
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oncol., 16 July 2024
Sec. Breast Cancer
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1418610
 Fardeen Bhimani1
Fardeen Bhimani1 Maureen McEvoy1
Maureen McEvoy1 Yu Chen1
Yu Chen1 Anjuli Gupta1
Anjuli Gupta1 Jessica Pastoriza1Arianna Cavalli2Liane Obaid2
Jessica Pastoriza1Arianna Cavalli2Liane Obaid2 Carolyn Rachofsky2Shani Fruchter1
Carolyn Rachofsky2Shani Fruchter1 Sheldon Feldman1*
Sheldon Feldman1*Background: Breast cancer-related lymphedema (BCRL) profoundly impacts patients’ quality of life, causing heightened depression, anxiety, and physical limitations. Surgical removal of the axillary nodes, combined with radiation therapy, is a significant risk factor for BCRL. Smarter axillary surgery, coupled with early detection and fostering lymphedema education, significantly improves BCRL management, promoting timely diagnosis and treatment. A lymphedema prevention program encompassing all these factors can significantly aid in preventing, treating, and reducing the severity of BCRL cases. Therefore, our study aims to share our insights and experiences gained from implementing a lymphedema prevention program at our institution.
Methods & Results: At our institution, axillary reverse mapping (ARM) is performed on all patients undergoing axillary surgery. We surveil these patients with pre- and postoperative SOZO® measurements using bioimpedance spectroscopy to detect sub-clinical lymphedema. Concerning education, we use a 3-pronged approach with surgeons, nurse practitioners, and video representation for patients. We have had 212 patients undergo the ARM procedure since 2019, with three (1.41%) developing persistent lymphedema.
Conclusion: Our study underscores the significance of a comprehensive lymphedema prevention program, integrating smarter axillary surgery, early detection, and patient education. The lymphedema rate of 1.41% not only validates the success rate of these interventions but also advocates for their widespread adoption to enhance the holistic care of breast cancer survivors. As we continue to refine and expand our program, further research, and long-term follow-up are crucial to improve prevention strategies continually and enhance the overall well-being of individuals at risk of BCRL.
Breast cancer-related lymphedema (BCRL) is a common complication associated with breast cancer treatment (1). It occurs as a result of disruptions in the lymphatic system, impeding proper drainage from lymphatic vessels and leading to the accumulation of protein-rich lymph fluid in the interstitial space (2, 3). This surplus fluid can result in abnormal swelling on the treated side’s breast, trunk, or upper extremity. The development of BCRL is multifaceted, stemming from a combination of treatment-related factors such as surgical interventions, radiation therapy, and chemotherapy (4–10). In addition to these treatment-related factors, patient-specific factors also play a key role in BCRL development. These include advanced age, race, an elevated body mass index (BMI), cellulitis, and variations in limb volume (11–14). Depending upon the severity of edema, BCRL symptoms include arm tightness, tingling, numbness, heaviness/fullness, pain, and impaired limb function (2, 15, 16). As fluid accumulation progresses, it may culminate in fibrosis, causing further dexterity issues (17). Apart from physical symptoms, BCRL also affects a patient’s quality of life (QoL); prior studies have demonstrated that BCRL significantly diminishes a patient’s QoL, leading to higher incidences of depression and anxiety, as well as greater physical impairment such as the risk of developing cellulitis and angiosarcoma when compared to individuals without BCRL (18–22). Therefore, identification and intervention for BCRL is of paramount importance, as it exerts a profound impact on the patient’s overall well-being.
A lymphedema prevention program could significantly aid in preventing, treating, and reducing the severity of BCRL cases. An important cause for the development of BCRL is the removal of arm nodes that drain the upper extremity at the time of surgery (23, 24). Adopting smarter axillary surgery, such as Axillary Reverse Mapping (ARM), can potentially reduce lymphedema by identifying and maintaining upper lymphatic drainage during Axillary Lymph Node Dissection (ALND) and Sentinel Lymph Node Biopsy (SLNB) (25). Several studies have attested to the effectiveness of ARM in diminishing the prevalence of lymphedema (26–31). Additionally, early detection also plays a crucial role in the management of BCRL. Multiple diagnostic modalities exist for the detection of BCRL, from traditional tape measurement to sophisticated techniques like Perometry and Bioimpedance Spectroscopy (BIS) (32–34). Moreover, fostering lymphedema education and awareness can significantly contribute to timely diagnosis and treatment. Prior studies have underscored the lack of knowledge and awareness among women diagnosed with breast cancer regarding lymphedema (16, 35). Therefore, our study aims to share our insights and experiences gained from implementing a lymphedema prevention program at our institution. Our multifaceted approach encompasses smarter axillary surgery, early detection modality, and a commitment to educating and raising awareness, collectively contributing to a more proactive stance against BCRL.
Smarter axillary surgery refers to novel surgical techniques and approaches to lower the risk of complications, particularly lymphedema, associated with procedures like ALND and SLNB. The surgical techniques aim to preserve lymphatic drainage pathways during surgery to minimize lymphatic system disruption. These include but are not limited to ARM, lymphatic microsurgical preventive healing approach (LyMPHA), simplified lymphatic microsurgical preventing healing approach (S-LyMPHA), and lymphatic re-approximation. Smarter axillary surgeries can be extremely beneficial in patients where ALND cannot be avoided by decreasing the level of morbidity, especially when 82% of women have at least one upper extremity symptom following ALND (36).
