 Xiangcheng Chen
Xiangcheng Chen Xinyi Hu
Xinyi Hu Tiancai Liu
Tiancai Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol., 03 June 2024
Sec. Gastrointestinal Cancers: Hepato Pancreatic Biliary Cancers
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1415260
Pancreatic cancer is a highly lethal malignant tumor, which has the characteristics of occult onset, low early diagnosis rate, rapid development and poor prognosis. The reason for the high mortality is partly that pancreatic cancer is usually found in the late stage and missed the best opportunity for surgical resection. As a promising detection technology, liquid biopsy has the advantages of non-invasive, real-time and repeatable. In recent years, the continuous development of liquid biopsy has provided a new way for the detection and screening of pancreatic cancer. The update of biomarkers and detection tools has promoted the development of liquid biopsy. Circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), circulating tumor RNA (ctRNA) and extracellular vesicles (EVs) provide many biomarkers for liquid biopsy of pancreatic cancer, and screening tools around them have also been developed. This review aims to report the application of liquid biopsy technology in the detection of pancreatic cancer patients, mainly introduces the biomarkers and some newly developed tools and platforms. We have also considered whether liquid biopsy technology can replace traditional tissue biopsy and the challenges it faces.
Pancreatic cancer is a highly lethal malignant tumor. In 2024, it is estimated that new cases of pancreatic cancer in the United States will reach 66440, and deaths will reach 51750 (1). Although the 5-year relative survival rate of pancreatic cancer has greatly improved since 1975, it remains the lowest among all cancers, with only 13% (1). Pancreatic cancer has a high lifetime mortality to morbidity risk ratio and is expected to become the second leading cause of cancer death in the United States by 2026 (2). It is worth noting that the lifetime risk of pancreatic cancer continues to increase with the increase of the Human Development Index (HDI) level (2). Pancreatic cancer can be divided into resectable, borderline resectable, locally advanced or metastatic diseases (3). Surgical resection is a very effective treatment option at present (3, 4). The 5-year survival rate of patients with surgical resection was significantly higher than the actual 5-year survival rate of patients with pancreatic cancer at all stages. (4). However, many patients are in unresectable cancer at the time of diagnosis, and effective treatment methods are limited to chemotherapy, leading to poor prognosis of pancreatic cancer (3). Approximately 80% -85% of pancreatic ductal adenocarcinoma (PDAC) patients have locally advanced or distant metastatic diseases, only 15–20% of patients being diagnosed at the early stage of the disease (3).
As a promising detection technology, liquid biopsy has the advantages of non-invasive, real-time and repeatable. In 1994, it was first reported that mutant Kristen rat sarcoma (KRAS) sequences were detected in plasma circulating tumor DNA (ctDNA) of pancreatic cancer patients by PCR with allele specific primers, which means that liquid biopsy is promising for cancer detection (5). In the past decade, non-invasive methods of cancer diagnosis and monitoring, such as liquid biopsy, have gradually replaced invasive techniques such as tissue biopsy. Circulating tumor cells (CTCs), ctDNA, extracellular vesicles (EVs) and circulating tumor RNA (ctRNA) are the main targets of liquid biopsy. This review focuses on the latest research progress of liquid biopsy in the detection and screening of patients with pancreatic cancer, and evaluates its prospects and challenges.
Medical imaging plays an important role in early screening of pancreatic cancer. Computed tomography (CT) scanning, magnetic resonance imaging (MRI) and endoscopic ultrasonography (EUS) have been used to screen pancreatic cancer in high-risk groups with genetic syndrome or family history. Some scholars suggest using CT or MRI as a first-line investigation for suspected cancer patients, as this cross-sectional imaging modality is considered the gold standard for detecting primary lesions and distant metastases (6). EUS has become a powerful diagnostic modality that can provide high-resolution images of the pancreas, with quality far superior to other imaging techniques (7). In the past few years, endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) has been considered the most advanced and accurate diagnostic technique (7). A major advantage of EUS-FNA is its high sensitivity and specificity. A meta-analysis showed that a pooled sensitivity of EUS-FNA in diagnosing the correct etiology of pancreatic solid masses was 86.8%, and a pooled specificity of EUS-FNA was 95.8% (7). The overall complication rate of EUS-FNA is very low, and the safety of EUS-FNA is high. In 2011, Wang et al. analyzed 51 articles and found that the specific incidence of EUS-FNA was 0.98%, mostly pancreatitis and postoperative pain, and the mortality rate was only 0.02% (8). However, compared with non-invasive liquid biopsy technology, puncture will inevitably cause damage, and there is a risk of cancer cell bleeding and spread.
