
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 09 July 2024
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1334564
This article is part of the Research TopicWomen in Neuro-Oncology and Neurosurgical Oncology Vol II: 2023View all 7 articles
 Evelynn Vergauwen1,2*
Evelynn Vergauwen1,2* Jan-Helge Klingler3
Jan-Helge Klingler3 Marie T. Krüger3,4
Marie T. Krüger3,4 Christine Steiert3Robert Kuijpers5
Christine Steiert3Robert Kuijpers5 Steffen Rosahl6Anne-Marie Vanbinst7Corina Emilia Andreescu8Sven Gläsker1,9
Steffen Rosahl6Anne-Marie Vanbinst7Corina Emilia Andreescu8Sven Gläsker1,9Introduction: Optic nerve and chiasm hemangioblastomas are rare tumors, occurring sporadically or in the context of von Hippel-Lindau (VHL) disease. They have only been portrayed in isolated case reports and small cohorts. Their natural history and therapeutic strategies are only scarcely described. To better characterize these rare tumors, we retrospectively analyzed an optic nerve and chiasm hemangioblastoma series of 12 VHL patients. By combining our own experience to a review of all known cases in literature, we intended to create treatment recommendations for optic nerve and chiasm hemangioblastomas in VHL patients.
Methods: We reviewed two electronic databases in the hospitals of our senior authors, searching for VHL patients with optic nerve or chiasm hemangioblastomas. Clinical data were summarized. Tumor size and growth rate were measured on contrast enhanced MRI. Comparable data were collected by literature review of all available cases in VHL patients (Pubmed, Trip, Google and Google Scholar).
Results: Of 269 VHL patients, 12 had optic nerve or chiasm hemangioblastomas. In 10 of 12 patients, tumors were diagnosed upon annual ophthalmoscopic/MRI screening. Of 8 patients who were asymptomatic at diagnosis, 7 showed absent or very slow annual progression, without developing significant vision impairment. One patient developed moderate vision impairment. Two symptomatic patients suffered from rapid tumor growth and progressive vision impairment. Both underwent late-stage surgery, resulting in incomplete resection and progressive vision impairment. One patient presented with acute vision field loss. A watchful-waiting approach was adopted because the hemangioblastoma was ineligible for vision-sparing surgery. One patient developed progressive vision impairment after watchful waiting. In the literature we found 45 patient cases with 48 hemangioblastomas.
Discussion: When optic nerve and chiasm hemangioblastomas are diagnosed, we suggest annual MRI follow-up as long as patients do not develop vision impairment. If tumors grow fast, threaten the contralateral eye, or if patients develop progressive vision deficiency; surgical resection must be considered because neurological impairment is irreversible, and resection of large tumors carries a higher risk of further visual decline.
Optic nerve hemangioblastomas are extrinsic primary tumors of the optic nerve, characterized by stromal tumor cells in a rich vascular capillary network (1). They can occur sporadically or as a feature of von Hippel-Lindau (VHL) disease, an autosomal dominantly inherited tumor syndrome. Patients with VHL disease can be affected by central nervous system hemangioblastomas, clear cell renal cell carcinomas, pancreatic neuro-endocrine tumors, pheochromocytomas and other tumors. Retinal hemangioblastomas occur in 49 to 62% of VHL patients and are usually detected at the peripheral retina or at the optic nerve head (2–4). In contrast, the occurrence of hemangioblastomas behind the optic nerve head, thus over the course of the optic nerve and chiasm, is uncommon. These optic nerve hemangioblastomas may be asymptomatic for a long time but can also cause varying degrees of slowly progressive and usually permanent vision impairment (1, 5, 6).
In 1930, Verga et al. were the first to describe a case of a right optic nerve hemangioblastoma in a 57-year-old patient. It is unclear whether this patient had VHL disease. The lesion was described as a “cystic angio-reticulo-glioma” (7).
Up to date, optic nerve and chiasm hemangioblastomas in VHL patients have only been portrayed in isolated case reports and small patient cohorts. It appears that many patients are treated with surgery, leading to further visual decline or blindness. No guidelines exist on the watchful waiting approach.
By combining our own experience to a review of the literature, we intended to create the first algorithm for management of optic nerve and chiasm hemangioblastomas in VHL patients.
We reviewed our databases of 2 hospitals where more than 269 VHL patients with hemangioblastomas of the central nervous system are followed. Patients with optic nerve and/or chiasm hemangioblastomas were included. Clinical data including age, sex, and clinical course (visual ability) were collected. Information about visual ability was derived from ophthalmological and neurological examinations during patient visits. The size of hemangioblastomas, and their location within the optic nerve and chiasm, was assessed on contrast-enhanced magnetic resonance imaging (MRI) (Figure 1). The size of the solid tumor (contrast-enhancing region) was measured in three dimensions (height, length, and width), divided by 2 and expressed in cubic millimeter (mm³). Tumor growth rate was measured and expressed as mm³/year.
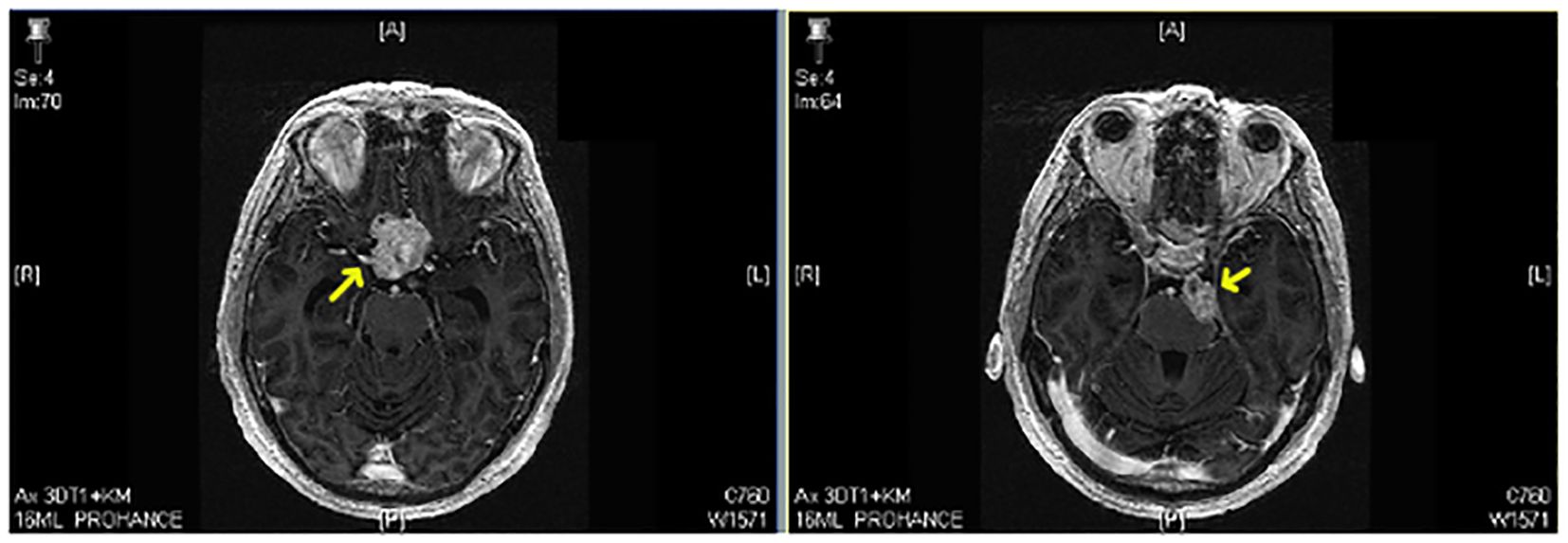
Figure 1 Contrast-enhanced MRI showing an optic nerve hemangioblastoma (yellow arrow) (patient number 12).
Scientific articles on VHL related optic nerve hemangioblastomas were collected by searching through Pubmed, Trip, Google, and Google Scholar databases. We used the following key word combinations: “optic hemangioblastoma”, “optic hemangioblastoma AND von Hippel-Lindau”, “optic nerve AND von Hippel-Lindau”, “optic chiasm AND von Hippel-Lindau”, “ophthalmology AND von Hippel-Lindau”. Also, we reviewed the reference lists of previously published articles on optic nerve hemangioblastomas in VHL patients. Articles on sporadic optic nerve hemangioblastomas were excluded; as decision-making in VHL patients is different and influenced by multi-system comorbidities or the presence of bilateral tumors. We focused on themes such as diagnostic approach, differential diagnosis, surgical pearls and pitfalls, and therapeutic decision making. Histopathologic description of optic nerve hemangioblastomas will not be described here, because more comprehensive papers can be found on this subject.
Of 269 VHL patients who are followed in the 2 hospitals, 12 patients with optic nerve or chiasm hemangioblastomas were included: 7 male and 5 female patients. One patient was included from a third hospital where one of the authors started to work recently. Age at first diagnosis of an optic hemangioblastoma ranged from 15 to 67 years, with a mean age of 44 years. All included patients had genetically confirmed VHL disease with other intracranial hemangioblastomas. Patient data are summarized in Table 1.
