
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 26 June 2024
Sec. Cancer Immunity and Immunotherapy
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1399171
This article is part of the Research TopicMonoclonal Antibodies and Immune Checkpoint Inhibitors in the treatment of CancerView all 28 articles
 Cecilia Olsson Ladjevardi1,2
Cecilia Olsson Ladjevardi1,2 Anthoula Koliadi1,2Viktoria Rydén1,2Ali Inan El-Naggar3
Anthoula Koliadi1,2Viktoria Rydén1,2Ali Inan El-Naggar3 Evangelos Digkas1,4
Evangelos Digkas1,4 Antonios Valachis3*†Gustav J. Ullenhag1,2†
Antonios Valachis3*†Gustav J. Ullenhag1,2†Introduction: Checkpoint inhibitors (CPI) are widely used in cancer treatment with a potential of causing immune-related adverse events (IRAEs). Several studies have reported a positive correlation between development of IRAEs and improved survival outcome. However, few studies have focused on the potential role of multiple IRAEs on treatment effectiveness. This study aimed at investigating the association between multiple IRAEs and treatment effectiveness in terms of progression-free survival (PFS) and overall survival (OS) in advanced cancer patients.
Methods: We performed a retrospective cohort study at three Swedish centers. All patients (n=600) treated with PD-L1 or PD-1 inhibitor, in monotherapy or in combination for advanced cancer between January 2017 and December 2021 were included. Multiple IRAEs were defined as IRAEs involving more than one organ system either simultaneously or sequentially. Time-depending Cox-regression model to mitigate the risk for immortal time bias (ITB) was applied.
Results: The major tumor types were non-small cell lung cancer (205 patients; 34.2%) and malignant melanoma (196 patients; 32.7%). Of all patients,32.8% developed single IRAE and 16.2% multiple IRAEs. Patients with multiple IRAEs showed significantly improved PFS (Hazard Ratio, HR=0.78 95% Confidence Interval, CI: 0.57–0.98) and OS (HR=0.65 95% CI: 0.44–0.95) compared to patients with single IRAE or no IRAE (HR=0.46 95% CI:0.34–0.62 for PFS vs HR=0.41 95% CI: 0.28-0.60 for OS).
Conclusion: In conclusion, our data supports a stronger association between development of multiple as opposed to single IRAEs and clinical effectiveness in advanced cancer patients treated with CPIs.
Immunotherapy with checkpoint inhibitors (CPI), i.e. anti-PD-1, anti PD-L1 and CTLA-4 antibodies has dramatically improved survival rates in various cancer types during the last decade and they are frequently used in different treatment settings (1–3). Although the introduction of CPIs has improved outcomes in several cancer types, their use cause a considerable risk for immune-related adverse events (IRAEs) which may appear in nearly every organ system and at any point during treatment and even after treatment discontinuation (4). Potential mechanisms resulting in IRAEs include increased T-cell activity against antigens present in both tumors and healthy tissue, increased levels of cytokines, and preexisting autoantibodies, and enhanced complement-mediated inflammation (4). Despite lack of knowledge considering the exact underlying pathophysiological mechanisms, the occurrence of IRAEs reflects activation of the immune system (4, 5). Since the development of IRAEs depends on the mechanism of action of CPIs, it has been assumed that patients developing IRAEs might have a better response to treatment.
The potential association between development of IRAEs and survival outcome is extensively studied. Several studies have shown a positive association between development of IRAEs and clinical benefit for different cancer types including malignant melanoma (MM), non-small cell lung cancer (NSCLC), renal cell carcinoma, urothelial cancer, head and neck cancer, and gastrointestinal cancer (6–10). Immune-related adverse events involving more than one organ, called multiple IRAEs have not been studied to the same extent. The current evidence suggests a better prognosis in patients with multiple IRAEs with a stronger effect magnitude compared to patients with single IRAEs (11–16), even if conflicting results exists (17). However, the current evidence can be questioned due to the high risk for immortal-time bias (ITB) that either has not been considered in some of the studies (14, 15) or it was dealt with in landmark analysis (12, 13, 17) that can also lead to bias compared to the more robust time-dependent Cox model (18). Besides, most of the studies only included patients with NSCLC (11–13, 16, 17), thus impacting the generalizability of study results.
The aim of the present study was to investigate the patterns of multiple IRAE occurrence and their impact on CPI effectiveness in an unselected cohort of patients with advanced cancer using time-dependent Cox models to mitigate the ITB risk.
In this multicenter retrospective cohort study, we identified all patients treated with CPIs (PD-1 or PD-L1 inhibitors) for advanced solid tumors between January 1st 2017 until December 31st 2021 from three regions (Södermland county, Uppsala county, Örebro county) in Sweden. Patients treated with a combination of PD-1 and anti-CTLA4 inhibitor were identified from local electronic prescribing systems for oncological therapy, alongside patients treated with CPIs as part of a clinical trial, and all were included in the analyses. We excluded patients treated with CPIs in a curative setting.
The study was approved by the Swedish Ethical Review Authority (reference number 019–02469 and 020–06801) and the requirement for informed consent was waived. The study has been performed in accordance with the principles of the Declaration of Helsinki.
Data were extracted from electronic medical records (EMR) by researchers (clinical oncologists) in a database with pre-specified variables of interest. The following data were collected: age at diagnosis (as years), sex, comorbidities expressed as Charlson Comorbidity Index, type of cancer, primary treatment at diagnosis, age at diagnosis of advanced cancer, metastatic sites, CPI initiation date, type of CPI, performance status (PS; WHO classification) at CPI initiation, number of previous lines of treatment, best treatment response on CPI, date of disease progression, IRAEs (date, type, grade, outcome), date of death and cause of death. IRAEs were collected before each treatment cycle or as acute events according to clinical practice.
Immune-related adverse events were categorized in grade according to CTCAE 5.0 grading system. If the grade was not included in the EMRs, an approximation of the grade was decided based on the description of adverse events in EMRs and the laboratory findings, whenever feasible.
Multiple IRAEs were defined as IRAEs involving more than one organ system either simultaneously or sequentially.
Progression-free survival (PFS) was defined as the time from initiation of treatment to the occurrence of disease progression (as stated in the EMRs) or death. Overall survival (OS) was defined as the time from treatment initiation to death, irrespective of cause of death.
For descriptive statistics, numbers with percentages and median with range or interquartile range (IQR) were used for categorical and continuous variables, respectively. For bivariate analyses, either chi-square or Kruskal-Wallis test were used for comparisons among the different groups (no IRAE, single IRAE, or multiple IRAEs).
