
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 21 February 2024
Sec. Cancer Molecular Targets and Therapeutics
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1324859
This article is part of the Research TopicIntegrating Transcriptional Modulation in Systemic Tumor TherapyView all 7 articles
 Yingjun Zhang1,2
Yingjun Zhang1,2 Ge Zhang1,2Yuefang Wang1,2Lei Ye1,2Luyun Peng1,2Rui Shi1,2Siqi Guo1,2Jiajing He1,2Hao Yang1,2Qingkai Dai1,2*
Ge Zhang1,2Yuefang Wang1,2Lei Ye1,2Luyun Peng1,2Rui Shi1,2Siqi Guo1,2Jiajing He1,2Hao Yang1,2Qingkai Dai1,2*Acute lymphocytic leukemia is a hematological malignancy that primarily affects children. Long-term chemotherapy is effective, but always causes different toxic side effects. With the application of a chemotherapy-free treatment strategy, we intend to demonstrate the most recent results of using one type of epigenetic drug, histone deacetylase inhibitors, in ALL and to provide preclinical evidence for further clinical trials. In this review, we found that panobinostat (LBH589) showed positive outcomes as a monotherapy, whereas vorinostat (SAHA) was a better choice for combinatorial use. Preclinical research has identified chidamide as a potential agent for investigation in more clinical trials in the future. In conclusion, histone deacetylase inhibitors play a significant role in the chemotherapy-free landscape in cancer treatment, particularly in acute lymphocytic leukemia.

Graphical Abstract
Leukemia is the leading cause of pediatric malignancies, with acute lymphocytic leukemia (ALL) accounting for over 70% of cases. ALL is a rapidly invasive disease that originates from B- or T-lymphocyte progenitors. Accumulation of blast lymphocytes and suppression of normal cells are the main characteristics of the disease course. ALL predominantly affects children, with an incidence of 3–4/100,000 in patients under 14 years of age. The five-year survival rate is approximately 90% in children and 65% in adults (1). Long-term chemotherapy is the standard treatment for ALL. Common regimens include vincristine, dexamethasone, prednisone, and doxorubicin, as recommended by the American Cancer Society. However, almost all chemotherapeutic drugs cause side effects that are significant factors in clinical trials and basic research. In the last decades, other anti-cancer agents like targeted therapy and immunotherapy play a crucial role in hematological diseases. Epigenetic drugs and its various biology functions are leading topics in the treatment strategies.
Histone deacetylase inhibitors (HDACi) are epigenetic drugs that target the regulation of histone modifications. Histone acetylation and deacetylation are essential processes that regulate the chromosomal integrity. These processes are controlled by two enzymes: histone acetyltransferases (HATs) and histone deacetylases (HDACs), respectively. Acetylation can cause a loose state by neutralizing the positive charge on the surface of histones, whereas deacetylation has the opposite effect. An imbalance in this process can mediate gene expression, thereby contributing to the occurrence of diseases, where HDACi inhibit histone deacetylation and reverse the aberrant expression of specific genes (2). (Figure 1) Further, acetylation or acetylation on non-histone proteins has been highlighted as well in recent years, which play a role in controlling not just cancer- related transcriptional factors, but also tumor suppressor genes and oncogenes. For instance, HDAC1 directly causes deacetylation of p53 while HDAC2 regulates p53 expression via deacetylating the C-terminal lysine on p53. HDAC6 can also bind to the C-terminal region of p53 and deacetylates it (3, 4). Similarly, STAT3-phosphorylation was prevented by inhibiting the function of HDAC3 (5). HDAC6 regulates STAT3 in the same way was also proved in 2014, indicating it can be served as a novel molecular target and also a prognostic marker in B-cell lymphoma (6). In previous research targeting the aberrantly expressions of HDAC in hematologic malignancies, expression level of HDAC1-11 were detected in primary ALL patients, in which HDAC1, HDAC2 and HDAC8 were higher expressed in investigated samples and HDAC4 can be used as a therapeutic target (7).Upregulation of HDAC1-3 were found in Hodgkin’s lymphoma, whereas HDAC1-2 and HDAC6 were overexpressed in diffuse large B-cell lymphoma as well (8).
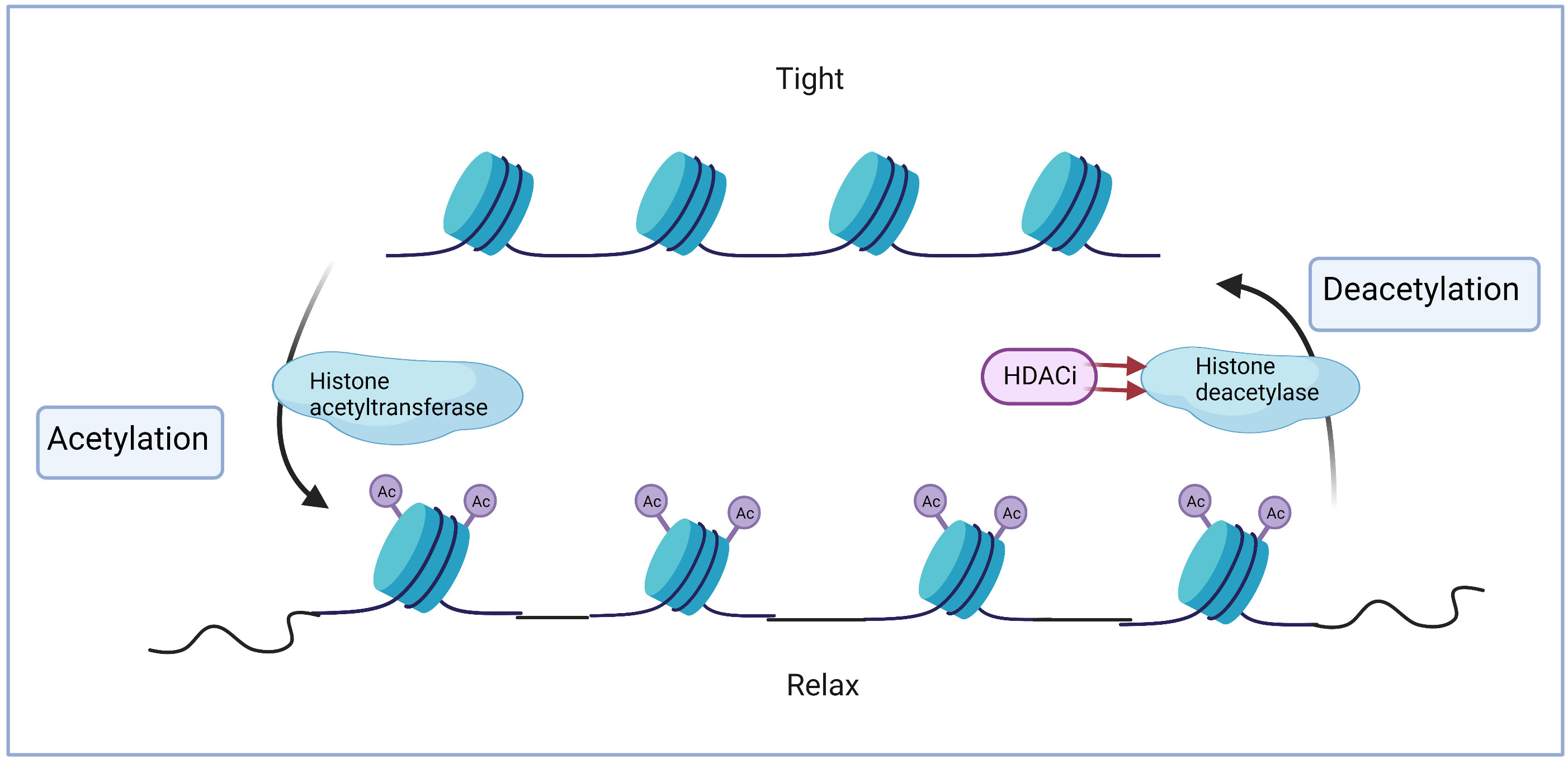
Figure 1 Histone acetylation and deacetylation.
Despite the irreplaceable role of chemotherapeutic drugs in cancer treatment, HDACi have been demonstrated to be effective against many cancer types when used alone or in combination with other drugs (Figure 2) (9–14). Currently there are over twenty HDACi which can be divided into pan-HDACi and specific HDACi based on their target on different classes of HDACs. HDACs was categorized as Class I (HDAC 1, 2, 3, and 8), ClassIIa (HDAC4,5,7 and 9), ClassIIb (HDAC6 and 10), Class IV (HDAC11) and Sirtuins III (SIRT 1, 2, 3, 4, 5, 6 and 7) by Zn2+ dependent and NAD+ dependent for deacetylation activity. The majority of HDACi are pan-HDACi which block more than one class of HDACs, while specific-HDACi only focus one class HDAC (15). Starting from 2006, the first HDACi was approved by Food and Drug Administration (FDA) for cutaneous T-cell lymphoma (CTCL), currently four HDACi have been approved for cancer treatment (Table 1), but none of them can be applied to leukemia.