We are increasingly avoiding axillary surgery for many patients who are elderly and clinically node negative per SSO Choosing Wisely guidelines and the recently published SOUND trial result. For those patients deemed to benefit from axillary surgery, we routinely perform the ARM technique (37, 38). The ARM technique can distinguish between lymphatic drainage pathways of the breast and the arm using agents like blue dye, ICG-Indocyanine green fluorescence, or radioisotope, which allow visualization of lymphatic channels in the upper extremities. The technique involves the injection of the agent dermally and subcutaneously in the upper inner arm along the medial intramuscular groove of the ipsilateral arm to locate the draining lymphatics from the arm and sparing the nodes identified by the agent to prevent lymphedema (39). Multiple studies have been conducted highlighting the effectiveness of the technique in reducing BCRL (26–31).
The LyMPHA procedure is usually performed in patients when a malignant node is identified, draining the arm. In such instances, a lymphovascular anastomosis is performed to proactively prevent secondary lymphedema. Plastic surgeons usually perform the procedure during cancer surgery and require a microscope. Following the excision of the blue arm node, the blue lymphatic vessel is placed inside a vein branch with a competent valve and secured with an 8-0 permanent suture (40).
The S-LyMPHA is a both simplified and modified technique that an operating surgeon usually performs without a microscope. During ALND, the transected blue lymphatic channels are identified. Upon completion of the dissection, these channels are meticulously dissected and invaginated into the cut end of a neighboring vein using a sleeve technique, secured with two 7-0 nonabsorbable sutures.
Lymphatic re-approximation involves the reanastomosis of afferent and efferent lymphatics. Following the removal of the Arm nodes (which drains both the breast and axilla), transected lymphatics can undergo re-approximation where afferent and efferent fatty bundles are reapproximated with 3-0 vicryl.
Notably, not all ALND patients undergo lymphatic re-approximation/LyMPHA procedure. In certain cases, a selective ALND is performed to preserve arm nodes that are not grossly malignant. However, if the arm nodes are deemed malignant, ALND with LYMPHA is performed, which involves removing the affected nodes as part of the ALND procedure and then restoring lymphatic drainage via LyMPHA.
At our institution, we perform the ARM technique on all patients undergoing SLNB and ALND. To perform the ARM technique, we primarily use a blue dye 15 minutes before making an incision in the axilla. The dye is injected in the upper medial aspect of the arm and massaged for approximately 5 minutes. For patients undergoing simultaneous reconstruction procedures alongside cancer surgery, we have implemented the LyMPHA procedure. In cases where a malignant blue node is removed, the breast surgeons routinely perform a lymphatic re-approximation procedure in the setting of SLNB. This additional step, similar to the LyMPHA procedure, has been highly effective in contributing to lower rates of lymphedema.
According to the ISL, lymphedema is categorized into 4 stages (41). Stage 0 is defined as a subclinical stage where the patient has an increase in limb volume but develops no signs and symptoms. Stage 1 manifests as early edema that shows improvement with limb elevation. Stage 2 is characterized by pitting edema that persists even with elevation. Stage 3 involves fibroadipose deposition and skin changes. Notably, Stages 0 and 1 are reversible and treatable in the majority of cases, whereas Stages 2 and 3 are deemed irreversible (42). Early detection and treatment are crucial for Stages 0 and 1 to prevent the patient from experiencing a lifetime of morbidity, highlighting the significance of early detection.
Various modalities can be employed to diagnose BCRL, encompassing basic physical examination using a measuring tape, limb immersion technique, Perometry, BIS, and Lymphoscintigraphy (43). However, each modality has its distinct strengths and limitations. Tape measurements are reliable, validated, and cost-effective, yet necessitate strict protocols and training (44). The water displacement technique with limb immersion is used for volumetric assessment but is time-consuming, involves bulky equipment, requires specific hospital protocols, and is discouraged in the presence of skin lesions. Moreover, it has the potential for inter- and intra-observer variations (45–50). Perometry is a validated and reliable tool capable of detecting subclinical lymphedema, but its cost, lack of portability, and need for dedicated space limit accessibility (43, 51–53). BIS is efficient, accurate, and aids in early detection of BCRL (54–56). However, it comes with monthly software and data management fees (43). Lymphoscintigraphy is considered the gold standard in diagnosing BCRL, offering direct visualization of lymphatic function (57). A radiotracer injected into the hand or wrist is absorbed by lymphatic vessels and nodes during this procedure. A single-photon emission computed tomography is used to evaluate dermal backflow and identify lymphatic blockages. While Lymphoscintigraphy is diagnostically accurate, it’s an invasive procedure, demands skilled personnel, and is costly (43).
We utilize the SOZO® device, which uses BIS to assess tissue resistance to an electrical current and converts it into a score in real-time reflecting interstitial fluid content (58) (Figure 1). Detecting sub-clinical lymphedema enables early intervention in BCRL, leading to timely resolution (32, 51, 59). Patients undergoing SLNB and/or ALND receive a preoperative L-Dex score assessment, followed by postoperative monitoring at 3 to 6-month intervals to detect sub-clinical lymphedema. Sub-clinical lymphedema is defined as an absolute L-Dex score exceeding +10 and an increase of 6.5 or more from baseline. SOZO® scores at each follow-up are compared to preoperative baseline scores to monitor changes. This has enabled prompt initiation of interventions like prescribing compression garments or physical therapy, leading to resolution for many patients and highlighting its clinical significance.

Figure 1 SOZO® Device.
