 Xinyi Zhang1Xiaofei Chu2Jun Wang1Wenjing Gu1Xiaoyan Fu1Jing Zhang1Congying Wang1Qinghui Han1Jing Zhou1Yongjing Zhang1
Xinyi Zhang1Xiaofei Chu2Jun Wang1Wenjing Gu1Xiaoyan Fu1Jing Zhang1Congying Wang1Qinghui Han1Jing Zhou1Yongjing Zhang1 Xiaoyan Liu1*
Xiaoyan Liu1*- 1Pharmacy Department, Baotou Cancer Hospital, Baotou, China
- 2Pharmacy Department, The Fourth Hospital of Baotou, Baotou, China
Introduction: The advent of bevacizumab has considerably transformed the therapeutic landscape for non-small cell lung cancer (NSCLC) patients devoid of specific genetic mutations. A pivotal milestone has been reached with the recent approval of a bevacizumab biosimilar, following rigorous phase III clinical investigations, poised to augment NSCLC therapeutic strategies.
Methods: This retrospective analysis encompasses a large-scale study conducted between January 2021 and December 2023, involving 1058 NSCLC patients (metastatic or locally advanced stages). The research design entailed a comparative assessment of the safety and efficacy profiles of combined therapies using the original bevacizumab and its biosimilar, adhering to RECIST v1.1 criteria. Adverse event grading was standardized using the National Cancer Institute’s CTCAE v5.0.
Results: Notably, the biosimilar demonstrated an objective response rate (ORR) of 29.79% in 606 patients, closely paralleling the 27.41% ORR observed in 452 patients receiving the original drug, with insignificant risk differences (-0.03) and a risk ratio of 0.987, affirming equivalence. Progression-free survival (PFS) was influenced by radiation status, treatment lines, and regimen combinations, while dosage intensity and genetic factors had negligible impacts. The incidence of treatment-emergent adverse events (TEAEs) was slightly higher in the biosimilar group (75.11%) versus the original drug group (72.78%), with grade 3 or more severe TEAEs occurring in 23.6% and 18.5% of patients, respectively (Detailed criteria for the definition and assessment of TEAEs have been added to the Methods section, including the use of the National Cancer Institute’s CTCAE v5.0 for grading).
Conclusions: The study affirms that bevacizumab biosimilars offer equivalent therapeutic efficacy and a similar safety profile to the originator product in the management of locally advanced or metastatic NSCLC. The tolerability of the toxicity profile, coupled with the absence of unforeseen adverse reactions, underscores the viability of biosimilar bevacizumab as a valuable addition to NSCLC treatment regimens. These findings also imply potential benefits for a broader patient population beyond clinical trial confines through the adoption of biosimilar beta-adrenergic blocking agents.
Introduction
Biosimilars are biologic medical products engineered to closely mirror approved biologic drugs, known as originator or reference drugs. Unlike generics, which replicate small-molecule drugs exactly, biosimilars are complex proteins produced through biotech processes, making them inherently variable from batch to batch (1–3). To qualify as a biosimilar, a product must exhibit no clinically significant differences in safety, purity, and potency compared to its reference drug, as enforced by regulatory bodies like the FDA and EMA (4). Post-patent expiration, biosimilars foster market competition, reducing costs and enhancing patient access to vital biologic therapies (5). Ongoing clinical monitoring is crucial to maintain high standards of safety and efficacy, particularly in critical areas like oncology treatment (6).
Biosimilars are medications closely modeled after approved biologic drugs, known as originator or reference products. Unlike traditional generics, which replicate small-molecule drugs identically, biosimilars are complex protein-based therapeutics produced through biotechnological processes, making them highly similar yet not identical to the original biologics (7–10). Examples include bevacizumab biosimilars (Mvasi by Amgen and Zaltrap by Sanofi), which closely resemble Avastin, used in treating multiple cancer types; trastuzumab biosimilars (Herzuma by Celltrion and Ontruzant by Samsung Bioepis), which mimic Herceptin for breast and stomach cancers; and adalimumab biosimilars (Amjevita by Amgen and Cyltezo by Boehringer Ingelheim), which are closely aligned with Humira for autoimmune disorders. These biosimilars, after passing rigorous tests and evaluations by regulatory authorities such as the FDA and EMA to ensure their safety, purity, and potency, offer the potential for reduced healthcare costs and increased accessibility to biologic medicines worldwide (11–14).
Lung cancer remains the leading cause of cancer-related deaths globally, with an estimated 1.8 million deaths annually (15). More than half of diagnosed patients present with distant metastases, making surgical interventions less viable (16). In China, where lung cancer is a major public health issue (17), non-small cell lung cancer (NSCLC) accounts for approximately 85% of cases. While early-stage NSCLC may be treated with surgery, chemotherapy is crucial for advanced stages. Advances in molecular biology have enabled personalized therapies such as immunotherapy and targeted therapy, improving patient outcomes (18). For advanced NSCLC without actionable oncogenes, immunocheckpoint inhibitors (ICIs) have become a new treatment option, although they show monotherapy efficacy in only 20% of cases (19).
Bevacizumab, a recombinant humanized monoclonal antibody, inhibits angiogenesis and VEGF activity by selectively blocking its binding to endothelial cell receptors (20). Randomized trials have shown improved overall survival (OS) and progression-free survival (PFS) when bevacizumab is used with chemotherapy (21). Innovations in maintenance therapy advocate combining bevacizumab with immunotherapies or targeted agents to address disease progression (22).
A biosimilar is a biological product closely resembling the reference product without substantial differences in safety, purity, or potency (23). They can significantly reduce healthcare spending without compromising therapeutic effectiveness (24). Although biosimilars are safe, they require special care due to their differences from the original product (25). Prospective clinical trials have demonstrated that a bevacizumab biosimilar combined with chemotherapy is as effective and safe as bevacizumab in advanced non-squamous NSCLC (26).
Biosimilars are therapeutic biological products that exhibit comparable quality, safety, and efficacy to the approved reference medicine (27). The rapid development of bevacizumab biosimilars follows the reduction in patent protection for Avastin. China has a competitive market with up to seven domestic bevacizumab biosimilars, five of which were approved in 2021. Due to their complex production and limited shelf life, further investigation is required to substantiate their efficacy and safety (28–33).
This study aims to compare the safety and effectiveness of bevacizumab biosimilars with the original drug in combination with chemotherapy for NSCLC (34–36).
