 Tämer El Saadany
Tämer El Saadany Anja Lorch2
Anja Lorch2 Matthew I. Milowsky
Matthew I. Milowsky Ursula Maria Vogl
Ursula Maria Vogl Richard Cathomas
Richard Cathomas- 1Division of Oncology/Hematology, Cantonal Hospital Graubünden, Chur, Switzerland
- 2Department of Medical Oncology and Hematology, University Hospital Zürich, Zürich, Switzerland
- 3Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
- 4IOSI (Oncology Institute of Southern Switzerland), Ente Ospedaliero Cantonale (EOC), Bellinzona, Switzerland
Immunotherapy with checkpoint inhibitors including atezolizumab, pembrolizumab and nivolumab has become an essential pillar in the management of muscle invasive and metastatic urothelial carcinoma. The field has evolved quickly in the past few years and several early beliefs have recently been upended. One such belief relates to the predictive value of PD-L1 expression based on immunohistochemistry. Nevertheless, requirements for PD-L1 expression from regulatory bodies still restrict the use of checkpoint inhibitors in urothelial carcinoma. This article provides a critical review of the available data from the registration trials on which the current regulations have been based with the conclusion that a review of the current approval status incorporating PD-1 expression is warranted.
Introduction
Immune checkpoint blockade (ICB) of the PD-1/PD-L1 (programmed death protein 1/programmed death-ligand 1) signaling pathway, have fundamentally changed the treatment of advanced urothelial carcinoma (UC). Immunohistochemical measurement of PD-L1 expression has been found to be a reliable predictive biomarker in some malignant diseases such as non-small cell lung cancer. Based on initial results published in 2014 (1), it was suggested that this might also be the case for UC. The first evidence, that PD-L1 expression might be an unreliable biomarker in UC derived from the results of the phase 3 trials in second line metastatic UC (mUC), IMvigor211 and Keynote 045 (2, 3).
This literature review aims to evaluate the key findings from registration trials in muscle invasive and metastatic UC, to delineate a clearer understanding of the role of PD-L1 expression on the efficacy of ICB therapy, thereby setting the stage for abandoning the use of PD-L1 immunohistochemistry for clinical decision-making in this disease setting.
Methods
This literature review was conducted by performing a comprehensive search of PubMed and abstracts from major oncology conferences (ASCO, ASCO GU, ESMO) up to February 2024, related to the use of ICB therapies for the treatment of muscle-invasive or metastatic UC. The search focused exclusively on those pivotal studies that have been used by regulatory bodies for drug approval.
Studies were selected based on their direct relevance to the approval of ICB therapies in the treatment of UC, thus focusing on high-quality evidence that has contributed to the current standard of care for muscle-invasive or metastatic disease. A detailed analysis of the identified studies was conducted, assessing key outcomes including overall survival (OS) and disease-free survival (DFS) in the intention-to-treat (ITT) population and in different PD-L1 expression-based subgroups.
The review also considered the regulatory decisions influenced by these trials, noting differences in approval statuses and indications between the United States of America (Food and Drug Administration [FDA]) and the European Union (European Medicines Agency [EMA]).
Results
The results of the different studies and PD-L1 expression-based subgroups are summarized in Figures 1A–C. In addition, Table 1 informs about the different PD-L1 testing assays and score calculations.