To identify factors associated with occurrence of IRAEs, logistic regression models were applied (no IRAE vs. multiple IRAEs or single IRAE vs. multiple IRAEs) to calculate Odds Ratios (OR) and their corresponding 95% Confidence Intervals (CI) using the following parameters as potential risk factors; age, sex, CCI, type of cancer, performance status, type of CPI, and treatment line.
To investigate the potential impact of IRAEs on time-to-event outcomes (PFS and OS), we performed time-dependent Cox regression models as the main analyses to calculate Hazard Ratios (HR) and their corresponding 95% CIs. Occurrence of the IRAE was considered as a time varying covariate. The rest of the covariates included were age, sex, CCI, performance status, type of CPI, type of cancer, and treatment line. A sensitivity analysis was performed by excluding all patients treated with combined CPI (monotherapy-only cohort). In addition, two subgroup analyses were performed based on cancer type (MM, NSCLC). Within NSCLC cohort, the analyses were stratified by treatment line.
All adjusted analyses were based on complete case approach, namely only cases with complete information for all the covariates included in each analysis were used.
Kaplan-Meier curves were used to visualize the impact of IRAEs on time-to-event outcomes. For the visualization of the distribution of organ systems involved in multiple IRAEs, a chord diagram was constructed.
All reported p-values were two-tailed with a 0.05 cut-off for statistical significance. All analyses were performed using SPSS (IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp).
Baseline characteristics of the study cohort are summarized in Table 1. In total, 600 patients were included in the study cohort with a median age of 66 years (range: 21 – 87). The most common underlying malignant disease was NSCLC (205 patients; 34.2%) followed by MM (196 patients; 32.7%) and renal cell carcinoma (87 patients; 14.6%). Monotherapy with nivolumab was the most used CPI treatment (283 patients; 47.2%) followed by single treatment with pembrolizumab (211 patients; 35.2%) whereas 41 patients (6.8%) were treated with the combination of nivolumab and ipilimumab. Furthermore, 57 patients (9.5%) were treated with atezolizumab, 4 patients (0.7%) with durvalumab and 4 patients (0.7%) with cemiplimab. Median follow-up time for the overall cohort was 15 months (IQR: 6 to 28 months), 23 months (IQR: 13 to 40 months) for patients with PS of 0, 12 months (IQR: 6 to 24 months) for patients with PS of 1, and 7 months (IQR: 1 to 16.5 months) for patients with PS of 2.

Table 1 Characteristics of study cohort based on the occurrence of IRAE.
In total, 97 patients (16.2%) developed multiple IRAEs whereas 197 (32.8%) had a single IRAE during follow-up. Severity, management, and outcome of patients with IRAEs based on number of IRAEs is shown in Table 2. Patients with multiple IRAEs were more likely to develop grade ≥ 2 or grade ≥3 IRAEs that could lead to higher discontinuation rate compared to patients with single IRAEs. Patients with a single IRAE recovered without sequelae to a higher extent than patients with multiple IRAEs (60% vs. 44.3% p=0.027).
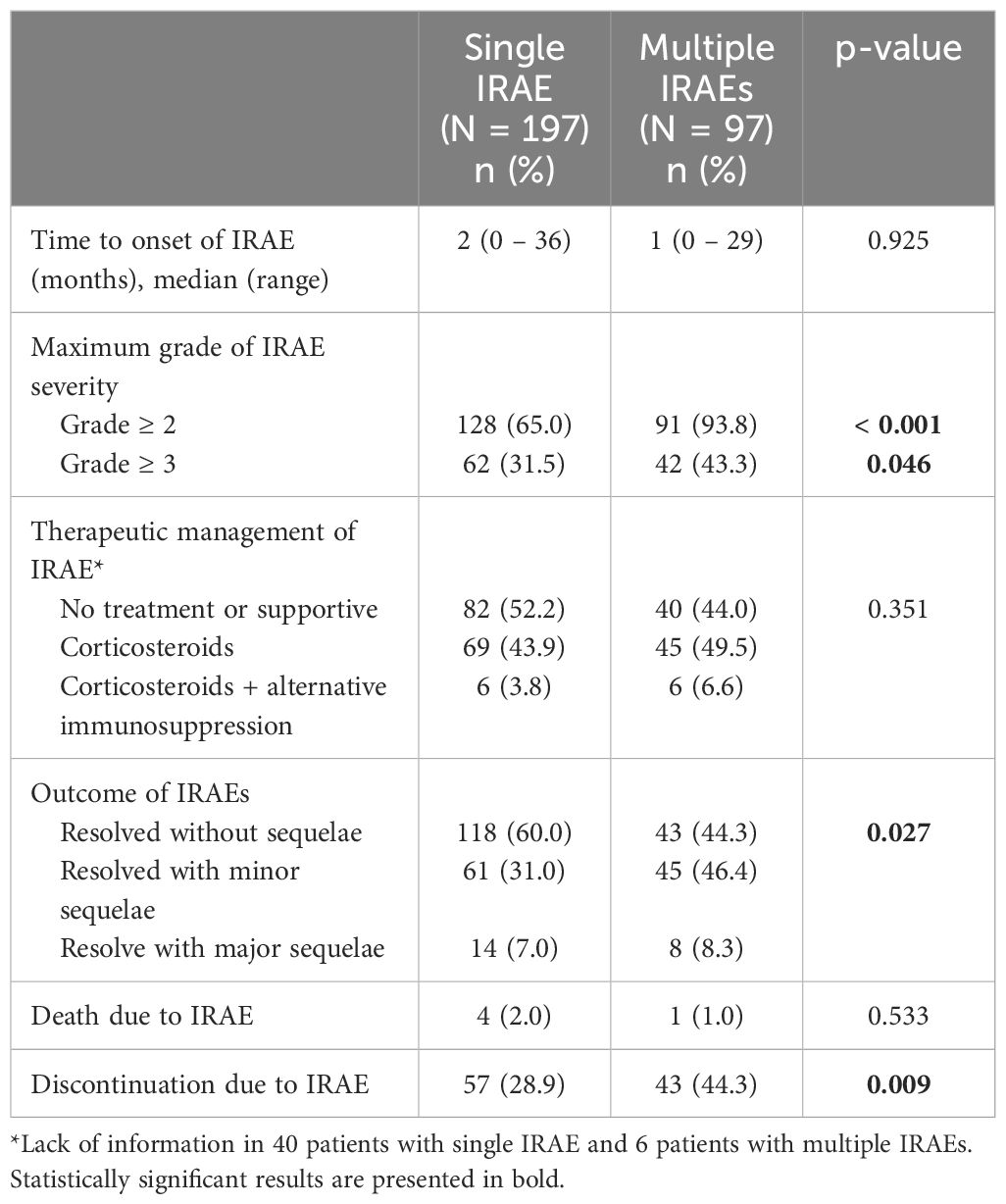
Table 2 Severity, management, and outcome of patients with immune-related adverse events (IRAEs) based on number of IRAEs.
