 Sebastián Aguiar-Rosas1,2
Sebastián Aguiar-Rosas1,2 Ricardo Plancarte-Sanchez1,2
Ricardo Plancarte-Sanchez1,2 B. Carolina Hernandez-Porras1,2Jorge García-Andreu3,4Brenda Olivia Lezcano-Velazquez1,2Ignacio Reyes-Torres5
B. Carolina Hernandez-Porras1,2Jorge García-Andreu3,4Brenda Olivia Lezcano-Velazquez1,2Ignacio Reyes-Torres5 Silvia Alarcón-Barrios1,2*
Silvia Alarcón-Barrios1,2*- 1Pain Clinic, Instituto Nacional de Cancerología, Mexico City, Mexico
- 2Independent Researcher, Mexico City, Mexico
- 3Star Medica Hospital, Queretaro, Mexico
- 4Independent Researcher, Queretaro, Mexico
- 5Independent Researcher, Saltillo, Mexico
Cervical cancer (CC) occupies the second place in incidence and mortality among women in México. Despite this, Cervical Cancer continues to have a late diagnosis which leads to a high rate of complications. Pain represents the most feared and disabling symptom, being present in up to 86% of patients with advanced disease. The approach to managing pain in this population has not been studied and described to a full extent. In addition, there is a pressing need to provide concise recommendations to promote adequate pain control. We performed a review of the literature in CC and had experts in the field of pain management evaluate the evidence found. We then issued relevant recommendations on pharmacology and interventional pain management. Thus, the approach to pain management must be comprehensive and individualized, considering the timely and appropriate use of pharmacologic treatment as well as interventional procedures.
1 Introduction
CC is potentially treatable, if detected during the early stages of the disease; however, despite advances in screening and treatment, it remains a leading cause of cancer death among women worldwide, as reported by GLOBOCAN 2020. In Mexico, it is the second leading cause of incidence and mortality in women (1). Diagnosis of cancer in advanced stages often results in severe complications and debilitating symptoms for the affected individual. Among these symptoms, pain is predominant, affecting approximately 86% of patients with advanced-stage cancer, 59% with locally advanced cancer, and up to 33% of cancer survivors (2, 3). The adequate management of pain in these patients continues to be a challenge potentially leading to emotional and physical distress, as well as a lack in quality of life (4–6). The International Association for the Study of Pain (IASP) definition of pain from 2020 provides valuable guidance in identifying pain (7). It is defined as an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage. Also taking into account the following points:
- Pain is always a personal experience influenced by biological, psychological, and social factors.
- Pain and nociception are different phenomena. Pain cannot be inferred from activity in sensory neurons.
- Through their life experiences, individuals learn the concept of pain.
- A person’s report of an experience as pain should be respected.
- Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
- Verbal description is only one of several behaviors to express pain; inability to communicate does not negate the possibility that a human or a nonhuman animal experiences pain.
Each patient’s experience of pain is unique, mandating a comprehensive evaluation. The intensity and characteristics of pain can be evaluated using several scales and questionnaires (8). These instruments assist in categorizing the type of pain, including neuropathic, nociceptive (somatic and visceral) as observed in CC patients. Commonly employed scales include the visual analog scale (VAS), numeric rating scale (NRS), and verbal rating scale (VRS). Questionnaires, like the McGill Pain Questionnaire and the Douleur Neuropathique-4 (DN4), can help identify neuropathic pain (9).
CC patients may suffer from nociceptive pain, neuropathic pain and mixed pain. Pain may originate from tumor invasion to viscera in the pelvic cavity, as well as infiltration to nearby tissue, nervous plexuses, peripheral nerves and even lead to bone metastasis in some cases. It is not uncommon for patients with CC to undergo certain procedures during their treatment like placement of percutaneous nephrostomies in order to improve renal function, unfortunately these procedures are associated with discomfort and pain. Lastly treatments used in CC may also be an important source of pain (10).
Radiation therapy (RT) has become a fundamental part in CC treatment and has increased survival rates among this group of patients. It may however be a potential cause of acute and in some instances, chronic pain. Damage of deoxyribonucleic acid (DNA) is one of the mechanisms of action of RT causing irreversible damage to cancer cells, it also induces an increase of several pro-inflammatory cytokines (TNF-alpha, IL-6, TGF-B and others), thus causing damage to nearby healthy tissue as well. Tissue with rapid cellular turnover as is the case with the epidermis and the gastrointestinal mucosa can be affected in an acute manner, presenting with dermatitis or acute enteritis. Other tissue with slow turnover like nerves may present with late adverse effects. In the case of CC, patients primarily present pain due to enteritis, dermatitis and neuropathic pain which may include radiation-induced plexitis (11, 12).. Chemotherapy plays a key role in CC, treatment, unfortunately these drugs may lead to microtubule disruption, mitochondrial damage, altered ion channel activity, neuroinflammation and myelin sheath destruction. Up to 68.1%, 60%, and 30% in the first, third, and sixth months after chemotherapy, respectively may present chemotherapy-induced peripheral neuropathy (CIPN). Platinum-based drugs (70–100%) and taxanes (up to 87%) pose the highest risk in CIPN development and drugs like paclitaxel can cause an acute neuropathy within days after each dose (13, 14).
Despite the available resources for pain management in cancer patients, there is a lack of specific guidance for Cervical and Uterine cancer (CUC) patients. This review aims to develop evidence-based recommendations to provide clinicians insight on the available treatments to effectively manage pain in CC patients, improving their quality of life and overall well-being.
