
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol., 21 January 2025
Sec. Breast Cancer
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1484750
 Ünal Metin Tokat1*
Ünal Metin Tokat1* Ashkan Adibi1,2
Ashkan Adibi1,2 Esranur Aydın1
Esranur Aydın1 Şevval Nur Bilgiç1
Şevval Nur Bilgiç1 Eylül Özgü1
Eylül Özgü1 Onur Tutar3
Onur Tutar3 Mutlu Demiray1*
Mutlu Demiray1*Breast cancer (BC) is the leading cause of cancer-related mortality among women. The backbone of first-line treatment in HR+/HER2+ BC is dual anti-HER2 blockade combined with taxane chemotherapy. Although this regimen exhibits high rates of response and disease control in both HR+ and HR− cohorts, some patients could have intrinsic or develop acquired resistance to trastuzumab and/or pertuzumab. Here, we achieved a near-complete response in HR+ HER2-amplified and overexpressing metastatic BC twice through molecular tumor board (MTB) discussions: initially, with trastuzumab deruxtecan (T-DXd) when HER2 IHC was positive, and, then, with neratinib plus fulvestrant plus paclitaxel when IHC was negative. Our case presents GATA3 and NOTCH2 mutations, MCL1 and CKS1B amplifications, as well as ERBB3/KRAS overexpression and ER signaling as potential new mechanisms of resistance to T-DXd. Furthermore, we demonstrated that triplet combination could induce a remarkable response in the T-DXd–refractory setting, which could be explored in future clinical trials in HR+ and HER2-activated (by RNA or protein overexpression, amplification, and mutation) patients. Our case also highlights the importance of the MTBs to dynamically and reactively manage the course of disease and treatment on a per-patient basis.
Breast cancer (BC) is the most frequently diagnosed cancer worldwide according to GLOBOCAN estimates (1), and the primary reason for cancer-related deaths among women (2). Hormone receptor (ER/HR)–positive patients constitute the vast majority (75%–80%) of all BC cases (3). Moreover, at least 50% of the Human Epidermal Growth Factor Receptor 2-positive (HER2+) tumors also express HRs, influencing response to anti-HER2 agents (4, 5).
The HR status is often not a primary concern for the treatment of HER2-enriched BC as the current standard of care [taxane plus trastuzumab plus pertuzumab (THP)] is clinically active in both HR+ and HR− subgroups (6, 7). Multiple HER2 Tyrosine Kinase Inhibitors (TKIs) [with anti-HER2, chemotherapy, or endocrine therapy (ET)] or two HER2 antibody-drug conjugates (ADCs), namely, trastuzumab emtansine (T-DM1) and trastuzumab deruxtecan (T-DXd), are also approved in the later lines. Although these drugs are indicated in BC based on Immunohistochemistry (IHC) and/or IHC/in situ hybridization (ISH) positivity, tumors may exhibit alterations at mRNA level, which may not be always concordant with IHC/ISH and may lead to differential clinical outcomes. Of the approved agents, T-DXd stands out as it showed unparalleled efficacy in previously treated HER2+ BC in the DESTINY-Breast01/02 trials (8, 9) and was superior to T-DM1 in the DESTINY-Breast03 (10). Moreover, T-DXd has recently received accelerated approval in patients with metastatic or unresectable HER2+ solid tumors who have received prior systemic treatment and have no other satisfactory options. Furthermore, DESTINY-Breast09 phase 3 trial assessing T-DXd ± pertuzumab (against THP) in the first-line treatment of HER2+ metastatic BC (MBC) is currently ongoing. However, data on progression and resistance to T-DXd remain limited. Neratinib, an irreversible pan-HER inhibitor, with chemotherapy, anti-HER2 or HER2 ADC consistently yielded favorable patient outcomes in the trastuzumab-refractory patients (11–14). Accordingly, it may also offer benefit in T-DXd–refractory setting through combinatorial approaches.
Here, we report a patient with HR+/HER2-amplified MBC who achieved a near-complete clinical response to trastuzumab deruxtecan but progressed after approximately 9 months. Upon progression on T-DXd, we observed rapid and near-complete resolution of the liver metastases through neratinib plus fulvestrant plus paclitaxel combination. This could offer an alternative therapeutic modality for HR+/HER2-amplified MBC in the post-T-DXd setting, which is currently not explored.
A 38-year-old female was diagnosed with invasive ductal breast carcinoma in 2015 and, consequently, underwent mastectomy. The surgical specimen was estrogen receptor-positive (ER+), progesterone receptor-negative (PR−), and HER2+ by IHC. She later received adjuvant anthracycline-based chemotherapy for 6 cycles, followed by tamoxifen. Bone metastases were detected approximately 1 year later, which were treated with palliative radiotherapy. The patient later received two anti-HER2–containing treatments: cisplatin, gemcitabine, and trastuzumab combination; and trastuzumab emtansine monotherapy (~8 months). Although partial responses were observed upon these regimens, it was followed by early progression. Capecitabine plus lapatinib was initiated, but the disease progressed with liver metastases, and the patient was admitted to our hospital for a personalized treatment approach.
The specimen from liver biopsy (liver segment II, Tru-cut) was ER+ (strong nuclear staining, 80%), PR− (no nuclear staining), and HER2− (no membranous staining, HercepTest score of 0) by pathological assessment in September 2023. Ki-67 proliferation index was 20% (at G1M phase by MIB-1 antibody). It exhibited carcinomatous infiltration consistent with metastatic breast ductal carcinoma. The tumor infiltrating the liver was characterized by low nuclear grade (modified Black I), low mitotic activity, and diffuse tubule formation (histological grade II), although it did not exhibit minimal distortion/deformation.
The initial comprehensive genomic profiling (Table 1) using the liver biopsy (Tempus, December 2022) detected GATA3 P409fs (c.1223_1224insT; VAF: 11.9%) mutation as well as copy number gains (CNGs) in ERBB2 (HER2, 11–13 copies, IHC-positive), ABBC3 (12), FGF3 (11), FGF4 (11), MCL1 (9), PPM1D (≥20), RARA (11), RPS6KB1 (≥20), and TOP2A (15). Tumor mutational burden was 3.7 muts/Mb, microsatellite instability status was stable, and Programmed death ligand 1 (PD-L1) tumor proportion score (TPS) and combined positive score (CPS) were <1% and <1, respectively. Transcriptomic profiling [research use only (RUO)] reported overexpression (OE) of ERBB2, TOP2A, AR, and MAPK3 but underexpression (UE) of CDKN2A. Considering that the patient exhausted all the standard treatment options as well as ERBB2 amplification with OE, we recommended trastuzumab deruxtecan (5.4 mg/kg) and achieved a near-complete response (Figures 1A, B).