Biosimilars, particularly bevacizumab biosimilars, offer a cost-effective alternative for treating NSCLC without compromising therapeutic efficacy. They present a compelling proposition in the context of rising healthcare costs, enhancing affordability and broadening patient access to life-saving treatments (37–39).
This study is critical for public health policies. Biosimilars facilitate a reduction in the financial burden on healthcare systems, enabling resource reallocation and stimulating market competition, which drives down prices and promotes innovation. Investigating biosimilars’ safety and efficacy in real-world settings contributes to informed policy decisions (31, 40–44).
Methodology
Study design and patient population
A total of 1058 patient records were retrospectively reviewed in the analysis. The study is retrospective, meaning it analyzes data collected from past medical records.
A comprehensive examination was conducted on the medical records of patients diagnosed with locally advanced or advanced non-squamous NSCLC who underwent treatment at Baotou Cancer Hospital between 1 January 2022 and 31 December 2023. Individuals who received either the original or biosimilar form of bevacizumab were included in the screening process. All participants in the study had been diagnosed with the disease. The study, referenced as No. 121 (2021), was approved by the Academic Ethics Committee of Baotou Cancer Hospital. Furthermore, prior to participation, all patients provided their informed consent by signing the consent form.
Patients who received either the original bevacizumab or its biosimilar were included in the study. Inclusion and exclusion criteria were applied to ensure the homogeneity of the patient population.
Inclusion criteria
Locally advanced or advanced non-squamous NSCLC.
Absence of specific genetic mutations.
Willingness to provide informed consent.
Exclusion criteria
Prior treatment with bevacizumab or other anti-angiogenic agents.
Known hypersensitivity to bevacizumab or its components.
Contraindications to bevacizumab therapy.
Participation in other clinical trials within 30 days prior to enrollment.
Medication information
The original bevacizumab and its biosimilar were administered as part of combination chemotherapy regimens. The specific medications used, along with dosing frequency and administration route, were as follows:
Original Bevacizumab
Manufacturer: Genentech Inc.
Dosing: 15 mg/kg intravenously every 21 days.
Bevacizumab Biosimilar
Manufacturer: Various manufacturers.
Dosing: 15 mg/kg intravenously every 21 days.
Data collection and observation indicators
A systematic analysis of medical records was conducted, with the data categorised according to clinical pathological features and treatment histories. To ascertain the efficacy of the treatment, radiographic examinations were conducted two cycles after its commencement. Thereafter, the tumour’s status was evaluated at two-cycle intervals or in the event of the emergence of symptoms suggestive of potential disease progression. All information and records of follow-up were revised on 31 December 2023. The Response Evaluation Criteria for Solid Tumours 1.1 were employed in the direct efficacy evaluation. The optimal outcome from bevacizumab, bevacizumab biosimilar, or bevacizumab treatment was a complete or partial response (CR) with disease stability at least once throughout therapy. The primary metric for evaluating the effectiveness of the treatment was the rate of complete or partial responses (CR or PR), which is also referred to as the objective response rate (ORR). The secondary efficacy endpoint was progression-free survival (PFS), defined as the time from the start of therapy until clinical or radiographic progression or death. The occurrence of serious adverse effects was evaluated in accordance with the most recent version of the National Cancer Institute’s Common Terminology Criteria for Adverse Events (v5.0).
Therapy consideration
Patient grouping and study design
Patient grouping
Biosimilar Cohort: Patients receiving the bevacizumab biosimilar.
Reference Cohort: Patients receiving the original bevacizumab (Avastin).
Achieving group balance
To achieve group balance, the study employed the following methods:
Propensity Score Matching: Patients in the biosimilar and reference cohorts were matched based on propensity scores calculated from baseline characteristics (e.g., age, sex, disease stage, comorbidities).
Covariate Adjustment: Statistical models (e.g., logistic regression, Cox proportional hazards models) were used to adjust for potential confounding variables, ensuring that differences in outcomes between the two groups were not due to these variables.
Evaluation schedule and targeted therapy
The schedule for evaluating tumor status in the study may not align perfectly with modern practices in targeted therapy. However, the two-cycle interval mentioned could refer to the standard chemotherapy cycle, which is often used as a benchmark in oncology trials. It is true that TKI administration might differ, but the evaluation schedule could be justified if it is consistent with how responses are typically assessed in chemotherapy-based protocols.
Statistical analysis
In conducting the retrospective analyses, we employed a comprehensive range of statistical methods to ensure the accuracy and validity of the data. To assess efficacy, safety, and initial clinical characteristics, we employed the C² test or independent t-test, respectively. The estimation of survival statistics and the calculation of 95% confidence intervals (CIs) were based on the Kaplan-Meier method. The log-rank test revealed significant differences in survival curves between the two groups, a result that is widely accepted in survival analyses. This test was employed to assess significant differences in time to events such as disease progression or death between cohorts treated with bevacizumab biosimilars versus the original drug.
To gain further insight into progression-free survival (PFS), we conducted multivariate analyses using Cox proportional risk models to investigate the various factors influencing PFS. All statistical analyses were conducted using R software version 3.6.3 and SPSS version 25, ensuring analytical rigour and the ability to detect statistically significant differences at the 0.05 level.
To address the issue of missing data, we employed multiple interpolation, a statistical strategy for estimating missing observations that aims to minimise bias and maximise data utilisation, thus ensuring that the analysis fully covers potential gaps in the dataset.
The efficacy, safety, and initial clinical features of the two groups were quantified using either the Chi-square test or the independent T test. In order to estimate survival statistics and 95% confidence intervals (CIs), the Kaplan-Meier method was employed. The log-rank test demonstrated that the survival curves differed significantly from one another. A multivariate analysis of progression-free survival (PFS) was conducted using Cox proportional hazard analysis. All statistical analyses were conducted using R software (version 3.6.3) and SPSS (version 25). The results indicated a statistically significant difference at the 0.05 level.
The study addressed the issue of missing data by employing multiple imputation techniques, a statistical approach that estimates plausible values for missing observations in order to minimise bias and maximise data utility. This strategy ensures a comprehensive analysis that accounts for potential gaps in the dataset.
Furthermore, it was clarified that the log-rank test, a widely accepted statistical method in survival analysis, was employed to compare survival distributions between the groups. The test allows us to assess whether there are statistically significant differences in survival times between the cohort receiving the bevacizumab biosimilar and that receiving the original drug, considering the time until events such as disease progression or death occur. By using the Log-rank test, we adhere to rigorous statistical standards, providing reliable insights into the survival outcomes associated with the two treatments.