2 Methods
A comprehensive literature review investigated existing approaches for managing pain in CC patients. The search terms “Cervix Cancer”, “Uterine Cervix Cancer”, “Pain”, “Cervix Cancer”, “Cancer Pain”, “Treatment”, “Opioids”, and “Interventional Pain” were utilized in PubMed. The goal was to focus on pelvic cancer pain, particularly in cervical cancer patients, as this area is often overlooked, the search included articles published in the year 2000 onward. After an initial screening of titles and abstracts, two authors pre-selected articles that met inclusion criteria. Subsequently, experts in the field of pain management evaluated the information using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) to identify the most relevant and current literature. Studies such as clinical cases, case series, letters to the editor, blocking technique descriptions, animal experiments, and those deemed weak recommendations or insufficient evidence were excluded. Out of 1251 articles found in PubMed, 25 were chosen for in-depth review, with 11 subsequently deemed most relevant by an expert panel. These articles are summarized in Table 1. Based on this review, specific recommendations were developed for pharmacological and interventional treatments and potential complications associated with the therapy.
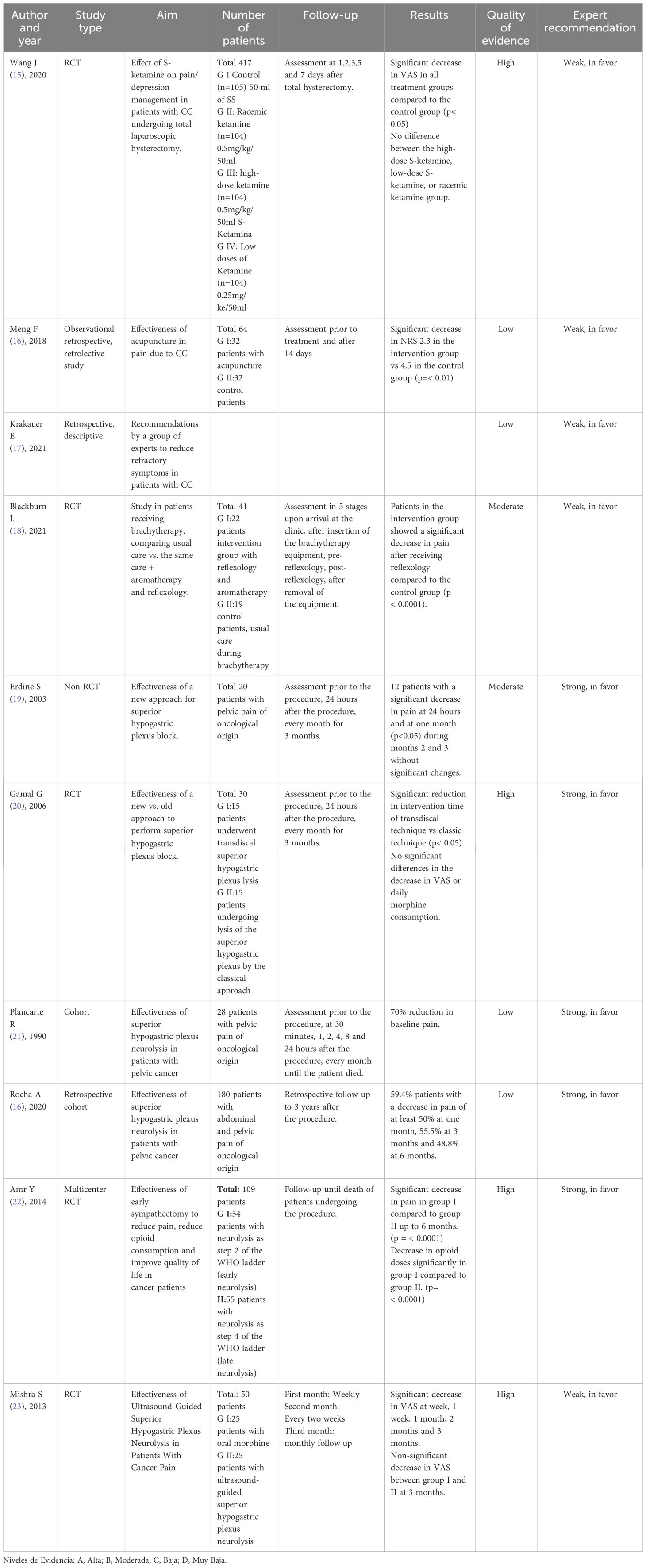
Table 1 Evaluation of the quality of studies on pain in cervical cancer.
3 Results
3.1 Pain treatment in CC
In 1986, the World Health Organization (WHO) introduced the analgesic ladder to guide and standardize pain treatment for cancer patients. The first three steps of this ladder suggest suitable analgesics based on the pain intensity reported by the patient. Over the years the ladder has gone through changes to include minimally invasive procedures, such as epidural or intrathecal analgesia, peripheral nerve blocks, neuromodulation, ablative blocks, and other surgical techniques, which are commonly employed for managing pain, including pelvic pain in patients with CC (24–26). Despite these modifications, the WHO analgesic ladder still has fundamental gaps regarding the treatment of pain in cancer patients. For instance, it does not address the etiology of pain that can be present and focuses primarily on the intensity of pain to guide treatment.
