 Céline Eldani1Marie Kostine2
Céline Eldani1Marie Kostine2 Maxime Faure3
Maxime Faure3 Estibaliz Lazaro4
Estibaliz Lazaro4 Claire Rigothier5Jean Baptiste Hiriart6Bérénice Teulières7Florian Poullenot7Magalie Haissaguerre8
Claire Rigothier5Jean Baptiste Hiriart6Bérénice Teulières7Florian Poullenot7Magalie Haissaguerre8 Maeva Zysman9
Maeva Zysman9 Rémi Veillon9Charlotte Vergnenegre9Nahema Issa10
Rémi Veillon9Charlotte Vergnenegre9Nahema Issa10 Charlotte Domblides11Sorilla Mary-Prey1Marie Beylot-Barry1,12Anne Pham-Ledard1,12Caroline Dutriaux1Guilhem Sole13
Charlotte Domblides11Sorilla Mary-Prey1Marie Beylot-Barry1,12Anne Pham-Ledard1,12Caroline Dutriaux1Guilhem Sole13 Fanny Duval13
Fanny Duval13 Emilie Gerard1*
Emilie Gerard1*- 1Department of Dermatology, Centre Hospitalier Universitaire (CHU) Bordeaux, Bordeaux, France
- 2Department of Rheumatology, CHU Bordeaux, Bordeaux, France
- 3Department of Cardiology, CHU Bordeaux, Bordeaux, France
- 4Department of Internal Medicine, Haut-Leveque, Bordeaux University Hospital, Bordeaux, France
- 5Department of Nephrology, Transplantation, and Dialysis, Bordeaux University Hospital Center, Bordeaux, France
- 6Hepatology Unit, Bordeaux University Hospital, Bordeaux, France
- 7Department of Gastroenterology and Hepatology, Centre Médico-chirurgical Magellan, Hôpital Haut-Lévêque, CHU de Bordeaux, Bordeaux, France
- 8Department of Endocrinology, University Hospital of Bordeaux, Bordeaux, France
- 9Pulmonary Department, Pôle Cardio-thoracique, CHU de Bordeaux, Bordeaux, France
- 10Intensive Care Unit and Infectious Disease, University Hospital Centre Bordeaux, Bordeaux, France
- 11Department of Medical Oncology, Bordeaux University Hospital, Bordeaux, France
- 12BRIC (BoRdeaux Institute of onCology), Institut National de la Santé et de la Recherche Médicale (INSERM), Univ. Bordeaux, Bordeaux, France
- 13AOC Referral Center for Neuromuscular Diseases, Neurology and Neuromuscular Diseases Department, FILNEMUS, University Hospitals of Bordeaux, Bordeaux, France
Immune checkpoint inhibitors (ICIs) present clinicians with the challenge of managing immune-related adverse events (irAEs), which can range from mild to severe due to immune system activation 1. While guidelines recommend discontinuing ICIs for grade 3 partial and all grade 4 irAEs, there is growing interest in rechallenging patients based on oncological outcomes, particularly for cardiovascular and neurological irAEs where data remains scarce 1,2. We retrospectively evaluated the safety of ICI rechallenge following grade 3-4 irAEs, specifically focusing on cardiovascular and neurological events, in patients discussed at our multidisciplinary immunotoxicity assessment board between 2019 and 2021. Fifteen patients were included, with a median time to severe irAE onset of 49 days. Among them, five patients experienced neurological adverse events (NAEs): aseptic meningitis (3), inflammatory polyradiculoneuropathy (1), and ophthalmoplegia (1), while one patient presented with myocarditis. Of the 15 patients retreated with ICIs after initial severe irAEs, 11 (73%) remained free of subsequent irAEs, two (13%) experienced recurrence of the initial irAE, and two (13%) developed new irAEs distinct from the initial event. The median time to event recurrence was 69 days, occurring no earlier than the initial severe irAE. In the subset analysis focusing on severe cardiovascular and neurological irAEs, rechallenge with ICIs was generally well tolerated. However, one patient treated with anti-PD1 experienced a relapse of grade 2 aseptic meningitis. Overall, our findings suggest that rechallenging with ICIs after severe irAEs, including those affecting the cardiovascular and neurological systems, may be safe, particularly after irAE regression and corticosteroid withdrawal.