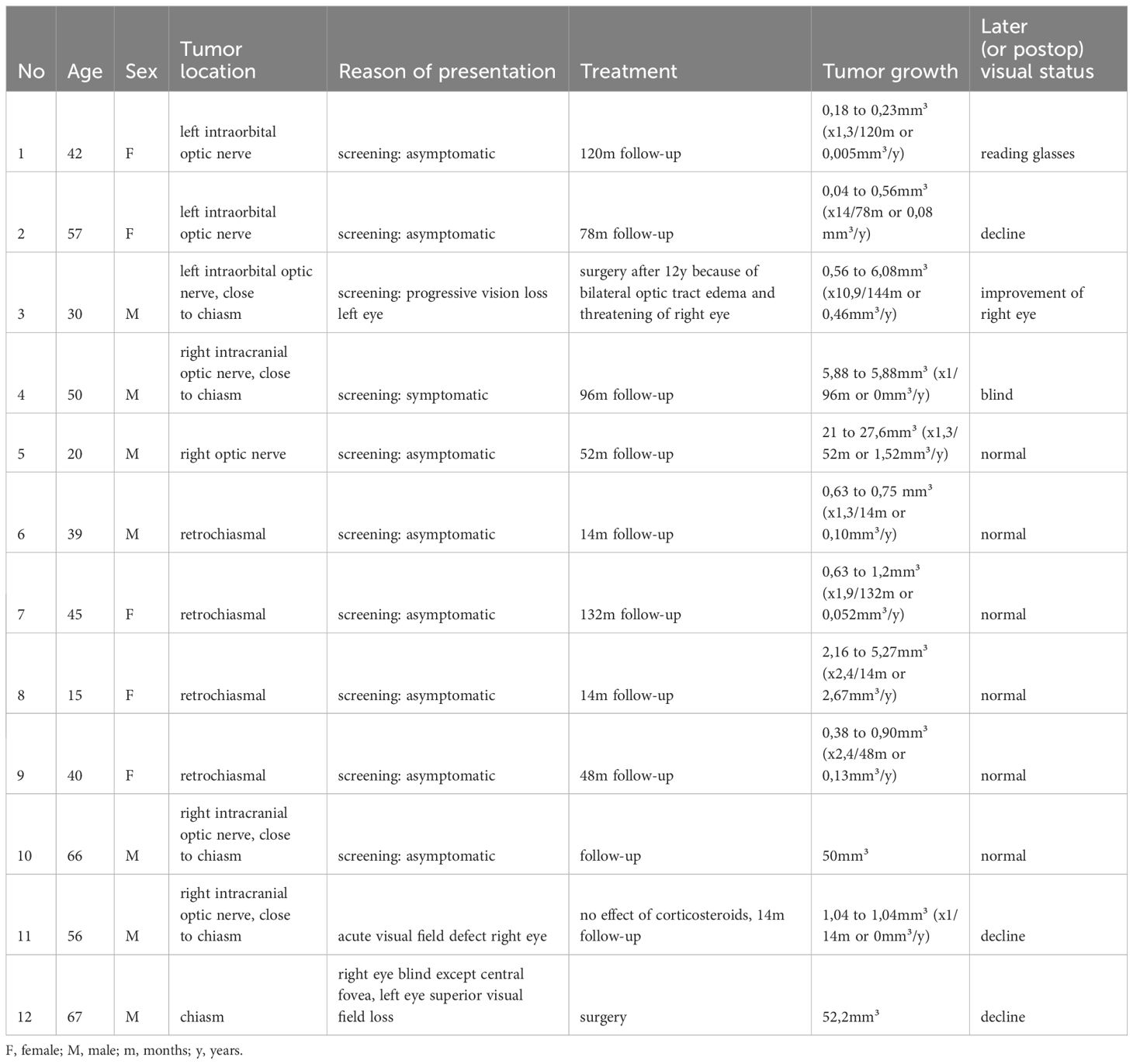
Table 1 VHL related optic nerve and chiasm hemangioblastomas in our institution: summary of patient and hemangioblastoma data.
In our patient series, 3 hemangioblastomas were located along the left optic nerve (all 3 intraorbital and 1 with intracranial extension), and 4 hemangioblastomas were located along the right optic nerve (all 4 intracranial). There was 1 hemangioblastoma within the chiasm, and there were 4 with a retro-chiasmal location. Location of tumors is graphically illustrated in Figure 2. Mean tumor size at time of diagnosis was 11,23 mm³ (median 0,86mm³). In patients who remained completely asymptomatic during follow up (N=6), tumor size at time of diagnosis ranged from 0,38 to 50mm³ and mean growth rate was 0,89mm³/year (range 0,052 – 2,67mm³/year). In symptomatic patients (N=6), tumor size ranged from 0,04 to 52,2mm³ at presentation and mean growth rate was 0,18mm³/year (range 0 – 0,46mm³/year). Mean growth rate of all tumors (both symptomatic and asymptomatic, N=12) was 0,56mm³/year (range 0 – 2,67mm³/year).
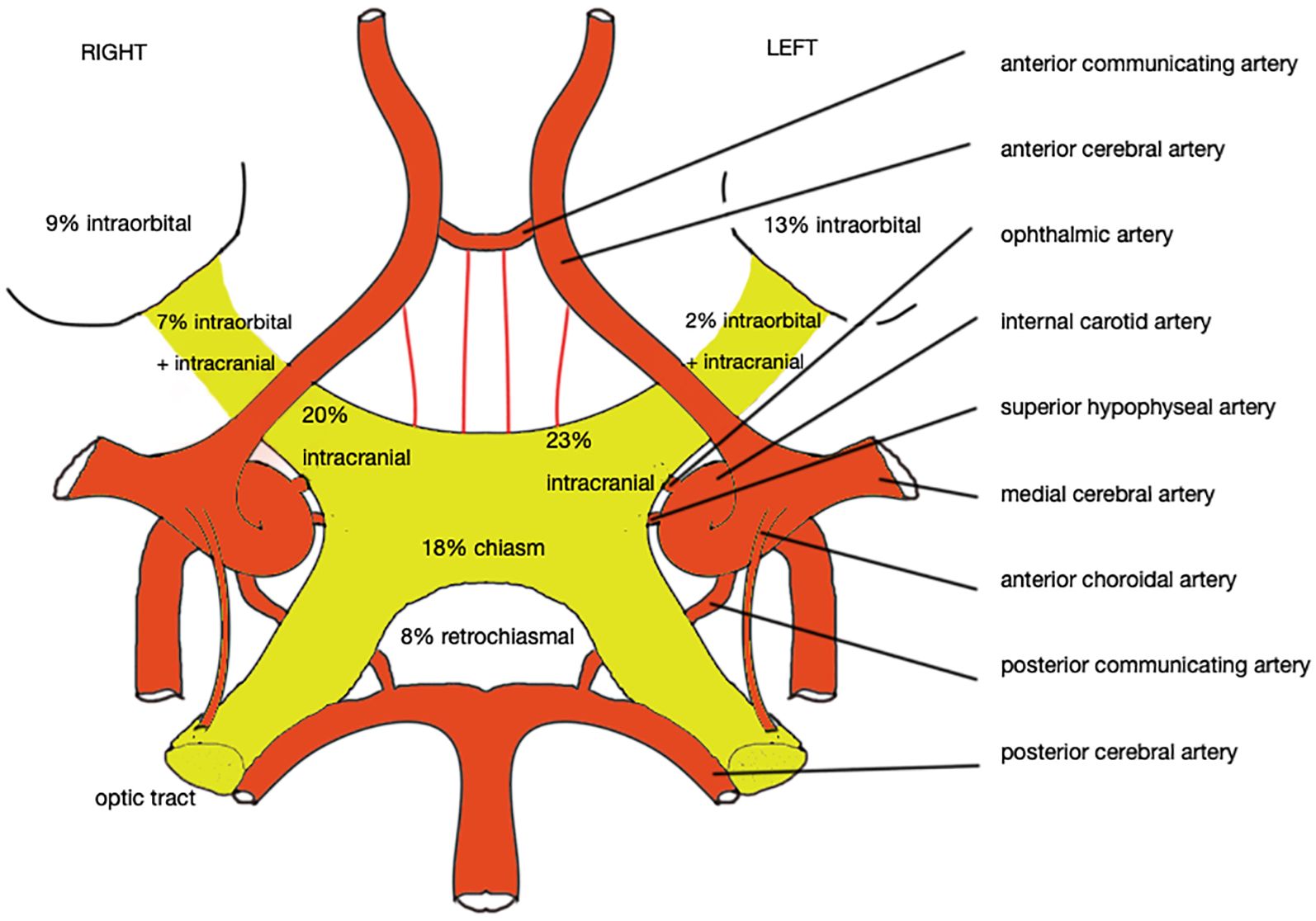
Figure 2 Schematic vascular supply of the optic nerve and chiasm, and the relative distribution of tumors from all available cases (design by E. Vergauwen).
Literature cases are summarized in Table 2. Literature search yielded 45 patient cases with 48 hemangioblastomas, some cases having been published twice in different years (asterixis in Table 2). Most authors presented a single case. One cohort of 19 patients was split up in different publications (Meyerle et. al). Between 1930 and now, 27 female and 28 male VHL patients with optic nerve and/or chiasm hemangioblastomas have been reported, their ages ranging from 15 to 64 years old. Of 48 hemangioblastomas, 17 were located on the right optic nerve (5 intraorbital, 7 intracranial and 5 with extension towards both sides), and 18 were located on the left optic nerve (5 intraorbital, 13 intracranial). There were 3 patients with bilateral optic nerve tumors and 6 patients with tumors of the chiasm. In 1 patient, tumor location was unknown. Location of tumors is graphically illustrated in Figure 2. At time of diagnosis, 11 patients were asymptomatic, 27 patients complained of varying ophthalmologic and/or systemic symptoms. In 7 patients, symptomatology is unknown.