We also consider subjective factors when evaluating arm symptoms related to lymphedema. We use the QuickDASH questionnaire, a validated patient-reported outcome tool that strongly correlates with the original DASH and has been used to assess the effectiveness of lymphedema treatment (60, 61). QuickDASH introduces an important subjective dimension to our safety measures. We administer this questionnaire preoperatively to establish a baseline and at each follow-up.
Lymphedema education and awareness could significantly contribute to early diagnosis and treatment. Studies conducted by Fu et al. (16, 35) have revealed that lack of awareness about lymphedema prevents women from seeking necessary support and assistance, thereby exacerbating their suffering and distress. Furthermore, Thomas-MacLean et al. (60) highlighted a lack of knowledge about BCRL among healthcare providers across various disciplines, encompassing surgeons, oncology department staff, and family physicians. Thus, physicians must remain vigilant, recognizing BCRL and its symptoms while prioritizing comprehensive patient education.
Our comprehensive patient education initiatives aim to fill knowledge gaps and empower patients through a three-pronged approach. The surgeon leads preoperative discussions on lymphedema, emphasizing the risks and benefits of lymph node surgery, including its causes, signs, symptoms, associated risks, and available treatment options. Subsequently, nurse practitioners offer detailed oral and written explanations, supplemented by educational materials, providing patients with comprehensive insights into their postoperative care. Providing written and oral information contributes to better outcomes, as patients who receive guidance exhibit improved management of BCRL (61). Furthermore, before their SOZO® measurements, patients view an informative graphic video available in both English and Spanish, illustrating the workings of the lymphatic system, the removal of nodes, stages of lymphedema, associated symptoms, and the measurement process to provide a visual representation for better understanding (See Supplementary Material for video link). With the introduction of our educational approach, we’ve observed a positive shift in patient engagement and proactivity. During follow-ups, patients are now actively requesting their SOZO® measurements without prompting from providers. Additionally, patients are independently researching lymphedema prevention online and incorporating lymphedema exercises into their routines, showcasing an increased awareness and proactive approach to their well-being.
We retrospectively analyzed data from 2019 to 2022, during which our institution performed the ARM procedure on 212 patients. The mean age and BMI, along with standard deviation, accounted for 57.4 + 11.3 years and 29.5 + 5.7 kg/m2, respectively. A majority of our patients (83%) belonged to ethnic minorities. Of the 212, 143 (67.5%) underwent lumpectomy, and 69 (32.5%) had mastectomy. Additionally, 177 (83.5%) had SLNB, and 35 (16.5%) underwent ALND (Table 1).
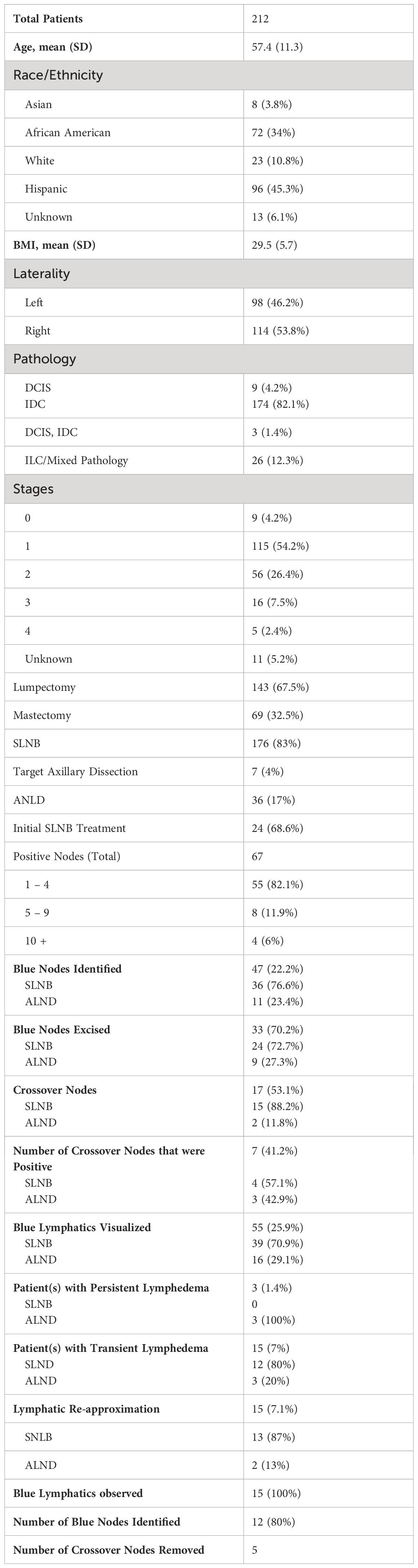
Table 1 Summary of patient data.
ARM was performed on all 212 patients undergoing axillary surgery of which 176 (83%) patients underwent SLNB, and 36 (17%) underwent ALND. Intraoperatively, blue nodes were identified in 47 patients (22.2%), 36 during SLNB, and 11 during ALND. Blue lymphatics were observed in 55 patients (23.4%), with 39 identified during SLNB and 16 during ALND. Of the identified blue nodes, 68.1% (n=32) were excised, and 53.1% (n=17) were diagnosed as crossover nodes, which are defined as sentinel nodes that are blue. Among the 67 patients with positive nodes, 19 had blue nodes removed, and 7 were crossover nodes. One patient experienced persistent lymphedema after crossover node removal.
In our cohort, lymphatic re-approximation was conducted on 15 patients, with 13 undergoing SLNB and 2 undergoing ALND. Among these patients, 12 had blue nodes identified, including 5 crossover nodes that were subsequently removed. Blue lymphatics were observed in all 15 patients. Notably, one patient undergoing Lymphatic re-approximation developed persistent lymphedema.