Introduction
Introduced 20 years ago, immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment, leading to substantial improvements in cancer outcomes and overall survival rates. These agents, including anti-CTLA-4, anti-PD-1, and anti-PD-L1 therapies, have been widely adopted in clinical practice, either as monotherapy or in combination, for the treatment of advanced solid tumors and hematologic malignancies. However, their mechanism of action, which involves activating T-cells, can also lead to immune-related adverse events (irAEs) affecting various organs. Severe irAEs, classified as grades 3-4, are reported in approximately 8% of patients receiving anti-PD-1 monotherapy, 25% with anti-CTLA-4 monotherapy, and up to 50% with combination ICIs (1). Algorithms for managing these toxicities have been developed based on the affected organ system and the severity grade. Current guidelines recommend the use of high-dose systemic corticosteroids and permanent discontinuation of ICIs for grades 3-4 irAEs (1, 2). For patients who discontinue ICI due to severe toxicity, the question of rechallenge becomes pertinent. This decision is complex and relies on the specialist’s assessment of the risk-reward ratio and the availability of alternative treatment options, often deliberated in a multidisciplinary setting. Despite the growing interest in ICI rechallenge, there is a paucity of data, particularly regarding severe neurological and cardiac toxicities (3, 4). Therefore, it is imperative to elucidate the clinical characteristics and outcomes of patients who undergo ICI rechallenge after experiencing severe irAEs. Such insights are crucial for informing clinical decision-making and optimizing the management of irAEs in patients receiving ICIs.
Methods
We conducted a retrospective monocentric study to investigate the rechallenge of ICIs following the occurrence of an initial grade 3 or 4 irAE. Patients were identified from the database of the multidisciplinary immunotoxicity assessment board (ImmunoTox) at Bordeaux University Hospital between December 2019 and December 2021. This board comprises a nationwide network of oncologists, immunologists, and organ specialists with expertise in managing irAEs.
Inclusion criteria encompassed patients treated with either single ICI (anti-PD-1, anti-PD-L1) or combination ICIs (anti-PD-1 + anti-CTLA-4), who experienced an initial severe toxicity graded as 3 or 4 according to the National Cancer Institute Common Terminology Criteria for Adverse Events. Board agreement for ICI rechallenge was mandatory for inclusion. Exclusion criteria were limited to cases with missing follow-up data or those where rechallenge did not occur despite board agreement.
We collected comprehensive data including patients’ socio-medical characteristics, type of initial ICI administered, characteristics and grading of the initial irAE, management strategies employed, and outcomes of the irAEs. Additionally, details regarding the second ICI used for rechallenge, disease status (progression, partial response, or stability) prior to rechallenge, and any concurrent immunosuppressive therapy (such as corticosteroids exceeding 20 mg/day or other immunosuppressive agents) were recorded.
This study design allowed for a thorough examination of the clinical parameters surrounding ICI rechallenge after severe irAEs, providing valuable insights into patient management and outcomes in this challenging clinical scenario.
Results
Among the 112 patients referred to our board during the study period, 28 patients were approved for ICI rechallenge following the occurrence of severe irAEs. However, 13 patients were excluded due to follow-up outside Bordeaux University Hospital (n=8), chemotherapy combined with immunotherapy (n=3), or failure to undergo rechallenge despite board agreement (n=2). Ultimately, our analysis included 15 patients who underwent ICI rechallenge after experiencing grade 3 or higher irAEs.
Patient characteristics are summarized in Table 1. The initial ICI regimen comprised anti-PD-1/anti-PD-L1 for 9 patients and combination ICIs for 6 patients. The median time from ICI initiation to initial toxicity onset was 49 days (interquartile range, 17-246 days). Detailed characteristics, management, and outcomes of the initial irAEs are presented in Table 2.
