
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 31 January 2024
Sec. Pediatric Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1340099
 Sofia Wallin1
Sofia Wallin1 Ingrid Øra2Gabriela Prochazka3Johanna Sandgren3,4Caroline Björklund5Gustaf Ljungman6Hartmut Vogt7Torben Ek8
Ingrid Øra2Gabriela Prochazka3Johanna Sandgren3,4Caroline Björklund5Gustaf Ljungman6Hartmut Vogt7Torben Ek8 Cornelis M. van Tilburg9,10,11,12
Cornelis M. van Tilburg9,10,11,12 Anna Nilsson1,13*
Anna Nilsson1,13*Background: Advances in treatment of childhood malignancies have improved overall cure rates to 80%. Nevertheless, cancer is still the most common cause of childhood mortality in Sweden. The prognosis is particularly poor for relapse of high-risk malignancies. In the international INFORM registry, tumor tissue from patients with relapsed, refractory, or progressive pediatric cancer as well as from very-high risk primary tumors is biologically characterized using next-generation sequencing to identify possible therapeutic targets. We analyzed data from Swedish children included in the INFORM registry concerning patient characteristics, survival, sequencing results and whether targeted treatment was administered to the children based on the molecular findings.
Methods: A registry-based descriptive analysis of 184 patients included in the INFORM registry in Sweden during 2016–2021.
Results: The most common diagnoses were soft tissue and bone sarcomas followed by high grade gliomas [including diffuse intrinsic pontine glioma (DIPG)]. Complete molecular analysis was successful for 203/212 samples originating from 184 patients. In 88% of the samples, at least one actionable target was identified. Highly prioritized targets, according to a preset scale, were identified in 48 (24%) samples from 40 patients and 24 of these patients received matched targeted treatment but only six children within a clinical trial. No statistically significant benefit in terms of overall survival or progression free survival was observed between children treated with matched targeted treatment compared to all others.
Conclusion: This international collaborative study demonstrate feasibility regarding sequencing of pediatric high-risk tumors providing molecular data regarding potential actionable targets to clinicians. For a few individuals the INFORM analysis was of utmost importance and should be regarded as a new standard of care with the potential to guide targeted therapy.
Childhood cancer treatment has continuously improved with significant progress during recent years reaching approximately 80% overall survival. Indeed, survival rates have improved for all pediatric cancers; leukemias, central nervous system (CNS) tumors and other/extra cranial solid tumors and more so for children than for adolescents and adults (1, 2). Despite this achievement using optimized chemotherapy, local treatment with surgery and radiotherapy as well as optimization of supportive care, the prognosis for very high-risk and refractory cancers remains poor. Thus, cancer is still the most common cause of death among children in Sweden (3–5), where patients with relapsed disease encounter survival rates of less than 20%. Moreover, survivors are often facing serious (long term) side effects from current treatments such as cardiac complications, endocrine deficiencies, cognitive problems, and secondary cancers (3). Therefore, to develop more effective and less toxic treatments it is critical to include molecular sequencing to enable treatment with targeted therapy (reviewed in (4), (5)).
Research in the field of molecular biology has led to a significantly increased understanding of cancer biology. Analysis of tumor samples with next-generation sequencing techniques enabling development of new targeted therapies has opened possibilities to tailor individual treatment (6). Cancers in adults are often driven by mutations derived from long time exposure to diverse environmental factors. In contrast, most pediatric cancers carry relatively few background mutations which facilitate identification of tumor driving genetic alterations (7). Although it is yet difficult to draw firm therapeutic conclusions due to limited patient numbers and comparability challenges, this is an area of clinical research that needs to be investigated. Several studies are currently underway worldwide to provide robust data and address the clinical benefit of precision medicine in pediatric oncology (8, 9).
The INFORM program (INdividualized Therapy FOr Relapsed Malignancies in Childhood) was initiated in 2015 in Germany by the German Cancer Research Center (DKFZ) (10) with the aim to characterize tumor material from pediatric patients with treatment-resistant high-risk cancer. In the pilot study, the molecular profiling included whole-exome, low-coverage whole-genome, and RNA sequencing as well as methylation and expression microarray analyses. In parallel, an analytical pathway based on a prioritization algorithm was developed to ensure rapid reporting of potential therapeutic targets for clinical use. Early data from the INFORM program demonstrated the readily available possibilities to perform fast and comprehensive molecular analyses of tumor samples and paired blood samples, further enabling clinical decision-making and the initiation of adequate targeted therapies (10). A separate study also showed how to perform similar analyses on patients with DIPG (Diffuse intrinsic pontine glioma) (11). The INFORM pilot study also enlightened the clinical relevance of re-analysis in the case of tumor recurrence, as some showed significant biological evolution between primary tumor and relapse. It is well documented that genomic characterization of neuroblastomas at the time of diagnosis and at relapse may provide valuable clinical information (12, 13).
Approximately 300 to 350 Swedish children and adolescents (0–18 years of age) are annually diagnosed and treated for cancer at one of the six childhood cancer centers located at regional university hospitals. Approximately 25–30% each are treated in Stockholm and Gothenburg, 15–20% each in Uppsala and Lund and additionally 5–10% each in Linköping and Umeå. The aim of this analysis was to structure and visualize information on the Swedish patient cohort enrolled in the INFORM registry regarding clinical patient data, analysis of target genes and subsequent treatment. Moreover, the study aimed to investigate whether these results were implemented in clinical care of pediatric cancer patients on a national level. A potential clinical benefit of providing targeted treatment was also assessed in this first implementation of precision medicine in Swedish pediatric oncology.
The overall patient criteria for inclusion in the INFORM registry study are children and adolescents with treatment-resistant high-risk malignancies, i.e. recurring and/or refractory disease, as described in detail (10). Clinical diagnostic tumor material (retrieved via biopsy) and reference material (blood sample or buccal swab) were obtained; DNA and RNA were prepared at the Swedish Childhood Tumor Biobank (BTB) before shipment to the DKFZ in Heidelberg, Germany for molecular analyses.
The INFORM study for Swedish patients was approved 2016 by the Regional Ethical Review Board in Stockholm (Ref-nr 2016/1782-31) and updated 2022 (Ref-nr 2022-00646-02). The study was conducted in accordance with the declaration of Helsinki. Informed consent from patients and/or legal guardians was obtained before collection of biological material and registration in the study-associated MARVIN database. The study was registered with the German Clinical Trials Register, number DRKS00007623.
The sequencing results and potential targeted treatments were presented and discussed at the weekly INFORM Target decision board during a teleconference with participation of molecular biologists, pediatric oncologists, pharmacologists, the treating physician, and the national PI for the registry in Sweden.