Lymphedema assessment using SOZO® involved a comparison of pre-operative and post-operative L-Dex scores. The mean pre-operative L-Dex score for the entire cohort was 0.12 ± 6.4 (normal range -10 to +10). Regarding BCRL, 18 patients exhibited an elevated L-Dex score during post-operative follow-up. Notably, 15 of these patients saw a resolution of lymphedema, as indicated by a decrease in their L-Dex score at the 3-month follow-up. Consequently, our overall lymphedema rate was 1.41% (3/212), with rates of 0% (0/176) following SLNB and 8.3% (3/36) after ALND. The remaining three patients who developed BCRL had all undergone ALND; two of them continued to have persistent lymphedema after blue node removal, with L-Dex scores of 23.77 and 22.39, respectively, at the 2-year follow-up. The third patient died from metastatic cancer progression, and her final L-Dex score was 77.8. All individuals with persistent lymphedema underwent treatment comprising a combination of compression sleeve therapy and physical therapy. Among the 15 individuals with transient lymphedema, 9 were treated with a sleeve and/or physical therapy, while the remaining 6 experienced spontaneous resolution of their condition during follow-up.
Our multifaceted lymphedema prevention program has significantly reduced our lymphedema rate through smarter axillary surgery and early detection using SOZO®. As a result, our lymphedema rate is significantly lower than previously reported data (14, 62, 63). Most patients in our cohort belong to ethnic minorities and had a higher BMI. This is particularly noteworthy, as prior studies have illustrated a two-fold increased risk of lymphedema in ethnic minority populations, particularly African-Americans (14, 62, 63). Flores et al. (14) reported a rate of lymphedema of 40.4% (42/104) among African-American patients, characterized by signs and symptoms. In contrast, our study found a significant reduction in the incidence of BCRL, particularly among African-American patients (3/72) (Chi-square test p<0.001). Moreover, having a BMI exceeding 25 kg/m² is a significant risk factor for developing lymphedema (64, 65). According to a study by Meeske et al. (66), women with a BMI greater than 25 kg/m² experienced a twofold increase in arm lymphedema, while those with a BMI exceeding 30 kg/m² had a threefold increase. Notably, despite our study participants having a mean BMI of 29.5 ± 5.7 kg/m², our observed rate of lymphedema was significantly lower. Our overall lymphedema rate of 1.41% is similar to that documented by Tummel et al. (67), who conducted a prospective single-arm phase II trial to determine if ARM prevents lymphedema and found that objective lymphedema rates for SLNB and ALND were 0.8% and 6.5%, respectively. Similarly, Yue et al. (31) randomized 265 patients to undergo ALND or ALND+ARM and reported that lymphedema occurred in 33% of the ALND and 6% of the ALND+ARM patients. Likewise, Yuan et al. (26) and Faisal et al. (27) performed ARM in ALND patients and found a lymphedema rate of 3.3% and 4.2% following ARM compared to 15.3% and 16.7% after ALND, respectively.
Furthermore, the LyMPHA and S-LyMPHA techniques have also shown effectiveness in lowering the incidence of BCRL. A study by Boccardo et al. (68) highlighted that ALND patients undergoing LyMPHA experienced a significantly lower lymphedema incidence of 4.34% compared to 30.43% in those without LyMPHA at their 6-month follow-up. In a subsequent study, they observed a 4% lymphedema rate after ALND over a 4-year follow-up period in 74 patients (69). Similarly, Feldman et al. (70) demonstrated that the lymphedema rate was 3 (12.5%) out of 24 patients who underwent a successfully completed LyMPHA procedure, compared to 50% among patients in whom LyMPHA was unsuccessful. Likewise, Ozmen et al. (71) found that patients undergoing S-LyMPHA had a lower rate of 3%, compared to 19% in those without S-LyMPHA (p=0.001). Apart from these, the lymphatic-reapproximation technique, when incorporated alongside the ARM procedure at our institution, demonstrated a low lymphedema incidence of only 1 out of 15 patients. Tummel et al. (67) similarly incorporated this technique into their ARM procedure, revealing a statistically significant difference in lymphedema outcomes. Patients undergoing re-approximation experienced a 0% rate, whereas those without re-approximation exhibited a BCRL rate of 18.7% (p=0.009) (67).
The integration of SOZO® into our program has been a transformative asset, significantly enhancing our ability to detect sub-clinical lymphedema. At our institution, 18 patients were diagnosed as having BCRL via SOZO®. However, the prompt treatment led to a resolution in 15 of these patients, highlighting the role of SOZO® in diagnosing early-stage BCRL and preventing these individuals from enduring lifelong morbidity. The PREVENT trial underscored the precision of BIS in identifying patients who would benefit from early compression treatment compared to traditional tape measurements (72). Similarly, in a prospective study, high-risk BCRL patients undergoing ALND had regular BIS assessments every 3-6 months. Those with sub-clinical lymphedema received physical therapy, compression garments, and lymphedema education. Notably, 4.4% developed clinically evident BCRL at the 19-month follow-up (54). This emphasizes the importance of establishing basic surveillance models to triage individuals for timely preventive measures effectively. However, it is crucial to acknowledge that accurate SOZO® measurements may necessitate basic training and require a dedicated space and a monthly subscription. Notably, Current Procedural Terminology (CPT®) codes facilitate reimbursement for SOZO® measurements, rendering the surveillance program financially feasible, thereby reducing both lymphedema incidence and overall financial burden. We adopted the QuickDASH questionnaire in 2022. The data is premature to draw conclusions. Nevertheless, the authors strongly advocate implementing a robust lymphedema prevention program. Such initiatives are pivotal in substantially reducing the incidence of BCRL.
