 Tatiana Galicia-Carmona1,2
Tatiana Galicia-Carmona1,2 Eder Alexandro Arango-Bravo1,2
Eder Alexandro Arango-Bravo1,2 Jaime A. Coronel-Martínez1,2
Jaime A. Coronel-Martínez1,2 Lucely Cetina-Pérez1,2
Lucely Cetina-Pérez1,2 Elva G. Vanoye-Carlo3
Elva G. Vanoye-Carlo3 Ricardo Villalobos-Valencia4
Ricardo Villalobos-Valencia4 José A. García-Pacheco5
José A. García-Pacheco5 Patricia Cortés-Esteban6*
Patricia Cortés-Esteban6*- 1Department of Clinical Research, Instituto Nacional de Cancerología (INCan), Mexico City, Mexico
- 2Department of Medical Oncology, Instituto Nacional de Cancerología (INCan), Mexico City, Mexico
- 3Department of Surgical Oncology, Hospital Regional de Alta Especialidad de la Península de Yucatán, Yucatán, Mexico
- 4Department of Medical Oncology, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social, Mexico City, Mexico
- 5NSR III Researcher assistant, Consejo Nacional de Humanidades, Ciencias y Tecnologías(CONACYT), Mexico City, Mexico
- 6Department of Medical Oncology, Centro Médico Nacional 20 de Noviembre, Mexico City, Mexico
Cervical cancer constitutes a significant health burden for women worldwide despite being preventable by vaccination and screening. Advanced stages of the disease are associated with a poor prognosis, and treatment approaches have seen little change over several decades, resulting in an overall survival rate of no more than 17 months. Additionally, there are limited options for second-line treatment. The urgent need for innovative and effective therapies to improve the outlook for this group of patients, along with an enhanced understanding of the interactions between the disease and the host’s immune system, has propelled immunotherapy into a rapidly advancing field with notable achievements. Among various immunotherapeutic approaches, immune checkpoint inhibitors emerge as the most advanced treatment option. Clinical trials assessing these inhibitors as single agents or in combination with chemotherapy show promising results. As immunotherapy begins to redefine standards of care for metastatic, recurrent, or persistent cervical cancer, this review addresses recent advances and current recommendations for its management in both first and second-line treatment. The goal is to provide insights into the evolving landscape of cervical cancer treatment, specifically focusing on immunotherapeutic interventions.
Introduction
Despite being a completely preventable disease, in developing countries, cervical cancer (CC) is a major contributor to cancer-related deaths in women. For a long time, cisplatin as monotherapy or in combination represented the standard treatment for this patient group, with an overall survival not exceeding 13 months. In recent years, the advent of targeted therapies such as immunotherapy has significantly improved the prognosis for these patients.
Immunity and cervical cancer
Human Papillomavirus (HPV) is a necessary but not sufficient etiological factor for developing cervical cancer. Infected basal epithelial cells hosting HPV express only early genes. However, HPV integration into the host genome leads to the expression of oncogenes E6 and E7 (1, 2). Integration of the HPV genome is a critical step in the development of HPV-associated cancers. This integration event preferentially occurs at fragile sites within the human DNA, regions characterized by increased susceptibility to breakage and rearrangement. The subsequent expression of viral oncogenes E6 and E7 is not only essential for the initiation and progression of premalignant lesions but also actively promotes genomic instability, further contributing to cellular transformation and malignant progression (3).
HPV-infected cells can evade immunosurveillance by inhibiting acute inflammation and immunological recognition. This viral and inflammatory cancer environment has been shown to be responsible for inducing PD-L1 expression (4). There is evidence that PD-L1 expression plays a significant role in creating an “immune privileged” site for initiating and persisting HPV infection by downregulating T-cell activity and generating adaptive immune resistance (5, 6). High-level PD-L1 expression is rare in healthy cervical tissue, but is increased in T cells and tumoral cells in 35 to 96% of cervical cancers (7).
Immunological escape is associated with local negative regulation as well as evasion of immune system detection, including increased regulatory T cells (Treg), loss of major histocompatibility complex (MHC) antigen presentation, chronic inflammation, and regulation of immune checkpoint molecules (8). Targeting tumor-specific antigens remains a cornerstone of cancer immunotherapy. However, the immunosuppressive tumor microenvironment presents a significant challenge, often hindering the efficacy of such targeted approaches. Therefore, therapeutic strategies aimed at reversing this immunosuppression within the tumor microenvironment are crucial for enhancing the efficacy of cancer immunotherapy. This can involve approaches such as inhibiting checkpoint molecules, depleting regulatory T cells, or promoting the activity of immunostimulatory cells and cytokines. Therapeutic interventions, such as immune checkpoint blockade targeting molecules like PD-1/PD-L1 and CTLA-4, aim to overcome this challenge; they are not specific for HPV antigens, and if successful, they can be efficient in the majority of cervical cancer cases, regardless of the associated HPV type (9). Tumor cells often exploit immune checkpoint pathways as a mechanism for immune evasion. Therapeutic interventions targeting immune checkpoints, such as PD-1/PD-L1 blockade, can restore T cell function and promote tumor cell killing. By preventing the inhibitory signals mediated by these checkpoints, T cell proliferation and cytotoxic activity against cancer cells are enhanced within the tumor microenvironment.