3.1.1 Pharmacological treatment
Cancer pain management is specific to its type, intensity, and characteristics. Various classes of drugs are available for pain relief, including non-steroidal anti-inflammatory drugs (NSAIDs) (27, 28), acetaminophen, opioids, and adjuvants. NSAIDs and acetaminophen are used for mild pain, in the case of CC these medications are usually indicated in the early stages of the disease and when acute pain presents, for instance undergoing procedures like percutaneous nephrostomies or catheter placement. NSAIDS can also be administered in patients that present with musculoskeletal pain secondary to tumor invasion or in cases of acute dermatitis secondary to radiotherapy. A significant number of patients with CC may present with deterioration in renal function and NSAIDs should be used with caution, avoiding their chronic use. Opioids are typically used for moderate to severe pain, and their dosage is titrated as needed. Weak and strong opioids are indicated in the context of visceral pain, somatic pain (musculoskeletal involvement), neuropathic pain and mixed pain secondary to tumor invasion. Acute or chronic pain secondary to adverse events due to chemotherapy or radiotherapy like CIPN, enteritis, dermatitis and radiation-induced plexitis may also be treated with opioids (29–31). Adjuvants are medications that are not typically used for pain relief but have characteristics that help in pain management (32). They include tricyclic antidepressants, serotonin reuptake inhibitors, anticonvulsants, local anesthetics, NMDA receptor antagonists, topical therapies, corticosteroids, bisphosphonates, and cannabinoids. Adjuvants are generally used to treat neuropathic pain that appears after radiotherapy, chemotherapy and in cases of tumor infiltration as well (28, 33–37). (See Table 2)
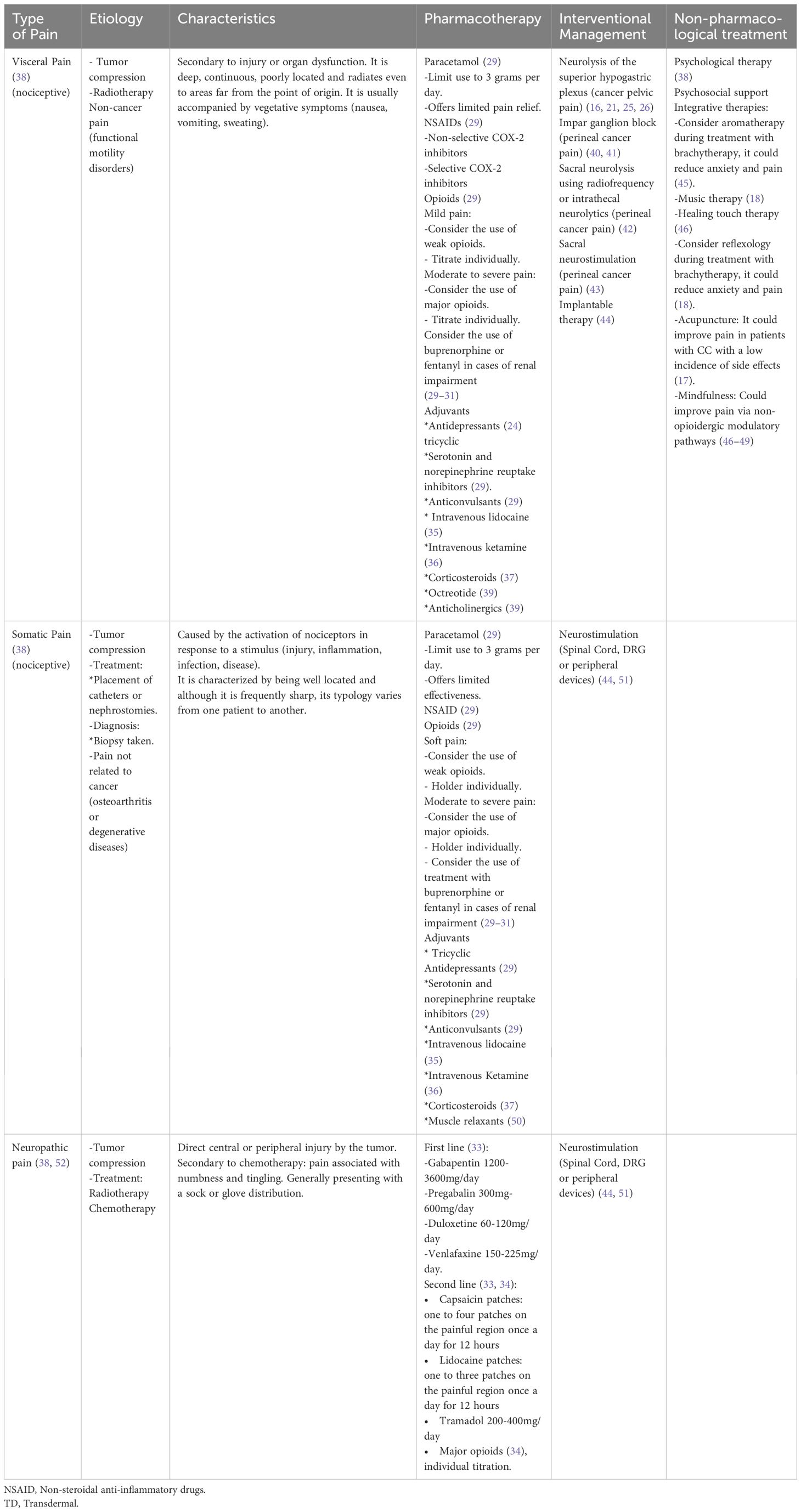
Table 2 Pain treatment approach in cervical cancer.