Risk factors for developing multiple IRAEs are shown in Table 3. Patients with PS ≥ 2 were less likely to develop multiple IRAEs (OR: 0.42 95% CI: 1.83–11.79) whereas combined CPI treatment was associated with development of multiple IRAEs (OR: 4.64 95% CI: 1.83–11.79) compared to no IRAE. We could not identify any risk factor associated with multiple IRAEs when compared to patients who developed a single IRAE.
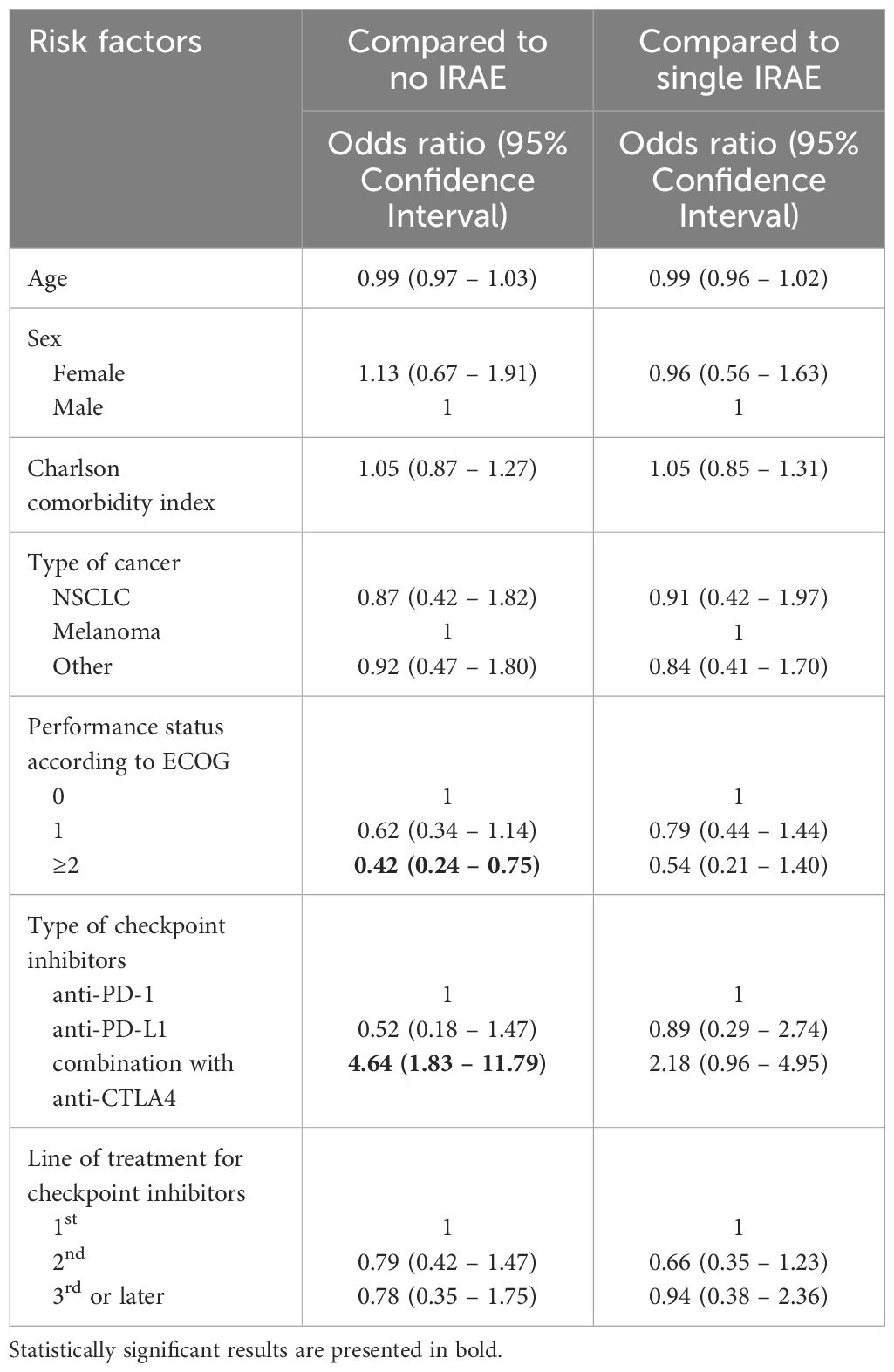
Table 3 Risk factors for developing multiple immune-related adverse events.
Distribution of organ systems involved in multiple IRAEs is demonstrated in Figure 1. The most common dyads of organs with IRAE development within the same patient were skin-gastrointestinal, skin-rheumatologic, skin-endocrine, and rheumatologic-endocrine.
