
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Oncol. , 05 July 2024
Sec. Gastrointestinal Cancers: Gastric and Esophageal Cancers
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1326970
This article is part of the Research Topic Advanced Molecular Targets in the Diagnosis and Treatment of Gastrointestinal Cancers, volume II View all 16 articles
 Luchang Cao1†
Luchang Cao1† Guanghui Zhu1,2†
Guanghui Zhu1,2† Xinmiao Wang1†
Xinmiao Wang1† Ziyu Kuang1,2
Ziyu Kuang1,2 Xiaotong Song1Xinyi Ma1
Xiaotong Song1Xinyi Ma1 Xiaoyu Zhu1
Xiaoyu Zhu1 Ruike Gao1
Ruike Gao1 Jie Li1*
Jie Li1*Introduction: Postoperative recurrence and metastasis of gastric cancer (GC) are primary factors that contribute to poor prognosis. GC recurs at a rate of approximately 70%–80% within 2 years after local treatment and approximately 90% within 5 years. “Yang-deficient toxic node” is the core pathogenesis of GC recurrence and metastasis. The Yiqi Wenyang Jiedu prescription (YWJP), a form of complementary and alternative medicine in China, is an empirical remedy to prevent postoperative recurrence and metastasis of GC. Taking the main therapeutic principles of “nourishing Qi and warming Yang, strengthening Zhengqi, and detoxifying” can aid in preventing the recurrence and metastasis of GC in patients during the watchful waiting period after surgery and adjuvant chemotherapy. This approach aims to enhance the quality of life of patients. However, high-quality evidence to support this hypothesis is lacking. This study will aim to investigate the efficacy and safety of YWJP to prevent and treat postoperative metastasis and GC recurrence.
Methods: The study will be a multicenter, randomized, double-blind, placebo-parallel-controlled clinical trial. A total of 212 patients who completed adjuvant chemotherapy within 8 months of radical gastrectomy will be enrolled. Patients in the intervention group will receive the YWJP, whereas those in the control group will receive a placebo. The main outcome was the disease-free survival (DFS) rate 2 years after surgery. The secondary outcomes included DFS time, overall survival, annual cumulative recurrence and rate of metastasis after 1–3 years, cumulative annual survival after 1–3 years, fat distribution-related indicators, tumor markers, peripheral blood inflammatory indicators, prognostic nutritional index, symptoms and quality of life evaluation, medication compliance, and adverse reaction rate.
Discussion: There is a lack of effective therapy after the completion of adjuvant therapy during the postoperative period of watchful waiting. This study will be the first randomized clinical trial to evaluate whether complementary and alternative medical interventions can effectively prevent recurrence and metastasis during the watchful waiting period after GC surgery and to provide evidence for surveillance treatment management after GC surgery.
Clinical trial registration: ClinicalTrials.gov, identifier NCT05229809.
● Question
● Can Yiqi Wenyang Jiedu prescription reduce the rate of recurrence and metastasis in patients with gastric cancer during the watchful waiting period after surgery?
● Findings
● This randomized clinical trial will involve 212 patients with GC who completed adjuvant chemotherapy after surgery. The primary outcome was disease-free survival at a rate of 2 years after surgery.
● Meaning
● This ongoing clinical trial will supply the treatment management during the watchful waiting period after GC surgery and provide evidence for the effectiveness of complementary and alternative medicine in reducing recurrence and metastasis rates after GC surgery.
Gastric cancer (GC) is a common malignant tumor of the digestive system, and according to the Global Cancer Statistics 2022, the number of new GC cases worldwide is 968,350, ranking fifth among all malignancies. The number of deaths was 659,853, ranking fifth among all cancer types (1, 2). China has the highest cancer burden worldwide, according to the National Cancer Center of China (3), and they projected that an estimated 4,824,700 new cancer cases and 2,574,200 new cancer deaths will occur in China in 2022. Among these, GC ranked fifth and third among new cases and deaths, respectively. Despite a decline in GC incidence observed in many countries, the total number of GC cases worldwide shows a slow upward trend, particularly in China (4, 5). Even more terrifying is that the global burden caused by the rising trend of GC cases is expected to increase by 62% to 1.77 million cases in 2040 (6). Studies have confirmed that various factors such as Helicobacter pylori infection (7), cigarette smoking (8, 9), heavy alcohol consumption (10–12), sex (13), obesity (14, 15), metabolic dysfunction (16, 17), and so on (18–26) are recognized as major risk factors for GC incidence.
Surgery is currently the preferred treatment for GC. The National Comprehensive Cancer Network guidelines (2023. V1) recommend that patients with stage pT3–4 cancer, any N, should undergo post-surgical chemoradiotherapy followed by a period of surveillance and management (27–39). Approximately 70%–80% of patients with GC relapsed within 2 years after local therapy. The median recurrence time for GC is approximately 16.8 months (40–42). Previous studies have shown that Yang deficiency is one of the main syndromes of GC (43), Yang deficiency and a low metabolic state can stimulate cancer cells to induce metabolic reprogramming and promote postoperative recurrence and metastasis of GC (44–48). Therefore, during the period between postoperative recovery and the onset of GC recurrence and metastasis, identifying effective treatment strategies is crucial and requires urgent attention.
Complementary and alternative medicine is a safe and effective potential choice that can improve the overall survival (OS) of patients with GC (49–51). Previous studies have indicated that patients with GC who experience Qi and Yang deficiencies after surgery are more susceptible to recurrence and metastasis than those with no Qi and Yang deficiencies (52, 53). The Yiqi Wenyang Jiedu prescription (YWJP) follows the treatment principles of nourishing Qi and warming Yang, strengthening Zhengqi, and detoxifying, and can improve the physical condition and alleviate clinical symptoms in patients with Yang deficiency (54, 55). YWJP may improve patients’ low metabolic state by regulating the tumor microenvironment and delaying or reversing recurrence and metastasis. Therefore, we plan to conduct a multicenter, randomized, double-blind, placebo-parallel-controlled clinical trial that will apply YWJP, an effective prescription for the prevention and treatment of recurrence and metastasis of postoperative GC at the Guang’anmen Hospital of China Academy of Chinese Medical Sciences, and explore its mechanisms.