Immune checkpoint inhibitors
The application of immunotherapy in CC treatment is grounded in several key molecular features observed in these tumors. Elevated Tumor Mutational Burden, Microsatellite Instability, high PD-L1 expression, and elevated Tumor Inflammatory State, suggest an environment conducive to successful immunotherapy intervention. Therefore, the convergence of these molecular features in CC provides a strong rationale for employing immunotherapy as a treatment strategy (10).
Various tumors, including CC, express PD-L1, an immune checkpoint molecule mediating tumor cell escape from immune system-mediated destruction (11). PD-L1 expression by tumors enables them to evade destruction by CD8+ T cells. PD-1 is a crucial immune checkpoint molecule involved in maintaining self-tolerance and modulating the immune response. During an inflammatory response to infection, PD-1 expression on activated effector T cells helps prevent autoimmunity by attenuating T cell activation. However, within the tumor microenvironment, PD-1 can contribute to immune resistance. PD-1 is expressed on various immune cells, including activated T cells and regulatory T cells (Tregs). Notably, PD-1 expression on Tregs, coupled with ligand engagement, enhances their proliferation and amplifies their immunosuppressive function. Furthermore, PD-1 expression extends beyond T lymphocytes to include B cells and other immune subsets (9).
PD-L1 and PD-L2 serve as the two ligands for PD-1. Binding of either ligand to PD-1 triggers a co-inhibitory signal within activated T cells, leading to suppression of their effector functions. In the context of cancer, PD-1 is frequently upregulated on tumor-infiltrating lymphocytes (TILs) across diverse tumor types (12). This, coupled with the common overexpression of PD-L1 on tumor cells, facilitates immune evasion by inhibiting anti-tumor T cell responses (13, 14). Further, PD-L1 expression is an independent prognostic factor for poor outcome, irrespective of established clinicopathological features, including stage, tumor size, depth of invasion, lymphovascular invasion, and lymph node involvement (15).
First-line treatment and recent advances
Advanced, persistent, or recurrent CC has a 5-year survival rate of 17%. Thus, median progression-free survival (PFS) (2 to 5 months) and overall survival (OS) (5 to 16 months) is low for individuals who can’t undergo surgery or radiotherapy (16).
For many years, platinum-based chemotherapy represented the standard treatment for this patient group, with response rates of 13% and 36% for monotherapy or combination therapy, respectively (17–19). The GOG 204 study, comparing four cisplatin combinations (cisplatin/paclitaxel, cisplatin/topotecan, cisplatin/gemcitabine, and cisplatin/vinorelbine), found no difference in overall survival. While not statistically significant, a trend towards improved efficacy was observed in the cisplatin/paclitaxel group compared to the other treatment combinations. This trend was evidenced by numerically higher response rates, as well as longer progression-free survival (PFS) and overall survival (OS) (12.9 months vs. 10 months), which have established it as the preferred regimen since 2009 (17). Subsequently, the phase III JCOG0505 non-inferiority study comparing carboplatin/paclitaxel vs. cisplatin/paclitaxel demonstrated the non-inferiority of the carboplatin/paclitaxel regimen in terms of median overall survival (17.5 months vs. 18.3 months, p=0.032), with a different toxicity profile but consolidating platinum and taxane chemotherapy as the first-line treatment choice (19).
In 2014, the first targeted therapy with a benefit in metastatic, recurrent or persistent cervical cancer was established with the GOG 240 study. Bevacizumab, a monoclonal antibody, acts as an antiangiogenic agent by neutralizing vascular endothelial growth factor (VEGF), inducing tumor vascular regression, normalizing residual vasculature, and inhibiting neovascularization and, therefore, tumor growth. The combination of bevacizumab with platinum-based chemotherapy showed a 4-month overall survival advantage compared to chemotherapy alone (17 months vs. 13 months) and a response rate of 48% vs. 36% (16).
In 2021, the KEYNOTE-826 study approved the first-line immunotherapy for palliative treatment in CC. Pembrolizumab, a monoclonal antibody, binds to the PD-1 receptor, preventing its interaction with PD-L1 and PD-L2. This interference enhances the anti-tumor immune response of T cells. This phase 3, double-blind clinical trial randomized patients with persistent, recurrent, or metastatic uterine CC to receive pembrolizumab (200 mg) or placebo every 3 weeks for up to 35 cycles plus platinum-based chemotherapy and, at the investigator’s discretion, bevacizumab. In 548 patients exhibiting PD-L1 expression levels of combined positive score (CPS) ≥1%, treatment with pembrolizumab demonstrated a statistically significant improvement in both progression-free survival (PFS) and overall survival (OS) when compared to the placebo group. Specifically, the median PFS for the pembrolizumab group was 10.4 months, exceeding the 8.2 months observed in the placebo group. This difference translated to a hazard ratio (HR) of 0.62 for disease progression or death (95% confidence interval [CI], 0.50 to 0.77; p <0.001). Furthermore, the 24-month OS rate was notably higher in the pembrolizumab group, reaching 53.0% compared to 41.7% in the placebo group (HR for death, 0.64; 95% CI, 0.50 to 0.81; p <0.001). Regarding safety, the most frequently observed grade 3-5 adverse events were anemia (30.3% in the pembrolizumab group and 26.9% in the placebo group) and neutropenia (12.4% and 9.7%, respectively) (20). In 2023, the results of the study were presented, with a median follow-up of 39.1 months. In the PD-L1 ≥1% population, the administration of pembrolizumab demonstrated a notable improvement in median overall survival compared to the chemotherapy-placebo group. Specifically, the pembrolizumab group achieved a median overall survival of 28.6 months, whereas the control group reached 16.5 months (HR for death: 0.60; 95% CI: 0.49 to 0.74). This survival benefit was further accentuated in the subgroup analysis of patients with PD-L1 expression >10%. In this cohort, the median overall survival for the pembrolizumab arm was 29.6 months versus 17.4 months in the control arm (HR: 0.58; 95% CI: 0.44 to 0.78). Pembrolizumab also exhibited superiority in PFS compared to the control regimen. This was observed in both the PD-L1 CPS ≥1% population (HR: 0.58; p-value <0.0001) and the PD-L1 CPS ≥10% population (HR: 0.52; p-value <0.0001). Regarding adverse events, the incidence of grade 3 or higher events was 82.4% in the pembrolizumab group and 75.4% in the placebo group.