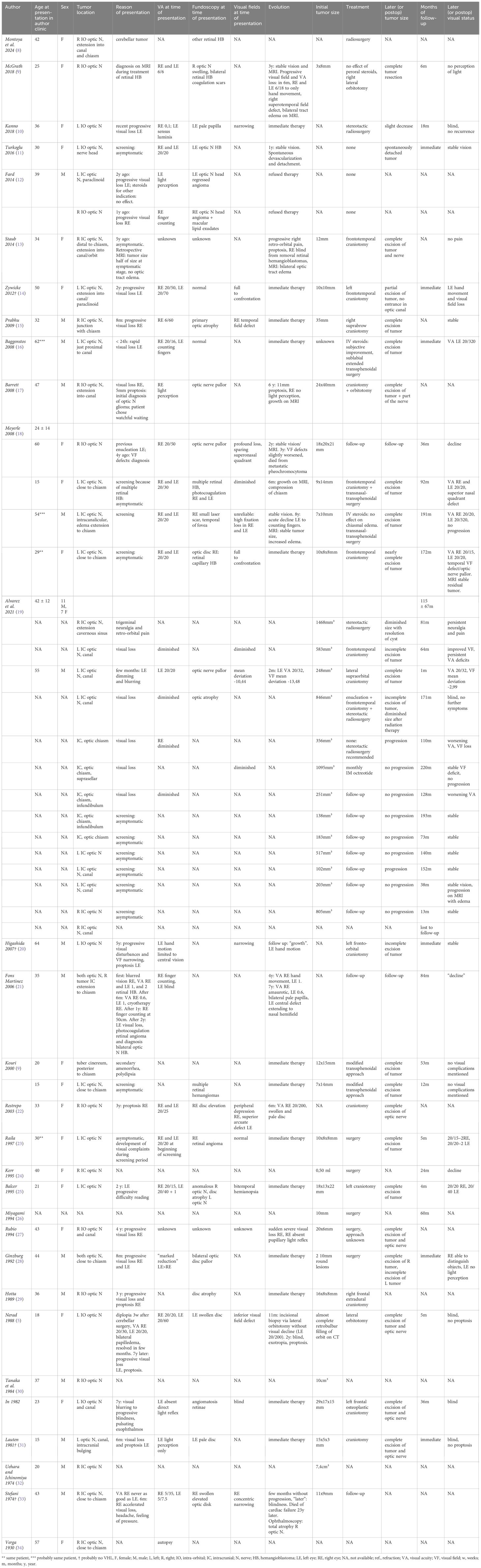
Table 2 VHL related optic nerve and chiasm hemangioblastomas reported in literature.
In the literature we found 45 cases of VHL patients with 48 optic nerve and chiasm hemangioblastomas. Often the key message of these case reports was that the discovery of a rare optic nerve tumor led to diagnosis of VHL disease. Of 45 reported patients, 24 underwent surgical resection, 4 were treated with stereotactic radiosurgery, 13 received no treatment other than pharmacological, and in 4 patients, treatment modality is unknown. Figure 3 is a graphical illustration of the different clinical scenarios in our own patients and the scenarios that could be reconstructed from literature cases. These possible scenarios are further described in the following section.
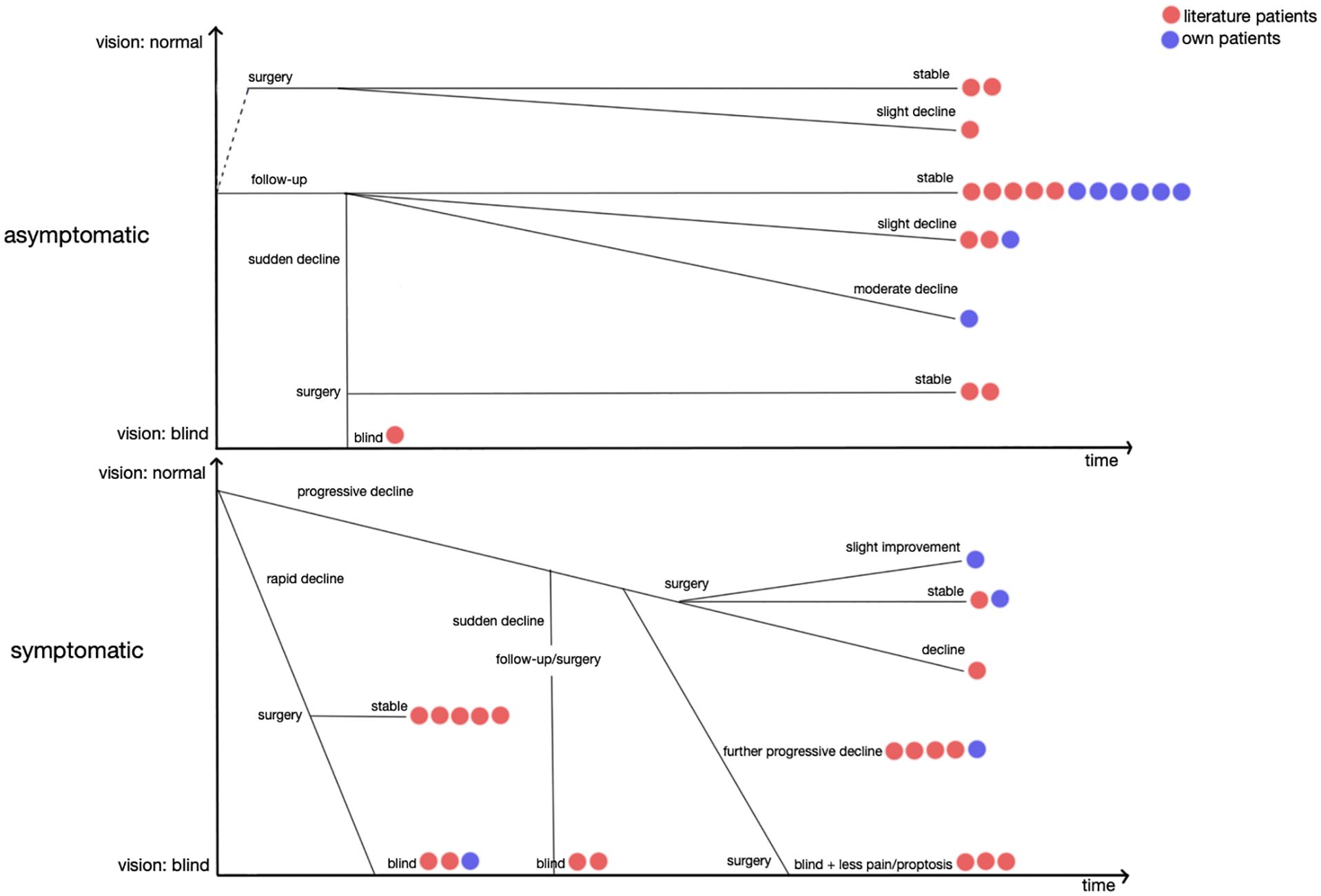
Figure 3 Possible clinical scenarios in patients with optic nerve hemangioblastomas. (Red dots = own patients. Blue dots = literature patients with available progression data. One dot represents one patient. Horizontal axis = progression over time. Vertical axis = vision, blind to normal).
Of 8 asymptomatic patients followed in our clinic, 6 patients remained asymptomatic during a mean watchful waiting period of 4,3 years (range 1,17–11 years). Mean tumor growth rate was 0,89 mm³/year (range 0,052 – 2,67mm³year).
In literature, 6 asymptomatic patients remained asymptomatic during varying follow-up periods. Remarkably, Turkoglu et al. observed spontaneous devascularization and detachment of an optic nerve head hemangioblastoma in a 30-year-old asymptomatic female patient, after 1 year of watchful waiting (11).
On annual MRI screening, we discovered an intraorbital left optic nerve hemangioblastoma in a 42-year-old asymptomatic female patient. During a follow-up time of 8 years without intervention, the tumor grew from 0,18 to 0,23mm³ (0,006mm³/year) on MRI, and the patient only needed reading glasses.
Also on annual MRI screening, we discovered an intraorbital left optic nerve hemangioblastoma in a 57-year-old asymptomatic female patient. After 6,5 years of watchful waiting, the tumor grew from 0,04 to 0,56mm³ (0,08mm³/year) and visual acuity in the left eye was +4,75/-0,25.
Meyerle et al. performed complete resection of an intracranial left optic nerve hemangioblastoma in a 29-year-old asymptomatic female patient. Postoperatively, the patient experienced slight visual decline in both eyes (18).
Kouri et al. performed complete transsphenoidal resection of a suprachiasmal hypothalamic hemangioblastoma in a 20-year-old female patient with hormonal changes and normal vision. Her vision remained stable after surgery. Kouri et al. also reported the case of a 15-year-old asymptomatic female patient with preservation of normal vision after complete transsphenoidal resection of a left optic nerve tumor close to the chiasm (9).
In our clinic, we followed a 50-year-old male patient with a right optic nerve hemangioblastoma close to the chiasm. The patient experienced visual complaints in the beginning and became progressively blind after a watchful waiting period of 8 years, although no growth was observed on MRI.
Meyerle et al. reported a 60-year-old female patient with a right intraorbital optic nerve hemangioblastoma. The patient experienced progressive visual field defects in the right eye, and after a watchful waiting period of 4 years, the optic nerve had a pale fundoscopic aspect. Her vision remained stable in the sixth and seventh year, but again mildly declined during the eighth year (18).
Fons Martinez et al. discovered bilateral optic nerve hemangioblastomas in a 35-year-old male patient who already had bilateral retinal hemangioblastomas. The patient could only count fingers with the right eye and had normal vision in the left eye. After 4 years of watchful waiting, his already poor left eye vision remained stable, but his right eye vision regressed to perceiving hand movements. After another 3 years, vision further declined in both eyes, and fundoscopy showed bilateral optic disc pallor (21).
Fard et al. reported a 39-year-old male patient who experienced bilateral progressive vision impairment over 2 years; to the point of finger counting in the right eye, where he had an intraorbital optic nerve hemangioblastoma; and of light perception in the left eye, where he had an intracranial optic nerve hemangioblastoma. The patient refused therapy (12).