The multicenter, randomized, double-blind, placebo-parallel-controlled clinical study will be conducted at seven hospitals, including Guang’anmen Hospital of the China Academy of Chinese Medical Sciences, Jiangsu Provincial Hospital of Traditional Chinese Medicine (TCM), the First Affiliated Hospital of Guangzhou University of Chinese Medicine, and Yueyang Hospital of Integrated Traditional Chinese and Western Medicine Affiliated to Shanghai University of Chinese Medicine. After signing the informed consent forms, 212 participants will be randomly assigned to the intervention group (YWJP) or the control group (YWJP placebo).
The key herbs of YWJP include Astragalus membranaceus (30 g), Codonopsis pilosula (15 g), Angelica dahurica (10 g), Curcuma zedoary (9 g), Rhizoma nardostachyos (10 g), Polygonum cuspidatum (10 g), Radix Actinidiae chinensis (15 g), and Paris polyphylla (9 g) (108 g in total). The control group will receive a YWJP placebo intervention comprising maltodextrin, lactose, bitters, citric acid, and other edible-grade raw materials (108 g in total). All experimental herbs and placebos used in this study will be provided by Jiangyin Tianjiang Pharmaceutical Co., Ltd. All raw materials have undergone safety assessments and quality inspection reports have been issued. YWJP and its placebo have been confirmed to be safe, reliable, controllable in quality, and similar in shape, color, smell, and taste.
The primary and secondary outcomes will be evaluated immediately at the end of the follow-up period. The study process is illustrated in Figure 1. The clinical trial protocol complied with the Clinical Trial Standard Protocol Items: Recommendations for Interventional Trials (56) and Consolidated Standards of Reporting Trials (CONSORT) (57).

Figure 1 CONSORT flow diagram.
We plan to recruit patients from seven traditional Chinese oncology hospitals nationwide, led by Guang’anmen Hospital, and enroll patients by following up with expert clinics, playing recruitment advertisements on hospital LED screens, and posting recruitment posters. When we encounter potential patients, we will introduce our study protocol, including the objectives, intervention methods, processes, and potential adverse reactions. The research team will conduct repeated screenings of patients on a two-person basis. Patients who meet the inclusion criteria and wish to voluntarily participate in the study will sign an informed consent form.
The diagnostic criteria for GC, according to the 2021 Chinese Society of Clinical Oncology (CSCO), will be followed. The diagnosis and treatment of GC follow the clinical guidelines outlined in the 8th edition of the International Union Against Cancer (UICC) classification system (58).
1. Research cases must be sourced from real-world registration platforms.
2. Stage II–III non-esophageal gastric junction GC that meets the diagnostic criteria and does not indicate tumor recurrence or metastasis by imaging.
3. Patients with GC who underwent radical gastrectomy (R0) within 8 months after surgery and completed at least six cycles of adjuvant chemotherapy with standard regimens (XELOX and SOX).
4. Eastern Cooperative Oncology Group (ECOG) performance status score of 0–2.
5. Patient ages ranging from 18 to 75 years, with no sex limitations.
6. Expected survival time ≥3 months.
7. Patients who voluntarily participated in the study, signed an informed consent form, and participated in the follow-up.
1. Patients with concomitant primary tumors in other areas.
2. Patients with GC who were pathologically diagnosed with adenosquamous carcinoma, lymphoid interstitial carcinoma (medullary carcinoma), hepatoid adenocarcinoma, squamous cell carcinoma, signet ring cell carcinoma, undifferentiated carcinoma, and other gastric malignancies, such as gastric neuroendocrine tumors, gastric interlobular tumors, and gastric malignant lymphoma.
3. Patients who received neoadjuvant chemotherapy before surgery.
4. Patients who have been and are currently receiving targeted drug therapy.
5. Patients who have undergone or are currently undergoing gastric radiation therapy.
6. Patients who have undergone or are currently undergoing tumor immunotherapy.
7. Patients with mental illness.
8. Patients with severe and uncontrollable organic lesions or infections such as decompensated heart, lung, or kidney failure, who cannot tolerate chemotherapy.
9. Patients who underwent clinical trials of small-molecule drugs within 28 days or large-molecule drugs within 3 months.
10. Patients who are known to be allergic or intolerant to the study drug.
1. Those who experienced unexpected events during the treatment process and were unable to adhere to the protocol.
2. Patients who voluntarily requested withdrawal.
3. The researchers judged patients who exhibited poor compliance and were unable to continue clinical research.
4. Patients experiencing pregnancy, death, or loss of follow-up.
This study will apply an Interactive Web Response System for central randomization and implement hidden allocation schemes. Patients will be randomly divided into intervention and control groups in a 1:1 ratio based on central randomization. The R software (V3.3.3) will be used to generate random sequences with three rounds of cyclic random statements. The blinding level will be double-blind, in which neither the researcher nor the participant have any idea of the specific details of the study. Anonymizing will be performed by statisticians who did not participate in the clinical trials and divided into two levels. This trial will establish a dedicated “emergency letter” for clinical trials that can only be urgently unblinded when the patient experiences an emergency. Handling this situation requires a clear understanding of the patient’s medication information.
The intervention group will receive YWJP, whereas the control group will receive YWJP placebo. Patients will take one pack each time, dilute it with boiling water, and administer it twice daily (in the morning and evening). The course of treatment will be 4 weeks, and six courses are planned.
After enrollment, patients will take their medication according to the method described in the “intervention” section. During the intervention, symptoms such as nausea, vomiting, liver and kidney dysfunction, diarrhea, and infection will be treated with medication. However, specific symptoms and combined medications must be recorded. Receiving modern antitumor treatment (including chemotherapy, immunotherapy, molecular targeted therapy, and radiotherapy) or taking other Chinese herbal decoctions, Chinese herbal injections, and traditional Chinese patent medicines with antitumor effects during the intervention will be prohibited.
If unexpected adverse events occur, participants should no longer follow the study guidelines for such events. The investigator should comprehensively analyze whether these events are related to the experimental and control drugs used, and should decide whether to discontinue the clinical trial based on the participant’s condition. Patients who discontinue trials owing to serious adverse events should be followed up, and their outcomes should be documented. In addition, participants who could not adhere to the treatment and those who requested active withdrawal, had poor compliance, were pregnant, dead, or lost to follow-up met the criteria for discontinuation.