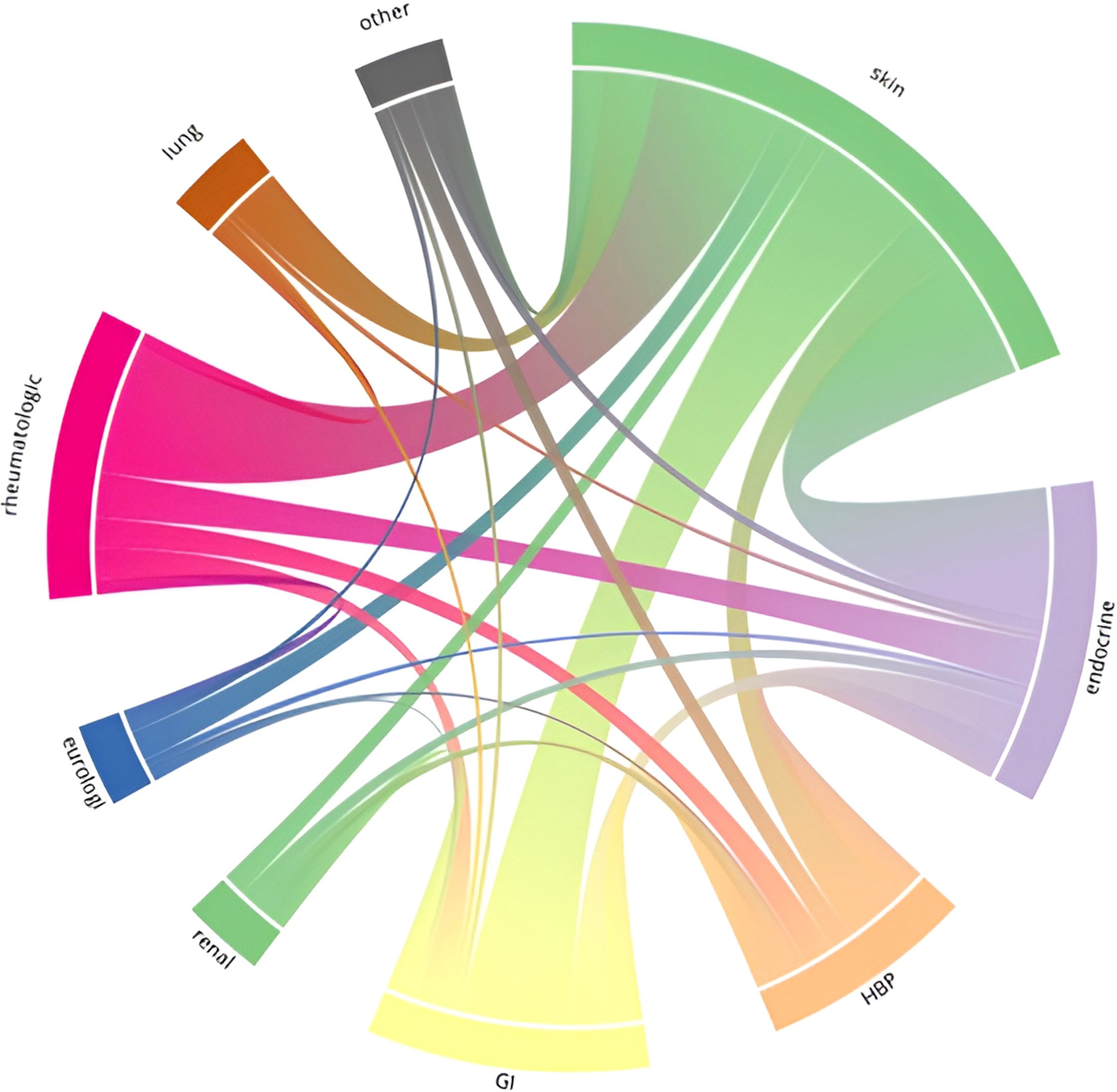
Figure 1 Chord diagram on the distribution of organ systems involved in multiple immune-related adverse events in a cohort of cancer patients with advanced disease treated with checkpoint inhibitors (n=600).
A summary of results from time-dependent Cox analyses regarding the occurrence of IRAE and prognosis in terms of PFS and OS is presented in Table 4.
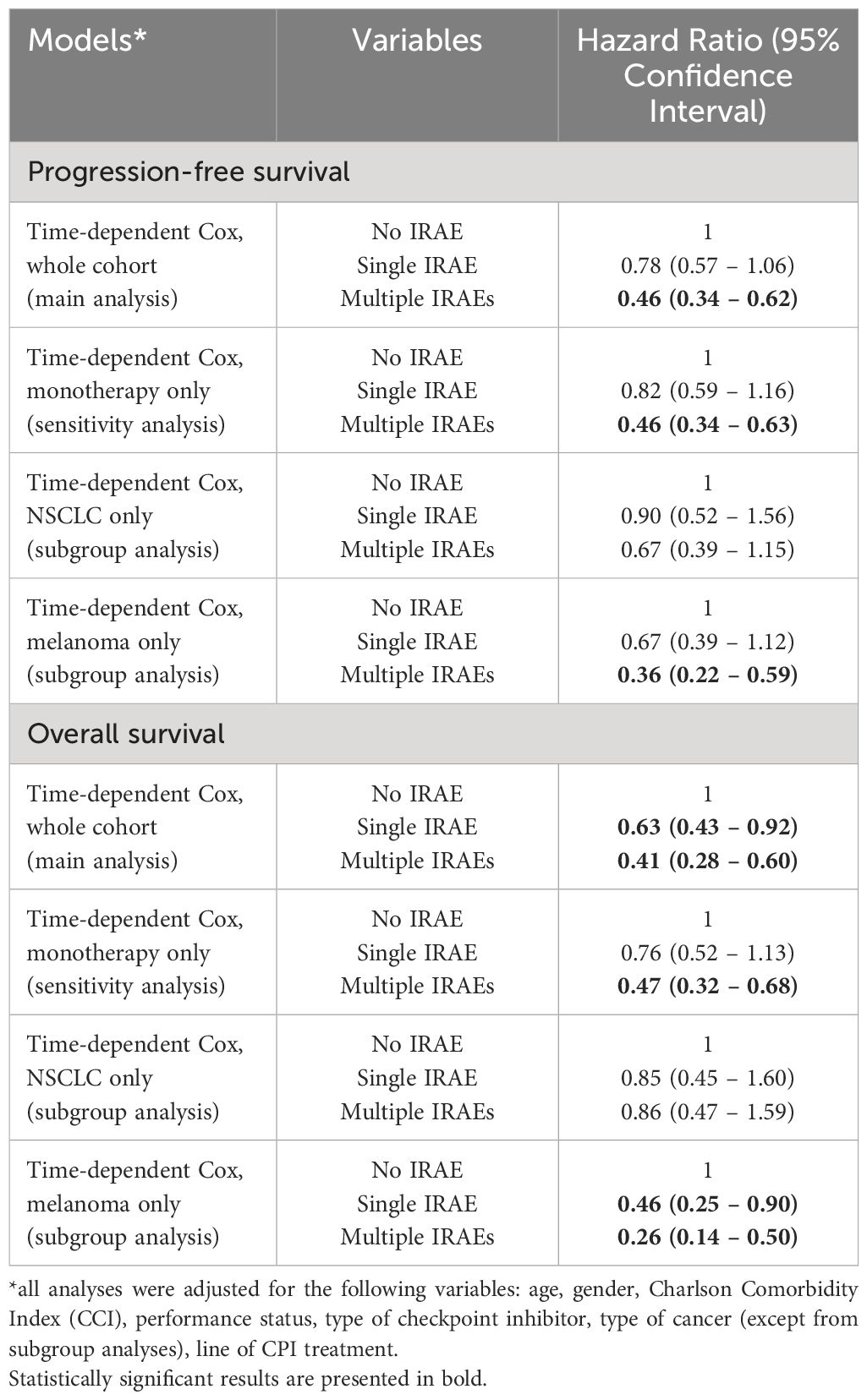
Table 4 Impact of multiple IRAEs on disease prognosis according to time-depending Cox regression models.