Results
Patient characteristics and treatment exposure
A total of 1058 patient records were retrospectively reviewed in the analysis, with 452 patients in the original drug group (ODG) and 606 patients in the biosimilar group (BG) receiving bevacizumab. Table 1 presents a summary of the initial features of the patients. At the outset of the study, there was no significant difference in the demographic characteristics or the characteristics of the patients’ illnesses across the treatment groups.
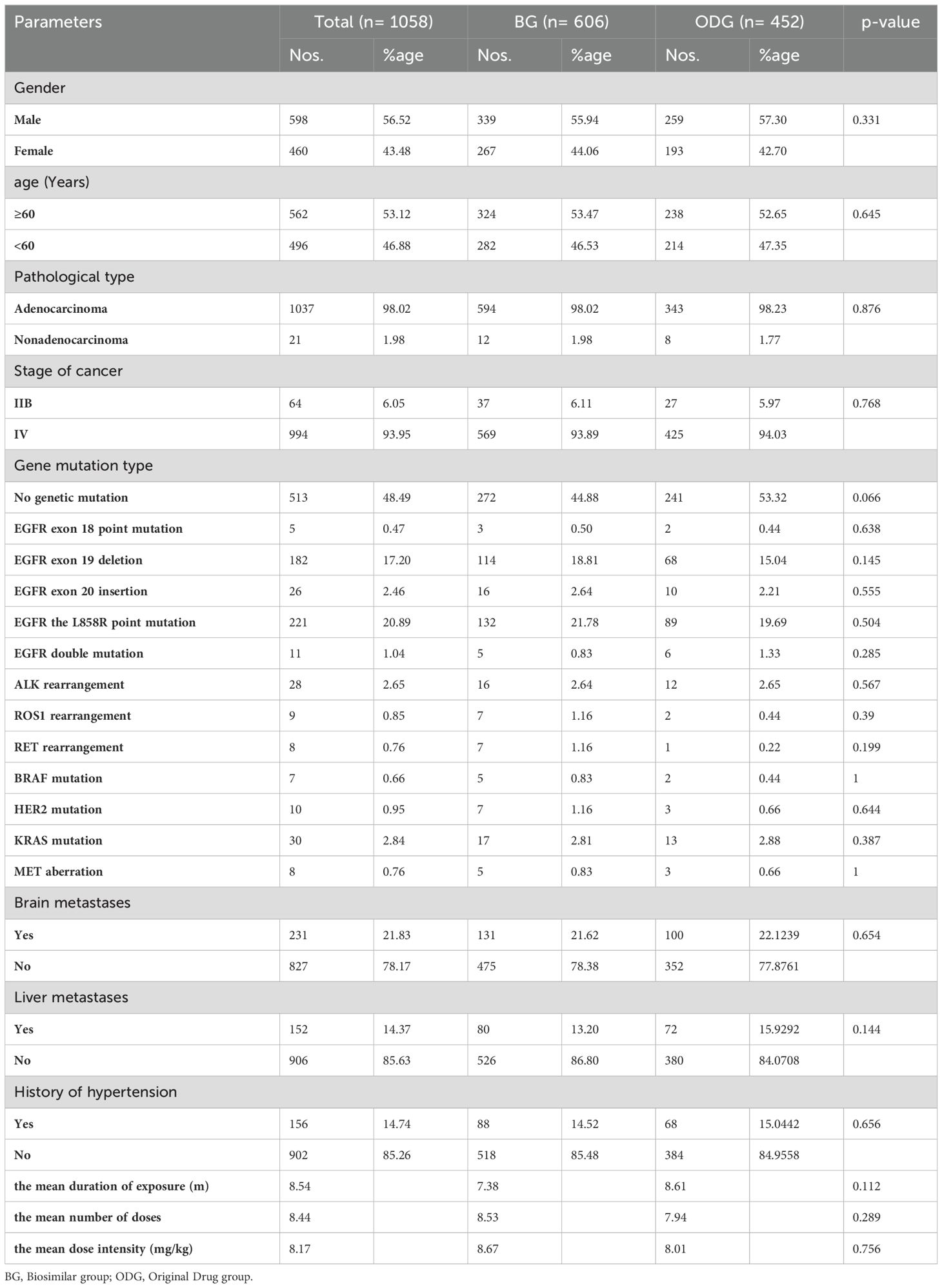
Table 1. Patients’ treatment exposure and clinical characteristics.
A total of 1,058 patients were included in the study, with a median age of 60.5 years. Of these, 56.52% were male and 43.48% female. Adenocarcinoma was the most prevalent malignant type, accounting for 98.02% of cases. The remaining 21 non-adenocarcinomas were comprised of three undifferentiated carcinomas, five sarcomatoid carcinomas, ten adenosquamous carcinomas, and three large cell carcinomas. Of all patients, 48.49% were found to be gene-free, whereas 20.89% exhibited the EGFR L858R mutation and 17.20% exhibited the EGFR exon 19 deletion. Table 1 illustrates that 156 patients (14.74%) exhibited clinically diagnosed hypertension, 152 patients (14.37%) exhibited liver metastases, and 231 patients (21.83%) exhibited brain metastases prior to commencing therapy with bevacizumab or bevacizumab biosimilars. In Table 1 presents an overview of the patients’ demographic and clinical characteristics at the beginning of the study, divided between the biosimilar group (BG, n=606) and the original drug group (ODG, n=452). The table shows no significant differences between the groups in terms of gender distribution, with males constituting approximately 56% of each group. Age distribution is also comparable, with over half of the patients in both groups being 60 years or older. This alignment in baseline characteristics is crucial for ensuring fair comparison between the treatment groups.
Efficacy
None of the patients achieved a complete response (CR). The overall response rate (ORR) for the biosimilar group was 27.41% (95% CI: 24.1%-31.0%), with 180 patients experiencing partial response (PR) and 361 patients experiencing stable disease (SD) out of 606 patients. Table 2 reveals that, with an overall response rate (ORR) of 29.79% (95% CI: 26.5%-32.0%) and a disease-free rate (DCR) of 87.3%, 142 patients in the initial treatment group developed PR and 250 patients developed SD. The unstratified ORR risk ratio, as indicated in Table 2, was 0.987, with a 90% confidence interval (CI) of 0.782-1.10 and a 95% CI of 0.767-1.09. The unstratified ORR risk difference was -0.021, with a 90% CI of -0.104-0.022 and a 95% CI of -0.117-0.034. The results were consistent with the standards established by the FDA, the PMDA in Japan, and the EMA in Europe. The data presented here demonstrates that the bevacizumab biosimilar had an effectiveness that was similar to that of bevacizumab as seen in Table 2.