This was a randomized controlled trial. The primary outcome was the 2-year disease-free survival (DFS) rate of patients with GC after surgery. It was estimated that the DFS rate 2 years after surgery in the control group was 43.9%, whereas the DFS rate in the intervention group was 63.9%. For α = 0.05 (bilateral), β = 0.2. Assuming that the enrollment rate of the study patients remained unchanged, the proportion of the intervention group to the control group was 1:1. The sample size for N1 was 96 cases in the intervention group, and for N2 was 96 cases in the control group, as calculated using the PASS 11 software. However, a detachment rate of 10% must be considered in the research process. Therefore, the intervention and control groups comprised 106 patients each (212 patients total).
The 2-year DFS rate as the primary outcome and DFS, OS, 1- to 3-year cumulative recurrence and metastasis rate, and 1- to 3-year cumulative survival rate as the secondary outcome will be calculated at the end of follow-up. The lymphocyte count-to-monocyte count ratio (LMR) (59), lymphocyte count-to-neutrophil count ratio (LNR) (60), prognostic nutritional index (PNI) (61), Quality of Life Questionnaire of Stomach 22 (QLQ-STO22) (62), M. D. Anderson Symptom Assessment Scale Gastrointestinal Tumor Specific Module (MDASI-GI) (63), Postgastrectomy Syndrome Assessment Scale-45 (PGSAS-45) (64) (diagnosis of the syndrome should refer to the 2014 Guidelines of Diagnosis and Therapy in Oncology with Traditional Chinese Medicine), and other secondary outcome indicators will be collected at weeks 0–6, whereas the total fat area (TFA) (65), visceral fat area (VFA) (66), subcutaneous fat area (SFA) (67), visceral adiposity index (VAI) (68), and tumor markers will be collected at weeks 0, 3, and 6. All measurement results will be recorded in the case report form (CRF). The details of outcome measurement projects are shown in Table 1.
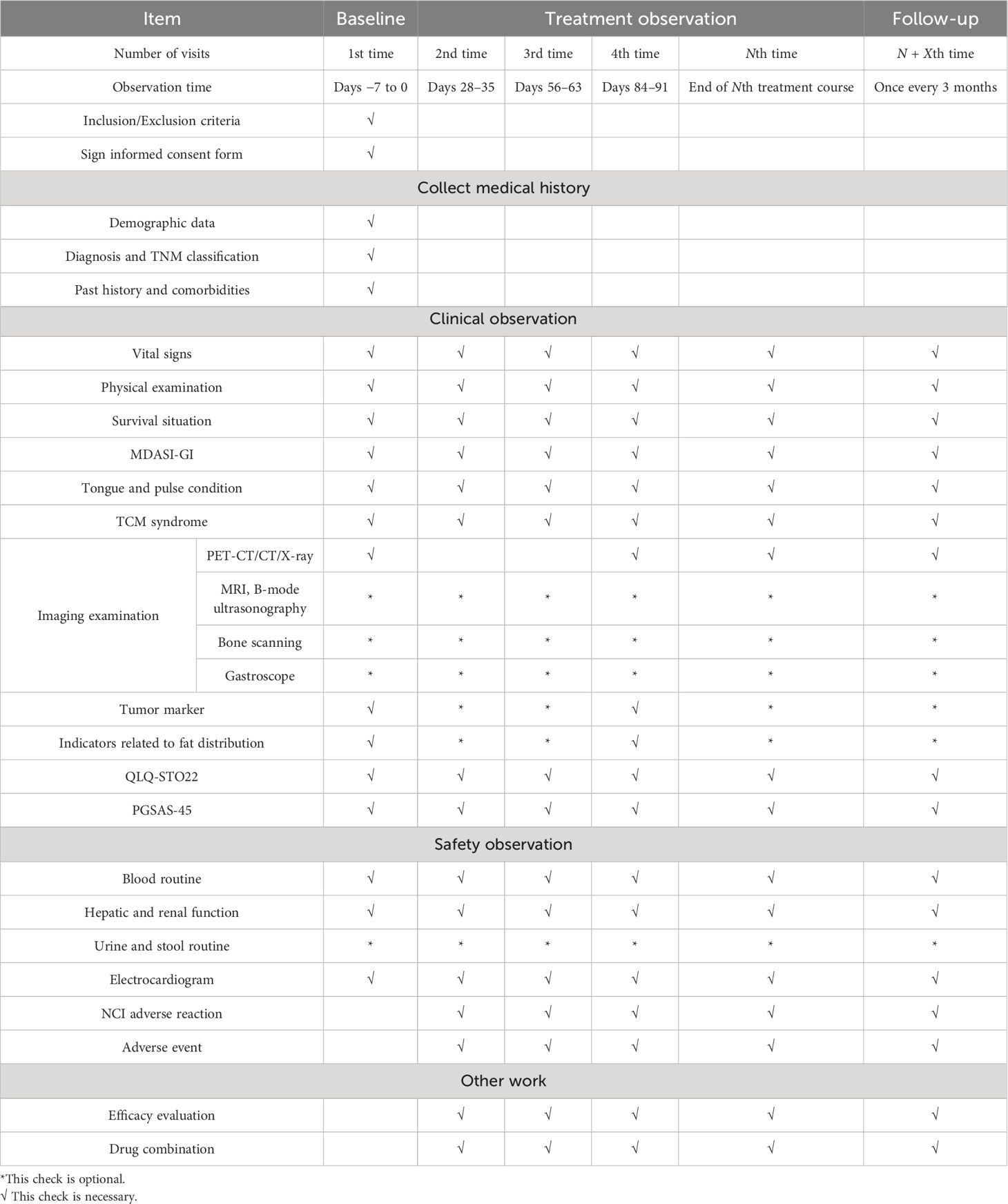
Table 1 Treatment stage flowchart.
The primary outcome of this study is the 2-year DFS rate after surgery, which refers to the proportion of patients who have not experienced recurrence, metastasis, or (for any reason) death within 2 years after surgery.
1. Prognosis related indicators
DFS: Time from randomization to the onset of tumor progression or (for any reason) death in patients.
OS: Time from randomization to death from any cause.
Annual cumulative recurrence and metastasis rate for 1–3 years: The proportion of patients who experience recurrence and metastasis within 1–3 years from the day of surgery to the total number of patients.