Recently, an exploratory subgroup analysis of this study demonstrated, in those patients with CPS ≥1%, a benefit in OS in favor of the pembrolizumab groups across all subgroups. The median OS was not reached (95% CI, 24.4-NR) in the pembrolizumab group, compared to 25.0 months (95% CI, 16.3-NR) in the placebo group among those who received bevacizumab (HR, 0.62; 95% CI, 0.45-0.87), and 17.1 months (95% CI, 14.9-20.0) in the pembrolizumab group versus 11.9 months (95% CI, 9.7-14.5) in the placebo group (HR, 0.67; 95% CI, 0.47-0.96). Regarding PFS, the HR for progression or death was significantly lower in the pembrolizumab groups compared to the placebo groups in both bevacizumab [HR of 0.61 (95% CI, 0.46-0.8)] and non-bevacizumab [HR of 0.66 (95% CI, 0.47-0.92)] subgroups. As for the use of platinum, it was shown that the median OS was 24.4 months (95% CI, 18.7-NR) in the pembrolizumab group versus 15.7 months (95% CI, 13.2-18.6) in the placebo group among those who received carboplatin (HR, 0.65; 95% CI, 0.50-0.85), and was not reached (95% CI, 22.3-NR) in the pembrolizumab group versus 24.7 months (95% CI, 16.0-NR) in the placebo group among those who received cisplatin (HR, 0.53; 95% CI, 0.27-10.04), while the PFS was 0.68 (95% CI, 0.53-0.85) in the carboplatin subgroup and 0.39 (95% CI, 0.22-0.68) in the cisplatin subgroup in CPS ≥1% (21).
Second-line treatment options
Following initial treatment, disease progression historically presented significant challenges due to the scarcity of effective therapeutic interventions. For an extended period, a standardized second-line chemotherapy regimen remained elusive. Commonly employed chemotherapeutic agents, including taxanes, topotecan, and gemcitabine, with response rates of 13.2%, with a median PFS of 3.2 months, and a median OS of 9.3 months (22).
Until 2018, there were no promising treatments in the palliative second-line setting for patients with CC. The KEYNOTE-158 study in 2018 showed promising results with pembrolizumab. In this phase 3, double-blind study, participants were administered pembrolizumab at a dose of 200 mg every three weeks for two years, or until disease progression, unacceptable toxicity, or withdrawal by either the patient or physician. A total of 98 patients were treated, with 83.7% having PD-L1 positivity. After a median follow-up duration of 10.2 months (range: 0.6 - 22.7 months), the observed objective response rate (ORR) was 12.2% (95% confidence interval [CI]: 6.5% - 20.4%). This included three complete responses and nine partial responses, all occurring within the PD-L1-positive patient subgroup. Consequently, the ORR for PD-L1-positive patients was 14.6% (95% CI: 7.8% - 24.2%). Notably, 14.3% (95% CI: 7.4% - 24.1%) of responders within this subgroup had previously received one or more lines of chemotherapy in the recurrent or metastatic setting. Treatment-related adverse events were observed in 65.3% of the study population. The most frequently reported adverse events included hypothyroidism (10.2%), decreased appetite (9.2%), and fatigue (9.2%). Grade 3-4 treatment-related adverse events were documented in 12.2% of patients (23).
Tisotumab vedotin is a monoclonal antibody attached to a chemotherapy agent called monomethyl auristatin E (MMAE). The innovaTV 204/GOG-3023/ENGOT-cx6 study, a phase II, multicenter, open-label, single-arm study conducted in 35 centers in Europe and the United States, included 102 patients with recurrent or metastatic CC. The study enrolled patients with cervical cancer who experienced disease progression during or after bevacizumab-based chemotherapy and had undergone no more than two prior systemic treatment regimens. Participants received tisotumab vedotin at a dose of 2.0 mg/kg (maximum 200 mg) intravenously every 3 weeks until disease progression or the onset of intolerable adverse effects. The analysis included 101 patients who received at least one dose of the drug, with a median follow-up duration of 10.0 months (range: 6.1 to 13.0 months). The confirmed ORR was 24% (95% confidence interval [CI]: 16-33%), with 7% complete responses and 17% partial responses. The most frequently observed treatment-related adverse events (TRAEs) were alopecia (38%), epistaxis (30%), nausea (27%), conjunctivitis (26%), fatigue (26%), and dry eye (23%). Grade ≥3 TRAEs occurred in 28% of patients, notably including neutropenia (3%), fatigue (2%), ulcerative keratitis (2%), and various peripheral neuropathies (sensory, motor, sensorimotor, and general peripheral neuropathy). Serious TRAEs were reported in 13% of patients, with sensory-motor peripheral neuropathy (2%) and pyrexia (2%) being the most common (24).