There is no effective serum tumor marker for early detection of pancreatic cancer in serological examination (6). Carbohydrate antigen 19–9 (CA19–9) is a recognized biomarker of pancreatic cancer, but the detection of CA19–9 often appears false positive and false negative. Experiments have shown that liver diseases, lung diseases, gynecological diseases, endocrine diseases, and spleen diseases can all lead to an increase in CA19–9, especially in cases of biliary obstruction (9). Furthermore, there is still a problem of insufficient secretion of CA19–9. As early as 1987, a study showed that Lewis antigen negative patients were unable to express CA19–9 in tumor tissue and had lower levels of CA19–9 in serum (10). As an aggressive subgroup with special clinical and molecular characteristics, Lewis negative pancreatic cancer accounts for about 5–10% of individuals (11). These factors have reduced the sensitivity and specificity of CA19–9 in the early detection of pancreatic cancer. An experiment proved that the sensitivity and specificity of CA19–9 level reached 60% and 99% within 0 to 6 months before diagnosis, and the sensitivity and specificity of cases diagnosed with early disease reached 50% and 99% (12). It can also effectively distinguish resectable pancreatic cancer from chronic pancreatitis and non-cancerous cysts, with specificity of 99% and sensitivity of 46% and 30%, respectively (12). In addition to CA19–9, other serological markers, such as carcinoembryonic antigen (CEA), carbohydrate antigen 125 (CA125) and carbohydrate antigen 242 (CA242), are also used for the detection of pancreatic cancer.
CTCs are cells shed into the bloodstream from primary tumors and metastatic deposits (13). The presence of CTCs usually represents the invasion and metastasis of primary tumors, which is of great significance for the detection of pancreatic cancer (13). Accurately isolating and detecting CTC from a large number of blood cells is a major challenge, as their abundance in patient blood is extremely low. Current methods for CTC enrichment are either based on physical properties, such as size, density, or dielectrophoretic mobility (14). Or based on biological characteristics, CTCs are separated by immunoaffinity enrichment, which is divided into positive selection and negative selection (14). CTCs have many cell surface markers. The most common cell surface marker is epithelial cell adhesion molecule (EpCAM). It is a calcium dependent transmembrane glycoprotein that mediates epithelial cell adhesion and was detected by the CellSearch® platform (14). However, biomarkers including EpCAM are significantly downregulated due to EMT in CTCs, which affects the detection rate of EpCAM positive CTCs (15). It suggests that relying solely on the detection of EpCAM-positive CTCs may not accurately reflect the full extent of the circulating tumor cell population (15). In addition to EpCAM, E-cadherin, vimentin and twist protein are also often used as molecular marker proteins to identify CTCs in pancreatic cancer.
As early as 20 years ago, two scholars mentioned in their articles that tumor cells can leave the primary lesion in the early stage of development (16). There is experimental evidence that CTCs can even spread in the early stages of tumor evolution. Rhim et al. detected circulating pancreatic cells in the blood of pancreatic intraepithelial neoplasia (PanIN) stage mice and found that some epithelial cells had undergone epithelial-to-mesenchymal transition (EMT) and entered the circulatory system (17). Later, Rhim et al. conducted experiments on PDAC patients, control population and patients with precancerous cystic disease. The detection rates were 73% (8/11), 0 (0/19) and 40% (8/21) respectively (18). CTCs could be detected in the blood of patients with precancerous cystic disease, suggesting that CTCs could be used for screening human pancreatic cancer.
A meta-analysis summarized dozens of literature between 2005 and 2020, and found a significant difference in the detection rate of CTCS in pancreatic cancer, with a total detection rate of 65%, but with very high specificity approaching 100% (19). The significant difference in the detection rate of CTC has raised doubts among many scientists about its diagnostic value. The currently widely used selection system is the CellSearch® platform, which is also the only platform approved by the Food and Drug Administration (FDA) for detecting and separating CTCs. However, the CTC detection rate of the CellSearch® system in pancreatic cancer is as low as 26% (19). Stoecklein et al. improved the sensitivity of CellSearch® system detection by using diagnostic leukapheresis (DLA), significantly improving the detection rate of CTC in M0 and M1 patients with pancreatic cancer, with 44% and 74% respectively, resulting in a 60 fold increase in CTCs count (20).
In the body fluid environment, a type of free DNA fragments that can be detected are called circulating free DNA(cfDNA). The cfDNA derived from tumor cells is called ctDNA. The genetic information carried by ctDNA is consistent with the tumor cells it is located in (21). DNA released from different tumor sites can provide a complete image of the tumor genome, which is considered to be more representative of heterogeneous cancer cells than genetic information obtained from single site tissue biopsy (21).