The occurrence of multiple IRAEs was associated with statistically significant improvement in PFS (HR: 0.46; 95% CI: 0.34 – 0.63) compared to no IRAE in the whole study cohort as well as in the sensitivity analysis when only patients with CPI as monotherapy were included. An addition analysis with single IRAE as a reference demonstrated statistically significant improvement in PFS (HR: 0.78; 95% CI: 0.57–0.98) for patients developing multiple IRAEs compared to single IRAEs. A graphical visualization of PFS based on the occurrence or absence of IRAEs is shown in Figure 2A. In subgroup analyses, multiple IRAEs were associated with improved PFS in MM cohort but not in NSCLC cohort (Table 4).
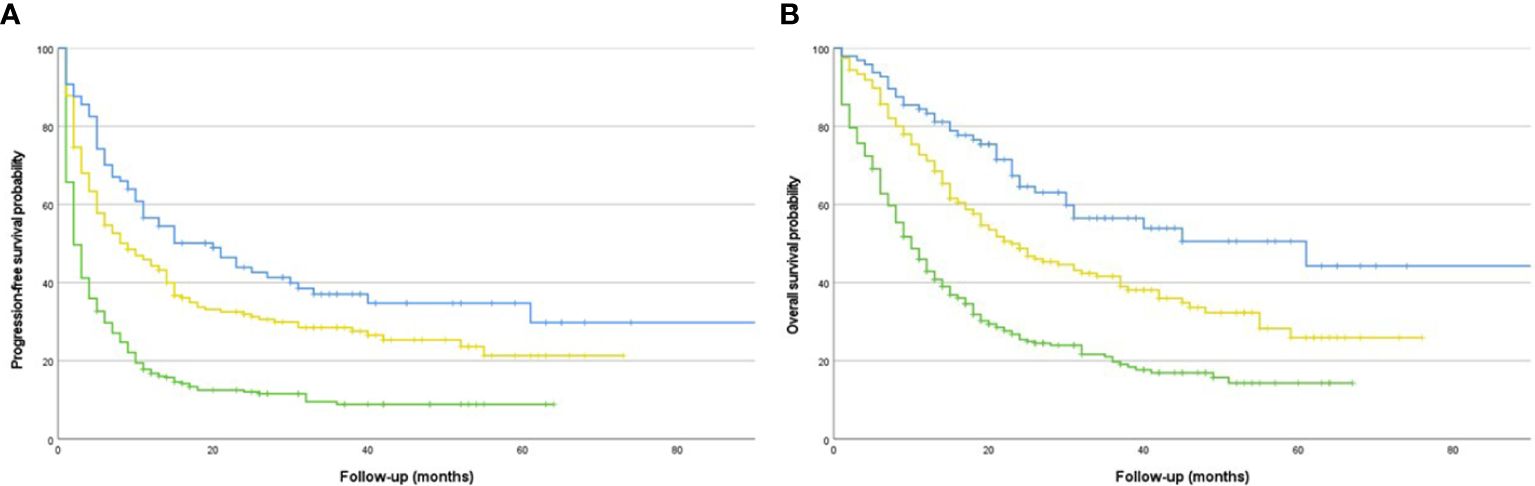
Figure 2 (A) Progression-free survival in a cohort of cancer patients with advanced disease treated with checkpoint inhibitors (n=600) based on the occurrence of immune-related adverse events. Blue line for multiple IRAEs; yellow line for single IRAE; green line for no IRAE. (B) Overall survival in a cohort of cancer patients with advanced disease treated with checkpoint inhibitors (n=600) based on the occurrence of immune-related adverse events. Blue line for multiple IRAEs; yellow line for single IRAE; green line for no IRAE.
In terms of OS, the occurrence of IRAEs resulted in statistically significant improvement in OS both in single IRAE (HR: 0.63; 95% CI: 0.43 - 0.92) and in multiple IRAEs (HR: 0.41; 95% CI: 0.28 - 0.60) cohorts (Figure 2B) compared to no IRAE. The association remained statistically significant in the sensitivity analysis with CPI monotherapy patients only for the occurrence of multiple IRAEs. In subgroup analyses, the occurrence of both single and multiple IRAEs was associated with improved OS in MM cohort whereas no similar association was observed in NSCLC cohort (Table 3). An addition analysis with single IRAE as a reference demonstrated statistically significant improvement in OS (HR: 0.65; 95% CI: 0.44–0.95) for patients developing multiple IRAEs compared to single IRAE.
After applying stratification based on treatment line in NSCLC cohort, a numerically lower HR for both PFS (n=77; HR: 0.51 95% CI: 0.21–1.23) and OS (HR: 0.58 95% CI: 0.20–1.67) for patients with multiple IRAEs when treatment was given as 1st line was observed compared to patients receiving CPI as 2nd (n=137 PFS HR 0.85 95% CI: 0.39–1.87 OS HR 0.84 95% CI: 0.47–1.52) or later treatment line (n=57 PFS HR: 1.77 95% CI: 0.22–13.7 OS HR: 1.12 95% CI: 0.17–10.7).
In all main analyses, we could not reveal any difference in survival outcomes between PD-1 vs. PD-L1 treatment (HR for PFS: 0.84; 95% CI: 0.61 – 1.17; HR for OS: 0.94; 95% CI: 0.65 – 1.36). In an additional time-dependent Cox regression analysis of whether treatment discontinuation due to toxicity was associated with survival outcomes, we could not find a statistically significant association with either PFS (HR 0.78; 95% CI: 0.52 – 1.17) or OS (HR: 0.83; 95% CI: 0.53 – 1.29).
In our study cohort of 600 patients with advanced cancer treated with CPIs, we observed that approximately one-sixth developed multiple IRAEs. The occurrence of multiple IRAEs was associated with better treatment effectiveness as demonstrated by improvements in both PFS and OS with a magnitude of benefit significantly stronger compared to patients with single IRAEs.
