 Shereen Ezzat1*
Shereen Ezzat1* Jesse D. Pasternak2
Jesse D. Pasternak2 Murali Rajaraman3Omar Abdel-Rahman4Andrée Boucher5Nicole G. Chau6Shirley Chen1Sabrina Gill7Martin D. Hyrcza8Nathan Lamond9Marie-Hélène Massicotte10
Murali Rajaraman3Omar Abdel-Rahman4Andrée Boucher5Nicole G. Chau6Shirley Chen1Sabrina Gill7Martin D. Hyrcza8Nathan Lamond9Marie-Hélène Massicotte10 Eric Winquist11
Eric Winquist11 Ozgur Mete12
Ozgur Mete12- 1Endocrine Oncology Site Group, Princess Margaret Cancer Centre, Toronto, ON, Canada
- 2Department of Surgery, University Health Network – Toronto Western Hospital, Toronto, ON, Canada
- 3Department of Radiation Oncology, Dalhousie University, Halifax, NS, Canada
- 4Department of Oncology, University of Alberta, Edmonton, AB, Canada
- 5Endocrinology Division, Centre Hospitalier de l'Université de Montréal, Montréal, QC, Canada
- 6Division of Medical Oncology, British Columbia Cancer – Vancouver, Vancouver, BC, Canada
- 7Division of Endocrinology, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada
- 8Department of Pathology and Laboratory Medicine, Arnie Charbonneau Cancer Institute, University of Calgary, Calgary, AB, Canada
- 9Division of Medical Oncology, Nova Scotia Cancer Centre, Halifax, NS, Canada
- 10Division of Endocrinology, Department of Medicine, Centre Hospitalier Universitaire de Sherbrooke, Université de Sherbrooke, Sherbrooke, QC, Canada
- 11Verspeeten Family Cancer Centre at London Health Sciences Centre, London, ON, Canada
- 12Department of Pathology, Laboratory Medicine Program, University Health Network and University of Toronto, Toronto, ON, Canada
Most follicular cell-derived differentiated thyroid carcinomas are regarded as low-risk neoplasms prompting conservative therapeutic management. Here, we provide consensus recommendations reached by a multidisciplinary group of endocrinologists, medical oncologists, pathologists, radiation oncology specialists, a surgeon and a medication reimbursement specialist, addressing more challenging forms of this malignancy, focused on radioactive iodine (RAI)-resistant or -refractory differentiated thyroid carcinoma (RAIRTC). In this document we highlight clinical, radiographic, and molecular features providing the basis for these management plans. We distinguish differentiated thyroid cancers associated with more aggressive behavior from thyroid cancers manifesting as poorly differentiated and/or anaplastic carcinomas. Treatment algorithms based on risk-benefit assessments of different multimodal therapy approaches are also discussed. Given the scarcity of data supporting management of this rare yet aggressive disease entity, these consensus recommendations provide much needed guidance for multidisciplinary teams to optimally manage RAIRTC.
1 Introduction
Follicular cell-derived differentiated thyroid carcinomas (DTC), which include papillary thyroid carcinoma, follicular thyroid carcinoma, invasive encapsulated follicular variant papillary thyroid carcinoma, and oncocytic carcinoma of the thyroid, arise from genetically modified follicular cells in the thyroid gland. Therapy with 131I, or radioactive iodine (RAI), exploits follicular cells’ iodine uptake machinery to facilitate cytotoxicity. RAI is a mainstay of post-operative DTC treatment; however, there is a subset of patients (<5%) who develop RAI-resistant or -refractory differentiated thyroid carcinoma (RAIRTC) (1). RAIRTC typically develops due to change of functional differentiation status, which is frequently accompanied by loss of the sodium iodide symporter required for iodine uptake (1). There is also a subset of DTCs that exhibit high-grade pathological features (tumor necrosis and/or ≥5 mitoses per 2 mm2) with a clinical course similar to poorly differentiated thyroid carcinoma (PDTC) that can be frequently associated with RAI-refractory disease (2).
RAIRTC has a dismal prognosis among all follicular cell-derived differentiated thyroid cancer types, with a 10-year survival rate of only 10% (3). Considering the suboptimal therapeutic benefit of repeated RAI therapy in patients with RAIRTC, and the availability of effective treatment regimens such as the vascular endothelial growth factor receptor (VEGFR) tyrosine kinase inhibitors (TKi) (lenvatinib and sorafenib), early identification and prediction of RAIRTC is critical (4–6). Selective v-raf murine sarcoma viral oncogene homolog B1 (BRAF), rearranged during transfection (RET), and tropomyosin receptor kinase (TRK) inhibitors are also potentially available. Thus, molecular testing is an integral consideration in the clinical management of patients with RAIRTC (7). Ultimately, treatment decisions for these patients require management by a multidisciplinary team equipped to interpret diagnostic assessments and evaluate patient-specific factors (8).
A Canadian consensus statement on RAIRTC management was published in 2021, which focused on the multidisciplinary management of patients with the disease post-diagnosis (7). This statement, which involved active participation of nuclear medicine specialists, defined RAIRTC by outlining five key clinical scenarios indicative of disease: progression of thyroid cancer metastases despite RAI uptake; no RAI uptake in post-therapy scan despite known structural recurrent/metastatic disease; RAI uptake in some but not all cancer foci; thyroid cancer metastases progression despite cumulative RAI activity of >22.2 GBq (600 mCi); and no RAI uptake on diagnostic radioiodine scan (7).
Here, we aim to update and expand upon the previous statement by providing guidance on early identification of patients at risk of developing RAIRTC and practical referral and implementation strategies. This statement highlights the role of molecular testing for gaining prognostic and therapeutic insights and discusses multimodal options to optimize the management of RAIRTC.
2 Methods
2.1 Survey design and consensus development
A multidisciplinary committee of five Canadian physicians was assembled to lead development of the consensus recommendations: an endocrinologist, a radiation oncologist, an endocrine surgeon, an endocrine pathologist, and a medical oncologist. This committee met in November 2022 to identify the key topics related to identification and management of adult patients with RAIRTC in need of consensus, falling under three categories: diagnosis, therapeutics, and logistics/implementation.
Following the committee meeting, a draft survey was developed and refined through asynchronous review by the committee. The survey was comprised of 31 questions (available in Supplementary Material), the majority of which were in multiple choice format with an optional open-ended response for rationale. All questions were optional to allow respondents of different specialties to only answer applicable questions as necessary. The survey was completed by 24 multidisciplinary participants across Canada, including the original committee, selected based on their expertise in their respective disciplines: seven from Ontario, seven from British Columbia, six from Alberta, two from Québec, and two from Nova Scotia (Figure 1).
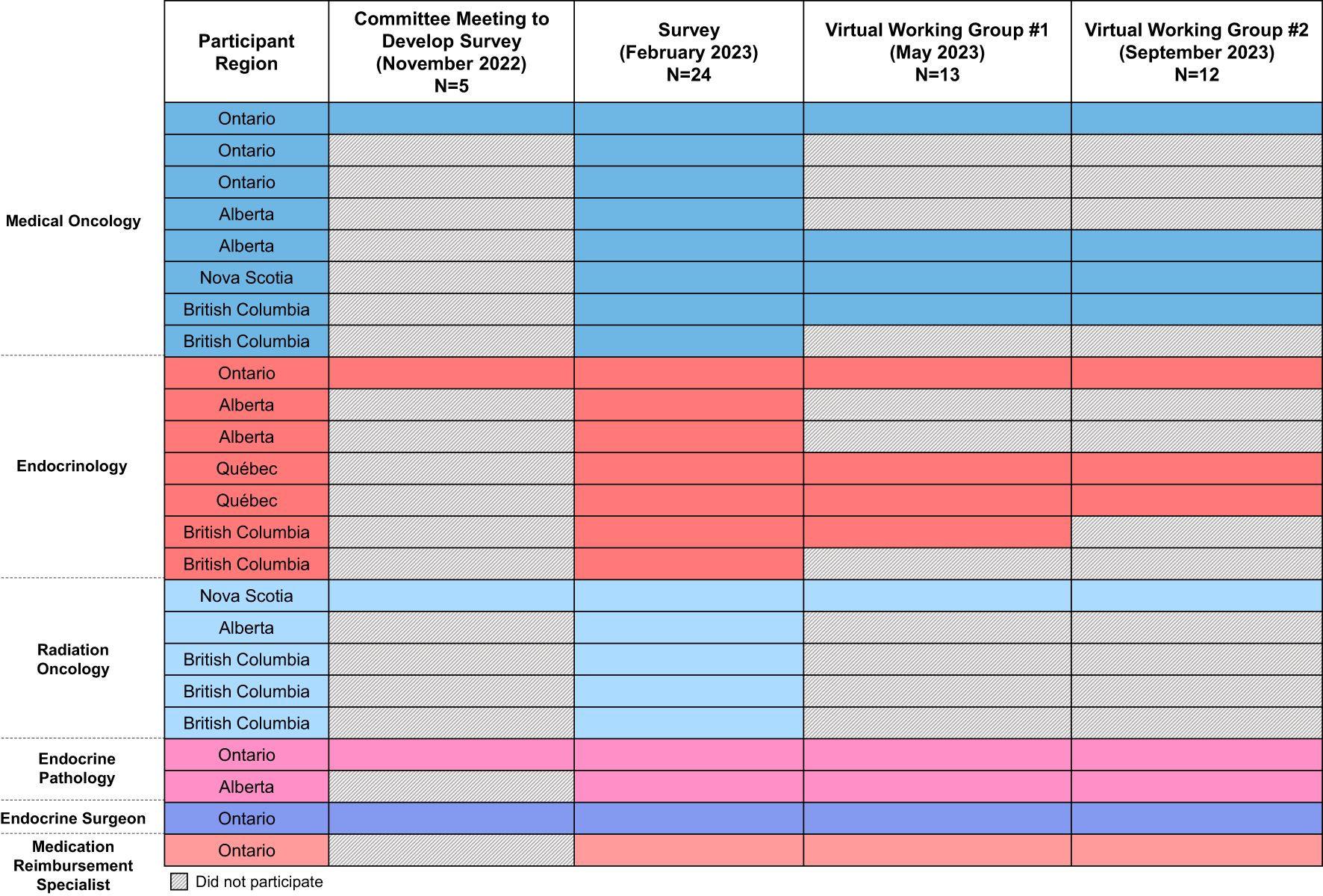
Figure 1. Overview of consensus participants. The specialties, regions, and extent of participation of consensus participants are summarized, with each row representing a different person. Participation in each step is indicated by a colored box, whereas absence/lack of participation is indicated by the hatched fill.
Following survey completion, the results were compiled and grouped by topic. If ≥50% agreement (i.e., agree + strongly agree OR disagree + strongly disagree) was achieved on a survey question, a draft recommendation was developed. The committee and 7-8 survey respondents (Figure 1) then met virtually twice via working group meetings and provided asynchronous feedback on the draft recommendations, refining the recommendations as needed, until consensus was reached (i.e. ≥50% agreement). A consensus was unable to be reached on one draft recommendation, related to poly (ADP-ribose) polymerase inhibitor (PARPi) use, which was ultimately omitted from this document.
2.2 Literature search and evidence grading
A comprehensive literature search was conducted using PubMed (search strategy available in Supplementary Material) to determine the level of evidence supporting the consensus recommendations. The American College of Physicians’ (ACP) Grading System, as used by the 2015 American Thyroid Association Management Guidelines (9), was adopted for use in this consensus statement. We reviewed other appraisal systems but determined their complexity was not necessary given the low level of evidence available in this area. The quality of evidence for all recommendations was low or insufficient, based on the absence of randomized controlled trials/strong observational data inherent to this rare patient subpopulation. For topics where evidence was insufficient, recommendations were based on Expert Opinion and reflect physician experience as well as evidence from the management of other types of thyroid cancer. All recommendations are summarized in Supplementary Table 1, Supplementary Material.