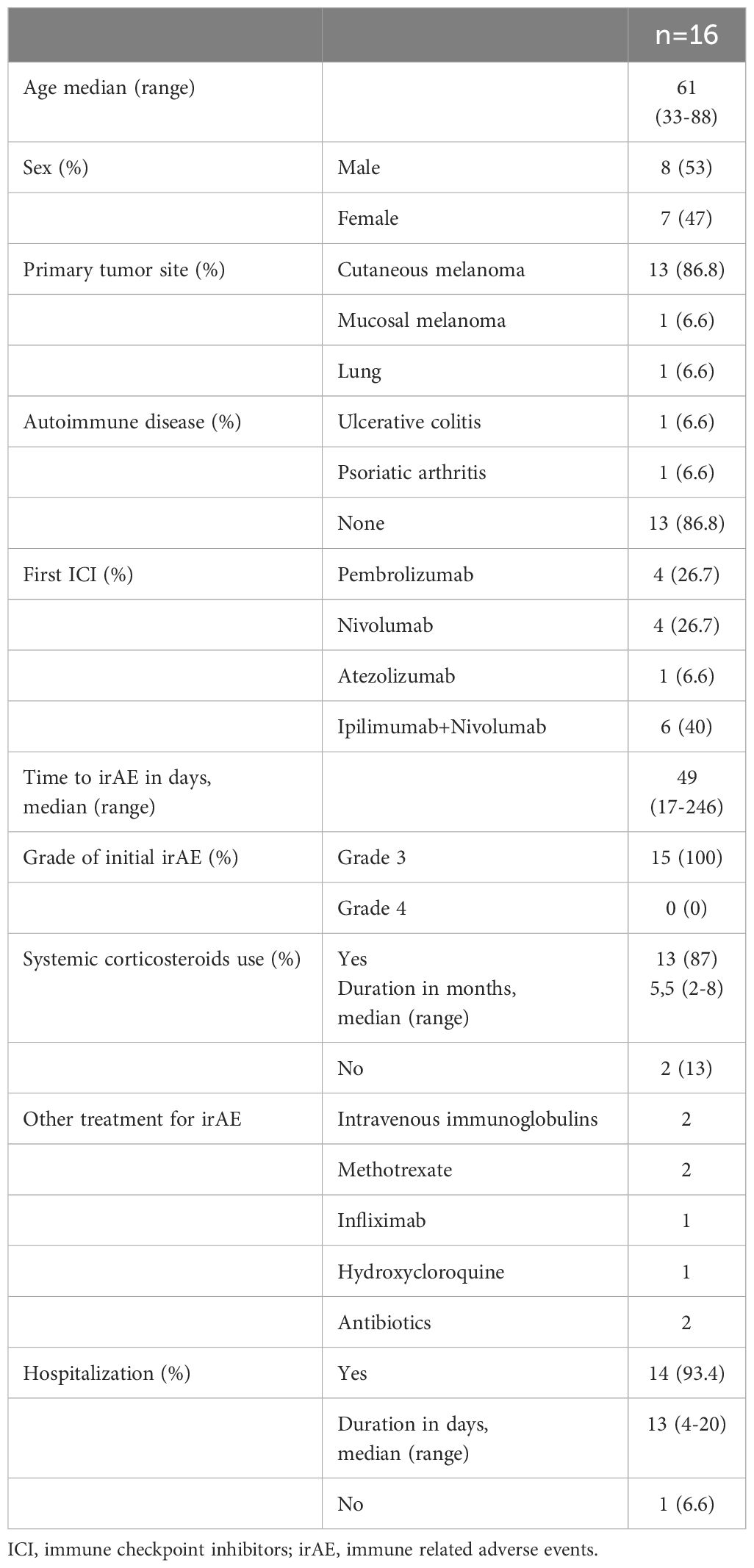
Table 1 Demographic and oncological characteristics of patients with rechallenge ICI after severe irAE.