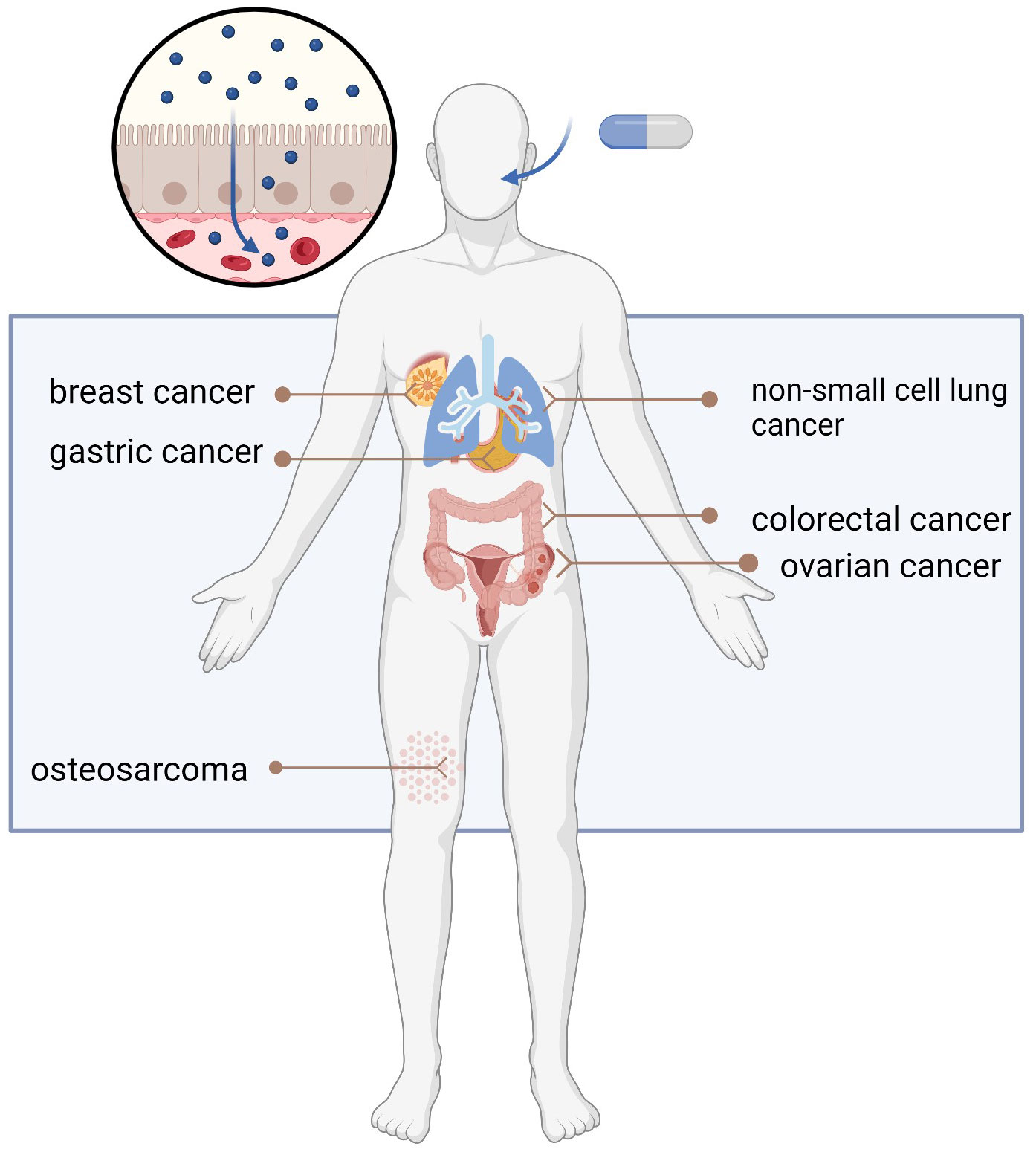
Figure 2 Appliance of HDACi in different cancer types.

Table 1 FDA approved HDACi in cancer treatment.
Given the potential effects of HDACi in the treatment of hematological malignancies and the promising effects observed in acute myeloid leukemia (AML) cases, we aimed to discuss the latest outcomes, starting from ongoing clinical trials to preclinical research on the use of HDACi in ALL, with the goal of identifying further directions for optimizing strategies for ALL treatment.
A comprehensive literature search was conducted via PubMed for suitable studies published until July 31, 2023. The keywords for searches include HDACi, ALL, chemotherapy, synergy effects and targeted therapy.
In 2009, a phase I study conducted by DeAngelo et al. successfully demonstrated the positive effects of the HDACi panobinostat (LBH589) when used in combination with chemotherapy for AML treatment, achieving the overall response rate (ORR) being 60.9% and one year survival rate being 78.3% (16). However, the role of HDACi in ALL remains unclear. Currently, there are approximately ten trials investigating HDACi in ALL that provide basic information on the clinical treatment of ALL (Table 2).
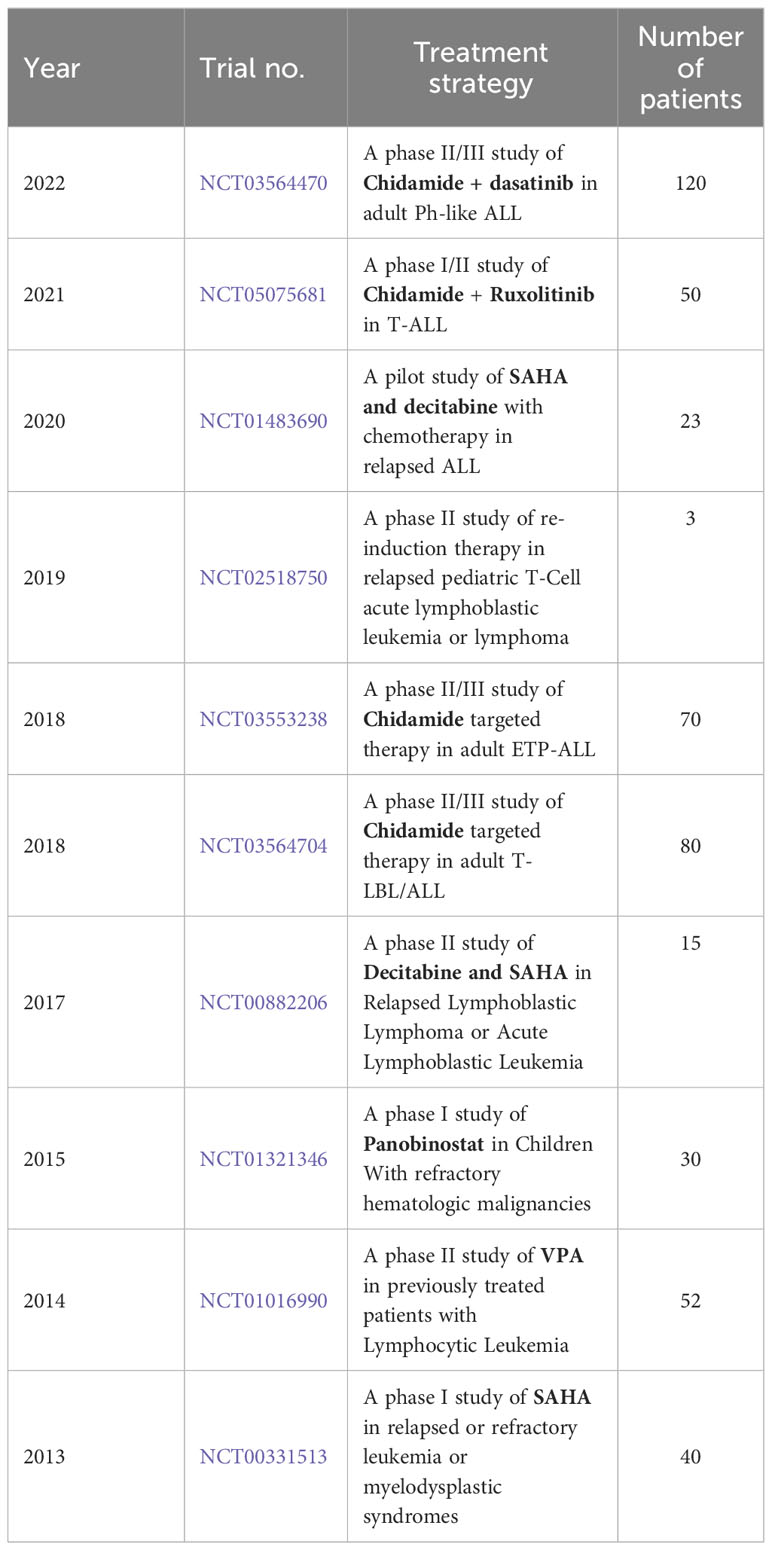
Table 2 Clinical trials of HDACi involved in ALL treatment.
A phase I study focused on LBH589 in children with relapsed and refractory hematological malignancies, including ALL. The results showed that LBH589 was well tolerated in pretreated pediatric leukemia patients, with no cardiac side effects, but the response to LBH589 was modest (17). Notably, a pilot study investigating the combination of SAHA and decitabine with chemotherapy in relapsed ALL was terminated due to toxicity firstly. Further, a subsequent pre-reductive study conducted by the same team demonstrated the effectiveness of this combination strategy by adjusting the doses of drugs. The study achieved an ORR of 46.2% and got the positive correlation between the methylation level and bone marrow response (18, 19).
Moreover, a phase IIb trial investigating chidamide showed significant clinical effects in relapsed or refractory adult T-cell leukemia, the ORR was 51.18% and the median progression free survival (PFS) rate was 152 days when combined with chemotherapy (20). Two phase II/III studies focusing on chidamide showed interest in subgroups such as Philadelphia chromosome (Ph)-like ALL and Early T-cell precursor (ETP)-ALL, the latest results indicate that chidamide is highly effective and well tolerated in these two subtypes, with the complete remission rate of 87% and 77% in ETP-ALL and Ph-like ALL respectively (21). Some other trials are underway currently which need further investigations. Nevertheless, there are encouraging data from preclinical research on several aspects (Table 3).