ctDNA fragment size and ctDNA level have potential to be used to identify patients with pancreatic cancer. In one study, the plasma of 61 patients with advanced pancreatic cancer and 28 healthy volunteers. The ctDNA fragment length of healthy control samples was longer than that of patient samples, and the ctDNA level of healthy control samples was significantly lower than that of patient samples (22). In the current research situation, it is known that the high mutation frequency of pancreatic cancer driving genes, such as KRAS. KRAS mutations were detected in plasma ctDNA of patients with pancreatic cancer as early as 1994 (5), and now KRAS mutations are widely used in diagnosis and monitoring. Combined detection of KRAS mutations and four protein markers increased sensitivity to 64% and specificity to 99.5% (23). It is worth noting that methylation analysis has been continuously developed in recent years. Epigenetic reprogramming, such as DNA methylation, occurs in the early stage of tumorigenesis and has potential as a target for early detection. In a 2024 experiment, comparative methylation analysis identified 9 differentially methylated loci in pancreatic exocrine DNA (24). Research shows that plasma ctDNA methylation has great potential to distinguish chronic pancreatitis from cancer pancreatic cancer (24). In a meta-analysis that assessed the utility of ctDNA for diagnosing cancer, it was found that liquid biopsy based on ctDNA had a sensitivity of 70% and a specificity of 86% (25). Low sensitivity has become the biggest obstacle to the detection of pancreatic cancer, so ctDNA detection is not suitable for large-scale screening. Table 1 summarizes the basic information of some experiments with ctDNA detection to diagnose pancreatic cancer since 2023.
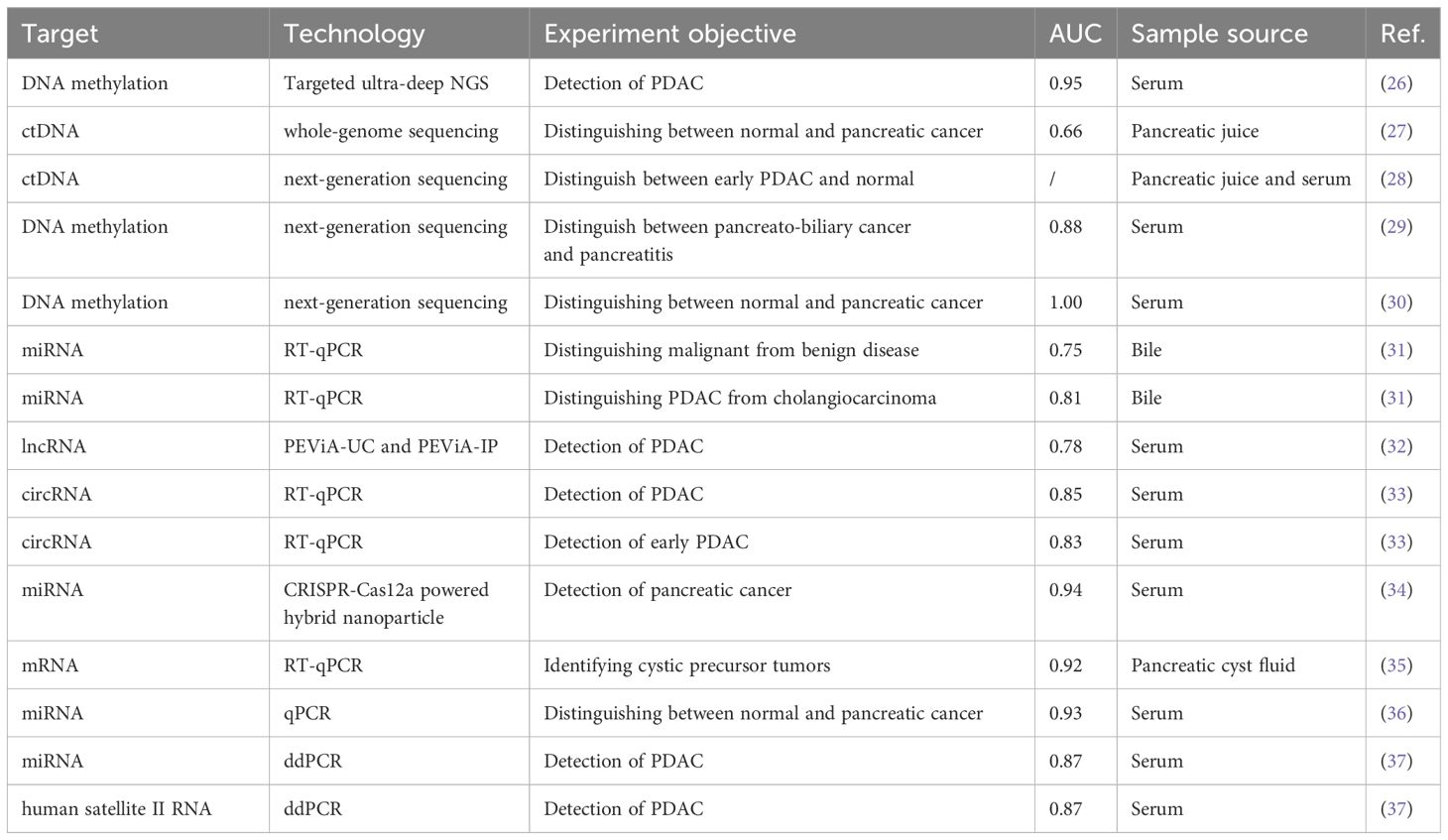
Table 1 Relevant experiments of cell-free nucleic acid in pancreatic cancer detection since 2023.
ctDNA is mixed with a large amount of DNA from non-cancer cells, so it is crucial to efficiently and accurately detect ctDNA. Currently, the technology available for ctDNA analysis is based on PCR or sequencing technology (38). At present, there are multiple commercial platforms available for detecting ctDNA from liquid biopsy, and research has been conducted on different KRAS ctDNA hotspot mutation detection platforms for in-depth evaluation (39). There are also studies evaluating the consistency of ctDNA mutation detection between the two most commonly used BEAMing and droplet digital PCR (ddPCR) (40). This comparison highlights the strong consistency between BEAMing and ddPCR, thus suggesting sufficient reproducibility for clinical applications.