The treatment of cancer pain should consider not only the intensity of pain but also its type (nociceptive, neuropathic, or mixed) (38, 39). The medication and dosage should be tailored to the patient’s characteristics, cases of mixed pain generally require a combination of the available options described (24, 29). Patients with special conditions such as impaired kidney or liver function or constipation may need special considerations, such as the use of buprenorphine or fentanyl (30, 31, 53, 54). (See Table 2)
3.1.2 Interventional treatment
An important number of patients may experience adverse effects or inadequate response to the pharmacologic treatment available (32). Therefore, implementing interventional pain management strategies can be beneficial, aiming to enhance pain control and potentially reduce opioid consumption (16). Among patients with cancer pain, particularly those with visceral pain invading the pelvis, such as in CC, commonly used intervention procedures include the superior hypogastric plexus and the impar ganglion block. Both procedures were described in 1990 for the first time by Plancarte et al. They continue to be a useful intervention in early and advanced stages of CC for managing pelvic cancer pain, reducing opioid consumption and their possible side effects. In advanced stages of CC with retroperitoneal invasion, the trans-discal and transvascular approaches for performing superior hypogastric plexus neurolysis (SHPN) achieve similar effects (21, 25, 26, 45).
In many cases of CC, patients present with radiation of pain to the genital or perineal region. The impar ganglion is a single retroperitoneal structure near the sacrococcygeal junction, contributing to pelvic, genital, and perianal innervation. Consequently, since the initial description of the impar ganglion neurolysis in 1990, various techniques and substances have been used, aiming to alleviate pain in this anatomical region. This procedure has demonstrated pain relief of up to 70% in multiple studies (40). These interventions should be considered in most cases of CC, particularly in the early stages presenting with perineal pain. Appropriate execution of these procedures is essential for successful pain management (4, 40, 41).
Finally, it is crucial to execute a thorough evaluation of the patient before performing any of the procedures mentioned. A detailed physical exam directed toward determining the etiology and type of pain presented as well as a previous detailed inspection of imaging studies to determine the best approach in each particular case depending on tumor location and anatomical variations. Some of the absolute contraindications include patient refusal, local or systemic infections, allergies to any of the medications used during the procedure including contrast media, patients with coagulopathy (Platelet count < 50,000 and INR > 1.5), lack of technical experience performing any procedures mentioned and uncertainty regarding the patient´s diagnosis. It is also important to consider patients with neutropenia due to chemotherapy and potential risk of infection, patients that cannot tolerate the adequate position necessary to perform the procedure, bowel obstruction and to avoid puncture of the tumor. Patients under treatment with anticoagulants should also have medication suspended and restarted in a timely manner in order to avoid risk of bleeding. In general, the benefits of interventional procedures should always outweigh potential risks (55, 56). (See Table 2)
3.1.3 Integrative therapies
Anxiety, discomfort and pain are significant issues for patients with CC due to tumor activity and treatment undergone by these patients. Various non-pharmacological therapies have shown promise in alleviating symptoms associated with the disease or its treatment. Acupuncture, a minimally invasive technique, has effectively reduced pain in CC patients (17). Psychological therapy, reflexology, and aromatherapy have also been reported to provide relief from anxiety and pain, particularly before brachytherapy treatment (18, 57).
Other non-pharmacological approaches, such as meditation, music therapy, and tai chi, have also exhibited benefits in reducing pain, anxiety, depression, and stress in patients. These therapies, when combined with conventional pain management strategies, can offer a comprehensive approach with minimal side effects, making them suitable for consideration in the treatment of CC patients (17, 18, 57) (See Table 2).
4 Discussion
Pain in patients with CC is a prevalent and debilitating symptom affecting a large proportion of patients. Research has consistently highlighted the prevalence of cancer pain in cervical cancer patients. In 2007, a pain prevalence of 64% in advanced disease and 59% in locally advanced disease was reported. Subsequent studies in 2016 yielded similar results, 66.4% and 55%, respectively (3, 58). Current data (2, 59, 60) also indicates a wide range of pain prevalence, from 53.8% to 68%, across diverse populations, including the Mexican population. Approximately 96% of patients experience mild pain, while 84% report moderate to severe pain during the disease course (7).
Pain management in CC patients poses challenges for healthcare professionals. It requires individualized treatment plans encompassing pharmacological and non-pharmacological interventions (29, 33, 38, 50). The choice of treatment depends on the distinct types of pain experienced by the patient, the availability of medications, the patient’s resources, and the regional healthcare context. As mentioned, NSAIDs and Acetaminophen are usually used in cases of mild nociceptive pain that may be secondary to tumor activity or as an adverse event as is the case of acute dermatitis after radiotherapy or after catheter or percutaneous nephrostomy placement. Opioids, due to their effectiveness, ease of titration, and favorable risk-benefit profile, constitute the mainstay of pharmacological pain management in patients with moderate to severe cancer pain secondary to tumor invasion of viscera in the pelvic cavity, the musculoskeletal system and nerves that may be compromised. In the case of neuropathic pain secondary to tumor invasion, chemotherapy or radiotherapy opioids are the second or in some cases the third line of choice (15, 52, 61–63). There is a lack of non-inferiority studies comparing the efficacy of different opioids in CC. The selection of an appropriate opioid should consider various barriers that influence access and availability, including regulatory and legal restrictions, knowledge gaps, and economic constraints as well as comorbidities such as renal failure that may limit the use of some of these analgesics (29, 64, 65).
Adjuvant therapies like antidepressants, gabapentinoids, lidocaine or ketamine infusions are often employed to address neuropathic and mixed pain in locally advanced and advanced cervical cancer, as mentioned before these medications are widely used not only in neuropathic pain secondary to tumor infiltration but also to treat possible painful adverse events that arise from chemotherapy and radiotherapy.