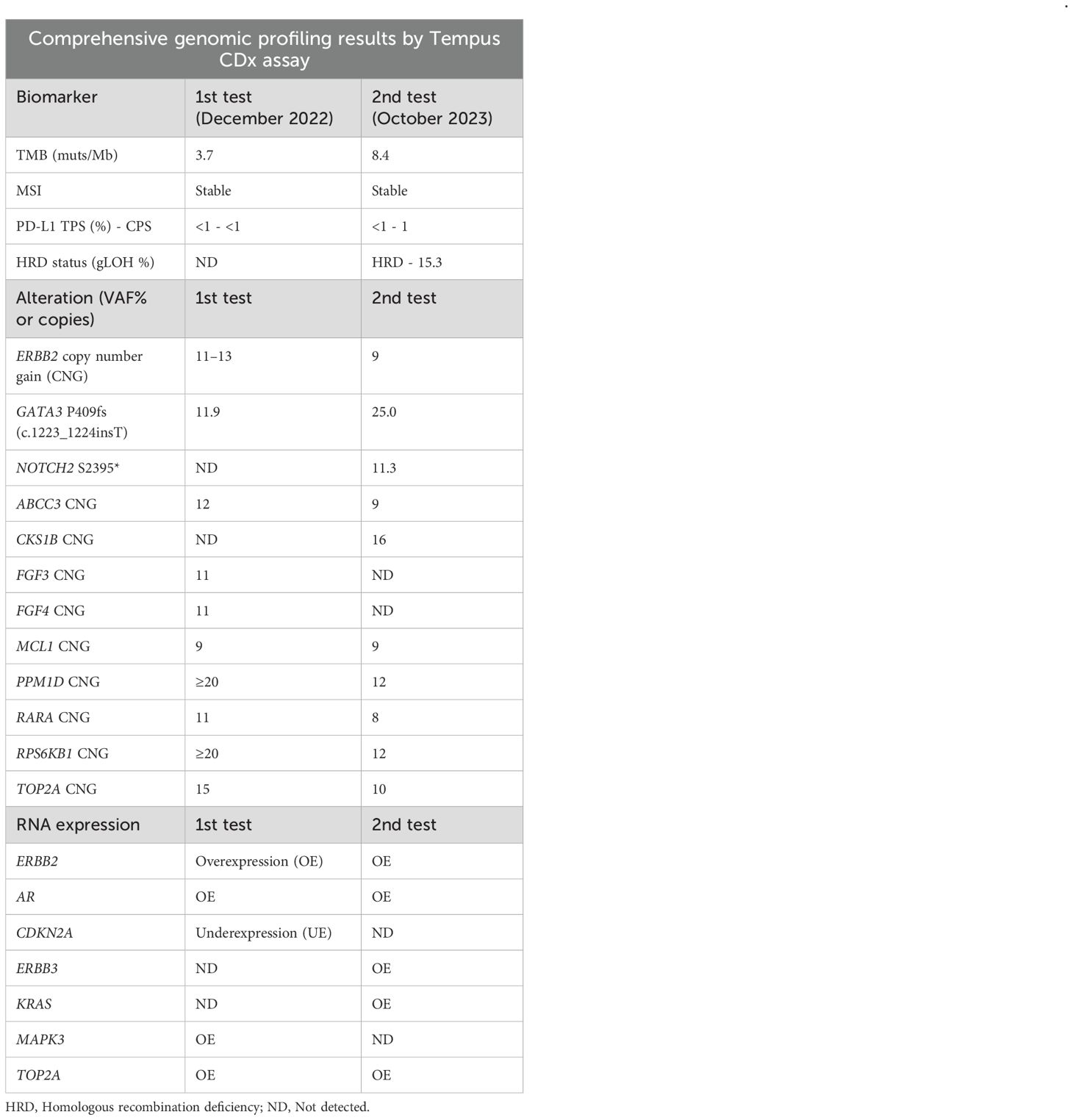
Table 1. Comparison of the genomic profiles (liver metastasis) before and after trastuzumab deruxtecan treatment.
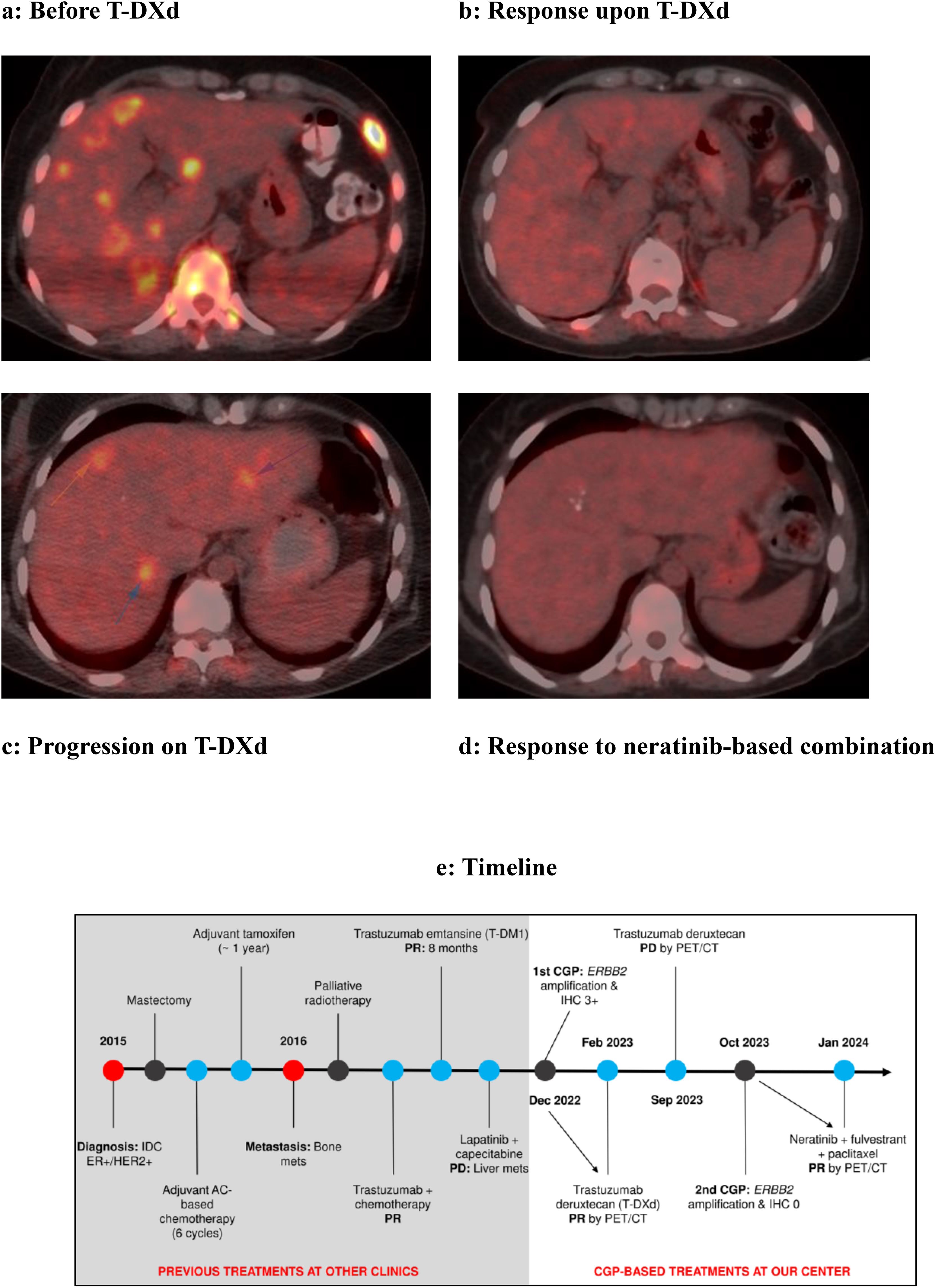
Figure 1. Near-complete responses in an HR+/HER2-amplified metastatic breast cancer patient, initially with trastuzumab deruxtecan (HER2 IHC–positive) and then with a neratinib-based combination (IHC-negative). (A) The December 2022 PET result showed multiple lesions with FDG uptake in the liver parenchyma consistent with metastasis. (B) The PET scan in February 2023 after T-DXd treatment did not reveal any lesions with significant FDG uptake. (C) In the September 2023 PET result, liver parenchyma shows several lesions with FDG uptake in the right and left lobes, consistent with metastasis (arrows). (D) In the January 2024 PET examination, no lesions showing FDG uptake could be detected in these lobes. (E) Disease and treatment timeline.
