
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol., 23 May 2024
Sec. Pediatric Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1381354
 Serafin Castellano-Damaso1
Serafin Castellano-Damaso1 Felisa Vazquez-Gomez1
Felisa Vazquez-Gomez1 Jose Luis Moreno-Carrasco1Begoña Arce2Pedro Borrego3
Jose Luis Moreno-Carrasco1Begoña Arce2Pedro Borrego3 Alvaro Lassaletta1*
Alvaro Lassaletta1*Dissemination in pediatric low-grade glioma may occur in about 4%–10% of patients according to retrospective cohort studies. Due to its low incidence, there is no consensus on treatment for these patients. According to the constitutional activation of the MAPK/ERK pathway in these tumors, MEK inhibitors such as trametinib have been used successfully in the relapsed setting. Skin toxicity is frequent in patients receiving trametinib, normally mild to moderate, but sometimes severe, needing to discontinue the drug, limiting the efficacy in the tumor. There is not much information in the literature regarding whether reducing the dose of trametinib is able to maintain efficacy while, at the same time, decreasing toxicity. Here, we present an adolescent, with severe skin toxicity, whose trametinib dose was reduced by 50% and efficacy on the tumor continued while skin toxicity significantly decreased.
Low-grade gliomas represent the most common central nervous system tumors in children (1). Although mostly localized at diagnosis, they can disseminate in up to 10% at progression or relapse (2–4). Dissemination in pediatric low-grade gliomas (pLGGs) is a phenomenon that is not fully understood (2, 5, 6), and its true incidence remains unknown due to the absence of prospective cohort studies (3). In addition, it can significantly reduce the overall survival of these patients (7, 8). According to the published case series, the frequency of dissemination in pLGG varies between 2% and 5% at diagnosis (2–4) and 2.4% and 10% at progression or relapse (2–4). Due to its low incidence, there is no universally established therapy for disseminated pLGG (3, 4, 7). As surgery is not feasible, and radiotherapy requires craniospinal radiation with many long-term side effects (7, 8), conventional chemotherapy has been the preferred treatment in disseminated pLGG (8). Recent reports state that specific molecular alterations (9–11), such as chromosome 1p deletion (11), KIAA1549-BRAF fusion (11), BRAF V600E mutation (12), and EGFR gene amplification (13), may contribute to cause dissemination in pLGGs. With this knowledge in mind, new targeted therapies are becoming part of its treatment (14).
MEK inhibitors have been used in the treatment of LGG in children and adolescents with promising results (14–28). However, their use in disseminated pLGG has been scarcely reported in the literature. Toxicity mainly consists of skin adverse events which can affect the quality of life of the patients sometimes needing to discontinue the drug (29). Here, we report an adolescent with a disseminated pLGG which progressed after conventional chemotherapy. Trametinib was started, resulting in a favorable tumor response but with significant toxicity. The dose was subsequently reduced by 50%, maintaining tumoral response while reducing toxicity.
An 18-year-old non-NF1 male patient with a diagnosis of pilocytic astrocytoma of the right temporal lobe was diagnosed at the age of 3 years in 2008 at our institution, with no prior family or personal background of interest. At first, he underwent surgery on two occasions, with a partial resection at diagnosis, and another partial resection in 2010 due to tumor local progression. Due to a slow but continuous progression over time of the residual tumor and the appearance of new periventricular enhancement showed in routine magnetic resonance imaging (MRI), in December 2016, he started treatment with weekly vinblastine as per the Canadian Pediatric Brain Tumor Consortium protocol (30). Initial surgical samples were sent to the molecular biology lab for testing BRAF V600E mutation, which came up as negative. He completed 70 weeks of treatment in May 2018 with stable disease described as the best response achieved under this treatment.
After finishing chemotherapy treatment, he started to develop weekly seizures, with no signs of tumoral growth and a stable appearance of the periventricular enhancement, and started anticonvulsant levetiracetam. During one of the seizures in November 2018, he suffered a parietal bone fracture, and after noticing hydrocephalus with no signs of tumor regrowth, a ventriculoperitoneal shunt was placed. Seizures resolved.