Furthermore, the treating physician had the opportunity to discuss further with other Swedish oncologists or colleagues from the other Nordic countries regarding relevant and matching trials at weekly multidisciplinary videoconferences (NOPHO Match) on demand.
Patient data on sex, age and diagnosis were collected from the MARVIN database. Additional data of interest were time between shipping of tissue samples and presentation of the results at the INFORM target decision board, the origin of the malignant tissue sample, whether complete molecular analysis according to study protocol was performed, quantity and prioritization level (1–7) of identified targets and exact genetic alteration if priority 1–2. Data on whether patients received precision-based treatment and/or other oncological treatments, and survival status was collected from MARVIN.
The data/parts of the data from 217 tumor samples evaluated in this study were produced and kindly provided by the INFORM registry (10, 14). Age differences between groups were analyzed using Kruskal-Wallis test followed by multiple comparisons test and data are presented with median (range). Figures and tables were completed using GraphPad Prism.
The overall survival and progression-free survival were illustrated using Kaplan-Meier estimates. Difference between curves were tested using Log-Rank test. The analysis of progression-free survival was repeated using cumulative incidence and treating death as a competing risk to progression. Difference in cause-specific cumulative incidence function were analyzed using Gray’s test (15) and this was done using “R” (16).
Patient tumor samples (n=217) were included in the INFORM registry during 2016-2021 from six university hospitals treating children with cancer in Sweden: Karolinska University Hospital, Stockholm (n=79 samples), Uppsala University Children´s Hospital (n=29), Lund University Hospital (n=51), Queen Silvia Children’s Hospital, Gothenburg (n=34), Crown Princess Victoria Children’s Hospital, Linköping (n=12) and Norrland University Hospital, Umeå (n=12) (Figure 1). Five cases were not analyzed: four due to insufficient amount of tumor DNA/RNA and one for not meeting the inclusion criteria for the study. Twenty-five patients were registered at subsequent relapse(s) and thus, the study cohort involves 184 unique subjects. The reason for inclusion was due to cancer relapse in 147 children, refractory disease in 20 children and 17 children were included at primary diagnosis.
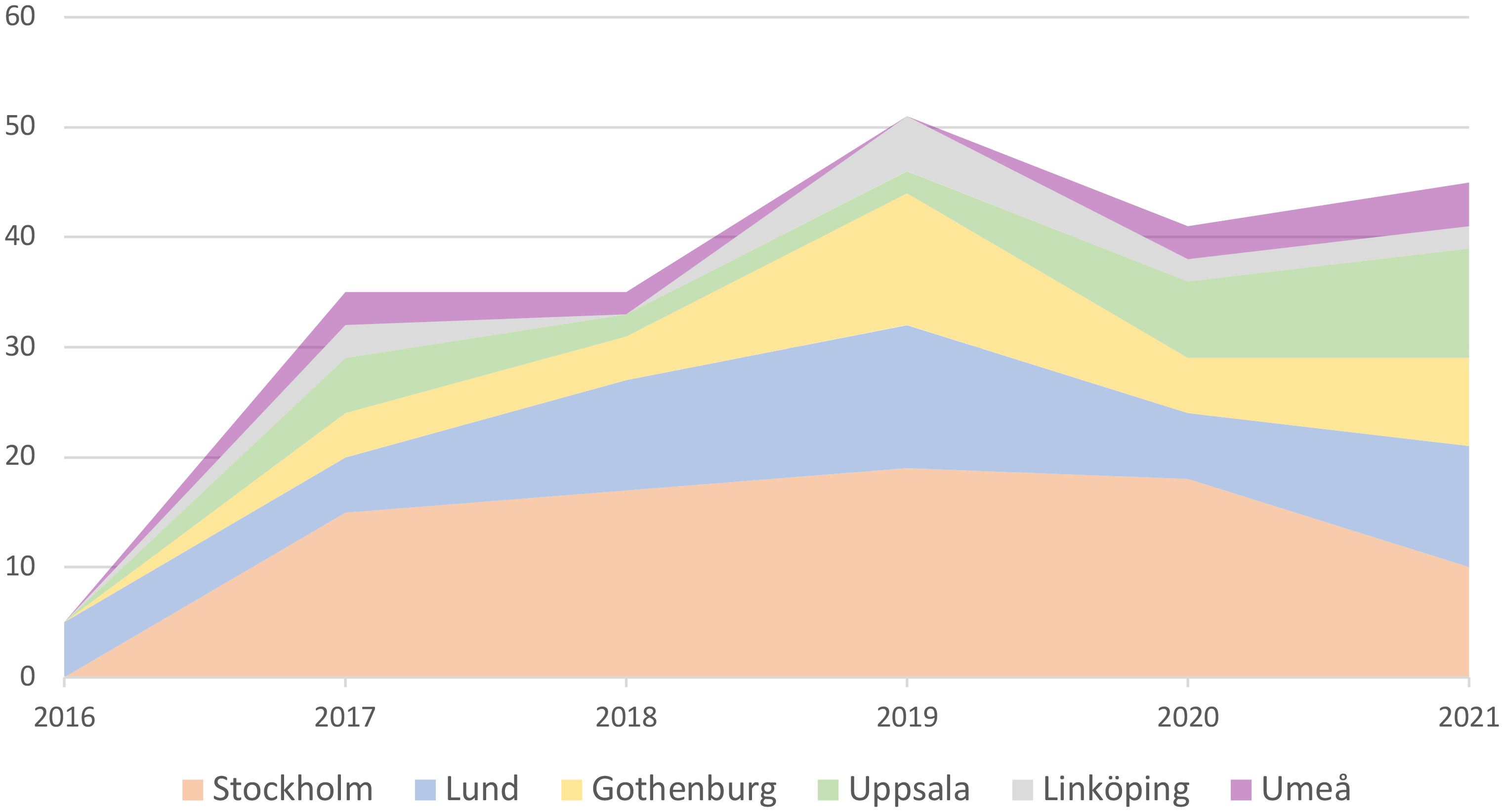
Figure 1 Inclusion rate in the INFORM registry from the six Swedish pediatric cancer centers 2016–2021, 18 cases were included at more than 1 relapse.
Patient characteristics are displayed in Table 1. The distribution of pediatric malignancies in the cohort was 62% solid tumors, 30% CNS tumors, 5% hematological malignancies and 3% others (Figures 2A, B). The small group “others” (3%) included children with infantile myofibromatosis, Langerhans cell histiocytosis and juvenile ossifying fibroma. The median age of the entire cohort was 13 years although 20 patients were older than 18 years, of which the primary diagnosis of the cancer had occurred at < 18 years of age. Children with solid tumors were significantly older than children in the group “others” [14 years (9-26) vs. 4 years (0-8), P=0.04]. The proportion of female patients was slightly higher than the proportion of male patients (53 vs. 47%), without any significant differences between groups. Twenty-two subjects were included twice, and three subjects were included three times. Most patients were included at relapse (80%) and the number of individual relapses varied between one and eight. The general condition of patients was assessed using the Karnofsky/Lansky score at inclusion and the median value was 90% for the whole cohort and the respective disease groups. This score decreased from the first inclusion in INFORM to the subsequent registrations at later relapse to a median of 80% (P>0.5).