The second CGP test (Tempus, October 2023, Table 1) from a new liver biopsy revealed GATA3 P409fs (c.1223_1224insT, VAF of 25.0%) and NOTCH2 S2395* (c.7184C>G, VAF of 11.3%), and CNGs in ERBB2 (9 copies, IHC-negative), ABCC3 (9), CKS1B (16), MCL1 (9), PPM1D (12), RARA (8), RPS6KB1 (12), and TOP2A (10). The TMB was 8.4 muts/Mb, and microsatellite instability status was stable. PD-L1 TPS and CPS were <1% and 1, respectively. Homologous recombination deficiency status was negative (= not detected, LOH score of 15.3%, where threshold is 21%). Transcriptomic profiling reported ERBB2, ERBB3, TOP2A, AR, and KRAS OE.
Because we have previously achieved a near-complete response following T-DXd (Figures 1A, B) before progression within 9 months (Figure 1C), and it is important to target HER2 even after progression, we switched to HER2 TKI neratinib combined with fulvestrant and paclitaxel. The patient responded quickly and remarkably to this combination with a near-complete regression of the liver metastases (Figures 1C, D). The treatment was well-tolerated with grade 2 asthenia and decreased appetite. The initial dose for paclitaxel was 80 mg/m2/week, but we switched to 120 mg/m2 every 2 weeks to manage asthenia. The majority of the patients with neratinib-associated diarrhea experience it within the first month (15), but the patient did not report diarrhea, potentially owing to drug dose modifications and upfront loperamide use (3 days). The neratinib dose was selected as 120 mg/day (three 40-mg tablets), instead of the regular 240 mg/day (six 40-mg tablets) dose indicated in combination with capecitabine for advanced or metastatic BC (A/MBC). The 120 mg/day dose is usually utilized in the dose escalation regimen; however, we did not increase it to avoid tolerability issues. We did not modify fulvestrant dose (500 mg). The disease and treatment timeline is provided in Figure 1E.
The standard first-line treatment in HR+ and HER2+ BC consists of dual anti-HER2 in combination with taxane chemotherapy. Nevertheless, many patients still do not benefit from this regimen due to de novo or acquired resistance (16). In these patients, T-DXd could be primarily considered based on results from multiple phase III clinical trials. However, treatment options for patients with progression on or after T-DXd are limited and not currently explored in the clinical trials (17), except for a French multicenter retrospective study testing tucatinib, trastuzumab, and capecitabine (18). To the best of our knowledge, our case represents the first example that neratinib and fulvestrant–containing treatment could be highly efficacious in the T-DXd refractory HR+ MBC (Figure 1).
Tumors may have alterations at DNA, RNA, and protein levels, which may not always be consistent and may result in differential clinical outcomes. A recent study in multiple cancer types reported that ERBB2 mRNA OE (33.3%) was much more common than cases with IHC-positive (9.3%) and amplification (4.1%) (19). In patients with all three tests, only 7.5% were positive, whereas more than 60% were negative for all the tests, where 20% of mRNA OE cases were negative for amplification and IHC. In line, whereas HER2 mRNA OE was retained in two different CGP tests in our case, HER2 IHC changed from 3+ to 0 upon 9 months of T-DXd treatment. Another study comparing IHC and RNA reported a strong positive correlation, but baseline RNA levels were significantly higher in responders to T-DXd compared to the non-responders (20). More importantly, ERBB2 mRNA OE exhibited a significant correlation with HER2 protein levels in the ER-negative tumors but not in the ER-positive tumors (21), in keeping with our patient (ER+) having ERBB2 OE in the second CGP test but negative HER2 IHC. Moreover, mRNA level could define HER2 dependency and response to treatment in certain tumors, reported for a cholangiocarcinoma patient (19) and a gastric cancer patient with high ERBB2 mRNA (22). In addition, although HER2 mRNA level, IHC and adjusted plasma copy number were all significant predictors of response to T-DXd in the phase 2 DESTINY-Gastric01 (DG01) trial, mRNA outperformed the other parameters in terms of separating patients by overall response rate (ORR) and median overall survival (OS) (23). Still, HER2 protein level could explain differences between response to HER2-based approaches in many other cases, especially among IHC 3+ versus IHC 0 and, to some extent, those with equivocal IHC (2+). This is more prominent in the case of anti-HER2 agents as compared to HER2 ADCs or TKIs. For example, patients with BC with HER2 amplification but equivocal expression experienced a worse prognosis with a lower response rate following anti-HER2 treatment. This was independent of the HER2 copy number. These specimens were also enriched for trastuzumab resistance and ER signaling genes. DESTINY-CRC01 (DCRC01) trial of T-DXd in CRC patients reported that higher levels of HER2 biomarkers in baseline tissue and liquid biopsies, including HER2 status (IHC/ISH), HER2/CEP17 ratio, HER2 ISH signals, HER2 H-score, plasma HER2 [Human Epidermal Growth Factor Receptor 2 (ERBB2)] amplification status, HER2-adjusted plasma copy number, and HER2 extracellular domain correlate with antitumor activity (24). The ORR for patients with IHC 3+ was 57.5%, whereas it was only 7.7% for IHC 2+/ISH+. The median progression-free survival (PFS) and overall survival (OS) were also dramatically more favorable in the former versus the latter group, potentially explaining near-complete response to T-DXd when IHC was 3+ in our patient, and it was 0 when disease progressed on T-DXd. In preclinical models, HER2 homodimer level was associated with response to trastuzumab compared to EGFR: HER2 and HER2:HER3 heterodimers (25). ERBB2 and ERBB3 OE in our post-T-DXd specimen (Table 1) could cause increased HER2:HER3 heterodimers, thus potentially limiting therapeutic efficacy. DESTINY-Breast04 (DB04) and DESTINY-Breast06 phase 3 trials reported that T-DXd provided significantly longer PFS even in previously-treated HR+ HER2-low (IHC 1+ or IHC 2+/ISH−) and HER2-ultralow (IHC 0 with membrane staining; IHC > 0 <1+) A/MBC (26, 27). Importantly, however, HER2 expression significantly decreased at the time of resistance to T-DXd, although there was no clear difference in T-DXd uptake in the phase 2 DAISY trial (28). In our case, ERBB2 OE was present in pre- and posttreatment specimens, but decrease of copy number from 11–13 to 9 in the posttreatment could be indicative of reduced expression (Table 1). The trial also reported that best overall response (BOR) confirmed was 70.6% and 29.7%, median PFS of 11.1 months and 4.2 months, and median of OS 31.2 months and 12.1 months in Cohort 1 (IHC 3+ or ISH+) and Cohort 3 (IHC 0), respectively (29). This is consistent with our case, considering near-complete response when IHC 3+ and progression when IHC 0. The duration of response in the Cohort 1 of the DAISY trial was also similar to our case (9.7 vs. 9 months).