3 Consensus recommendations
Consensus recommendations related to diagnosis, testing, and management flow for patients with DTC are outlined in Figure 2.
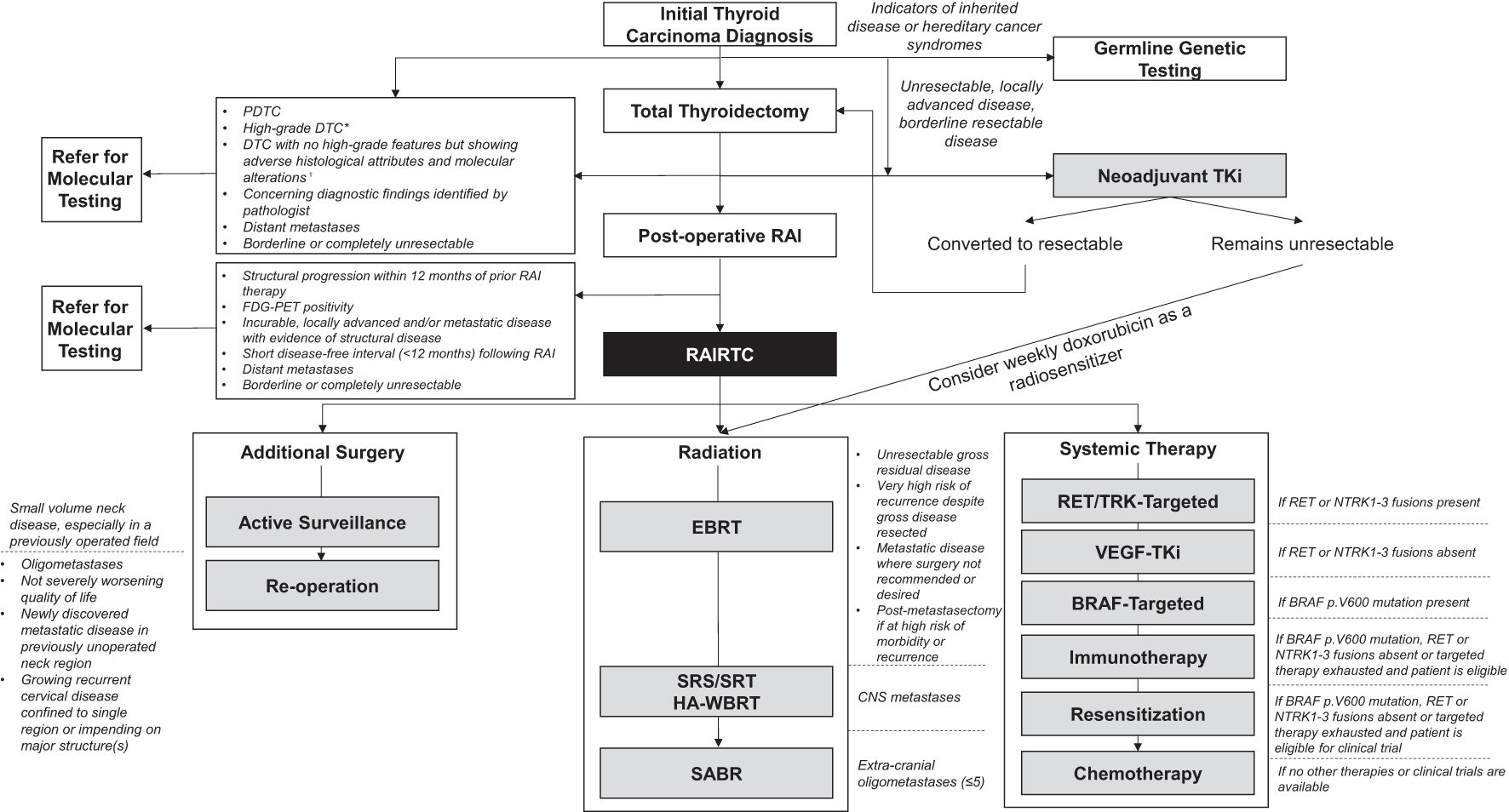
Figure 2. Recommended management options for high-risk and RAI-refractory follicular cell-derived differentiated thyroid cancer. All consensus recommendations are summarized in a management algorithm spanning from initial thyroid carcinoma diagnosis to development of RAIRTC. *Defined by the presence of tumor necrosis and/or mitotic count of at least 5 per 2 mm2 and no histologic or cytologic features of morphologic dedifferentiation (PDTC or ATC); †Such as TERT promoter, TP53 mutations, PLEKHS1 promoter, miR21 overexpression, miR204 downregulation, DNA hypomethylation, chromosome 1q gain, as well as chromosome 5/7 duplication and near haploid genome, particularly in oncocytic carcinomas. ATC, anaplastic thyroid carcinoma; BRAF, v-raf murine sarcoma viral oncogene homolog B1; CNS, central nervous system; DTC, differentiated thyroid carcinoma; EBRT, external beam radiotherapy; FDG-PET, [18F]2-fluoro-2-deoxy-D-glucose-positron emission tomography; HA-WBRT, hippocampal-avoidance whole brain radiation therapy; miR, microribonucleic acid; NTRK, neurotrophic tyrosine receptor kinase; PDTC, poorly differentiated thyroid carcinoma; PLEKHS1, pleckstrin homology domain containing S1; RAI, radioactive iodine; RAIRTC, radioactive iodine-resistant differentiated thyroid carcinoma; RET, rearranged during transfection; SABR, stereotactic ablative radiotherapy; SRS/SRT, stereotactic radiosurgery or stereotactic radiotherapy; TERT, telomerase reverse transcriptase; TKi, tyrosine kinase inhibitor; TP53, tumor protein p53; TRK, tropomyosin receptor kinase; VEGF, vascular endothelial growth factor.
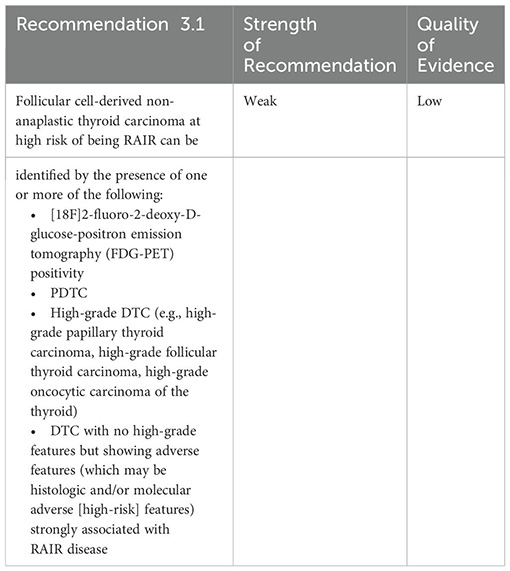
3.1 What features are suggestive of RAIRTC?
3.1.1 Imaging features
While elevated serum thyroglobulin can be a marker for residual, recurrent, or metastatic disease in DTC, approximately one quarter of these patients have negative radioiodine whole-body scans (WBS) (10). Indeed, RAIRTC does not concentrate 131I and is therefore unable to be diagnosed/detected via radioiodine WBS. In contrast, FDG-PET scans, which visualize increased glucose metabolism found in tumors, have emerged as a valuable tool for the diagnosis and staging of RAIRTC. 18F-FDG uptake increases with the level of dedifferentiation and there is an inverse relationship between the ability to concentrate radioiodine and the uptake of 18F-FDG (10).
FDG-PET has shown sensitivity and specificity for the detection of recurrent and metastatic lesions of DTC in patients with signs of biochemical progression but negative iodine WBS (10–13). It is also capable of simultaneously detecting disease in both bone and soft tissues (10). Our group considers FDG-PET a complementary test, used on a case-by-case basis, for RAIRTC diagnosis and staging, with heterogeneity in terms of timing of when it should be used. While especially valuable in cases of discordance between structural imaging and clinical suspicion, access to FDG-PET scanning is variable across Canada, and thus it may not be feasible as part of routine monitoring paradigms. Indeed, discordance between biochemical parameters and structural imaging (e.g. rising thyroglobulin levels in the absence of anatomical disease measured by standard cross-sectional imaging) permits access to FDG-PET scanning in some Canadian provinces and is a valid scenario where this tool could be used (e.g. thyroid-stimulating hormone-stimulated FDG-PET). FDG-PET may also be valuable for staging of suspected RAIRTC resistant to treatment.
3.1.2 Histopathologic features
From a histopathological standpoint, PDTC represents a separate entity on the spectrum between DTC and anaplastic thyroid carcinoma (ATC), which is less likely to respond to RAI therapy (14). PDTC is defined as an invasive follicular cell-derived non-anaplastic thyroid carcinoma with solid/trabecular/insular growth that is unassociated with nuclear alterations of papillary thyroid carcinomas and that shows tumor necrosis and/or mitotic count of at least 3 mitoses per 2 mm2 (15). These tumors have intermediate behavior between DTC and ATC (15).
Similar to PDTCs, high-grade DTCs are also less likely to concentrate RAI (16). High-grade DTCs are defined by the presence of tumor necrosis and/or mitotic count of at least 5 per 2 mm2 and no histologic or cytologic features of morphologic dedifferentiation (PDTC or ATC) (15).
3.1.3 Molecular features
Molecular alterations including telomerase reverse transcriptase (TERT) promoter, tumor protein p53 (TP53) mutations, pleckstrin homology domain containing S1 (PLEKSH1) promoter, microRNA (miR)21 overexpression, miR204 downregulation, DNA hypomethylation, chromosome 1q gain, as well as chromosome 5/7 duplication and near haploid genome, particularly in oncocytic carcinomas, have been recognized to be associated with disease progression (9, 15). Among these, TERT promoter alterations have shown a strong prediction for RAIRTC (17, 18).
Given the potentially poor outcomes associated with RAIRTC, it is of utmost importance to identify potential RAIRTC as early as possible to initiate appropriate referral and management paradigms. We acknowledge that true RAI refractoriness must ultimately be confirmed by attempting RAI therapy (and to qualify for systemic treatment); however, additional metabolic, histopathologic, genotypic, and molecular features can indicate the possibility of RAIRTC, prompting consideration of further investigation.