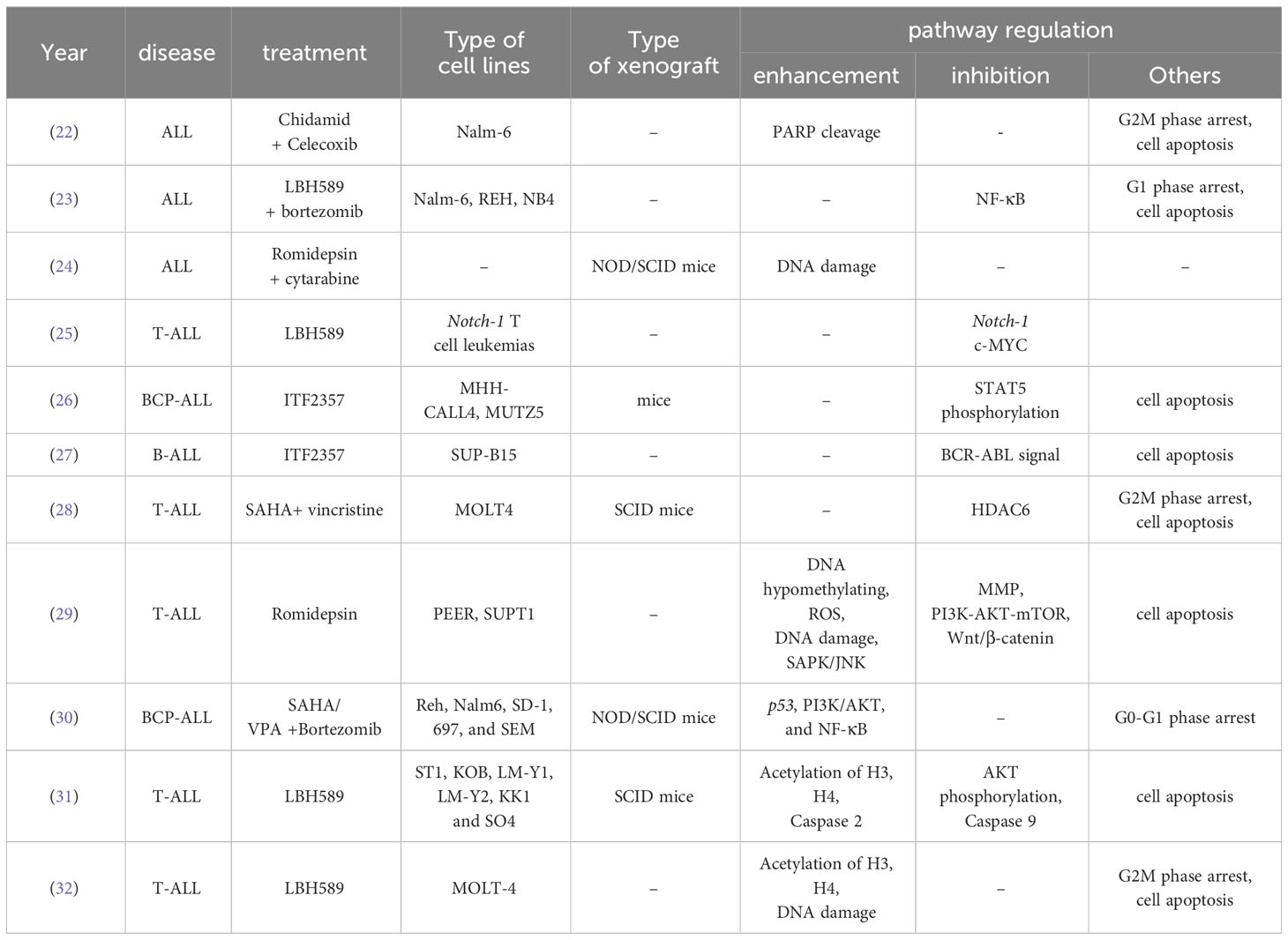
Table 3 Pre-clinical research of HDACi involved in ALL treatment.
LBH589 is a pan-HDAC inhibitor of class I, II and IV HDACs. In the preclinical stage, LBH589 has shown positive effects on ALL both in vitro and in vivo. Gastro et al. demonstrated that LBH589 inhibited cell growth in T-ALL cell lines and effectively reduced tumor size in human ALL xenografts, providing further evidence of the clinical value of combination treatment (33).
Previous studies indicated that oncogene Notch1-driven transcription is the main target of LBH589 in ALL therapy (25). More than 70% of T-ALL cases present Notch1-activating mutations (gain-of-function), which can increase the regulation of cell cycle-related proteins by Notch1 and thereby facilitate the proliferation of leukemia cells (34–36). Exposure to LBH589 in ALL cell lines has been shown to induce cell cycle progression, cell apoptosis, and DNA damage (32). The connection between HDACi and the Notch pathway was analyzed in detail. HDAC3 is recognized as a regulator of Notch1 signaling response, and HDAC6 is another target closely related to the expression levels of Notch3 in T-ALL (37, 38). HDACi including trichostatin A downregulate the NAML3 pathway (39, 40).
Furthermore, LBH589 increased the survival of adult ALL xenograft models with t (4;11). LBH589 alone, as well as the combination of methotrexate (MTX) and 6MP, were investigated, but the combination groups did not show better effects than monotherapy (41). The latest results of genome-wide Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR)/CRISPR-associated (Cas)9 (CRISPR/Cas9) loss-of-function screening in B-ALL cells also indicate that patients with higher SIRT1 expression in cancer cells may benefit more from LBH589 treatment (42). These are all good hints that investigations of LBH589 are positive at the current stage, which can be further applied in clinical trials.
Vorinostat (SAHA) is the first FDA-approved pan-HDACi used for CTCL, targeting class I, II, and IV HDACs. SAHA has shown predominate effects in AML (43), whereas related publications on ALL conclude that SAHA is unsatisfactory as a monotherapy. The latest preclinical research suggests that acetylation of H3 and H4 is related to the drug resistance mechanism in T-ALL, and SAHA can reverse this resistance (44). SAHA also exhibits antileukemia effects in TYK2-rearranged ALL mice models (45). In general, most studies have focused on the synergistic effects of SAHA in combination with chemotherapy, which are discussed in the next section.
Belinostat (PXD101) was approved by FDA in 2014 for the treatment of peripheral T-cell lymphoma (PTCL). Targeting class 1 and 2 HDACs increases the acetylation of H3 and H4 proteins, thereby inhibiting tumor cell growth in various cancer types such as T-cell lymphoma and breast cancer (46, 47). In the field of hematology, previous reports have demonstrated the potential effects of PDX101 on AML earlier (48, 49). The role of PDX101 in ALL has been reported as well. Interestingly, primary childhood ALL samples and several chemo-resistant ALL cell lines are sensitive to PDX101 through the apoptotic pathway, with even better cytotoxic effects than dexamethasone (50).
Romidepsin is another HDACi currently available for CTCL. A case study on the clinical use of romidepsin described that it was useful for an adult patient with T-ALL refractory to hyper-CVAD, providing a valuable indication for further research in hematology (51). Mechanistically, romidepsin is associated with DNA hypermethylation, thereby increasing reactive oxygen species (ROS) and decreasing the mitochondrial membrane. These changes may trigger T cell apoptosis and DNA damage (29). In infants, romidepsin was also found to have strong efficacy in KMT2A-r ALL through the DNA damage pathway, and rearrangement of this gene is a specific characteristic in more than 80% of cases (24). Similar effects can also be seen in LBH589 (33).
Several reports have investigated givinostat (ITF2357) in preclinical stages. Previous studies have shown that ITF2357 reduces the number of blasts in target organs through cell cycle regulation and DNA repair. It has also been found to have an antileukemic effect in xenografts (52). Moreover, ITF2357 is potential to be a treatment strategy for Ph-like ALL patients. These patients typically do not respond well to targeted agents, such as tyrosine kinase inhibitors (TKI) like imatinib, but ITF2357 has been found to induce potent apoptotic effects in Ph-like ALL cell lines (27).
Chidamide is a HDACi that inhibits HDAC1, HDAC2, HDAC3, and HDAC10. It has been approved by the Chinese FDA for PTCL treatment and can be used in adult patients with T-ALL in Japan (53, 54). The role of chidamide in leukemia has been extensively studied in recent years. Chidamide has shown promising effects on IKZF1 deletion in high-risk ALL, both in vitro and in vivo (55). The antitumor effects of chidamide on ALL cells are also correlated with Notch1-MYC gene downregulation and this mechanism gives a support to the reduction of minimal residual disease in ALL patients (56). Recent studies have shown that chidamide can regulate CD8 + cells in T-ALL by increasing the expression of CXCL9, which promotes tumor growth in many cancer types (57–60). Moreover, chidamide promoted CAR-T cell therapy by upregulating CD22 in B-ALL (61). Chidamide demonstrated promising effects and good safety in a preliminary study in children, with an overall survival (OS) of 94.1% and event-free survival rate of 95.2% (62).
Overall, the preclinical research of several HDACi in ALL treatment provides directions for further investigations in specific target like Notch signaling pathway. Correlations between agents show a closed cycle in regulations of cancers. (Figure 3) Moreover, some other HDACi are potential candidates for ALL based on their good effects in treating other hematological diseases (53, 63).