Like the definition of ctDNA, circulating cell-free RNA (cfRNA) from cancer cells is called ctRNA. Due to the protection of cell membrane-like structures and RNA binding proteins, as well as their own specific structure, they have a certain degree of stability. cfRNA includes many RNA types, such as microRNA (miRNA), long non-coding RNA (lncRNA), circular RNA (circRNA), small nuclear RNA (snRNA), small nucleolar RNA (snoRNA), and so on. Since 2023, the research of RNA in the detection of pancreatic cancer has attracted extensive attention from scientists all over the world, and the research has gradually become diversified. Table 1 summarizes the basic information of some experiments related to this aspect since 2023. Interestingly, current experiments have different targets, methods, and sample sources. However, miRNA remains a hot topic in experimental research, reverse transcription-quantitative PCR (RT-qPCR) is the most popular technology today, and serum is the most commonly used sample source, with at least half of the experiments related to them.
Although cfRNAs include many RNA types, miRNAs are currently the focus of research and have received much attention. Shi et al. identified mir-1246, mir-205–5p, and mir-191–5p as serum biomarkers to identify pancreatic cancer (41). Moreover, the elevated levels of these miRNAs serve as significant indicators of the advanced stage of the disease, enabling the distinction between pancreatitis and pancreatic cancer with a precision of 91.5% (41). Prado et al. have established a distinctive miRNA signature in bile, which serves as an effective tool to differentiate between malignant and benign pancreaticobiliary diseases (31). Among these, mir-148a-3p has been particularly identified as a unique marker and its efficacy in distinguishing the two conditions has been validated (31). Furthermore, a dual miRNA signature encompassing mir-125b-5p and mir-194–5p has been formulated, enabling the precise differentiation of PDAC from cholangiocarcinoma (31).
EVs are lipid bilayer particles secreted by cells into the extracellular space. EVs can carry cellular components such as DNA, RNA, proteins, lipids, amino acids and metabolites, reflecting the state of the cell. Now, according to their biogenesis, content and secretion pathway, EVs can be divided into two major categories: exosomes and microvesicles. A comprehensive description of the nomenclature, collection and pre-processing, separation and concentration, characterization, functional studies and some general considerations of EVs was provided in the Minimum information for studies of extracellar vessels (MISEV2018). In order to provide researchers with the latest snapshot of available methods, MISEV2018 has been recently modified. The release of MISEV2023 aims to encourage more researchers to invest in the research field of EVs biomarkers and the therapeutic potential of EVs (42).
Compared to the previously mentioned ctDNA and CTC, EVs have unique advantages, with the highest sensitivity and specificity (25). Similar to ctDNA, KRAS mutations can also be detected in exosomal DNA with better sensitivity and specificity. Allenson et al. conducted experiments in age matched control groups, limited, locally advanced and metastatic PDAC patients, and found KRAS mutations in 7.4%, 66.7%, 80% and 85% of exosomal DNA, respectively (43). The experiment also compared exosomal DNA with ctDNA, and PDAC patients showed a higher proportion of detectable KRAS mutations in exosomal DNA (43). In addition, the methylation of exosomal DNA has also been confirmed to be different, which has the potential to distinguish chronic pancreatitis from pancreatic cancer (24).
EVs not only contain DNA but also RNA, which can also serve as biomarkers for tumor detection. Among them, exosomal miRNA is currently a hot research topic. The expression of miRNA-191, miRNA-21 and miRNA-451a in EVs of pancreatic cancer and IPMN patients was significantly up-regulated compared with the control group (44). Experiments have proved that the levels of these three exosomal miRNAs can be used as early diagnosis and progression markers of pancreatic cancer and IPMN, and are considered more useful than circulating miRNAs (44). Makler et al. analyzed the exosomal miRNAs in cell culture medium and detected the expression of miRNAs in pancreatic cancer (45). Seven mature miRNAs showed statistical significance, and these identified miRNAs have the potential for early detection of PDAC (45).
In 2015, a study identified a cell surface protein polysaccharide called glycan-1 (GPC1), which is particularly enriched in cancer cell-derived exosomes (46). The detection of GPC1-positive exosomes (GPC1-Exos) in the serum of pancreatic cancer patients has absolute specificity and sensitivity, which can distinguish healthy subjects and patients with a benign pancreatic disease from patients with early- and late-stage pancreatic cancer (46). Lewis et al. integrated direct exosomes and other extracellular vesicles onto an alternating current microarray chip to detect PDAC using biomarkers GPC-1 and CD63, with a sensitivity of 99% and specificity of 82% (47). In 2023, a graphene field-effect transistor (GFET) based biosensor was successfully developed for detecting PDAC through GPC-1 expression within 45 minutes (48). The GFET biosensor array can accurately distinguish between PDAC patients and healthy controls, while also being able to detect early stages of cancer, including stages 1 and 2 (48). Yang et al. identified the signature of five markers for PDAC detection, and one of the best markers, GPC1 alone, had 82% sensitivity and only 52% specificity (49). However, the combined detection of five marker signals showed 86% sensitivity and 81% specificity (49). Table 2 summarizes the relevant experiments of the citations that have appeared.