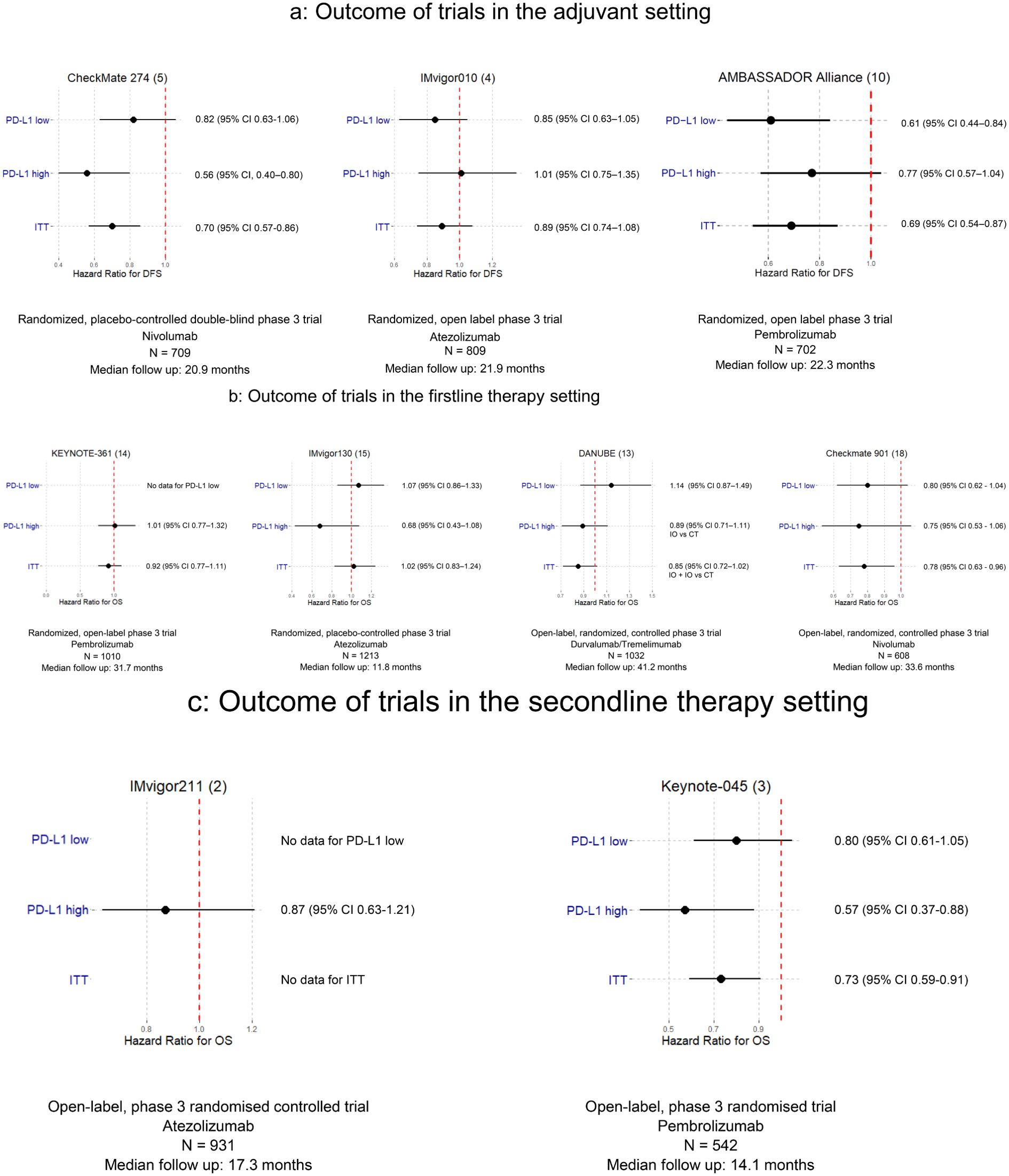
Figure 1. (A) DFS comparison according to PD-L1 status – adjuvant trials. (B) OS comparison according to PD-L1 status – first line trials. (C) OS comparison according to PD-L1 status – second line trials.