Genomic profiling of patients with ERBB2-positive BC before and after trastuzumab plus chemotherapy revealed that NOTCH2 and GATA3 mutations, along with others, were clonally enriched and/or acquired in the post-treatment samples (30), which could be also relevant in our case. The GATA3 P409fs variant allele frequency increased from 11.9% to 25.0% in the second CGP test, whereas the NOTCH2 mutation was only detected in the post-trastuzumab deruxtecan biopsy (Table 1). GATA3 mutations were identified in approximately 15% of HR+ patients (31, 32). P409fs was the most frequent variant in the SCAN-B BC cohort, and more common in the luminal/HER2− or ER+ subtype (33, 34). Although the initial tumor specimen from our patient was reported to be ER+/HER2+, the refractory tumor was ER+/HER2-. Frameshift GATA3 mutations could lead to either truncation or elongation of the protein, with potentially distinct downstream consequences. Accordingly, GATA3 could function as tumor suppressor or oncogene depending on the mutation (31, 32). Therefore, its role should be assessed on a per-patient basis. P409fs mutation results in an elongated protein product, and such extension mutations were associated with shorter disease-free survival (DFS) compared to other GATA3 mutations among The Cancer Genome Atlas (TCGA) Program BC patients (35). GATA3 mutations are associated with an increased GATA3 mRNA level (32). A positive correlation was also reported between GATA3 mRNA and protein levels in BC (36). Importantly, GATA3 IHC is routinely employed to ascertain breast or urothelial origin in carcinomas of unknown primary (37). GATA3 positivity was significantly associated with ER+ and p53 wild-type pattern in BC. GATA3 mutations and/or expression were shown to cause resistance to certain endocrine therapies while retaining sensitivity to others. For instance, patients with GATA3-mutant ER+ MBC had worse PFS and OS compared to those with GATA3 WT upon treatment with selective estrogen receptor degraders alone or in combination with CDK4/6 inhibitors (38). On the contrary, these mutations were associated with sensitivity to aromatase inhibitors (36, 39–41) and tamoxifen (42–44) in diverse settings. Considering significant outcomes in patients with HR+/HER2-low MBC upon T-DXd combined with anastrozole or fulvestrant in the DESTINY-Breast08 trial, T-DXd plus anastrozole could be prioritized for the HR+/HER2+ or HR+/HER2-low patients with GATA3 mutations. Another strategy could be the use of inhibitors against other proteins to limit GATA3-driven mechanisms, as there are no approved GATA3 inhibitors despite some preclinical molecules, such as pyrrothiogatain (45). For example, GATA3 and MDM2 were found to be synthetic lethal in ER+ BC (46), and MDM2 inhibitor milademetan was tested in a phase II clinical trial (DEMETER – NCT05932667) in combination with fulvestrant in patients with GATA3-mutant, ER+/HER2− A/MBC but it was terminated due to financial issues. Similarly, Histone deacetylase (HDAC) inhibition was shown to impair GATA3-dependent gene transcription (47), and HDAC inhibitor (HDACi) vorinostat in combination with tamoxifen was found to be clinically active in patients with endocrine-resistant BC (48). This approach could be re-tested in trials by combining HDACi with new generation of endocrine therapies. Direct and/or indirect strategies to NOTCH2 alterations are even less explored than GATA3 alterations. Gamma secretase inhibitors (GSIs) or pan-NOTCH inhibitors could be utilized to target NOTCH signaling; however, GSIs predominantly function through the inhibition of NOTCH1 signaling. Moreover, whereas NOTCH1 was characterized as an oncogene in BC, the role of NOTCH2 remains elusive (49, 50). Although GSI nirogacestat was approved by FDA for desmoid tumors and could be used off-label in other cancer types including the breast, GSI activity against NOTCH rearrangement and mutations could display significant differences by rearrangement product and location of the mutation, limiting their use as a general strategy for all NOTCH2 alterations. Very recently, a pan-NOTCH inhibitor RO4929097 was shown to reverse paclitaxel resistance in preclinical cancer models (51). Considering that dual anti-HER2 plus taxane and carboplatin plus paclitaxel with anti-HER2 regimens utilized in BC, such a strategy could be important in treatment-refractory patients.
Among the amplified genes, only MCL1 did not have a decreased copy number, and CKS1B CNG was only detected in the post-T-DXd specimen (Table 1). These genes are located on the same amplicon (1q21). CKS1B is involved in cell cycle regulation through its interaction with cyclin-dependent kinases (CDKs). Its overexpression has been associated with decreased OS and DFS, in part due to its association with loss of differentiation, young age, and negative Estrogen receptor/Progesterone receptor (ER/PR) status (52), whereas our patient was ER+/PR−. This OE could drive apoptosis in preclinical BC models upon Polo Like Kinase 1 (PLK1) inhibition (53), which could be activated by ERBB receptors (54). Consequently, response or resistance to HER2 ADC or HER2 TKI could be improved or overcome by PLK inhibition (55). Considering the lack of approved PLK1 inhibitors and its activity in kinetochore-microtubule dynamics and mitosis, microtubule-targeting agents or mitotic inhibitors could represent alternative therapeutic options. Taxanes are regularly used with anti-HER2 agents in HER2-positive BC. Furthermore, a mitotic inhibitor-bound HER2 ADC, T-DM1 is indicated for HER2-positive unresectable A/MBC who have previously received trastuzumab and taxane. MCL1, anti-apoptotic protein in Bcl-2 family, was identified as a clinical target in both HER2-amplified and triple-negative BCs (56) and implicated in resistance to HER2-targeted therapies (57). In these models, however, MCL1 inhibitor (S63845) demonstrated a synergistic activity with lapatinib, trastuzumab, and docetaxel. In line, constitutive BAK/MCL1 complexes were associated with paclitaxel and S63845 response in ovarian cancer PDX models.