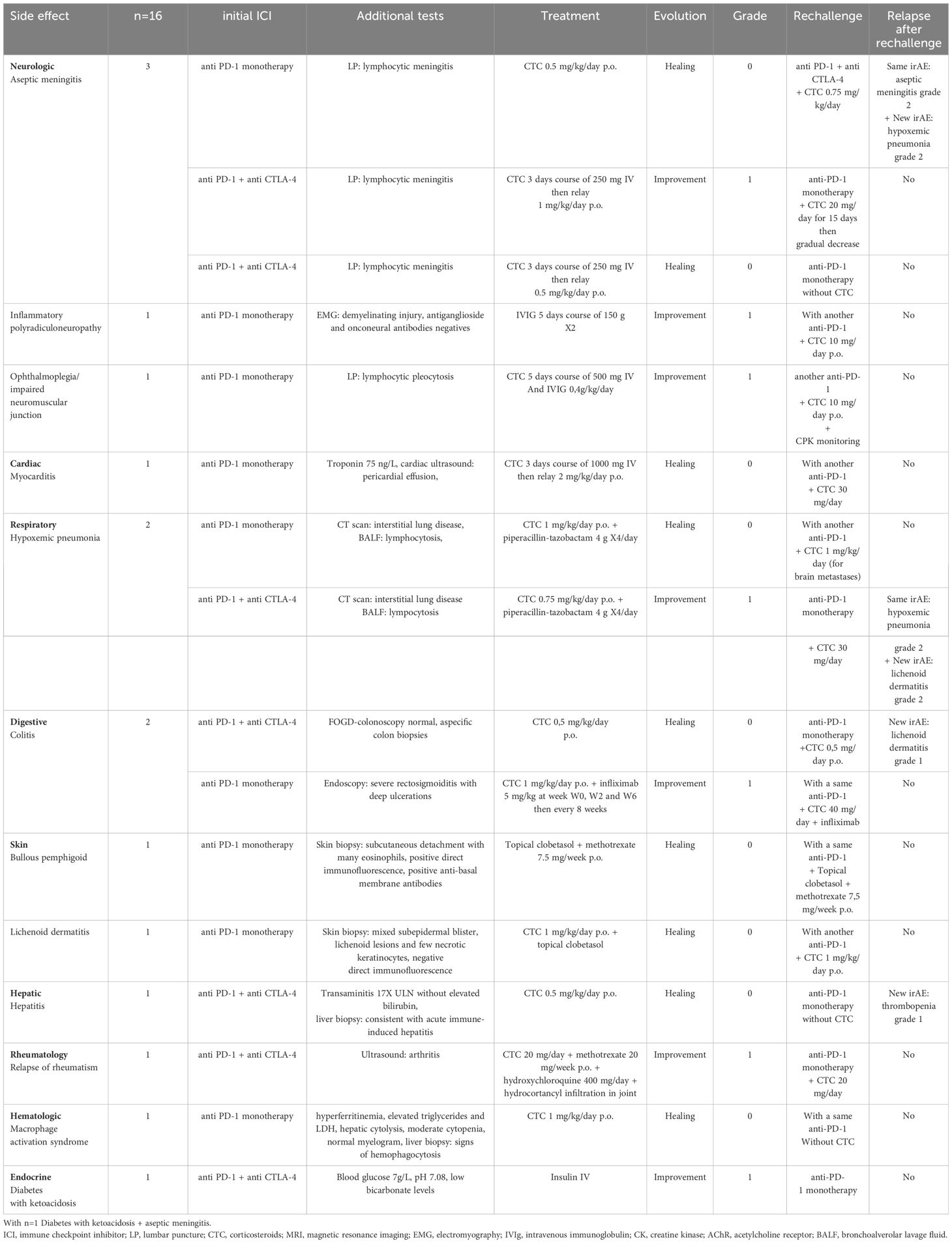
Table 2 Recurrence of irAEs after ICI rechallenge.