In January 2019, a reassessment MRI showed signs of worsening leptomeningeal dissemination, both spinal and supratentorial, as well as progressive growth of the tumor remnants. Therefore, it was decided to start a second line of chemotherapy using the SIOP-LGG 2004 protocol approach (31) with vincristine and carboplatin in March 2019. Only 2 months later (May 2019), this chemotherapy regimen had to be discontinued due to significant toxicity: grade 3 peripheral sensory-motor neuropathy, grade 4 neutropenia, grade 3 thrombocytopenia, grade 3 fatigue, and grade 2 constipation. Also, he developed two new episodes of hydrocephalus and needed shunt reprogramming. Initial tumor samples were sent for further molecular studies for the purpose of testing the presence of a KIAA1549-BRAF fusion, as it was not tested at first due to the initial unavailability of the test. This result was positive, involving a fusion between KIAA1549 exon 16 and BRAF exon 9. As a result, in July 2019, he started MEK inhibitor trametinib at standard dose (0.025 mg/kg once daily orally) (15).
During the following 3 years of treatment, with a partial response in the follow-up MRI that was done 6 months after starting treatment, he developed grade 3 skin dermatitis, folliculitis, acneiform lesions, and paronychia (Figure 1), which progressively impaired the patient’s quality of life. Because of that, in May 2022, we decided to reduce the dose of trametinib to 50% of the current dose (0.0125 mg/kg once daily orally). With this new dose, all skin lesions partially resolved, and his subjective quality of life significantly improved. Despite this dose reduction, trametinib continued to reduce the size of the tumor in the 3-monthly MRIs that followed the dose reduction (Figure 2), maintaining a partial response even at this reduced dose. After 1 year of treatment with this reduced dose, Trametinib was finally discontinued in June 2023, after completing 4 years of therapy. So far, the patient has not developed any signs of tumor re-growth and continues to be under close follow-up at our institution (Figure 3).

Figure 1 Skin toxicity in the patient showing severe paronychia in both feet.
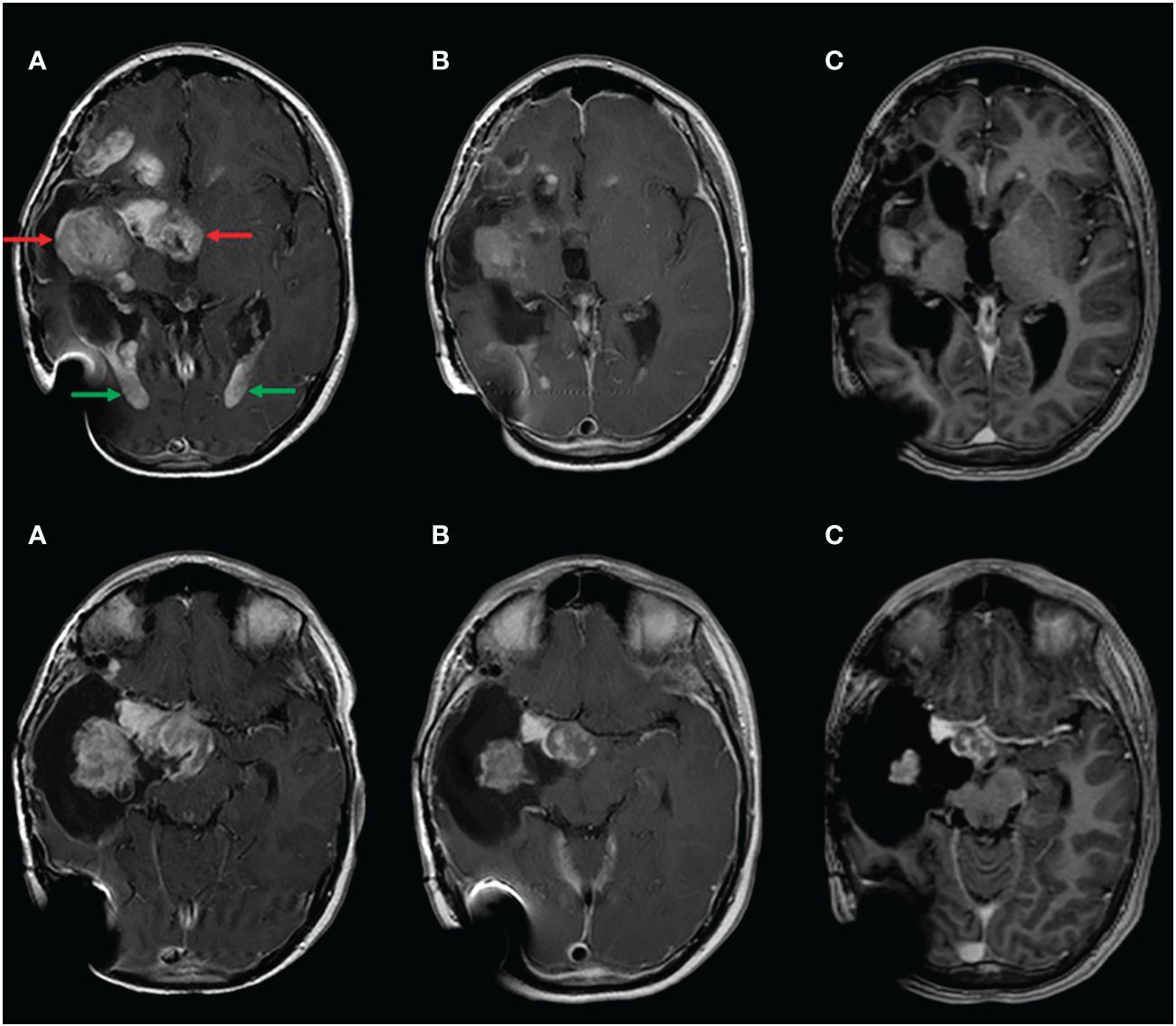
Figure 2 Contrast material-enhanced T1-weighted MR image shows reduction of the solid part of the main tumor (red arrows) as well as the intraventricular enhancing masses (green arrows). (A) Pre-treatment with trametinib; (B) before reducing trametinib dose; (C) end of treatment.

Figure 3 Timeline describing the treatment of the patient.
Written informed consent to publish the case report including clinical information and images was obtained from the patient.