Our study underscores the significance of a comprehensive lymphedema prevention program, integrating smarter axillary surgery, early detection, and patient education. The lymphedema rate of 1.41% not only validates the success rate of these interventions but also advocates for their widespread adoption to enhance the holistic care of breast cancer survivors. As we continue to refine and expand our program, further research, and long-term follow-up are crucial to continually improve prevention strategies and enhance the overall well-being of individuals at risk of BCRL.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Office of Human Research Affairs - Albert Einstein College of Medicine/Montefiore Medical Center. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because of the retrospective design of the study.
FB: Conceptualization, Data curation, Formal analysis, Investigation, Project administration, Writing – original draft, Writing – review & editing. MM: Project administration, Visualization, Writing – original draft, Writing – review & editing. YC: Data curation, Formal analysis, Resources, Software, Visualization, Writing – original draft, Writing – review & editing. AG: Project administration, Visualization, Writing – original draft, Writing – review & editing. JP: Project administration, Supervision, Writing – original draft, Writing – review & editing. AC: Data curation, Investigation, Writing – original draft, Writing – review & editing. LO: Data curation, Investigation, Writing – original draft, Writing – review & editing. CR: Data curation, Investigation, Writing – original draft, Writing – review & editing. SFr: Investigation, Methodology, Writing – original draft, Writing – review & editing. SFe: Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1418610/full#supplementary-material
1. Akezaki Y, Nakata E, Kikuuchi M, Tominaga R, Kurokawa H, Okamoto M, et al. Factors affecting participation in leisure activities in patients after breast cancer surgery. Healthc (Basel). (2021) 9. doi: 10.3390/healthcare9081078
2. Chowdhry M, Rozen WM, Griffiths M. Lymphatic mapping and preoperative imaging in the management of post-mastectomy lymphoedema. Gland Surg. (2016) 5:187–96. doi: 10.3978/j.issn.2227-684X.2015.11.06
3. Hespe GE, Nitti MD, Mehrara BJ. Pathophysiology of lymphedema. Springer: Lymphedema: Presentation, diagnosis, and treatment. (2015), 9–18. doi: 10.1007/978-3-319-14493-1_2
4. Siegel R, DeSantis C, Virgo K, Stein K, Mariotto A, Smith T, et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. (2012) 62:220–41. doi: 10.3322/caac.21149
5. Lee TS, Kilbreath SL, Refshauge KM, Herbert RD, Beith JM. Prognosis of the upper limb following surgery and radiation for breast cancer. Breast Cancer Res Treat. (2008) 110:19–37. doi: 10.1007/s10549-007-9710-9
6. Gärtner R, Jensen MB, Kronborg L, Ewertz M, Kehlet H, Kroman N. Self-reported arm-lymphedema and functional impairment after breast cancer treatment–a nationwide study of prevalence and associated factors. Breast. (2010) 19:506–15. doi: 10.1016/j.breast.2010.05.015
7. Bulley C, Gaal S, Coutts F, Blyth C, Jack W, Chetty U, et al. Comparison of breast cancer-related lymphedema (upper limb swelling) prevalence estimated using objective and subjective criteria and relationship with quality of life. BioMed Res Int. (2013) 2013:807569. doi: 10.1155/2013/807569
8. Armer J, Fu MR, Wainstock JM, Zagar E, Jacobs LK. Lymphedema following breast cancer treatment, including sentinel lymph node biopsy. Lymphology. (2004) 37:73–91.
9. McLaughlin SA, Wright MJ, Morris KT, Sampson MR, Brockway JP, Hurley KE, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: patient perceptions and precautionary behaviors. J Clin Oncol. (2008) 26:5220–6. doi: 10.1200/JCO.2008.16.3766
10. Gillespie TC, Sayegh HE, Brunelle CL, Daniell KM, Taghian AG. Breast cancer-related lymphedema: risk factors, precautionary measures, and treatments. Gland Surg. (2018) 7:379–403. doi: 10.21037/gs
11. Leray H, Malloizel-Delaunay J, Lusque A, Chantalat E, Bouglon L, Chollet C, et al. Body mass index as a major risk factor for severe breast cancer-related lymphedema. Lymphat Res Biol. (2020) 18:510–6. doi: 10.1089/lrb.2019.0009
12. Guliyeva G, Huayllani MT, Boczar D, Avila FR, Forte AJ. Correlation of older age with severity of lymphedema in breast cancer survivors: A systematic review. Breast Dis. (2021) 40:191–7. doi: 10.3233/BD-201067
13. Ferguson CM, Swaroop MN, Horick N, Skolny MN, Miller CL, Jammallo LS, et al. Impact of ipsilateral blood draws, injections, blood pressure measurements, and air travel on the risk of lymphedema for patients treated for breast cancer. J Clin Oncol. (2016) 34:691–8. doi: 10.1200/JCO.2015.61.5948