Pain management in CC is frequently complicated and occasionally challenging to control using pharmacological treatments. Consequently, interventional therapies, such as SHPN, are used. SHPN was first described as a traditional technique by Plancarte et al. in 1990, along with two alternative approaches (trans-discal and transvascular) (21, 26). Erdine et al. in 2003 describes in depth the trans-discal approach; offering a significantly faster procedure with similar results as the classic approach (19). WHO suggests SHPN and other interventional procedures as a final resort in pain management, a study by Amr Y et al. in 2014 showed significant pain relief and reduced opioid consumption when performed in patients with pelvic cancer pain during early stages of disease (22). In 2015 a systematic review by Mercadante et al. suggested a low recommendation level for SHPN due to the scarcity of high-quality studies. Recent research (Rocha et al., 2020 and Pérez-Moreno et al., 2020) however, indicates that SHPN is an effective technique for managing oncological pelvic pain (4, 16, 66).
Technological advances have led to novel pain management techniques, such as ultrasonography in SHPN, proving safer for cancer pain patients (23, 67). Similar pain relief and a lower rate of severe side effects have been observed using ablative radiofrequency compared to chemical neurolysis for sacral nerve pain (42). Moreover, pulsed radiofrequency combined with SHPN at the sacral level enhanced pain relief without increased adverse effects (43). Additionally, intrathecal therapies and neurostimulation devices have shown promising results in cancer pain management (44, 51). However, more controlled studies in patients with CC are needed to explore the full efficacy of these treatments, and this is an area of opportunity for future research.
Non-pharmacological therapies, including psychosocial support and integrative therapies (mindfulness, tai chi, acupuncture among others), offer additional pain relief in patients with CC when used alongside pharmacological and interventional measures. These therapies have effectively provided relief with minimal side effects, making them suitable as complementary support therapies for this patient population (17, 18, 32, 38, 46). In the case of mindfulness, studies using magnetic resonance imaging have allowed the identification of different areas of the brain involved in the perception and modulation of pain after such therapies. These areas identified include the orbitofrontal cortex, the anterior cingulate cortex and the anterior insular cortex. Mindfulness meditation appears to not only target pain via multiple unique non-opioidergic modulatory pathways but to also mitigate the psychological risks of developing opioid use disease, therefore this could prove useful in providing a more adequate pain control in CC patients and in avoiding opioid misuse in this population (46–49).
4.1 Recommendations
Pharmacologic treatment:
1) Use acetaminophen to start treatment in cases of mild pain. 1C
2) Use of NSAIDs to start treatment in mild to moderate pain or inflammatory process. 2C
3) Use of acetaminophen and weak opioids in mild to moderate pain. 2C
4) Use morphine as the first option in cases of moderate to severe pain. Consider the use of another significant opioid if morphine is not available. 1A
5) Opioid titration must be carried out on an individualized basis. 1A
6) In case of breakthrough pain, use transmucosal Fentanyl. Use of fentanyl is also recommended in cases of opioid tolerance. 2A
7) Make use of neuromodulators (gabapentinoids, tricyclic antidepressants, serotonin and norepinephrine reuptake inhibitors, local anesthetics, and ketamine) in cases of neuropathic or mixed pain. 1A
8) Indicate prophylactic treatment for nausea and timely treatment in case of other events—adverse events associated with opioids. 1A
Interventional therapy:
9) Employ early interventional approaches to control pain: Neurolysis of the superior hypogastric plexus and impar ganglion. 1A
10) Use of implantable therapy and neurostimulators. 2B
Non-pharmacologic therapy:
11) Integrative therapies (aromatherapy, reflexology, acupuncture, mindfulness) can play a role as adjuvants for pain control. 2C
5 Conclusion
Effective pain management in cervical cancer patients necessitates a comprehensive and individualized approach. A thorough assessment of the pain characteristics is paramount in selecting targeted treatments. Timely management of potential side effects is crucial for optimal outcomes.
Author contributions
SA-R: Investigation, Writing – original draft, Writing – review & editing. RP-S: Supervision, Writing – original draft, Writing – review & editing. BH-P: Writing – original draft, Writing – review & editing. JG-A: Writing – review & editing. BL-V: Writing – review & editing. IR-T: Writing – review & editing. SA-B: Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The author(s) received financial support from ROCHE Mexico for the publication of this article. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Allende-Perez S, Dominguez-Ocadio G, Velez-Salas V, Isla-Ortiz D, Peña-Nieves A, Verastegui E. Snapshot of symptoms of advanced cervical cancer patients referred to the palliative care service in a cancer center in Mexico. Int J Gynecol Obstet. (2021) 153:335–9. doi: 10.1002/ijgo.13479
3. van den Beuken-van Everdingen MHJ, de Rijke JM, Kessels AG, Schouten HC, van Kleef M, Patijn J. Prevalence of pain in patients with cancer: A systematic review of the past 40 years. Ann Oncol. (2007) 18:1437–49. doi: 10.1093/annonc/mdm056