This report displays a continuous response to reduced-dose treatment with MEK-inhibitor trametinib in a patient with an initially localized pLGG, which spread over time along the neuroaxis and required a new treatment for controlling the disease.
Dissemination in pLGG may occur in about 2.4%–10% of relapses according to retrospective cohort studies (3, 4, 7). Owning to its rarity, there is no consensus about treatment for these patients (3, 4, 7). Usually, these patients have already received multiple chemotherapy lines of treatment. Craniospinal radiotherapy carries important long-term side effects, and surgery is not feasible in disseminated disease.
Almost all pLGGs have MAPK pathway alterations (1); the most frequent are the BRAF fusion KIAA1549-BRAF and the BRAFV600E mutation (9). Since these alterations were discovered at the beginning of the century, targeted therapy (BRAF and MEK inhibitors) has been studied in clinical trials in the relapsed/progression and new diagnosis setting (14–28). MEK inhibitors have shown efficacy in relapsed pLGG as has been reported elsewhere (16–23, 32, 33). Current knowledge in this field seems to affirm that patients with the KIAA1549-BRAF fusion seem to respond better to MEK inhibitors than the ones that are BRAF-fused negative (32), as in our patient´s case, whereas paradoxical reactions to BRAF inhibitors with tumor accelerated growth has been reported in these BRAF-fused patients (21, 34, 35).
There are several phase I and II clinical trials involving MEK inhibitors for treating pLGG, including selumetinib (20, 21, 26), trametinib (15–19, 23), cobimetinib (22), binimetinib (24), and mirdametinib (25). The two most researched about are selumetinib and trametinib. So far, there are multiple published results regarding selumetinib in NF1 and non-NF1 patients with pLGG. Trametinib also has been used successfully in treating progressive/relapsed low-grade gliomas in children, although achieving a complete response in monotherapy has turned out to be difficult (27, 28). Sustained responses in low-grade glioma patients have typically been achieved through the administration of these drugs; however, there are documented cases of relapse or progression following dose reduction or the discontinuation of the drug (20). In the reported literature, there have been described at least 15 patients (14, 18, 23, 32, 33) with a disseminated low-grade glioma who underwent treatment with MEK inhibitors as our patient. However, only three of them harbored the KIAA1549-BRAF fusion (23, 33), with an unknown BRAF status in the one reported by Selt et al, and comprising different BRAF mutations in the other eleven patients.