Current evidence concerning development of multiple IRAEs for patients treated with CPIs and its impact on treatment effectiveness is scarce. There are only few previous studies (11–13, 16, 17), most of them indicating a stronger association between the development of multiple IRAEs, as opposed to single and survival (11, 12, 16). However, the cohorts in these studies included only patients with NSCLC and, therefore, the generalizability of study results can be questioned. Two earlier studies included patients with various malignant diseases, but smaller cohorts of approximately 200 patients (14, 15) demonstrated results in line with our larger cohort that provides more convincing evidence on this potential association in a broader patient population. A major methodological drawback of previous studies is how the risk for ITB was dealt. Immortal-time bias is a challenge to consider in the association between IRAEs and clinical outcome since patients responding to therapies continue treatment for a longer time and therefore increase their risk of developing IRAEs. To eliminate the risk of ITB in observational studies of survival outcomes established methodology such as landmark analysis, Cox model with time-varying variable or inverse-probability weighed models are routinely used (18–21). These methodological approaches cannot be considered as equal in terms of the validity of results since Cox model with time-varying variable seems to outperform landmark analysis (18). Considering the current evidence on potential association between multiple IRAEs and CPI effectiveness, some studies did not deal with ITB at all (14, 15) whereas others used landmark analysis only (12, 13, 17). We found two previous studies with a proper analysis of ITB reporting positive correlation between multiple IRAEs and outcome. However, both face issues related to generalizability of results to the clinical setting since only patients with NSCLC were included (11, 16) and one of the studies only analyzed patients participating in clinical trials and not in real-world setting (16). Until today, the current study is the first investigating the association between multiple IRAEs and CPI effectiveness in a broader cohort of patients with various malignancies using the preferable Cox regression model with time-dependent covariate as methodological approach for mitigating the ITB.
Subgroup analysis in our cohort showed statistically significantly improved PFS and OS for patients with MM but, as opposed to Shankar et al, not for patients with NSCLC. The lower number of NSCLC patients in our cohort compared to the study by Shankar et al. which only included NSCLC patients (n=205 vs. n=623) may, in part, explain this discrepancy (11). Interestingly, a trend towards improved PFS and OS for patients given CPI as a first line treatment that was diminished in later lines was observed in our cohort of patients with NSCLC highlighting treatment line as a source of heterogeneity among studies that could impact the results. This information was lacking from Shankar et al. and could also contribute to the discrepancy of study results. At the same time, one could argue that the ability of IRAEs to predict CPI effectiveness might depend on cancer type, a notion that is supported by the observations on the substantial differences on tumor immunogenicity among different cancer types (22, 23). In fact, the treatment effect is not equal in patients with different cancer types and differences in adverse effects among different cancer types have also been observed. A systematic review of 48 trials reported higher risk of developing skin and gastrointestinal IRAEs and lower risk of experiencing lung IRAEs for patients with MM compared to those with NSCLC whereas higher incidence of arthralgia and hypothyroidism in MM patients compared to patients with renal cell carcinoma was observed (5). Furthermore, it has been demonstrated that specific types of IRAEs exhibit a more profound correlation to treatment effectiveness and the type of these IRAEs differ across various cancer types. For example, vitiligo has been linked to treatment response in melanoma patients and thyroid dysfunction in NSCLC and renal cell carcinoma patients (24–28).
Checkpoint inhibitor combination therapy with PD-1 and anti-CTLA4 inhibitor is, for subgroups of patients, known to have better clinical efficacy than monotherapy, but the incidence of IRAEs is higher (29, 30). In our study cohort, we confirmed that the combination was a risk factor for development of multiple IRAEs. However, subgroup analyses of monotherapy only showed significantly better PFS and OS for patients developing multiple IRAEs, indicating that the improved outcome for patients with MM is not only due to the well-known better effect of combination therapy. Performance status ≥2 was associated with lower risk for developing multiple IRAEs in our study. A conceivable explanation is that patients with worse PS are more vulnerable in general with higher risk for earlier treatment discontinuation after the first IRAE episode and thus are less likely to develop multiple IRAEs.
Immunosenescent, a term describing impaired function of the immune system that develops with aging, has been supposed to influence the effect of immunotherapies and the development of IRAEs. However, many studies did not find a higher risk for development of IRAEs in older patients (31–34), but conflicting results exist (35). In a previous study from our research group, we found that a simplified frailty score based on PS, age and comorbidity expressed as Charlson Comorbidity Index (CCI) could predict development of all grade and multiple IRAEs, whereas age, CCI or PS did not separately predict increased risk for development of IRAEs (36). Although not supported by our adjusted analyses, another potential explanation of the association between PS and the risk of IRAEs might be more related to the line of treatment rather than the PS per se. In fact, some evidence suggests a negative impact of prior chemotherapy to immune microenvironment (37) that might influence the risk for IRAEs as well. In this equation, PS could serve as a surrogate for later treatment lines rather than as an explanatory parameter for the risk of IRAEs.
In terms of occurrence patterns and outcomes of IRAEs, we found a higher frequency of IRAE grade ≥ 2 and ≥ 3 in patients with multiple IRAEs than in patients with a single IRAE which could explain why a greater proportion of patients with multiple IRAEs than patients with a single IRAE discontinued treatment due to IRAE. At the same time, multiple IRAEs were not associated with higher risk for major sequelae from IRAEs. The organ systems involved in multiple IRAEs in this study consists of combinations of common single IRAEs without identifying any specific pattern. The number of patients within each pattern of distribution was too small and precludes any further analyses for potential associations of specific patterns with prognosis.
Besides from ITB potentially being the main bias in the association between IRAEs and clinical outcome, the present study has some additional limitations associated with its retrospective nature. These include the risk for misclassification bias regarding both IRAE grading but also classification between single and multiple IRAE as well as information bias where EMRs as data sources for identifying IRAEs might not include information on low grade IRAEs. The study is restricted to tree Swedish centers thus limiting its external validity whereas the relatively lower number of patients with tumor types other than melanoma and NSCLC limits the generalizability of the results. Finally, some variables of potential interest that could be associated with both the development of IRAEs and prognosis, as ethnicity, co-medication with immunosuppressive therapy, pre-existing autoimmune disease, were not available and were, therefore, not taken into account for the analyses. For some variables of interest as prior oncological treatment, the information was available, but the subgroups were too small for relevant analyses.
In conclusion, our study results suggest a statistically significant association between development of multiple IRAEs and CPI treatment effectiveness (measured as PFS and OS) that is mainly driven by patients with MM. These results support not discontinuing immunotherapy, even upon multiple but not severe IRAEs to increase the likelihood of treatment benefit. In addition, our findings suggest that multiple IRAEs may constitute a suitable surrogate marker for treatment efficacy that might be used in clinical trials. However, further studies with larger sample size and prospective design to overcome the inherent biases of retrospective studies is essential to further address the potential interplay between the development of IRAEs and treatment outcome.
The raw data are not available due to ethical restrictions but anonymized data might be available upon request.