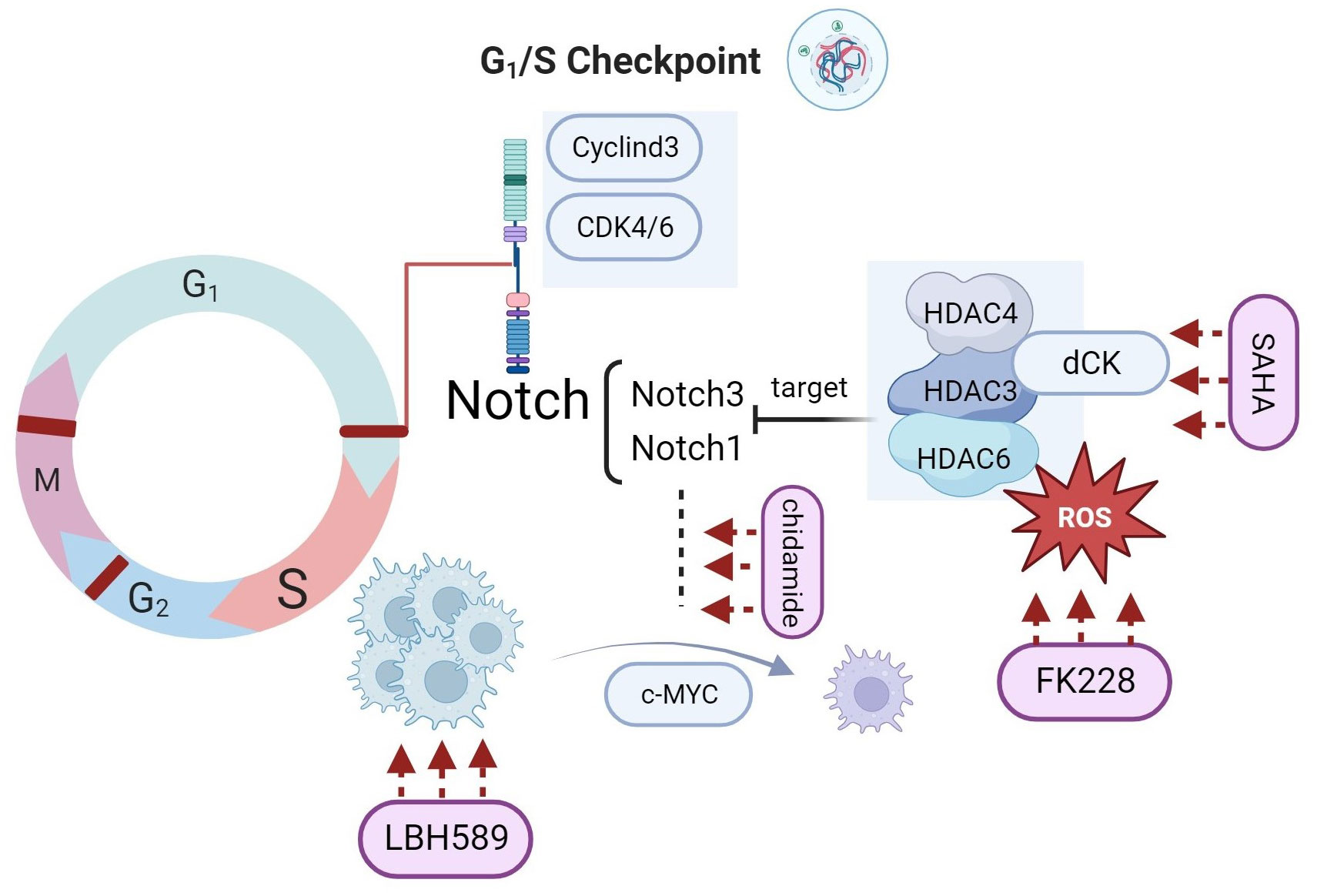
Figure 3 HDACi target the Notch-dependent ALL cells in different pathways.
LBH589 and azacitidine are epigenetic drugs, with LBH589 being an HDACi and azacitidine being a DNA methyltransferase inhibitor (DNMTi). The combination of these two drugs can generate synergistic effects by inducing chemoprotection in several ALL samples (64). This combination has been shown to be more efficient than using cytarabine or other drugs as monotherapy, as it can overcome the protective effects of osteoblasts on ALL cells. However, it is important to note that this specific combination has not yet been investigated in any clinical trials. Furthermore, similar strategies involving SAHA and decitabine have been tested in clinical trials and have shown promising effects in patients with relapsed ALL (18, 19, 65). Low doses of decitabine and SAHA caused cell death in leukemic cells and reduced p21 levels without significant changes in normal peripheral blood lymphocytes (66). Additionally, pretreatment with SAHA and decitabine can enhance the cytotoxicity of chemotherapy in relapsed childhood B-ALL, suggesting that epigenetic mechanisms play a role in the acquisition of chemoresistance during ALL recurrence (67). Connective map analysis, validated by RT-PCR and gene expression arrays, identified SAHA as the most effective agent for reversing the expression of chemoresistance genes (BIRC5, FOXM1, TYMS, FANCD2, NR3C1, HRK, and SMEK2) in ALL relapse. Furthermore, a study reported that the combination of low-dose decitabine and chidamide enhanced apoptosis activation in adult ALL cases, particularly in patients with p16 deletion. This enhancement was achieved by regulating checkpoint kinase 1 phosphorylation and γH2A.X expression (68).
The synergistic effects of HDACi and conventional antileukemic chemotherapy drugs have been reported in several studies, in which LBH589 and SAHA have been widely discussed. In a preclinical study, LBH589 was shown to amplify vincristine's cytotoxicity in B-ALL cells (23). The study also highlighted LBH589’s ability to prolong the cell cycle and suggested that combining an autophagy inhibitor with HDACi could reverse the negative effects on nuclear factor-kappa B (NF-κB) genes in ALL treatment. Additionally, Agirre et al. demonstrated the synergistic effects of LBH589 and vincristine in xenografts of human leukemia in BALB/c-RAG2−/− γc −/− mice, and suggested that this combinatorial strategy could also be applied with dexamethasone (69). Another study by Leclerc found that SAHA enhanced the cytotoxicity of MTX in childhood ALL (70). This combination strategy has also been described for central nervous system lymphoma (71). SAHA was also shown to increase the expression of FPGS by 2-5-fold, while simultaneously reducing the level of DHFR and reversing its inhibitory on chemotherapy. The combination of SAHA and idarubicin is effective in pre-B-ALL, with HDAC2 implicated as a possible effector of synergism with SAHA (72). Chidamide plus chemotherapy is another strategy that has achieved better CR and ORR in patients with T-cell acute lymphoblastic lymphoma/leukemia (T-LBL/ALL) than chemotherapy alone (68). However, the underlying mechanism for this improvement remains unclear.
The clinical benefits of targeted therapeutic strategies for ALL have been observed in recent decades. According to the American Cancer Society, ALL patients with Ph+ protein show sensitivity to TKIs, such as imatinib, dasatinib, and nilotinib, particularly in B-ALL (73). While the positive effects of combining HDACi and targeted therapy have been extensively discussed in chronic lymphocytic leukemia (CLL), they have been less studied in of ALL. CLL is characterized by the aberrant accumulation of CD5+ B cells that can be targeted by HDAC6 (74, 75). Preclinical research on ALL has shown that the combination of HDACi and proteasome inhibitors such as PXD101 and bortezomib, exhibits synergistic effects through inhibiting NF-κB pathways and weakening HDAC6- mediated α-tubulin acetylation, expressions of apoptosis proteins like bim were found after the synergy use of two drugs (76). Cotreatment with a low dose of bortezomib has been found to increase apoptosis in hematological diseases (77).
Immunotherapy is a trending topic in medical oncology because it has fewer toxic side effects and is efficient. A reduction in immune evasion was found with a combination of epigenetic agents and immunotherapy, and the positive influence of HDACi on immune cells has been demonstrated in other cases (78, 79). The rationale behind the synergy between HDACi and immunotherapy can be attributed to several key factors. First, epigenetic modifications like HDACi and DNMTi can regulate T helper cells (Th) Th1 and Th2 through interferon-γ (IFN-γ). This connection was also supported by another study showing that the HDAC-Sin3A complex inhibits the accumulation of H4 acetylation by recruiting to IFNg-locus in Th0 cells, whereas the Th1 differential causes the loss of HDAC-Sin3A (80). Moreover, HDACs play a crucial role in regulating the functions of various immune cells such as neutrophils, eosinophils, and mast cells (81). Currently, most studies have focused on the combination of HDACi and programmed death-ligand 1(PD-L1). HDACi is a PD-L1 enhancer that inhibits tumor growth and helps overcome PD-L1 antibody resistance (82–84). In hematology, a combination of an anti-PD-1 antibody called sintilimab and chidamide has shown synergistic effects in newly diagnosed extranidal natural killer/T-cell lymphoma with minimal toxicity (85). The same combination was also mentioned by Chen et al. in a patient with relapsed/refractory transformed diffuse large B-cell lymphoma who was primarily refractory to R2-CHOP, R2-MTX, and Gemox regimens (86). Song et al. reported the first successful use of this combination strategy in the maintenance therapy of T-ALL. Bone marrow evaluation and minimal residual disease detection implied complete remission after the two-year term therapy (68). HDACi are also helpful in leukemia treatment after CAR-T cell therapy (87, 88). CD20 is a key factor in the interaction between HDACi and CAR-T cells. Reports reveal that HDACi including VPA, romidepsin could increase the expression levels of CD20 CAR-T cells as well as CAR-NK cells in cancer cells, leading to increased production of IFN-γ and tumor necrosis factor (TNF)-α (89, 90)
The combination use of two types of drugs gives more chances for increasing treatment efficiency as well as discovering binding sites in two therapeutic strategies (Figure 4). Currently, HDACi is mainly used as an adjuvant therapy together with other types of agents, thereby promoting drug efficiency in antileukemic process.