Toxicities are a major drawback in the treatment with MEK inhibitors. Skin toxicity is common in patients receiving trametinib (28), normally mild to moderate, but sometimes severe, needing to discontinue the drug and limiting the efficacy in the tumor. From our personal experience, side effects are usually worse in adolescents compared to younger children, although there is no strong evidence for it in the scientific literature. In our patient’s case, skin toxicity severely impaired his quality of life and obliged us to reduce trametinib’s dose as fully stopping treatment was a difficult option to take as he was responding very well to the drug. Thus, the dose reduction successfully helped to control skin toxicity while maintaining tumor response. This was in line with one of the cases published by Kondyli et al. in 2018, the only one with a detailed report in the literature. In that case, the patient was a 15-year-old female who started trametinib after progression to several lines of treatment and who also developed severe paronychia. That patient also harbored the KIAA1549-BRAF fusion. However, in that case, she was only followed for 6 months with no further information regarding her outcome. To our knowledge, this case report represents the longest follow-up of a disseminated low-grade glioma patient who has maintained a continuous tumoral response to trametinib despite a dose reduction to 50% due to severe adverse events.
Treatment in our patient was discontinued when the patient turned 18 years old, due to having already finished puberty. This was done based on the proposed theory that pediatric low grade gliomas stop growing after pubertal development has been completed (36). An ongoing problem in treating pLGGs with MEK and BRAF inhibitors remains regarding for how long does the treatment needs to be given. In melanoma, another MEK-pathway-driven malignant tumor, the current consensus is to maintain targeted therapy as long as a response is achieved (37), and treatment discontinuity is usually secondary to treatment toxicity or disease progression (38). Given the benign nature of pLGGs, whereas these tumors usually stop growing over time, it seems reasonable to stop treatment and do a wait-and-see approach afterward. However, the true efficacy of this management should be tested in a prospective, randomized, clinical trial. So far, our patient has not presented any kind of tumor regrowth. He is doing well and continues to be under close follow-up at our center.
This case report shows that, in very selected cases with significant toxicity to MEK inhibitors, dose reduction may improve toxicity while maintaining anti-tumor response.
The clinical characteristics of patients who may benefit from this dose-reduction approach still require further definition. Additional research is needed to determine whether pLGG patients with specific molecular alterations, such as the KIAA1549-BRAF fusion, may derive benefits from treatment with MEK inhibitors like trametinib.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
SC-D: Formal analysis, Data curation, Writing – review & editing, Writing – original draft, Methodology, Investigation, Conceptualization. FV-G: Supervision, Writing – review & editing, Writing – original draft. JLM-C: Writing – review & editing, Writing – original draft, Supervision. BA: Validation, Investigation, Writing – original draft, Supervision. PB: Software, Writing – original draft, Validation, Supervision. AL: Writing – review & editing, Methodology, Investigation, Funding acquisition, Conceptualization, Writing – original draft, Validation, Supervision.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. SC-D has received funds for completing a neuro-oncology fellowship from El Sueño de Vicky Foundation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1381354/full#supplementary-material