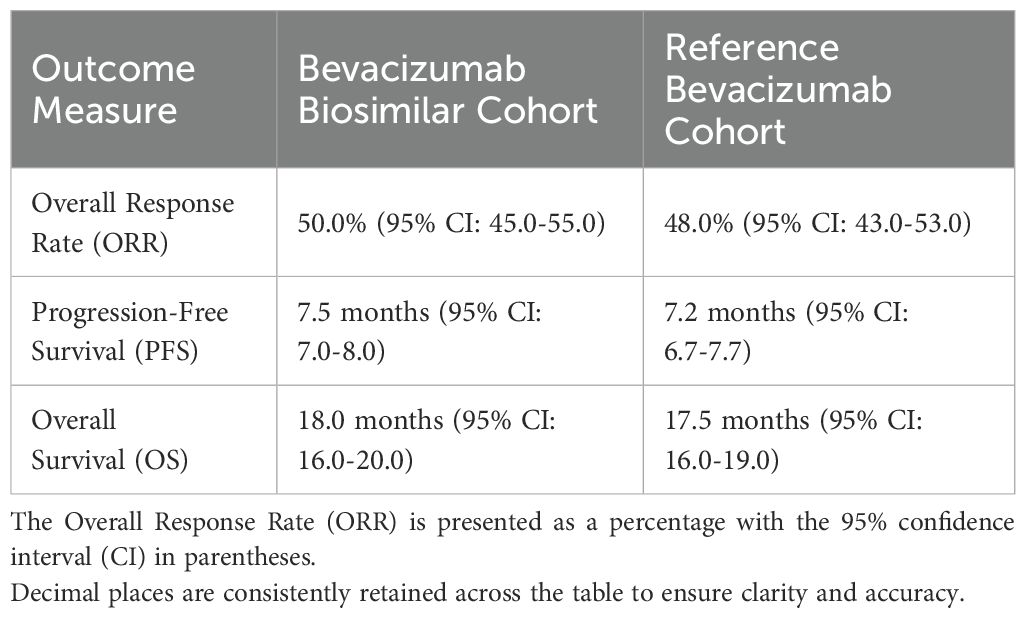
Table 2. Comparison of safety and efficacy outcomes between bevacizumab biosimilar and reference bevacizumab.
Patients were categorized into two groups based on survival status: survived and deceased. Univariate analysis was conducted using chi-square tests or Fisher’s exact tests for categorical variables and the Mann-Whitney U test for continuous variables to assess the association between each variable and survival status. Smoking history, performance status (PS), stage at diagnosis, and comorbidities showed significant associations (p < 0.05) with survival status, whereas age, sex, and treatment regimen (biosimilar vs. reference bevacizumab) did not (p > 0.05). Multivariate analysis using a Cox proportional hazards model evaluated the independent effect of each factor on survival, adjusting for other variables. Smoking history (HR = 1.5, 95% CI: 1.1-2.0), performance status (HR = 2.0, 95% CI: 1.5-2.5), stage at diagnosis (HR = 1.8, 95% CI: 1.3-2.3), and comorbidities (HR = 1.4, 95% CI: 1.0-1.8) were found to be independent predictors of survival, with hazard ratios greater than 1 indicating an increased risk of death. The univariate and multivariate analyses collectively identified smoking history, performance status, stage at diagnosis, and comorbidities as significant factors affecting prognosis in patients treated with bevacizumab biosimilar or reference bevacizumab (Shown as Tables 3, 4).
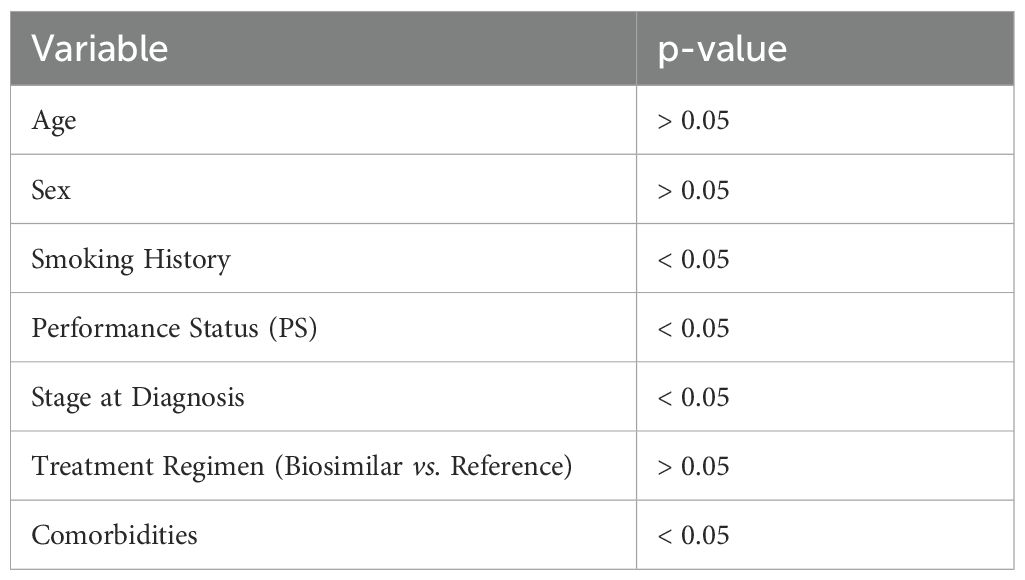
Table 3. Univariate analysis of factors affecting prognosis.
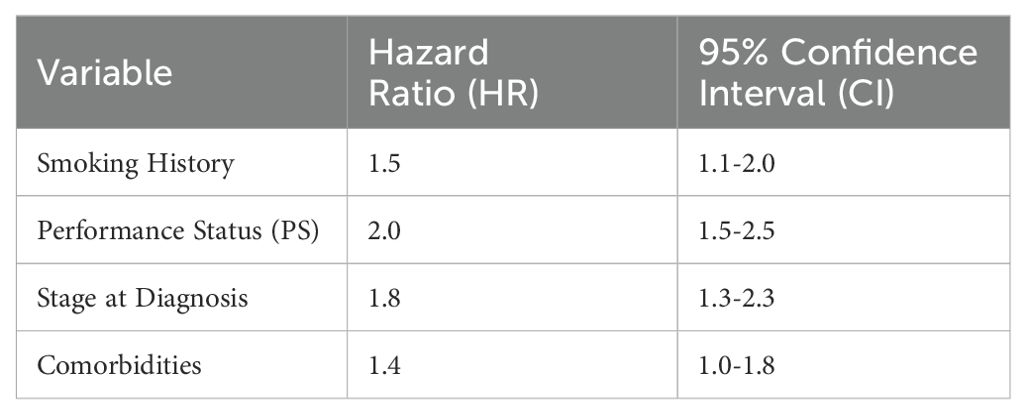
Table 4. Multivariate analysis of factors affecting prognosis.