4. Mercadante S, Klepstad P, Kurita GP, Sjøgren P, Giarratano A. Sympathetic blocks for visceral cancer pain management: A systematic review and EAPC recommendations. Crit Rev Oncol Hematol. (2015) 96:577–83. doi: 10.1016/j.critrevonc.2015.07.014
5. Deandrea S, Montanari M, Moja L, Apolone G. Prevalence of undertreatment in cancer pain. A review of published literature. Ann Oncol. (2008) 19:1985–91. doi: 10.1093/annonc/mdn419
6. Breivik H, Cherny N, Collett B, de Conno F, Filbet M, Foubert AJ, et al. Cancer-related pain: A pan-European survey of prevalence, treatment, and patient attitudes. Ann Oncol. (2009) 20:1420–33. doi: 10.1093/annonc/mdp001
7. Krakauer EL, Kwete X, Kane K, Afshan G, Bazzett-Matabele L, Bien-Aimé DDR, et al. Cervical cancer-associated suffering: estimating the palliative care needs of a highly vulnerable population. JCO Glob Oncol. (2021) 7:862–72. doi: 10.1200/GO.21.00025
8. Vicente Herrero MT, Delgado Bueno S, Bandrés Moyá F, Ramírez Iñiguez de la Torre MV, Capdevila García L. Pain assessment. Comparative review of scales and questionnaires. Rev Soc Esp Dolor. (2018) 25:228–36. doi: 10.20986/resed.2018.3632/2017
9. Oosterling A, te Boveldt N, Verhagen C, van der Graaf WT, Van Ham M, van der Drift M, et al. Neuropathic pain components in patients with cancer: prevalence, treatment, and interference with daily activities. Pain Pract. (2016) 16:413–21. doi: 10.1111/papr.12291
10. Caraceni A, Shkodra M. Cancer pain assessment and classification. Cancers (Basel). (2019) 11:510. doi: 10.3390/cancers11040510
11. Karri J, Lachman L, Hanania A, Marathe A, Singh M, Zacharias N, et al. Radiotherapy-specific chronic pain syndromes in the cancer population: an evidence-based narrative review. Adv Ther. (2021) 38:1425–46. doi: 10.1007/s12325-021-01640-x
12. Chua GWY, Vig PS. Overview of radiotherapy-induced chronic pain in childhood cancer survivors: A narrative review. Paediatr Neonatal Pain. (2023) 5:1–9. doi: 10.1002/pne2.12094
13. D'Souza RS, Alvarez GAM, Dombovy-Johnson M, Eller J, Abd-Elsayed A. Evidence-based treatment of pain in chemotherapy-induced peripheral neuropathy. Curr Pain Headache Rep. (2023) 27:99–116. doi: 10.1007/s11916-023-01107-4
14. Aguiar-Rosas S, Plancarte-Sanchez R, Hernandez-Porras BC, García-Andreu J, Lezcano-Velazquez BO, Alarcón-Barrios S, et al. Chemotherapy-induced neuropathy in cancer survivors. J Pain Symp Manage. (2017) 54:204–218.e2. doi: 10.1016/j.jpainsymman.2016.12.342
15. Wang J, Wang Y, Xu X, Peng S, Xu F, Liu P. Use of various doses of S-ketamine in treatment of depression and pain in cervical carcinoma patients with mild/moderate depression after laparoscopic total hysterectomy. Med Sci Monit. (2020) 26:1–6. doi: 10.12659/MSM.922028
16. Rocha A, Plancarte R, Natarén RGR, Carrera IHS, Pacheco VALR, Hernández-Porras BC. Effectiveness of superior hypogastric plexus neurolysis for pelvic cancer pain. Pain Phys. (2020) 23:203–8.
17. Meng FF, Feng YH. A pilot study of acupuncture at pain acupoints for cervical cancer pain. Medicine. (2018) 97:e13736. doi: 10.1097/MD.0000000000013736
18. Blackburn L, Hill C, Lindsey AL, Sinnott LT, Thompson K, Quick A. Effect of foot reflexology and aromatherapy on anxiety and pain during brachytherapy for cervical cancer. Oncol Nurs Forum. (2021) 48:265–76. doi: 10.1188/21.ONF.265-276
19. Erdine S, Yucel A, Celik M, Talu GK. Transdiscal approach for hypogastric plexus block. Reg Anesth Pain Med. (2003) 28:304–8. doi: 10.1097/00115550-200307000-00009
20. Gamal G, Helaly M, Labib YM. Superior hypogastric block: Transdiscal versus classic posterior approach in pelvic cancer pain. Clin J Pain. (2006) 22:544–7. doi: 10.1097/01.ajp.0000202978.06045.24
21. Plancarte R, Amescua C. Superior hypogastric plexus block for pelvic cancer pain. Anesthesiology. (1990) 73:236–9. doi: 10.1097/00000542-199008000-00008
22. Amr YM, Makharita MY. Neurolytic sympathectomy in the management of cancer pain-time effect: a prospective, randomized multicenter study. J Pain Symp Manage. (2014) 48:944–56. doi: 10.1016/j.jpainsymman.2014.01.015
23. Mishra S, Bhatnagar S, Rana SP, Khurana D, Thulkar S. Efficacy of the anterior ultrasound-guided superior hypogastric plexus neurolysis in pelvic cancer pain in advanced gynecological cancer patients. Pain Med. (2013) 14:837–42. doi: 10.1111/pme.12106
24. Ventafridda V. WHO guidelines for the use of analgesics in cancer pain. Int J Tissue React. (1985) 7:93–6.
25. De Oliveira R, Dos Reis MP, Prado WA. The effects of early or late neurolytic sympathetic plexus block on the management of abdominal or pelvic cancer pain. Pain. (2004) 110:400–8. doi: 10.1016/j.pain.2004.04.023
26. Plancarte-Sánchez R, Leon-Casasola O, El-Helaly M, Allende S, Lema MJ. Neurolytic superior hypogastric plexus block for chronic pelvic pain associated with cancer. Reg Anesth. (1997) 22:562–8. doi: 10.1136/rapm-00115550-199722060-00012
27. Tielemans MM, Eikendal T, Jansen JB, van Oijen MG. Identification of NSAID users at risk for gastrointestinal complications: a systematic review of current guidelines and consensus agreements. Drug Saf. (2010) 33:443–53. doi: 10.2165/11534590-000000000-00000
28. Roumie C, Choma N, Kaltenbach L, Mitchel E, Arbogast P, Griffin M. Non-aspirin NSAIDs, cyclooxygenase-2 inhibitors and risk for cardiovascular events–stroke, acute myocardial infarction, and death from coronary heart disease. Pharmacoepidemiol Drug Saf. (2009) 18:1053–63. doi: 10.1002/pds.1820
29. Cervical Cancer. National Comprehensive Cancer Network. (NCCN Guidelines). Adult Cancer Pain Guidelines. version 1.2023, march 7,2023. NCCN.org. NCCN Guidelines Panel Disclosures.