Staub et al. presented a similar case of a 34-year-old female patient, who had both retinal hemangioblastomas and an intracranial nerve hemangioblastoma in the right eye. The hemangioblastoma doubled in size over a 5-year period, during which her right eye vision evolved from normal to blind. Because of acute and rapidly progressive pain with bilateral white tract edema on MRI, the hemangioblastoma together with the right optic nerve were completely resected. Vision in the left eye was spared and pain resolved (13).
Zywicke et al. followed a 50-year-old female patient who had an intracranial left optic nerve hemangioblastoma that extended into the optic canal. The patient experienced bilateral progressive vision impairment over a 2-year period. After the intracranial part of the tumor was resected, she experienced visual decline in the left eye, but right eye vision remained stable (14).
We followed a 30-year-old male patient with progressive vision impairment in the left eye because of a left optic nerve hemangioblastoma close to the chiasm. After 12 years of watchful waiting, the tumor had grown from 0,56 to 6,08mm³ (0,46mm³/year) on MRI, and the left optic disc had become pale on fundoscopy. During the twelfth year, the patient developed a visual field defect in his other – right – eye. MRI showed tumor and edema progression from the left optic hemangioblastoma to the right optic nerve, as far as the geniculate bodies. In order to prevent further spread of edema, the patient underwent complete surgical resection of the hemangioblastoma. Bilateral visual acuity slightly decreased after surgery. Visual field restriction improved in the right eye, and slightly deteriorated in the left eye.
We followed a 67-year-old male patient with a large chiasmal hemangioblastoma that extended to both optic nerves. The patient was almost blind in his right eye but nevertheless he was operated because of progressive visual field loss in the left eye. Visual status remained stable after complete left-sided and incomplete right-sided resection of the tumor.
In 1995, Balcer et al. reported a 21-year-old female patient with an intracranial left optic nerve hemangioblastoma, who experienced bilateral progressive slight visual decline over 2 years. After total excision of the left optic nerve tumor, she experienced bilateral mild visual improvement (25).
Rubio et al. reported a 43-year-old female patient with an intraorbital right optic nerve hemangioblastoma that extended into the optic canal. After 4 years of slight visual decline in the right eye, she experienced sudden blindness of the right eye. The right optic nerve was completely resected, resulting in blindness of the right eye (27).
McGrath et al. published a case of a 25-year-old asymptomatic female patient with a right intraorbital optic nerve tumor. For 3 years she remained clinically and radiographically stable, until rapid visual decline developed over a six-month period, due to bilateral optic tract edema that could be seen on MRI. The tumor was completely resected and postoperatively the patient was only able to discern light in the right eye (35).
Meyerle et al. reported a 54-year-old male asymptomatic patient with a left intracranial optic nerve hemangioblastoma extending to the optic canal, who remained stable for 8 years, until his vision suddenly declined to counting fingers only. As in McGrath’s case, bilateral white tract edema was seen on MRI. The tumor was completely resected, resulting in slight visual improvement in the left eye and sparing of vision in the right eye (18).
Kanno et al. wrote a case report on a 36-year-old female patient, who had rapid visual decline until the left eye could only perceive light and the optic disc became pale on fundoscopy. A large left intraorbital optic nerve hemangioblastoma was discovered. The patient became completely blind after stereotactic radiosurgery (10).
In 1992, Ginzburg et al. reported a 44-year-old male patient who experienced severe bilateral vision impairment over an 8-month period, due to bilateral optic nerve hemangioblastomas. Partial tumor resection in the left eye led to blindness, and total tumor resection in the right eye led to being able to distinguish objects (28).
Prabhu et al. described a 32-year-old male patient, with a right intracranial optic nerve hemangioblastoma that caused visual decline in the right eye over an 8-month period. Vision remained stable after complete tumor resection (15).
Baggenstos et al. reported a 62-year-old male patient with an intracranial left optic nerve hemangioblastoma with bilateral white tract edema, who experienced progressive vision impairment in the right eye and sudden vision impairment in the left eye. After complete resection of the tumor, edema resolved and left eye vision improved (16).
Meyerle et al. presented a 15-year-old female patient who had no visual complaints; however, there was slight vision loss in the left eye on measuring. She had an intracranial left optic nerve hemangioblastoma that radiologically grew over a 6-month period and then started to compress the chiasm. The tumor was completely resected, and after 9 years, the patient had a small quadranopsia but regained visual acuity (18).
A 56-year-old patient in our clinic experienced an acute visual field defect in the right eye. Fundoscopy was normal and MRI showed a large right intraorbital optic nerve hemangioblastoma without surrounding edema (Figure 4, Discussion). Corticosteroids did not improve his symptoms. Because surgical resection was unfeasible and was anticipated to lead to total blindness of the right eye, the patient was not operated – to cherish a couple more “good” years. Surgery will be planned as soon as peritumoral edema develops and threatens the contralateral eye. Tumor volume has now remained stable for 4 years.
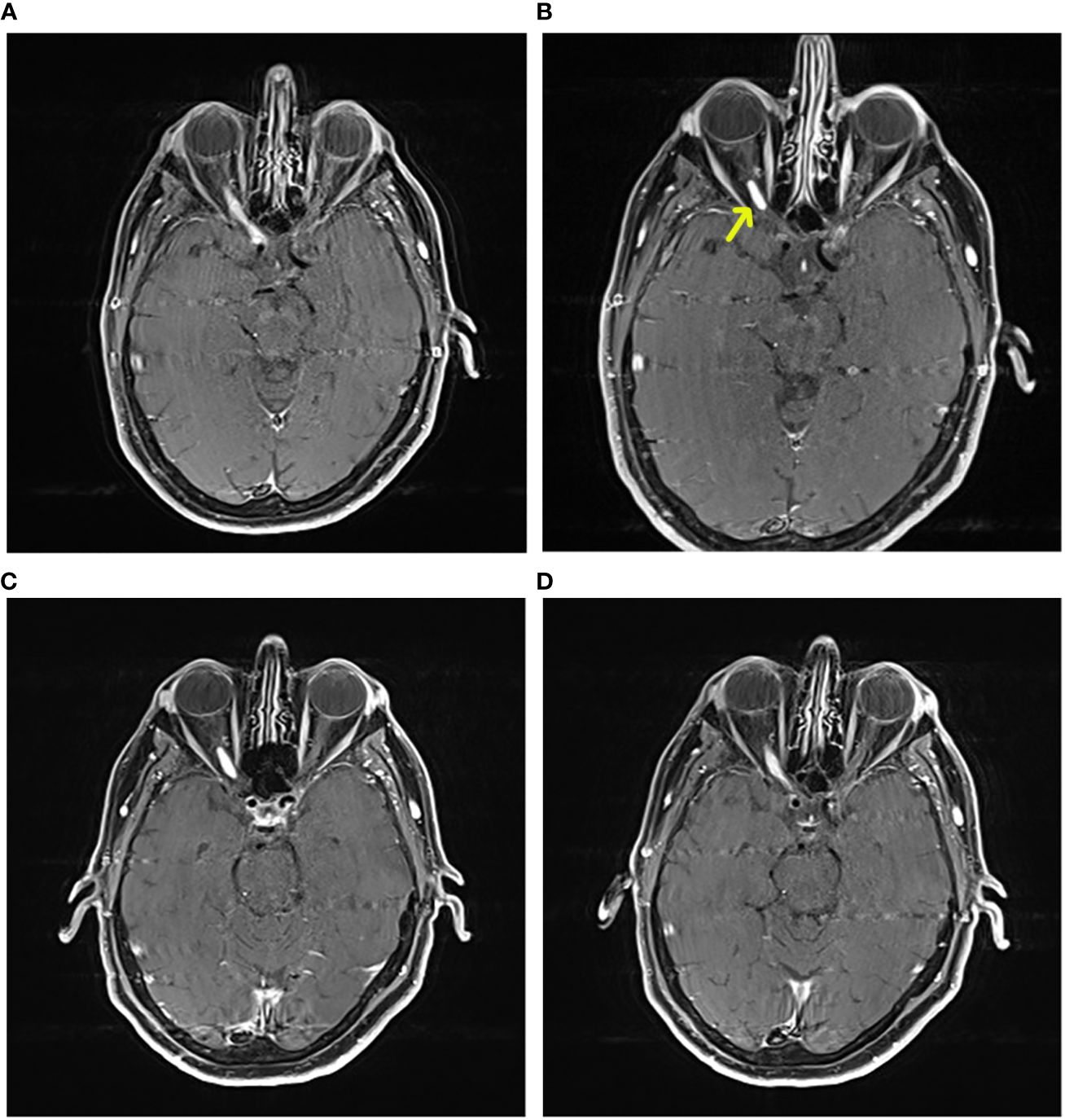
Figure 4 Axial contrast enhanced T1 MRI. A 56-year-old male VHL patient followed in our clinic with a right optic nerve hemangioblastoma. The patient experienced acute visual field defects in the right eye. Fundoscopy was normal. MRI showed a large right intraorbital optic nerve hemangioblastoma without edema (yellow arrow). Corticosteroids were not effective for reducing symptoms. Because surgical resection was unfeasible and was anticipated to lead to total blindness of the right eye, the patient was not operated – to cherish a couple more “good” years. Surgery will be planned as soon as peritumoral edema develops and threatens the contralateral eye. Tumor volume has now remained stable for 4 years. (A) time at diagnosis, tumor length 13mm and width 4mm. (B) 20 months later, tumor length 31mm and width 6.7mm (= growth); note progression towards optic chiasm, and less intense contrast enhancement, compared to (A, C): also 20 months, but shorter image acquisition time after contrast administration, now there is no growth compared to (A, D): longer image acquisition time after contrast administration, tumor length 24mm, width 6mm, there is growth compared to (A) Note peritumoral contrast leakage along optic nerve tract, similar to (B).