In 2022, another treatment showed promising results in this patient group. The EMPOWER-Cervical 1 study, a phase 3 trial, in patients who had disease progression after first-line platinum-based chemotherapy, regardless of their PD-L1 status. Cemiplimab, a monoclonal antibody, similarly to pembrolizumab, targets PD-1, preventing T-cell inactivation, and enhancing T-cell mediated immune responses against tumors. This randomized controlled trial investigated the efficacy and safety of cemiplimab versus the investigator’s choice chemotherapy in women with advanced cervical cancer. A total of 608 patients were equally randomized to receive either cemiplimab (350mg every 3 weeks) or chemotherapy. The cemiplimab group demonstrated a significant improvement in median OS compared to the chemotherapy group (12.0 months vs. 8.5 months, respectively). This survival benefit was reflected in a HR for death of 0.69 (95% CI, 0.56 to 0.84; p < 0.001) favoring cemiplimab. Notably, this survival advantage remained consistent across both squamous cell carcinoma and adenocarcinoma (including adenosquamous carcinoma) histological subgroups. PFS was also significantly longer in the cemiplimab group compared to the chemotherapy group, as evidenced by a HR for disease progression or death of 0.75 (95% CI, 0.63 to 0.89; p < 0.001). The ORR was notably higher in the cemiplimab group (16.4%; 95% CI, 12.5 to 21.1) compared to the chemotherapy group (6.3%; 95% CI, 3.8 to 9.6). Interestingly, within the cemiplimab group, the response rate was 18% (95% CI, 11 to 28) for patients with PD-L1 expression ≥1% and 11% (95% CI, 4 to 25) for those with PD-L1 expression <1%. Grade ≥3 adverse events were observed in 45.0% of patients in the cemiplimab group and 53.4% of patients in the chemotherapy group. This study suggests that cemiplimab provides a significant improvement in OS and PFS compared to chemotherapy in women with advanced CC. The observed benefit was consistent across histological subgroups and PD-L1 expression levels. While adverse events were noted in both groups, the incidence of grade ≥3 events was numerically lower in the cemiplimab group (25).
Table 1 summarizes clinical trials investigating the efficacy and safety of immunotherapy for the treatment of metastatic, recurrent, or persistent cervical cancer.
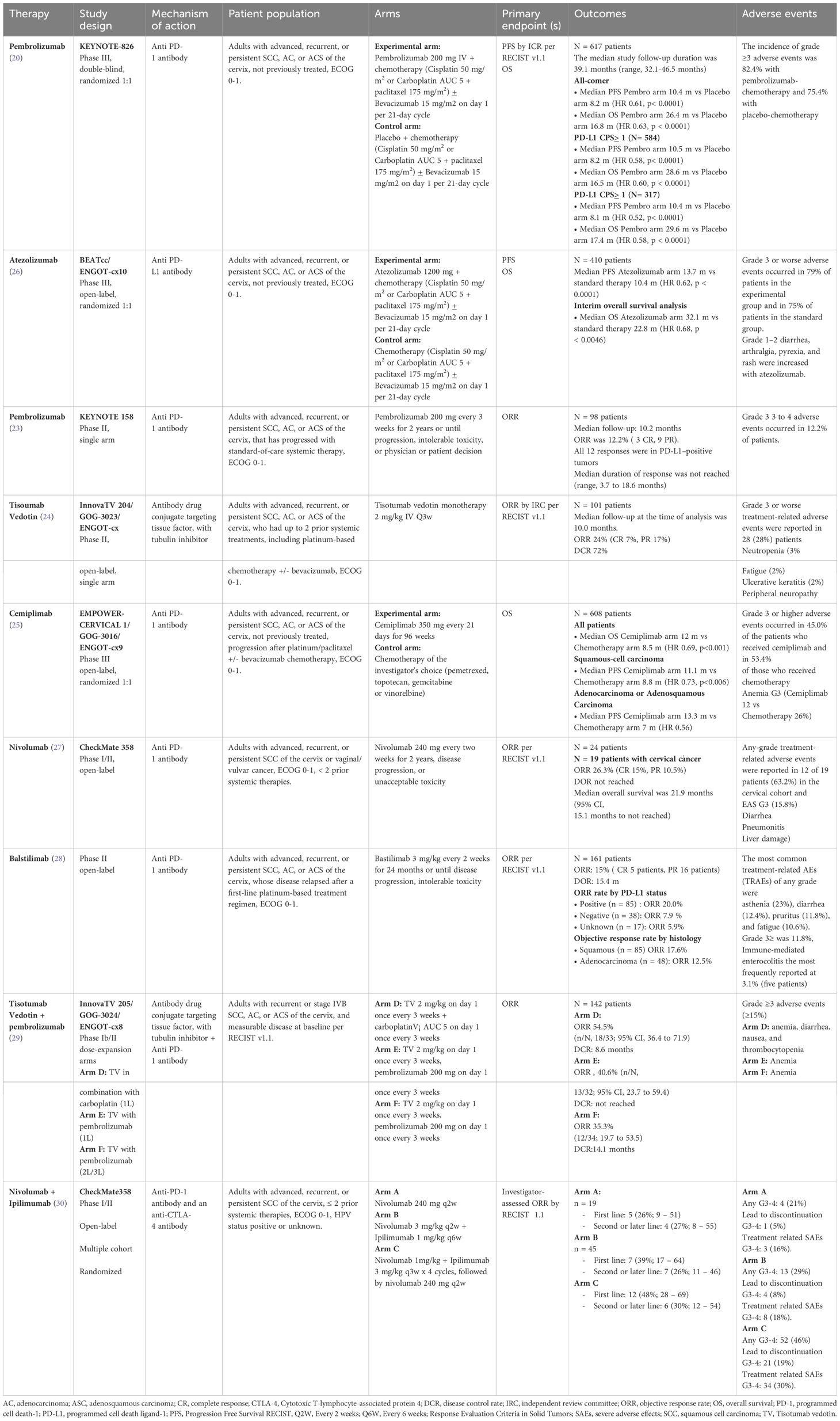
Table 1 Advanced, recurrent, and persistent cervical cancer targeted therapies.