1. Packer RJ, Pfister S, Bouffet E, Avery R, Bandopadhayay P, Bornhorst M, et al. Pediatric low-grade gliomas: implications of the biologic era. Neuro-oncol. (2017) 19:750–61. doi: 10.1093/neuonc/now209
2. Perilongo G, Garrè ML, Giangaspero F. Low-grade gliomas and leptomeningeal dissemination: a poorly understood phenomenon. Child’s nervous system. (2003) 19:197–203. doi: 10.1007/s00381-003-0733-1
3. Chamdine O, Broniscer A, Wu S, Gajjar A, Qaddoumi I. Metastatic low-grade gliomas in children: 20 years’ experience at St. Jude Children’s Research Hospital. Pediatr Blood cancer. (2016) 63:62–70. doi: 10.1002/pbc.25731
4. von Hornstein S, Kortmann RD, Pietsch T, Emser A, Warmuth-Metz M, Soerensen N, et al. Impact of chemotherapy on disseminated low-grade glioma in children and adolescents: report from the HIT-LGG 1996 trial. Pediatr Blood cancer. (2011) 56:1046–54. doi: 10.1002/pbc.23006
5. Hukin J, Siffert J, Velasquez L, Zagzag D, Allen J. Leptomeningeal dissemination in children with progressive low-grade neuroepithelial tumors. Neuro-oncol. (2002) 4:253–60. doi: 10.1093/neuonc/4.4.253
6. D’Haene N, Coen N, Neugroschl C, Balériaux D, Salmon I. Leptomeningeal dissemination of low-grade intramedullary gliomas: about one case and review. Clin Neurol neurosurgery. (2009) 111:390–4. doi: 10.1016/j.clineuro.2008.11.013
7. Tsang DS, Murphy ES, Ezell SE, Lucas JT, Tinkle C, Merchant TE. Craniospinal irradiation for treatment of metastatic pediatric low-grade glioma. J neuro-oncol. (2017) 2:134:317–24. doi: 10.1007/s11060-017-2525-6
8. Mazloom A, Hodges JC, Teh BS, Chintagumpala M, Paulino AC. Outcome of patients with pilocytic astrocytoma and leptomeningeal dissemination. Int J Radiat Oncol Biol Physics. (2012) 84:350–4. doi: 10.1016/j.ijrobp.2011.12.044
9. Ryall S, Zapotocky M, Fukuoka K, Nobre L, Stucklin AG, Bennett J, et al. Integrated molecular and clinical analysis of 1,000 pediatric low-grade gliomas. Cancer Cell. (2020) 37:569–83. doi: 10.1016/j.ccell.2020.03.011
10. Ryall S, Tabori U, Hawkins C. Pediatric low-grade glioma in the era of molecular diagnostics. Acta neuropathologica Commun. (2020) 8:1–22. doi: 10.1186/s40478-020-00902-z
11. Haizel-Cobbina J, Thakkar R, Richard K, Du L, Levine A, Bennett J, et al. Clinical and molecular features of disseminated pediatric low-grade glioma and glioneuronal tumors: a systematic review and survival analysis. Neuro-Oncol Adv. (2022) 4:vdac122. doi: 10.1093/noajnl/vdac122
12. Dodgshun AJ, SantaCruz N, Hwang J, Ramkissoon SH, Malkin H, Bergthold G, et al. Disseminated glioneuronal tumors occurring in childhood: treatment outcomes and BRAF alterations including V600E mutation. J neuro-oncol. (2016) 128:293–302. doi: 10.1007/s11060-016-2109-x
13. Tabori U, Rienstein S, Dromi Y, Leider-Trejo L, Constantini S, Burstein Y, et al. Epidermal growth factor receptor gene amplification and expression in disseminated pediatric low-grade gliomas. J Neurosurgery: Pediatrics. (2005) 103:357–61. doi: 10.3171/ped.2005.103.4.0357
14. Bouffet E, Hansford JR, Garrè ML, Hara J, Plant-Fox A, Aerts I, et al. Dabrafenib plus trametinib in pediatric glioma with BRAF V600 Mutations. New Engl J Med. (2023) 389:1108–20. doi: 10.1056/NEJMoa2303815