According to both literature and our own experience, sudden visual decline is often related to rapid development of (bilateral) white matter tract edema. Also, progressive disk swelling appears to be a red flag. Restrepo et al. reported a 33-year-old female patient with an intraorbital right optic nerve hemangioblastoma, who experienced bilateral progressive slight visual decline and proptosis over a 3-year period. What started as a right optic disc elevation, further evolved to a swollen and pale disc until the patient experienced sudden deterioration of vision in the right eye. The right optic nerve was completely resected and the patient became blind in her right eye (22). Stefani et al. published a similar case report on a 43-year-old male patient with an intracranial right optic nerve hemangioblastoma. The moment when the swollen optic disk became atrophic on fundoscopy, the patient experienced rapidly progressive blindness of the right eye over less than one year (33).
In some case reports, there is no focus on symptomatology or it is not mentioned (Kerr et al. (24), Hotta et al. (29), Miyagami et al. (26), Tanaka et al. (30), Uehara and Ichinomiya (32) and Verga et al. (7), Vásquez Montoya et al. (8).
Optic nerve hemangioblastomas cause symptoms by compression, displacement, and ultimately replacement of native optic nerve fibers and their vasculature (22, 36). We found 7 case reports on patients who were asymptomatic at time of diagnosis; hence, hemangioblastomas were discovered on annual MRI screening. Some hemangioblastomas were discovered by screening the family members of VHL patients (9, 11, 18, 23). All other reported patients were symptomatic at time of diagnosis. The time interval between initiation of symptoms and the seeking of medical attention ranged from 24 hours to 7 years.
Patients complain of sudden or gradual “vision loss” (5, 10, 12, 14–18, 20, 21, 25, 27–29, 31, 33), blurry vision (37), difficulty reading (25) or narrowing of the visual field (10, 20). Sometimes patients become progressively or very suddenly blind (28, 37). Other patients experience headache or a feeling of pressure (33). Rarely, hypopituitarism due to pituitary compression leads to diabetes insipidus with polydipsia, irregular menses, or secondary amenorrhea (9, 25).
A fairly large group of patients suffers from painful or painless (pulsating) proptosis with secondary lagophthalmos and corneal epithelial exposure changes (5, 13, 17, 18, 20, 22, 29, 31, 37). Ocular movement may be normal (14, 20), or patients may have motility disturbances such as skew deviation or exotropia (5). Intracanalicular compression may cause hypoesthesia in the V1 dermatome (5). Patients with advanced optic nerve or anterior optic pathway destruction may have a sluggish pupillary reaction to light (12), an afferent pupillary light defect (16, 22, 25), a relative afferent pupillary light defect (5, 12, 31, 35), or a dilated pupil without direct light reflex (20, 21, 27, 37). Visual acuity may range from normal to blind. Color vision may be diminished; this is not the case with most hemangioblastomas of the retina in VHL disease (16, 18). Visual fields may be full to confrontation (14, 18, 23). On formal visual field testing, various defects may be encountered: monocular blindness, concentric field narrowing (20, 33), quadranopsia (35), central or arcuate monocular defects (5, 15, 18, 21, 22, 35), peripheral field narrowing (22) or bitemporal hemianopia (18, 25). In our clinic we sometimes use optical coherence tomography (OCT) to visualize thinning of the ganglion cell layer secondary to central lesions causing visual field defects. Visual evoked potentials may be decreased or absent (27).
Fundus examination is normal in some patients (14, 16, 18, 23). When they are located in the anterior optic nerve, or just posterior to the lamina cribrosa, optic nerve hemangioblastomas cause optic disc elevation (5, 22, 33), progressive disc pallor (10, 17, 18, 21, 22, 28, 31), disc atrophy (5, 15, 25, 29, 33), pseudo-papilledema (false swelling), or anterior optic neuropathy due to infiltration. When located more posteriorly in the optic nerve, hemangioblastomas cause true swelling of the optic nerve and a posterior optic neuropathy (1, 6). Retinal pigment epithelium granularity may have an abnormal aspect, and epiretinal membranes or choroidal folds may be seen (18). Bilateral papilledema is caused by either bilateral optic hemangioblastomas or by edema spread through the chiasm.
Fluorescein angiography may be useful for discovery of optic nerve head hemangioblastomas, by showing early hyper-fluorescence and venous staining (12), or by directly exposing the tumors (21). VHL patients may simultaneously suffer from retinal and optic nerve hemangioblastomas; hence, making it difficult to identify the cause of vision loss. Clinicians need to be aware that retinal hemangioblastomas may mask and delay the discovery of intraorbital and intracranial optic nerve hemangioblastomas. The presence of an optic nerve hemangioblastoma should be considered when the type of vision disturbances cannot be explained by retinal lesions (18), and in the absence of visual improvement after photocoagulation. Also, previous enucleation of the eye due to large retinal lesions does not exclude the development of a hemangioblastoma along the course of the optic nerve, which can potentially harm the other eye by edematous spread.
In et al. mentioned normal blood biochemical analysis in their patient (37). Rubio et al. reported an erythrocyte sedimentation rate of 40mm/h in a patient with a right optic nerve hemangioblastoma. However, the patient had VHL disease with multi-organ involvement that may have interfered with the result. According to our own previous research, hematocrit may be high due to tumoral erythropoietin production that may be seen in hemangioblastomas (38).
As described in two cases, we recommend testing of pituitary function before surgery if the optic nerve hemangioblastomas is in close contact to the pituitary stalk or gland (9, 25).
Stefani and colleagues reported normal spinal fluid analysis in one patient. We found no other data on spinal fluid analysis in the literature (33).
On computed tomography (CT) imaging, optic nerve and chiasm hemangioblastomas appear isodense compared to normal brain parenchyma and show moderate or dense and diffuse enhancement after iodinated contrast administration (1, 22, 28, 29, 35). They can result in enlargement and/or kinking of the optic nerve or chiasm (17, 22). Tumors can be found at the optic nerve head, along the course of the optic nerve or at the chiasm, and therefore they can be situated intraorbitally, intracranially or both. They can be located on the sheath or the center of the optic nerve (22). On coronal CT images, optic nerve hemangioblastomas cannot be clearly distinguished from the optic nerve, and just seem to enlarge the optic nerve mass in toto (27, 35). Sometimes, optic hemangioblastomas cause concentric enlargement of the bony optic canal (31). Intraorbital tumors may extend intracranially towards the chiasm (23), or cause erosion of the planum sphenoidale, the anterior clinoid process (12, 14, 23, 31) or the tuberculum sellae (23). On CT, this bony infiltration may be seen as a widened area between the latter two (23). Orbital X-rays or CT may be used for evaluation of bony expansion and surgical planning (5, 22, 29, 37).
Optic nerve hemangioblastomas are usually well-defined solid iso-intense masses on T1-weighted MRI (15, 20, 23), and show intermediate or high signal intensity with varying degrees of homogeneity and vascular flow-voids on T2-weighted MRI (15, 18, 20, 22, 23, 35). If large enough, they intensely and homogeneously stain on contrast enhanced MRI, with clearly depicted borders (9, 10, 12–18, 20–23, 25, 27, 28, 35) and without dural enhancement, in comparison to meningiomas (15). According to our own experience, it may be tricky to distinguish hemangioblastomas from intraorbital fat on contrast enhanced T1-weighted MRI or Fluid Attenuated Inversion Recovery (FLAIR). When in doubt, Short Tau Inversion Recovery (STIR) or fat suppression sequences may be used.
Large peritumoral cysts are less often encountered than with cerebellar hemangioblastomas, which can also be found in VHL patients (20, 22).
Optic nerve hemangioblastomas have immature dilated vasculature, sometimes visible on MRI, with weak tight junctions and secondary leakage of plasma ultrafiltrate. The tumors are usually supplied by the high-flow ophthalmic artery. We believe that secretion of vasoactive substances and leakage of plasma ultrafiltrate may be the cause of the massive interstitial edema that is sometimes seen around the tumor. Edema typically spreads through low-resistance white matter tracts; hence, it preferentially spreads to the chiasm, the optic white matter tracts, the lateral geniculate bodies, the neuronal synapses and the optic radiations (13, 16, 18, 22, 28, 35). This vasogenic edema can have a disproportionately large volume compared to the tumor itself (13). Peritumoral edema has intermediate or high signal intensity on T2-MRI (22). It can be easily seen on FLAIR-images (13, 15, 16), but does not enhance after gadolinium contrast administration (22). Sometimes, edema spreads to the contralateral visual pathways, resulting in bilateral vision loss (13, 16, 28).
On conventional angiography, or CT/MRI angiography, optic nerve hemangioblastomas appear as highly vascular masses (22, 29, 37), showing homogenous staining (31). Tumors can be supplied by the usual vasculature of the optic nerve and chiasm i.e. the ophthalmic artery (17, 20, 22, 23, 29, 37), anterior cerebral artery, anterior communicating artery, superior hypophyseal artery, posterior communicating artery and anterior choroidal artery; or as described by some authors: the meningohypophyseal trunc (23), long posterior ciliary artery (22), superficial temporal artery (17) and internal maxillary artery (17). (Figure 2) Optic nerve hemangioblastomas have deep dilated draining veins (20, 31).
In cases where high perioperative bleeding is expected, preoperative embolization of major supplying vessels may be considered, but this is usually not feasible because of shared blood supply with the optic nerve.