Neratinib is a potentially overlooked treatment option for A/MBC, especially after progression on the standard-of-care (SOC) and could be utilized in combination with other therapeutics (11–14, 58, 59). Neratinib is even under investigation with T-DXd in advanced refractory gastric cancer patients (60). The initial phase I/II trials investigating neratinib and trastuzumab combination documented their tolerability and encouraging clinical activity, with durable responses up to 10-year observed in some patients (14). In phase III NALA trial, for example, neratinib plus capecitabine resulted in significantly prolonged PFS compared to lapatinib plus capecitabine in HER2+ MBC previously treated with at least two HER2-directed regimens (59), of whom almost all or more than half received trastuzumab or T-DM1, respectively. Furthermore, phase II NSABP FB-10 trial yielded an ORR of 63% upon neratinib plus T-DM1 in the HER2+ MBC (13, 61). ERBB2 amplification in study entry biopsies, ERBB2 RNA levels, and loss of detectable ctDNA and ERBB2 amplification in the ctDNA were identified as biomarkers of response. Our case is consistent with the first two biomarkers, although we do not have any data on ctDNA. Similar to T-DXd and unlike anti-HER2 agents, neratinib monotherapy could be also effective in HER2-low cases (62), explaining near-complete response in our patient despite HER2 IHC 0 with ERBB2 mRNA OE. Moreover, whereas p95HER2 was associated with trastuzumab resistance (63), two complete responders in the NSABP FB-10 trial had high total HER2 and p95HER2 levels in the baseline tissue. The p95HER2 is also likely to limit T-DXd activity (64), which could be one of the reasons driving resistance in our patient. Resistance to HER2-targeted therapies in HR+/HER2+ tumors following an initial response could be also caused by ER overexpression and/or activation (65, 66), potentially due to extensive bidirectional crosstalk between ER and HER2 signaling. Very recently, DESTINY-Breast08 reported remarkable outcomes in chemotherapy-naïve patients with HER2-low, HR+ MBC upon T-DXd combine with anastrozole or fulvestrant. Similarly, neratinib resulted in longer DFS only in HR+/HER2+ patients, almost all of whom also received ET, in the phase 3 ExteNET trial (12). Finally, the SUMMIT phase II trial in the patients with HR+/HER2−, HER2-mutant MBC not only supported a synergistic activity of neratinib with fulvestrant plus trastuzumab but also proved requirement for neratinib as there were no responses with fulvestrant or fulvestrant plus trastuzumab (67). HER2 mRNA expression did not significantly differ between partial response (PR), stable disease (SD), or progressive disease (PD) subgroups, although the sample numbers are quite low. Neratinib-containing regimen was even active in ERBB3 co-alterations (overexpressed in our case), implicating that HER2:HER3 heterodimer activity could be blocked in these tumors. Briefly, HER2 ADCs (with different platforms or payloads) or TKIs with ET combination could be tested in future clinical trials in the HR+ patients upon progression on T-DXd (17). These trials could be designed to not only assess the mutational profile but also other omics data such as transcriptome profiling by RNA sequencing, relevant serum/plasma biomarkers and cancer-specific clinical parameters. For example, the DG01 trial presented subgroup analyses regarding HER2 IHC, HER2 mRNA expression, plasma HER2 copy number/amplification and gain-of-function (GOF) mutations, and serum HER2 extracellular domain (ECD) (23). The DCRC01 also included HER2/CEP17 ratio, HER2 ISH signals, and HER2 H-score (24). The future trials of the T-DXd could be designed to analyze the efficacy by multiple HER2-related parameters utilized in this trial to define their relative importance as well as the outcomes for discordant cases (such as HER2 amplification and OE with IHC-negative status in our case). Unlike detailed analysis on the HER2, the DG01 performed subgroup analyses for only MET, EGFR, FGFR2, PIK3CA, and KRAS/NRAS based on their mutational status. Other DESTINY trials, such as Breast04 (ESR1, PIK3CA, and CDK4/6i resistance genes) (68), CRC01 (RAS, PIK3CA, and HER2) (24), and Lung01 (EGFR, KRAS/NRAS, and BRAF) (69), similarly focused on the mutational status of few genes. Accordingly, the alterations in genes with potential association to the T-DXd resistance in our case (GATA3, NOTCH2, CKS1B, and MCL1) could be highly relevant for multiple cancer types, primarily for breast, bladder, and gynecologic cancers as well as lung adenocarcinoma, lung squamous cell carcinoma, cholangiocarcinoma, and hepatocellular carcinoma [cBioPortal (70)]. However, these analyses should ideally be expanded to incorporate individual mRNA–, gene expression signature–, and even pathway activity scoring–based analyses while still considering alteration status, although the genes selected for mutational subgroup analysis in the DESTINY trials make sense given their frequency and clinical relevance on the studied cancer type. According to the results from potential studies outlined above, T-DXd combinations with HER2 TKIs (such as neratinib) and other drugs could be tested as the next step. It is important to note that these combinations should be assessed on the basis of precision oncology principles to match the right treatment with the right patient, maximize the clinical activity, and minimize the drug and financial toxicity through dose modifications and regimen scheduling.
Overall, to our knowledge, this is the first report showing the efficacy of HER2 TKI–based combination therapy in T-DXd–refractory MBC (Figure 1). Although T-DXd could be utilized even in HER2-ultralow patients, HER2 expression loss could impair its activity and cause disease progression. In this setting, we achieved a near-complete response with neratinib in combination with fulvestrant and paclitaxel in patients with heavily pretreated HR+, HER2-amplified but HER2-negative (by IHC) MBC.
CGP was performed by Tempus Labs Inc. (Chicago, IL, USA) through their proprietary technology. However, the methodology could be broadly outlined as follows: Formalin-fixed, paraffin-embedded tumor tissue blocks were retrieved, and hematoxylin and eosin–stained slides were reviewed by a board-certified pathologist to confirm tumor presence and assess tumor cellularity. Only samples with ≥20% tumor cellularity were included. Blood samples were also collected as a control for germline analysis. DNA and RNA were extracted from the tissue samples using the Tempus xT proprietary extraction protocols. The concentration and quality of the extracted nucleic acids were assessed. For DNA sequencing, libraries were prepared using the Tempus xT library preparation kit. For RNA sequencing, cDNA synthesis was performed, followed by library preparation using the Tempus xT RNA-seq kit. Paired-end sequencing was performed using an Illumina NextSeq or NovaSeq platform. DNA libraries were sequenced to an average depth of 500× coverage, whereas RNA libraries were sequenced to an average depth of 100 million reads per sample. Raw sequencing data were processed using the Tempus xT bioinformatics pipeline. A detailed report was generated for each patient, summarizing the clinically relevant findings. The report included information on actionable mutations, potential therapeutic targets, and relevant clinical trials.