Currently, there are several phase I-II clinical trials evaluating the use of immunotherapy as second-line treatment for recurrent and persistent metastatic cervical cancer, with promising outcomes expected for this patient group (Table 2). Furthermore, the related mechanisms of combined immunotherapy with other treatments such as chemotherapy or targeted therapies, as well as combinations of immunotherapies, are being assessed in different clinical studies and are anticipated to alter current treatment guidelines in the future.
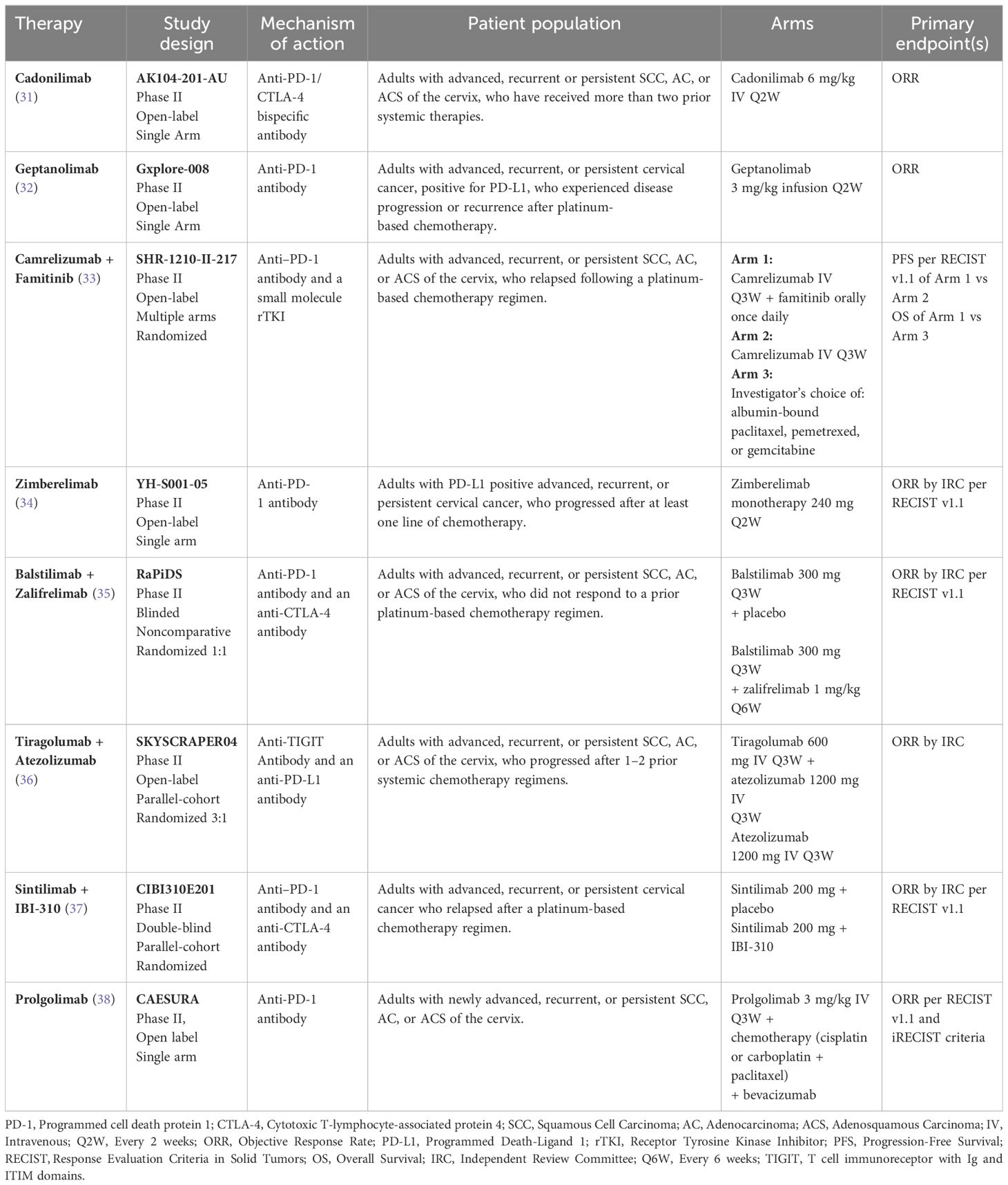
Table 2 Therapies under investigation for the treatment of advanced, persistent, and recurrent cervical cancer.