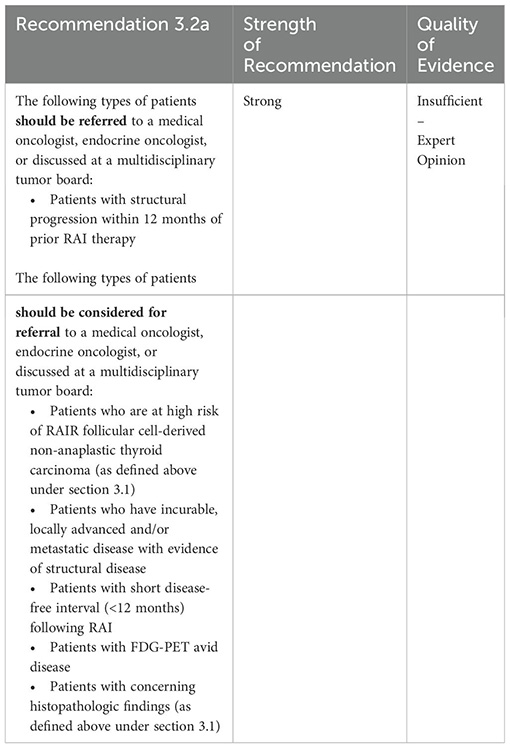
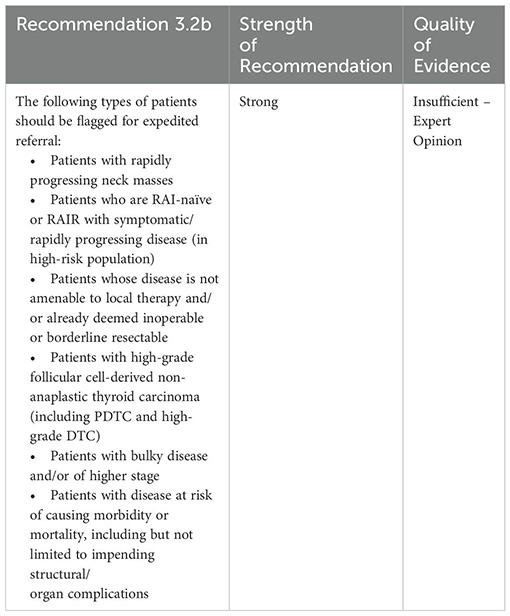
3.2 What types of patients should be referred for consideration of localized and/or systemic therapy?
We recommend a list of patient scenarios that should trigger referral for consideration of localized and/or systemic therapy. While those with structural disease progression despite RAI therapy are of highest priority, we also suggest scenarios that could be considered for referral, at the physician’s discretion. These scenarios, while less confirmatory of RAIRTC, are indicative of advanced disease warranting further investigation (15, 19). Although these recommendations may result in more patients being referred than usual, it will benefit patients to err on the side of caution and refer too soon rather than too late. We also note that patients with a high burden of disease and those at risk of complications should be fast-tracked for an expedited referral where possible.
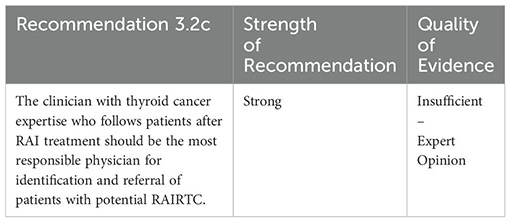
The management of thyroid cancer in Canada, as well as globally, spans many disciplines, including primary care, medical oncology, general endocrinology, radiation oncology, nuclear medicine, head and neck surgery, otolaryngology surgery, and endocrine surgery. The physician responsible for care also varies depending on the stage of the patient journey. However, given the diversity of practitioners involved in care, our group felt it was essential to assign the responsibility of referral, so patients are adequately evaluated and directed appropriately.
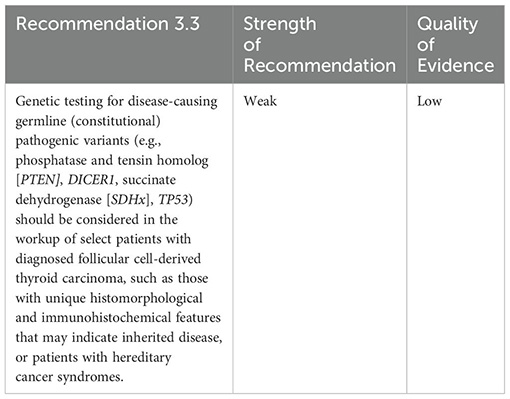
3.3 What is the role of germline (constitutional) genetic testing to predict prognosis?
Most thyroid cancers occur sporadically; however, familial non-medullary thyroid carcinoma occurs in ~3-9% of cases, 5% of which are syndromic (20). These hereditary predisposition syndromes for non-medullary thyroid cancer manifest with other types of lesions/tumors and include familial adenomatosis polyposis (FAP), PTEN-hamartoma tumor, Carney complex, Wermer syndrome (Multiple Endocrine Neoplasia Type 1 [MEN 1]), and DICER1 syndrome (20, 21). Patients with syndromic thyroid cancer usually have known history of inherited predisposition syndrome or a family history of the associated manifestations. However, some syndromes, such as McCune-Albright, are not inherited (20). Histologic findings of the thyroid, such as multiple cellular follicular thyroid neoplasms (PTEN-hamartoma tumor syndromes) or multiple follicular adenomas with papillary architecture in association with multifocal follicular nodular disease and DTC (DICER1 syndrome), should trigger the evaluation for an inherited predisposition syndrome.
A pre-operative diagnosis of most inherited predisposition syndromes does not generally alter the diagnostic approach for a thyroid nodule, with the exception of a known familial RET mutation (MEN2 syndrome), which may impact the extent of thyroidectomy or consideration for prophylactic thyroidectomy as well as guide management of related manifestations and monitoring of at-risk family members (20).
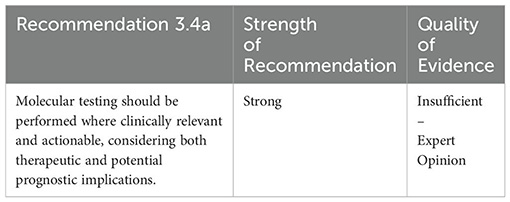
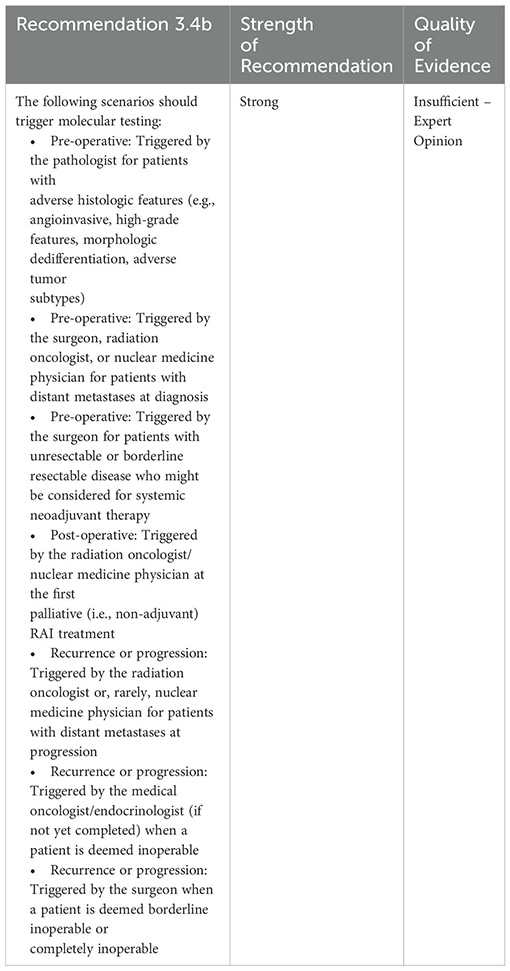
3.4 What is the role of molecular (somatic) tissue testing?
After diagnosis, molecular tissue testing is typically not performed until patients have developed RAI-refractory disease. However, molecular testing can provide invaluable insights on prognosis and can identify patients with driver mutations eligible for efficacious and targeted therapies. Considering certain features previously identified, such as FDG-PET positivity, are indicative of RAIRTC, we recommend earlier use of molecular testing when such features are present in patients with potential RAIRTC to help optimize care.
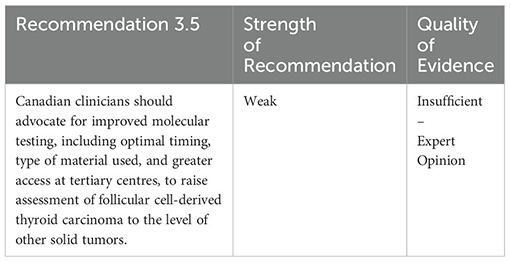
3.5 What advocacy regarding molecular testing is needed?
Molecular testing for biomarkers is broadly implemented in other areas of oncology, such as non-small cell lung cancer (NSCLC), even though the incidence of oncogenic driver alterations is not significantly higher than in DTC; BRAF p.V600 mutations occur in 3%, Kirsten rat sarcoma virus (KRAS) mutations in 20-30%, RET fusions in 1%, neurotrophic tyrosine receptor kinase (NTRK) fusions in <1%, and anaplastic lymphoma kinase (ALK) fusions in 3-5% of NSCLC (22). In comparison, BRAF p.V600E occurs in over 50% of adult papillary thyroid carcinoma (PTC) and NRAS/HRAS/KRAS mutations in 30-45% of follicular thyroid cancer and follicular variant PTC (23, 24). The BRAF p.V600E mutation is mutually exclusive with kinase fusions in the pre-treatment setting; thus in BRAF p.V600E-negative PTC, RET fusions occur in 14%, NTRK fusions in 8%, and ALK fusions in 3% of adult PTCs (25). A case of dual NTRK fusions in PTC has even been reported (26). Current access to molecular testing for thyroid cancer at tertiary centres in Canada is relatively limited in comparison with testing for NSCLC.
Molecular testing approaches for thyroid cancer are variable across Canada and globally, with differing selection of relevant tests and detection platforms. RNA or DNA next-generation sequencing (NGS) panels that detect alterations are preferred in patients with potential RAIRTC due to high sensitivity and maximal output of results for a given sample (i.e., detect multiple mutations/fusions) (19). This can be performed on core biopsy of the primary tumor, incisional/excisional biopsy of primary tumor or metastasis, or fine needle aspiration biopsy (FNAB) (27–30). We recommend patients with high-risk and RAIR follicular cell-derived non-anaplastic thyroid carcinoma have access to timely and high-quality molecular testing.
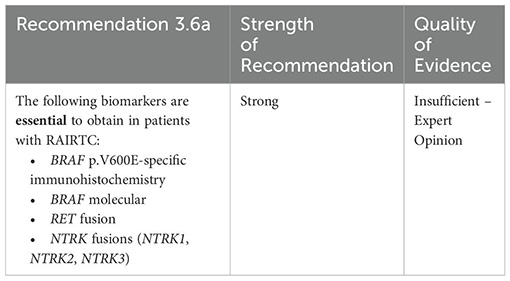
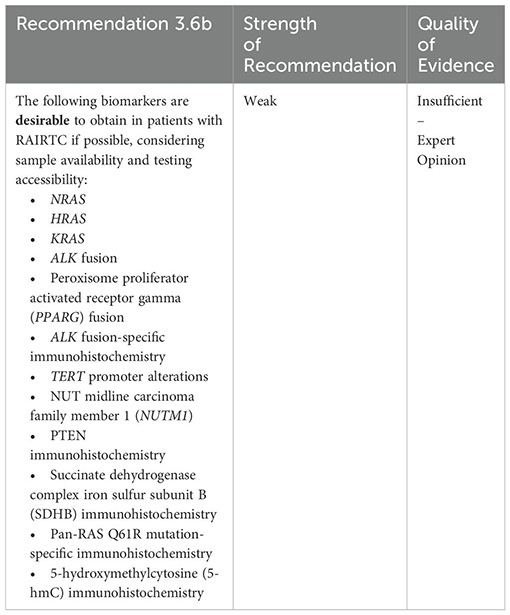
3.6 What biomarkers should be tested?
BRAF mutations, RET fusions, and NTRK1-3 fusions are essential to measure to determine eligibility for targeted therapies. BRAF p.V600E-specific immunohistochemistry has been found to be highly sensitive and specific for mutation detection (31–33), but variability in reproducibility/reliability in clinical practice is known to occur. BRAF p.V600E-specific immunohistochemistry is therefore recommended as a potential screening tool, if rigorously validated using molecularly characterized cases and available with rapid turnaround.
