:459–65. doi: 10.1016/S1470-2045(12)70090-6
17. Loise MF, Peter TS, Arlene HS. The PD-1 pathway in tolerance and autoimmunity. Immunol Rev. (2010) 236:219–42. doi: 10.1111/j.1600-065X.2010.00923.x
18. Kluger HM, Chiang V, Mahajan A, Zito CR, Sznol M, Tran T, et al. Long-term survival of patients with melanoma with active brain metastases treated with pembrolizumab on a phase II trial. J Clin Oncol. (2019) 37:52–60. doi: 10.1200/JCO.18.00204
19. Goldberg SB, Gettinger SN, Mahajan A, Chiang AC, Herbst RS, Sznol M, et al. Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol. (2016) 17:976–83. doi: 10.1016/S1470-2045(16)30053-5
20. Long GV, Atkinson V, Lo S, Sandhu S, Guminski AD, Brown MP, et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: a multicentre randomised phase 2 study. Lancet Oncol. (2018) 19:672–81. doi: 10.1016/S1470-2045(18)30139-6
21. Parakh S, Park JJ, Mendis S, Rai R, Xu W, Lo S, et al. Efficacy of anti-PD-1 therapy in patients with melanoma brain metastases. Br J Cancer. (2017) 116:1558–63. doi: 10.1038/bjc.2017.142
22. Rulli E, Legramandi L, Salvati L, Mandala M. The impact of targeted therapies and immunotherapy in melanoma brain metastases: A systematic review and meta-analysis. Cancer. (2019) 125:3776–89. doi: 10.1002/cncr.v125.21
23. Mandalà M, Lorigan P, Sergi MC, Benannoune N, Serra P, Vitale MG, et al. Combined immunotherapy in melanoma patients with brain metastases: A multicenter international study. Eur J Cancer. (2024) 199:113542. doi: 10.1016/j.ejca.2024.113542
24. Long GV, Atkinson V, Lo S, Guminski AD, Sandhu SK, Brown MP, et al. Five-year overall survival from the anti-PD1 brain collaboration (ABC Study): Randomized phase 2 study of nivolumab (nivo) or nivo+ipilimumab (ipi) in patients (pts) with melanoma brain metastases (mets). J Clin Oncol. (2021) 39:9508. doi: 10.1200/JCO.2021.39.15_suppl.9508
25. Tawbi HA, Forsyth PA, Hodi FS, Algazi AP, Hamid O, Lao CD, et al. Long-term outcomes of patients with active melanoma brain metastases treated with combination nivolumab plus ipilimumab (CheckMate 204): final results of an open-label, multicentre, phase 2 study. Lancet Oncol. (2021) 22:1692–704. doi: 10.1016/S1470-2045(21)00545-3
26. Tan XL, Le A, Lam FC, Scherrer E, Kerr RG, Lau AC, et al. Current treatment approaches and global consensus guidelines for brain metastases in melanoma. Front Oncol. (2022) 12:885472. doi: 10.3389/fonc.2022.885472
27. Manacorda S, Carmena MT, Malone C, Linh Le HM, Furness AJS, Larkin J, et al. Ipilimumab plus nivolumab in patients with symptomatic melanoma brain metastasis requiring corticosteroids. Eur J Cancer. (2023) 188:98–107. doi: 10.1016/j.ejca.2023.04.018
28. Phillips S, Burton EM, Kreidieh FY, Glitza IC, Mcquade JL, Amaria RN, et al. Phase II study of nivolumab (nivo) in combination with relatlimab (rela) in patients (pts) with active melanoma brain metastases (MBM). J Clin Oncol. (2023) 41:TPS9605–TPS. doi: 10.1200/JCO.2023.41.16_suppl.TPS9605
29. Soldozy S, Mulligan KM, Zheng DX, Levoska MA, Cullison CR, Elarjani T, et al. Oncolytic virotherapy for melanoma brain metastases, a potential new treatment paradigm? Brain Sci. (2021) 11:1260. doi: 10.3390/brainsci11101260
30. Blake Z, Marks DK, Gartrell RD, Hart T, Horton P, Cheng SK, et al. Complete intracranial response to talimogene laherparepvec (T-Vec), pembrolizumab and whole brain radiotherapy in a patient with melanoma brain metastases refractory to dual checkpoint-inhibition. J Immunother Cancer. (2018) 6:25. doi: 10.1186/s40425-018-0338-6
31. Chesney J, Lewis KD, Kluger H, Hamid O, Whitman E, Thomas S, et al. Efficacy and safety of lifileucel, a one-time autologous tumor-infiltrating lymphocyte (TIL) cell therapy, in patients with advanced melanoma after progression on immune checkpoint inhibitors and targeted therapies: pooled analysis of consecutive cohorts of the C-144-01 study. J ImmunoTherapy Cancer. (2022) 10:e005755. doi: 10.1136/jitc-2022-005755