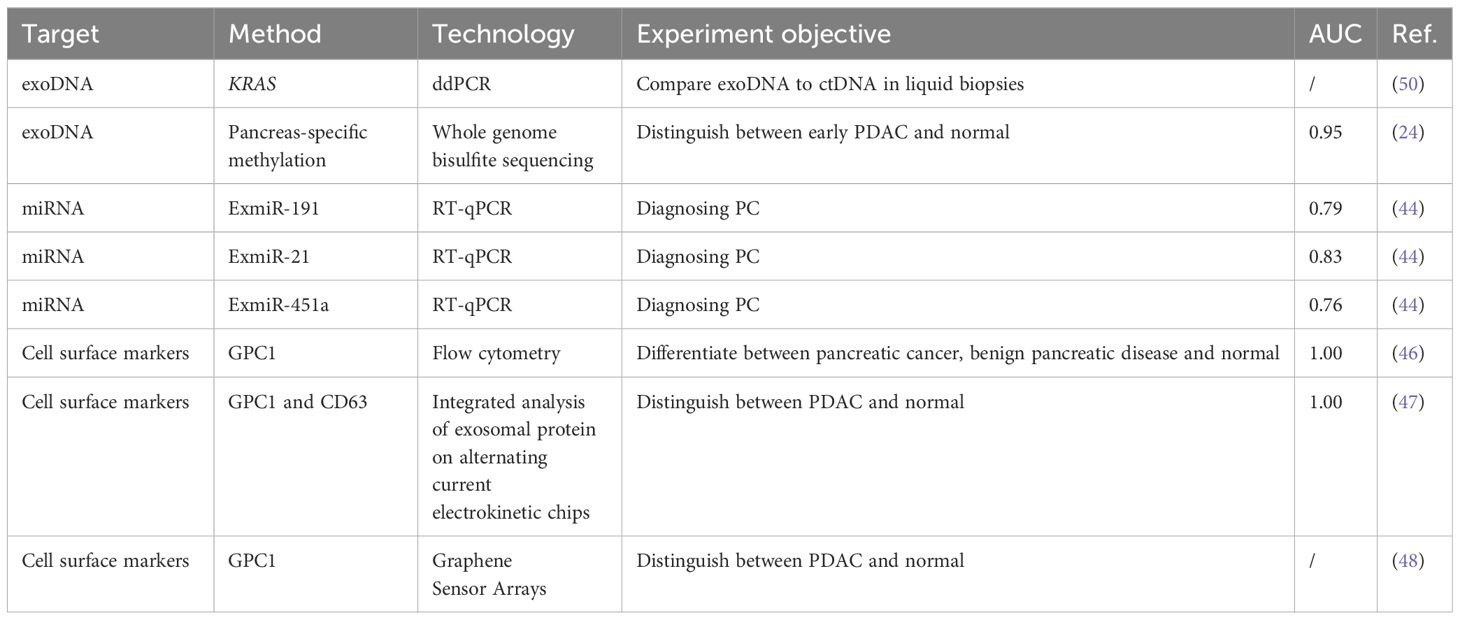
Table 2 Summary of some researches on the use of EVs detection for pancreatic cancer diagnosis.
Liquid biopsy technology has significant advantages over tissue biopsy due to its non-invasive, real-time, and high reproducibility characteristics. The biggest obstacle of liquid biopsy is that the sensitivity and specificity of early detection are not high enough. None of the various biomarkers can provide the required high sensitivity and specificity for early detection of pancreatic cancer. However, the current multi-component combination detection can to some extent improve sensitivity and specificity, and improve diagnostic accuracy. The development of new detection tools and the introduction of new technologies are pushing liquid biopsy to a new climax. Entering clinical practice, liquid biopsy still needs to be studied in practical clinical applications, and the technology needs to be standardized and rationalized. In conclusion, liquid biopsy technology has a good application prospect in the detection of pancreatic cancer, but more researchers need to invest in further in-depth research.