Additional biomarkers with potential prognostic implications are desirable to obtain, if accessible, to aid in clinical decision-making (34–37).
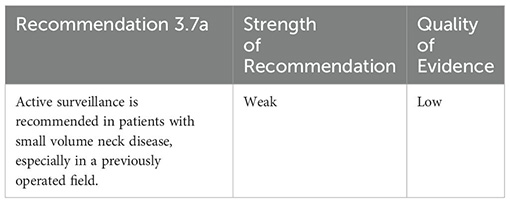
3.7 What is the role of re-operation?
Repeat resections in patients with potential RAIRTC must be approached cautiously, as re-operative thyroid surgery has been shown to have high rates of post-operative morbidity, including both transient (7.1%) and permanent (2.7%) hypoparathyroidism, and iatrogenic unilateral recurrent laryngeal nerve (RLN) palsy (1.6%), specifically in scenarios where the nerve is functioning pre-operatively (38).
Active surveillance may be considered, instead of re-operation, in those with small volume neck disease in a previously operated field. These patients should not have progressively enlarging metastatic lymph nodes or aggressive cytological features (9). Active surveillance requires informed surgical discussion, patient compliance, and an experienced multidisciplinary team with high-quality monitoring tools (20).
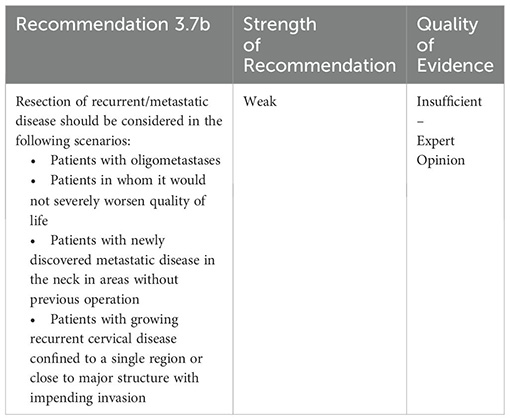
Patients who should be considered for re-operation include those with oligometastatic, rapidly progressive or symptomatic disease, newly discovered metastatic disease in the neck or where recurrent disease is considered to potentially threaten major structures (39). Re-operation may also be considered based on patient/endocrinologist preference, where it would be tolerated by the patient (20). Radiation or local therapies may be an alternative to surgery for inoperable patients (see sections 3.9-3.10).
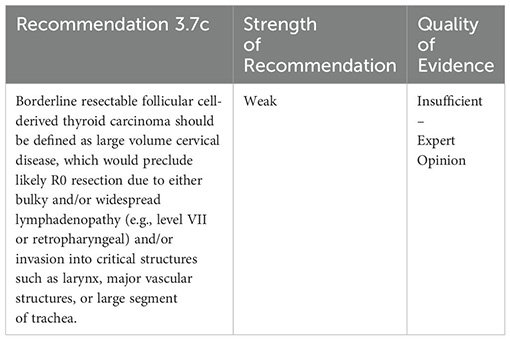
Eligibility for resection should consider the impact on patient quality of life in addition to technical feasibility of the surgery. Indeed, surgical removal of disease invading the trachea, esophagus, or larynx may be particularly detrimental to patients’ quality of life by impacting their airway, speech, and swallowing (40). Patients who are unresectable or borderline resectable are considered for alternative treatments; however, the definition of “borderline resectable” disease is variable across surgeons. We recommend borderline resectable thyroid cancer be defined as: large volume cervical disease, which would preclude likely R0 resection, including invasion into critical structures such as larynx, major vascular structures, or large segment of trachea.
While the notion of borderline resectable thyroid cancer has not been discussed at length in the literature given its rarity in this population, other similar progressive cancers have been studied at length when scenarios such as this are encountered. Certain cancers, such as pancreatic and other solid organ malignancies, are similarly progressive and fatal to advanced stages of undifferentiated, RAIR, and anaplastic cancer, and have been shown to have dismal operative outcomes (41–44). Innovative strategies such as neoadjuvant targeted or chemotherapy can create a hope for positive outcome from subsequent surgical management. Surgical oncological principles such as these should be applied to both classifying borderline resectable thyroid cancer as well as determining treatment strategies to yield better outcomes for these patients.
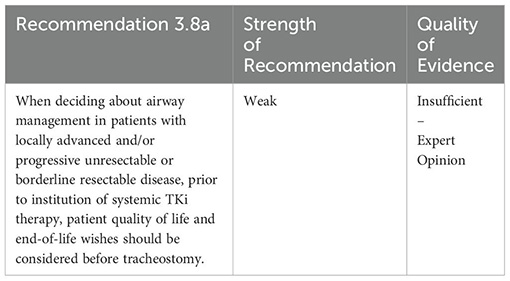
3.8 How should patient airway be managed?
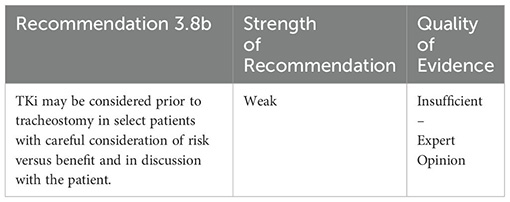
In the absence of data on airway management in DTC, we use evidence in ATC as a guide. Tracheostomy may be offered as a palliative approach to provide symptom relief. Indeed, mortality due to airway compromise occurs in up to 60% of patients (45). However, upper airway obstruction is often present despite tracheostomy, and the intervention is associated with risk of major hemorrhage and decreased quality of life (e.g., tumor can erode the tracheostomy site) (45–47). It is therefore recommended to avoid tracheostomy for as long as possible because of the potential complications and deterioration of quality of life. Alternatively, once a patient develops acute symptoms, such as stridor or unmanageable secretions, a tracheostomy may be considered (45). Indeed, complete resection of disease without the need for tracheostomy has been reported with use of neoadjuvant targeted therapy for ATC (46).
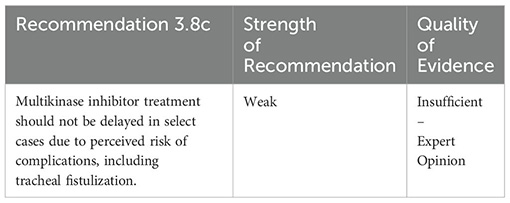
Tracheal fistulization following TKi therapy has been reported in rare instances (48–50). Despite this, even in cases with higher rates of fistulization/perforation, disease control and continued survival were observed (51). Furthermore, while tumor infiltration and histological type may be risk factors for fistulization, decreasing the TKi dose did not impact fistula risk (51). Therefore, given these observations, we recommend not delaying TKi due to the concern of rare risks of tracheal fistulization. Thyroid surgery specialists should review the extent of disease, including transmural invasion into trachea and esophagus simultaneously as highest risk features for trachea-esophageal fistula to occur on use of TKi.
3.9 What is the role of radiotherapy?
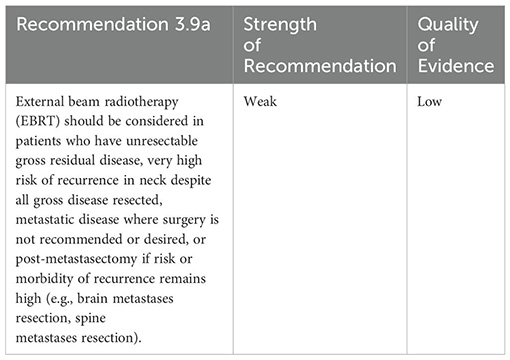
Published studies of EBRT for DTC do not support improved overall survival or rates of distant metastases (52). However, there is evidence that EBRT improves locoregional control with acceptable toxicity, especially with use of modern precision radiation therapy technologies (19, 52–54). Consistent with published guidelines, we recommend EBRT in select cases for locoregional control (7, 9, 55, 56). Weekly doxorubicin may also be considered to help sensitize to radiation (57).
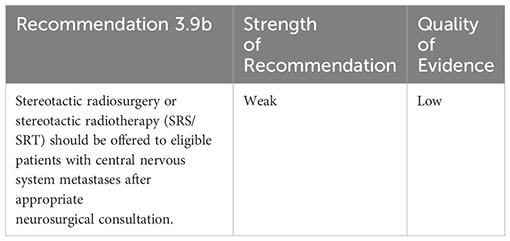
Consistent with published guidelines, we recommend SRS/SRT be offered to eligible patients with limited central nervous system metastases after appropriate neurosurgical consultation (9, 55). The treatment approach (i.e., use of SRS, SRT, and/or hippocampal-avoidance whole brain radiation therapy [HA-WBRT]) should be decided based on the extent and number of central nervous system metastases present.
Consistent with published guidelines, we recommend SABR for treatment of oligometastases (extra-cranial, bony, or soft-tissue) (55). There is no consensus on the precise definition of the oligometastatic state or clarity on how many metastatic lesions are amenable to ablative therapies that may benefit the patient. Although the definition of oligometastatic disease varies from 3-5 metastatic lesions in clinical trials (58) and studies with up to 10 metastases or more are ongoing (59, 60), Phase II studies show favorable progression-free survival and local control were observed after SABR in select patients with up to 5 metastases (61, 62). Despite the development of thyroid cancer hematogenous metastases, disease progression is relatively indolent with a generally longer survival than in those with similar advanced disease due to other primary malignancies. Therefore, aggressive management of patients who progress to M1 thyroid cancer, including those with high-risk or RAIRTC, is indicated, especially in those who are younger or have a good performance status (63).

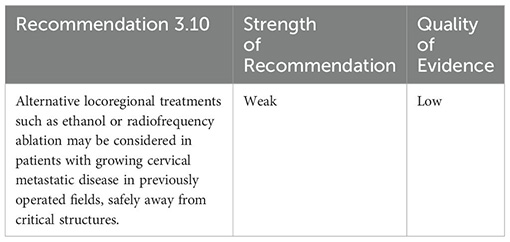
3.10 What is the role of alternative locoregional treatments?
Alternative treatments such as ethanol or radiofrequency ablation may be considered for locoregional control of lymph node metastases, as a directed approach for progressive/symptomatic disease (7, 9, 55). For example, a growing symptomatic lymph node in the lateral neck could be targeted with ablative therapy.
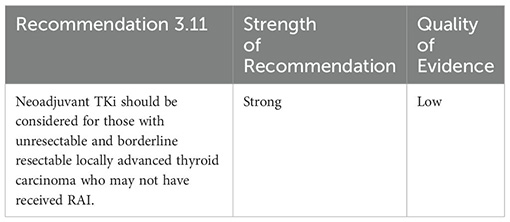
3.11 What is the role of neoadjuvant TKi?
Unresectable DTC occurs in <10% of advanced DTC (64). Patients with unresectable DTC have poor outcomes, with a 5-year cumulative survival rate of 21.5% seen in a retrospective study of 22 patients (64). These patients are also typically unable to qualify for clinical trials as the lack of thyroidectomy means RAI cannot be attempted, and thus RAI refractoriness cannot be proven. In many other disease sites, including rectal cancer and esophagogastric cancer, neoadjuvant therapy prior to surgical resection has been standard of care for decades (65, 66). TKis have recently been reported to have a role in neoadjuvant treatment of unresectable or locally advanced DTC to reduce tumor volume and surgical morbidity (67–73). This has also been observed in ATC and medullary thyroid cancer (46, 74, 75). The 2023 National Comprehensive Cancer Network (NCCN) guidelines also recommend systemic therapy be considered for tumors that are not surgically resectable, or enrollment in neoadjuvant clinical trials, of which there are multiple ongoing (NCT04321954, NCT04180007, NCT04524884) (55).