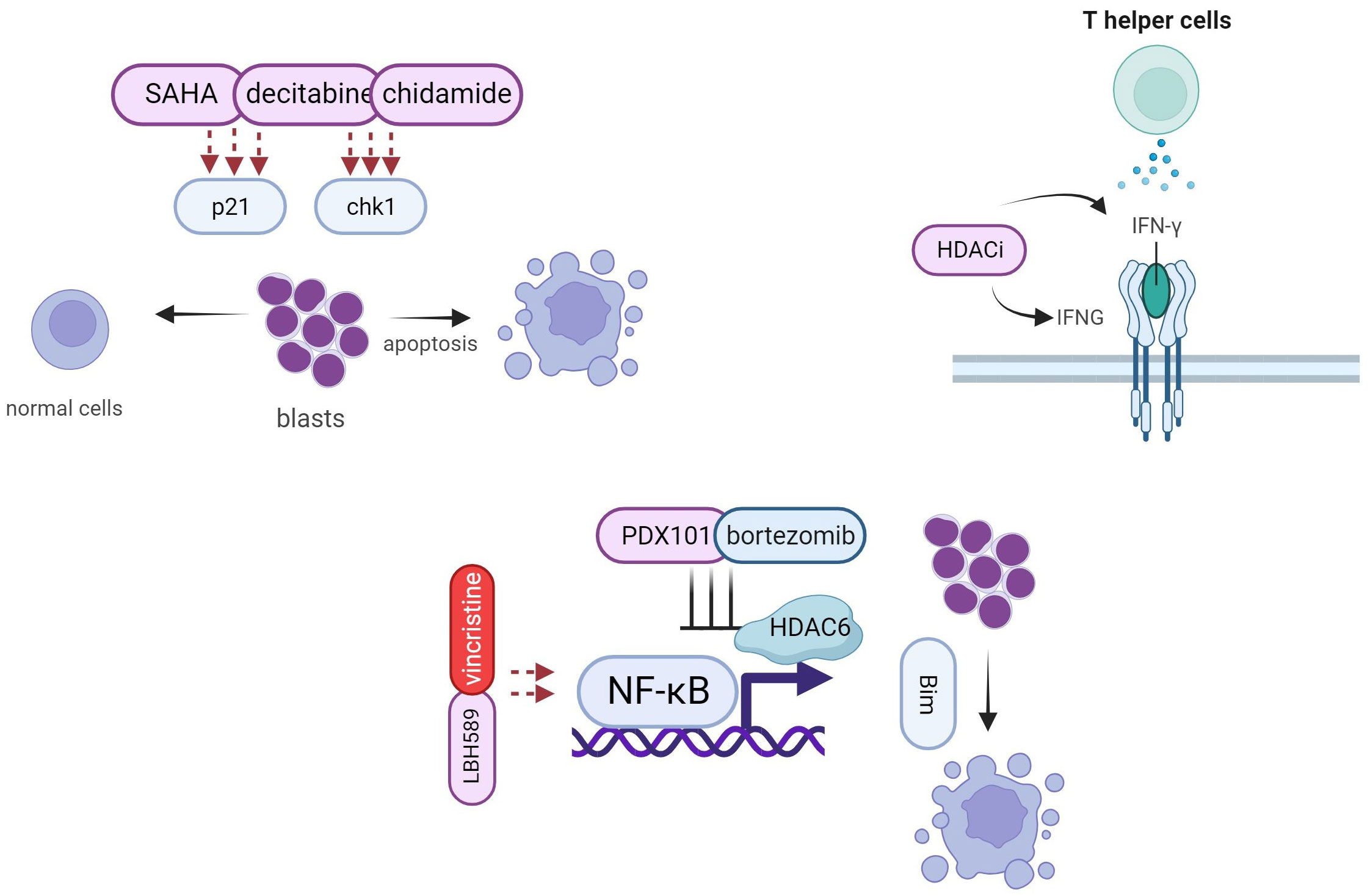
Figure 4 Synergy effects of HDACi and other anticancer agents.
Based on previous studies, LBH589 is more important as a monotherapy than SAHA in the treatment of ALL. On the other hand, SAHA has shown potential effects mainly in co-treatment strategies. SAHA and MTX can synergize to promote ALL cell apoptosis, but lacks efficiency when combined with LBH589 (41, 70). Another strategy involving SAHA and decitabine has proven to be highly effective in both clinical trials and preclinical studies in leukemia cells (65, 91), however, very few studies have reported positive results when SAHA was used as a single agent (92). To date, numerous studies have demonstrated the effects of LBH589 as a monotherapy for ALL, providing different insights into the effects of LBH589 and SAHA. Chidamide was the first approved HDACi for T cell leukemia-lymphoma, although only in China and Japan (93). Numerous studies have investigated chidamide in the field of hematological diseases. Currently, there are 17 registered studies on ClincialTrials.gov, including 4 trials on ALL. Positive results have been widely reported in leukemia, including AML and ALL (94–97), with more cases of AML than ALL. Moreover, the role of chidamide has spread to include a maintenance effect after chemotherapy or stem cell transplantation in ALL patients (62). The efficiency of maintenance therapy after CAR-T for refractory ALL was also observed in another study (98). Considering the potential positive effects in treating ALL, further investigations on the use of chidamide as an adjuvant therapy in ALL are warranted.
In recent years, chemotherapy has led to curative outcomes but with aggressive side effects. Small molecular regimens, such as HDACi or targeted therapy, have been tried as a combinational therapeutic strategy in order to enhance the sensitivity and reduce the toxicity of chemotherapy alone. Regarding the detailed combinatorial strategies, Dieter suggested when used in combination, chemotherapy induction should be initiated in adults, followed by adolescents and finally children, as survival rates in children undergoing chemotherapy were the highest among all age groups (90%) (99). Successful treatment has been achieved in patients with aggressive non-Hodgkin lymphoma cases. Chidamide and lenalidomide resulted in complete and durable remission. Although the number of cases was limited (three patients), further evaluation of this strategy is warranted (100). Moreover, the combination of chidamide and the anti-PD-1 agent sintilimab is suitable for early-stage non-Hodgkin lymphoma (85).
In addition, toxicity issues caused by HDACi are concerns in clinics, although the side effects are less than chemo drugs. Relative toxicities have been reported in other diseases, primarily affecting the gastrointestinal, cardiac and hematology systems, in which hematological toxicities in leukemia patients should be considered carefully (101, 102). A phase I trial assessed the safety of HDACi found that the most frequent hematological effects include thrombocytopenia (28% grade 1-2; 10% grade 3-4) and neutropenia (20% grade 1-2; 16% grade 3-4) (103). Safety and tolerability should be evaluated in further clinical trials by adjusting dose of HDACi. Besides, long term toxicity indicates the epigenic modifications may promote the oncogene expression and a risk of second malignancy (104).
In conclusion, above results indicate that HDACi are promising factors in combinatorial treatment for ALL patients. Furthermore, individualized treatment should be tried in specific targets in patients with different gene mutations. Only using appropriate strategies can maximize the treatment efficiency and thereby increasing the life quality of ALL patients.
YZ: Writing – original draft, Writing – review & editing, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision. GZ: Data curation, Methodology, Writing – original draft. YW: Methodology, Data curation, Writing – original draft. LY: Methodology, Data curation, Writing – original draft. LP: Methodology, Data curation, Writing – original draft. RS: Data curation, Methodology, Writing – original draft. SG: Data curation, Methodology, Writing – original draft. JH: Data curation, Methodology, Writing – original draft. HY: Data curation, Methodology, Writing – original draft. QD: Investigation, Software, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Medical Science and Technology Project of Health Commission of Sichuan Province (No. 21PJ054).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ALL, acute lymphocytic leukemia; AML, acute myeloid leukemia; B-ALL, B cell lymphocytic leukemia; BCP-ALL, B cell precursor acute lymphocytic leukemia; CLL, chronic lymphocytic leukemia; CRISPR, Clustered Regularly Interspaced Short Palindromic Repeats; CTCL, cutaneous T-cell lymphoma; DNMTi, DNA methyltransferase inhibitor; ETP, Early T-cell precursor; FDA, Food and Drug Administration; FK-228, romidepsin; HATs, histone acetyltransferases; HDACi, histone deacetylase inhibitors; HDACs, histone deacetylases; IFN-γ, interferon-γ; ITF2357, givinostat; LBH589, panobinostat; MM, multiple myeloma; MTX, methotrexate; NF-κB, nuclear factor-kappa B; ORR, overall response rate; OS, overall survival; PD-L1, programmed death-ligand 1; PFS, progression free survival; Ph, Philadelphia chromosome; PTCL, peripheral T-cell lymphoma; PXD101, belinostat; ROS, reactive oxygen species; SAHA, vorinostat; T-ALL, T-cell acute lymphocytic leukemia; Th, T helper; TKI, tyrosine kinase inhibitors; T-LBL, T-cell acute lymphoblastic lymphoma; TNF, tumour necrosis factor; VPA, valproic acida.