30. Clark AJ, Ahmedzai SH, Allan LG, Camacho F, Horbay GL, Richarz U, et al. Efficacy and safety of transdermal fentanyl and sustained-release oral morphine in patients with cancer and chronic non-cancer pain. Curr Med Res Opin. (2004) 20:1419–28. doi: 10.1185/030079904X2114
31. Melilli G, Samolsky Dekel BG, Frenquelli C, Mellone R, Pannuti F. Transdermal opioids for cancer pain control in patients with renal impairment. J Opioid Manage. (2014) 10:85–93. doi: 10.5055/jom.2014.0197
32. Müller-Schwefe G, Ahlbeck K, Aldington D, Alon E, Coaccioli S, Coluzzi F, et al. Pain in the cancer patient: different pain characteristics CHANGE pharmacological treatment requirements. Curr Med Res Opin. (2014) 30:1895–908. doi: 10.1185/03007995.2014.925439
33. Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R, Dworkin RH, et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. (2015) 14:162–73. doi: 10.1016/S1474-4422(14)70251-0
34. Moulin D, Boulanger A, Clark AJ, Clarke H, Dao T, Finley GA, et al. Canadian Pain Society. Pharmacological management of chronic neuropathic pain: revised consensus statement from the Canadian Pain Society. Pain Res Manage. (2014) 19:328–35. doi: 10.1155/2014/754693
35. Ferrini R, Paice JA. How to initiate and monitor infusional lidocaine for severe and neuropathic pain. J Support Oncol. (2004) 2:90–4.
36. Mercadante S, Arcuri E, Tirelli W, Casuccio A. Analgesic effect of intravenous ketamine in cancer patients on morphine therapy: A randomized, controlled, double-blind, crossover, double-dose study. J Pain Symp Manage. (2000) 20:246–52. doi: 10.1016/S0885-3924(00)00194-9
37. Haywood A, Good P, Khan S, Leupp A, Jenkins-Marsh S, Rickett K, et al. Corticosteroids for the management of cancer-related pain in adults. Cochrane Database Syst Rev. (2015) 2015:CD010756. doi: 10.1002/14651858.CD010756.pub2
38. Smith TJ, Saiki CB. Cancer pain management. Mayo Clin Proc. (2015) 90:1428–39. doi: 10.1016/j.mayocp.2015.08.009
39. Davis MP. Drug management of visceral pain: concepts from basic research. Pain Res Treat. (2012) 2012:265605. doi: 10.1155/2012/265605
40. Gomaa Ahmed D, Ahmed DG, Mohamad MF, Abd-Elbaky Mohamed S. Case series superior hypogastric plexus combined with ganglion impar neurolytic blocks for pelvic and/or perineal cancer pain relief. Pain Phys. (2015) 18:49–56.
41. Cortiñas M, Martín TM, Vara C, Salmeron J, Villalba FG. Eficacia del bloqueo del ganglio impar en dolor pélvico y perineal de etiología ginecológica rebelde a tratamiento médico-quirúrgico. Clin Invest Ginecol Obstet. (2011) 38:95–9. doi: 10.1016/j.gine.2010.10.010
42. Reyad RM, Hakim SM, Abbas DN, Ghobrial HZ, Mansour E. A novel technique of saddle rhizotomy using thermal radiofrequency for intractable perineal pain in pelvic Malignancy: A pilot study. Pain Phys. (2018) 21:E651–60.
43. Hetta DF, Mohamed AA, Abdel Eman RM, Abd El Aal FA, Helal ME. Pulsed radiofrequency of the sacral roots improves the success rate of superior hypogastric plexus neurolysis in controlling pelvic and perineal cancer pain. Pain Phys. (2020) 23:149–57. doi: 10.36076/ppj
44. Magee DJ, Schutzer-Weissmann J, Pereira EAC, Brown MRD. Neuromodulation techniques for cancer pain management. Curr Opin Support Palliat Care. (2021) 15:77–83. doi: 10.1097/SPC.0000000000000549
45. Krakauer EL, Kane K, Kwete X, Afshan G, Bazzett-Matabele L, Ruthnie Bien-Aimé DD, et al. Essential package of palliative care for women with cervical cancer: responding to the suffering of a highly vulnerable population. JCO Glob Oncol. (2021) 7:873–85. doi: 10.1200/GO.21.00026
46. Greenlee H, DuPont-Reyes MJ, Balneaves LG, Carlson LE, Cohen MR, Deng G, et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin. (2017) 67:194–232. doi: 10.3322/caac.21397
47. Jinich-Diamant A, Garland E, Baumgartner J, Gonzalez N, Riegner G, Birenbaum J, et al. Neurophysiological mechanisms supporting mindfulness meditation-based pain relief: an updated review. Curr Pain Headache Rep. (2020) 24:56. doi: 10.1007/s11916-020-00890-8
48. Zeidan F, Baumgartner JN, Coghill RC. The neural mechanisms of mindfulness-based pain relief: a functional magnetic resonance imaging-based review and primer. Pain Rep. (2019) 4::e759. doi: 10.1097/PR9.0000000000000759
49. Lu C, Moliadze V, Nees F. Dynamic processes of mindfulness-based alterations in pain perception. Front Neurosci. (2023) 17:1253559. doi: 10.3389/fnins.2023.1253559