Our team in the molecular tumor board discussions consists of medical oncologists, molecular biologists, geneticists, radiologists, and, sometimes, surgeons, a pathologist, and a medical geneticist. Considering that the patient has been previously benefited from anti-HER2–based treatment, tumor specimen was still HER2-positive and remarkable responses to trastuzumab deruxtecan in multiple settings in breast and pan-cancer cohorts, we initially started treatment with T-DXd. A near-complete response was observed in the liver metastases. Upon progression, we switched to neratinib, fulvestrant, and paclitaxel combination. This was based on the following rationale: ER signaling could impair clinical activity of anti-HER2 agents, HER2 blockade is still important even in patients progressing on or after anti-HER2 treatment, neratinib could irreversibly inhibit both membranous and intracellular (if any) HER2 proteins, and mitotic inhibitor paclitaxel could help targeting CKS1B and MCL1 CNGs within the combination regimen.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethical approval was not required for the studies involving humans because they were conducted in accordance with the local legislation and institutional requirements, which do not stipulate an ethical committee application & approval for the case studies as the patient provided a written informed consent to participate and publication of her anonymized data in this study. Each treatment is patient-specific as all the treatment decisions are taken via molecular tumor board discussions based on comprehensive genomic profiling. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
ÜMT: Conceptualization, Data curation, Visualization, Writing – original draft, Writing – review & editing. AA: Writing – review & editing. EA: Writing – review & editing. ŞNB: Writing – review & editing. EÖ: Writing – review & editing. OT: Visualization, Writing – review & editing. MD: Conceptualization, Project administration, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We are grateful to our patient who made this study possible and all the members of the medical oncology team involved in the treatment and care process.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Sedeta ET, Jobre B, Avezbakiyev B. Breast cancer: Global patterns of incidence, mortality, and trends. J Clin Oncol. (2023). doi: 10.1200/JCO.2023.41.16_suppl.10528
3. Fitzgibbons PL, Dillon DA, Alsabeh R, Berman MA, Hayes DF, Hicks DG, et al. Template for reporting results of biomarker testing of specimens from patients with carcinoma of the breast. Arch Pathol Lab Med. (2014) 138:595–601. doi: 10.5858/arpa.2013-0566-CP
4. Debien V, de Azambuja E, Piccart-Gebhart M. Optimizing treatment for HER2-positive HR-positive breast cancer. Cancer Treat Rev. (2023) 115:102529. doi: 10.1016/j.ctrv.2023.102529
5. Boscolo Bielo L, Trapani D, Nicolo E, Valenza C, Guidi L, Belli C, et al. The evolving landscape of metastatic HER2-positive, hormone receptor-positive Breast Cancer. Cancer Treat Rev. (2024) 128:102761. doi: 10.1016/j.ctrv.2024.102761
6. Miles D, Ciruelos E, Schneeweiss A, Puglisi F, Peretz-Yablonski T, Campone M, et al. Final results from the PERUSE study of first-line pertuzumab plus trastuzumab plus a taxane for HER2-positive locally recurrent or metastatic breast cancer, with a multivariable approach to guide prognostication. Ann Oncol. (2021) 32:1245–55. doi: 10.1016/j.annonc.2021.06.024
7. Swain SM, Miles D, Kim S-B, Im Y-H, Im S-A, Semiglazov V, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. (2020) 21:519–30. doi: 10.1016/S1470-2045(19)30863-0
8. Modi S, Saura C, Yamashita T, Park YH, Kim S-B, Tamura K, et al. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. New Engl J Med. (2020) 382:610–21. doi: 10.1056/NEJMoa1914510
9. André F, Park YH, Kim S-B, Takano T, Im S-A, Borges G, et al. Trastuzumab deruxtecan versus treatment of physician’s choice in patients with HER2-positive metastatic breast cancer (DESTINY-Breast02): a randomised, open-label, multicentre, phase 3 trial. Lancet. (2023) 401:1773–85. doi: 10.1016/S0140-6736(23)00725-0
10. Cortés J, Kim S-B, Chung W-P, Im S-A, Park YH, Hegg R, et al. Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. New Engl J Med. (2022) 386:1143–54. doi: 10.1056/NEJMoa2115022
11. Tao Z, Li SX, Shen K, Zhao Y, Zeng H, Ma X. Safety and efficacy profile of neratinib: a systematic review and meta-analysis of 23 prospective clinical trials. Clin Drug Invest. (2019) 39:27–43. doi: 10.1007/s40261-018-0719-0
12. Chan A, Delaloge S, Holmes FA, Moy B, Iwata H, Harvey VJ, et al. Neratinib after trastuzumab-based adjuvant therapy in patients with HER2-positive breast cancer (ExteNET): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. (2016) 17:367–77. doi: 10.1016/S1470-2045(15)00551-3
13. Abraham J, Montero AJ, Jankowitz RC, Salkeni MA, Beumer JH, Kiesel BF, et al. Safety and efficacy of T-DM1 plus neratinib in patients with metastatic HER2-positive breast cancer: NSABP foundation trial FB-10. J Clin Oncol. (2019) 37:2601. doi: 10.1200/JCO.19.00858
14. Blackwell KL, Zaman K, Qin S, Tkaczuk KH, Campone M, Hunt D, et al. Neratinib in combination with trastuzumab for the treatment of patients with advanced HER2-positive breast cancer: a phase I/II study. Clin Breast Cancer. (2019) 19:97–104. doi: 10.1016/j.clbc.2018.12.011
15. Mortimer J, Di Palma J, Schmid K, Ye Y, Jahanzeb M. Patterns of occurrence and implications of neratinib-associated diarrhea in patients with HER2-positive breast cancer: analyses from the randomized phase III ExteNET trial. Breast Cancer Res. (2019) 21:32. doi: 10.1186/s13058-019-1112-5
16. Ishii K, Morii N, Yamashiro H. Pertuzumab in the treatment of HER2-positive breast cancer: an evidence-based review of its safety, efficacy, and place in therapy. Core evidence. (2019) 14:51–70. doi: 10.2147/CE.S217848
17. Nader-Marta G, Martins-Branco D, De Azambuja E. How we treat patients with metastatic HER2-positive breast cancer. ESMO Open. (2022) 7:100343. doi: 10.1016/j.esmoop.2021.100343
18. Frenel J-S, Zeghondy J, Guerin C, Mailliez A, Volant E, Poumeaud F, et al. Efficacy of tucatinib+ trastuzumab+ capecitabine (TTC) after trastuzumab-deruxtecan (T-DXd) exposure in Her2-positive metastatic breast cancer: A French multicentre retrospective study. Am Soc Clin Oncol. (2023) 41(16). doi: 10.1200/JCO.2023.41.16_suppl.1014
19. Shayeb AM, Kurzrock R, Adashek JJ, Kato S. Comprehensive analysis of human epidermal growth factor receptor 2 through DNA, mRNA, and protein in diverse Malignancies. JCO Precis Oncol. (2023) 7:e2200604. doi: 10.1200/PO.22.00604