Annual cumulative survival rate for 1–3 years: The proportion of patients with a survival period of 1–3 years or more from the day of surgery to the total number of patients.
2. Fat distribution-related indicators
TFA of the abdomen: A CT plain scan will be used to measure the fat area on cross-sectional images, directly reflecting the accumulation of abdominal fat in the human body. It is generally believed that the umbilical plane or L2/L3 gap can better reflect the body’s abdominal fat.
VFA: A commonly used indicator in clinical practice to evaluate the level of visceral fat. The precise measurement method is usually based on imaging methods, specifically the area occupied by adipose tissue in a certain section of abdominal CT (flat umbilical section or third lumbar section).
SFA: SFA = TFA − VFA.
VAI: This is another indicator for evaluating visceral adipose tissue accumulation and dysfunction, and is a new visceral fat assessment index calculated based on waist circumference (WC), body mass index (BMI), triglycerides (TG), and high-density lipoprotein (HDL).
Male VAI = [WC/(39.68 + 1.88 × BMI)] × (TG/1.03) × (1.31/HDL);
Female VAI = [WC/(36.58 + 1.89 × BMI)] × (TG/0.81) × (1.52/HDL).
3. Tumor markers: Carcinoembryonic antigen (CEA), carbohydrate antigen 724 (CA724), and carbohydrate antigen 199 (CA199) should be included as tumor markers.
4. Peripheral blood inflammatory indicators:
LMR: Ratio of lymphocyte count to monocyte count
LNR: Ratio of lymphocyte count to neutrophil count
5. Prognostic nutritional index (PNI): Record serum albumin (ALB) and lymphocyte (TLC) counts, with the formula PNI = ALB + 5 × TLC.
6. Symptoms and quality of life evaluation:
The QLQ-STO22 developed by the European Organization for Research and Treatment of Cancer will be used to evaluate the impact of treatment protocols on the quality of life of GC patients.
The impact of treatment regimens on patient symptoms will be evaluated using the MDASI-GI.
The quality of life with GC patients after gastrectomy will be measured using the PGSAS-45, and the intensity of various symptoms of post-gastrectomy syndrome will be understood.
7. Medication compliance: The number and percentage of cases will be calculated based on <80%, 80%–120%, and >120% medication compliance.
Medication compliance = actual dosage/expected dosage × 100% (rounded to two decimal places).
8. Adverse reaction rate: The proportion of adverse reactions caused by drugs in the enrolled population.
Safety evaluations were performed according to the National Cancer Institute’s Common Terminology Standard for Adverse Events (CTCAE v.5.0), and patient adverse events were monitored every 3 months from baseline to disease progression, death, or 2 years after surgery. The evaluation methods included routine blood tests, urine tests, biochemical tests, and electrocardiography.
Patients will undergo periodic follow-up (once a month during the treatment period and once every 3 months during the follow-up period, including electronic questionnaires or telephone follow-up). After surgery, they will be observed for at least 3 years. Data on vital signs, physical examination, weight, height, body surface area, BMI, ECOG score, KPS score, QLQ-STO22, MDASI-GI, PGSAS-45, peripheral blood inflammatory indicators, blood and urine routine, complete biochemical tests, electrocardiogram, and blood tumor markers will be collected for each treatment cycle and during follow-up visits every 3 months. For participants who did not experience disease progression after completing six courses of treatment, imaging follow-up was conducted every 3 months for 2 years post-surgery and then every 6 months after that until disease recurrence or initiation of alternative therapies. The basic information of the patients and the relevant information required for the study will be recorded in the CRF. Only authorized researchers, representatives of research-undertaking units, ethics committees, and higher-level management departments can access patient records upon reasonable request. No public reports of the results of this study disclose the patient’s name or identity. The research team will protect the privacy of the patient’s medical data as much as possible within the scope permitted by law.
This study will introduce and promote an ISO quality management system. Personnel at all levels will receive the necessary training in management and quality awareness. A quality control system will be established during project implementation, and relevant quality control measures and evaluation plans will be formulated. The project lead unit will assign special personnel to conduct quality control and supervision of this study, including clinical data collection standards and data verification quality control measures. In addition, the project involves task verification and quality control of participating units to ensure completion. A quality-verification document was created and stored for archival purposes. In addition, Guang’anmen Hospital of the China Academy of Chinese Medical Sciences selected a third party to establish the clinical database of the participants and conducted a statistical analysis of the data.
SAS 9.4 statistical software will be used, and full analysis set (FAS) and protocol compliance set (PPS) analyses will be performed on the efficacy indicators. A safety dataset analysis should be conducted for adverse reactions. All statistical tests will be conducted bilaterally, and statistical significance will be set at p ≤ 0.05. We will analyze whether there are outliers in the data and conduct a professional analysis of outliers to decide whether to accept or reject them. After this, we will analyze the data for missing values and conduct a professional analysis to determine whether the missing values are listed as missing or data transferred. The proportion of shedding cases should not exceed 10%; otherwise, analysis and explanation should be provided. The measurement data were described as mean, standard deviation, median, minimum, and maximum whereas counting data were described as frequency, percentage, etc. Quantitative data analysis will be performed using t-tests, rank-sum tests, etc. Counting data analysis will be performed using chi-square tests, ridit analyses, etc. Survival data analysis will be performed using the Kaplan–Meier method, Wilcoxon rank sum test, or log-rank test. A Cox-proportional risk regression model was used for multivariate survival analysis.