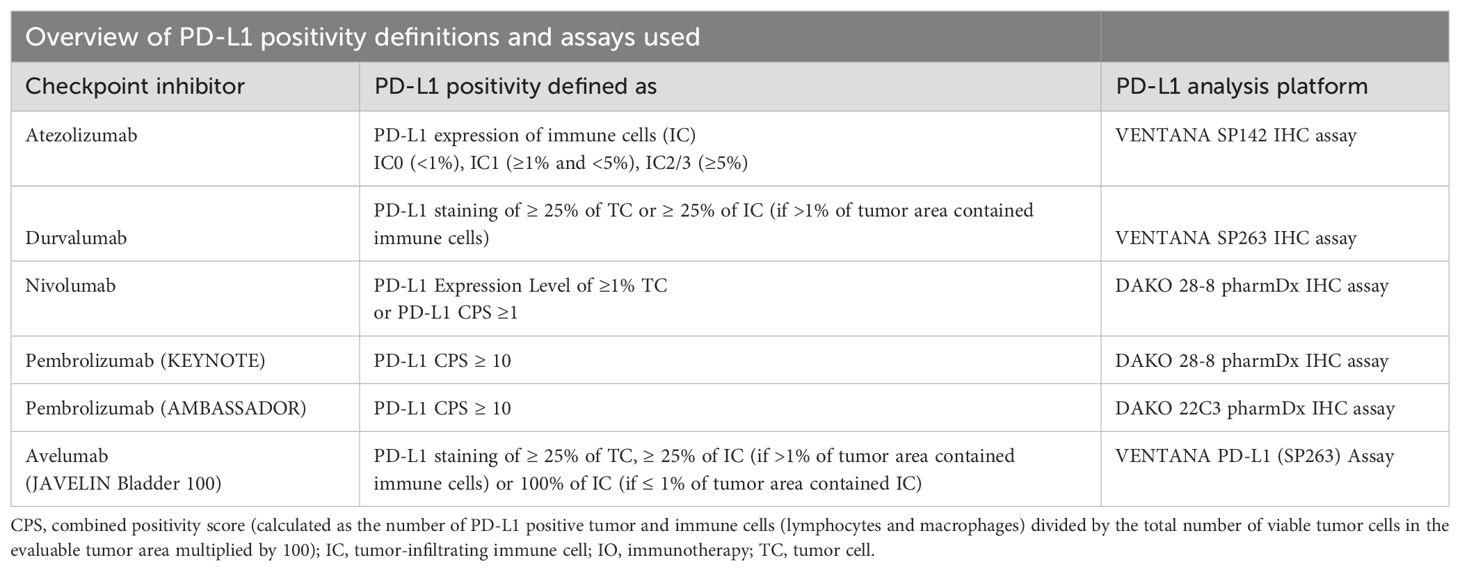
Table 1. Different PD-L1 testing assays and score calculations.
Adjuvant setting
Three trials investigated the benefit of ICB in the adjuvant treatment of resected muscle-invasive UC. The IMvigor010 study involving atezolizumab achieved no positive DFS outcome regardless of PD-L1 status (4), whereas the CheckMate 274 trial with nivolumab reported positive DFS results across all patients analyzed (ITT) (5). Notably, patients with positive PD-L1 status exhibited a more favorable hazard ratio and in a subgroup analysis, patients with a PD-L1 expression level of less than 1% in tumor cells did not experience a significant therapeutic benefit (5). A subsequent post-hoc analysis, which applied a different calculation for PD-L1 positivity using the combined positivity score (CPS) instead of solely PD-L1 expression on tumor cells, identified 89% of all trial participants as PD-L1 positive, revealing a significant DFS benefit for this group (6). This specific analysis demonstrates that PD-L1 expression measurements can be tailored to fit different arguments and lastly renders them futile. Interestingly in this case, while the FDA approved nivolumab regardless of PD-L1 status (7), the EMA and Swissmedic granted approval only for cases demonstrating PD-L1 positivity of ≥1% on tumor cells (8, 9).
The recently presented AMBASSADOR trial demonstrated a significantly improved DFS for adjuvant treatment with pembrolizumab in the ITT population. Interestingly, a subgroup analysis showed no significant DFS benefit in the PD-L1 high group (CPS ≥ 10%) whereas DFS was significantly improved in the PD-L1 low population (CPS <10%) (10). These results suggest that PD-L1 expression is probably a prognostic but not a predictive factor.
First line therapy
In the first-line treatment of patients with metastatic UC, the outcomes of ICB therapy have varied significantly in PD-L1-based subgroups. A phase 2 trial with single agent pembrolizumab revealed an advantage for patients exhibiting high PD-L1 expression with longer OS compared to those with lower PD-L1 levels (11). Conversely, in a similar trial, single agent atezolizumab showed that patients with low PD-L1 expression (<5% of immune cells) appeared to benefit more than those with higher PD-L1 expression (≥5% of immune cells) (12).
However, in two major trials (KEYNOTE-361, IMvigor130), ICB therapy did not demonstrate OS superiority over standard chemotherapy, including both ITT populations and PD-1 positive subgroups (13–15). This also applied to the ICB combination of durvaluamb plus tremelimumab (DANUBE) (13). Moreover, a subgroup analysis of cisplatin-ineligible patients from the Keynote 361 study demonstrated no OS benefit for single agent pembrolizumab vs standard carboplatin/gemcitabine (14, 16). Maintenance therapy with avelumab showed a significant OS benefit (JAVELIN Bladder 100). In this study, the treatment was given after a response to previous chemotherapy. Patients with high PD-L1 expression were identical to the corresponding ITT group regarding the OS while there was no OS benefit in patients with low PD-L1 expression (17). Recently the results of the Checkmate 901 trial were reported; an OS benefit was demonstrated for patients treated with nivolumab and cisplatin/gemcitabine chemotherapy regardless of the PD-L1 status (18).