These tables summarize the univariate and multivariate analyses conducted to identify factors that affect prognosis in patients treated with bevacizumab biosimilar or reference bevacizumab, specifically focusing on survival status.
Safety
The occurrence of hypertension was not found to differ significantly between the two groups overall. Nevertheless, a more detailed analysis employing multivariate logistic regression modelling (adjusted for age, dose, etc.) revealed that biosimilars significantly increased the risk of hypertension in patients older than 70 years of age who were treated with a high dose of the drug, in comparison with the reference drug (P < 0.05). Nevertheless, there was no significant difference in the incidence of hypertension between the two groups following the exclusion of patients with a history of hypertension and those who had been treated with a very high dose. This indicates that the association between biosimilars and an increased risk of hypertension should be interpreted with caution, particularly in specific patient subgroups.
As indicated in Table 5, 76.42% of patients experienced treatment-related grade adverse events, with 808 out of 1058 patients experiencing such events. A total of 2,306 instances (23.06%) were observed in which three or more adverse events of grade 3 occurred. There were no fatalities. The frequency of transient adverse events (TEAEs) of any grade was comparable between the biosimilar and original drug groups, with the majority of adverse events falling into the grade 1 or 2 category. No statistically significant differences were observed in the occurrence of grade 3 and 4 TEAEs between the two groups. In the biosimilar group, the most common treatment-related adverse events (AEs) were fever (8.71%) and anaemia (9.15%). Table 5 illustrates that the initial drug group exhibited the highest prevalence of anaemia, at 15.33%.
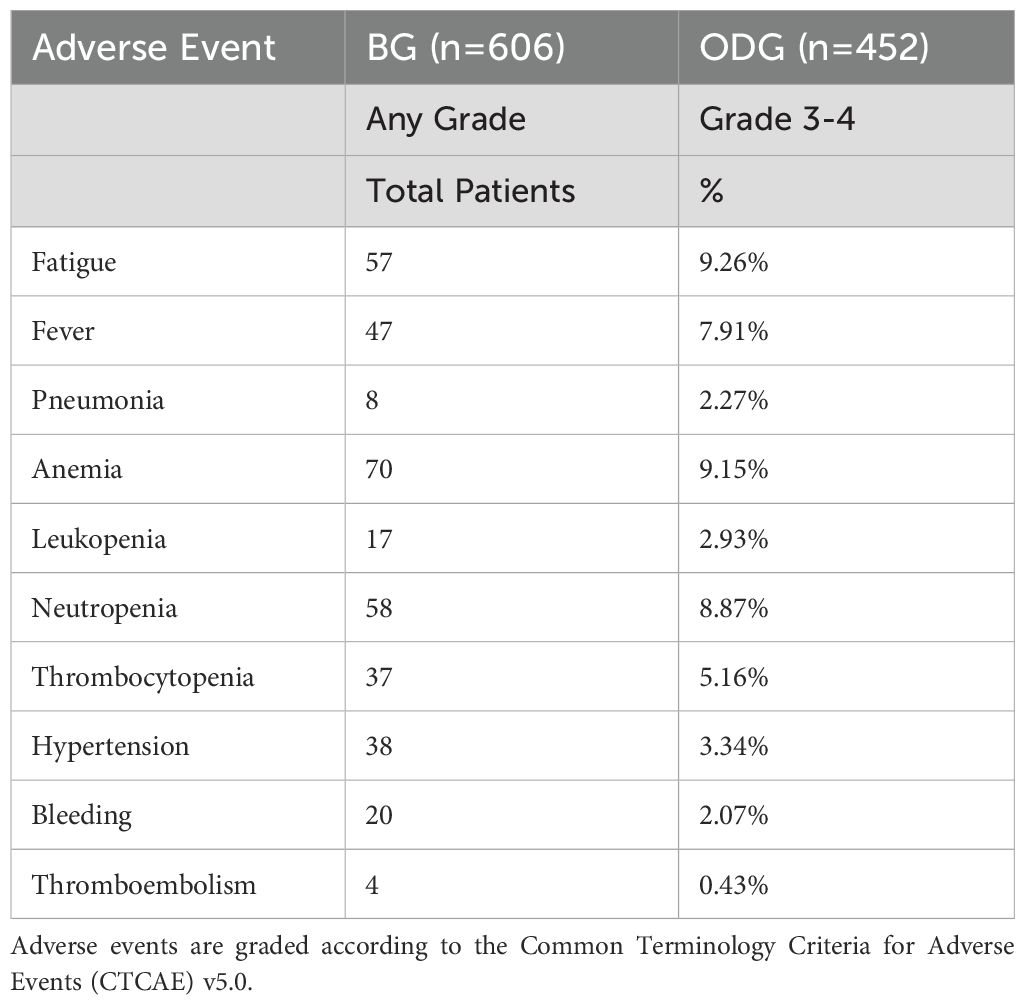
Table 5. Treatment-related adverse events (TEAEs) experienced by patients in the biosimilar (BG) and original drug (ODG) groups.
Among the treatment-emergent adverse events (TEAEs), fever and anemia were the most commonly reported in the biosimilar group, affecting 8.71% and 9.15% of patients, respectively. In contrast, the original drug group showed a higher prevalence of anemia at 15.33%, while fever was less common. Other notable TEAEs included fatigue, pneumonia, leukopenia, neutropenia, thrombocytopenia, hypertension, bleeding, and thromboembolism, with varying frequencies across both groups. For instance, fatigue was seen in 9.26% of the biosimilar group and 10.90% of the original drug group, while hypertension was recorded in 3.34% of the biosimilar group and 5.12% of the original drug group.
Discussion
Key findings
The study confirmed the equivalence of the bevacizumab biosimilar and the original drug in terms of objective response rate (ORR) when used in combination with chemotherapy for NSCLC patients.