Gastric cancer is an important component of the global cancer burden, and local recurrence or distant metastasis after radical gastrectomy is the primary cause of poor prognosis (26). The guidelines recommend no standard treatment after postoperative adjuvant treatment for GC; watchful waiting is recommended. However, most patients with GC experience recurrence and metastasis within 2–3 years after surgery. Therefore, exploring the efficacy of complementary and alternative medicines during surveillance and watchful waiting periods is necessary to promote adjustment of postoperative monitoring and management programs. Several studies have shown that TCM plays a significant role in preventing and treating GC. TCMs stabilize tumors, reduce recurrence and metastasis rates, alleviate clinical symptoms, improve patient survival and quality of life, and decrease the occurrence of adverse reactions (69, 70). However, the quality of most clinical research on TCM treatment of GC is low. These studies provide a low level of evidence, making it challenging to effectively promote and guide clinical practice. Moreover, no large-sample study has explored the correlation between Yang deficiency syndrome and the postoperative recurrence and metastasis of GC. Carrying out well-designed, high-quality clinical research and obtaining robust evidence-based data on TCM treatment for GC are key challenges hindering the widespread adoption of TCM in treating GC. A meta-analysis (71) demonstrated that integrated Chinese and Western medicine treatment could decrease the recurrence rate of GC at 12, 24, and 36 months postoperatively. It was significantly superior to Western medicine treatment alone. Fuzheng Jiedu is an effective treatment for postoperative recurrence and metastasis of GC that is used in the Oncology Department of Guang’anmen Hospital of the China Academy of Chinese Medical Sciences. Studies have shown (52) that the addition of the Fuzheng Jiedu prescription (predecessor of the YWJP) for patients with GC can reduce the recurrence and metastasis rates of GC for 2 years after surgery by 18.60%, which is approximately a 25% reduction compared to patients in the same period. Therefore, TCM has therapeutic advantages in reducing the recurrence and metastasis of GC.
The YWJP has the effects of nourishing Qi and warming Yang, strengthening Zhengqi, and detoxifying, which can improve the “Yang-deficient toxic node” status of postoperative patients with GC. In this study, we aim to clarify the efficacy and safety of YWJP in preventing and treating postoperative recurrence and metastasis of GC. Furthermore, we aim to explore the correlation between Yang deficiency, metabolic abnormalities, gut microbiota, and other factors and their impact on long-term prognosis. Lastly, we seek to identify the mechanisms of postoperative recurrence and metastasis of GC under the guidance of core pathogenesis and possible targets of TCM. The advantages of this study are as follows: (1) it is a high-quality, randomized, double-blind, controlled, multicenter clinical study with a 1:1 random allocation. This design will ensure a better balance between groups and effectively avoid the impact of potentially unknown factors on the test results. Furthermore, simultaneously observing both groups of patients helps to avoid the effect of the trial sequence on the results, thereby enhancing the credibility of the research findings. (2) This research provides a solid clinical foundation for the initial phase. It is centered on the core pathogenesis of the “Yang-deficient toxic node” following surgery for GC. The treatment approach of “supplementing Qi and warming Yang and detoxify” aims to guide personalized treatment strategies aligned with the principles of precision medicine, focused on the effective intervention effect on GC recurrence and metastasis. However, this study has limitations: (1) The experimental design and implementation requirements are demanding. The intervention time is lengthy, the workload is substantial, and the implementation is challenging. (2) The intervention and follow-up periods were lengthy, with a high probability of dropout. (3) Considering the limitations of manpower, economy, and time involved in this clinical study, our follow-up time will be set at 3 years after surgery. However, we will continue to monitor this study to compensate for the restricted follow-up time.
The aims of this study were to evaluate the effectiveness and safety of supplementary and alternative drugs (YWJP) for recurrence and metastasis in patients with GC after surgery and to reveal the influence of Yang deficiency syndrome and gut microbiota on recurrence and metastasis. In addition, based on the core pathogenesis of the Yang-deficient toxic node, exploring the preventive and therapeutic effects and molecular mechanisms of TCM after GC surgery will establish a foundation for developing a new theoretical framework for preventing and treating GC post-surgery. Ultimately, the results of this study will provide a crucial foundation for patients with GC, clinicians, and policymakers to monitor postoperative treatment management and establish a standardized treatment protocol. In the future, we will promote the clinical transformation of YWJP, develop new Chinese medicines, and conduct high-quality, multicenter, randomized controlled studies internationally to enhance the standardized clinical diagnosis and treatment of GC. In addition, with the advancement of spatial tumor ecology (72, 73), it is crucial to investigate the biological implications of the “disease-symptom-syndrome” of GC and the biological foundation of the population that benefits from TCM prevention and treatment.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
This study has been performed in accordance with the Declaration of Helsinki and has been approved by ethics Committee of Guang 'anmen Hospital, China Academy of Chinese Medical Sciences (Ethics Approval Number: 2021-147-KY). Written informed consent was obtained from the individual(s) for the publication of any potentiallyidentifiable images or data included in this article.
LC: Writing – original draft, Writing – review & editing, Data curation, Methodology. GZ: Methodology, Writing – review & editing. XW: Methodology, Supervision, Writing – review & editing. ZK: Methodology, Writing – review & editing. XS: Supervision, Writing – review & editing. XM: Supervision, Writing – review & editing. XZ: Methodology, Writing – review & editing. RG: Supervision, Writing – review & editing. JL: Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Science and Technology Innovation Project of China Academy of Chinese Medical Sciences (No. CI2021A01802), National Postdoctoral Research Program (No. GZC20233128), Beijing Major Difficult Diseases Collaborative Research Project of Chinese and Western Medicine (2023BJSZDYNJBXTGG-013), High Level Chinese Medical Hospital Promotion Project (HLCMHPP2023085, HLCMHPP2023001, HLCMHPP2023097).