1. Pui C-H, Nichols KE, Yang JJ. Somatic and germline genomics in paediatric acute lymphoblastic leukaemia. Nat Rev Clin Oncol (2019) 16(4):227–40. doi: 10.1038/s41571-018-0136-6
2. Park S-Y, Kim J-S. A short guide to histone deacetylases including recent progress on class II enzymes. Exp Mol Med (2020) 52(2):204–12. doi: 10.1038/s12276-020-0382-4
3. Xia C, Tao Y, Li M, Che T, Qu J. Protein acetylation and deacetylation: An important regulatory modification in gene transcription. Exp Ther Med (2020) 20(4):2923–40. doi: 10.3892/etm.2020.9073
4. Nagasaka M, Miyajima C, Aoki H, Aoyama M, Morishita D, Inoue Y, et al. Insights into regulators of p53 acetylation. Cells (2022) 11(23):3825. doi: 10.3390/cells11233825
5. Gupta M, Han J, Stenson M, Wellik L, Witzig T. Regulation of STAT3 by histone deacetylase-3 in diffuse large B-cell lymphoma: implications for therapy. Leukemia (2012) 26(6):1356–64. doi: 10.1038/leu.2011.340
6. Cheng F, Lienlaf M, Wang H-W, Perez-Villarroel P, Lee C, Woan K, et al. A novel role for histone deacetylase 6 in the regulation of the tolerogenic STAT3/IL-10 pathway in APCs. J Immunol (2014) 193(6):2850–62. doi: 10.4049/jimmunol.1302778
7. Chen HP, Zhao YT, Zhao TC. Histone deacetylases and mechanisms of regulation of gene expression. Crit Reviews™ Oncogenesis (2015) 20:(1–2). doi: 10.1615/CritRevOncog.2015012997
8. Marquard L, Poulsen CB, Gjerdrum LM, de Nully Brown P, Christensen IJ, Jensen PB, et al. Histone deacetylase 1, 2, 6 and acetylated histone H4 in B-and T-cell lymphomas. Histopathology (2009) 54(6):688–98. doi: 10.1111/j.1365-2559.2009.03290.x
9. Kong Y, Ren W, Fang H, Shah NA, Shi Y, You D, et al. Histone deacetylase inhibitors (HDACi) promote KLF5 ubiquitination and degradation in basal-like breast cancer. Int J Biol Sci (2022) 18(5):2104. doi: 10.7150/ijbs.65322
10. Seidlitz T, Schmäche T, Lee JH, Qin N, Kochall S, Fohgrub J, et al. Sensitivity towards HDAC inhibition is associated with RTK/MAPK pathway activation in gastric cancer. EMBO Mol Med (2022) 14(10):e15705. doi: 10.15252/emmm.202215705
11. Bai M, Cui M, Li M, Yao X, Wu Y, Zheng L, et al. Discovery of a novel HDACi structure that inhibits the proliferation of ovarian cancer cells in vivo and in vitro. Int J Biol Sci (2021) 17(13):3493. doi: 10.7150/ijbs.62339
12. Mamdani H, Jalal SI. Histone deacetylase inhibition in non-small cell lung cancer: hype or hope? Front Cell Dev Biol (2020) 8:582370. doi: 10.3389/fcell.2020.582370
13. Salek Farrokhi A, Mohammadlou M, Abdollahi M, Eslami M, Yousefi B. Histone deacetylase modifications by probiotics in colorectal cancer. J Gastrointestinal Cancer (2020) 51:754–64. doi: 10.1007/s12029-019-00338-2
14. Collier CD, Getty PJ, Greenfield EM. Targeting the cancer epigenome with histone deacetylase inhibitors in osteosarcoma. In: Eds. Kleinerman E., Gorlick R. Current Advances in the Science of Osteosarcoma. Advances in Experimental Medicine and Biology. Cham: Springer (2020) vol 1258. doi: 10.1007/978-3-030-43085-6_4
15. Seto E, Yoshida M. Erasers of histone acetylation: the histone deacetylase enzymes. Cold Spring Harbor Perspect Biol (2014) 6(4):a018713. doi: 10.1101/cshperspect.a018713
16. DeAngelo DJ, Walker AR, Schlenk RF, Sierra J, Medeiros BC, Ocio EM, et al. Safety and efficacy of oral panobinostat plus chemotherapy in patients aged 65 years or younger with high-risk acute myeloid leukemia. Leukemia Res (2019) 85:106197. doi: 10.1016/j.leukres.2019.106197
17. Goldberg J, Sulis ML, Bender J, Jeha S, Gardner R, Pollard J, et al. A phase I study of panobinostat in children with relapsed and refractory hematologic Malignancies. Pediatr Hematol Oncol (2020) 37(6):465–74. doi: 10.1080/08880018.2020.1752869
18. Burke MJ, Lamba J, Weigel B, Bachanova V, Verneris MR, Miller JS. A phase II trial of decitabine and vorinostat in combination with chemotherapy for relapsed/refractory acute lymphoblastic leukemia. Am Soc Hematol (2012). doi: 10.1182/blood.V120.21.4307.4307
19. Burke MJ, Kostadinov R, Sposto R, Gore L, Kelley SM, Rabik C, et al. Decitabine and vorinostat with chemotherapy in relapsed pediatric acute lymphoblastic leukemia: A TACL pilot studyDecitabine and vorinostat for relapsed ALL. Clin Cancer Res (2020) 26(10):2297–307. doi: 10.1158/1078-0432.CCR-19-1251
20. Shi Y, Jia B, Xu W, Li W, Liu T, Liu P, et al. Chidamide in relapsed or refractory peripheral T cell lymphoma: a multicenter real-world study in China. J Hematol Oncol (2017) 10(1):1–5. doi: 10.1186/s13045-017-0439-6
21. Zhou H, Gao Y, Wang Q, Cao R, Zhen Z, Li Q, et al. A novel oral histone deacetylase inhibitor chidamide is highly effective and well-tolerated in adult early T-cell precursor and Ph-like acute lymphoblastic leukemia. Blood (2018) 132:4011. doi: 10.1182/blood-2018-99-113712
22. Liu J, Zhang L, Guo L, Zeng Y, Guo Q, Yang C, et al. Novel bioactive hybrid Celecoxib-HDAC Inhibitor, induces apoptosis in human acute lymphoblastic leukemia cells. Bioorganic Medicinal Chem (2022) 75:117085. doi: 10.1016/j.bmc.2022.117085
23. Mehrpouri M, Safaroghli-Azar A, Momeny M, Bashash D. Anti-leukemic effects of histone deacetylase (HDAC) inhibition in acute lymphoblastic leukemia (ALL) cells: Shedding light on mitigating effects of NF-κB and autophagy on panobinostat cytotoxicity. Eur J Pharmacol (2020) 875:173050. doi: 10.1016/j.ejphar.2020.173050
24. Cheung LC, Cruickshank MN, Hughes AM, Singh S, Chua G-A, Ford J, et al. Romidepsin enhances the efficacy of cytarabine in vivo, revealing histone deacetylase inhibition as a promising therapeutic strategy for KMT2A-rearranged infant acute lymphoblastic leukemia. haematologica (2019) 104(7):e300. doi: 10.3324/haematol.2018.192906
25. Waibel M, Vervoort S, Kong I, Heinzel S, Ramsbottom K, Martin B, et al. Epigenetic targeting of Notch1-driven transcription using the HDACi panobinostat is a potential therapy against T-cell acute lymphoblastic leukemia. Leukemia (2018) 32(1):237–41. doi: 10.1038/leu.2017.282
26. Savino AM, Sarno J, Trentin L, Vieri M, Fazio G, Bardini M, et al. The histone deacetylase inhibitor givinostat (ITF2357) exhibits potent anti-tumor activity against CRLF2-rearranged BCP-ALL. Leukemia (2017) 31(11):2365–75. doi: 10.1038/leu.2017.93
27. Li Y, Zhao K, Yao C, Kahwash S, Tang Y, Zhang G, et al. Givinostat, a type II histone deacetylase inhibitor, induces potent caspase-dependent apoptosis in human lymphoblastic leukemia. Genes Cancer (2016) 7(9-10):292. doi: 10.18632/genesandcancer.117
28. Chao M-W, Lai M-J, Liou J-P, Chang Y-L, Wang J-C, Pan S-L, et al. The synergic effect of vincristine and vorinostat in leukemia in vitro and in vivo. J Hematol Oncol (2015) 8:1–15. doi: 10.1186/s13045-015-0176-7
29. Valdez B, Brammer J, Li Y, Murray D, Liu Y, Hosing C, et al. Romidepsin targets multiple survival signaling pathways in Malignant T cells. Blood Cancer J (2015) 5(10):e357–7. doi: 10.1038/bcj.2015.83
30. Bastian L, Hof J, Pfau M, Fichtner I, Eckert C, Henze G, et al. Synergistic activity of bortezomib and HDACi in preclinical models of B-cell precursor acute lymphoblastic leukemia via modulation of p53, PI3K/AKT, and NF-κB. Clin Cancer Res (2013) 19(6):1445–57. doi: 10.1158/1078-0432.CCR-12-1511
31. Hasegawa H, Yamada Y, Tsukasaki K, Mori N, Tsuruda K, Sasaki D, et al. LBH589, a deacetylase inhibitor, induces apoptosis in adult T-cell leukemia/lymphoma cells via activation of a novel RAIDD-caspase-2 pathway. Leukemia (2011) 25(4):575–87. doi: 10.1038/leu.2010.315
32. Scuto A, Kirschbaum M, Kowolik C, Kretzner L, Juhasz A, Atadja P, et al. The novel histone deacetylase inhibitor, LBH589, induces expression of DNA damage response genes and apoptosis in Ph– acute lymphoblastic leukemia cells. Blood J Am Soc Hematol (2008) 111(10):5093–100. doi: 10.1182/blood-2007-10-117762
33. Castro PG, Van Roon E, Pinhanços S, Trentin L, Schneider P, Kerstjens M, et al. The HDAC inhibitor panobinostat (LBH589) exerts in vivo anti-leukaemic activity against MLL-rearranged acute lymphoblastic leukaemia and involves the RNF20/RNF40/WAC-H2B ubiquitination axis. Leukemia (2018) 32(2):323–3. doi: 10.1038/leu.2017.216
34. Cordó V, van der Zwet JC, Canté-Barrett K, Pieters R, Meijerink JP. T-cell acute lymphoblastic leukemia: A roadmap to targeted therapiesT-ALL: A roadmap to targeted therapies. Blood Cancer Discovery (2021) 2(1):19–31. doi: 10.1158/2643-3230.BCD-20-0093
35. Schnapp LM. Another notch on the belt. Blood J Am Soc Hematol (2009) 113(8):1615–6. doi: 10.1182/blood-2008-12-192815
36. Vujovic F, Hunter N, Farahani RM. Notch pathway: a bistable inducer of biological noise? Cell Communication Signaling (2019) 17:1–13. doi: 10.1186/s12964-019-0453-0