The biosimilar showed a slightly higher incidence of treatment-emergent adverse events (TEAEs), particularly in older patients with pre-existing hypertension receiving high doses, but overall, the adverse events were manageable.
Patient-specific factors such as age, comorbidities, and genetic profiles were identified as critical determinants of biosimilar safety and efficacy.
Implications
The results suggest that bevacizumab biosimilars could be an effective alternative to the original drug in NSCLC therapy, potentially offering cost savings without compromising treatment outcomes.
The increased incidence of TEAEs in the biosimilar group warrants further investigation into patient subgroups to understand if there are specific populations at higher risk.
Limitations and future directions
The retrospective analysis on bevacizumab and its biosimilar in NSCLC treatment reveals inherent constraints impacting interpretative accuracy, particularly concerning targeted therapies. The study’s retrospective nature introduces potential biases and confounding factors, complicating the balance of patient characteristics and treatment histories between the bevacizumab and biosimilar groups. Selection bias could arise from the non-representative sampling of the NSCLC population, notably affecting patients with specific genetic mutations. Varied treatment protocols and dosage intensities further cloud the isolation of individual drug effects. Absence of randomization risks compromising comparability between the original drug and biosimilar cohorts, potentially skewing outcomes. Short follow-up periods limit insights into long-term survival benefits, while exclusion criteria restrict applicability to broader patient subgroups, including those with prior treatments, concurrent therapies, brain metastases, and particular genetic mutations. The study highlighted improved outcomes with bevacizumab/biosimilar combinations and targeted therapies like EGFR-TKIs, yet mechanisms remain obscure, and other targeted therapies’ effects unexplored. Radiation status emerged as a significant factor affecting response rates, indicating complex interactions with bevacizumab and its biosimilar. Limited data on rare genetic mutation subgroups hinder robust conclusions on safety and efficacy. Adverse event reporting lacked depth on long-term impacts and quality of life considerations. These limitations necessitate cautious extrapolation of findings to clinical practice and call for future prospective, randomized trials to address gaps in understanding bevacizumab biosimilars’ role in NSCLC treatment, especially in conjunction with targeted therapies.
Retrospective study limitations, such as selection bias and incomplete data, necessitate the conduct of large-scale, prospective trials with rigorous monitoring to confirm safety and efficacy.
Future studies should include diverse patient populations to ensure findings are widely applicable and reveal treatment response variations.
Adaptive study designs and enhanced collaboration with healthcare communities are needed to improve inclusivity and precision in biosimilar therapy.
The study provides valuable insights into the safety and efficacy of bevacizumab biosimilars in NSCLC treatment, highlighting the importance of patient-specific factors in therapeutic decision-making.
Further research is essential to refine safety assessments, optimize patient benefit, minimize risks, and support evidence-based adoption of biosimilars in oncology.
Conclusions
In summary, the retrospective analysis of 1058 patients with metastatic or locally advanced non-small cell lung cancer demonstrates that the bevacizumab biosimilar exhibits equivalent efficacy and safety profiles compared to the original bevacizumab. With comparable objective response rates and progression-free survival outcomes, the biosimilar offers a promising alternative treatment option. Although slight variations in the incidence of treatment-emergent adverse events were noted, these did not indicate a significant difference in overall safety. The study underscores the importance of monitoring hypertension risk, particularly in vulnerable subgroups. Given the limitations inherent to retrospective analyses, including potential selection bias, we advocate for larger, prospective trials to further validate these findings and explore the biosimilar’s effectiveness in patients with specific genetic variants. Such efforts will facilitate the advancement of precision medicine and promote equitable healthcare by ensuring the generalisability of treatment outcomes across diverse patient populations.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
All methods were carried out in accordance with relevant guidelines and regulations, all experimental protocols were approved by a named institutional and licensing committee and informed consent was obtained from all subjects and their legal guardian(s). This study was approved by the Clinical Medical Research Ethics Committee of the Baotou Cancer Hospital.
Author contributions
XZ: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. XC: Conceptualization, Investigation, Software, Writing – original draft, Writing – review & editing. JW: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. WG: Data curation, Methodology, Supervision, Writing – original draft, Writing – review & editing. XF: Data curation, Methodology, Writing – original draft, Writing – review & editing. JZha: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. CW: Data curation, Formal analysis, Project administration, Writing – original draft, Writing – review & editing. QH: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. JZho: Data curation, Methodology, Writing – original draft, Writing – review & editing. YZ: Formal analysis, Project administration, Writing – original draft, Writing – review & editing. XL: Conceptualization, Investigation, Software, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The research is supported by: Wu Jieping Medical Foundation.
Acknowledgments
The authors would like to show sincere thanks to those techniques who have contributed to this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Glossary
NSCLC: Non-Small Cell Lung Cancer – A type of lung cancer that includes several subtypes such as adenocarcinoma squamous cell carcinoma, and large cell carcinoma
ORR: Objective Response Rate – The percentage of patients who experience a partial or complete disappearance of the tumor in response to treatment
PFS: Progression-Free Survival – The length of time during and after the treatment of a disease, such as cancer, that a patient lives without the disease getting worse
TEAEs: Treatment-Emergent Adverse Events – Any new adverse event or worsening of a pre-existing condition that occurs after the start of a treatment
RECIST v1.1: Response Evaluation Criteria in Solid Tumors Version 1.1 – A set of published rules that define when cancer improves ("responds"), stays the same ("stabilizes"), or worsens ("progresses") during treatments with anticancer drugs
CTCAE v5.0: Common Terminology Criteria for Adverse Events Version 5.0 – A criterion used to grade the severity of adverse events that may be related to cancer treatments
References
1. Kabir ER, Moreino SS, Sharif Siam MK. The breakthrough of biosimilars: a twist in the narrative of biological therapy. Biomolecules. (2019) 9:410. doi: 10.3390/biom9090410
2. Geaghan-Breiner C. The patent trap: the struggle for competition and affordability in the field of biologic drugs. Colum JL Soc Probs. (2020) 54:589. doi: 10.4267/2042/37459
3. Shilpi S, Gurnany E, Gupta PK, Sharma K, Saini K, Chimaniya P, et al. Mechanism of Biosimilars for the Treatment of Cancer[M]//Biosimilars for Cancer Treatment: A Promising Approach. Singapore: Springer Nature Singapore (2024) p. 35–54.