We would like to thank Editage (www.editage.cn) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
2. Zeng Y, Jin RU. Molecular pathogenesis, targeted therapies, and future perspectives for gastric cancer. Semin Cancer Biol. (2022) 86:566–82. doi: 10.1016/j.semcancer.2021.12.004
3. Han B, Zheng R, Zeng H, Wang S, Sun K, Chen R, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Center. (2024) 4(1):47–53. doi: 10.1016/j.jncc.2024.01.006
5. Wang Z, Han W, Xue F, Zhao Y, Wu P, Chen Y, et al. Nationwide gastric cancer prevention in China, 2021-2035: a decision analysis on effect, affordability and cost-effectiveness optimisation. Gut. (2022) 71:2391–400. doi: 10.1136/gutjnl-2021-325948
6. Morgan E, Arnold M, Camargo MC, Gini A, Kunzmann AT, Matsuda T, et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020-40: A population-based modelling study. EClinicalMedicine. (2022) 47:101404. doi: 10.1016/j.eclinm.2022.101404
7. Gonzalez CA, Megraud F, Buissonniere A, Lujan Barroso L, Agudo A, Duell EJ, et al. Helicobacter pylori infection assessed by ELISA and by immunoblot and noncardia gastric cancer risk in a prospective study: the Eurgast-EPIC project. Ann Oncol. (2012) 23:1320–4. doi: 10.1093/annonc/mdr384
8. Sadjadi A, Derakhshan MH, Yazdanbod A, Boreiri M, Parsaeian M, Babaei M, et al. Neglected role of hookah and opium in gastric carcinogenesis: a cohort study on risk factors and attributable fractions. Int J cancer. (2014) 134:181–8. doi: 10.1002/ijc.28344
9. Steevens J, Schouten LJ, Goldbohm RA, van den Brandt PA. Alcohol consumption, cigarette smoking and risk of subtypes of oesophageal and gastric cancer: a prospective cohort study. Gut. (2010) 59:39–48. doi: 10.1136/gut.2009.191080
10. Na HK, Lee JY. Molecular basis of alcohol-related gastric and colon cancer. Int J Mol Sci. (2017) 18(6):1116. doi: 10.3390/ijms18061116
11. Tramacere I, Negri E, Pelucchi C, Bagnardi V, Rota M, Scotti L, et al. A meta-analysis on alcohol drinking and gastric cancer risk. Ann Oncol. (2012) 23:28–36. doi: 10.1093/annonc/mdr135
12. Moy KA, Fan Y, Wang R, Gao YT, Yu MC, Yuan JM. Alcohol and tobacco use in relation to gastric cancer: a prospective study of men in Shanghai, China. Cancer Epidemiol Biomarkers Prev. (2010) 19:2287–97. doi: 10.1158/1055-9965.EPI-10-0362
13. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. (2010) 127:2893–917. doi: 10.1002/ijc.25516
14. Jang J, Lee S, Ko KP, Abe SK, Rahman MS, Saito E, et al. Association between body mass index and risk of gastric cancer by anatomic and histologic subtypes in over 500,000 east and Southeast Asian cohort participants. Cancer epidemiology Biomarkers Prev. (2022) 31:1727–34. doi: 10.1158/1055-9965.EPI-22-0051
15. Yang P, Zhou Y, Chen B, Wan HW, Jia GQ, Bai HL, et al. Overweight, obesity and gastric cancer risk: results from a meta-analysis of cohort studies. Eur J Cancer (Oxford England: 1990). (2009) 45:2867–73. doi: 10.1016/j.ejca.2009.04.019
16. Dabo B, Pelucchi C, Rota M, Jain H, Bertuccio P, Bonzi R, et al. The association between diabetes and gastric cancer: results from the Stomach Cancer Pooling Project Consortium. Eur J Cancer Prev. (2022) 31:260–9. doi: 10.1097/CEJ.0000000000000703
17. Dai D, Yang Y, Yu J, Dang T, Qin W, Teng L, et al. Interactions between gastric microbiota and metabolites in gastric cancer. Cell Death disease. (2021) 12:1104. doi: 10.1038/s41419-021-04396-y
18. Song P, Wu L, Guan W. Dietary nitrates, nitrites, and nitrosamines intake and the risk of gastric cancer: A meta-analysis. Nutrients. (2015) 7:9872–95. doi: 10.3390/nu7125505
19. Tricker AR, Preussmann R. Carcinogenic N-nitrosamines in the diet: occurrence, formation, mechanisms and carcinogenic potential. Mutat Res. (1991) 259:277–89. doi: 10.1016/0165-1218(91)90123-4
20. Zhao Z, Yin Z, Zhao Q. Red and processed meat consumption and gastric cancer risk: a systematic review and meta-analysis. Oncotarget. (2017) 8:30563–75. doi: 10.18632/oncotarget.v8i18
21. Harrison LE, Zhang ZF, Karpeh MS, Sun M, Kurtz RC. The role of dietary factors in the intestinal and diffuse histologic subtypes of gastric adenocarcinoma: a case-control study in the U.S. Cancer. (1997) 80:1021–8. doi: 10.1002/(ISSN)1097-0142
22. Gonzalez CA, Agudo A. Carcinogenesis, prevention and early detection of gastric cancer: where we are and where we should go. Int J cancer. (2012) 130:745–53. doi: 10.1002/ijc.26430
23. Choi IJ, Kim CG, Lee JY, Kim YI, Kook MC, Park B, et al. Family history of gastric cancer and helicobacter pylori treatment. New Engl J Med. (2020) 382:427–36. doi: 10.1056/NEJMoa1909666
24. Camargo MC, Murphy G, Koriyama C, Pfeiffer RM, Kim WH, Herrera-Goepfert R, et al. Determinants of Epstein-Barr virus-positive gastric cancer: an international pooled analysis. Br J Cancer. (2011) 105:38–43. doi: 10.1038/bjc.2011.215
25. Murphy G, Dawsey SM, Engels EA, Ricker W, Parsons R, Etemadi A, et al. Cancer risk after pernicious anemia in the US elderly population. Clin Gastroenterol Hepatol. (2015) 13:2282–9.e1-4. doi: 10.1016/j.cgh.2015.05.040
26. Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. (2020) 396:635–48. doi: 10.1016/S0140-6736(20)31288-5
27. Bornschein J, Rugge M. Bright future for endoscopy: the new frontier of gastric cancer secondary prevention. Gut. (2020) 69:1723–4. doi: 10.1136/gutjnl-2020-321570
28. Noh SH, Park SR, Yang HK, Chung HC, Chung IJ, Kim SW, et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. (2014) 15:1389–96. doi: 10.1016/S1470-2045(14)70473-5
29. Al-Batran SE, Hartmann JT, Probst S, Schmalenberg H, Hollerbach S, Hofheinz R, et al. Phase III trial in metastatic gastroesophageal adenocarcinoma with fluorouracil, leucovorin plus either oxaliplatin or cisplatin: a study of the Arbeitsgemeinschaft Internistische Onkologie. J Clin Oncol. (2008) 26:1435–42. doi: 10.1200/JCO.2007.13.9378