3.12 What is the role of targeted therapy?
Genotype-directed targeted therapies currently available in Canada include dabrafenib (+/- trametinib)/vemurafenib (BRAF p. V600E mutation; off-label for DTC), selpercatinib (RET fusions), and larotrectinib/entrectinib (NTRK fusions). While VEGFR-targeting multikinase inhibitors lenvatinib, sorafenib, and cabozantinib are currently indicated for systemic treatment of RAIRTC, they can be associated with considerable adverse effects. In the SELECT trial of lenvatinib, ~76% of patients experienced grade 3 or higher treatment-related adverse events, with 14.2% of patients discontinuing the study drug due to adverse events compared to 2.3% with placebo (3). The most common adverse effects associated with lenvatinib were hypertension, diarrhea, and fatigue/asthenia (3). Although the populations are small, due to the rarity of the driver mutations being targeted, and have not been compared head-to-head, genotype-directed targeted therapies show high response rates and comparably lower serious adverse events compared to lenvatinib (Table 1).
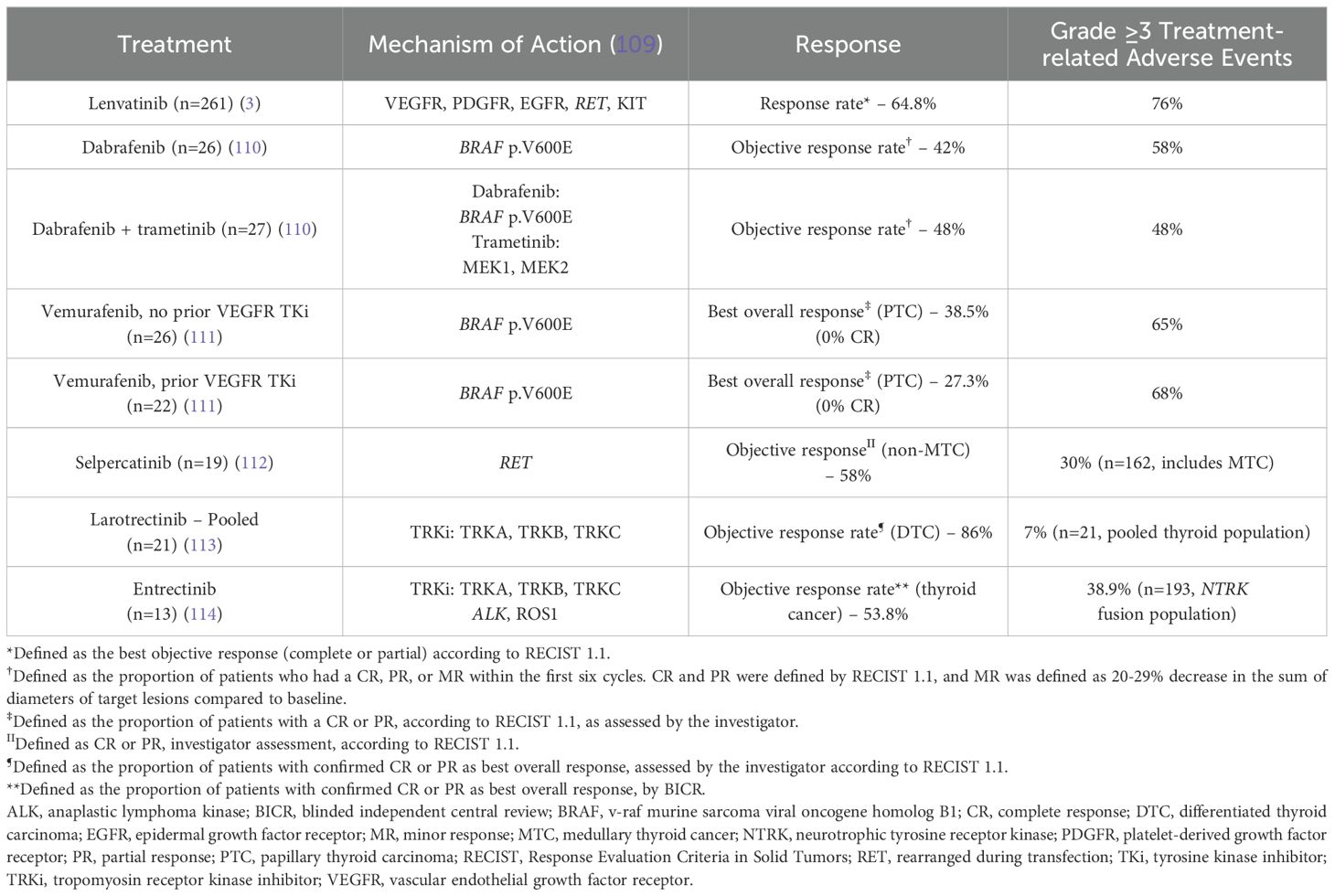
Table 1. Efficacy and safety of targeted precision therapeutics in non-medullary thyroid carcinoma.
In the absence of formal head-to-head comparisons but given the favorable efficacy/safety profile of targeted therapies, we recommend patients with confirmed, clinically actionable genomic alterations be considered for targeted therapy. While the response rates for NTRK and RET fusion-targeting therapies appear to be promising, supporting their use before lenvatinib in eligible patients, we would not recommend routine use of BRAF inhibitors before lenvatinib, given their lower efficacy and weaker evidence.

3.13 What is the role of chemotherapy/immunotherapy?
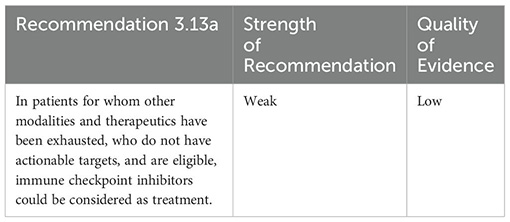
Immune checkpoint inhibitors, including antibodies against cytotoxic T-lymphocyte associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1), have shown promise in cancer types such as melanoma, NSCLC, and head and neck cancers (76–79). Indeed, tumoral programmed cell death-ligand 1 (PD-L1) expression has been observed in thyroid carcinomas (80, 81) and has been associated with increased risk of recurrence and poor prognosis (81, 82). In the Phase 2 KEYNOTE-158 study, pembrolizumab was found to be effective (~7% overall response rate) for a small subset of patients with advanced DTC, regardless of tumor PD-L1 status, with manageable toxicities (83). Responses to other immunotherapies have also been reported in DTC (84, 85).
Despite these preliminary data, the use of immunotherapy/immune checkpoint inhibitors in thyroid cancer is still new. Thus, we recommend immune checkpoint inhibitors if no other treatments are available and patients are eligible (e.g. DNA mismatch repair deficient).
Chemotherapy (i.e., doxorubicin alone and in combination with other cytotoxic therapy, such as cisplatin) for patients with RAIRTC is generally considered ineffective, with response rates of ~20% (56, 86, 87); however, data are limited and large trials in contemporary thyroid cancer populations have not yet been conducted. Case studies have shown unique success of chemotherapy (88–92). Given the limited evidence, generally low response rates, and risk of adverse events, chemotherapy should be considered as a last resort, consistent with treatment guidelines (9, 56).
3.14 What is the role of RAI resensitization?
Efforts have been made to resensitize advanced thyroid tumors to RAI by inducing redifferentiation and/or restoring uptake of iodine. Retinoic acids, histone deacetylase (HDAC) inhibitors, sorafenib, and PPARγ agonist rosiglitazone have been investigated, but with limited success (93–98). Larotrectinib was also observed to re-induce RAI uptake in NTRK rearranged PTC (99). Loss of the sodium iodide symporter, NIS, has been shown to occur when BRAF p.V600E is present (100, 101). Thus, the most promising resensitizing therapies are those that act on BRAF: BRAF inhibitor dabrafenib and downstream MEK inhibitors trametinib and selumetinib. While data have shown increased radioiodine avidity/uptake post treatment with BRAF/MEK inhibitors (102–105), re-induction of RAI uptake is variable, with co-occurrence of TERT mutations with NTRK fusions as a possible contributor (106 107). Additionally, a recent Phase 3 trial showed the addition of selumetinib to adjuvant RAI did not significantly improve 18-month complete remission (CR) rate versus placebo plus RAI in patients with DTC at high risk of primary treatment failure (108). Given the limited evidence and disappointing results of the selumetinib Phase 3 trial, we recommend resensitization only be attempted as part of a clinical trial, with careful monitoring.
4 Conclusion
Thyroid cancer management can be relatively straightforward for the large proportion of patients diagnosed with well differentiated disease. This makes the recognition of the much less frequent but problematic cases more challenging. With this perspective in mind, we provide the evidence underlying clinical, radiographic, histomorphologic, and molecular hallmarks that portend more aggressive disease behavior. Tailoring a management strategy that optimizes risks versus benefits requires a thoughtful multidisciplinary approach. This includes multimodal therapies that consider the immediate and longer-term objectives for each patient. The hope is that such management paradigms will offer strategic pathways that can evolve as advances in their respective disciplines are achieved.
Author contributions
SE: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. JP: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. MR: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. OA-R: Data curation, Writing – review & editing. AB: Data curation, Writing – review & editing. NC: Data curation, Writing – review & editing. SC: Data curation, Writing – review & editing. SG: Data curation, Writing – review & editing. MH: Data curation, Writing – review & editing. NL: Data curation, Writing – review & editing. MH-M: Data curation, Writing – review & editing. EW: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. OM: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Unrestricted funding for the research and development of these guidelines was provided by Bayer Inc. Bayer Inc. reviewed the manuscript for scientific accuracy but had no involvement in its content.
Acknowledgments
Sana Ghaznavi, Jonn Wu, Stuart Kreisman, Stephanie Brulé, Christopher W. Lee, Cynthia Card, Ralf Paschke, Sebastien J. Hotte, Dylan Narinesingh, Wei Ning Jiang, Yizhou Zhao who completed the survey. Andrea Brumwell of MEDUCOM Health Inc. for editorial support.
Conflict of interest
The authors declare the following potential conflicts of interests: SE reports: Advisory board/consulting honoraria from Bayer, Eisai, Eli Lilly, Ipsen, Novartis, Medunik, Merck, Pfizer, and Recordati. OM reports: Advisory board/consulting honoraria from Bayer and Precision Rx-Dx Inc. via Eli Lilly. JP reports: Advisory board/ consulting honoraria from Bayer. MR reports: Advisory board/ consulting honoraria from Bayer, Sanofi Canada, and Sanofi- Aventis Canada. EW reports: Advisory board/consulting honoraria from Bayer, Eisai, EMD Serono, Ipsen, Merck, and Roche; Research support from Merck, Novartis, and Roche/ Genentech. OA-R reports: Advisory board/consulting honoraria from Amgen, Bayer, Eisai, Eli Lilly, Ipsen, and Roche. AB reports: Advisory board/consulting honoraria from Bayer, Eisai, and Precision; Research support from Bayer, Eisai, and Ipsen; Speaker’s bureau from Bayer and Eisai. NC reports: Advisory board/consulting honoraria from Bayer, Eisai, Eli Lilly, Ipsen, Merck, and Roche; Research grant from GlaxoSmithKline; Clinical trial funding to institution from BeiGene, Bristol Myers Squibb, Erasca, Genentech, and Roche. SC reports: Advisory board/consulting honoraria from Bayer, BeiGene, Organon, Pfizer, Sandoz, and TerSera. SG reports: Advisory board/consulting honoraria from Amgen, Boehringer Ingelheim, and Merck. MH reports: Advisory board/consulting honoraria from Bayer, Merck, and Roche; Research support from Bayer. NL reports: Advisory board/consulting honoraria from Amgen, Eisai, Ipsen, Merck, Pfizer, and Taiho. M-HM reports: Advisory board/consulting honoraria from Bayer, Eisai, and Ipsen.