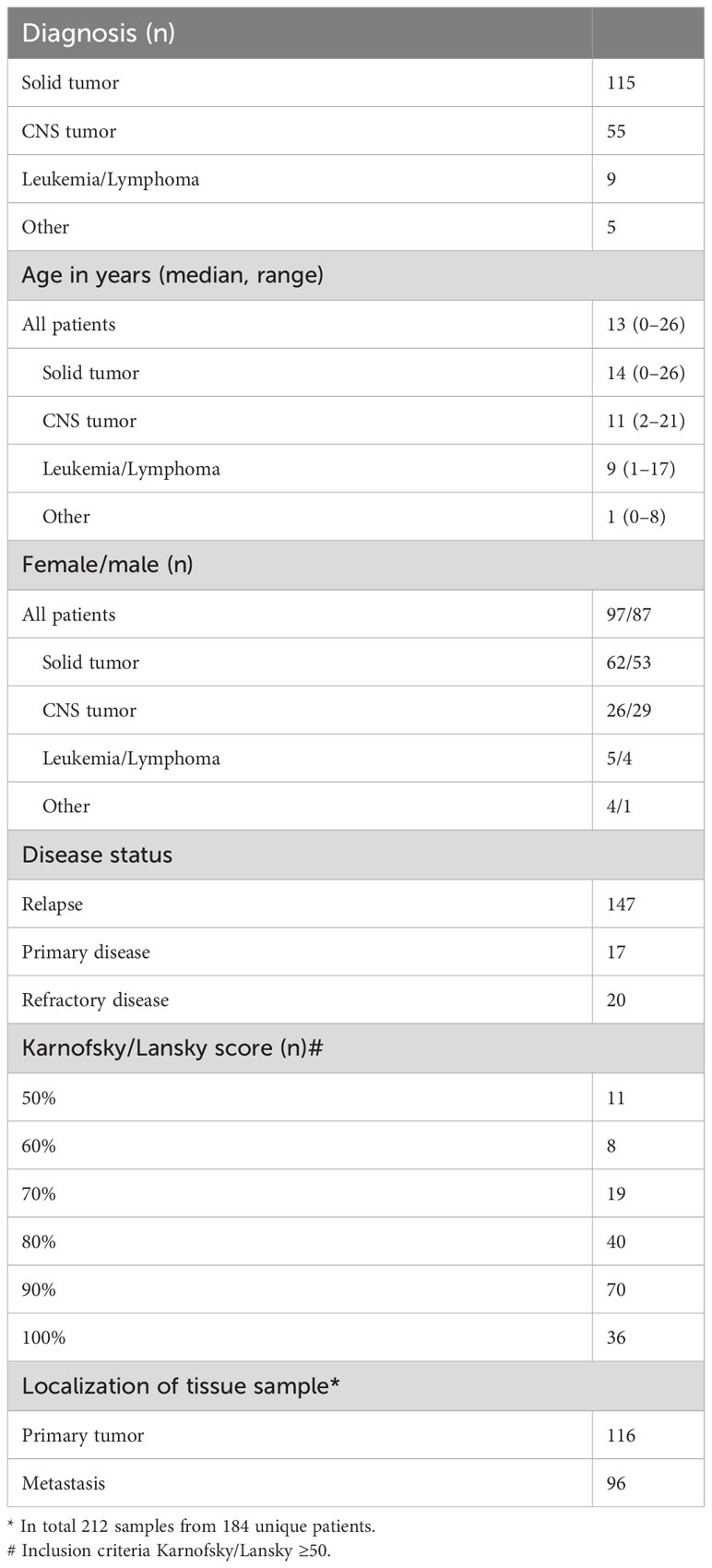
Table 1 Patient characteristics of 184 Swedish patients included in the INFORM registry 2016–2021.
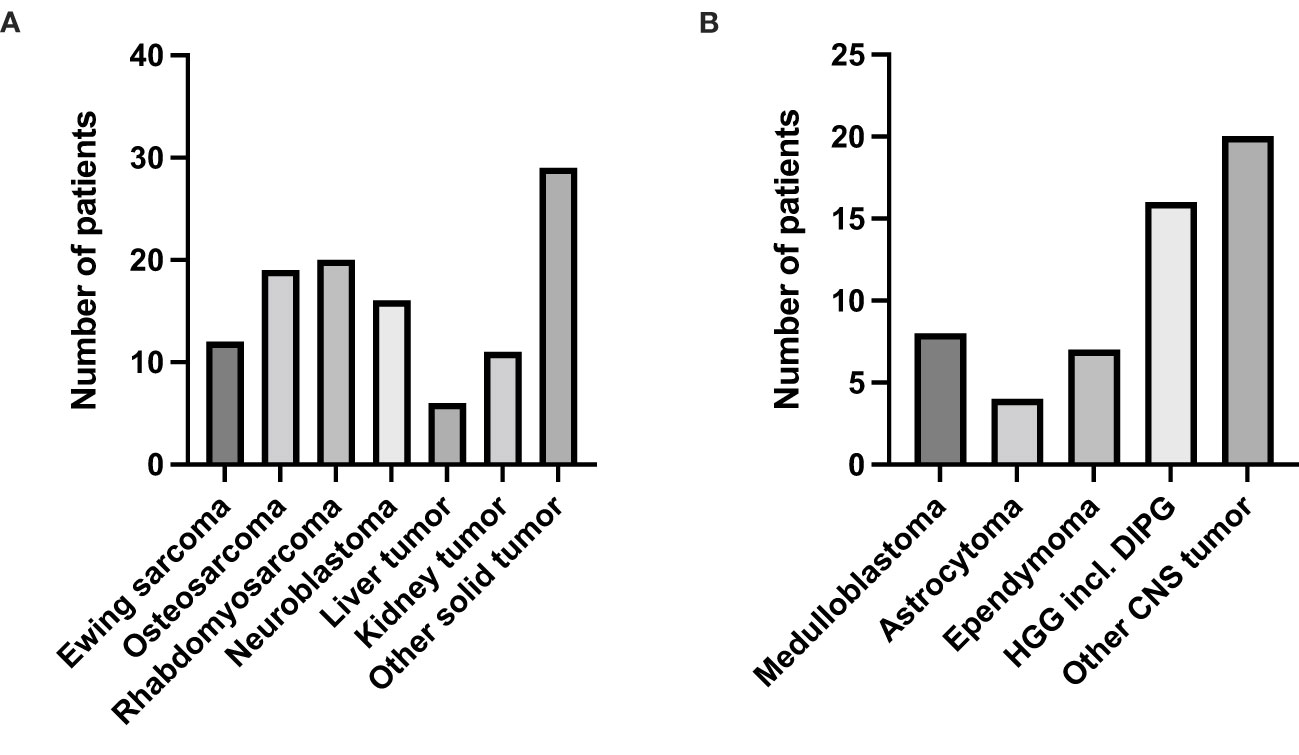
Figure 2 Diagnosis distribution in the two largest disease groups. (A) Number of patients with solid tumors. (B) Number of patients with CNS tumors.