15. Bouffet E, Geoerger B, Moertel C, Whitlock JA, Aerts I, Hargrave D, et al. Efficacy and safety of trametinib monotherapy or in combination with dabrafenib in pediatric BRAF V600–mutant Low-grade glioma. J Clin Oncol. (2023) 41:664. doi: 10.1200/JCO.22.01000
16. Perreault S, Larouche V, Tabori U, Hawkin C, Lippé S, Ellezam B, et al. A phase 2 study of trametinib for patients with pediatric glioma or plexiform neurofibroma with refractory tumor and activation of the MAPK/ERK pathway: TRAM-01. BMC cancer. (2019) 19:1–9. doi: 10.1186/s12885-019-6442-2
17. Manoharan N, Choi J, Chordas C, Zimmerman MA, Scully J, Clymer J, et al. Trametinib for the treatment of recurrent/progressive pediatric low-grade glioma. J Neuro-Oncol. (2020) 149:253–62. doi: 10.1007/s11060-020-03592-8
18. Selt F, van Tilburg CM, Bison B, Sievers P, Harting I, Ecker J, et al. Response to trametinib treatment in progressive pediatric low-grade glioma patients. J Neuro-oncol. (2020) 149:499–510. doi: 10.1007/s11060-020-03640-3
19. Geoerger B, Moertel CL, Whitlock J, McCowage GB, Kieran MW, Broniscer A, et al. Phase 1 trial of trametinib alone and in combination with dabrafenib in children and adolescents with relapsed solid tumors or neurofibromatosis type 1 (NF1) progressive plexiform neurofibromas (PN). J Clin Oncol. (2018) 36:10537–7. doi: 10.1200/JCO.2018.36.15_suppl.10537
20. Fangusaro J, Onar-Thomas A, Poussaint TY, Wu S, Ligon AH, Lindeman N, et al. Selumetinib in paediatric patients with BRAF-aberrant or neurofibromatosis type 1-associated recurrent, refractory, or progressive low-grade glioma: a multicentre, phase 2 trial. Lancet Oncol. (2019) 20:1011–22. doi: 10.1016/S1470-2045(19)30277-3
21. Banerjee A, Jakacki RI, Onar-Thomas A, Wu S, Nicolaides T, Young Poussaint T, et al. A phase I trial of the MEK inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or refractory low-grade glioma: a Pediatric Brain Tumor Consortium (PBTC) study. Neuro-oncol. (2017) 19:1135–44. doi: 10.1093/neuonc/now282
22. Trippett T, Toledano H, Campbell Hewson Q, Verschuur A, Langevin AM, Aerts I, et al. Cobimetinib in pediatric and young adult patients with relapsed or refractory solid tumors (iMATRIX-cobi): a multicenter, phase I/II study. Targeted Oncol. (2022) 17:283–93. doi: 10.1007/s11523-022-00888-9
23. Kondyli M, Larouche V, Saint-Martin C, Ellezam B, Pouliot L, Sinnett D, et al. Trametinib for progressive pediatric low-grade gliomas. J Neuro-Oncol. (2018) 140:435–44. doi: 10.1007/s11060-018-2971-9
24. Robison N, Pauly J, Malvar J, Gardner S, Allen J, Margol A, et al. LTBK-04. LATE BREAKING ABSTRACT: MEK162 (binimetinib) in children with progressive or recurrent low-grade glioma: a multi-institutional phase II and target validation study. Neuro-Oncology. (2022) 24:i191–2. doi: 10.1093/neuonc/noac079.716
25. Vinitsky A, Chiang J, Bag AK, Campagne O, Stewart CF, Dunphy P, et al. LGG-22. SJ901: Phase I/II evaluation of single agent mirdametinib (PD-0325901), a brain-penetrant MEK1/2 inhibitor, for the treatment of children, adolescents, and young adults with low-grade glioma (LGG). Neuro-Oncology. (2022) 24:i92–. doi: 10.1093/neuonc/noac079.336
26. Eckstein OS, Allen CE, Williams PM, Roy-Chowdhuri S, Patton DR, Coffey B, et al. Phase II study of selumetinib in children and young adults with tumors harboring activating mitogen-activated protein kinase pathway genetic alterations: arm E of the NCI-COG pediatric MATCH trial. J Clin Oncol. (2022) 40:2235–45. doi: 10.1200/JCO.21.02840