32. Baulu E, Gardet C, Chuvin N, Depil S. TCR-engineered T cell therapy in solid tumors: State of the art and perspectives. Sci Adv. (2023) 9:eadf3700. doi: 10.1126/sciadv.adf3700
33. He K, Hong DS, Ke D, Kebriaei P, Wang T, Danesi H, et al. Durable control of metastases in an HLA-A2+ patient with refractory melanoma after low-dose radiotherapy in combination with MAGE-A4 T cell therapy: a case report. Melanoma Res. (2023) 33:332–7. doi: 10.1097/CMR.0000000000000869
34. Di Giacomo AM, Chiarion-Sileni V, del Vecchio M, Ferrucci PF, Guida M, Quaglino P, et al. Nivolumab plus ipilimumab in melanoma patients with asymptomatic brain metastases: 7-year outcomes and quality of life from the multicenter phase III NIBIT-M2 trial. Eur J Cancer. (2024) 199:113531. doi: 10.1016/j.ejca.2024.113531
35. Hou X, Zhou C, Wu G, Lin W, Xie Z, Zhang H, et al. Efficacy, safety, and health-related quality of life with camrelizumab plus pemetrexed and carboplatin as first-line treatment for advanced nonsquamous NSCLC with brain metastases (CAP-BRAIN): A multicenter, open-label, single-arm, phase 2 study. J Thorac Oncol. (2023) 18:769–79. doi: 10.1016/j.jtho.2023.01.083
36. Lee RJ, Khandelwal G, Baenke F, Cannistraci A, Macleod K, Mundra P, et al. Brain microenvironment-driven resistance to immune and targeted therapies in acral melanoma. ESMO Open. (2020) 5. doi: 10.1136/esmoopen-2020-000707
37. Mao L, Lian B, Li C, Bai X, Zhou L, Cui C, et al. Camrelizumab plus apatinib and temozolomide as first-line treatment in patients with advanced acral melanoma: the CAP 03 phase 2 nonrandomized clinical trial. JAMA Oncol. (2023) 9:1099–107. doi: 10.1001/jamaoncol.2023.1363
38. Davies MA, Saiag P, Robert C, Grob JJ, Flaherty KT, Arance A, et al. Dabrafenib plus trametinib in patients with BRAF(V600)-mutant melanoma brain metastases (COMBI-MB): a multicentre, multicohort, open-label, phase 2 trial. Lancet Oncol. (2017) 18:863–73. doi: 10.1016/S1470-2045(17)30429-1
39. Gutzmer R, Stroyakovskiy D, Gogas H, Robert C, Lewis K, Protsenko S, et al. Atezolizumab, vemurafenib, and cobimetinib as first-line treatment for unresectable advanced BRAF(V600) mutation-positive melanoma (IMspire150): primary analysis of the randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. (2020) 395:1835–44. doi: 10.1016/S0140-6736(20)30934-X
40. Maio M, Carlino MS, Joshua AM, Mcwhirter E, Ribas A, Ascierto PA, et al. KEYNOTE-022: Pembrolizumab with trametinib in patients with BRAF wild-type melanoma or advanced solid tumours irrespective of BRAF mutation. Eur J Cancer. (2022) 160:1–11. doi: 10.1016/j.ejca.2021.09.024
41. Dummer R, Long GV, Robert C, Tawbi HA, Flaherty KT, Ascierto PA, et al. Randomized phase III trial evaluating spartalizumab plus dabrafenib and trametinib for BRAF V600-mutant unresectable or metastatic melanoma. J Clin Oncol. (2022) 40:1428–38. doi: 10.1200/JCO.21.01601
42. Ascierto PA, Stroyakovskiy D, Gogas H, Robert C, Lewis K, Protsenko S, et al. Overall survival with first-line atezolizumab in combination with vemurafenib and cobimetinib in BRAF(V600) mutation-positive advanced melanoma (IMspire150): second interim analysis of a multicentre, randomised, phase 3 study. Lancet Oncol. (2023) 24:33–44. doi: 10.1016/S1470-2045(22)00687-8
43. Ascierto PA, Atkins MB. Sequencing and combinations of molecularly targeted and immunotherapy for BRAF-mutant melanoma. In: Balch CM, Atkins MB, Garbe C, Gershenwald J, Halpern AC, Kirkwood JM, et al, editors. Cutaneous Melanoma. Springer International Publishing, Cham (2020). p. 1215–41.