The median turnover time, from shipment of tumor and reference DNA/RNA material to presentation at the INFORM target board was 28 days (range 16-105 days) for samples in the Swedish cohort. Complete molecular genetic analyses were performed on 203 out of 212 patient samples. Nine samples were not analyzed: six deaths occurred before sample analysis. Identified targets were classified according to a seven-grade scale prioritization algorithm by the INFORM registry interdisciplinary review board as previously described (10). At least one actionable target was found in 178 out of the 203 analyzed samples (88%) (corresponding to 157 unique patients) and the median value was 4 targets (range 0-12) per patient (Figure 3A). At least one actionable target with a priority score of 1-4 was reported for 110 individuals (60%) and a priority target score 1-2 (corresponding to very high and high) was reported in 48 samples (24%) corresponding to 40 unique patients (Figure 3B). The molecular alterations with a target score 1-2 are presented in Table 2. The most frequent level 1 gene targets (n=20) were NTRK (n=4), BRAF (n=6) and ALK (n=3). Targets with prioritization level 2 (n=28) were found in NRAS and KRAS (n=10), CDK4 (n=4) but also NTRK (n=2) and NF1 (n=5). It was also noted that the molecular profile of tumors could change between the first and subsequent analyses in INFORM (Supplementary Table 1).
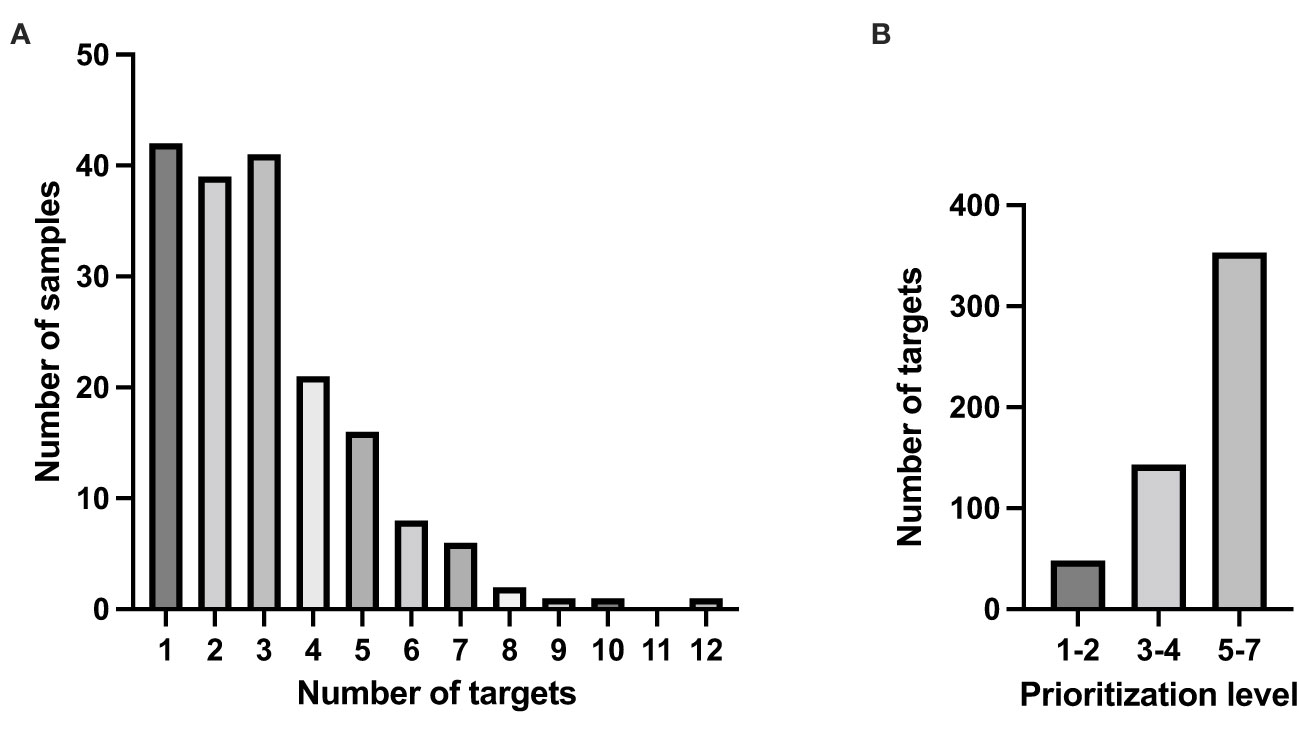
Figure 3 Number of defined targets for treatment in the Swedish study cohort. (A) Number of targets among the samples, median=4. (B) Number of targets with a prioritization level 1–2, 3–4 and 5–7.