In VHL patients, symptomatic retinal and other nervous system hemangioblastomas may lead to delay in diagnosis of an optic nerve hemangioblastoma (21). Also, hemangioblastomas may be mistaken on imaging for retrobulbar optic neuritis (20, 27, 33), optic nerve (microcystic) glioma either related or unrelated to neurofibromatosis type 1 (10, 12, 13, 17, 20–23, 25, 28, 31, 35), optic nerve sheath (angioblastic) clinoid or sphenoid wing meningioma either related or unrelated to neurofibromatosis type 2 (5, 10, 12, 14, 15, 20–23, 25, 27, 31, 37), schwannoma (10, 12, 20), germinoma (25), teratoma (25), craniopharyngioma (25), lymphoma (22, 28), granuloma (12, 22, 28), aneurysm (28), hemangioma (37), and hemangiopericytoma (5). Last, brain metastasis of a clear cell renal cell carcinoma should be considered, especially in VHL patients who are prone for the development of these malignant tumors (12, 17, 22).
The typical growth patterns of the abovementioned other tumors can be used for differentiation with optic nerve hemangioblastomas. Low-grade meningiomas grow slowly while gliomas and especially brain metastasis show rapid progression. It is however frustrating that hemangioblastomas are known for their capricious growth, which may be linear, exponential, saltatory or very rapid after years of stability (39).
Meningiomas can be calcified on CT (22). Optic nerve hemangioblastomas may cause expansion of the bony optic canal on coronal CT. This expansion is benign and usually non-erosive, while brain metastases may cause wide bony destruction (17).
Hemangioblastomas, meningiomas and gliomas can seem hyperintense on T1 MRI (23). Usually, optic nerve gliomas and optic neuritis do not fiercely enhance after contrast administration; whereas meningiomas, brain metastases and hemangioblastomas can enhance brightly; however, hemangioblastomas usually cause the largest mass of edema spreading throughout white matter tracts (17, 20–22, 35). Caution must be taken not to misidentify an infiltrating optic glioma or an astrocytoma from hemangioblastomatous edema or peritumoral gliosis respectively (13, 35).
Vascular flow voids can be seen in hemangioblastomas with thick vessels, but flow voids are absent in gliomas and can only rarely be seen in large meningiomas (18).
In meningiomas, a contrast enhancing dural tail may be seen on coronal MRI images, while hemangioblastomas and brain metastases are located within the nerve (12, 17).
On angiography, both hemangioblastomas and brain metastases seem like highly vascularized masses compared to gliomas (17). However, nevertheless its vascular nature, spontaneous bleeding in a hemangioblastoma is very rare. Nerad et al. suggested incisional biopsy for diagnosis of optic hemangioblastomas in patients with good vision and doubt of diagnosis; however, we do not recommend it because of the high risk of iatrogenic hemorrhage and morbidity. Also, an optic nerve tumor in a known VHL patient, is very likely to be a hemangioblastoma and not another rare optic nerve tumor (5). Conversely, if the patient is not known with VHL disease, the diagnosis of an optic nerve hemangioblastoma warrants screening for VHL disease.
No guidelines exist on the management on optic nerve hemangioblastomas. The authors of the VHL handbook recognize that optic nerve-sparing surgery can be very challenging; thus, they suggest not to operate on asymptomatic optic nerve hemangioblastomas, without further specification on the broad range of possible clinical scenarios (40). By combining our own experience to an in-depth review of all available cases in literature, we intended to create the first algorithm for management of optic nerve and chiasm hemangioblastomas in VHL patients.
Growth of an optic nerve hemangioblastoma can cause progressive vision impairment and proptosis. Even though optic nerve hemangioblastomas cause only compression and splicing of the optic nerve fibers, complete excision or restoration of lost visual function is usually not possible. Especially if tumors have resided for a long time in the optic nerve, some compressed nerve fibers may have become permanently damaged and replaced by tumor tissue (5, 16, 22, 28).
Postoperative visual prognosis depends on timing of diagnosis, preoperative visual function, tumor size, tumor location, and number of tumors. Postoperative improvement of vision may take a couple of hours to one week if vision loss is caused by peritumoral edema (16, 23, 35). Different authors have reported that the resolution of peritumoral edema may take three days to one week after transsphenoidal removal of optic nerve hemangioblastomas (13, 16, 18). Vision may transiently deteriorate immediately after surgery (23).
The surgical indications we found in the literature included: (1) young age, (2) radiographical growth, (3) postoperative vision loss expected to be minimal, (4) to prevent symptoms in an asymptomatic patient, and (5) to preserve contralateral vision (18). Some authors have stated that watchful waiting always results in vision impairment (21); however, based on our own success with the watchful waiting approach, we cannot agree with this statement. We only recommend considering surgery if patients develop vision impairment, if tumors grow fast, or if there is contralateral spread of either tumor or edema.
Rapid visual decline and bilateral symptoms due to peritumoral edema are major indications for urgent surgery (18, 35, 41). Edema is an early indicator of impending vision disturbance (16).
Most authors recommend complete excision of the optic nerve if vision is already lost and the patient has severe or painful proptosis (5, 35). Incomplete resection of such hemangioblastomas usually leads to recurrence and accelerated growth (22, 42–44). Postoperatively, regression of proptosis may take some months (5).
In VHL patients, contralateral eye function and prognosis of other VHL-associated tumors are also major influencers on surgical decision making.
A suggested follow-up and treatment protocol is graphically summarized in Figure 5.
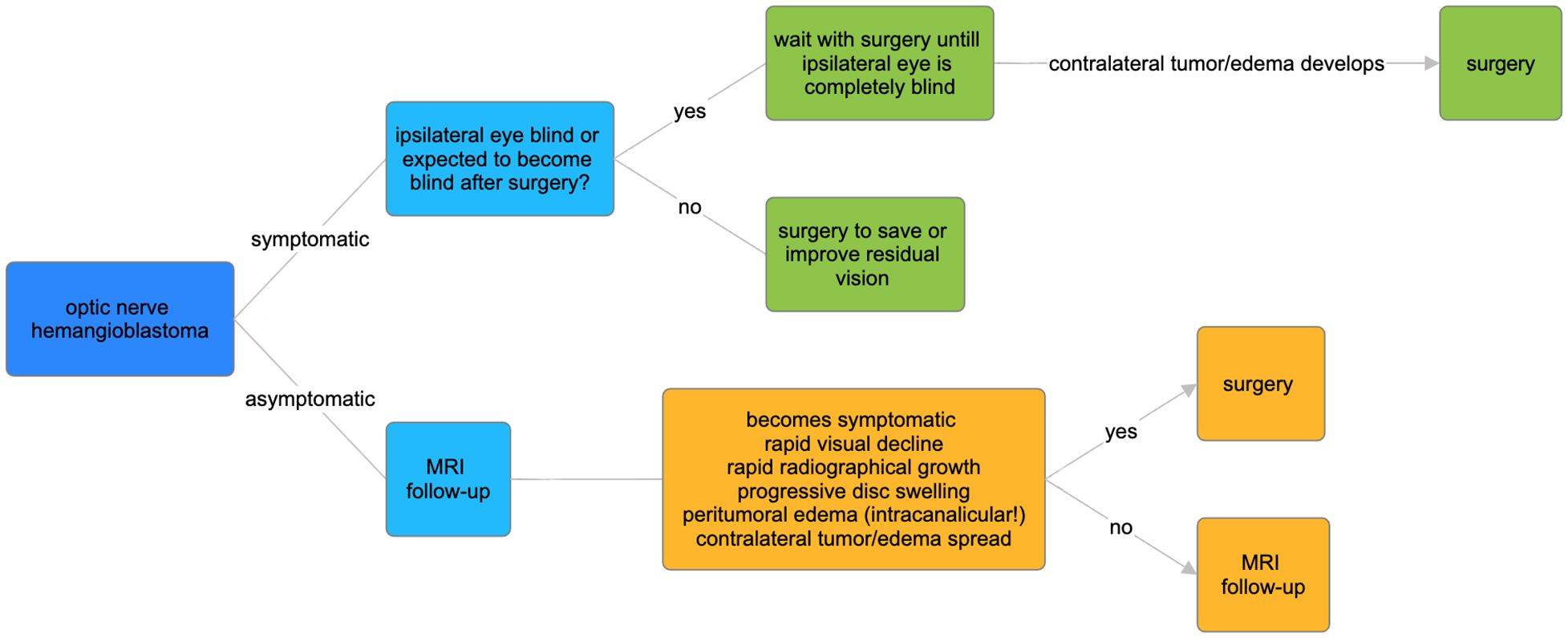
Figure 5 Suggested protocol for treatment and follow-up of VHL optic nerve hemangioblastomas.
Various surgical techniques for removal of optic nerve hemangioblastomas can be found in the literature. The lateral orbitotomy (5, 35), frontal orbitotomy (20) and frontal extradural approach (29) have been described for intraorbital tumors. For intracranial tumors nearby the chiasm, authors have described the suprabrow craniotomy (15), transnasal-transsphenoidal approach (18) and sublabial transseptal transsphenoidal approach (i.e. removing the posterior portion of the planum sphenoidale). The anterior chiasm can also be reached with orbitotomy, while frontal (extradural) craniotomy can be used for posterior intraorbital tumors (37). The fronto-temporal craniotomy (13, 14), mini-pterional craniotomy and transnasal-transsphenoidal approach can be used for intracranial tumors with intracanalicular extension. In order to reach intracranial tumors proximal to the canal, the sublabial extended transsphenoidal approach (16) has been described. Nerad et al. used a CO2 laser to reach intracranially extending orbital tumors (5). By using a frontal approach, the entry of the optic canal can also be exposed (37). However, some neurosurgeons prefer not to disturb canalicular anatomy because of the risk of disrupting the annulus of Zinn where the four rectus muscles originate.