30. Lee JH, Kim HI, Kim MG, Ha TK, Jung MS, Kwon SJ. Recurrence of gastric cancer in patients who are disease-free for more than 5 years after primary resection. Surgery. (2016) 159:1090–8. doi: 10.1016/j.surg.2015.11.002
31. Cao L, Selby LV, Hu X, Zhang Y, Janjigian YY, Tang L, et al. Risk factors for recurrence in T1-2N0 gastric cancer in the United States and China. J Surg Oncol. (2016) 113:745–9. doi: 10.1002/jso.24228
32. Jin LX, Moses LE, Squires MH 3rd, Poultsides GA, Votanopoulos K, Weber SM, et al. Factors associated with recurrence and survival in lymph node-negative gastric adenocarcinoma: A 7-institution study of the US gastric cancer collaborative. Ann surg. (2015) 262:999–1005. doi: 10.1097/SLA.0000000000001084
33. Baiocchi GL, Marrelli D, Verlato G, Morgagni P, Giacopuzzi S, Coniglio A, et al. Follow-up after gastrectomy for cancer: an appraisal of the Italian research group for gastric cancer. Ann Surg Oncol. (2014) 21:2005–11. doi: 10.1245/s10434-014-3534-8
34. Fields RC, Strong VE, Gonen M, Goodman KA, Rizk NP, Kelsen DP, et al. Recurrence and survival after pathologic complete response to preoperative therapy followed by surgery for gastric or gastrooesophageal adenocarcinoma. Br J cancer. (2011) 104:1840–7. doi: 10.1038/bjc.2011.175
35. Youn HG, An JY, Choi MG, Noh JH, Sohn TS, Kim S. Recurrence after curative resection of early gastric cancer. Ann Surg Oncol. (2010) 17:448–54. doi: 10.1245/s10434-009-0772-2
36. Yoo CH, Noh SH, Shin DW, Choi SH, Min JS. Recurrence following curative resection for gastric carcinoma. Br J surg. (2000) 87:236–42. doi: 10.1046/j.1365-2168.2000.01360.x
37. D'Angelica M, Gonen M, Brennan MF, Turnbull AD, Bains M, Karpeh MS. Patterns of initial recurrence in completely resected gastric adenocarcinoma. Ann surg. (2004) 240:808–16. doi: 10.1097/01.sla.0000143245.28656.15
38. Song J, Lee HJ, Cho GS, Han SU, Kim MC, Ryu SW, et al. Recurrence following laparoscopy-assisted gastrectomy for gastric cancer: a multicenter retrospective analysis of 1,417 patients. Ann Surg Oncol. (2010) 17:1777–86. doi: 10.1245/s10434-010-0932-4
39. Honda M, Hiki N, Kinoshita T, Yabusaki H, Abe T, Nunobe S, et al. Long-term outcomes of laparoscopic versus open surgery for clinical stage I gastric cancer: the LOC-1 study. Ann surg. (2016) 264:214–22. doi: 10.1097/SLA.0000000000001654
40. Park SH, Lim DH, Sohn TS, Lee J, Zang DY, Kim ST, et al. A randomized phase III trial comparing adjuvant single-agent S1, S-1 with oxaliplatin, and postoperative chemoradiation with S-1 and oxaliplatin in patients with node-positive gastric cancer after D2 resection: the ARTIST 2 trial(☆). Ann Oncol. (2021) 32:368–74. doi: 10.1016/j.annonc.2020.11.017
41. Yan X. Investigation of the timing, patterns and prognostic factors of recurrence after curative radical resection for gastric cancer. Nanjing Med Univ. (2018) 13–23. doi: 10.27249/d.cnki.gnjyu.2018.000325
42. Turanli S, Atalay C, Berberoglu U, Gulben K. Adjuvant chemoradiation versus chemotherapy for stage III gastric cancer after surgery with curative intent. J Cancer Res Ther. (2015) 11:369–74. doi: 10.4103/0973-1482.160050
43. Cao LC. Investigation of bias constitution and related factors in patients with recurrence and metastasis of gastric cancer and study on the intervention effect of Fuzheng Jiedu prescription. Beijing: China Academy of Chinese Medical Sciences (2022). doi: 10.27658/d.cnki.gzzyy.2022.000196
44. Zeng H, Liu Z, Wang Z, Zhou Q, Qi Y, Chen Y, et al. Intratumoral IL22-producing cells define immunoevasive subtype muscle-invasive bladder cancer with poor prognosis and superior nivolumab responses. Int J Cancer. (2020) 146:542–52. doi: 10.1002/ijc.32715
45. Wang JH. Study on fecal metabolomics of Yang deficiency and its correlation with intestinal flora structure. Beijing: Beijing University of Chinese Medicine (2017).
46. Yun MR, Seo JM, Park HY. Visfatin contributes to the differentiation of monocytes into macrophages through the differential regulation of inflammatory cytokines in THP-1 cells. Cell Signal. (2014) 26:705–15. doi: 10.1016/j.cellsig.2013.12.010
47. Koundouros N, Poulogiannis G. Reprogramming of fatty acid metabolism in cancer. Br J Cancer. (2020) 122:4–22. doi: 10.1038/s41416-019-0650-z
48. Bergers G, Fendt SM. The metabolism of cancer cells during metastasis. Nat Rev Cancer. (2021) 21:162–80. doi: 10.1038/s41568-020-00320-2
49. Xie R, Xia Y, Chen Y, Li H, Shang H, Kuang X, et al. The RIGHT extension statement for traditional Chinese medicine: development, recommendations, and explanation. Pharmacol Res. (2020) 160:105178. doi: 10.1016/j.phrs.2020.105178
50. Liu Q, Tang J, Chen S, Hu S, Shen C, Xiang J, et al. Berberine for gastric cancer prevention and treatment: Multi-step actions on the Correa's cascade underlie its therapeutic effects. Pharmacol Res. (2022) 184:106440. doi: 10.1016/j.phrs.2022.106440
51. Hung KF, Hsu CP, Chiang JH, Lin HJ, Kuo YT, Sun MF, et al. Complementary Chinese herbal medicine therapy improves survival of patients with gastric cancer in Taiwan: A nationwide retrospective matched-cohort study. J ethnopharmacol. (2017) 199:168–74. doi: 10.1016/j.jep.2017.02.004
52. Zhang Y. Study on the correlation between traditional Chinese medicine constitution and postoperative recurrence and metastasis of gastric cancer and quality of life. Beijing: Beijing University of Chinese Medicine (2019).
53. Cao LC, Wang XM, Zhu GH, Xu BW, Li J. Based on "Yang deficiency and toxin knot" to explore the intervention of five methods of treating yang in gastrointestinal tumors. J Basic Chin Med. (2022) 28:1359–62. doi: 10.19945/j.cnki.issn.1006-3250.2022.08.002
54. Yan A. Study on the intervention of Fuzheng Jiedu prescription on recurrence and metastasis of gastric cancer patients after operation and quality of life. Beijing: Beijing University of Chinese Medicine (2018).