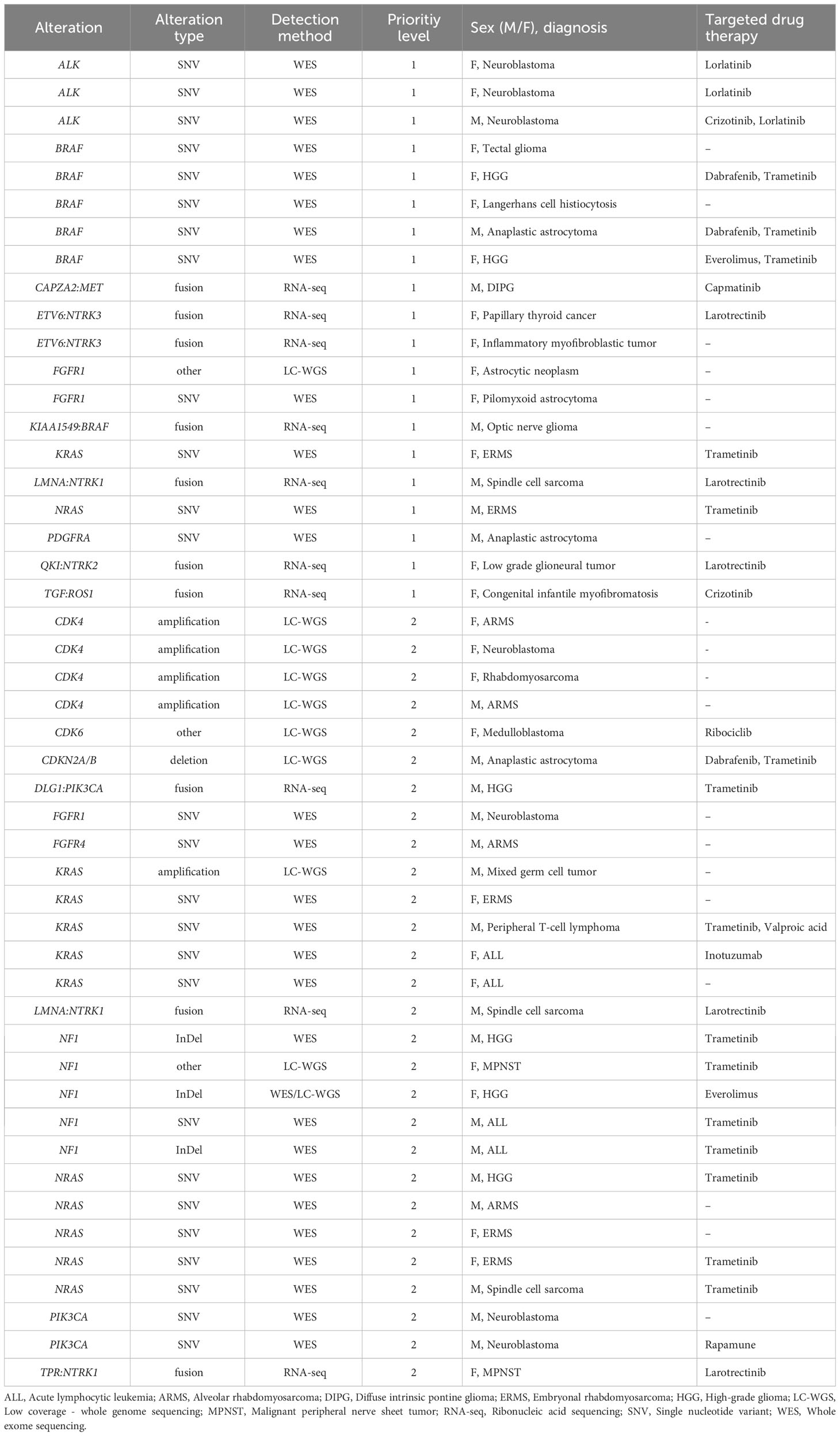
Table 2 Targets with priority level 1-2.
In total 70/184 patients (38%) were prescribed targeted treatment and 13 were included in a clinical phase I/II study based on the data generated from the INFORM registry. Among the 40 individuals with a highly prioritized target (level 1-2), 24 patients (60%) were prescribed targeted treatment based on the INFORM data. Out of the 24 patients, only six patients received targeted treatment (larotrectinib, dabrafenib and trametinib) within a clinical phase I/II study based on the molecular profile of the tumor. The remaining 18 patients had matched targeted drug treatment via compassionate use programs or off-label, consisting of trametinib (n=11), larotrectinib (n=5), crizotinib (n=2), everolimus (n=2), dabrafenib (n=2), ribociclib (n=1), lorlatinib (n=1), capmatinib (n=1), rapamune (n=1) and inotuzumab (n=1).
The remaining patients included in INFORM registry received conventional treatment such as drug therapies, radiotherapy, or surgery. In most cases, those receiving targeted therapies had one or more of the conventional cancer drugs at some time-point during follow up due to progressive disease. Twelve patients went to symptomatic palliative care without any further treatment for the relapse.
The active follow-up period in the INFORM registry study (14) is set to approximately 2 years although patients living longer were followed longer. As the INFORM registry primarily focuses on patients at relapse, the outcome for the Swedish cohort was evaluated only for children included at relapse (n=147 with data missing for 2 individuals) from the time-point of first registration in MARVIN to the event of interest. Initially, relapsed patients who were provided matched targeted therapy (MTT) (n=54) were compared to those relapsed patients (n=91) who did not receive targeted treatment (Figures 4A, B). Median overall survival (OS) in the MTT group was 514 days (95% CI, 389- 767) compared to 584 days [95% confidence interval (CI), 407-not applicable (NA)] in the latter group. No difference in median progression free survival (PFS) was observed between the groups [208 days (95% CI, 173-346) and 254 days (95% CI, 196-448) respectively].
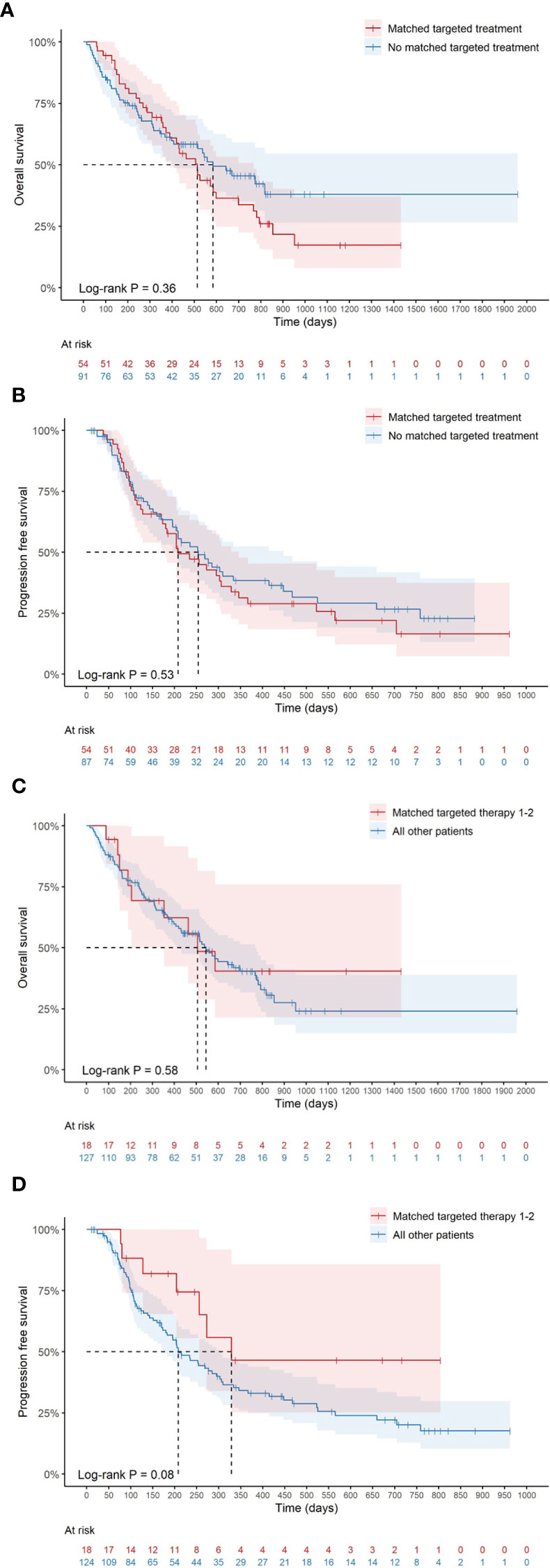
Figure 4 Survival analyses (Kaplan-Meier) where median time of survival for duplicates/triplicates was measured from the last registration. (A) Median overall survival (OS) for patients receiving matched therapy compared to all other patients and in (B) median progression free survival (PFS) is shown. In (C) median OS overall survival is shown for those children with matched targeted therapy 1-2 and in (D) median PFS is displayed for the same group.