Second line therapy
In the second line setting, IMvigor211 failed to demonstrate an OS benefit in PD-L1 selected patients, whereas Keynote 045 demonstrated improved OS in the ITT including high and low PD-L1 expression (2, 19).
Discussion
This review of the registration trials reveals no consistent association between PD-L1 expression and benefit from ICB. There is likely not a single reason with many potential explanations at play. For one, there is significant variability related to the testing performed including antibody clone, scoring system and threshold of positivity. As outlined in Table 1 several different antibodies are used in test kits, different cells are taken into account (tumor cells, immune cells) resulting in different scores (TPS, CPS, IC) with changing thresholds and finally resulting in the impossibility to compare anything. In addition, prior therapies may alter the expression of PD-L1over time as compared to baseline (20). There also may be discordance in PD-L1 expression between the primary tumor and metastatic lesions temporally and spatially (21). This means, that there is intratumoral heterogeneity within the primary tumor as well as within the metastases rendering any result very difficult to interpret. Moreover, so far unknown differences between ICB drugs might lead to different results in predictive ability of PD-L1.
When examining across all studies, the value of PD-L1 IHC in predicting benefit from ICB is uncertain and it is in fact impossible to understand the value of PD-L1 in UC. For example, it is striking that the predictive value of PD-L1 status in the first line setting in phase 2 single-arm studies (in cisplatin-ineligible patients) and in phase 3 randomized studies turns out to be entirely different with the same drugs (atezolizumab and pembrolizumab) and the same testing kit used in both instances. The same effect is seen in the adjuvant trials and in the second line studies. All of these seemingly contradictory results suggest that PD-L1 expression measured by immunohistochemistry may have prognostic but not predictive value.
The regulatory agencies and the manufacturers have only in part reacted to the updated and contradictory findings with regards to PD-L1 status and outcome in patients with muscle-invasive and metastatic UC. The FDA changed the label to omit requirement for PD-L1 and now has restricted the use of pembrolizumab in the first line metastatic setting to any platinum (cisplatin and carboplatin)-ineligible patients regardless of PD-L1 status (22). In contrast, atezolizumab was approved by FDA for first line therapy in cisplatin-ineligible patients with PD-L1 tumor proportion score of at least 5% or independent of PD-L1 expression for any platinum-ineligible patients but the indication was withdrawn voluntarily in November 2022. These changes reflect the ongoing discussions about accelerated approval of novel drugs by FDA taking into account updated and extended trial result as well as results from competing trials in the field ultimately leading to meaningful adaptations in some instances (23, 24).
In Europe, EMA restricts the use of pembrolizumab and atezolizumab in first line mUC to cisplatin-ineligible patients with PD-L1 overexpression (CPS ≥10% in case of pembrolizumab and tumor expression PD-L1 of ≥5% for atezolizumab). Adjuvant nivolumab has been approved by FDA for patients with muscle-invasive urothelial carcinoma at high risk of relapse without PD-L1 restrictions whereas EMA so far limits the use to patients with tumor cell PD-L1 expression of ≥1%. Whether this distinction is still justified appears questionable in view of the discussed lack of evidence of a predictive role of PD-L1 in urothelial cancer. Moreover, updated longterm results of Checkmate 274 indicate possible overall survival benefit in the ITT population (25) leading to further questions about the meaningfulness of PD-L1 expression restrictions.
In conclusion, PD-L1 expression does not appear to be a valuable predictive biomarker in urothelial carcinoma, neither in the muscle-invasive nor in the metastatic disease setting. While subgroup analyses remain hypothesis generating, the totality of data must be taken into account. In our view there are simply too many inconsistencies using PD-L1 immunhistochemistry expression for decision making. Finally, the research community should learn from the mistakes made and aim to develop predictive biomarkers that rely on consistent sampling and measurements with comparable and reproducible assays.
Patient summary
Regulatory bodies restrict the use of nivolumab (adjuvant setting) and pembrolizumab and atezolizumab (metastatic setting) based on PD-L1 expression in the tumor. This practice appears outdated in view of a review of the full data from the registration trials.