44. Dummer R, Queirolo P, Gerard Duhard P, Hu Y, Wang D, De Azevedo SJ, et al. Atezolizumab, vemurafenib, and cobimetinib in patients with melanoma with CNS metastases (TRICOTEL): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. (2023) 24:e461–e71. doi: 10.1016/S1470-2045(23)00334-0
45. Eroglu Z, Moon J, Najjar YG, Kotecha R, Spektor V, Wu M, et al. A randomized phase 2 trial of encorafenib + binimetinib + nivolumab vs ipilimumab + nivolumab in BRAFV600-mutant melanoma brain metastases: SWOG S2000. J Clin Oncol. (2023) 41:TPS9603–TPS. doi: 10.1200/JCO.2023.41.16_suppl.TPS9603
46. Matsui JK, Perlow HK, Upadhyay R, Mccalla A, Raval RR, Thomas EM, et al. Advances in radiotherapy for brain metastases. Surg Oncol Clin N Am. (2023) 32:569–86. doi: 10.1016/j.soc.2023.02.007
47. Wang Y, Liu ZG, Yuan H, Deng W, Li J, Huang Y, et al. The reciprocity between radiotherapy and cancer immunotherapy. Clin Cancer Res. (2019) 25:1709–17. doi: 10.1158/1078-0432.CCR-18-2581
48. Staniszewska M, Iking J, Lückerath K, Hadaschik B, Herrmann K, Ferdinandus J, et al. Drug and molecular radiotherapy combinations for metastatic castration resistant prostate cancer. Nucl Med Biol. (2021) 96-97:101–11. doi: 10.1016/j.nucmedbio.2021.03.009
49. Cao Y, Tsien CI, Shen Z, Tatro DS, Ten Haken R, Kessler ML, et al. Use of magnetic resonance imaging to assess blood-brain/blood-glioma barrier opening during conformal radiotherapy. J Clin Oncol. (2005) 23:4127–36. doi: 10.1200/JCO.2005.07.144
50. Tang C, Wang X, Soh H, Seyedin S, Cortez MA, Krishnan S, et al. Combining radiation and immunotherapy: a new systemic therapy for solid tumors? Cancer Immunol Res. (2014) 2:831–8. doi: 10.1158/2326-6066.Cir-14-0069
51. Kalbasi A, June CH, Haas N, Vapiwala N. Radiation and immunotherapy: a synergistic combination. J Clin Invest. (2013) 123:2756–63. doi: 10.1172/JCI69219
52. Anvari A, Sasanpour P, Kheradmardi MR. Radiotherapy and immunotherapy in melanoma brain metastases. Hematol Oncol Stem Cell Ther. (2023) 16:1–20. doi: 10.1016/j.hemonc.2021.11.001
53. Moyers JT, Chong EG, Peng J, Tsai HHC, Sufficool D, Shavlik D, et al. Real world outcomes of combination and timing of immunotherapy with radiotherapy for melanoma with brain metastases. Cancer Med. (2021) 10:1201–11. doi: 10.1002/cam4.v10.4
54. Andrews DW, Scott CB, Sperduto PW, Flanders AE, Gaspar LE, Schell MC, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. (2004) 363:1665–72. doi: 10.1016/S0140-6736(04)16250-8
55. Brown PD, Jaeckle K, Ballman KV, Farace E, Cerhan JH, Anderson SK, et al. Effect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: A randomized clinical trial. JAMA. (2016) 316:401–9. doi: 10.1001/jama.2016.9839