Furthermore, patients with priority targets 1-2 (MTT 1-2; n=18) were compared to remaining patients (n=127) (Figures 4C, D). No significant difference in OS was observed for the MTT 1-2 group compared to remaining patients [506 days (95% CI, 353-NA) and 544 days (95% CI, 420-767) respectively, log rank test p=0.58]. In the MTT 1-2 group, there were three children harboring NTRK fusions and two with BRAFV600E mutations who are long term survivors after targeted therapy for more than 2 years. Patients in the MTT 1-2 group had a trend to longer PFS than the remaining patients [329 days, 95% CI, 256-NA) and 208 days (95% CI, 180-303) respectively, log rank p=0.08].
As death may occur before progression of a malignant disease in each patient, these events were considered as competing events when analyzing PFS. The cumulative incidence of the specific events of interest may be informative since ignoring competing events may lead to informative censoring and therefore incorrect estimates of the main event of interest. In Table 3, the cumulative incidence for death and progression, respectively, is shown for the MTT 1-2 group and all other patients. While no difference was observed in the 1-year cumulative incidence of death (p=0.4), there was a trend towards decreased 1-year cumulative incidence of progression in the MTT 1-2 group (p=0.068).
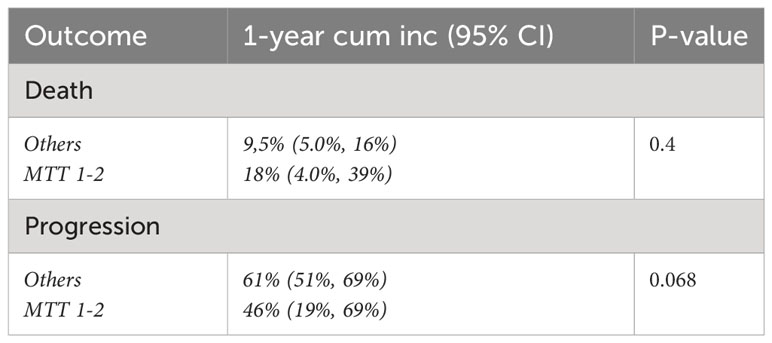
Table 3 Cumulative incidence of death or progression in patients with level 1-2 targets receiving therapy compared to all other patients.
Pediatric cancer patients at relapse have limited effective treatment options. The INFORM registry uses next-generation sequencing, to detect actionable molecular alterations as a step towards precision medicine (10). The current study analyzed the Swedish patient cohort included in the INFORM registry regarding clinical data, molecular analysis of tumor samples, the subsequent treatment and survival. Our data demonstrate that sample preparation, shipment and reporting was feasible and timely in this international setting and that the molecular analyses also provided important clinical information. The Swedish cohort shares similarities with the international INFORM registry cohort presented earlier (10, 14). Sweden and Germany have much in common and are both partners in the EU, but still health systems, health financing, regulations governing health and much more differ. In terms of survival on a group basis, no clinical benefit of targeted treatment could be observed although patients with high priority targets treated with a matched drug had a trend towards a longer PFS. Individual patients have achieved long term benefits from molecular screening followed by targeted therapy, especially when harboring druggable targets as NTRK fusions and BRAFV600E mutations.
The Swedish INFORM cohort as well as the previously reported INFORM registry cohort included mainly CNS tumors and sarcomas (14) whereas only few leukemia cases were included despite being the most common childhood cancer diagnosis. The average age at pediatric cancer diagnosis is during preschool, yet the patients included in the INFORM registry were older as most of them had undergone 1st and 2nd line of treatment before inclusion. In addition, several treatment-resistant cancers, such as Ewing sarcoma and osteosarcoma, occur in the adolescence period. Most patients were in good general condition (assessed by the Karnofsky/Lansky score) at study inclusion despite that most children were included at relapse. Patient inclusion in the INFORM registry was not evenly spread between the pediatric oncology centers in Sweden and did not reflect the number of cases the center cares for. In the first years of the study, the centers with the closest collaboration with the national coordinating center enrolled the largest number of patients.
Pharmacologically actionable targets were detected in 88% of the patient samples in the Swedish cohort. A potentially druggable target with a priority level of 1–4 was present in approximately 60% of patients as compared to 67% in the latest publication from the INFORM registry (14). Similar numbers in terms of priority targets have also been reported from the European Mappyacts trial (17) although lower compared to the molecular profiling platform ZERO that presented with 71.4% (18). In the current cohort, actionable targets were not present at the first analysis but detected at later timepoints which is in accordance with previously published papers (9 (17). We demonstrate that the INFORM registry may impact treatment and that renewed biopsies in patients with chemo-resistant relapse is mandatory for potential personalized targeting treatment. In tumors with priority level 1 targets, several known actionable targets such as ALK, BRAF and NTRK were detected in extracranial solid and CNS tumors. In addition, targetable mutations as well as fusion genes need to be analyzed as they provide therapeutic options for pediatric cancer (19), such as BRAF fusions/mutation in low-grade gliomas and NTRK fusions in several tissue types showing promising results in pediatric clinical trials (20).
Two thirds of patients with high priority targets (1, 2) were treated with targeted drugs either included in a phase I/II trial or provided by pharma. This may reflect a lack of early phase clinical studies for children with cancer in Sweden or reluctancy to refer very sick children to other national study centers or abroad for participation in phase I/II trials. Possibly, some patients with advanced disease may not have been eligible to trials or to novel treatments due to a poor general condition although most patients were in good general condition (assessed by the Karnofsky/Lansky score) at study inclusion. In total, only 13 out of 70 patients who received targeted treatments were enrolled in a clinical trial. The remaining 57 patients where no trials were available received targeted therapies prescribed off label, or by compassionate use programs.