The authors declare that this study received funding from Bayer Inc. The funder had the following involvement in the study: Bayer Inc. reviewed the final manuscript for scientific accuracy.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1437360/full#supplementary-material
References
1. Gild ML, Topliss DJ, Learoyd D, Parnis F, Tie J, Hughes B, et al. Clinical guidance for radioiodine refractory differentiated thyroid cancer. Clin Endocrinol (Oxf). (2018) 88:529–37. doi: 10.1111/cen.2018.88.issue-4
2. Christofer Juhlin C, Mete O, Baloch ZW. The 2022 WHO classification of thyroid tumors: novel concepts in nomenclature and grading. Endocr Relat Cancer. (2023) 30:e220293. doi: 10.1530/ERC-22-0293
3. Schlumberger M, Tahara M, Wirth LJ, Robinson B, Brose MS, Elisei R, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. (2015) 372:621–30. doi: 10.1056/NEJMoa1406470
4. Meng C, Song J, Long W, Mu Z, Sun Y, Liang J, et al. A user-friendly nomogram for predicting radioiodine refractory differentiated thyroid cancer. Front Endocrinol (Lausanne). (2023) 14:1109439. doi: 10.3389/fendo.2023.1109439
5. Kang SY, Bang JI, Kang KW, Lee HY, Chung JK. FDG PET/CT for the early prediction of RAI therapy response in patients with metastatic differentiated thyroid carcinoma. PloS One. (2019) 14:e0218416. doi: 10.1371/journal.pone.0218416
6. Mu ZZ, Zhang X, Lin YS. Identification of radioactive iodine refractory differentiated thyroid cancer. Chonnam Med J. (2019) 55:127–35. doi: 10.4068/cmj.2019.55.3.127
7. Boucher A, Ezzat S, Hotte S, Rachinsky I, Rajaraman M, Ruether D, et al. Canadian consensus statement on the management of radioactive iodine-resistant differentiated thyroid cancer. Oral Oncol. (2021) 121:105477. doi: 10.1016/j.oraloncology.2021.105477
8. Fugazzola L, Elisei R, Fuhrer D, Jarzab B, Leboulleux S, Newbold K, et al. 2019 European thyroid association guidelines for the treatment and follow-Up of advanced radioiodine-Refractory thyroid cancer. Eur Thyroid J. (2019) 8:227–45. doi: 10.1159/000502229
9. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. (2016) 26:1–133. doi: 10.1089/thy.2015.0020
10. Boktor RR, Lee ST, Berlangieri SU, Scott AM. Impact of 18F-FDG PET/CT on treatment of patients with differentiated thyroid carcinoma, negative 131I whole body scan and elevated serum thyroglobulin. Asia Ocean J Nucl Med Biol. (2022) 10:20–7. doi: 10.22038/AOJNMB.2021.58276.1406
11. Caetano R, Bastos CR, de Oliveira IA, da Silva RM, Fortes CP, Pepe VL, et al. Accuracy of positron emission tomography and positron emission tomography-CT in the detection of differentiated thyroid cancer recurrence with negative (131) I whole-body scan results: A meta-analysis. Head Neck. (2016) 38:316–27. doi: 10.1002/hed.23881
12. Asa S, Aksoy SY, Vatankulu B, Aliyev A, Uslu L, Ozhan M, et al. The role of FDG-PET/CT in differentiated thyroid cancer patients with negative iodine-131 whole-body scan and elevated anti-Tg level. Ann Nucl Med. (2014) 28:970–9. doi: 10.1007/s12149-014-0897-7
13. Dong MJ, Liu ZF, Zhao K, Ruan LX, Wang GL, Yang SY, et al. Value of 18F-FDG-PET/PET-CT in differentiated thyroid carcinoma with radioiodine-negative whole-body scan: a meta-analysis. Nucl Med Commun. (2009) 30:639–50. doi: 10.1097/MNM.0b013e32832dcfa7
14. Tong J, Ruan M, Jin Y, Fu H, Cheng L, Luo Q, et al. Poorly differentiated thyroid carcinoma: a clinician's perspective. Eur Thyroid J. (2022) 11:e220021. doi: 10.1530/ETJ-22-0021
15. Baloch ZW, Asa SL, Barletta JA, Ghossein RA, Juhlin CC, Jung CK, et al. Overview of the 2022 WHO classification of thyroid neoplasms. Endocr Pathol. (2022) 33:27–63. doi: 10.1007/s12022-022-09707-3
16. Xu B, David J, Dogan S, Landa I, Katabi N, Saliba M, et al. Primary high-grade non-anaplastic thyroid carcinoma: a retrospective study of 364 cases. Histopathology. (2022) 80:322–37. doi: 10.1111/his.14550
17. Póvoa AA, Teixeira E, Bella-Cueto MR, Batista R, Pestana A, Melo M, et al. Genetic determinants for prediction of outcome of patients with papillary thyroid carcinoma. Cancers (Basel). (2021) 13:2048. doi: 10.3390/cancers13092048
18. Yang J, Gong Y, Yan S, Chen H, Qin S, Gong R. Association between TERT promoter mutations and clinical behaviors in differentiated thyroid carcinoma: a systematic review and meta-analysis. Endocrine. (2020) 67:44–57. doi: 10.1007/s12020-019-02117-2
19. Shonka DC, Ho A, Chintakuntlawar AV, Geiger JL, Park JC, Seetharamu N, et al. American Head and Neck Society Endocrine Surgery Section and International Thyroid Oncology Group consensus statement on mutational testing in thyroid cancer: Defining advanced thyroid cancer and its targeted treatment. Head Neck. (2022) 44:1277–300. doi: 10.1002/hed.27025
20. Patel KN, Yip L, Lubitz CC, Grubbs EG, Miller BS, Shen W, et al. The American association of endocrine surgeons guidelines for the definitive surgical management of thyroid disease in adults. Ann Surg. (2020) 271:e21–93. doi: 10.1097/SLA.0000000000003580
21. Thakker RV. Multiple endocrine neoplasia type 1 (MEN1) and type 4 (MEN4). Mol Cell Endocrinol. (2014) 386:2–15. doi: 10.1016/j.mce.2013.08.002
22. Melosky B, Blais N, Cheema P, Couture C, Juergens R, Kamel-Reid S, et al. Standardizing biomarker testing for Canadian patients with advanced lung cancer. Curr Oncol. (2018) 25:73–82. doi: 10.3747/co.25.3867
23. Xing M. Clinical utility of RAS mutations in thyroid cancer: a blurred picture now emerging clearer. BMC Med. (2016) 14:12. doi: 10.1186/s12916-016-0559-9
24. Johnson DN, Sadow PM. Exploration of BRAFV600E as a diagnostic adjuvant in the non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP). Hum Pathol. (2018) 82:32–8. doi: 10.1016/j.humpath.2018.06.033
25. Chu YH, Sadow PM. Kinase fusion-related thyroid carcinomas: towards predictive models for advanced actionable diagnostics. Endocr Pathol. (2022) 33:421–35. doi: 10.1007/s12022-022-09739-9
26. Yu QX, Zhao WJ, Wang HY, Zhang L, Qin L, Han JL. Case report: identification of a novel. Front Oncol. (2023) 13:1123812. doi: 10.3389/fonc.2023.1123812
27. Turner SA, Abou Shaar R, Yang Z. The basics of commonly used molecular techniques for diagnosis, and application of molecular testing in cytology. Diagn Cytopathol. (2023) 51:83–94. doi: 10.1002/dc.25067
28. Juhlin CC, Baloch ZW. The 3rd edition of Bethesda system for reporting thyroid cytopathology: highlights and comments. Endocr Pathol. (2023) 35:77–9. doi: 10.1007/s12022-023-09795-9
29. Artifon ELA, Guedes HG, Cheng S. Maximizing the diagnostic yield of endoscopic ultrasound-guided fine-needle aspiration biopsy. Gastroenterology. (2017) 153:881–5. doi: 10.1053/j.gastro.2017.08.058
30. Yi QQ, Yang R, Shi JF, Zeng NY, Liang DY, Sha S, et al. Effect of preservation time of formalin-fixed paraffin-embedded tissues on extractable DNA and RNA quantity. J Int Med Res. (2020) 48:300060520931259. doi: 10.1177/0300060520931259
31. Parker KG, White MG, Cipriani NA. Comparison of molecular methods and BRAF immunohistochemistry (VE1 clone) for the detection of BRAF V600E mutation in papillary thyroid carcinoma: A meta-analysis. Head Neck Pathol. (2020) 14:1067–79. doi: 10.1007/s12105-020-01166-8
32. Pyo JS, Sohn JH, Kang G. BRAF immunohistochemistry using clone VE1 is strongly concordant with BRAF(V600E) mutation test in papillary thyroid carcinoma. Endocr Pathol. (2015) 26:211–7. doi: 10.1007/s12022-015-9374-7
33. Singarayer R, Mete O, Perrier L, Thabane L, Asa SL, Van Uum S, et al. A systematic review and meta-analysis of the diagnostic performance of BRAF V600E immunohistochemistry in thyroid histopathology. Endocr Pathol. (2019) 30:201–18. doi: 10.1007/s12022-019-09585-2
34. Nannini M, Repaci A, Nigro MC, Colapinto A, Vicennati V, Maloberti T, et al. Clinical relevance of gene mutations and rearrangements in advanced differentiated thyroid cancer. ESMO Open. (2023) 8:102039. doi: 10.1016/j.esmoop.2023.102039
35. Barletta JA, Gilday SD, Afkhami M, Bell D, Bocklage T, Boisselier P, et al. NUTM1 -rearranged carcinoma of the thyroid : A distinct subset of NUT carcinoma characterized by frequent NSD3 - NUTM1 fusions. Am J Surg Pathol. (2022) 46:1706–15. doi: 10.1097/PAS.0000000000001967
36. Saliba M, Katabi N, Dogan S, Xu B, Ghossein RA. NRAS Q61R immunohistochemical staining in thyroid pathology: sensitivity, specificity and utility. Histopathology. (2021) 79:650–60. doi: 10.1111/his.14396
37. Oishi N, Vuong HG, Mochizuki K, Kondo T. Loss of 5-hydroxymethylcytosine is an epigenetic hallmark of thyroid carcinomas with TERT promoter mutations. Endocr Pathol. (2020) 31:359–66. doi: 10.1007/s12022-020-09652-z
38. Deo S, Bansal B, Bhoriwal S, Bal CS, Mishra A, Sharma J, et al. Re-operative surgery for differentiated thyroid cancer: A single institutional experience of 182 cases. Eur J Surg Oncol. (2023) 49:107042. doi: 10.1016/j.ejso.2023.107042
39. Matrone A, Campopiano MC, Nervo A, Sapuppo G, Tavarelli M, De Leo S. Differentiated thyroid cancer, from active surveillance to advanced therapy: toward a personalized medicine. Front Endocrinol (Lausanne). (2019) 10:884. doi: 10.3389/fendo.2019.00884
40. Russell MD, Kamani D, Randolph GW. Modern surgery for advanced thyroid cancer: a tailored approach. Gland Surg. (2020) 9:S105–S19. doi: 10.21037/gs.2019.12.16
41. Soloff EV, Zaheer A, Meier J, Zins M, Tamm EP. Staging of pancreatic cancer: resectable, borderline resectable, and unresectable disease. Abdom Radiol (NY). (2018) 43:301–13. doi: 10.1007/s00261-017-1410-2
42. Shaib WL, Ip A, Cardona K, Alese OB, Maithel SK, Kooby D, et al. Contemporary management of borderline resectable and locally advanced unresectable pancreatic cancer. Oncologist. (2016) 21:178–87. doi: 10.1634/theoncologist.2015-0316
43. Tamburrino D, De Stefano F, Belfiori G, Partelli S, Crippa S, Falconi M. Surgical planning for "Borderline resectable" and "Locally advanced" Pancreatic cancer during open pancreatic resection. J Gastrointest Surg. (2023) 27:3014–23. doi: 10.1007/s11605-023-05848-w
44. Czarnecka AM, Ostaszewski K, Borkowska A, Szumera-Ciećkiewicz A, Kozak K, Świtaj T, et al. Efficacy of neoadjuvant targeted therapy for borderline resectable III B-D or IV stage BRAF. Cancers (Basel). (2021) 14:110. doi: 10.3390/cancers14010110
45. Moyer KF, Marcadis AR, Shaha AR. Airway management, symptom relief and best supportive care in anaplastic thyroid cancer. Curr Opin Otolaryngol Head Neck Surg. (2020) 28:74–8. doi: 10.1097/MOO.0000000000000619