55. Tan Y. Correlation analysis of Yang deficiency and biological index after gastric cancer operation and intervention study of Yiqingyang Jiedu prescription. Beijing: China Academy of Chinese Medical Sciences (2023). doi: 10.27658/d.cnki.gzzyy.2023.000277
56. Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gotzsche PC, Krleza-Jeric K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Internal Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
57. Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Ann Internal Med. (2010) 152:726–32. doi: 10.7326/0003-4819-152-11-201006010-00232
58. Amin MB, Edge SB, Greene FL, Brierley JD. AJC. AJCC cancer staging manual[M]. 8th ed. New York: Springer (2017).
59. Ma JY, Liu Q. Clinicopathological and prognostic significance of lymphocyte to monocyte ratio in patients with gastric cancer: A meta-analysis. Int J Surg. (2018) 50:67–71. doi: 10.1016/j.ijsu.2018.01.002
60. Peng CW, Wang LW, Fang M, Yang GF, Li Y, Pang DW. Combined features based on MT1-MMP expression, CD11b + immunocytes density and LNR predict clinical outcomes of gastric cancer. J Trans Med. (2013) 11:153. doi: 10.1186/1479-5876-11-153
61. Nogueiro J, Santos-Sousa H, Pereira A, Devezas V, Fernandes C, Sousa F, et al. The impact of the prognostic nutritional index (PNI) in gastric cancer. Langenbecks Arch Surg. (2022) 407:2703–14. doi: 10.1007/s00423-022-02627-0
62. Rausei S, Mangano A, Galli F, Rovera F, Boni L, Dionigi G, et al. Quality of life after gastrectomy for cancer evaluated via the EORTC QLQ-C30 and QLQ-STO22 questionnaires: surgical considerations from the analysis of 103 patients. Int J Surg. (2013) 11 Suppl 1:S104–9. doi: 10.1016/S1743-9191(13)60028-X
63. Wang XS, Williams LA, Eng C, Mendoza TR, Shah NA, Kirkendoll KJ, et al. Validation and application of a module of the M. D. Anderson Symptom Inventory for measuring multiple symptoms in patients with gastrointestinal cancer (the MDASI-GI). Cancer. (2010) 116:2053–63. doi: 10.1002/cncr.24920
64. Misawa K, Terashima M, Uenosono Y, Ota S, Hata H, Noro H, et al. Evaluation of postgastrectomy symptoms after distal gastrectomy with Billroth-I reconstruction using the Postgastrectomy Syndrome Assessment Scale-45 (PGSAS-45). Gastric Cancer. (2015) 18:675–81. doi: 10.1007/s10120-014-0407-6
65. Kurtenkov O, Klaamas K, Miljukhina L. The lower level of natural anti-Thomsen-Friedenreich antigen (TFA) agglutinins in sera of patients with gastric cancer related to ABO(H) blood-group phenotype. Int J cancer. (1995) 60:781–5. doi: 10.1002/ijc.2910600609
66. Chen X, Chen W, Huang Y, Xu J, Zeng Y, Shi M, et al. A quantified risk-scoring system including the visceral fat area for peritoneal metastasis of gastric cancer. Cancer Manage Res. (2019) 11:2903–13. doi: 10.2147/CMAR
67. Han S, Wang Z, Liu J, Wang HD, Yuan Q. miR-29a-3p-dependent COL3A1 and COL5A1 expression reduction assists sulforaphane to inhibit gastric cancer progression. Biochem Pharmacol. (2021) 188:114539. doi: 10.1016/j.bcp.2021.114539
68. Matsui R, Inaki N, Tsuji T, Kokura Y, Momosaki R. Preoperative high visceral fat increases severe complications but improves long-term prognosis after gastrectomy for patients with advanced gastric cancer: a propensity score matching analysis. Nutrients. (2022) 14(20):4236. doi: 10.3390/nu14204236
69. Xu B, Wang X, Wang H, Cao L, Ge Y, Yuan B, et al. Efficacy and safety of herbal formulas with the function of gut microbiota regulation for gastric and colorectal cancer: A systematic review and meta-analysis. Front Cell Infect Microbiol. (2022) 12:875225. doi: 10.3389/fcimb.2022.875225
70. Yang M, Zhu SJ, Shen C, Zhai R, Li DD, Fang M, et al. Clinical application of Chinese herbal injection for cancer care: evidence-mapping of the systematic reviews, meta-analyses, and randomized controlled trials. Front Pharmacol. (2021) 12:666368. doi: 10.3389/fphar.2021.666368
71. Wen YH, Lang J, Deng X, Zhou XX. Meta-analysis of traditional Chinese medicine combined with chemotherapy in preventing postoperative recurrence of gastric cancer. Hunan J Traditional Chin Med. (2016) 32:145–7. doi: 10.16808/j.cnki.issn1003-7705.2016.09.073
72. Sammut SJ, Crispin-Ortuzar M, Chin SF, Provenzano E, Bardwell HA, Ma W, et al. Multi-omic machine learning predictor of breast cancer therapy response. Nature. (2022) 601:623–9. doi: 10.1038/s41586-021-04278-5
Keywords: randomized controlled trial, recurrence, metastasis, traditional Chinese medicine, gastric cancer
Citation: Cao L, Zhu G, Wang X, Kuang Z, Song X, Ma X, Zhu X, Gao R and Li J (2024) Yiqi Wenyang Jiedu prescription for preventing and treating postoperative recurrence and metastasis of gastric cancer: a randomized controlled trial protocol. Front. Oncol. 14:1326970. doi: 10.3389/fonc.2024.1326970
Received: 24 October 2023; Accepted: 17 June 2024;
Published: 05 July 2024.
Edited by:
Zsolt Kovács, George Emil Palade University of Medicine, Pharmacy, Sciences and Technology of Târgu Mureş, RomaniaReviewed by:
Chen Jue, Yangzhou University, ChinaCopyright © 2024 Cao, Zhu, Wang, Kuang, Song, Ma, Zhu, Gao and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie Li, cWZtMjAyMGppZWxpQHllYWgubmV0
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.