The study was approved by the Swedish Ethical Review Authority (reference number 019-02469 and 020-06801). The studies were conducted in accordance with the local legislation and institutional requirements. Informed consent was waived from the Swedish Ethical Review Authority since the eligible patients were already treated with checkpoint inhibitors and the current study would not influence their subsequent treatment or prognosis.
CO: Data curation, Writing – original draft. AK: Data curation, Writing – review & editing. VR: Data curation, Writing – review & editing. AI: Data curation, Writing – review & editing. ED: Data curation, Writing – review & editing. AV: Conceptualization, Formal analysis, Methodology, Project administration, Software, Supervision, Writing – original draft. GU: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by grants to GU from The Research Foundation Stiftelsen Onkologiska Klinikens i Uppsala Forskningsfond and Uppsala University Hospital (ALF).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CPI, checkpoint inhibitor; IRAE, immune-related adverse events; EMR, electronic medical records; ITB, immortal-time bias.
1. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. (2019) 381:1535–46. doi: 10.1056/NEJMoa1910836
2. Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson VG, Dalle S, et al. Longer follow-up confirms recurrence-free survival benefit of adjuvant pembrolizumab in high-risk stage III melanoma: Updated results from the EORTC 1325-MG/KEYNOTE-054 trial. J Clin Oncol. (2020) 38:3925–36. doi: 10.1200/JCO.20.02110
3. Hargadon KM, Johnson CE, Williams CJ. Immune checkpoint blockade therapy for cancer: An overview of FDA-approved immune checkpoint inhibitors. Int Immunopharmacol. (2018) 62:29–39. doi: 10.1016/j.intimp.2018.06.001
4. Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. (2018) 378:158–68. doi: 10.1056/NEJMra1703481
5. Khoja L, Day D, Wei-Wu Chen T, Siu LL, Hansen AR. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. (2017) 28:2377–85. doi: 10.1093/annonc/mdx286
6. Hussaini S, Chehade R, Boldt RG, Raphael J, Blanchette P, Maleki Vareki S, et al. Association between immune-related side effects and efficacy and benefit of immune checkpoint inhibitors - A systematic review and meta-analysis. Cancer Treat Rev. (2021) 92:102134. doi: 10.1016/j.ctrv.2020.102134
7. Petrelli F, Grizzi G, Ghidini M, Ghidini A, Ratti M, Panni S, et al. Immune-related adverse events and survival in solid tumors treated with immune checkpoint inhibitors: A systematic review and meta-analysis. J Immunother. (2020) 43:1–7. doi: 10.1097/CJI.0000000000000300
8. Eggermont AMM, Kicinski M, Blank CU, Mandala M, Long GV, Atkinson V, et al. Association between immune-related adverse events and recurrence-free survival among patients with stage III melanoma randomized to receive pembrolizumab or placebo: A secondary analysis of a randomized clinical trial. JAMA Oncol. (2020) 6:519–27. doi: 10.1001/jamaoncol.2019.5570
9. Maher VE, Fernandes LL, Weinstock C, Tang S, Agarwal S, Brave M, et al. Analysis of the association between adverse events and outcome in patients receiving a programmed death protein 1 or programmed death ligand 1 antibody. J Clin Oncol. (2019) 37:2730–7. doi: 10.1200/JCO.19.00318
10. Cortellini A, Buti S, Agostinelli V, Bersanelli M. A systematic review on the emerging association between the occurrence of immune-related adverse events and clinical outcomes with checkpoint inhibitors in advanced cancer patients. Semin Oncol. (2019) 46:362–71. doi: 10.1053/j.seminoncol.2019.10.003
11. Shankar B, Zhang J, Naqash AR, Forde PM, Feliciano JL, Marrone KA, et al. Multisystem immune-related adverse events associated with immune checkpoint inhibitors for treatment of non-small cell lung cancer. JAMA Oncol. (2020) 6:1952–6. doi: 10.1001/jamaoncol.2020.5012
12. Cortellini A, Friedlaender A, Banna GL, Porzio G, Bersanelli M, Cappuzzo F, et al. Immune-related adverse events of pembrolizumab in a large real-world cohort of patients with NSCLC with a PD-L1 expression ≥ 50% and their relationship with clinical outcomes. Clin Lung Cancer. (2020) 21:498–508.e2. doi: 10.1016/j.cllc.2020.06.010
13. Ricciuti B, Genova C, De Giglio A, Bassanelli M, Dal Bello MG, Metro G, et al. Impact of immune-related adverse events on survival in patients with advanced non-small cell lung cancer treated with nivolumab: long-term outcomes from a multi-institutional analysis. J Cancer Res Clin Oncol. (2019) 145:479–85. doi: 10.1007/s00432-018-2805-3
14. Shimozaki K, Sukawa Y, Beppu N, Kurihara I, Suzuki S, Mizuno R, et al. Multiple immune-related adverse events and anti-tumor efficacy: Real-world data on various solid tumors. Cancer Manag Res. (2020) 12:4585–93. doi: 10.2147/CMAR.S247554
15. Hata H, Matsumura C, Chisaki Y, Nishioka K, Tokuda M, Miyagi K, et al. A retrospective cohort study of multiple immune-related adverse events and clinical outcomes among patients with cancer receiving immune checkpoint inhibitors. Cancer Control. (2022) 29:10732748221130576. doi: 10.1177/10732748221130576
16. Kichenadasse G, Miners JO, Mangoni AA, Rowland A, Hopkins AM, Sorich MJ. Multiorgan immune-related adverse events during treatment with atezolizumab. J Natl Compr Canc Netw. (2020) 18:1191–9. doi: 10.6004/jnccn.2020.7567
17. Cortellini A, Chiari R, Ricciuti B, Metro G, Perrone F, Tiseo M, et al. Correlations between the immune-related adverse events spectrum and efficacy of anti-PD1 immunotherapy in NSCLC patients. Clin Lung Cancer. (2019) 20:237–247.e1. doi: 10.1016/j.cllc.2019.02.006
18. Jones M, Fowler R. Immortal time bias in observational studies of time-to-event outcomes. J Crit Care. (2016) 36:195–9. doi: 10.1016/j.jcrc.2016.07.017
19. Cho IS, Chae YR, Kim JH, Yoo HR, Jang SY, Kim GR, et al. Statistical methods for elimination of guarantee-time bias in cohort studies: a simulation study. BMC Med Res Methodol. (2017) 17:126. doi: 10.1186/s12874-017-0405-6