The patients included in the INFORM registry suffer from treatment resistant diseases at a stage where the chance of curative treatment is very low. Relapse of soft tissue and bone sarcomas is associated with a particularly poor prognosis, and despite targeted treatment no long-time survivors were observed. In the most recent article summarizing more than 500 patients in the INFORM registry, an increased PFS for patients with targets prioritized to the highest level 1 who received targeted treatment was shown when compared to all other patients (14). In the same cohort, no significant difference was observed in OS. In the presented Swedish cohort, no significant difference in OS was observed between patients with priority targets who received targeted therapy (MTT 1-2) compared to all other patients. However, there was a trend for a longer PFS in this group of children compared to all other patients. This finding was supported by the lower cumulative 1-year incidence of progression in the MTT 1-2 group. Contrary to the previously published paper from the INFORM registry (14), patients who had tumors with both actionable target score 1-2 were included in our survival analyses.
It is important to keep in mind that the INFORM registry determines potentially treatable targets, but as reported for many other cancers, single agents do not, with only rare exceptions induce sustainable response or cure. Many cancer phenotypes, including those influencing response to therapy are in addition determined by non-genetic mechanisms in addition to genetic alterations such mutations/translocations concerning BRAF, ALK and NTRK (20).
This study describing data on Swedish patients included in the INFORM registry has several limitations. Foremost, the patients were included in a non-interventional registry where any decision on treatment was left to the treating physician at the different sites. The limited numbers of patients and the small fraction of children with priority targets 1-2 hampers the statistical analyses on PFS and OS. We cannot exclude that some children who received a matched targeted drug also received other concomitant treatment. In addition, data management was done at the different pediatric cancer centers and data quality, consistency and accuracy in reporting may have differed. On the other hand, a strength in this study is the low number of children who were lost to follow up.
This study, as well as previous studies, has demonstrated the feasibility of sequencing pediatric tumor material and to provide data on molecular findings and potentially actionable targets to clinicians. However, as opposed to adult oncology, there is a lack of innovative trials, specific biomarker research, immunotherapy, and drugs targeting pediatric cancers. Consequently, a low number of patients in Sweden were enrolled in a clinical trial with monotherapy at relapse which also was shown for the INFORM registry in total (14). As targeted monotherapy in late-stage disease seldom provides a durable response (4, 5, 14, 17), it is not surprising that there was no survival benefit for the children in our cohort.
However, molecular profiling at diagnosis is now offered to newly diagnosed patients in Sweden within the frame of the precision medicine program Genomic Medicine Sweden (21, 22). This may provide an opportunity to apply targeted therapy already at primary diagnosis and in combination with other treatment modalities. Pediatric precision oncology has moved slowly but is now gaining momentum world-wide with different technical and analytic approaches. To further gain impact on patient survival will require a combination of continuous preclinical testing in relevant pediatric tumor models as well as biomarker driven multinational clinical trials. In addition, the different national molecular profiling platforms should team up to provide a robust and sustainable framework, covering all components from technology development to the design and execution of clinical trials as outlined by the Swedish and German centers for personalized medicine (23, 24).
The datasets presented in this study can be found in online repositories. The names of the repository and accession number can be found below: European Genome Archive, accession number EGAS00001005112.
The studies involving humans were approved by Swedish Ethical Review Authority, Uppsala, Sweden. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
SW: Data curation, Formal analysis, Investigation, Writing – original draft. IØ: Data curation, Investigation, Project administration, Writing – review & editing. GP: Investigation, Methodology, Writing – review & editing. JS: Methodology, Resources, Writing – review & editing. CB: Investigation, Writing – review & editing. GL: Investigation, Writing – review & editing, Validation. HV: Investigation, Writing – review & editing. TE: Investigation, Writing – review & editing. CV: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – review & editing. AN: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Project administration, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We are grateful for the financial support from the Swedish Childhood Cancer Fund (BCF), Entrepreneurs for good and ARMEC Lindeberg Foundation directed to inclusion and follow up of children in Sweden included in the Inform registry. The INFORM program is financially supported by the German Cancer Research Center (DKFZ), the German Cancer Consortium (DKTK), the German Federal Ministry of Education and Research (BMBF), the German Federal Ministry of Health (BMG), the Ministry of Science, Research and the Arts of the State of Baden-Württemberg (MWK BW); the German Cancer Aid (DKH), the German Childhood Cancer Foundation (DKS), RTL television, the aid organization BILD hilft e.V. (Ein Herz für Kinder) and the generous private donation of the Scheu family.
The authors would like to thank the local study nurses in the Swedish university centers who organized sampling of tumor material. The Swedish Childhood Tumor Biobank (BTB) has been instrumental in handling samples from the different centra, extracting DNA/RNA and organizing the shipment to Heidelberg, Germany. We are grateful for the financial support from the Swedish Childhood Cancer Fund (BCF), Entrepreneurs for good and ARMEC Lindeberg Foundation. The INFORM program is financially supported by the German Cancer Research Center (DKFZ), the German Cancer Consortium (DKTK), the German Federal Ministry of Education and Research (BMBF), the German Federal Ministry of Health (BMG), the Ministry of Science, Research and the Arts of the State of Baden-Württemberg (MWK BW); the German Cancer Aid (DKH), the German Childhood Cancer Foundation (DKS), RTL television, the aid organization BILD hilft e.V. (Ein Herz für Kinder) and the generous private donation of the Scheu family.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1340099/full#supplementary-material
INFORM, INdividualized Therapy FOr Relapsed Malignancies in Childhood; CNS, Central nervous system; DIPG, Diffuse intrinsic pontine glioma; DKFZ, German Cancer Research Center; BTB, Swedish Childhood Tumor Biobank; DNA, Deoxyribonucleic acid; RNA, Ribonucleic acid; NTRK, Neurotrophic receptor tyrosine kinase; BRAF, B-Raf proto-oncogene; ALK, Anaplastic lymphoma kinase; NRAS, Neuroblastoma RAS viral oncogene homolog; KRAS, Kirsten Rat Sarcoma virus; CDK4, Cyclin-dependent kinase 4; NF1, Neurofibromatosis type 1; CAR-T cells, Chimeric antigen receptor T-cells; MTT, Matched targeted therapy; OS, Overall survival; PFS, Progression-free survival.