56. Palmer JD, Klamer BG, Ballman KV, Brown PD, Cerhan JH, Anderson SK, et al. Association of long-term outcomes with stereotactic radiosurgery vs whole-brain radiotherapy for resected brain metastasis: A secondary analysis of the N107C/CEC.3 (Alliance for clinical trials in oncology/Canadian cancer trials group) randomized clinical trial. JAMA Oncol. (2022) 8:1809–15. doi: 10.1001/jamaoncol.2022.5049
57. Ahmed KA, Stallworth DG, Kim Y, Johnstone PA, Harrison LB, Caudell JJ, et al. Clinical outcomes of melanoma brain metastases treated with stereotactic radiation and anti-PD-1 therapy. Ann Oncol. (2016) 27:434–41. doi: 10.1093/annonc/mdv622
58. Yusuf M, Rattani A, Gaskins J, Oliver AL, Mandish SF, Burton E, et al. Stereotactic radiosurgery for melanoma brain metastases: dose-size response relationship in the era of immunotherapy. J Neurooncol. (2022) 156:163–72. doi: 10.1007/s11060-021-03899-0
59. Minniti G, Anzellini D, Reverberi C, Cappellini GCA, Marchetti L, Bianciardi F, et al. Stereotactic radiosurgery combined with nivolumab or Ipilimumab for patients with melanoma brain metastases: evaluation of brain control and toxicity. J Immunother Cancer. (2019) 7:102. doi: 10.1186/s40425-019-0588-y
60. Dohm AE, Nakashima JY, Kalagotla H, Jiang SX, Tang JD, Bhandari M, et al. Stereotactic radiosurgery and anti-PD-1 + CTLA-4 therapy, anti-PD-1 therapy, anti-CTLA-4 therapy, BRAF/MEK inhibitors, BRAF inhibitors, or conventional chemotherapy for the management of melanoma brain metastases. Eur J Cancer. (2023) 192:113287. doi: 10.1016/j.ejca.2023.113287
61. Qian JM, Yu JB, Kluger HM, Chiang VL. Timing and type of immune checkpoint therapy affect the early radiographic response of melanoma brain metastases to stereotactic radiosurgery. Cancer. (2016) 122:3051–8. doi: 10.1002/cncr.v122.19
62. Lehrer EJ, Peterson J, Brown PD, Sheehan JP, Quiñones-Hinojosa A, Zaorsky NG, et al. Treatment of brain metastases with stereotactic radiosurgery and immune checkpoint inhibitors: An international meta-analysis of individual patient data. Radiother Oncol. (2019) 130:104–12. doi: 10.1016/j.radonc.2018.08.025
Keywords: melanoma, brain metastasis, immunotherapy, immune checkpoint inhibitors, combination therapy
Citation: Zheng S, Lin Z, Zhang R, Cheng Z, Li K, Gu C, Chen Y and Lin J (2025) Progress in immunotherapy for brain metastatic melanoma. Front. Oncol. 14:1485532. doi: 10.3389/fonc.2024.1485532
Received: 28 August 2024; Accepted: 07 November 2024;
Published: 28 January 2025.
Edited by:
Siming Li, Peking University, ChinaReviewed by:
Lili Mao, Peking University, ChinaCopyright © 2025 Zheng, Lin, Zhang, Cheng, Li, Gu, Chen and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Lin, NDIzNTU5MTQ4QHFxLmNvbQ==; Yu Chen, Y2hlbnl1MTk4MEBmam11LmVkdS5jbg==
†These authors share first authorship
‡ORCID: Jing Lin, orcid.org/0000-0002-9025-1721
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.