XC: Conceptualization, Methodology, Writing – original draft. XH: Conceptualization, Methodology, Writing – review & editing. TL: Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by National Natural Science Foundation of China (Grant No. 82372344) and Natural Science Foundation of Guangdong Province (Grant No. 2023A1515011925). The funders had no role in study design, data collection and analysis, manuscript preparation or decision to publish.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistic. CA Cancer J Clin. (2024) 74:12–49. doi: 10.3322/caac.21820
2. Wang S, Zheng R, Li J, Zeng H, Li L, Chen R, et al. Global, regional, and national lifetime risks of developing and dying from gastrointestinal cancers in 185 countries: a population-based systematic analysis of GLOBOCAN. Lancet Gastroenterol Hepatol. (2024) 9:229–37. doi: 10.1016/S2468–1253(23)00366–7
3. Ducreux M. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up (vol 26, pg v56, 2015). Ann Oncol. (2017) 28:167–8. doi: 10.1093/annonc/mdx258
4. Bengtsson A, Andersson R, Ansari D. The actual 5-year survivors of pancreatic ductal adenocarcinoma based on real-world data. Sci Rep. (2020) 10(1):16425. doi: 10.1038/s41598-020-73525-y
5. Sorenson GD, Pribish DM, Valone FH, Memoli VA, Bzik DJ, Yao SL. Soluble normal and mutated DNA sequences from single-copy genes in human blood. Cancer Epidemiol Biomarkers Prev. (1994) 3:67–71.
6. Zhang LL, Sanagapalli S, Stoita A. Challenges in diagnosis of pancreatic cancer. World J Gastroenterol. (2018) 24:2047–60. doi: 10.3748/wjg.v24.i19.2047
7. Puli SR, Bechtold ML, Buxbaum JL, Eloubeidi MA. How good is endoscopic ultrasound-guided fine-needle aspiration in diagnosing the correct etiology for a solid pancreatic mass?: A meta-analysis and systematic review. Pancreas. (2013) 42:20–6. doi: 10.1097/MPA.0b013e3182546e79
8. Wang KX, Ben QW, Jin ZD, Du YQ, Zou DW, Liao ZA, et al. Assessment of morbidity and mortality associated with EUS-guided FNA: a systematic review. Gastrointestinal Endoscopy. (2011) 73:283–90. doi: 10.1016/j.gie.2010.10.045
9. Kim S, Park BK, Seo JH, Choi J, Choi JW, Lee CK, et al. Carbohydrate antigen 19–9 elevation without evidence of Malignant or pancreatobiliary diseases. Sci Rep. (2020) 10(1):8820. doi: 10.1038/s41598–020-65720–8
10. Tempero MA, Uchida E, Takasaki H, Burnett DA, Steplewski Z, Pour PM. Relationship of carbohydrate antigen 19–9 and Lewis antigens in pancreatic cancer. Cancer Res. (1987) 47:5501–3.
11. Liu C, Deng SM, Jin KZ, Gong YT, Cheng H, Fan ZY, et al. Lewis antigen-negative pancreatic cancer: An aggressive subgroup. Int J Oncol. (2020) 56:900–8. doi: 10.3892/ijo.2020.4989
12. Fahrmann JF, Schmidt CM, Mao X, Irajizad E, Loftus M, Zhang J, et al. Lead-time trajectory of CA19–9 as an anchor marker for pancreatic cancer early detection. Gastroenterology. (2021) 1601373–1383. e1376. doi: 10.1053/j.gastro.2020.11.052
13. Pantel K, Speicher MR. The biology of circulating tumor cells. Oncogene. (2016) 35:1216–24. doi: 10.1038/onc.2015.192
14. Riethdorf S, O’Flaherty L, Hille C, Pantel K. Clinical applications of the CellSearch platform in cancer patients. Advanced Drug Delivery Rev. (2018) 125:102–21. doi: 10.1016/j.addr.2018.01.011
15. Hyun KA, Goo KB, Han H, Sohn J, Choi W, Kim SI, et al. Epithelial-to-mesenchymal transition leads to loss of EpCAM and different physical properties in circulating tumor cells from metastatic breast cancer. Oncotarget. (2016) 7:24677–87. doi: 10.18632/oncotarget.8250
16. Pantel K, Brakenhoff RH. Dissecting the metastatic cascade. Nat Rev Cancer. (2004) 4:448–56. doi: 10.1038/nrc1370
17. Rhim AD, Mirek ET, Aiello NM, Maitra A, Bailey JM, McAllister F, et al. EMT and dissemination precede pancreatic tumor formation. Cell. (2012) 148:349–61. doi: 10.1016/j.cell.2011.11.025
18. Rhim AD, Thege FI, Santana SM, Lannin TB, Saha TN, Tsai S, et al. Detection of circulating pancreas epithelial cells in patients with pancreatic cystic lesions. Gastroenterology. (2014) 146:647–51. doi: 10.1053/j.gastro.2013.12.007
19. Pang TCY, Po JW, Becker TM, Goldstein D, Pirola RC, Wilson JS, et al. Circulating tumour cells in pancreatic cancer: A systematic review and meta-analysis of clinicopathological implications. Pancreatology. (2021) 21:103–14. doi: 10.1016/j.pan.2020.11.022