20. Li X, Lee J-H, Gao Y, Zhang J, Bates KM, Rimm DL, et al. Correlation of HER2 protein level with mRNA level quantified by RNAscope in breast cancer. Modern Pathol. (2024) 37:100408. doi: 10.1016/j.modpat.2023.100408
21. Triulzi T, Regondi V, Venturelli E, Gasparini P, Ghirelli C, Groppelli J, et al. HER2 mRNA levels, estrogen receptor activity and susceptibility to trastuzumab in primary breast cancer. Cancers. (2022) 14:5650. doi: 10.3390/cancers14225650
22. Griguolo G, Braso-Maristany F, Gonzalez-Farre B, Pascual T, Chic N, Sauri T, et al. ERBB2 mRNA expression and response to ado-trastuzumab emtansine (T-DM1) in HER2-positive breast cancer. Cancers (Basel). (2020) 12:1902. doi: 10.3390/cancers12071902
23. Shitara K, Bang YJ, Iwasa S, Sugimoto N, Ryu MH, Sakai D, et al. Trastuzumab deruxtecan in HER2-positive advanced gastric cancer: exploratory biomarker analysis of the randomized, phase 2 DESTINY-Gastric01 trial. Nat Med. (2024) 30:1933–42. doi: 10.1038/s41591-024-02992-x
24. Siena S, Raghav K, Masuishi T, Yamaguchi K, Nishina T, Elez E, et al. HER2-related biomarkers predict clinical outcomes with trastuzumab deruxtecan treatment in patients with HER2-expressing metastatic colorectal cancer: biomarker analyses of DESTINY-CRC01. Nat Commun. (2024) 15:10213. doi: 10.1038/s41467-024-53223-3
25. Ghosh R, Narasanna A, Wang SE, Liu S, Chakrabarty A, Balko JM, et al. Trastuzumab has preferential activity against breast cancers driven by HER2 homodimers. Cancer Res. (2011) 71:1871–82. doi: 10.1158/0008-5472.CAN-10-1872
26. Modi S, Jacot W, Yamashita T, Sohn J, Vidal M, Tokunaga E, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. (2022) 387:9–20. doi: 10.1056/NEJMoa2203690
27. Bardia A, Hu X, Dent R, Yonemor K, Barrios CH, O'Shaughnessy JA, et al. Trastuzumab aeruxtecan after endocrine therapy in metastatic breast cancer. N Engl J Med. (2024) 391(22):2110–22. doi: 10.1056/NEJMoa2407086
28. Mosele F, Deluche E, Lusque A, Le Bescond L, Filleron T, Pradat Y, et al. Trastuzumab deruxtecan in metastatic breast cancer with variable HER2 expression: the phase 2 DAISY trial. Nat Med. (2023) 29:2110–20. doi: 10.1038/s41591-023-02478-2
29. Dieras V, André F, Lusque A, Pistilli B, Bachelot T, Pierga J, et al. 7P Trastuzumab deruxtecan (T-DXd) for advanced breast cancer (ABC) patients (pts), regardless of HER2 status: A phase II study with biomarkers analysis (DAISY)-update analysis with longer follow-up. ESMO Open. (2024) 9. doi: 10.1016/j.esmoop.2024.103016
30. Lipsyc-Sharf M, Jain E, Collins LC, Rosenberg SM, Ruddy KJ, Tamimi RM, et al. Genomics of ERBB2-Positive breast cancer in young women before and after exposure to chemotherapy plus trastuzumab. JCO Precis Oncol. (2023) 7:e2300076. doi: 10.1200/PO.23.00076
31. Luen SJ, Viale G, Nik-Zainal S, Savas P, Kammler R, Dell'Orto P, et al. Genomic characterisation of hormone receptor-positive breast cancer arising in very young women. Ann Oncol. (2023) 34:397–409. doi: 10.1016/j.annonc.2023.01.009
32. Liu J, Prager-van der Smissen WJ, Look MP, Sieuwerts AM, Smid M, Meijer-van Gelder ME, et al. GATA3 mRNA expression, but not mutation, associates with longer progression-free survival in ER-positive breast cancer patients treated with first-line tamoxifen for recurrent disease. Cancer Lett. (2016) 376:104–9. doi: 10.1016/j.canlet.2016.03.038
33. Brueffer C, Gladchuk S, Winter C, Vallon-Christersson J, Hegardt C, Hakkinen J, et al. The mutational landscape of the SCAN-B real-world primary breast cancer transcriptome. EMBO Mol Med. (2020) 12:e12118. doi: 10.1101/2020.01.30.926733
34. Lang GT, Jiang YZ, Shi JX, Yang F, Li XG, Pei YC, et al. Characterization of the genomic landscape and actionable mutations in Chinese breast cancers by clinical sequencing. Nat Commun. (2020) 11:5679. doi: 10.1038/s41467-020-19342-3
35. Mair B, Konopka T, Kerzendorfer C, Sleiman K, Salic S, Serra V, et al. Gain- and loss-of-Function mutations in the breast cancer gene GATA3 result in differential drug sensitivity. PloS Genet. (2016) 12:e1006279. doi: 10.1371/journal.pgen.1006279
36. Chen X, Zhao W, Huang Y, Luo S, Tang X, Yi Q. Association of GATA3 expression in triple-positive breast cancer with overall survival and immune cell infiltration. Sci Rep. (2024) 14:17795. doi: 10.1038/s41598-024-68788-8
37. Querzoli P, Pedriali M, Rinaldi R, Secchiero P, Rossi PG, Kuhn E. GATA3 as an adjunct prognostic factor in breast cancer patients with less aggressive disease: A study with a review of the literature. Diagnostics (Basel). (2021) 11:604. doi: 10.3390/diagnostics11040604
38. Velimirovic M, Gerratana L, Davis AA, Dai CS, Cheng J, Iafrate AJ, et al. Landscape of GATA3 mutations identified from circulating tumor DNA clinical testing and their impact on disease outcomes in estrogen receptor-positive (ER+) metastatic breast cancers treated with endocrine therapies. J Clin Oncol. (2021). doi: 10.1200/JCO.2021.39.15_suppl.1065
39. Parikh P, Palazzo JP, Rose LJ, Daskalakis C, Weigel RJ. GATA-3 expression as a predictor of hormone response in breast cancer. J Am Coll Surg. (2005) 200:705–10. doi: 10.1016/j.jamcollsurg.2004.12.025
40. Dunbier AK, Ghazoui Z, Anderson H, Salter J, Nerurkar A, Osin P, et al. Molecular profiling of aromatase inhibitor-treated postmenopausal breast tumors identifies immune-related correlates of resistance. Clin Cancer Res. (2013) 19:2775–86. doi: 10.1158/1078-0432.CCR-12-1000
41. Rodrigues Alves N, Duarte AF, Ribeiro DF, Silva RS, Carvalho BA, Alpuim Costa D. Successful management of bilateral orbital metastases from invasive lobular breast cancer with abemaciclib and letrozole: a case report and literature review. Front Oncol. (2024) 14:1286910. doi: 10.3389/fonc.2024.1286910
42. Jacquemier J, Charafe-Jauffret E, Monville F, Esterni B, Extra JM, Houvenaeghel G, et al. Association of GATA3, P53, Ki67 status and vascular peritumoral invasion are strongly prognostic in luminal breast cancer. Breast Cancer Res. (2009) 11:R23. doi: 10.1186/bcr2249
43. Goetz MP, Hamilton EP, Campone M, Hurvitz SA, Cortes J, Johnston S, et al. Landscape of baseline and acquired genomic alterations in circulating tumor DNA with abemaciclib alone or with endocrine therapy in advanced breast cancer. Clin Cancer Res. (2024) 30:2233–44. doi: 10.1158/1078-0432.CCR-22-3573
44. Sandstrom J, Bomanson J, Perez-Tenorio G, Jonsson C, Nordenskjold B, Fornander T, et al. GATA3 and markers of epithelial-mesenchymal transition predict long-term benefit from tamoxifen in ER-positive breast cancer. NPJ Breast Cancer. (2024) 10:78. doi: 10.1038/s41523-024-00688-6
45. Nomura S, Takahashi H, Suzuki J, Kuwahara M, Yamashita M, Sawasaki T. Pyrrothiogatain acts as an inhibitor of GATA family proteins and inhibits Th2 cell differentiation in vitro. Sci Rep. (2019) 9:17335. doi: 10.1038/s41598-019-53856-1