Conclusions
Cervical cancer patients facing metastatic, persistent, or recurrent disease experience a dismal prognosis, with a 5-year survival rate below 20%. This underscores the critical need for novel therapeutic interventions to improve outcomes for this patient population. Recent advancements in understanding the mechanisms of immunosuppression within the tumor microenvironment have paved the way for the development of innovative immunotherapeutic strategies. These approaches aim to counteract immunosuppressive pathways and bolster effector immune cell function, leading to promising improvements in both progression-free survival (PFS) and overall survival (OS), particularly in the first-line treatment setting.
Recommendations
● The use of pembrolizumab with platinum + paclitaxel ± bevacizumab is recommended for patients with metastatic, recurrent, or persistent CC with PD-L1 CPS ≥1%, of squamous, adenocarcinoma, or adenosquamous histology, as first-line treatment. Quality of evidence (GRADE: High) Level of recommendation IA.
● The use of platinum + paclitaxel ± bevacizumab is recommended for patients with metastatic, recurrent, or persistent CC with PD-L1 CPS <1%, of squamous, adenocarcinoma, or adenosquamous histology, as first-line treatment. Quality of evidence (GRADE: High) Level of recommendation IA.
● For patients not eligible for combination antiangiogenic or immunotherapy plus chemotherapy, chemotherapy following international guidelines is recommended. Quality of evidence (GRADE: Moderate) Level of recommendation IIB.
● The use of pembrolizumab as monotherapy is recommended in patients with metastatic, recurrent, or persistent CC, of squamous, adenocarcinoma, or adenosquamous histology, with progression on at least one line of platinum-based chemotherapy (PD-L1 CPS ≥1%, MSI-H, dMMR, TMB-H). Quality of evidence (GRADE: Moderate) Level of recommendation IIB.
● The use of tisotumab/vedontin is recommended in patients with metastatic, recurrent, or persistent CC, of squamous, adenocarcinoma, or adenosquamous histology, with progression on chemotherapy, as second-line treatment. Quality of evidence (GRADE: Moderate) Level of recommendation IIB.
● The use of cemiplimab monotherapy is recommended in patients with metastatic, recurrent, or persistent CC, of squamous, adenocarcinoma, or adenosquamous histology, with progression on chemotherapy, as second-line treatment. Quality of evidence (GRADE: High) Level of recommendation IB.
● The use of chemotherapy as monotherapy (paclitaxel, docetaxel, gemcitabine, topotecan, vinorelbine) may be an option in second-line treatment for patients with advanced, recurrent, or persistent CC, not eligible for immunotherapy. Quality of evidence (GRADE: Moderate) Level of recommendation IIB.
Author contributions
TG-C: Conceptualization, Data curation, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. EA-B: Investigation, Resources, Writing – original draft, Writing – review & editing. JC-M: Investigation, Writing – original draft, Writing – review & editing. LC-P: Project administration, Writing – original draft, Writing – review & editing. EV-C: Writing – original draft, Writing – review & editing. RV-V: Writing – original draft, Writing – review & editing. JG-P: Data curation, Investigation, Visualization, Writing – original draft, Writing – review & editing. PC-E: Conceptualization, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The authors have secured a sponsor, Laboratorios PiSA S.A. de C.V. (PiSA), to cover the publication fee. Please note that PiSA's involvement is limited to the payment of this fee; the research and authorship were entirely conducted by the authors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Klaes R, Woerner SM, Ridder R, Wentzensen N, Duerst M, Schneider A, et al. Detection of high-risk cervical intraepithelial neoplasia and cervical cancer by amplification of transcripts derived from integrated papillomavirus oncogenes. Cancer Res. (1999) 59:6132–6.
2. Vici P, Pizzuti L, Mariani L, Zampa G, Santini D, Di Lauro L, et al. Targeting immune response with therapeutic vaccines in premalignant lesions and cervical cancer: hope or reality from clinical studies. Expert Rev Vaccines. (2016) 15:1327–36. doi: 10.1080/14760584.2016.1176533
3. Duensing S, Münger K. Mechanisms of genomic instability in human cancer: Insights from studies with human papillomavirus oncoproteins. Int J Cancer. (2004) 109:157–62. doi: 10.1002/ijc.11691
4. Wang J, Sun H, Zeng Q, Guo XJ, Wang H, Liu HH, et al. HPV-positive status associated with inflamed immune microenvironment and improved response to anti-PD-1 therapy in head and neck squamous cell carcinoma. Sci Rep. (2019) 9:1–10. doi: 10.1038/s41598-019-49771-0