46. Wang JR, Zafereo ME, Dadu R, Ferrarotto R, Busaidy NL, Lu C, et al. Complete surgical resection following neoadjuvant dabrafenib plus trametinib in BRAF(V600E)-mutated anaplastic thyroid carcinoma. Thyroid. (2019) 29:1036–43. doi: 10.1089/thy.2019.0133
47. Mani N, McNamara K, Lowe N, Loughran S, Yap BK. Management of the compromised airway and role of tracheotomy in anaplastic thyroid carcinoma. Head Neck. (2016) 38:85–8. doi: 10.1002/hed.23857
48. Blevins DP, Dadu R, Hu M, Baik C, Balachandran D, Ross W, et al. Aerodigestive fistula formation as a rare side effect of antiangiogenic tyrosine kinase inhibitor therapy for thyroid cancer. Thyroid. (2014) 24:918–22. doi: 10.1089/thy.2012.0598
49. Song E, Song KM, Kim WG, Choi CM. Development of tracheoesophageal fistula afterthe use of sorafenib in locally advanced papillary thyroid carcinoma: a case report. Int J Thyroid. (2016) 9:210–4. doi: 10.11106/ijt.2016.9.2.210
50. Perdoni C, Olcott C, Lieb DC, Karakla DW. Development of upper aerodigestive tract complications in patients with stage IV thyroid cancer receiving tyrosine kinase inhibitors. AACE Clin Case Rep. (2018) 4:e270–e4. doi: 10.4158/ACCR-2017-0082
51. Valerio L, Giani C, Agate L, Molinaro E, Viola D, Bottici V, et al. Prevalence and risk factors of developing fistula or organ perforation in patients treated with lenvatinib for radioiodine-refractory thyroid cancer. Eur Thyroid J. (2021) 10:399–407. doi: 10.1159/000514182
52. Jacomina LE, Jacinto JKM, Co LBA, Yu KKL, Agas RAF, Co JL, et al. The Role of postoperative external beam radiotherapy for differentiated thyroid carcinoma: A Systematic review and meta-analysis. Head Neck. (2020) 42:2181–93. doi: 10.1002/hed.26133
53. Fussey JM, Crunkhorn R, Tedla M, Weickert MO, Mehanna H. External beam radiotherapy in differentiated thyroid carcinoma: A systematic review. Head Neck. (2016) 38 Suppl 1:E2297–305. doi: 10.1002/hed.v38.S1
54. Kiess AP, Agrawal N, Brierley JD, Duvvuri U, Ferris RL, Genden E, et al. External-beam radiotherapy for differentiated thyroid cancer locoregional control: A statement of the American Head and Neck Society. Head Neck. (2016) 38:493–8. doi: 10.1002/hed.24357
55. Haddad RI, Bischoff L, Ball D, Bernet V, Blomain E, Busaidy NL, et al. NCCN clinical practice guidelines in oncology - thyroid carcinoma. J Natl Compr Canc Netw. (2022) 20:925–51. doi: 10.6004/jnccn.2022.0040
56. Filetti S, Durante C, Hartl D, Leboulleux S, Locati LD, Newbold K, et al. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-updagger. Ann Oncol. (2019) 30:1856–83. doi: 10.1093/annonc/mdz400
57. Beckham TH, Romesser PB, Groen AH, Sabol C, Shaha AR, Sabra M, et al. Intensity-modulated radiation therapy with or without concurrent chemotherapy in nonanaplastic thyroid cancer with unresectable or gross residual disease. Thyroid. (2018) 28:1180–9. doi: 10.1089/thy.2018.0214
58. Tan VS, Palma DA. Top ten lessons learned from trials in oligometastatic cancers. Cancer Res Treat. (2023) 55:5–14. doi: 10.4143/crt.2022.1460
59. Bauman GS, Corkum MT, Fakir H, Nguyen TK, Palma DA. Ablative radiation therapy to restrain everything safely treatable (ARREST): study protocol for a phase I trial treating polymetastatic cancer with stereotactic radiotherapy. BMC Cancer. (2021) 21:405. doi: 10.1186/s12885-021-08020-2
60. Palma DA, Olson R, Harrow S, Correa RJM, Schneiders F, Haasbeek CJA, et al. Stereotactic ablative radiotherapy for the comprehensive treatment of 4-10 oligometastatic tumors (SABR-COMET-10): study protocol for a randomized phase III trial. BMC Cancer. (2019) 19:816. doi: 10.1186/s12885-019-5977-6
61. Lievens Y, Guckenberger M, Gomez D, Hoyer M, Iyengar P, Kindts I, et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother Oncol. (2020) 148:157–66. doi: 10.1016/j.radonc.2020.04.003
62. Baker S, Jiang W, Mou B, Lund CR, Liu M, Bergman AM, et al. Progression-free survival and local control after SABR for up to 5 oligometastases: an analysis from the population-based phase 2 SABR-5 trial. Int J Radiat Oncol Biol Phys. (2022) 114:617–26. doi: 10.1016/j.ijrobp.2022.05.033
63. Sampson E, Brierley JD, Le LW, Rotstein L, Tsang RW. Clinical management and outcome of papillary and follicular (differentiated) thyroid cancer presenting with distant metastasis at diagnosis. Cancer. (2007) 110:1451–6. doi: 10.1002/cncr.v110:7
64. Lamartina L, Godbert Y, Nascimento C, Do Cao C, Hescot S, Borget I, et al. Locally unresectable differentiated thyroid cancer: outcomes and perspectives. Endocrine. (2020) 69:133–41. doi: 10.1007/s12020-020-02245-0
65. Johnson GGRJ, Park J, Helewa RM, Goldenberg BA, Nashed M, Hyun E. Total neoadjuvant therapy for rectal cancer: a guide for surgeons. Can J Surg. (2023) 66:E196–201. doi: 10.1503/cjs.005822
66. Hou S, Pan Z, Hao X, Hang Q, Ding Y. Recent progress in the neoadjuvant treatment strategy for locally advanced esophageal cancer. Cancers (Basel). (2021) 13:5162. doi: 10.3390/cancers13205162
67. Danilovic DLS, Castro G Jr., Roitberg FSR, Vanderlei FAB, Bonani FA, Freitas RMC, et al. Potential role of sorafenib as neoadjuvant therapy in unresectable papillary thyroid cancer. Arch Endocrinol Metab. (2018) 62:370–5. doi: 10.20945/2359-3997000000046
68. Gay S, Monti E, Trambaiolo Antonelli C, Mora M, Spina B, Ansaldo G, et al. Case report: lenvatinib in neoadjuvant setting in a patient affected by invasive poorly differentiated thyroid carcinoma. Future Oncol. (2019) 15:13–9. doi: 10.2217/fon-2019-0099
69. Hartl DM, Guerlain J, Bresuskin I, Baudin E, Lamartina L, Hadoux J, et al. Surgery in the context of kinase inhibitor therapy for locally invasive thyroid cancer. Eur J Surg Oncol. (2020) 46:650–5. doi: 10.1016/j.ejso.2019.09.184
70. Nava CF, Scheffel RS, Cristo AP, Ferreira CV, Weber S, Zanella AB, et al. Neoadjuvant multikinase inhibitor in patients with locally advanced unresectable thyroid carcinoma. Front Endocrinol (Lausanne). (2019) 10:712. doi: 10.3389/fendo.2019.00712
71. Stewart KE, Strachan MWJ, Srinivasan D, MacNeill M, Wall L, Nixon IJ. Tyrosine kinase inhibitor therapy in locally advanced differentiated thyroid cancer: A case report. Eur Thyroid J. (2019) 8:102–7. doi: 10.1159/000494880
72. Tsuboi M, Takizawa H, Aoyama M, Tangoku A. Surgical treatment of locally advanced papillary thyroid carcinoma after response to lenvatinib: A case report. Int J Surg Case Rep. (2017) 41:89–92. doi: 10.1016/j.ijscr.2017.10.010
73. Katoh H KS, Yakota M, Sengoku N, Sangai T. Neoadjuvant use of lenvatinib in locally advanced papillary thyroid carcinoma involving critical vessels. Int J Endocrine Oncol. (2021) 7:IJE33. doi: 10.2217/ije-2020-0014
74. Contrera KJ, Gule-Monroe MK, Hu MI, Cabanillas ME, Busaidy NL, Dadu R, et al. Neoadjuvant selective RET inhibitor for medullary thyroid cancer: A case series. Thyroid. (2023) 33:129–32. doi: 10.1089/thy.2022.0506
75. Jozaghi Y, Zafereo M, Williams MD, Gule-Monroe MK, Wang J, Grubbs EG, et al. Neoadjuvant selpercatinib for advanced medullary thyroid cancer. Head Neck. (2021) 43:E7–E12. doi: 10.1002/hed.26527
76. Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. (2010) 363:711–23. doi: 10.1056/NEJMoa1003466
77. Long GV, Atkinson V, Ascierto PA, Robert C, Hassel JC, Rutkowski P, et al. Effect of nivolumab on health-related quality of life in patients with treatment-naive advanced melanoma: results from the phase III CheckMate 066 study. Ann Oncol. (2016) 27:1940–6. doi: 10.1093/annonc/mdw265
78. Brahmer J, Reckamp KL, Baas P, Crino L, Eberhardt WE, Poddubskaya E, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. (2015) 373:123–35. doi: 10.1056/NEJMoa1504627
79. Cohen EEW, Soulieres D, Le Tourneau C, Dinis J, Licitra L, Ahn MJ, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet. (2019) 393:156–67. doi: 10.1016/S0140-6736(18)31999-8
80. Ahn S, Kim TH, Kim SW, Ki CS, Jang HW, Kim JS, et al. Comprehensive screening for PD-L1 expression in thyroid cancer. Endocr Relat Cancer. (2017) 24:97–106. doi: 10.1530/ERC-16-0421
81. Chowdhury S, Veyhl J, Jessa F, Polyakova O, Alenzi A, MacMillan C, et al. Programmed death-ligand 1 overexpression is a prognostic marker for aggressive papillary thyroid cancer and its variants. Oncotarget. (2016) 7:32318–28. doi: 10.18632/oncotarget.v7i22
82. Girolami I, Pantanowitz L, Mete O, Brunelli M, Marletta S, Colato C, et al. Programmed death-ligand 1 (PD-L1) is a potential biomarker of disease-free survival in papillary thyroid carcinoma: a systematic review and meta-analysis of PD-L1 immunoexpression in follicular epithelial derived thyroid carcinoma. Endocr Pathol. (2020) 31:291–300. doi: 10.1007/s12022-020-09630-5
83. Oh DY, Algazi A, Capdevila J, Longo F, Miller W Jr., Chun Bing JT, et al. Efficacy and safety of pembrolizumab monotherapy in patients with advanced thyroid cancer in the phase 2 KEYNOTE-158 study. Cancer. (2023) 129:1195–204. doi: 10.1002/cncr.v129.8
84. Li J, Zhang X, Mu Z, Sun D, Sun Y, Lin Y. Response to apatinib and camrelizumab combined treatment in a radioiodine refractory differentiated thyroid cancer patient resistant to prior anti-angiogenic therapy: A case report and literature review. Front Immunol. (2022) 13:943916. doi: 10.3389/fimmu.2022.943916
85. Michel Ocampo M, Lerner J, Tosonian S, Dasanu CA. Advanced papillary thyroid carcinoma responding to nivolumab. J Oncol Pharm Pract. (2021) 27:453–6. doi: 10.1177/1078155220929967
86. Riesco-Eizaguirre G, Galofre JC, Grande E, Zafon Llopis C, Ramon y Cajal Asensio T, Navarro Gonzalez E, et al. Spanish consensus for the management of patients with advanced radioactive iodine refractory differentiated thyroid cancer. Endocrinol Nutr. (2016) 63:e17–24. doi: 10.1016/j.endonu.2015.08.007
87. Albero A, Lopez JE, Torres A, de la Cruz L, Martin T. Effectiveness of chemotherapy in advanced differentiated thyroid cancer: a systematic review. Endocr Relat Cancer. (2016) 23:R71–84. doi: 10.1530/ERC-15-0194
88. Yang H, Chen Z, Wu M, Lei T, Yu H, Ge M. Remarkable response in 2 cases of Advanced Poorly Differentiated Thyroid Carcinoma with liposomal doxorubicin plus cisplatin. Cancer Biol Ther. (2016) 17:693–7. doi: 10.1080/15384047.2016.1167295
89. Tulloch-Reid M, Skarulis MC, Sherman SI, Sarlis NJ, Santarpia L. Long-term eradication of locally recurrent invasive follicular thyroid carcinoma after taxane-based concomitant chemoradiotherapy. Anticancer Res. (2009) 29:4665–71.