1. Smith L, Stiller CA, Aitken JF, Hjalgrim LL, Johannesen T, Lahteenmaki P, et al. International variation in childhood cancer mortality rates from 2001 to 2015: Comparison of trends in the International Cancer Benchmarking Partnership countries. Int J Cancer (2022) 150(1):28–37. doi: 10.1002/ijc.33774
2. Rostgaard K, Hjalgrim H, Madanat-Harjuoja L, Johannesen TB, Collin S, Hjalgrim LL. Survival after cancer in children, adolescents and young adults in the Nordic countries from 1980 to 2013. Br J Cancer (2019) 121(12):1079–84. doi: 10.1038/s41416-019-0632-1
3. Grabow D, Kaiser M, Hjorth L, Byrne J, Alessi D, Allodji RS, et al. The PanCareSurFup cohort of 83,333 five-year survivors of childhood cancer: a cohort from 12 European countries. Eur J Epidemiol (2018) 33(3):335–49. doi: 10.1007/s10654-018-0370-3
4. Forrest SJ, Geoerger B, Janeway KA. Precision medicine in pediatric oncology. Curr Opin Pediatr (2018) 30(1):17–24. doi: 10.1097/MOP.0000000000000570
5. Laetsch TW, DuBois SG, Bender JG, Macy ME, Moreno L. Opportunities and challenges in drug development for pediatric cancers. Cancer Discovery (2021) 11(3):545–59. doi: 10.1158/2159-8290.CD-20-0779
6. Vogelstein B, Papadopoulos N, Velculescu VE, Zhou S, Diaz LA Jr., Kinzler KW. Cancer genome landscapes. Science (2013) 339(6127):1546–58. doi: 10.1126/science.1235122
7. Grobner SN, Worst BC, Weischenfeldt J, Buchhalter I, Kleinheinz K, Rudneva VA, et al. The landscape of genomic alterations across childhood cancers. Nature (2018) 555(7696):321–7. doi: 10.1038/nature25480
8. Langenberg KPS, Looze EJ, Molenaar JJ. The landscape of pediatric precision oncology: program design, actionable alterations, and clinical trial development. Cancers (Basel) (2021) 13(17):4324. doi: 10.3390/cancers13174324
9. Lee J, Gillam L, Visvanathan K, Hansford JR, McCarthy MC. Clinical utility of precision medicine in pediatric oncology: A systematic review. JCO Precis Oncol (2021) 5:1088–102. doi: 10.1200/PO.20.00405
10. Worst BC, van Tilburg CM, Balasubramanian GP, Fiesel P, Witt R, Freitag A, et al. Next-generation personalised medicine for high-risk paediatric cancer patients - The INFORM pilot study. Eur J Cancer (2016) 65:91–101. doi: 10.1016/j.ejca.2016.06.009
11. Pfaff E, El Damaty A, Balasubramanian GP, Blattner-Johnson M, Worst BC, Stark S, et al. Brainstem biopsy in pediatric diffuse intrinsic pontine glioma in the era of precision medicine: the INFORM study experience. Eur J Cancer (2019) 114:27–35. doi: 10.1016/j.ejca.2019.03.019
12. Schramm A, Koster J, Assenov Y, Althoff K, Peifer M, Mahlow E, et al. Mutational dynamics between primary and relapse neuroblastomas. Nat Genet (2015) 47(8):872–7. doi: 10.1038/ng.3349
13. Mosse YP. Anaplastic lymphoma kinase as a cancer target in pediatric Malignancies. Clin Cancer Res (2016) 22(3):546–52. doi: 10.1158/1078-0432.CCR-14-1100
14. van Tilburg CM, Pfaff E, Pajtler KW, Langenberg KPS, Fiesel P, Jones BC, et al. The pediatric precision oncology INFORM registry: clinical outcome and benefit for patients with very high-evidence targets. Cancer Discov (2021) 11(11):2764–79. doi: 10.1158/2159-8290.CD-21-0094
15. RJ G. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Statist (1988) 16(3):1141–54. doi: 10.1214/aos/1176350951
16. Team RC. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing (2022).
17. Berlanga P, Pierron G, Lacroix L, Chicard M, Adam de Beaumais T, Marchais A, et al. The European MAPPYACTS trial: precision medicine program in pediatric and adolescent patients with recurrent Malignancies. Cancer Discov (2022) 12(5):1266–81. doi: 10.1158/2159-8290.CD-21-1136
18. Wong M, Mayoh C, Lau LMS, Khuong-Quang DA, Pinese M, Kumar A, et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat Med (2020) 26(11):1742–53. doi: 10.1038/s41591-020-1072-4
19. Dupain C, Harttrampf AC, Urbinati G, Geoerger B, Massaad-Massade L. Relevance of fusion genes in pediatric cancers: toward precision medicine. Mol Ther Nucleic Acids (2017) 6:315–26. doi: 10.1016/j.omtn.2017.01.005
20. Filbin M, Monje M. Developmental origins and emerging therapeutic opportunities for childhood cancer. Nat Med (2019) 25(3):367–76. doi: 10.1038/s41591-019-0383-9
21. Edsjo A, Friedman M, Rosenquist R. [Genomic Medicine Sweden - a national initiative for the broad introduction of precision medicine in Swedish healthcare]. Lakartidningen (2021) 118:21023.
22. Wadensten E, Wessman S, Abel F, Diaz De Stahl T, Tesi B, Orsmark Pietras C, et al. Diagnostic yield from a nationwide implementation of precision medicine for all children with cancer. JCO Precis Oncol (2023) 7:e2300039. doi: 10.1200/PO.23.00039
23. Marshall M, Ivanovich J, Schmitt M, Helvie A, Langsford L, Casterline J, et al. Pediatric precision oncology: “better three hours too soon than a minute too late”. Front Oncol (2023) 13:1279953. doi: 10.3389/fonc.2023.1279953
Keywords: pediatric oncology, pediatric cancer, precision medicine, molecular diagnostic techniques, molecular targeted therapy
Citation: Wallin S, Øra I, Prochazka G, Sandgren J, Björklund C, Ljungman G, Vogt H, Ek T, van Tilburg CM and Nilsson A (2024) Implementing data on targeted therapy from the INFORM registry platform for children with relapsed cancer in Sweden. Front. Oncol. 14:1340099. doi: 10.3389/fonc.2024.1340099
Received: 17 November 2023; Accepted: 09 January 2024;
Published: 31 January 2024.
Edited by:
Martin Distel, St. Anna Children’s Cancer Research Institute (CCRI), AustriaReviewed by:
Wafaa M. Rashed, Clinical Pharmacy Department- Faculty of Pharmacy- Ahram Canadian University, EgyptCopyright © 2024 Wallin, Øra, Prochazka, Sandgren, Björklund, Ljungman, Vogt, Ek, van Tilburg and Nilsson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Nilsson, YW5uYS5uaWxzc29uLjFAa2kuc2U=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.