50. Lussier D, Huskey AG, Portenoy RK. Adjuvant analgesics in cancer pain management. Oncologist. (2004) 9:571–91. doi: 10.1634/theoncologist.9-5-571
51. Abdullah N, Sindt JE, Whittle J, Anderson JS, Odell DW, Mahan M, et al. Impact of neuromodulation on opioid use, adjunct medication use, and pain control in cancer-related pain: a retrospective case series. Pain Med. (2023) 24:903–6. doi: 10.1093/pm/pnad001
52. Yoon SY, Oh J. Neuropathic cancer pain: prevalence, pathophysiology, and management. Korean J Intern Med. (2018) 33:1058–69. doi: 10.3904/kjim.2018.162
53. Tassinari D, Sartori S, Tamburini E, Scarpi E, Tombesi P, Santelmo C, et al. Transdermal fentanyl as a front-line approach to moderate-severe pain: a meta-analysis of randomized clinical trials. J Palliat Care. (2009) 25:172–80. doi: 10.1177/082585970902500304
54. Swarm RA, Paice JA, Anghelescu DL, Are M, Bruce JY, Buga S, et al. Adult cancer pain, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2019) 17:977–1007. doi: 10.6004/jnccn.2019.0038
55. Kaye AD, Manchikanti L, Novitch MB, Mungrue IN, Anwar M, Jones MR, et al. Responsible, safe, and effective use of antithrombotics and anticoagulants in patients undergoing interventional techniques: American society of interventional pain physicians (ASIPP) guidelines. Pain Phys. (2019) 22:S75–S128.
56. Bhatnagar S, Gupta M. Evidence-based clinical practice guidelines for interventional pain management in cancer pain. Indian J Palliat Care. (2015) 21:137–47. doi: 10.4103/0973-1075.156466
57. Kebebew T, Mavhandu-Mudzusi AH, Mosalo A. A cross-sectional assessment of symptom burden among patients with advanced cervical cancer. BMC Palliat Care. (2021) 20:1–10. doi: 10.1186/s12904-021-00883-3
58. Van Den Beuken-Van Everdingen MHJ, Hochstenbach LMJ, Joosten EAJ, Tjan-Heijnen VCG, Janssen DJA. Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symp Manage. (2016) 51:1070–90. doi: 10.1016/j.jpainsymman.2015.12.340
59. Rogers E, Mehta S, Shengelia R, Reid MC. Four strategies for managing opioid-induced side effects in older adults. Clin Geriatr. (2013) 21:1–14.
60. Kuguyo O, Misi FD, Chibonda S, Matimba A, Nhachi C, Tsikai N. Pain management strategies among cervical cancer patients in Zimbabwe. Pain Manage. (2021) 11:715–29. doi: 10.2217/pmt-2020-0108
61. Palat G, Biji MS, Rajagopal MR. Pain management in cancer cervix. Indian J Palliat Care. (2005) 11:64–73. doi: 10.4103/0973-1075.19182
62. Freynhagen R, Parada HA, Calderon-Ospina CA, Chen J, Rakhmawati Emril D, Fernández-Villacorta FJ, et al. Current understanding of the mixed pain concept: a brief narrative review. Curr Med Res Opin. (2019) 35:1011–8. doi: 10.1080/03007995.2018.1552042
63. Fernandez-Fairen M, Calderón-Ospina CA, Chen J, Duarte Vega M, Fernández-Villacorta F, Gómez-García F, et al. A Latin American consensus meeting on the essentials of mixed pain. Curr Med Res Opin. (2023) 39:451–66. doi: 10.1080/03007995.2023.2177401
64. Mawatari H, Shinjo T, Morita T, Kohara H, Yomiya K. Revision of pharmacological treatment recommendations for cancer pain: clinical guidelines from the Japanese society of palliative medicine. J Palliat Med. (2022) 25:1095–114. doi: 10.1089/jpm.2021.0438
65. WHO. Pain in Adults. Who Guidelines for the Pharmacological and Radiotherapeutic Manag. World Healt Organization. (2018). National Library of Medicine.
66. Pérez-Moreno DP, Plancarte-Sánchez R, Hernández-Porras C, Guillén-Núñez MR. Effectiveness of the superior hypogastric plexus neurolytic block in the management of pelvic abdominal pain in adult patients diagnosed with cancer: A systematic literature review. Rev Chil Anest. (2020) 49:813–21. doi: 10.25237/revchilanest
Keywords: cervix cancer, uterine cervix cancer, pain, cancer pain, treatment, opioids, interventional pain
Citation: Aguiar-Rosas S, Plancarte-Sanchez R, Hernandez-Porras BC, García-Andreu J, Lezcano-Velazquez BO, Reyes-Torres I and Alarcón-Barrios S (2024) Pain management in cervical cancer. Front. Oncol. 14:1371779. doi: 10.3389/fonc.2024.1371779
Received: 17 January 2024; Accepted: 01 April 2024;
Published: 25 April 2024.
Edited by:
Mwansa Ketty Lubeya, University of Zambia, ZambiaReviewed by:
Romina Rossi, University of Bologna, ItalyCopyright © 2024 Aguiar-Rosas, Plancarte-Sanchez, Hernandez-Porras, García-Andreu, Lezcano-Velazquez, Reyes-Torres and Alarcón-Barrios. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvia Alarcón-Barrios, c2lsdmlhYWxhcmNvbjIxQGhvdG1haWwuY29t