46. Bianco G, Coto-Llerena M, Gallon J, Kancherla V, Taha-Mehlitz S, Marinucci M. GATA3 and MDM2 are synthetic lethal in estrogen receptor-positive breast cancers. Commun Biol. (2022) 5:373. doi: 10.1038/s42003-022-03296-x
47. Geng X, Wang C, Abdelrahman S. et al: GATA-3-dependent Gene Transcription is Impaired upon HDAC Inhibition. Clin Cancer Res. (2024) 30:1054–66. doi: 10.1158/1078-0432.CCR-23-1699
48. Munster PN, Thurn KT, Thomas S, Raha P, Lacevic M, Miller A, et al. A phase II study of the histone deacetylase inhibitor vorinostat combined with tamoxifen for the treatment of patients with hormone therapy-resistant breast cancer. Br J Cancer. (2011) 104:1828–35. doi: 10.1038/bjc.2011.156
49. Nandi A, Chakrabarti R. The many facets of Notch signaling in breast cancer: toward overcoming therapeutic resistance. Genes Dev. (2020) 34:1422–38. doi: 10.1101/gad.342287.120
50. Yousefi H, Bahramy A, Zafari N, Delavar MR, Nguyen K, Haghi A, et al. Notch signaling pathway: a comprehensive prognostic and gene expression profile analysis in breast cancer. BMC Cancer. (2022) 22:1282. doi: 10.1186/s12885-022-10383-z
51. Yu F, Zhou Q, Zhou T, Xie Y, Zhang P, He W, et al. Targeting NOTCH2-JAG1 juxtacrine signaling reverses macrophage-mediated tumor resistance to taxol. bioRxiv. (2024), 602467. doi: 10.1101/2024.07.08.602467
52. Slotky M, Shapira M, Ben-Izhak O, Linn S, Futerman B, Tsalic M, et al. The expression of the ubiquitin ligase subunit Cks1 in human breast cancer. Breast Cancer Res. (2005) 7:1–8. doi: 10.1186/bcr1278
53. Reid RJ, Du X, Sunjevaric I, Rayannavar V, Dittmar J, Bryant E, et al. A synthetic dosage lethal genetic interaction between CKS1B and PLK1 is conserved in yeast and human cancer cells. Genetics. (2016) 204:807–19. doi: 10.1534/genetics.116.190231
54. Momeny M, Zarrinrad G, Moghaddaskho F, Poursheikhani A, Sankanian G, Zaghal A, et al. Dacomitinib, a pan-inhibitor of ErbB receptors, suppresses growth and invasive capacity of chemoresistant ovarian carcinoma cells. Sci Rep. (2017) 7:4204. doi: 10.1038/s41598-017-04147-0
55. Saatci Ö, Borgoni S, Akbulut Ö, Durmuş S, Raza U, Eyüpoğlu E, et al. Targeting PLK1 overcomes T-DM1 resistance via CDK1-dependent phosphorylation and inactivation of Bcl-2/xL in HER2-positive breast cancer. Oncogene. (2018) 37:2251–69. doi: 10.1038/s41388-017-0108-9
56. Merino D, Whittle JR, Vaillant F, Serrano A, Gong JN, Giner G, et al. Synergistic action of the MCL-1 inhibitor S63845 with current therapies in preclinical models of triple-negative and HER2-amplified breast cancer. Sci Transl Med. (2017) 9. doi: 10.1126/scitranslmed.aam7049
57. Floros KV, Lochmann TL, Hu B, Monterrubio C, Hughes MT, Wells JD, et al. Coamplification of miR-4728 protects HER2-amplified breast cancers from targeted therapy. Proc Natl Acad Sci U.S.A. (2018) 115:E2594–603. doi: 10.1073/pnas.1717820115
58. Guo L, Shao W, Zhou C, Yang H, Yang L, Cai Q, et al. Neratinib for HER2-positive breast cancer with an overlooked option. Mol Med. (2023) 29:134. doi: 10.1186/s10020-023-00736-0
59. Saura C, Oliveira M, Feng Y-H, Dai M-S, Chen S-W, Hurvitz SA, et al. Neratinib plus capecitabine versus lapatinib plus capecitabine in HER2-positive metastatic breast cancer previously treated with≥ 2 HER2-directed regimens: phase III NALA trial. J Clin Oncol. (2020) 38:3138. doi: 10.1200/JCO.20.00147
60. Nakrani R, Singh T, Handorf E, Alpaugh KR, Vijayvergia N. TIP24-198: A multi-center phase I trial of neratinib and fam-trastuzumab deruxtecan in advanced refractory gastric cancer patients. J Natl Compr Cancer Network. (2024) 22. doi: 10.6004/jnccn.2023.7221
61. Swain SM, Tang G, Brauer HA, Goerlitz DS, Lucas PC, Robidoux A, et al. NSABP B-41, a randomized neoadjuvant trial: Genes and signatures associated with pathologic complete response. Clin Cancer Res. (2020) 26:4233–41. doi: 10.1158/1078-0432.CCR-20-0152
62. Arshad M, Azad A, Chan PYK, Vigneswara V, Feldinger K, Nafi SNM, et al. Neratinib could be effective as monotherapy or in combination with trastuzumab in HER2-low breast cancer cells and organoid models. Br J Cancer. (2024) 130:1990–2002. doi: 10.1038/s41416-024-02665-z
63. Canonici A, Gijsen M, Mullooly M, Bennett R, Bouguern N, Pedersen K, et al. Neratinib overcomes trastuzumab resistance in HER2 amplified breast cancer. Oncotarget. (2013) 4:1592. doi: 10.18632/oncotarget.v4i10
64. Guidi L, Pellizzari G, Tarantino P, Valenza C, Curigliano G. Resistance to antibody-drug conjugates targeting HER2 in breast cancer: molecular landscape and future challenges. Cancers. (2023) 15:1130. doi: 10.3390/cancers15041130
65. Fumagalli D, Venet D, Ignatiadis M, Azim HA, Maetens M, Rothé F, et al. RNA sequencing to predict response to neoadjuvant anti-HER2 therapy: a secondary analysis of the NeoALTTO randomized clinical trial. JAMA Oncol. (2017) 3:227–34. doi: 10.1001/jamaoncol.2016.3824
66. Atallah NM, Alsaleem M, Toss MS, Mongan NP, Rakha E. Differential response of HER2-positive breast cancer to anti-HER2 therapy based on HER2 protein expression level. Br J Cancer. (2023) 129:1692–705. doi: 10.1038/s41416-023-02426-4
67. Jhaveri K, Eli LD, Wildiers H, Hurvitz SA, Guerrero-Zotano A, Unni N, et al. Neratinib+ fulvestrant+ trastuzumab for HR-positive, HER2-negative, HER2-mutant metastatic breast cancer: outcomes and biomarker analysis from the SUMMIT trial. Ann Oncol. (2023) 34:885–98. doi: 10.1016/j.annonc.2023.08.003
68. Modi S, Niikura N, Yamashita T, Jacot W, Sohn J, Tokunaga E, et al. Trastuzumab deruxtecan (T-DXd) vs treatment of physician’s choice (TPC) in patients (pts) with HER2-low, hormone receptor-positive (HR+) unresectable and/or metastatic breast cancer (mBC): Exploratory biomarker analysis of DESTINY-Breast04. J Clin Oncol. (2023). doi: 10.1200/JCO.2023.41.16_suppl.1020
69. Smit EF, Felip E, Uprety D, Nagasaka M, Nakagawa K, Rodríguez LP-A, et al. Trastuzumab deruxtecan in patients with metastatic non-small-cell lung cancer (DESTINY-Lung01): Primary results of the HER2-overexpressing cohorts from a single-arm, phase 2 trial. Lancet Oncol. (2024) 25:439–54. doi: 10.1016/S1470-2045(24)00064-0
Keywords: breast cancer, precision oncology, cancer genomics, HER2 antibody-drug conjugates (HER2 ADC), trastuzumab deruxtecan, neratinib, molecular tumor board (MTB)
Citation: Tokat ÜM, Adibi A, Aydın E, Bilgiç ŞN, Özgü E, Tutar O and Demiray M (2025) Case report: Near-complete response to neratinib-based treatment in HR-positive HER2-amplified metastatic breast cancer refractory to trastuzumab deruxtecan. Front. Oncol. 14:1484750. doi: 10.3389/fonc.2024.1484750
Received: 22 August 2024; Accepted: 27 December 2024;
Published: 21 January 2025.
Edited by:
Hailin Tang, Sun Yat-sen University Cancer Center (SYSUCC), ChinaReviewed by:
Zhou Wen, South China University of Technology, ChinaCopyright © 2025 Tokat, Adibi, Aydın, Bilgiç, Özgü, Tutar and Demiray. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ünal Metin Tokat, dW10b2thdEBnbWFpbC5jb20=; Mutlu Demiray, ZHJkZW1pcmF5QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.