14. Flores AM, Nelson J, Sowles L, Stephenson RG, Robinson K, Cheville A, et al. Lymphedema signs, symptoms, and diagnosis in women who are in minority and low-income groups and have survived breast cancer. Phys Ther. (2020) 100:487–99. doi: 10.1093/ptj/pzaa002
15. Armer JM, Radina ME, Porock D, Culbertson SD. Predicting breast cancer-related lymphedema using self-reported symptoms. Nurs Res. (2003) 52:370–9. doi: 10.1097/00006199-200311000-00004
16. Fu MR, Rosedale M. Breast cancer survivors’ experiences of lymphedema-related symptoms. J Pain Symptom Manage. (2009) 38:849–59. doi: 10.1016/j.jpainsymman.2009.04.030
17. Hespe GE, Nores GG, Huang JJ, Mehrara BJ. Pathophysiology of lymphedema-Is there a chance for medication treatment? J Surg Oncol. (2017) 115:96–8. doi: 10.1002/jso.24414
18. Chachaj A, Małyszczak K, Pyszel K, Lukas J, Tarkowski R, Pudełko M, et al. Physical and psychological impairments of women with upper limb lymphedema following breast cancer treatment. Psychooncology. (2010) 19:299–305. doi: 10.1002/pon.1573
19. Khan F, Amatya B, Pallant JF, Rajapaksa I. Factors associated with long-term functional outcomes and psychological sequelae in women after breast cancer. Breast. (2012) 21:314–20. doi: 10.1016/j.breast.2012.01.013
20. Vassard D, Olsen MH, Zinckernagel L, Vibe-Petersen J, Dalton SO, Johansen C. Psychological consequences of lymphoedema associated with breast cancer: a prospective cohort study. Eur J Cancer. (2010) 46:3211–8. doi: 10.1016/j.ejca.2010.07.041
21. Jørgensen MG, Hermann AP, Madsen AR, Christensen S, Ingwersen KG, Thomsen JB, et al. Cellulitis is associated with severe breast cancer-related lymphedema: an observational study of tissue composition. Cancers (Basel). (2021) 13. doi: 10.3390/cancers13143584
22. Mesli SN, Ghouali AK, Benamara F, Taleb FA, Tahraoui H, Abi-Ayad C. Stewart-treves syndrome involving chronic lymphedema after mastectomy of breast cancer. Case Rep Surg. (2017) 2017:4056459. doi: 10.1155/2017/4056459
23. Wijaya WA, Peng J, He Y, Chen J, Cen Y. Clinical application of axillary reverse mapping in patients with breast cancer: A systematic review and meta-analysis. Breast. (2020) 53:189–200. doi: 10.1016/j.breast.2020.08.007
24. Liu S, Wang N, Gao P, Liu P, Yang H, Xie F, et al. Using the axillary reverse mapping technique to screen breast cancer patients with a high risk of lymphedema. World J Surg Oncol. (2020) 18:118. doi: 10.1186/s12957-020-01886-9
25. Shao X, Sun B, Shen Y. Axillary reverse mapping (ARM): where to go. Breast Cancer. (2019) 26:1–10. doi: 10.1007/s12282-018-0886-0
26. Yuan Q, Wu G, Xiao SY, Hou J, Ren Y, Wang H, et al. Identification and preservation of arm lymphatic system in axillary dissection for breast cancer to reduce arm lymphedema events: A randomized clinical trial. Ann Surg Oncol. (2019) 26:3446–54. doi: 10.1245/s10434-019-07569-4
27. Faisal M, Sayed MG, Antonious K, Abo Bakr A, Farag SH. Prevention of lymphedema via axillary reverse mapping for arm lymph-node preservation following breast cancer surgery: a randomized controlled trial. Patient Saf Surg. (2019) 13:35. doi: 10.1186/s13037-019-0217-1
28. Abdelhamid MI, Bari AA, Farid MI, Nour H. Evaluation of axillary reverse mapping (ARM) in clinically axillary node negative breast cancer patients - Randomised controlled trial. Int J Surg. (2020) 75:174–8. doi: 10.1016/j.ijsu.2020.01.152
29. Gennaro M, Maccauro M, Mariani L, Listorti C, Sigari C, De Vivo A, et al. Occurrence of breast-cancer-related lymphedema after reverse lymphatic mapping and selective axillary dissection versus standard surgical treatment of axilla: A two-arm randomized clinical trial. Cancer. (2022) 128:4185–93. doi: 10.1002/cncr.34498
30. Beek MA, Gobardhan PD, Klompenhouwer EG, Menke-Pluijmers MB, Steenvoorde P, Merkus JW, et al. A patient- and assessor-blinded randomized controlled trial of axillary reverse mapping (ARM) in patients with early breast cancer. Eur J Surg Oncol. (2020) 46:59–64. doi: 10.1016/j.ejso.2019.08.003
31. Yue T, Zhuang D, Zhou P, Zheng L, Fan Z, Zhu J, et al. A prospective study to assess the feasibility of axillary reverse mapping and evaluate its effect on preventing lymphedema in breast cancer patients. Clin Breast Cancer. (2015) 15:301–6. doi: 10.1016/j.clbc.2015.01.010
32. Cornish BH, Chapman M, Hirst C, Mirolo B, Bunce IH, Ward LC, et al. Early diagnosis of lymphedema using multiple frequency bioimpedance. Lymphology. (2001) 34:2–11.