5. Mezache L, Paniccia B, Nyinawabera A, Nuovo GJ. Enhanced expression of PD L1 in cervical intraepithelial neoplasia and cervical cancers. Mod Pathol. (2015) 28:1594–602. doi: 10.1038/modpathol.2015.108
6. Lyford-Pike S, Peng S, Young GD, Taube JM, Westra WH, Akpeng B, et al. Evidence for a role of the PD-1:PD-L1 pathway in immune resistance of HPV-associated head and neck squamous cell carcinoma. Cancer Res. (2013) 73:1733–41. doi: 10.1158/0008-5472.CAN-12-2384
7. Enwere EK, Kornaga EN, Dean M, Koulis TA, Phan T, Kalantarian M, et al. Expression of PD-L1 and presence of CD8-positive T cells in pre-treatment specimens of locally advanced cervical cancer. Mod Pathol. (2017) 30:577–86. doi: 10.1038/modpathol.2016.221
8. Mortezaee K. Immune escape: A critical hallmark in solid tumors. Life Sci. (2020) 258:118110. doi: 10.1016/j.lfs.2020.118110
9. Peters R, Yanase Y. Strong enhancement of the Edelstein effect in f -electron systems. Phys Rev B. (2018) 97:252–64. doi: 10.1103/PhysRevB.97.115128
10. Alexandrov LB, Nik-zainal S, Wedge DC, Aparicio SAJR. Europe PMC Funders Group Signatures of mutational processes in human cancer. Nature. (2014) 500:415–21. doi: 10.1038/nature12477
11. Chen DS, Mellman I. Oncology meets immunology: The cancer-immunity cycle. Immunity. (2013) 39:1–10. doi: 10.1016/j.immuni.2013.07.012
12. Ohaegbulam KC, Assal A, Lazar-Molnar E, Yao Y, Zang X. Human cancer immunotherapy with antibodies to the PD-1 and PD-L1 pathway. Trends Mol Med. (2015) 21(1):24–33. doi: 10.1016/j.molmed.2014.10.009
13. Ohigashi Y, Sho M, Yamada Y, Tsurui Y, Hamada K, Ikeda N, et al. Clinical significance of programmed death-1 ligand-1 and programmed death-1 ligand-2 expression in human esophageal cancer. Clin Cancer Res. (2005) 11:2947–53. doi: 10.1158/1078-0432.CCR-04-1469
14. Brahmer J, Reckamp KL, Baas P, Crinò L, Eberhardt WEE, Poddubskaya E, et al. Nivolumab versus docetaxel in advanced squamous-cell non–small-cell lung cancer. N Engl J Med. (2015) 373:123–35. doi: 10.1056/NEJMoa1504627
15. Wendel Naumann R, Leath CA 3rd. Advances in immunotherapy for cervical cancer. Curr Opin Oncol. (2020) 32(5):481–7. doi: 10.1097/CCO.00000000000006
16. Tewari KS, Sill MW, Long HJ, Penson RT, Huang H, Ramondetta LM, et al. 1Final overall survival of the phase III randomised trial of chemotherapy with and without bevacizumab for advanced cervical cancer: an NRG oncology/gynecologic oncology group study. Obstet Gynecol Surv. (2017) 69:331–2. doi: 10.1016/S0140-6736(17)31607-0
17. Monk BJ, Sill MW, McMeekin DS, Cohn DE, Ramondetta LM, Boardman CH, et al. Phase III trial of four cisplatin-containing doublet combinations in stage IVB, recurrent, or persistent cervical carcinoma: A Gynecologic Oncology Group study. J Clin Oncol. (2009) 27:4649–55. doi: 10.1200/JCO.2009.21.8909
18. Long HJ, Bundy BN, Grendys EC, Benda JA, McMeekin DS, Sorosky J, et al. Randomized phase III trial of cisplatin with or without topotecan in carcinoma of the uterine cervix: A Gynecologic Oncology Group study. J Clin Oncol. (2005) 23:4626–33. doi: 10.1200/JCO.2005.10.021
19. Kitagawa R, Katsumata N, Shibata T, Kamura T, Kasamatsu T, Nakanishi T, et al. Paclitaxel plus carboplatin versus paclitaxel plus cisplatin in metastatic or recurrent cervical cancer: The open-label randomized phase III trial JCOG0505. J Clin Oncol. (2015) 33:2129–35. doi: 10.1200/JCO.2014.58.4391
20. Colombo N, Dubot C, Lorusso D, Caceres MV, Hasegawa K, Shapira-Frommer R, et al. Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N Engl J Med. (2021) 385:1856–67. doi: 10.1056/NEJMoa2112435
21. Tewari KS, Colombo N, Monk BJ, Dubot C, Cáceres MV, Hasegawa K, et al. Pembrolizumab or placebo plus chemotherapy with or without bevacizumab for persistent, recurrent, or metastatic cervical cancer. JAMA Oncol. (2023) 92868:185–92. doi: 10.1001/jamaoncol.2023.5410
22. Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical cancer. Lancet. (2019) 393:169–82. doi: 10.1016/S0140-6736(18)32470-X
23. Chung HC, Ros W, Delord JP, Perets R, Italiano A, Shapira-Frommer R, et al. Efficacy and safety of pembrolizumab in previously treated advanced cervical cancer: Results from the phase II KEYNOTE-158 study. J Clin Oncol. (2019) 37:1470–8. doi: 10.1200/JCO.18.01265
24. Coleman RL, Lorusso D, Gennigens C, González-Martín A, Randall L, Cibula D, et al. Efficacy and safety of tisotumab vedotin in previously treated recurrent or metastatic cervical cancer (innovaTV 204/GOG-3023/ENGOT-cx6): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. (2021) 22:609–19. doi: 10.1016/S1470-2045(21)00056-5
25. Tewari KS, Monk BJ, Vergote I, Miller A, de Melo AC, Kim H-S, et al. Survival with cemiplimab in recurrent cervical cancer. N Engl J Med. (2022) 386:544–55. doi: 10.1056/NEJMoa2112187