20. Stoecklein NH, Fluegen G, Guglielmi R, Neves RPL, Hackert T, Birgin E, et al. Ultra-sensitive CTC-based liquid biopsy for pancreatic cancer enabled by large blood volume analysis. Mol Cancer. (2023) 22(1):181. doi: 10.1186/s12943–023-01880–1
21. Parikh AR, Leshchiner I, Elagina L, Goyal L, Levovitz C, Siravegna G, et al. Liquid versus tissue biopsy for detecting acquired resistance and tumor heterogeneity in gastrointestinal cancers. Nat Med. (2019) 25:1415–+. doi: 10.1038/s41591–019-0561–9
22. Lapin M, Oltedal S, Tjensvoll K, Buhl T, Smaaland R, Garresori H, et al. Fragment size and level of cell-free DNA provide prognostic information in patients with advanced pancreatic cancer. J Trans Med. (2018) 16(1):300. doi: 10.1186/s12967–018-1677–2
23. Cohen JD, Javed AA, Thoburn C, Wong F, Tie J, Gibbs P, et al. Combined circulating tumor DNA and protein biomarker-based liquid biopsy for the earlier detection of pancreatic cancers. Proc Natl Acad Sci U.S.A. (2017) 114:10202–7. doi: 10.1073/pnas.1704961114
24. Ben-Ami R, Wang QL, Zhang J, Supplee JG, Fahrmann JF, Lehmann-Werman R, et al. Protein biomarkers and alternatively methylated cell-free DNA detect early stage pancreatic cancer. Gut. (2024) 73:639–48. doi: 10.1136/gutjnl-2023–331074
25. Luchini C, Veronese N, Nottegar A, Cappelletti V, Daidone MG, Smith L, et al. Liquid biopsy as surrogate for tissue for molecular profiling in pancreatic cancer: A meta-analysis towards precision medicine. Cancers (Basel). (2019) 11(8):1152. doi: 10.3390/cancers11081152
26. Zhao GC, Jiang RJF, Shi Y, Gao SZ, Wang DS, Li ZL, et al. Circulating cell-free DNA methylation-based multi-omics analysis allows early diagnosis of pancreatic ductal adenocarcinoma. Mol Oncol. (2024). doi: 10.1002/1878-0261.13643
27. Levink IJM, Srebniak MI, De Valk WG, van Veghel-Plandsoen MM, Wagner A, Cahen DL, et al. An 8q24 gain in pancreatic juice is a candidate biomarker for the detection of pancreatic cancer. Int J Mol Sci. (2023) 24(6):5097. doi: 10.3390/ijms24065097
28. Levink IJM, Jansen MPHM, Azmani Z, van IJcken W, van Marion R, Peppelenbosch MP, et al. Mutation analysis of pancreatic juice and plasma for the detection of pancreatic cancer. Int J Mol Sci. (2023) 24(17):13116. doi: 10.3390/ijms241713116
29. Hartwig C, Müller J, Klett H, Kouhestani D, Mittelstädt A, Anthuber A, et al. Discrimination of pancreato-biliary cancer and pancreatitis patients by non-invasive liquid biopsy. Mol Cancer. (2024) 23(1):28. doi: 10.1186/s12943-024-01943-x
30. Bahado-Singh RO, Turkoglu O, Aydas B, Vishweswaraiah S. Precision oncology: Artificial intelligence, circulating cell-free DNA, and the minimally invasive detection of pancreatic cancer-A pilot study. Cancer Med. (2023) 12:19644–55. doi: 10.1002/cam4.6604
31. Prado MM, Puik JR, Castellano L, López-Jiménez E, Liu DSK, Meijer LL, et al. A bile-based microRNA signature for differentiating Malignant from benign pancreaticobiliary disease. Exp Hematol Oncol. (2023) 12(1):101. doi: 10.1186/s40164-023-00458-3
32. Takahashi K, Inuzuka T, Shimizu Y, Sawamoto K, TaNiue K, Ono Y, et al. Liquid biopsy for pancreatic cancer by serum extracellular vesicle-encapsulated long noncoding RNA HEVEPA. Pancreas. (2024) 53(5):e395–404. doi: 10.1097/MPA.0000000000002315
33. Xu CM, Jun ES, Okugawa Y, Toiyama Y, Borazanci E, Bolton J, et al. A circulating panel of circRNA biomarkers for the noninvasive and early detection of pancreatic ductal adenocarcinoma. Gastroenterology. (2024) 166(1):178–90.e116. doi: 10.1053/j.gastro.2023.09.050
34. Zhang TH, Xie ZH, Zheng XH, Liang YX, Lu Y, Zhong HK, et al. CRISPR-Cas12a powered hybrid nanoparticle for extracellular vesicle aggregation and in-situ microRNA detection. Biosensors Bioelectronics. (2024) 245:115856. doi: 10.1016/j.bios.2023.115856
35. Nikiforova M, Wald A, Spagnolo D, Melan M, Grupillo M, Lai YT, et al. A combined DNA/rna-based next-generation sequencing platform to improve the classification of pancreatic cysts and early detection of pancreatic cancer arising from pancreatic cysts. Gastrointestinal Endoscopy. (2023) 97:Ab784–4. doi: 10.1016/j.gie.2023.04.1280