33. Ridner SH, Dietrich MS, Cowher MS, Taback B, McLaughlin S, Ajkay N, et al. A randomized trial evaluating bioimpedance spectroscopy versus tape measurement for the prevention of lymphedema following treatment for breast cancer: interim analysis. Ann Surg Oncol. (2019) 26:3250–9. doi: 10.1245/s10434-019-07344-5
34. O’Toole J, Jammallo LS, Miller CL, Skolny MN, Specht MC, Taghian AG. Screening for breast cancer-related lymphedema: the need for standardization. Oncologist. (2013) 18:350–2. doi: 10.1634/theoncologist.2012-0387
35. Fu MR, Axelrod D, Haber J. Breast-cancer-related lymphedema: information, symptoms, and risk-reduction behaviors. J Nurs Scholarsh. (2008) 40:341–8. doi: 10.1111/j.1547-5069.2008.00248.x
36. McEvoy MP, Ravetch E, Patel G, Fox J, Feldman S. Prevention of breast cancer-related lymphedema. Clin Breast Cancer. (2021) 21:128–42. doi: 10.1016/j.clbc.2021.02.009
37. Sentinel node biopsy | Choosing Wisely. Available online at: https://www.choosingwisely.org/clinician-lists/sso-sentinel-node-biopsy-in-node-negative-women-70-and-over/.
38. Gentilini OD, Botteri E, Sangalli C, Galimberti V, Porpiglia M, Agresti R, et al. Sentinel lymph node biopsy vs no axillary surgery in patients with small breast cancer and negative results on ultrasonography of axillary lymph nodes: the SOUND randomized clinical trial. JAMA Oncol. (2023) 9:1557–64. doi: 10.1001/jamaoncol.2023.3759
39. Thompson M, Korourian S, Henry-Tillman R, Adkins L, Mumford S, Westbrook KC, et al. Axillary reverse mapping (ARM): a new concept to identify and enhance lymphatic preservation. Ann Surg Oncol. (2007) 14:1890–5. doi: 10.1245/s10434-007-9412-x
40. Boccardo F, Casabona F, De Cian F, Friedman D, Villa G, Bogliolo S, et al. Lymphedema microsurgical preventive healing approach: a new technique for primary prevention of arm lymphedema after mastectomy. Ann Surg Oncol. (2009) 16:703–8. doi: 10.1245/s10434-008-0270-y
41. Lymphology ISo. The diagnosis and treatment of peripheral lymphedema: 2013 Consensus Document of the International Society of Lymphology. Lymphology. (2013) 46:1–11.
42. Sleigh BC MB. Lymphedema statPearls. Treasure Island, Fl: StatPearls Publishing (2023). Available at: https://www.ncbi.nlm.nih.gov/books/NBK537239/.
43. McLaughlin SA, Brunelle CL, Taghian A. Breast cancer-related lymphedema: risk factors, screening, management, and the impact of locoregional treatment. J Clin Oncol. (2020) 38:2341–50. doi: 10.1200/JCO.19.02896
44. Tidhar D, Armer JM, Deutscher D, Shyu CR, Azuri J, Madsen R. Measurement issues in anthropometric measures of limb volume change in persons at risk for and living with lymphedema: A reliability study. J Pers Med. (2015) 5:341–53. doi: 10.3390/jpm5040341
45. Sander AP, Hajer NM, Hemenway K, Miller AC. Upper-extremity volume measurements in women with lymphedema: a comparison of measurements obtained via water displacement with geometrically determined volume. Phys Ther. (2002) 82:1201–12. doi: 10.1093/ptj/82.12.1201
46. Campbell JL, Coyer FM, Osborne SR. The skin safety model: reconceptualizing skin vulnerability in older patients. J Nurs Scholarsh. (2016) 48:14–22. doi: 10.1111/jnu.12176
47. Taylor R, Jayasinghe UW, Koelmeyer L, Ung O, Boyages J. Reliability and validity of arm volume measurements for assessment of lymphedema. Phys Ther. (2006) 86:205–14. doi: 10.1093/ptj/86.2.205
48. Deltombe T, Jamart J, Recloux S, Legrand C, Vandenbroeck N, Theys S, et al. Reliability and limits of agreement of circumferential, water displacement, and optoelectronic volumetry in the measurement of upper limb lymphedema. Lymphology. (2007) 40:26–34.
49. Meijer RS, Rietman JS, Geertzen JH, Bosmans JC, Dijkstra PU. Validity and intra- and interobserver reliability of an indirect volume measurements in patients with upper extremity lymphedema. Lymphology. (2004) 37:127–33.
50. Invernizzi M, Runza L, De Sire A, Lippi L, Blundo C, Gambini D, et al. Integrating augmented reality tools in breast cancer related lymphedema prognostication and diagnosis. J Vis Exp. (2020) 10:422. doi: 10.3389/fonc.2020.00422
51. Stout Gergich NL, Pfalzer LA, McGarvey C, Springer B, Gerber LH, Soballe P. Preoperative assessment enables the early diagnosis and successful treatment of lymphedema. Cancer. (2008) 112:2809–19. doi: 10.1002/cncr.23494
52. Stanton AW, Northfield JW, Holroyd B, Mortimer PS, Levick JR. Validation of an optoelectronic limb volumeter (Perometer). Lymphology. (1997) 30:77–97.