The transsphenoidal access may be valuable for growing children with normal pituitary function because it avoids frontotemporal lobe retraction and separation of the sylvian fissure. Depending on the experience of the surgeon, transsphenoidal surgery is less likely to cause morbidity and mortality. Nevertheless, an large sella is required for broad exposure because internal carotid artery injury is an eminent threat (9).
In the literature, all authors describe optic hemangioblastomas as soft, highly vascular orange-red tumors, with tortuous blood vessels on the surface. Hemangioblastomas are solid or partly cystic. They are not attached to the dura mater and do not have a capsule. The tumor may be centrally or peripherally located in the optic nerve (22). It may be difficult to differentiate tumor from native nerve fibers (20). Sometimes, the tumor is firmly attached to the pial nerve sheet (18). If tumors are completely embedded in the optic nerve, surgeons seem to prefer a longitudinal dissection through the damaged part of the nerve, close to the surface of the tumor, thus minimizing the risk of nerve fiber loss (13, 15, 24). Raila et al. described removal of an optic hemangioblastoma using piecemeal dissection (23); however, we do not recommend it because hemangioblastomas typically bleed profoundly; and to avoid optic nerve ischemia, care should be taken with coagulation. Following other authors, we rather recommend coagulation of the major supplying vessel prior to circumferential dissection from the pia in toto (15, 16). When there is an associated cyst, we suggest to first fenestrate the cyst in order to widen the surgical field and facilitate dissection of the nodule.
We found many literature cases where the optic nerve was resected together with the tumor, resulting in blindness of the eye. Different portions of the optic nerve can be resected: the intraorbital portion up to the entry point in the optic canal, the intracanalicular portion, and the extraorbital portion up to the chiasm. Staub et al. have advised not to transect the optic nerve too close to the chiasm. This action may harm “Wilbrand’s knee”: a loop of decussating fibers that originates from the contralateral optic nerve, and heads to the ipsilateral optic tract. Lee and colleagues believe that this loop is a histological artifact, and that it is only seen in enucleated eyes with secondary optic atrophy of the contralateral eye. We conclude that it seems reasonable to section the optic nerve 1–2mm in front of the chiasm (13, 45); however, there are no studies on optic tractography to support our suggestion (13).
Optic nerve hemangioblastomas may bleed profoundly, leading to postoperative visual decline. Therefore, we do not recommend performing a biopsy or incision unless the tumor is totally resected (28). Some optic hemangioblastomas may be difficult to access, because of their central location in the optic nerve, or involvement of the surrounding structures such as the internal carotid artery.
It may be challenging to reach tumors inside the optic canal. Even though intracanalicular hemangioblastomas may remain stable for a long time (46), sudden white matter edema and swelling of the optic nerve in this narrow alley may result in rapidly evolving blindness. The intracanalicular and intraorbital portions of the optic nerve are poorly vascularized and collateralized. This natural vascular handicap can be magnified by a steal phenomenon from the hemangioblastoma (47). The intracanalicular portion of the optic nerve is supplied by two or three small trunks from the superior hypophyseal artery, and to a lesser part by the ophthalmic artery; branching into a microscopic dense capillary network that is prone to perioperative bleeding (34, 48). The vulnerability of this vasculature, together with the imminent threat of edema, makes this narrow alley a worthy adversary during surgery.
Other reported surgical complications are eye motility disturbance (5) and transient diabetes insipidus due to hypophyseal traction (23). Transsphenoidal approaches may be complicated by bleeding, cerebrospinal fluid rhinorrhea and meningitis (9).
Contrast-enhanced MRI can be used for follow-up of tumor volume and peritumoral edema. According to our own experience, the typical leaky vasculature of hemangioblastomas may cause contrast extravasation and therefore an overestimation of tumor volume on MRI. We suggest standardizing the time interval between intravenous gadolinium administration and MRI image acquisition, to minimize the effect of this overestimation on tumor volume comparison (Figure 4).
We found some case-reports mentioning that high-dose radiation therapy is ineffective for reduction of hemangioblastoma volume (5, 10). We have the same experience, and believe that the use of radiotherapy is not justifiable due to devastating side-effects and potential worsening of ipsilateral or contralateral vision. Stereotactic radiosurgery may be considered in very selected cases with multifocal, nonresectable, partially resected or recurrent tumors, or for patients with surgical contraindications, or if there is surgical fatigue. The latter can be a major issue in patients with VHL disease (10, 14, 49, 50). However, chances are high that radiosurgery will not influence tumor volume.
The use of high dose intravenous corticosteroids has been described in several case reports, and often because optic neuritis was suspected at initial presentation. Subjective improvement of vision has been described by patients; however, we found no reports on objective improvement as measured by technical examination (12, 16, 35). The administration of corticosteroids seems reasonable for temporary relief of vasogenic edema surrounding hemangioblastomas.
For non-optic nerve VHL related hemangioblastomas, surgical resection remains the gold standard. Pharmacological trials have recently been focusing on the inhibition of Hypoxia Response Elements and their respective receptors, especially vascular endothelial growth factor and receptor (VEGF, VEGFR). There have been pharmacological triumphs in the treatment of VHL clear cell carcinomas, for example with the HIF2α inhibitor belzutifan. Belzutifan also seems to be efficacious for hemangioblastoma tumor control; however, intratumoral hemorrhages have been described, necessitating the development of other therapies. The effect on optic nerve hemangioblastomas has not been investigated and this will remain challenging given their rarity.
If hemangioblastomas of the optic nerve and chiasm are diagnosed, we suggest annual routine follow-up as long as patients do not develop vision deficiency. If tumors grow fast and/or patients develop vision impairment we recommend resection, because impairment is irreversible, and resection of large tumors carries a higher risk of further vision decline. If the patient is already blind, we recommend surgical resection if MRI shows imminent edema or tumor spread to the chiasm or contralateral optic nerve. Edema can be present before vision impairment becomes clinically evident. If the patient is almost blind, we recommend waiting until full blindness (because vision sparing surgery is unlikely at this stage), unless the contralateral eye is threatened by spreading edema.
All relevant data is contained within the article: the original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving humans were approved by Universitair Ziekenhuis Brussel ethics committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
EV: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. J-HK: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. MK: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. CS: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. RK: Data curation, Formal analysis, Writing – original draft, Conceptualization. SR: Data curation, Formal analysis, Investigation, Writing – original draft, Conceptualization. A-MV: Data curation, Formal analysis, Investigation, Writing – original draft, Conceptualization. CA: Writing – original draft, Conceptualization, Methodology. SG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Miller NR. Primary tumours of the optic nerve and its sheath. Eye (Lond). (2004) 18:1026–37. doi: 10.1038/sj.eye.6701592
2. Poulsen ML, Budtz-Jorgensen E, Bisgaard ML. Surveillance in von Hippel-Lindau disease (vHL). Clin Genet. (2010) 77:49–59. doi: 10.1111/j.1399-0004.2009.01281.x
3. Toy BC, Agron E, Nigam D, Chew EY, Wong WT. Longitudinal analysis of retinal hemangioblastomatosis and visual function in ocular von Hippel-Lindau disease. Ophthalmology. (2012) 119:2622–30. doi: 10.1016/j.ophtha.2012.06.026
4. Wittstrom E, Nordling M, Andreasson S. Genotype-phenotype correlations, and retinal function and structure in von Hippel-Lindau disease. Ophthalmic Genet. (2014) 35:91–106. doi: 10.3109/13816810.2014.886265
5. Nerad JA, Kersten RC, Anderson RL. Hemangioblastoma of the optic nerve. Report of a case and review of literature. Ophthalmology. (1988) 95:398–402. doi: 10.1016/s0161-6420(88)33184-2
6. Volpe NJ. Compressive and infiltrative optic neuropathies. In: Miller NR, Newman NJ, editors. Walsh and hoyt's clinical neuro-ophthalmology, vol. 396. Philadelphia: Lippincott Williams & Wilkins (2005). p. 403–7.