37. Ferrante F, Giaimo BD, Bartkuhn M, Zimmermann T, Close V, Mertens D, et al. HDAC3 functions as a positive regulator in Notch signal transduction. Nucleic Acids Res (2020) 48(7):3496–512. doi: 10.1093/nar/gkaa088
38. Hosseini-Alghaderi S, Baron M. Notch3 in development, health and disease. Biomolecules (2020) 10(3):485. doi: 10.3390/biom10030485
39. Pinazza M, Ghisi M, Minuzzo S, Agnusdei V, Fossati G, Ciminale V, et al. Histone deacetylase 6 controls Notch3 trafficking and degradation in T-cell acute lymphoblastic leukemia cells. Oncogene (2018) 37(28):3839–51. doi: 10.1038/s41388-018-0234-z
40. Palermo R, Checquolo S, Giovenco A, Grazioli P, Kumar V, Campese A, et al. Acetylation controls Notch3 stability and function in T-cell leukemia. Oncogene (2012) 31(33):3807–17. doi: 10.1038/onc.2011.533
41. Moreno DA, Junior HLR, Laranjeira ABA, Cruzeiro GAV, Borges KS, Salomão KB, et al. Panobinostat (LBH589) increase survival in adult xenografic model of acute lymphoblastic leukemia with t (4; 11) but promotes antagonistic effects in combination with MTX and 6MP. Med Oncol (2022) 39(12):216. doi: 10.1007/s12032-022-01813-w
42. Jiang C, Qian M, Gocho Y, Yang W, Du G, Shen S, et al. Genome-wide CRISPR/Cas9 screening identifies determinant of panobinostat sensitivity in acute lymphoblastic leukemia. Blood Adv (2022) 6(8):2496–509. doi: 10.1182/bloodadvances.2021006152
43. San José-Enériz E, Gimenez-Camino N, Agirre X, Prosper F. HDAC inhibitors in acute myeloid leukemia. Cancers (2019) 11(11):1794. doi: 10.3390/cancers11111794
44. Yoshida K, Fujita A, Narazaki H, Asano T, Itoh Y. Drug resistance to nelarabine in leukemia cell lines might be caused by reduced expression of deoxycytidine kinase through epigenetic mechanisms. Cancer Chemother Pharmacol (2022) 89:83–91. doi: 10.1007/s00280-021-04373-4
45. Shirazi PT, Eadie LN, Heatley SL, Page EC, François M, Hughes TP, et al. Exploring the oncogenic and therapeutic target potential of the MYB-TYK2 fusion gene in B-cell acute lymphoblastic leukemia. Cancer Gene Ther (2022) 29(8-9):1140–52. doi: 10.1038/s41417-021-00421-6
46. Johnston PB, Cashen AF, Nikolinakos PG, Beaven AW, Barta SK, Bhat G, et al. Belinostat in combination with standard cyclophosphamide, doxorubicin, vincristine and prednisone as first-line treatment for patients with newly diagnosed peripheral T-cell lymphoma. Exp Hematol Oncol (2021) 10:1–11. doi: 10.1186/s40164-021-00203-8
47. Zuo Y, Xu H, Chen Z, Xiong F, Zhang B, Chen K, et al. 17−AAG synergizes with Belinostat to exhibit a negative effect on the proliferation and invasion of MDA−MB−231 breast cancer cells. Oncol Rep (2020) 43(6):1928–44. doi: 10.3892/or.2020.7563
48. Kirschbaum MH, Foon KA, Frankel P, Ruel C, Pulone B, Tuscano JM, et al. A phase 2 study of belinostat (PXD101) in patients with relapsed or refractory acute myeloid leukemia or patients over the age of 60 with newly diagnosed acute myeloid leukemia: a California Cancer Consortium Study. Leukemia lymphoma (2014) 55(10):2301–4. doi: 10.3109/10428194.2013.877134
49. Holkova B, Shafer D, Yazbeck V, Dave S, Bose P, Tombes MB, et al. Phase 1 study of belinostat (PXD-101) and bortezomib (Velcade, PS-341) in patients with relapsed or refractory acute leukemia and myelodysplastic syndrome. Leukemia lymphoma (2021) 62(5):1187–94. doi: 10.1080/10428194.2020.1861270
50. Diamanti P, Cox CV, Blair A, Kearns PR. Investigation of the efficacy of PXD101 (Belinostat) on primary leukaemic cells and cell lines as a novel agent for childhood acute lymphoblastic leukaemia (ALL). Blood (2007) 110(11):2793. doi: 10.1182/blood.V110.11.2793.2793
51. Brunvand MW, Carson J. Complete remission with romidepsin in a patient with T-cell acute lymphoblastic leukemia refractory to induction hyper-CVAD. Hematological Oncol (2018) 36(1):340–3. doi: 10.1002/hon.2421
52. Pinazza M, Borga C, Agnusdei V, Minuzzo S, Fossati G, Paganin M, et al. An immediate transcriptional signature associated with response to the histone deacetylase inhibitor Givinostat in T acute lymphoblastic leukemia xenografts. Cell Death Dis (2016) 7(1):e2047–7. doi: 10.1038/cddis.2015.394
53. Sun Y, Hong JH, Ning Z, Pan D, Fu X, Lu X, et al. Therapeutic potential of tucidinostat, a subtype-selective HDAC inhibitor, in cancer treatment. Front Pharmacol (2022) 13:932914. doi: 10.3389/fphar.2022.932914
54. Tsukasaki K, Fukushima T. JSH practical guidelines for hematological Malignancies, 2018: II. Lymphoma-8. Adult T-cell leukemia–lymphoma. Int J Hematol (2019) 109:249–59. doi: 10.1007/s12185-018-02588-5
55. Huang K, Tang B, Cai Z, He X, Li Q, Liu N, et al. HDACi targets IKZF1 deletion high-risk acute lymphoblastic leukemia by inducing IKZF1 expression and rescuing IKZF1 function in vitro and in vivo. Blood (2021) 138:514. doi: 10.1182/blood-2021-152926
56. Xi M, Guo S, Bayin C, Peng L, Chuffart F, Bourova-Flin E, et al. Chidamide inhibits the NOTCH1-MYC signaling axis in T-cell acute lymphoblastic leukemia. Front Med (2022) 16:442–58. doi: 10.1007/s11684-021-0877-y
57. Yan M-M, Li Z-X, Chen C, Zhang W, Zhou D-B. Study on the regulation of chidamide on CD8+ T cells in T-cell acute lymphoblastic leukemia. Zhongguo Shi Yan Xue Ye Xue Za Zhi (2023) 31(1):71–5. doi: 10.19746/j.cnki.issn.1009-2137.2023.01.011
58. Neo SY, Lundqvist A. The multifaceted roles of CXCL9 within the tumor microenvironment. In: Ed. Birbrair A. Tumor Microenvironment. Advances in Experimental Medicine and Biology. Cham: Springer (2020) vol 1231. doi: 10.1007/978-3-030-36667-4_5
59. Seitz S, Dreyer TF, Stange C, Steiger K, Bräuer R, Scheutz L, et al. CXCL9 inhibits tumour growth and drives anti-PD-L1 therapy in ovarian cancer. Br J Cancer (2022) 126(10):1470–80. doi: 10.1038/s41416-022-01763-0
60. Xiu W, Luo J. CXCL9 secreted by tumor-associated dendritic cells up-regulates PD-L1 expression in bladder cancer cells by activating the CXCR3 signaling. BMC Immunol (2021) 22(1):1–9.
61. Yang X, Yu Q, Xu H, Zhou J. Upregulation of CD22 by Chidamide promotes CAR T cells functionality. Sci Rep (2021) 11(1):20637. doi: 10.1038/s41598-021-00227-4
62. Li X-Y, Han X-W, Huang K, Zhang Y-T, Xu H-G, Zhou D-H, et al. Chidamide as maintenance after chemotherapy or hematopoietic stem cell transplantation in 27 children with T-cell lymphoblastic leukemia: A real-world prospective study. Front Med (2023) 10. doi: 10.3389/fmed.2023.1096529
63. Qualls D, Noy A, Straus D, Matasar M, Moskowitz C, Seshan V, et al. Molecularly targeted epigenetic therapy with mocetinostat in relapsed and refractory non-Hodgkin lymphoma with CREBBP or EP300 mutations: an open label phase II study. Leukemia Lymphoma (2023) 64(3):738–41. doi: 10.1080/10428194.2022.2164194
64. Quagliano A, Gopalakrisnapillai A, Kolb EA, Barwe S. Epigenetic drug combination overcomes bone marrow microenvironment-induced chemoprotection in pediatric acute lymphoblastic leukemia via modulation of CD81. Blood (2018) 132:3957. doi: 10.1182/blood-2018-99-120275
65. Burke MJ, Lamba JK, Pounds S, Cao X, Ghodke-Puranik Y, Lindgren BR, et al. A therapeutic trial of decitabine and vorinostat in combination with chemotherapy for relapsed/refractory acute lymphoblastic leukemia. Am J Hematol (2014) 89(9):889–95. doi: 10.1002/ajh.23778
66. Li G, Li D, Yuan F, Cheng C, Chen L, Wei X. Synergistic effect of chidamide and venetoclax on apoptosis in acute myeloid leukemia cells and its mechanism. Ann Trans Med (2021) 9:(20). doi: 10.21037/atm-21-5066
67. Bhatla T, Wang J, Morrison DJ, Raetz EA, Burke MJ, Brown P, et al. Epigenetic reprogramming reverses the relapse-specific gene expression signature and restores chemosensitivity in childhood B-lymphoblastic leukemia. Blood J Am Soc Hematol (2012) 119(22):5201–10. doi: 10.1182/blood-2012-01-401687
68. Song Y, Chen S, Liu C, Chen L, Wang W, Wu B, et al. Chemo-free maintenance therapy in adult T-cell acute lymphoblastic leukemia: A case report and literature review. Front Pharmacol (2023) 14:1051305. doi: 10.3389/fphar.2023.1051305
69. Vilas-Zornoza A, Agirre X, Abizanda G, Moreno C, Segura V, De Martino Rodriguez A, et al. Preclinical activity of LBH589 alone or in combination with chemotherapy in a xenogeneic mouse model of human acute lymphoblastic leukemia. Leukemia (2012) 26(7):1517–26. doi: 10.1038/leu.2012.31
70. Leclerc G, Mou C, Leclerc G, Mian A, Barredo J. Histone deacetylase inhibitors induce FPGS mRNA expression and intracellular accumulation of long-chain methotrexate polyglutamates in childhood acute lymphoblastic leukemia: implications for combination therapy. Leukemia (2010) 24(3):552–62. doi: 10.1038/leu.2009.282
71. Fujimoto K, Shinojima N, Hayashi M, Nakano T, Ichimura K, Mukasa A. Histone deacetylase inhibition enhances the therapeutic effects of methotrexate on primary central nervous system lymphoma. Neuro-Oncology Adv (2020) 2(1):vdaa084. doi: 10.1093/noajnl/vdaa084