53. Ancukiewicz M, Russell TA, Otoole J, Specht M, Singer M, Kelada A, et al. Standardized method for quantification of developing lymphedema in patients treated for breast cancer. Int J Radiat Oncol Biol Phys. (2011) 79:1436–43. doi: 10.1016/j.ijrobp.2010.01.001
54. Soran A, Ozmen T, McGuire KP, Diego EJ, McAuliffe PF, Bonaventura M, et al. The importance of detection of subclinical lymphedema for the prevention of breast cancer-related clinical lymphedema after axillary lymph node dissection; a prospective observational study. Lymphat Res Biol. (2014) 12:289–94. doi: 10.1089/lrb.2014.0035
55. Kilgore LJ, Korentager SS, Hangge AN, Amin AL, Balanoff CR, Larson KE, et al. Reducing breast cancer-related lymphedema (BCRL) through prospective surveillance monitoring using bioimpedance spectroscopy (BIS) and patient directed self-interventions. Ann Surg Oncol. (2018) 25:2948–52. doi: 10.1245/s10434-018-6601-8
56. Koelmeyer L, Gaitatzis K, Ridner SH, Boyages J, Nelms J, Hughes TM, et al. Implementing a prospective surveillance and early intervention model of care for breast cancer-related lymphedema into clinical practice: application of the RE-AIM framework. Support Care Cancer. (2021) 29:1081–9. doi: 10.1007/s00520-020-05597-5
57. Ogata F, Azuma R, Kikuchi M, Koshima I, Morimoto Y. Novel lymphography using indocyanine green dye for near-infrared fluorescence labeling. Ann Plast Surg. (2007) 58:652–5. doi: 10.1097/01.sap.0000250896.42800.a2
59. Shah C, Arthur DW, Wazer D, Khan A, Ridner S, Vicini F. The impact of early detection and intervention of breast cancer-related lymphedema: a systematic review. Cancer Med. (2016) 5:1154–62. doi: 10.1002/cam4.691
60. Thomas-MacLean R, Miedema B, Tatemichi SR. Breast cancer-related lymphedema: women’s experiences with an underestimated condition. Can Fam Physician. (2005) 51:246–7.
61. Conway MM. Professional education on breast cancer-related lymphoedema and its relation to patient wellbeing. Wounds UK. (2016) 12:22–9.
62. Black DM, Jiang J, Kuerer HM, Buchholz TA, Smith BD. Racial disparities in adoption of axillary sentinel lymph node biopsy and lymphedema risk in women with breast cancer. JAMA Surg. (2014) 149:788–96. doi: 10.1001/jamasurg.2014.23
63. Kwan ML, Yao S, Lee VS, Roh JM, Zhu Q, Ergas IJ, et al. Race/ethnicity, genetic ancestry, and breast cancer-related lymphedema in the Pathways Study. Breast Cancer Res Treat. (2016) 159:119–29. doi: 10.1007/s10549-016-3913-x
64. Mehrara BJ, Greene AK. Lymphedema and obesity: is there a link? Plast Reconstr Surg. (2014) 134:154e–60e. doi: 10.1097/PRS.0000000000000268
65. Kwan ML, Darbinian J, Schmitz KH, Citron R, Partee P, Kutner SE, et al. Risk factors for lymphedema in a prospective breast cancer survivorship study: the Pathways Study. Arch Surg. (2010) 145:1055–63. doi: 10.1001/archsurg.2010.231
66. Meeske KA, Sullivan-Halley J, Smith AW, McTiernan A, Baumgartner KB, Harlan LC, et al. Risk factors for arm lymphedema following breast cancer diagnosis in Black women and White women. Breast Cancer Res Treat. (2009) 113:383–91. doi: 10.1007/s10549-008-9940-5
67. Tummel E, Ochoa D, Korourian S, Betzold R, Adkins L, McCarthy M, et al. Does axillary reverse mapping prevent lymphedema after lymphadenectomy? Ann Surg. (2017) 265:987–92. doi: 10.1097/SLA.0000000000001778
68. Boccardo F, Valenzano M, Costantini S, Casabona F, Morotti M, Sala P, et al. LYMPHA technique to prevent secondary lower limb lymphedema. Ann Surg Oncol. (2016) 23:3558–63. doi: 10.1245/s10434-016-5282-4
69. Boccardo F, Casabona F, De Cian F, Friedman D, Murelli F, Puglisi M, et al. Lymphatic microsurgical preventing healing approach (LYMPHA) for primary surgical prevention of breast cancer-related lymphedema: over 4 years follow-up. Microsurgery. (2014) 34:421–4. doi: 10.1002/micr.v34.6
70. Feldman S, Bansil H, Ascherman J, Grant R, Borden B, Henderson P, et al. Single institution experience with lymphatic microsurgical preventive healing approach (LYMPHA) for the primary prevention of lymphedema. Ann Surg Oncol. (2015) 22:3296–301. doi: 10.1245/s10434-015-4721-y
71. Ozmen T, Lazaro M, Zhou Y, Vinyard A, Avisar E. Evaluation of simplified lymphatic microsurgical preventing healing approach (S-LYMPHA) for the prevention of breast cancer-related clinical lymphedema after axillary lymph node dissection. Ann Surg. (2019) 270:1156–60. doi: 10.1097/SLA.0000000000002827
Keywords: breast cancer-related lymphedema, BCRL, SOZO®, bioimpedance spectroscopy, BIS, lymphedema education, axillary reverse mapping, ARM
Citation: Bhimani F, McEvoy M, Chen Y, Gupta A, Pastoriza J, Cavalli A, Obaid L, Rachofsky C, Fruchter S and Feldman S (2024) Comprehensive strategies in breast cancer-related lymphedema prevention: insights from a multifaceted program. Front. Oncol. 14:1418610. doi: 10.3389/fonc.2024.1418610
Received: 16 April 2024; Accepted: 24 June 2024;
Published: 16 July 2024.
Edited by:
Sharon R. Pine, University of Colorado Anschutz Medical Campus, United StatesReviewed by:
Luigi Losco, University of Salerno, ItalyCopyright © 2024 Bhimani, McEvoy, Chen, Gupta, Pastoriza, Cavalli, Obaid, Rachofsky, Fruchter and Feldman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheldon Feldman, c2ZlbGRtYW5AbW9udGVmaW9yZS5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.