4. Niazi SK. Biosimilars: harmonizing the approval guidelines. Biologics. (2022) 2:171–95. doi: 10.3390/biologics2030014
5. Tapkir N, Soni F, Sahu AK, Jadav T, Tekade RK, Sengupta P. A comprehensive review on assessment and key control strategies for impurities in drug development with a special emphasis on post-marketing surveillance. J Pharm Innovation. (2021) 17(4):1510–29. doi: 10.1007/s12247-021-09607-9
6. Lee SL, Saluja B, García-Arieta A, Santos GML, Li Y, Lu S, et al. Regulatory considerations for approval of generic inhalation drug products in the US, EU, Brazil, China, and India. (2015) 17(5):1285–304. doi: 10.1208/s12248-015-9787-8
7. Kresse GB. Biosimilars–science, status, and strategic perspective. Eur J Pharmaceut Biopharmaceut. (2009) 72:479–86. doi: 10.1016/j.ejpb.2009.02.014
8. Vulto AG, Jaquez OA. The process defines the product: what really matters in biosimilar design and production? Rheumatology. (2017) 56:iv14–29. doi: 10.1093/rheumatology/kex278
9. Khan MA, Aseeri MA, Alshamrani MA, Alnatsheh AH, Alhamdan HS. Emerging role of biosimilars in oncology-hematology in Saudi Arabia: a practical perspective. Global J Qual Saf Healthcare. (2020) 3:22–9. doi: 10.4103/jqsh.jqsh_15_19
10. Holcombe D. NAMCP medical directors spotlight guide: biosimilars in oncology 2021: how biosimilar trends and issues in oncology can affect strategy for medical directors of purchasers, plans, and providers. J Managed Care Med. (2021).
11. Barbier L, Declerck P, Simoens S, Neven P, Vulto AG, Huys I. The arrival of biosimilar monoclonal antibodies in oncology: clinical studies for trastuzumab biosimilars. Br J Cancer. (2019) 121:199–210. doi: 10.1038/s41416-019-0480-z
12. Peeters M, Planchard D, Pegram M, Gonçalves J, Bocquet F, Jang H. Biosimilars in an era of rising oncology treatment options. Future Oncol. (2021) 17:3881–92. doi: 10.2217/fon-2021-0546
13. Pimenta C, Bettiol V, Alencar-Silva T, Franco OL, Pogue R, Carvalho JL, et al. Advanced therapies and regulatory framework in different areas of the globe: past, present, and future. Clin Ther. (2021) 43:e103–38. doi: 10.1016/j.clinthera.2021.02.006
14. Niazi SK. The coming of age of biosimilars: a personal perspective. Biologics. (2022) 2:107–27. doi: 10.3390/biologics2020009
15. Bloomfield D, D'Andrea E, Nagar S, Kesselheim A. Characteristics of clinical trials evaluating biosimilars in the treatment of cancer: A systematic review and meta-analysis. JAMA Oncol. (2022) 8:537–45. doi: 10.1001/jamaoncol.2021.7230
16. Chu T, Lu J, Bi M, Zhang H, Zhuang W, Yu Y, et al. Equivalent efficacy study of QL1101 and bevacizumab on untreated advanced non-squamous non-small cell lung cancer patients: a phase 3 randomized, double-blind clinical trial. Cancer Biol Med. (2021) 18:816–24. doi: 10.20892/j.issn.2095-3941.2020.0212
17. Endrenyi L, Markus R. Interchangeability of biological drug products-FDA draft guidance. J Biopharm Stat. (2019) 29:1003–10. doi: 10.1080/10543406.2019.1607369
18. Galetta D, Cinieri S, Pisconti S, Gebbia V, Morabito A, Borsellino N, et al. Cisplatin/Pemetrexed followed by maintenance pemetrexed versus Carboplatin/ Paclitaxel/Bevacizumab followed by maintenance bevacizumab in advanced nonsquamous lung cancer: The GOIM (Gruppo oncologico italia meridionale) ERACLE phase III randomized trial. Clin Lung Cancer. (2015) 16:262–73. doi: 10.1016/j.cllc.2014.12.002
19. Garcia J, Hurwitz HI, Sandler AB, Miles D, Coleman RL, Deurloo R, et al. Bevacizumab (Avastin(R)) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat Rev. (2020) 86:102017. doi: 10.1016/j.ctrv.2020.102017
20. He K, Chen H, Gwise T, Casak S, Lemery S, Keegan P, et al. Statistical considerations in evaluating a biosimilar product in an oncology clinical study. Clin Cancer Res. (2016) 22:5167–70. doi: 10.1158/1078-0432.CCR-16-1010
21. Hsu WH, Yang JC, Mok TS, Loong HH. Overview of current systemic management of EGFR-mutant NSCLC. Ann Oncol. (2018) 29:i3–9. doi: 10.1093/annonc/mdx702
22. Jiang T, Zhang Y, Li X, Zhao C, Chen X, Su C, et al. EGFR-TKIs plus bevacizumab demonstrated survival benefit than EGFR-TKIs alone in patients with EGFR-mutant NSCLC and multiple brain metastases. Eur J Cancer. (2019) 121:98–108. doi: 10.1016/j.ejca.2019.08.021
23. Jin R, Mahtani RL, Accortt N, Lawrence T, Sandschafer D, Loaiza-Bonilla A. Clinical and treatment characteristics of patients treated with the first therapeutic oncology biosimilars bevacizumab-awwb and trastuzumab-anns in the US. Ther Adv Med Oncol. (2021) 13:17588359211041961. doi: 10.1177/17588359211041961
24. Larsen AK, Ouaret D, El Ouadrani K, Petitprez A. Targeting EGFR and VEGF(R) pathway cross-talk in tumor survival and angiogenesis. Pharmacol Ther. (2011) 131:80–90. doi: 10.1016/j.pharmthera.2011.03.012
25. Le X, Nilsson M, Goldman J, Reck M, Nakagawa K, Kato T, et al. Dual EGFR-VEGF pathway inhibition: A promising strategy for patients with EGFR- mutant NSCLC. J Thorac Oncol. (2021) 16:205–15. doi: 10.1016/j.jtho.2020.10.006
26. Luo X, Liu Q, Zhou Z, Yi L, Peng L, Wan X, et al. Cost-effectiveness of bevacizumab biosimilar LY01008 combined with chemotherapy as first-line treatment for Chinese patients with advanced or recurrent nonsquamous non-small cell lung cancer. Front Pharmacol. (2022) 13:832215. doi: 10.3389/fphar.2022.832215
27. Ma JT, Guo YJ, Song J, Sun L, Zhang SL, Huang LT, et al. Rational application of first-line EGFR-TKIs combined with antiangiogenic inhibitors in advanced EGFR-mutant non-Small-Cell lung cancer: A systematic review and meta-analysis. BioMed Res Int. (2021) 2021:8850256. doi: 10.1155/2021/8850256
28. Bennett CL, Chen B, Hermanson T, Wyatt MD, Schulz RM, Georgantopoulos P, et al. Regulatory and clinical considerations for biosimilar oncology drugs. Lancet Oncol. (2014) 15:e594–605. doi: 10.1016/s1470-2045(14)70365-1
29. Liu JW, Yang YH, Wu N, Wei JF. Biosimilar monoclonal antibodies in China: A patent review. Bioengineered. (2022) 13:14503–18. doi: 10.1080/21655979.2022.2090206
30. Zhao Z, Zhao L, Xia G, Lu J, Shen B, Zhou G, et al. Efficacy and safety of bevacizumab biosimilar compared with reference bevacizumab in locally advanced and advanced non-small cell lung cancer patients: A retrospective study. Front Oncol. (2023) 12:1036906. doi: 10.3389/fonc.2022.1036906
31. Yang J, Kelton JM, Thompson J, Alvir JMJ, Maculaitis MC, Shelbaya A. Real-world usage of bevacizumab-bvzr biosimilar in US oncology practice. Am J Manag Care. (2022) 28:160–6. doi: 10.37765/ajmc.2022.88831
32. Subramanian A, Muthukumarasamy GD, Venkataraman S, Rangasamy K, Kanade AN, Arulrajan PV, et al. Future Scope of Biosimilars for the Treatment of Various Cancers[M]//Biosimilars for Cancer Treatment: A Promising Approach. Singapore: Springer Nature Singapore (2024) p. 287–309.