Among the 15 patients, 5 (33%) developed neurological adverse events (NAEs), including aseptic meningitis (n=3), inflammatory polyradiculoneuropathy (n=1), and neurological ophthalmoplegia (n=1). Prompt treatment with systemic corticosteroids and/or intravenous immunoglobulins (IVIg) resulted in complete recovery for 2 patients. However, sequelae persisted in cases of inflammatory polyradiculoneuropathy and ophthalmoplegia.
Additionally, one patient presented with immune-induced myocarditis, which was promptly managed with high-dose intravenous corticosteroids, leading to clinical and biological improvement. Other initial severe irAEs resulting in treatment interruption included pneumonitis, colitis, rash, hepatitis, rheumatoid arthritis, macrophage activation syndrome, and endocrine disorders.
ICI treatment was discontinued for all 15 patients due to severe irAEs. Most patients (87%) received systemic corticosteroid therapy, with a median hospitalization duration of 13 days (IQR: 4-20 days). In our study, 13 out of 16 patients treated with systemic corticosteroids for immune-related adverse events (irAEs) responded positively, showing healing or improvement. The corticosteroid doses varied, typically starting with high initial doses (e.g., 250-1000 mg IV) followed by maintenance doses (e.g., 0.5-2 mg/kg/day p.o.), with treatment duration adjusted based on clinical response. Two patients did not respond to corticosteroid therapy, either developing new irAEs or not achieving improvement. Three patients were managed without corticosteroids, with one showing improvement with alternative treatment.
Rechallenge strategies varied, with the majority (66%) initiated due to cancer progression. At the time of rechallenge, 7 patients were under immunosuppressive therapy.
Overall, only 2 patients (13%) experienced recurrence of the same irAE, with an additional 2 patients (13%) developing new irAEs. The median duration of irAE occurrence after rechallenge was consistent with the initial event (69 days; IQR: 54-168 days). Median follow-up after rechallenge was 8 months (range: 6-68 months), with varying responses observed, including complete response, partial response, stability, and cancer-related deaths.
Discussion
In our study, 11 out of 15 patients (73%) who experienced initial severe irAEs did not encounter a recurrence of irAE after ICI rechallenge. Although the initial cohort consisted of 112 patients, the final sample size was reduced to 15 due to stringent inclusion criteria, focusing on patients with comprehensive data on irAEs and their treatment outcomes. This selective approach, while limiting the sample size, ensures a high-quality dataset and enhances the reliability of our findings.
The safety of rechallenge following grade 2 or higher irAEs, particularly involving neurological or cardiac toxicities, remains inadequately explored in the literature (3–5). Pollack et al. demonstrated that among 80 patients who underwent anti-PD-1 rechallenge following irAEs (69% grade 3 or 4) during combination ICIs for metastatic melanoma, 18% experienced recurrence of the initial irAE, 21% developed a different irAE, and 61% did not encounter irAE recurrence (6). Notably, this study did not include initial neurological, cardiac, or muscular irAEs. Similarly, Simonaggio et al. reported on 40 patients undergoing anti-PD-1 rechallenge after irAEs (54% grade 3 or 4) during initial anti-PD-1 therapy for various cancers, with 42.5% experiencing recurrence of the initial irAE, 12.5% developing a different irAE, and 45% not encountering irAE recurrence. Notably, retreatment was avoided for life-threatening toxicities such as cardiac irAEs, neurological adverse events (NAE), and severe myositis (3). Neurological toxicities associated with anti-PD-1 therapy alone or in combination with anti-CTLA-4 agents have been reported with varying incidence rates, ranging from 0.5% to 6.1% (7).
Rechallenge after neurological toxicities remains rare, often considered as a last-line treatment following cancer progression and failed alternative therapies. Persistent neurological symptoms, often graded as 1 or 2, are frequently observed despite high-dose corticosteroids and IVIg therapy, resembling ICI sequelae (8, 9). Park et al. reported on ICI rechallenge in patients with initial myocarditis and NAE, with no flare or toxicity observed in 45.2%, recurrence of the rare irAE in 22.6%, and a different irAE in 37.1% (10). Similarly, Weill et al. described ICI rechallenge in patients with immune-related myositis, with no myositis relapse observed and only one patient experiencing a different irAE (11).