27. Galvin R, Watson AL, Largaespada DA, Ratner N, Osum S, Moertel CL. Neurofibromatosis in the era of precision medicine: development of MEK inhibitors and recent successes with selumetinib. Curr Oncol Rep. (2021) 23:1–0. doi: 10.1007/s11912-021-01032-y
28. De Blank PM, Gross AM, Akshintala S, Blakeley JO, Bollag G, Cannon A, et al. MEK inhibitors for neurofibromatosis type 1 manifestations: Clinical evidence and consensus. Neuro-oncol. (2022) 24:1845–56. doi: 10.1093/neuonc/noac165
29. Manousaridis I, Mavridou S, Goerdt S, Leverkus M, Utikal J. Cutaneous side effects of inhibitors of the RAS/RAF/MEK/ERK signalling pathway and their management. J Eur Acad Dermatol Venereol. (2013) 27:11–8. doi: 10.1111/j.1468-3083.2012.04546.x
30. Lassaletta A, Scheinemann K, Zelcer SM, Hukin J, Wilson BA, Jabado N, et al. Phase II weekly vinblastine for chemotherapy-naïve children with progressive low-grade glioma: a Canadian Pediatric Brain Tumor Consortium Study. J Clin Oncol. (2016) 34:3537–43. doi: 10.1200/JCO.2016.68.1585
31. Gnekow AK, Walker DA, Kandels D, Picton S, Perilongo G, Grill J, et al. A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (≤ 16 years) low grade glioma–a final report. Eur J cancer. (2017) 81:206–25. doi: 10.1016/j.ejca.2017.04.019
32. Drobysheva A, Klesse LJ, Bowers DC, Rajaram V, Rakheja D, Timmons CF, et al. Targeted MAPK pathway inhibitors in patients with disseminated pilocytic astrocytomas. J Natl Compr Cancer Network. (2017) 15:978–82. doi: 10.6004/jnccn.2017.0139
33. Pérez JP, Muchart J, López VS, Capella MS, Salvador N, Jaume SP, et al. Targeted therapy for pediatric low-grade glioma. Child’s Nervous System. (2021) 37:2511–20. doi: 10.1007/s00381-021-05138-3
34. Schreck KC, Grossman SA, Pratilas CA. BRAF mutations and the utility of RAF and MEK inhibitors in primary brain tumors. Cancers. (2019) 11:1262. doi: 10.3390/cancers11091262
35. Sievert AJ, Lang SS, Boucher KL, Madsen PJ, Slaunwhite E, Choudhari N, et al. Paradoxical activation and RAF inhibitor resistance of BRAF protein kinase fusions characterizing pediatric astrocytomas. Proc Natl Acad Sci. (2013) 110:5957–62. doi: 10.1073/pnas.1219232110
36. Jones DT, Kieran MW, Bouffet E, Alexandrescu S, Bandopadhayay P, Bornhorst M, et al. Pediatric low-grade gliomas: next biologically driven steps. Neuro-oncol. (2018) 20:160–73. doi: 10.1093/neuonc/nox141
37. Grimaldi AM, Simeone E, Festino L, Vanella V, Strudel M, Ascierto PA. MEK inhibitors in the treatment of metastatic melanoma and solid tumors. Am J Clin Dermatol. (2017) 18:745–54. doi: 10.1007/s40257-017-0292-y
Keywords: low-grade gliomas, trametinib, MEK inhibitor, children, BRAF fusion, response
Citation: Castellano-Damaso S, Vazquez-Gomez F, Moreno-Carrasco JL, Arce B, Borrego P and Lassaletta A (2024) Continuous response despite reduced dose of trametinib as single agent in an adolescent with a relapsed disseminated pediatric low-grade glioma KIAA1549-BRAF fusion positive: a case report and review of the literature. Front. Oncol. 14:1381354. doi: 10.3389/fonc.2024.1381354
Received: 03 February 2024; Accepted: 25 April 2024;
Published: 23 May 2024.
Edited by:
Angela Mastronuzzi, Bambino Gesù Children’s Hospital (IRCCS), ItalyReviewed by:
DeeDee Smart, National Cancer Institute (NIH), United StatesCopyright © 2024 Castellano-Damaso, Vazquez-Gomez, Moreno-Carrasco, Arce, Borrego and Lassaletta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alvaro Lassaletta, bGFzc2FhbHZhcm9AeWFob28uY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.