36. Chi H, Chen HQ, Wang R, Zhang JY, Jiang L, Zhang SK, et al. Proposing new early detection indicators for pancreatic cancer: Combining machine learning and neural networks for serum miRNA-based diagnostic model. Front Oncol. (2023) 13:1244578. doi: 10.3389/fonc.2023.1244578
37. Seimiya T, Suzuki T, Iwata T, Kishikawa T, Sekiba K, Shibata C, et al. Combination of serum human satellite RNA and miR-21–5p levels as a biomarker for pancreatic cancer. Iscience. (2023) 26(2):106021. doi: 10.1016/j.isci.2023.106021
38. De Rubis G, Krishnan SR, Bebawy M. Liquid biopsies in cancer diagnosis, monitoring, and prognosis. Trends Pharmacol Sci. (2019) 40:172–86. doi: 10.1016/j.tips.2019.01.006
39. Vessies DCL, Greuter MJE, van Rooijen KL, Linders TC, Lanfermeijer M, Ramkisoensing KL, et al. Performance of four platforms for KRAS mutation detection in plasma cell-free DNA: ddPCR, Idylla, COBAS z480 and BEAMing. Sci Rep. (2020) 10:8122. doi: 10.1038/s41598–020-64822–7
40. O’Leary B, Hrebien S, Beaney M, Fribbens C, Garcia-Murillas I, Jiang J, et al. Comparison of BEAMing and droplet digital PCR for circulating tumor DNA analysis. Clin Chem. (2019) 65:1405–13. doi: 10.1373/clinchem.2019.305805
41. Shi WJ, Wartmann T, Accuffi S, Al-Madhi S, Perrakis A, Kahlert C, et al. Integrating a microRNA signature as a liquid biopsy-based tool for the early diagnosis and prediction of potential therapeutic targets in pancreatic cancer. Br J Cancer 130(1):125–34. (2023). doi: 10.1038/s41416–023-02488–4
42. Welsh JA, Goberdhan DCI, O’Driscoll L, Buzas EI, Blenkiron C, Bussolati B, et al. Minimal information for studies of extracellular vesicles (MISEV2023): From basic to advanced approaches. J Extracellular Vesicles. (2024) 13(2):e12404. doi: 10.1002/jev2.12404
43. Allenson K, Castillo J, San Lucas FA, Scelo G, Kim DU, Bernard V, et al. High prevalence of mutant KRAS in circulating exosome-derived DNA from early-stage pancreatic cancer patients. Ann Oncol. (2017) 28:741–7. doi: 10.1093/annonc/mdx004
44. Goto T, Fujiya M, Konishi H, Sasajima J, Fujibayashi S, Hayashi A, et al. An elevated expression of serum exosomal microRNA-191,-21,-451a of pancreatic neoplasm is considered to be efficient diagnostic marker. BMC Cancer. (2018) 18(1):116. doi: 10.1186/s12885–018-4006–5
45. Makler A, Narayanan R, Asghar W. An exosomal miRNA biomarker for the detection of pancreatic ductal adenocarcinoma. Biosensors-Basel. (2022) 12(10):831. doi: 10.3390/bios12100831
46. Melo SA, Luecke LB, Kahlert C, Fernandez AF, Gammon ST, Kaye J, et al. Glypican-1 identifies cancer exosomes and detects early pancreatic cancer. Nature. (2015) 523:177–U182. doi: 10.1038/nature14581
47. Lewis JM, Vyas AD, Qiu YQ, Messer KS, White R, Heller MJ. Integrated analysis of exosomal protein biomarkers on alternating current electrokinetic chips enables rapid detection of pancreatic cancer in patient blood. ACS Nano. (2018) 12:3311–20. doi: 10.1021/acsnano.7b08199
48. Yin TY, Xu LZ, Gil B, Merali N, Sokolikova MS, Gaboriau DCA, et al. Graphene sensor arrays for rapid and accurate detection of pancreatic cancer exosomes in patients’ Blood plasma samples. ACS Nano. (2023) 17:14619–31. doi: 10.1021/acsnano.3c01812
49. Yang KS, Im H, Hong S, Pergolini I, del Castillo AF, Wang R, et al. Multiparametric plasma EV profiling facilitates diagnosis of pancreatic Malignancy. Sci Trans Med. (2017) 9(391):eaal3226. doi: 10.1126/scitranslmed.aal3226
Keywords: liquid biopsy, pancreatic cancer, early detection, circulating tumor cells, circulating tumor DNA, extracellular vesicles, circulating tumor RNA
Citation: Chen X, Hu X and Liu T (2024) Development of liquid biopsy in detection and screening of pancreatic cancer. Front. Oncol. 14:1415260. doi: 10.3389/fonc.2024.1415260
Received: 12 April 2024; Accepted: 14 May 2024;
Published: 03 June 2024.
Edited by:
Yan-Shen Shan, National Cheng Kung University Hospital, TaiwanReviewed by:
Yung-Yeh Su, National Health Research Institutes, TaiwanCopyright © 2024 Chen, Hu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tiancai Liu, bGl1dGNAc211LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.