Pharmacovigilance data indicate a low incidence of myocarditis with immune checkpoint inhibitors (ICIs), ranging from 0.27% to 0.9%, with higher rates in combination therapy and anti-PD-1/anti-CTLA-4 therapy. Risk factors such as underlying autoimmune diseases and cardiovascular conditions may increase susceptibility, though differences in incidence between ICI classes are not significant, suggesting a similar toxicity profile among agents (12). The ASCO guidelines advise against ICI therapy rechallenge following grade 1 myocarditis due to its severity, emphasizing individualized decision-making with cardiologists and oncologists, supported by limited literature consisting of a few case reports and series, warranting rigorous monitoring if rechallenge is contemplated (1). The study of Frascaro and al. aimed to review the literature on rechallenging immunotherapy after myocarditis caused by ICI (13). Nine case reports involving 16 patients were identified, showing varied outcomes ranging from successful rechallenge to recurrent myocarditis or cancer progression. In four cases, rechallenging with ICI after myocarditis led to ineffective outcomes, with cardiac-related issues such as myocarditis recurrence or worsening symptoms. Notably, patients initially diagnosed with severe myocarditis did not encounter these challenges, suggesting additional factors influence relapse risk. Additionally, in two cases, patients experienced fatal cancer progression despite rechallenge, emphasizing the critical need for thorough risk-benefit assessment by oncologists and further clinical studies on this complex clinical scenario. These findings underscore the importance of carefully assessing the risk-benefit ratio before considering rechallenge and highlight the need for further research in this area.
In our study, rechallenge following severe neurological toxicities resulted in one recurrence out of five cases, while rechallenge after myocarditis did not lead to recurrence. Notably, recurrence of NAE (aseptic meningitis) prompted rechallenge with combination ICIs and high-dose corticosteroids. Conversely, cases without recurrence of NAE did not involve high-dose corticosteroids during rechallenge, often opting for ICI monotherapy. Data indicated a significantly higher risk of irAE recurrence in patients receiving corticosteroids exceeding 20 mg/day at rechallenge, possibly due to masking of unresolved toxicity. Therefore, complete regression or at least grade 1 toxicity before rechallenge is crucial. Nonetheless, rechallenge after neurological or cardiac toxicity remains a viable option under vigilant monitoring.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
CE: Writing – original draft. MK: Writing – review & editing. MF: Writing – review & editing. EL: Writing – review & editing. CR: Writing – review & editing. JH: Writing – review & editing. BT: Writing – review & editing. FP: Writing – review & editing. MH: Writing – review & editing. MZ: Writing – review & editing. RV: Writing – review & editing. CV: Writing – review & editing. NI: Writing – review & editing. CDo: Writing – review & editing. SM-P: Writing – review & editing. MB-B: Writing – review & editing. AP-L: Writing – review & editing. CDu: Writing – review & editing. GS: Writing – review & editing. FD: Writing – review & editing. EG: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
EG: congress fees and investigator for BMS and MSD. RV: speakers’ bureau for BMS. SM-P: consultant on boards for BMS. AP-L: congress fees for BMS. CDu: Clinical investigation in trials, congress fees and member of boards for BMS, MSD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Postow MA, Callahan MK, Wolchok JD. Immune checkpoint blockade in cancer therapy. J Immunother Cancer. (2015) 3:32. doi: 10.1186/s40425-015-0070-1