90. Crouzeix G, Michels JJ, Sevin E, Aide N, Vaur D, Bardet S, et al. Unusual short-term complete response to two regimens of cytotoxic chemotherapy in a patient with poorly differentiated thyroid carcinoma. J Clin Endocrinol Metab. (2012) 97:3046–50. doi: 10.1210/jc.2012-1630
91. Santini F, Bottici V, Elisei R, Montanelli L, Mazzeo S, Basolo F, et al. Cytotoxic effects of carboplatinum and epirubicin in the setting of an elevated serum thyrotropin for advanced poorly differentiated thyroid cancer. J Clin Endocrinol Metab. (2002) 87:4160–5. doi: 10.1210/jc.2001-011151
92. Dias D, Damasio I, Marques P, Simoes H, Rodrigues R, Cavaco BM, et al. Metastatic follicular thyroid cancer with a longstanding responsiveness to gemcitabine plus oxaliplatin. Eur Thyroid J. (2023) 12:e220227. doi: 10.1530/ETJ-22-0227
93. Gruning T, Tiepolt C, Zophel K, Bredow J, Kropp J, Franke WG. Retinoic acid for redifferentiation of thyroid cancer–does it hold its promise? Eur J Endocrinol. (2003) 148:395–402. doi: 10.1530/eje.0.1480395
94. Short SC, Suovuori A, Cook G, Vivian G, Harmer C. A phase II study using retinoids as redifferentiation agents to increase iodine uptake in metastatic thyroid cancer. Clin Oncol (R Coll Radiol). (2004) 16:569–74. doi: 10.1016/j.clon.2004.06.018
95. Liu YY, Stokkel MP, Pereira AM, Corssmit EP, Morreau HA, Romijn JA, et al. Bexarotene increases uptake of radioiodide in metastases of differentiated thyroid carcinoma. Eur J Endocrinol. (2006) 154:525–31. doi: 10.1530/eje.1.02123
96. Sherman EJ, Su YB, Lyall A, Schoder H, Fury MG, Ghossein RA, et al. Evaluation of romidepsin for clinical activity and radioactive iodine reuptake in radioactive iodine-refractory thyroid carcinoma. Thyroid. (2013) 23:593–9. doi: 10.1089/thy.2012.0393
97. Kebebew E, Lindsay S, Clark OH, Woeber KA, Hawkins R, Greenspan FS. Results of rosiglitazone therapy in patients with thyroglobulin-positive and radioiodine-negative advanced differentiated thyroid cancer. Thyroid. (2009) 19:953–6. doi: 10.1089/thy.2008.0371
98. Hoftijzer H, Heemstra KA, Morreau H, Stokkel MP, Corssmit EP, Gelderblom H, et al. Beneficial effects of sorafenib on tumor progression, but not on radioiodine uptake, in patients with differentiated thyroid carcinoma. Eur J Endocrinol. (2009) 161:923–31. doi: 10.1530/EJE-09-0702
99. Groussin L, Theodon H, Bessiene L, Bricaire L, Bonnet-Serrano F, Cochand-Priollet B, et al. Redifferentiating effect of larotrectinib in. Thyroid. (2022) 32:594–8. doi: 10.1089/thy.2021.0524
100. Oler G, Cerutti JM. High prevalence of BRAF mutation in a Brazilian cohort of patients with sporadic papillary thyroid carcinomas: correlation with more aggressive phenotype and decreased expression of iodide-metabolizing genes. Cancer. (2009) 115:972–80. doi: 10.1002/cncr.v115:5
101. Riesco-Eizaguirre G, Rodriguez I, de la Vieja A, Costamagna E, Carrasco N, Nistal M, et al. The BRAFV600E oncogene induces transforming growth factor beta secretion leading to sodium iodide symporter repression and increased Malignancy in thyroid cancer. Cancer Res. (2009) 69:8317–25. doi: 10.1158/0008-5472.CAN-09-1248
102. Leboulleux S, Do Cao C, Zerdoud S, Attard M, Bournaud C, Lacroix L, et al. A phase II redifferentiation trial with dabrafenib-trametinib and 131I in metastatic radioactive iodine refractory BRAF p.V600E-mutated differentiated thyroid cancer. Clin Cancer Res. (2023) 29:2401–9. doi: 10.1158/1078-0432.CCR-23-0046
103. Rothenberg SM, Daniels GH, Wirth LJ. Redifferentiation of iodine-refractory BRAF V600E-mutant metastatic papillary thyroid cancer with dabrafenib-response. Clin Cancer Res. (2015) 21:5640–1. doi: 10.1158/1078-0432.CCR-15-2298
104. Wadsley J, Ainsworth G, Coulson AB, Garcez K, Moss L, Newbold K, et al. Results of the SEL-I-METRY phase II trial on resensitization of advanced iodine refractory differentiated thyroid cancer to radioiodine therapy. Thyroid. (2023) 33:1119–23. doi: 10.1089/thy.2022.0707
105. Jaber T, Waguespack SG, Cabanillas ME, Elbanan M, Vu T, Dadu R, et al. Targeted therapy in advanced thyroid cancer to resensitize tumors to radioactive iodine. J Clin Endocrinol Metab. (2018) 103:3698–705. doi: 10.1210/jc.2018-00612
106. Goring S, Mahood Q. Radioiodine resensitization for radioiodine-refractory metastatic differentiated thyroid cancer. Can J Health Technol. (2022) 2. doi: 10.51731/cjht.2022.309
107. Syed AR, Gorana A, Nohr E, Yuan XK, Amin P, Ghaznavi S, et al. Predictors of radioiodine (RAI)-avidity restoration for NTRK fusion-positive RAI resistant metastatic thyroid cancers. Eur Thyroid J. (2024). doi: 10.1530/ETJ-23-0227
108. Ho AL, Dedecjus M, Wirth LJ, Tuttle RM, Inabnet WB 3rd, Tennvall J, et al. Selumetinib plus adjuvant radioactive iodine in patients with high-risk differentiated thyroid cancer: A phase III, randomized, placebo-controlled trial (ASTRA). J Clin Oncol. (2022) 40:1870–8. doi: 10.1200/JCO.21.00714
109. Al-Jundi M, Thakur S, Gubbi S, Klubo-Gwiezdzinska J. Novel targeted therapies for metastatic thyroid cancer-A comprehensive review. Cancers (Basel). (2020) 12:2104. doi: 10.3390/cancers12082104
110. Busaidy NL, Konda B, Wei L, Wirth LJ, Devine C, Daniels GA, et al. Dabrafenib versus dabrafenib + Trametinib in BRAF-mutated radioactive iodine refractory differentiated thyroid cancer: results of a randomized, phase 2, open-label multicenter trial. Thyroid. (2022) 32:1184–92. doi: 10.1089/thy.2022.0115
111. Brose MS, Cabanillas ME, Cohen EE, Wirth LJ, Riehl T, Yue H, et al. Vemurafenib in patients with BRAF(V600E)-positive metastatic or unresectable papillary thyroid cancer refractory to radioactive iodine: a non-randomised, multicentre, open-label, phase 2 trial. Lancet Oncol. (2016) 17:1272–82. doi: 10.1016/S1470-2045(16)30166-8
112. Wirth LJ, Sherman E, Robinson B, Solomon B, Kang H, Lorch J, et al. Efficacy of selpercatinib in RET-altered thyroid cancers. N Engl J Med. (2020) 383:825–35. doi: 10.1056/NEJMoa2005651
113. Waguespack SG, Drilon A, Lin JJ, Brose MS, McDermott R, Almubarak M, et al. Efficacy and safety of larotrectinib in patients with TRK fusion-positive thyroid carcinoma. Eur J Endocrinol. (2022) 186:631–43. doi: 10.1530/EJE-21-1259
Keywords: thyroid cancer, targeted therapy, molecular diagnosis, radioiodine-refractory differentiated thyroid cancer, multidisciplinary
Citation: Ezzat S, Pasternak JD, Rajaraman M, Abdel-Rahman O, Boucher A, Chau NG, Chen S, Gill S, Hyrcza MD, Lamond N, Massicotte M-H, Winquist E and Mete O (2024) Multidisciplinary Canadian consensus on the multimodal management of high-risk and radioactive iodine-refractory thyroid carcinoma. Front. Oncol. 14:1437360. doi: 10.3389/fonc.2024.1437360
Received: 23 May 2024; Accepted: 10 September 2024;
Published: 04 November 2024.
Edited by:
Sharon R. Pine, University of Colorado, United StatesReviewed by:
Ming Song, Sun Yat-sen University Cancer Center (SYSUCC), ChinaFrank Berger, LMU Munich University Hospital, Germany
Copyright © 2024 Ezzat, Pasternak, Rajaraman, Abdel-Rahman, Boucher, Chau, Chen, Gill, Hyrcza, Lamond, Massicotte, Winquist and Mete. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shereen Ezzat, U2hlcmVlbi5FenphdEB1aG4uY2E=