7. Verga P. Angio-reticolo-glioma cistico del nervo ottico. Rivista Oto-neuro-oftalmologica. (1930) 7:101–33.
8. Vasquez Montoya JD, Velez JM, Naranjo Vanegas M, Montes Jimenez N. Optic nerve haemangioblastoma in association with von Hippel-Lindau syndrome: case report and literature review. BJR Case Rep. (2024) 10:uaae007. doi: 10.1093/bjrcr/uaae007
9. Kouri JG, Chen MY, Watson JC, Oldfield EH. Resection of suprasellar tumors by using a modified transsphenoidal approach. Report of four cases. J Neurosurg. (2000) 92:1028–35. doi: 10.3171/jns.2000.92.6.1028
10. Kanno H, Osano S, Shinonaga M. VHL-associated optic nerve hemangioblastoma treated with stereotactic radiosurgery. J Kidney Cancer VHL. (2018) 5:1–6. doi: 10.15586/jkcvhl.2018.104
11. Turkoglu EB, Say EA, Shields CL. Spontaneous devascularization and detachment of optic nerve hemangioblastoma in a patient with von hippel-lindau disease. JAMA Ophthalmol. (2016) 134:e161119. doi: 10.1001/jamaophthalmol.2016.1119
12. Fard MA, Hassanpoor N, Parsa R. Bilateral optic nerve head angiomas and retrobulbar haemangioblastomas in von hippel-lindau disease. . Neuroophthalmology. (2014) 38:254–6. doi: 10.3109/01658107.2014.944622
13. Staub BN, Livingston AD, Chevez-Barrios P, Baskin DS. Hemangioblastoma of the optic nerve producing bilateral optic tract edema in a patient with von Hippel-Lindau disease. Surg Neurol Int. (2014) 5:33. doi: 10.4103/2152-7806.128430
14. Zywicke H, Palmer CA, Vaphiades MS, Riley KO. Optic nerve hemangioblastoma: a case report. Case Rep Pathol. (20122012) 915408. doi: 10.1155/2012/915408
15. Prabhu K, Daniel RT, Chacko G, Chacko AG. Optic nerve haemangioblastoma mimicking a planum sphenoidale meningioma. Br J Neurosurg. (2009) 23:561–3. doi: 10.1080/02688690902965964
16. Baggenstos M, Chew E, Butman JA, Oldfield EH, Lonser RR. Progressive peritumoral edema defining the optic fibers and resulting in reversible visual loss. J Neurosurg. (2008) 109(2):313–7. doi: 10.3171/JNS/2008/109/8/0313
17. Barrett R, Meyer D, Boulos A, Eames F, Torres-Mora J. Optic nerve hemangioblastoma. Ophthalmology. (2008) 115:2095. doi: 10.1016/j.ophtha.2008.06.003
18. Meyerle CB, Dahr SS, Wetjen NM, Jirawuthiworavong GV, Butman JA, Lonser RR, et al. Clinical course of retrobulbar hemangioblastomas in von Hippel-Lindau disease. Ophthalmology. (2008) 115:1382–9. doi: 10.1016/j.ophtha.2008.01.027
19. Alvarez R, Mastorakos P, Hogan E, Scott G, Lonser RR, Wiley HE, et al. Retrobulbar hemangioblastomas in von hippel-lindau disease: clinical course and management. Neurosurgery. (2021) 88(5):1012–20. doi: 10.1093/neuros/nyaa565
20. Higashida T, Sakata K, Kanno H, Kawasaki T, Tanabe Y, Yamamoto I. Hemangioblastoma of the optic nerve–case report. Neurol Med Chir (Tokyo). (2007) 47:215–8. doi: 10.2176/nmc.47.215
21. Fons Martinez MR, Espana Gregori E, Avino Martinez JA, Hernandez Pardines F. [An optic nerve tumor in von Hippel-Lindau disease, masquerading as a retinal hemangioma]. Arch Soc Esp Oftalmol. (2006) 81:293–6. doi: 10.4321/s0365-66912006000500009
22. Restrepo S, Carter JE, Friedman M, Arabandi M, Kagan-Hallett K. Case 5: An optic nerve mass in von Hippel-Lindau disease. 35th Annu Frank B Walsh Soc Sessions City. (2003).
23. Raila FA, Zimmerman J, Azordegan P, Fratkin J, Parent AD. Successful surgical removal of an asymptomatic optic nerve hemangioblastoma in von Hippel-Lindau disease. J Neuroimaging. (1997) 7:48–50. doi: 10.1111/jon19977148
24. Kerr DJ, Scheithauer BW, Miller GM, Ebersold MJ, McPhee TJ. Hemangioblastoma of the optic nerve: case report. Neurosurgery. (1995) 36:573–80. doi: 10.1227/00006123-199503000-00017. discussion 580-571.
25. Balcer LJ, Galetta SL, Curtis M, Maguire A, Judy K. von Hippel-Lindau disease manifesting as a chiasmal syndrome. Surv Ophthalmol. (1995) 39:302–6. doi: 10.1016/s0039-6257(05)80107-9
26. Miyagami M, Miyagi A, Kido G, Satoh K, Tsubokawa T. [The two familial occurrence of von Hippel-Lindau disease]. No To Shinkei. (1994) 46:683–9.
27. Rubio A, Meyers SP, Powers JM, Nelson CN, de Papp EW. Hemangioblastoma of the optic nerve. Hum Pathol. (1994) 25:1249–51. doi: 10.1016/0046-8177(94)90044-2
28. Ginzburg BM, Montanera WJ, Tyndel FJ, Griesman JA, McLennan MK, TerBrugge KG, et al. Diagnosis of von Hippel-Lindau disease in a patient with blindness resulting from bilateral optic nerve hemangioblastomas. AJR Am J Roentgenol. (1992) 159:403–5. doi: 10.2214/ajr.159.2.1632366
29. Hotta H, Uede T, Morimoto S, Tanabe S, Hashi K, Takeda M. Optic nerve hemangioblastoma. Case report]. Neurol Med Chir (Tokyo). (1989) 29:948–52. doi: 10.2176/nmc.29.948
30. Tanaka E, Kimura C, Inoue H, Kigasawa K, Shiga H. A case of intraorbital hemangioblastoma of the optic nerve. Folia Jpn Ophthalmol. (1984) 35:1390–5.
31. Lauten GJ, Eatherly JB, Ramirez A. Hemangioblastoma of the optic nerve: radiographic and pathologic features. AJNR Am J Neuroradiol. (1981) 2:96–9.
32. Uehara M, Ichinomiya T. A case of intraorbital optic nerve hemangioblastoma associated with von Hippel's disease. Folia Opthalmol Jpn. (1975) 26:1219–26.
33. Stefani FH, Rothemund E. Intracranial optic nerve angioblastoma. Br J Ophthalmol. (1974) 58:823–7. doi: 10.1136/bjo.58.9.823
34. van Overbeeke J, Sekhar L. Microanatomy of the blood supply to the optic nerve. Orbit. (2003) 22:81–8. doi: 10.1076/orbi.22.2.81.14316
35. McGrath LA, Mudhar HS, Salvi SM. Optic nerve haemangioblastoma: signs of chronicity. Ocul Oncol Pathol. (2018) 4:370–4. doi: 10.1159/000486863
36. Christmas NJ, Mead MD, Richardson EP, Albert DM. Secondary optic nerve tumors. Surv Ophthalmol. (1991) 36:196–206. doi: 10.1016/0039-6257(91)90002-w
37. In S, Miyagi J, Kojho N, Kuramoto S, Uehara M. Intraorbital optic nerve hemangioblastoma with von Hippel-Lindau disease. Case report. J Neurosurg. (1982) 56:426–9. doi: 10.3171/jns.1982.56.3.0426
38. Glasker S, Kruger MT, Klingler JH, Wlodarski M, Klompen J, Schatlo B, et al. Hemangioblastomas and neurogenic polyglobulia. Neurosurgery. (2013). doi: 10.1227/NEU.0b013e31828ba793
39. Wanebo JE, Lonser RR, Glenn GM, Oldfield EH. The natural history of hemangioblastomas of the central nervous system in patients with von Hippel-Lindau disease. J Neurosurg. (2003) 98:82–94. doi: 10.3171/jns.2003.98.1.0082
40. VHLalliance. What you need to know about VHL. In: A reference handbook for people with von Hippel-Lindau, their families, and their medical teams. (2020).
41. Eckstein RP, Wills EJ, Segelov JN. Haemangioblastoma of the optic nerve. Case report with study by light and electron microscopy. Pathology. (1981) 13:357–64. doi: 10.3109/00313028109081675
42. Okawara SH. Solid cerebellar hemangioblastoma. J Neurosurg. (1973) 39:514–8. doi: 10.3171/jns.1973.39.4.0514
43. Olivecrona H. The cerebellar angioreticulomas. J Neurosurg. (1952) 9:317–30. doi: 10.3171/jns.1952.9.4.0317
44. Silver ML, Hennigar G. Cerebellar hemangioma (hemangioblastoma); a clinicopathological review of 40 cases. J Neurosurg. (1952) 9:484–94. doi: 10.3171/jns.1952.9.5.0484
45. Lee JH, Tobias S, Kwon JT, Sade B, Kosmorsky G. Wilbrand's knee: does it exist? Surg Neurol. (2006) 66:11–7. doi: 10.1016/j.surneu.2005.11.004
46. Turel MK, Kucharczyk W, Gentili F. Optic nerve hemangioblastomas?A review of visual outcomes. Turk Neurosurg. (2017) 27:827–31. doi: 10.5137/1019-5149.JTN.16680-15.1
47. Handa J, Nakazawa T, Watanabe K, Suzuki F. Haemangioblastoma with multiple dural arterial supply. Case report. Acta Neurochir (Wien). (1984) 73:193–9. doi: 10.1007/BF01400852
48. Hayreh SS, Dass R. The ophthalmic artery: I. Origin and intra-cranial and intra-canalicular course. Br J Ophthalmol. (1962) 46:65–98. doi: 10.1136/bjo.46.2.65
49. Kano H, Shuto T, Iwai Y, Sheehan J, Yamamoto M, McBride HL, et al. Stereotactic radiosurgery for intracranial hemangioblastomas: a retrospective international outcome study. J Neurosurg. (2015) 122:1469–78. doi: 10.3171/2014.10.JNS131602
Keywords: von Hippel-Lindau, eye, optic nerve, optic chiasm, optic hemangioblastoma, hemangioblastoma, review, VHL
Citation: Vergauwen E, Klingler J-H, Krüger MT, Steiert C, Kuijpers R, Rosahl S, Vanbinst A-M, Andreescu CE and Gläsker S (2024) Optic nerve and chiasm hemangioblastomas in von Hippel-Lindau disease: report of 12 cases and review of the literature. Front. Oncol. 14:1334564. doi: 10.3389/fonc.2024.1334564
Received: 07 November 2023; Accepted: 19 June 2024;
Published: 09 July 2024.
Edited by:
Maria Caffo, University of Messina, ItalyReviewed by:
Kristin Huntoon, University of Texas MD Anderson Cancer Center, United StatesCopyright © 2024 Vergauwen, Klingler, Krüger, Steiert, Kuijpers, Rosahl, Vanbinst, Andreescu and Gläsker. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Evelynn Vergauwen, ZXZlbHlubi12QGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.