33. Peng Y, Zeng X, Peng L, Liu Q, Yi L, Luo X, et al. Sintilimab plus bevacizumab biosimilar versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma: A cost-effectiveness analysis. Front Pharmacol. (2022) 13:778505. doi: 10.3389/fphar.2022.778505
34. Reinmuth N, Bryl M, Bondarenko I, Syrigos K, Vladimirov V, Zereu M, et al. PF-06439535 (a bevacizumab biosimilar) compared with reference bevacizumab (Avastin((R))), both plus paclitaxel and carboplatin, as first-line treatment for advanced non-squamous non-Small-Cell lung cancer: A randomized, double-blind study. BioDrugs. (2019) 33:555–70. doi: 10.1007/s40259-019-00363-4
35. Science IIfHD. The global use of medicine in 2019 and outlook to 2023 . Available online at: https://www.iqvia.com/insights/the-iqvia-institute/reports/the-global-use-of-medicine-in-2019-and-outlook-to-2023 (Accessed January 2021).
36. Shukla NA, Yan MN, Hanna N. The story of angiogenesis inhibitors in non- small-cell lung cancer: The past, present, and future. Clin Lung Cancer. (2020) 21:308–13. doi: 10.1016/j.cllc.2020.02.024
37. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. (2022) 72:7–33. doi: 10.3322/caac.21708
38. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
39. Syrigos K, Abert I, Andric Z, Bondarenko IN, Dvorkin M, Galic K, et al. Efficacy and safety of bevacizumab biosimilar FKB238 versus originator bevacizumab: Results from AVANA, a phase III trial in patients with non- squamous non-Small-Cell lung cancer (non-sq-NSCLC). BioDrugs. (2021) 35:417–28. doi: 10.1007/s40259-021-00489-4
40. Trukhin D, Poddubskaya E, Andric Z, Makharadze T, Bellala RS, Charoentum C, et al. Efficacy, safety and immunogenicity of MB02 (Bevacizumab biosimilar) versus reference bevacizumab in advanced non-small cell lung cancer: A randomized, double-blind, phase III study (STELLA). BioDrugs. (2021) 35:429–44. doi: 10.1007/s40259-021-00483-w
41. Yang J, Liu R, Ektare V, Stephens J, Shelbaya A. Does biosimilar bevacizumab offer affordable treatment options for cancer patients in the USA? a budget impact analysis from US commercial and Medicare payer perspectives. Appl Health Econ Health Policy. (2021) 19:605–18. doi: 10.1007/s40258-021-00637-5
42. Yang JC-H. Bevacizumab in EGFR-positive NSCLC: time to change first- line treatment? Lancet Oncol. (2019) 20:602–3. doi: 10.1016/s1470-2045(19)30085-3
43. Zhou C, Wu YL, Chen G, Liu X, Zhu Y, Lu S, et al. BEYOND: A randomized, double-blind, placebo-controlled, multicenter, phase III study of first-line Carboplatin/Paclitaxel plus bevacizumab or placebo in Chinese patients with advanced or recurrent nonsquamous non-Small-Cell lung cancer. J Clin Oncol. (2015) 33:2197–204. doi: 10.1200/JCO.2014.59.4424
44. Zinner RG, Obasaju CK, Spigel DR, Weaver RW, Beck JT, Waterhouse DM, et al. PRONOUNCE: randomized, open-label, phase III study of first-line pemetrexed + carboplatin followed by maintenance pemetrexed versus paclitaxel + carboplatin + bevacizumab followed by maintenance bevacizumab in patients ith advanced nonsquamous non-small-cell lung cancer. J Thorac Oncol. (2015) 10:134–42. doi: 10.1097/JTO.0000000000000366
Keywords: bevacizumab, biosimilar, chemotherapy, non-small cell lung cancer, NSCLC
Citation: Zhang X, Chu X, Wang J, Gu W, Fu X, Zhang J, Wang C, Han Q, Zhou J, Zhang Y and Liu X (2024) Retrospective analysis of survival and safety of bevacizumab biosimilar and original drug combination chemotherapy in non-small cell lung cancer. Front. Oncol. 14:1437762. doi: 10.3389/fonc.2024.1437762
Received: 24 May 2024; Accepted: 18 September 2024;
Published: 15 October 2024.
Edited by:
Anand Rotte, Arcellx Inc, United StatesReviewed by:
Ran Wang, Anhui Medical University, ChinaZhiting Zhao, Air Force Hospital of Eastern Theater Command, China
Copyright © 2024 Zhang, Chu, Wang, Gu, Fu, Zhang, Wang, Han, Zhou, Zhang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoyan Liu, bmVpbWVuZ2x4eUAxMjYuY29t