72. Boncan J, Hamilton J, McCloskey K, Mills KI. New mechanistic and therapeutic insights into purified phospholipase A2 from Pseudechis australis snake venom-a novel anticancer agent for the treatment of precursor B-cell acute lymphoblastic leukaemia. Blood (2022) 140(Supplement 1):3120–1. doi: 10.1182/blood-2022-166114
73. Foà R, Bassan R, Vitale A, Elia L, Piciocchi A, Puzzolo M-C, et al. Dasatinib–blinatumomab for Ph-positive acute lymphoblastic leukemia in adults. New Engl J Med (2020) 383(17):1613–23. doi: 10.1056/NEJMoa2016272
74. Kipps TJ, Choi MY. Targeted therapy in chronic lymphocytic leukemia. Cancer J (Sudbury Mass) (2019) 25(6):378. doi: 10.1097/PPO.0000000000000416
75. Maharaj K, Powers JJ, Mediavilla-Varela M, Achille A, Gamal W, Quayle S, et al. HDAC6 inhibition alleviates CLL-induced T-cell dysfunction and enhances immune checkpoint blockade efficacy in the Eμ-TCL1 model. Front Immunol (2020) 11:590072. doi: 10.3389/fimmu.2020.590072
76. Dai Y, Chen S, Wang L, Pei XY, Kramer LB, Dent P, et al. Bortezomib interacts synergistically with belinostat in human acute myeloid leukaemia and acute lymphoblastic leukaemia cells in association with perturbations in NF-κB and Bim. Br J haematology (2011) 153(2):222–35. doi: 10.1111/j.1365-2141.2011.08591.x
77. He Y, Jiang D, Zhang K, Zhu Y, Zhang J, Wu X, et al. Chidamide, a subtype-selective histone deacetylase inhibitor, enhances Bortezomib effects in multiple myeloma therapy. J Cancer (2021) 12(20):6198. doi: 10.7150/jca.61602
78. Xu Y, Li P, Liu Y, Xin D, Lei W, Liang A, et al. Epi-immunotherapy for cancers: rationales of epi-drugs in combination with immunotherapy and advances in clinical trials. Cancer Commun (2022) 42(6):493–516. doi: 10.1002/cac2.12313
79. Chen X, Pan X, Zhang W, Guo H, Cheng S, He Q, et al. Epigenetic strategies synergize with PD-L1/PD-1 targeted cancer immunotherapies to enhance antitumor responses. Acta Pharm Sin B (2020) 10(5):723–33. doi: 10.1016/j.apsb.2019.09.006
80. Chang S, Collins PL, Aune TM. T-bet dependent removal of Sin3A-histone deacetylase complexes at the Ifng locus drives Th1 differentiation. J Immunol (2008) 181(12):8372–81. doi: 10.4049/jimmunol.181.12.8372
81. Zhang S, Zhan L, Li X, Yang Z, Luo Y, Zhao H. Preclinical and clinical progress for HDAC as a putative target for epigenetic remodeling and functionality of immune cells. Int J Biol Sci (2021) 17(13):3381. doi: 10.7150/ijbs.62001
82. Li X, Su X, Liu R, Pan Y, Fang J, Cao L, et al. HDAC inhibition potentiates anti-tumor activity of macrophages and enhances anti-PD-L1-mediated tumor suppression. Oncogene (2021) 40(10):1836–50. doi: 10.1038/s41388-020-01636-x
83. Hegedűs L, Rittler D, Garay T, Stockhammer P, Kovács I, Döme B, et al. HDAC inhibition induces PD-L1 expression in a novel anaplastic thyroid cancer cell line. Pathol Oncol Res (2020) 26:2523–35. doi: 10.1007/s12253-020-00834-y
84. Zhang P, Du Y, Bai H, Wang Z, Duan J, Wang X, et al. Optimized dose selective HDAC inhibitor tucidinostat overcomes anti-PD-L1 antibody resistance in experimental solid tumors. BMC Med (2022) 20(1):1–19. doi: 10.1186/s12916-022-02598-5
85. Yan G, Zhang Y, Wang X, Bai B, Huang Y, He H, et al. Novel induction therapy for newly diagnosed extranodal natural killer/T cell lymphoma (ENKTL) treated by anti-PD-1 antibody plus histone deacetylase inhibitor followed by P-GemOx regimen. Blood (2021) 138(Supplement 1):137–7. doi: 10.1182/blood-2021-147169
86. Chen C, Zhang W, Zhou D, Zhang Y. Sintilimab and chidamide for refractory transformed diffuse large B cell lymphoma: A case report and A literature review. Front Oncol (2021) 11:757403. doi: 10.3389/fonc.2021.757403
87. Wen J, Chen Y, Yang J, Dai C, Yu S, Zhong W, et al. Valproic acid increases CAR T cell cytotoxicity against acute myeloid leukemia. J Immunotherapy Cancer (2023) 11:(7). doi: 10.1136/jitc-2023-006857
88. Luo L, Zhou X, Zhou L, Liang Z, Yang J, Tu S, et al. Current state of CAR-T therapy for T-cell Malignancies. Ther Adv Hematol (2022) 13:20406207221143025. doi: 10.1177/20406207221143025
89. Cao X, Jin X, Zhang X, Utsav P, Zhang Y, Guo R, et al. Small-molecule compounds boost CAR-T cell therapy in hematological Malignancies. Curr Treat Options Oncol (2023) 24(3):184–211. doi: 10.1007/s11864-023-01049-4
90. Yang Y, Zhou J, Cao C, Cai P, Wang X, Chang C, et al. Additional possibilities of chimeric antigen receptor T-cells in B-cell lymphoma: combination therapy. Trans Cancer Res (2020) 9(11):7310. doi: 10.21037/tcr-20-72
91. Brodská B, Holoubek A, Otevřelová P, Kuželová K. Combined treatment with low concentrations of decitabine and SAHA causes cell death in leukemic cell lines but not in normal peripheral blood lymphocytes. BioMed Res Int (2013). doi: 10.1155/2013/659254
92. Keshelava N, Houghton PJ, Morton CL, Lock RB, Carol H, Keir ST, et al. Initial testing (stage 1) of vorinostat (SAHA) by the pediatric preclinical testing program. Pediatr Blood Cancer (2009) 53(3):505–8. doi: 10.1002/pbc.21988
93. He B, Wang Q, Liu X, Lu Z, Han J, Pan C, et al. A novel HDAC inhibitor chidamide combined with imatinib synergistically targets tyrosine kinase inhibitor resistant chronic myeloid leukemia cells. Biomedicine Pharmacotherapy (2020) 129:110390. doi: 10.1016/j.biopha.2020.110390
94. Wang H, Liu Y-c, Zhu C-y, Yan F, Wang M-z, Chen X-s, et al. Chidamide increases the sensitivity of refractory or relapsed acute myeloid leukemia cells to anthracyclines via regulation of the HDAC3-AKT-P21-CDK2 signaling pathway. J Exp Clin Cancer Res (2020) 39:1–19. doi: 10.1186/s13046-020-01792-8
95. Lin L, Que Y, Lu P, Li H, Xiao M, Zhu X, et al. Chidamide inhibits acute myeloid leukemia cell proliferation by lncRNA VPS9D1-AS1 downregulation via MEK/ERK signaling pathway. Front Pharmacol (2020) 11:569651. doi: 10.3389/fphar.2020.569651
96. Liu J, Lv N, Zhou L, Li Y, Yu L. Chidamide inhibits t (8; 21) AML cell proliferation and AMK1/ETO and C-KIT expression by inhibiting ERK1/2 signaling pathway. Trans Cancer Res (2020) 9(2):827.
97. Guo Z, Guo D, Kong D, Bian S, Lin L, Fan S, et al. Efficacy and safety of an HDACi-and HMA-based protocol in adults with acute myeloid leukemia of intermediate-and adverse-risk categories: a retrospective study. Hematology (2023) 28(1):2219930. doi: 10.1080/16078454.2023.2219930
98. Zhang X, Huang L, Zhang G, Su Y, Hu X, Xia S, et al. The efficacy of chidamide maintenance therapy after CAR-T therapy for refractory or relapsed B-cell acute lymphoblastic leukemia. Blood (2022) 140(Supplement 1):8884–5. doi: 10.1182/blood-2022-168603
99. Hoelzer D. Chemotherapy-free treatment—a new era in acute lymphoblastic leukemia? N Engl J Med (2020) 383:1673–4. doi: 10.1056/NEJMe2027937
100. Hu S, Zou D, Zhou D, Zhang Y, Wang W, Zhang W. Successful treatment with lenalidomide plus chidamide combination therapy in 3 heavily treated patients with non-Hodgkin lymphoma: three cases report. Medicine (2020) 99:(43). doi: 10.1097/MD.0000000000022788
101. Zhou Y-b, Zhang Y-m, Huang H-h, Shen L-j, Han X-f, Hu X-b, et al. Pharmacodynamic, pharmacokinetic, and phase 1a study of bisthianostat, a novel histone deacetylase inhibitor, for the treatment of relapsed or refractory multiple myeloma. Acta Pharmacologica Sin (2022) 43(4):1091–9. doi: 10.1038/s41401-021-00728-y
102. Gao X, Shen L, Li X, Liu J. Efficacy and toxicity of histone deacetylase inhibitors in relapsed/refractory multiple myeloma: Systematic review and meta−analysis of clinical trials. Exp Ther Med (2019) 18(2):1057–68. doi: 10.3892/etm.2019.7704
103. Eyre TA, Collins GP, Gupta A, Sheikh S, Woodcock V, Whittaker J, et al. Results of a phase I study to assess the safety, tolerability, pharmacokinetics and pharmacodynamics of CXD101: preliminary safety and activity in relapsed or refractory hodgkin and non-hodgkin lymphoma patients. Blood (2016) 128(22):1817. doi: 10.1182/blood.V128.22.1817.1817
Keywords: acute lymphocytic leukemia (ALL), histone deacetylase inhibitors (HDACi), chemotherapy, immunotherapy, targeted therapy
Citation: Zhang Y, Zhang G, Wang Y, Ye L, Peng L, Shi R, Guo S, He J, Yang H and Dai Q (2024) Current treatment strategies targeting histone deacetylase inhibitors in acute lymphocytic leukemia: a systematic review. Front. Oncol. 14:1324859. doi: 10.3389/fonc.2024.1324859
Received: 20 October 2023; Accepted: 29 January 2024;
Published: 21 February 2024.
Edited by:
Daniel Heudobler, University Hospital Regensburg, GermanyReviewed by:
Duohui Jing, Shanghai Jiao Tong University, ChinaCopyright © 2024 Zhang, Zhang, Wang, Ye, Peng, Shi, Guo, He, Yang and Dai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qingkai Dai, ZHFrMDgxOUAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.