Author contributions
TES: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AL: Writing – original draft, Writing – review & editing. MM: Writing – original draft, Writing – review & editing. UV: Writing – original draft, Writing – review & editing. RC: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
TES – Travel support: Amgen, Sanofi. RC – Advisory role institutional: Astellas, Bayer, Merck, BMS, MSD, Janssen, Pfizer, Roche, Novartis, Astra Zeneca, Accord, Ipsen; Honoraria institutional: Accord, Roche, Merck, MSD; Travel support institutional: Astra Zeneca, Ipsen. AL – Advisory role: Astellas, Astra Zeneca, Bayer, BMS, Esai, Ipsen, Janssen, Merck, MSD, Novartis, Pfizer, Roche; Honoraria: Astellas, Novartis; Travel support: Ipsen, Janssen, Bayer. UV – Advisory board and speaker honorary institutional: Astellas, Roche, Janssen, Sanofi, Bayer, Merck, MSD, BMS, Pfizer, Novartis AAA, The Healthbook; Speaker honorary personal: The Healthbook, Kantonsspital St.Gallen, SAMO, Inselspital Bern; Travel grants: Merck, Ipsen, Janssen; Grant Funding: Fond’Action contre le cancer, Krebsliga. MIM – Stock and Other Ownership Interests: Pfizer, Merck, Gilead Sciences; Research Funding to Institution: Merck, Bristol-Myers Squibb, Mirati Therapeutics, Seagen, Alliance Foundation Trials, Alliance for Clinical Trials in Oncology, Clovis Oncology, Arvinas, ALX Oncology, Hoosier Cancer Research Network, Novartis, Acrivon Therapeutics, Astellas Pharma, Genentech, Accuray, PCCTC, G1 Therapeutics, OncoC4, Flare Therapeutics, Loxo/Lilly, Roche; Other Relationship: Elsevier, Medscape, Research to Practice; Uncompensated Relationships: G1 Therapeutics, Loxo/Lilly.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Powles T, Eder JP, Fine GD, Braiteh FS, Loriot Y, Cruz C, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. (2014) 515:558–62. doi: 10.1038/nature13904
2. Powles T, Durán I, van der Heijden MS, Loriot Y, Vogelzang NJ, De Giorgi U, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, phase 3 randomised controlled trial. Lancet. (2018) 391:748–57. doi: 10.1016/S0140-6736(17)33297-X
3. Bellmunt J, Bajorin DF. Pembrolizumab for advanced urothelial carcinoma. N Engl J Med. (2017) 376:2304. doi: 10.1056/NEJMc1704612
4. Bellmunt J, Hussain M, Gschwend JE, Albers P, Oudard S, Castellano D, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. (2021) 22:525–37. doi: 10.1016/S1470-2045(21)00004-8
5. Bajorin DF, Witjes JA, Gschwend JE, Schenker M, Valderrama BP, Tomita Y, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. (2021) 384:2102–14. doi: 10.1056/NEJMoa2034442
6. Galsky MD, Bajorin DF, Witjes JA, Gschwend JE, Tomita Y, Nasroulah F, et al. Analysis of disease-free survival in CheckMate 274 by PD-L1 combined positive score and tumor proportion score. J Clin Oncol. (2022) 40:491–1. doi: 10.1200/JCO.2022.40.6_suppl.491
7. FDA. OPDIVO (nivolumab) injection, for intravenous use (2021). Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125554s097lbledt.pdf (accessed April 26, 2024).
8. EMA. Opdivo: EPAR - Product information. 2015 - 2024 . Available online at: https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf (accessed April 26, 2024).
9. Swissmedic. Fachinformation OPDIVO® (2024). Available online at: https://swissmedicinfo.ch/showText.aspx?textType=FI&lang=DE&authNr=65660 (accessed April 26, 2024).