26. Oaknin A, Gladieff L, Martínez-García J, Villacampa G, Takekuma M, De Giorgi U, et al. Atezolizumab plus bevacizumab and chemotherapy for metastatic, persistent, or recurrent cervical cancer (BEATcc): a randomised, open-label, phase 3 trial. Lancet. (2023), 31–43. doi: 10.1016/S0140-6736
27. Naumann RW, Leath CA. Advances in immunotherapy for cervical cancer. Curr Opin Oncol. (2020) 32:481–7. doi: 10.1097/CCO.0000000000000663
28. O’Malley DM, Oaknin A, Monk BJ, Selle F, Rojas C, Gladieff L, et al. Phase II study of the safety and efficacy of the anti-PD-1 antibody balstilimab in patients with recurrent and/or metastatic cervical cancer. Gynecol Oncol. (2021) 163:274–80. doi: 10.1016/j.ygyno.2021.08.018
29. Vergote I, Van Nieuwenhuysen E, O’Cearbhaill RE, Westermann A, Lorusso D, Ghamande S, et al. Tisotumab vedotin in combination with carboplatin, pembrolizumab, or bevacizumab in recurrent or metastatic cervical cancer: results from the innovaTV 205/GOG-3024/ENGOT-cx8 study. J Clin Oncol. (2023) 41:5536–49. doi: 10.1200/JCO.23.00720
30. Oaknin A, Moore K, Meyer T, López-Picazo González J, Devriese LA, Amin A, et al. Nivolumab with or without ipilimumab in patients with recurrent or metastatic cervical cancer (CheckMate 358): a phase 1-2, open-label, multicohort trial. Lancet Oncol. (2024) 25(5):588–602. doi: 10.1016/S1470-2045(24)00088-3
31. Wu X, Ji J, Lou H, Li Y, Feng M, Xu N, et al. Efficacy and safety of cadonilimab, an anti-PD-1/CTLA4 bi-specific antibody, in previously treated recurrent or metastatic (R/M) cervical cancer: a multicenter, open-label, single-arm, phase II trial (075). Gynecologic Oncol. (2022) 166:S47–8. doi: 10.1016/S0090-8258(22)01293-8
32. An J, Zhang Y, Feng M, Zhang K, Zhu J, He A, et al. A multicenter, open-label, single-arm, phase II trial to evaluate the efficacy and safety of geptanolimab (GB226) in the treatment of patients (pts) with programmed cell death ligand 1 (PD-L1)–positive recurrent or metastatic cervical cancer, for whom prior platinum-containing chemotherapy has failed. JCO. (2023) 41:5535–5. doi: 10.1200/JCO.2023.41.16_suppl.5535
33. Xia L, Zhou Q, Gao Y, Hu W, Lou G, Sun H, et al. A multicenter phase 2 trial of camrelizumab plus famitinib for women with recurrent or metastatic cervical squamous cell carcinoma. Nat Commun. (2022) 13(1):7581. doi: 10.1038/s41467-022-35133-4
34. Wu X, Xia L, Zhou Q, Zhu J, Wang K, Chen J, et al. 357 GLS-010 (zimberelimab), a novel fully human anti-PD-1 mAb in chinese patients with recurrent/metastatic cervical cancer: results from a multicenter, open-label, single-arm phase II trial. Int J Gynecol Cancer. (2020) 30:A147. doi: 10.1136/ijgc-2020-IGCS.307
35. O'Malley DM, Neffa M, Monk BJ, Melkadze T, Huang M, Kryzhanivska A, et al. Dual PD-1 and CTLA-4 checkpoint blockade using balstilimab and zalifrelimab combination as second-line treatment for advanced cervical cancer: An open-label phase II study. J Clin Oncol. (2022) 40(7):762–71. doi: 10.1200/JCO.21.02067
36. Salani R, McCormack M, Kim YM, Ghamande S, Hall SL, Lorusso D, et al. A non-comparative, randomized, phase II trial of atezolizumab or atezolizumab plus tiragolumab for programmed death-ligand 1-positive recurrent cervical cancer (SKYSCRAPER-04). Int J Gynecol Cancer. (2024), ijgc–2024-005588. doi: 10.1136/ijgc-2024-005588
37. Gao Q, Wang J, Xu Q, Tang Y, Zhang J, Chang B, et al. Efficacy and safety of sintilimab (anti-PD-1 mAb) for advanced cervical cancer: Results from a phase II trial [abstract]. In: Proceedings of the american association for cancer research annual meeting 2023; part 2 (Clinical trials and late-breaking research), vol. 83. . Orlando, FL. Philadelphia (PA: AACR (2023). p. Abstract nr CT079.
Keywords: cervical cancer, metastatic cervical cancer, immunotherapy, recurrent and persistent disease, checkpoint inhibitors
Citation: Galicia-Carmona T, Arango-Bravo EA, Coronel-Martínez JA, Cetina-Pérez L, Vanoye-Carlo EG, Villalobos-Valencia R, García-Pacheco JA and Cortés-Esteban P (2024) Advanced, recurrent, and persistent cervical cancer management: in the era of immunotherapy. Front. Oncol. 14:1392639. doi: 10.3389/fonc.2024.1392639
Received: 27 February 2024; Accepted: 02 July 2024;
Published: 05 August 2024.
Edited by:
Peter Hamar, Semmelweis University, HungaryReviewed by:
Ke Hu, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaCopyright © 2024 Galicia-Carmona, Arango-Bravo, Coronel-Martínez, Cetina-Pérez, Vanoye-Carlo, Villalobos-Valencia, García-Pacheco and Cortés-Esteban. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patricia Cortés-Esteban, ZHJhLnBjb3J0ZXNAZ21haWwuY29t