2. Haanen J, Obeid M, Spain L, Wang Y, Ernstoff M, Cummings C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. (2022) 33:1217–38. doi: 10.1016/j.annonc.2022.08.271
3. Simonaggio A, Michot JM, Voisin AL, Champiat S, Collins M, Mazieres J, et al. Evaluation of readministration of immune checkpoint inhibitors after immune-related adverse events in patients with cancer. JAMA Oncol. (2019) 5:1310–7. doi: 10.1001/jamaoncol.2019.1028
4. Haanen J, Ernstoff M, Wang Y, Menzies AM, Puzanov I, Grivas P, et al. Rechallenge patients with immune checkpoint inhibitors following severe immune-related adverse events: review of the literature and suggested prophylactic strategy. J Immunother Cancer. (2020) 8:e000604. doi: 10.1136/jitc-2020-000604
5. Guo M, VanderWalde AM, Yu X, Vidal GA, Tian GG. Immune checkpoint inhibitor rechallenge safety and efficacy in stage IV non-small cell lung cancer patients after immune-related adverse events. Clin Lung Cancer. (2022) 23:686–93. doi: 10.1016/j.cllc.2022.04.003
6. Pollack MH, Betof A, Dearden H, Rapisuwon S, Valentine I, Brohl AS, et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma. Ann Oncol. (2018) 29:250–5. doi: 10.1093/annonc/mdx642
7. Johnson DB, Manouchehri A, Haugh AM, Zwerner JP, Powers J, Pirsch JD, et al. Neurologic toxicity associated with immune checkpoint inhibitors: A pharmacovigilance study. J Immunother Cancer. (2019) 7:134. doi: 10.1186/s40425-019-0619-9
8. Moon H, Kim SG, Kim SK, Kim J, Lee SR, Moon YW. A case report of re-challenge of immune checkpoint inhibitors after immune-related neurological adverse events: Review of literature. Med (Baltimore). (2022) 101:e30236. doi: 10.1097/MD.0000000000030236
9. Zimmer L, Goldinger SM, Hofmann L, Loquai C, Ugurel S, Thomas I, et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur J Cancer. (2016) 60:210–25. doi: 10.1016/j.ejca.2016.02.025
10. Park BC, Narayanan S, Gavraldis A, Pappas V, Ricciotti RW, Lee S, et al. Rare immune-related adverse events in patients with melanoma: incidence, spectrum, and clinical presentations. Oncoimmunology. (2021) 12:2188719. doi: 10.1080/2162402X.2021.2188719
11. Weill A, Delyon J, Descamps V, Avouac J, Banu E, Allayous C, et al. Treatment strategies and safety of rechallenge in the setting of immune checkpoint inhibitors-related myositis: a national multicentre study. Rheumatol. (2021) 60:5753–64. doi: 10.1093/rheumatology/keab553
12. Shalata W, Abu-Salman A, Steckbeck R, Jacob BM, Massalha I, Yakobson A. Cardiac toxicity associated with immune checkpoint inhibitors: A systematic review. Cancers. (2021) 13:5218. doi: 10.3390/cancers13205218
Keywords: immune checkpoint inhibitors (ICIs), immune related adverse events (irAEs), rechallenge, neurological immune-related adverse events, myocarditis
Citation: Eldani C, Kostine M, Faure M, Lazaro E, Rigothier C, Hiriart JB, Teulières B, Poullenot F, Haissaguerre M, Zysman M, Veillon R, Vergnenegre C, Issa N, Domblides C, Mary-Prey S, Beylot-Barry M, Pham-Ledard A, Dutriaux C, Sole G, Duval F and Gerard E (2024) Safety of immune checkpoint inhibitor rechallenge after severe immune-related adverse events: a retrospective analysis. Front. Oncol. 14:1403658. doi: 10.3389/fonc.2024.1403658
Received: 19 March 2024; Accepted: 17 June 2024;
Published: 08 July 2024.
Edited by:
Sophia Z. Shalhout, Massachusetts Eye & Ear Infirmary and Harvard Medical School, United StatesReviewed by:
Alexa Meara, The Ohio State University, United StatesShamshad Alam, University at Buffalo, United States
Copyright © 2024 Eldani, Kostine, Faure, Lazaro, Rigothier, Hiriart, Teulières, Poullenot, Haissaguerre, Zysman, Veillon, Vergnenegre, Issa, Domblides, Mary-Prey, Beylot-Barry, Pham-Ledard, Dutriaux, Sole, Duval and Gerard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emilie Gerard, ZW1pbGllLmdlcmFyZEBjaHUtYm9yZGVhdXguZnI=