10. Apolo AB, Ballman KV, Sonpavde GP, Berg SA, Kim WY, Parikh RA, et al. AMBASSADOR Alliance A031501: Phase III randomized adjuvant study of pembrolizumab in muscle-invasive and locally advanced urothelial carcinoma (MIUC) vs observation. J Clin Oncol. (2024) 42:LBA531–1. doi: 10.1200/JCO.2024.42.4_suppl.LBA531
11. Vuky J, Balar AV, Castellano D, O'Donnell PH, Grivas P, Bellmunt J, et al. Long-term outcomes in KEYNOTE-052: phase II study investigating first-line pembrolizumab in cisplatin-ineligible patients with locally advanced or metastatic urothelial cancer. J Clin Oncol. (2020) 38:2658–66. doi: 10.1200/JCO.19.01213
12. Balar AV, Galsky MD, Rosenberg JE, Powles T, Petrylak DP, Bellmunt J, et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet. (2017) 389:67–76. doi: 10.1016/S0140-6736(16)32455-2
13. Powles T, van der Heijden MS, Castellano D, Galsky MD, Loriot Y, Petrylak DP, et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. (2020) 21:1574–88. doi: 10.1016/S1470-2045(20)30541-6
14. Powles T, Csőszi T, Özgüroğlu M, Matsubara N, Géczi L, Cheng SY, et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. (2021) 22:931–45. doi: 10.1016/S1470-2045(21)00152-2
15. Galsky MD, Arija JÁA, Bamias A, Davis ID, De Santis M, Kikuchi E, et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet. (2020) 395:1547–57. doi: 10.1016/S0140-6736(20)30230-0
16. Powles T, Csőszi T, Özgüroğlu M, Matsubara N, Géczi L, Cheng SY, et al. 1L pembrolizumab (pembro) versus chemotherapy (chemo) for choice-of-carboplatin patients with advanced urothelial carcinoma (UC) in KEYNOTE-361. J Clin Oncol. (2021) 39:450–0. doi: 10.1200/JCO.2021.39.6_suppl.450
17. Powles T, Park SH, Voog E, Caserta C, Valderrama BP, Gurney H, et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N Engl J Med. (2020) 383:1218–30. doi: 10.1056/NEJMoa2002788
18. van der Heijden MS, Sonpavde G, Powles T, Necchi A, Burotto M, Schenker M, et al. Nivolumab plus gemcitabine–cisplatin in advanced urothelial carcinoma. New Engl J Med. (2023) 389:1778–89. doi: 10.1056/NEJMoa2309863
19. Bellmunt J, de Wit R, Vaughn DJ, Fradet Y, Lee JL, Fong L, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. (2017) 376:1015–26. doi: 10.1056/NEJMoa1613683
20. Zhang J, Dang F, Ren J, Wei W. Biochemical aspects of PD-L1 regulation in cancer immunotherapy. Trends Biochem Sci. (2018) 43:1014–32. doi: 10.1016/j.tibs.2018.09.004
21. Burgess EF, Livasy C, Hartman A, Robinson MM, Symanowski J, Naso C, et al. Discordance of high PD-L1 expression in primary and metastatic urothelial carcinoma lesions. Urol Oncol. (2019) 37:299 e19–299 e25. doi: 10.1016/j.urolonc.2019.01.002
22. FDA. KEYTRUDA® (pembrolizumab) for injection, for intravenous use (2017). Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/125514s017s018lbl.pdf (accessed April 26, 2024).
23. Beaver JA, Pazdur R. Dangling” Accelerated approvals in oncology. N Engl J Med. (2021) 384:e68. doi: 10.1056/NEJMp2104846
24. Gyawali B, Kesselheim AS, Ross JS. The accelerated approval program for cancer drugs - finding the right balance. N Engl J Med. (2023) 389:968–71. doi: 10.1056/NEJMp2306872
Keywords: PD-L1, regulatory, urothelial carcinoma, adjuvant, metastatic, immunotherapy
Citation: El Saadany T, Lorch A, Milowsky MI, Vogl UM and Cathomas R (2024) PD-L1 expression and correlation with outcome in muscle-invasive and metastatic urothelial carcinoma: review and critical discussion. Front. Oncol. 14:1427452. doi: 10.3389/fonc.2024.1427452
Received: 03 May 2024; Accepted: 14 August 2024;
Published: 30 August 2024.
Edited by:
Marco Maruzzo, Veneto Institute of Oncology (IRCCS), ItalyReviewed by:
R.C. Koumar, Yenepoya University, IndiaCopyright © 2024 El Saadany, Lorch, Milowsky, Vogl and Cathomas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Richard Cathomas, cmljaGFyZC5jYXRob21hc0Brc2dyLmNo