20. Putter H, van Houwelingen HC. Understanding landmarking and its relation with time-dependent cox regression. Stat Biosci. (2017) 9:489–503. doi: 10.1007/s12561-016-9157-9
21. Giobbie-Hurder A, Gelber RD, Regan MM. Challenges of guarantee-time bias. J Clin Oncol. (2013) 31:2963–9. doi: 10.1200/JCO.2013.49.5283
22. Riaz N, Morris L, Havel JJ, Makarov V, Desrichard A, Chan TA. The role of neoantigens in response to immune checkpoint blockade. Int Immunol. (2016) 28:411–9. doi: 10.1093/intimm/dxw019
23. Haibe Y, El Husseini Z, El Sayed R, Shamseddine A. Resisting resistance to immune checkpoint therapy: A systematic review. Int J Mol Sci. (2020) 21:6176. doi: 10.3390/ijms21176176
24. Verkhovskaia S, Di Pietro FR, Mastroeni S, Carbone ML, Abeni D, Morese R, et al. Vitiligo-like leukoderma as an indicator of clinical response to immune checkpoint inhibitors in late-stage melanoma patients. J Cancer Res Clin Oncol. (2022) 148:2529–38. doi: 10.1007/s00432-021-03811-3
25. Teulings HE, Limpens J, Jansen SN, Zwinderman AH, Reitsma JB, Spuls PI, et al. Vitiligo-like depigmentation in patients with stage III-IV melanoma receiving immunotherapy and its association with survival: a systematic review and meta-analysis. J Clin Oncol. (2015) 33:773–81. doi: 10.1200/JCO.2014.57.4756
26. Thuillier P, Joly C, Alavi Z, Crouzeix G, Descourt R, Quere G, et al. Thyroid dysfunction induced by immune checkpoint inhibitors is associated with a better progression-free survival and overall survival in non-small cell lung cancer: an original cohort study. Cancer Immunol Immunother. (2021) 70:2023–33. doi: 10.1007/s00262-020-02802-6
27. Kim HI, Kim M, Lee SH, Park SY, Kim YN, Kim H, et al. Development of thyroid dysfunction is associated with clinical response to PD-1 blockade treatment in patients with advanced non-small cell lung cancer. Oncoimmunology. (2017) 7:e1375642. doi: 10.1080/2162402X.2017.1375642
28. Martini DJ, Goyal S, Liu Y, Evans ST, Olsen TA, Case K, et al. Immune-related adverse events as clinical biomarkers in patients with metastatic renal cell carcinoma treated with immune checkpoint inhibitors. Oncologist. (2021) 26:e1742–50. doi: 10.1002/onco.13868
29. Da L, Teng Y, Wang N, Zaguirre K, Liu Y, Qi Y, et al. Organ-specific immune-related adverse events associated with immune checkpoint inhibitor monotherapy versus combination therapy in cancer: A meta-analysis of randomized controlled trials. Front Pharmacol. (2019) 10:1671. doi: 10.3389/fphar.2019.01671
30. Park R, Lopes L, Cristancho CR, Riano IM, Saeed A. Treatment-related adverse events of combination immune checkpoint inhibitors: systematic review and meta-analysis. Front Oncol. (2020) 10:258. doi: 10.3389/fonc.2020.00258
31. Bastiaannet E, Battisti N, Loh KP, de Glas N, Soto-Perez-de-Celis E, Baldini C, et al. Immunotherapy and targeted therapies in older patients with advanced melanoma; Young International Society of Geriatric Oncology review paper. J Geriatr Oncol. (2019) 10:389–97. doi: 10.1016/j.jgo.2018.06.009
32. Kalinich M, Murphy W, Wongvibulsin S, Pahalyants V, Yu KH, Lu C, et al. Prediction of severe immune-related adverse events requiring hospital admission in patients on immune checkpoint inhibitors: study of a population level insurance claims database from the USA. J Immunother Cancer. (2021) 9:e001935. doi: 10.1136/jitc-2020-001935
33. Ksienski D, Wai ES, Croteau NS, Freeman AT, Chan A, Fiorino L, et al. Association of age with differences in immune related adverse events and survival of patients with advanced nonsmall cell lung cancer receiving pembrolizumab or nivolumab. J Geriatr Oncol. (2020) 11:807–13. doi: 10.1016/j.jgo.2020.01.006
34. Basak EA, Vermeer NS, de Joode K, Hurkmans DP, Velthuis DEM, Oomen-de Hoop E, et al. Associations between patient and disease characteristics and severe adverse events during immune checkpoint inhibitor treatment: An observational study. Eur J Cancer. (2022) 174:113–20. doi: 10.1016/j.ejca.2022.07.015
35. Baldini C, Martin Romano P, Voisin AL, Danlos FX, Champiat S, Laghouati S, et al. Impact of aging on immune-related adverse events generated by anti-programmed death (ligand)PD-(L)1 therapies. Eur J Cancer. (2020) 129:71–9. doi: 10.1016/j.ejca.2020.01.013
36. Olsson Ladjevardi C, Koliadi A, Rydén V, Inan El-Naggar A, Digkas E, Valachis A, et al. Predicting immune-related adverse events using a simplified frailty score in cancer patients treated with checkpoint inhibitors: A retrospective cohort study. Cancer Med. (2023) 12:13217–24. doi: 10.1002/cam4.6013
37. Amrein MA, Bührer ED, Amrein ML, Li Q, Rothschild S, Riether C, et al. Chemotherapy negatively impacts the tumor immune microenvironment in NSCLC: an analysis of pre- and post-treatment biopsies in the multi-center SAKK19/09 study. Cancer Immunol Immunother. (2021) 70:405–15. doi: 10.1007/s00262-020-02688-4
Keywords: checkpoint inhibitors, multiple immune-related adverse events, immortal time bias, advanced cancer, cohort study
Citation: Olsson Ladjevardi C, Koliadi A, Rydén V, El-Naggar AI, Digkas E, Valachis A and Ullenhag GJ (2024) Multiple immune-related adverse events secondary to checkpoint inhibitor therapy in patients with advanced cancer: association with treatment effectiveness. Front. Oncol. 14:1399171. doi: 10.3389/fonc.2024.1399171
Received: 11 March 2024; Accepted: 07 June 2024;
Published: 26 June 2024.
Edited by:
Cory L. Brooks, California State University, Fresno, United StatesReviewed by:
Oliver Bechter, University Hospitals Leuven, BelgiumCopyright © 2024 Olsson Ladjevardi, Koliadi, Rydén, El-Naggar, Digkas, Valachis and Ullenhag. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonios Valachis, YW50b25pb3MudmFsYWNoaXNAb3J1LnNl
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.