{kind=link}

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 14 February 2024
Sec. Cancer Epidemiology and Prevention
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1304633
This article is part of the Research TopicChildhood Leukemias in Latin America: Epidemiology, Causality, Novel Predictive Profiles and Therapeutic StrategiesView all 22 articles
 David Aldebarán Duarte-Rodríguez1
David Aldebarán Duarte-Rodríguez1 Janet Flores-Lujano2
Janet Flores-Lujano2 Richard J. Q. McNally3
Richard J. Q. McNally3 María Luisa Pérez-Saldivar2
María Luisa Pérez-Saldivar2 Elva Jiménez-Hernández4
Elva Jiménez-Hernández4 Jorge Alfonso Martín-Trejo5Laura Eugenia Espinoza-Hernández5
Jorge Alfonso Martín-Trejo5Laura Eugenia Espinoza-Hernández5 Aurora Medina-Sanson6Rogelio Paredes-Aguilera7Laura Elizabeth Merino-Pasaye8Martha Margarita Velázquez-Aviña9
Aurora Medina-Sanson6Rogelio Paredes-Aguilera7Laura Elizabeth Merino-Pasaye8Martha Margarita Velázquez-Aviña9 José Refugio Torres-Nava4
José Refugio Torres-Nava4 Rosa Martha Espinosa-Elizondo10
Rosa Martha Espinosa-Elizondo10 Raquel Amador-Sánchez11Juan José Dosta-Herrera12Javier Anastacio Mondragón-García13Juana Esther González-Ulibarri14Sofía Irene Martínez-Silva15Gilberto Espinoza-Anrubio16María Minerva Paz-Bribiesca17Perla Salcedo-Lozada18Rodolfo Ángel Landa-García19Rosario Ramírez-Colorado20Luis Hernández-Mora21Marlene Santamaría-Ascencio22Anselmo López-Loyola23Arturo Hermilo Godoy-Esquivel24Luis Ramiro García-López25Alison Ireri Anguiano-Ávalos26Karina Mora-Rico27Alejandro Castañeda-Echevarría28Roberto Rodríguez-Jiménez29José Alberto Cibrian-Cruz30Karina Anastacia Solís-Labastida5Rocío Cárdenas-Cardos31Norma López-Santiago7Luz Victoria Flores-Villegas8
Raquel Amador-Sánchez11Juan José Dosta-Herrera12Javier Anastacio Mondragón-García13Juana Esther González-Ulibarri14Sofía Irene Martínez-Silva15Gilberto Espinoza-Anrubio16María Minerva Paz-Bribiesca17Perla Salcedo-Lozada18Rodolfo Ángel Landa-García19Rosario Ramírez-Colorado20Luis Hernández-Mora21Marlene Santamaría-Ascencio22Anselmo López-Loyola23Arturo Hermilo Godoy-Esquivel24Luis Ramiro García-López25Alison Ireri Anguiano-Ávalos26Karina Mora-Rico27Alejandro Castañeda-Echevarría28Roberto Rodríguez-Jiménez29José Alberto Cibrian-Cruz30Karina Anastacia Solís-Labastida5Rocío Cárdenas-Cardos31Norma López-Santiago7Luz Victoria Flores-Villegas8 José Gabriel Peñaloza-González9Ana Itamar González-Ávila11
José Gabriel Peñaloza-González9Ana Itamar González-Ávila11 Martin Sánchez-Ruiz18
Martin Sánchez-Ruiz18 Roberto Rivera-Luna31Luis Rodolfo Rodríguez-Villalobos25Francisco Hernández-Pérez26Jaime Ángel Olvera-Durán27Luis Rey García-Cortés32
Roberto Rivera-Luna31Luis Rodolfo Rodríguez-Villalobos25Francisco Hernández-Pérez26Jaime Ángel Olvera-Durán27Luis Rey García-Cortés32 Minerva Mata-Rocha33
Minerva Mata-Rocha33 Omar Alejandro Sepúlveda-Robles33
Omar Alejandro Sepúlveda-Robles33 Vilma Carolina Bekker-Méndez34
Vilma Carolina Bekker-Méndez34 Silvia Jiménez-Morales35
Silvia Jiménez-Morales35 Jorge Meléndez-Zajgla36
Jorge Meléndez-Zajgla36 Haydée Rosas-Vargas37
Haydée Rosas-Vargas37 Elizabeth Vega38
Elizabeth Vega38 Juan Carlos Núñez-Enríquez2,39*
Juan Carlos Núñez-Enríquez2,39* Juan Manuel Mejía-Aranguré36,40*
Juan Manuel Mejía-Aranguré36,40*Background: A heterogeneous geographic distribution of childhood acute lymphoblastic leukemia (ALL) cases has been described, possibly, related to the presence of different environmental factors. The aim of the present study was to explore the geographical distribution of childhood ALL cases in Greater Mexico City (GMC).
Methods: A population-based case-control study was conducted. Children <18 years old, newly diagnosed with ALL and residents of GMC were included. Controls were patients without leukemia recruited from second-level public hospitals, frequency-matched by sex, age, and health institution with the cases. The residence address where the patients lived during the last year before diagnosis (cases) or the interview (controls) was used for geolocation. Kulldorff’s spatial scan statistic was used to detect spatial clusters (SCs). Relative risks (RR), associated p-value and number of cases included for each cluster were obtained.
Results: A total of 1054 cases with ALL were analyzed. Of these, 408 (38.7%) were distributed across eight SCs detected. A relative risk of 1.61 (p<0.0001) was observed for the main cluster. Similar results were noted for the remaining seven ones. Additionally, a proximity between SCs, electrical installations and petrochemical facilities was observed.
Conclusions: The identification of SCs in certain regions of GMC suggest the possible role of environmental factors in the etiology of childhood ALL.
The frequency of childhood acute leukemias (AL) in Mexico City has been reported to be amongst the highest in the world, mainly, for the acute lymphoblastic leukemia (ALL) subtype (1–3). The etiology of AL remains unclear in most cases. It seems to be the result from an interaction between genetic susceptibility and exposure to environmental factors (4; 5–7).
The spatial analysis of disease incidence distribution has been acknowledged as a valuable approach for uncovering essential insights into the etiology of a disease. (8, 9). In Mexico, there have been limited spatial analysis studies conducted to date related to childhood leukemia. In a preliminary report, a significant spatial cluster (SC) of childhood ALL cases was detected at the eastern side of Mexico City (10). In another research, conducted in the city of Guadalajara, three SCs of ALL cases were also described (11).
On the other hand, in a recent investigation conducted in Mexico City, AL incidence rates displayed differences among municipalities suggesting a potential heterogeneous geographical distribution (3). Noteworthy, Mexico City and its surrounding metropolitan area [also known as the Greater Mexico City (GMC)] has seventy-five municipalities being one of the largest urban agglomerations globally. The core of the metropolis is a proper urban area whereas the outer is considered as a rural–urban fringe area (see Figure 1). When these areas are well-delimited they may significantly differ in demographic factors such as the population density, the main economic activities, exposure to environmental hazards among other which could have an impact in the incidence of childhood leukemia (12–14).
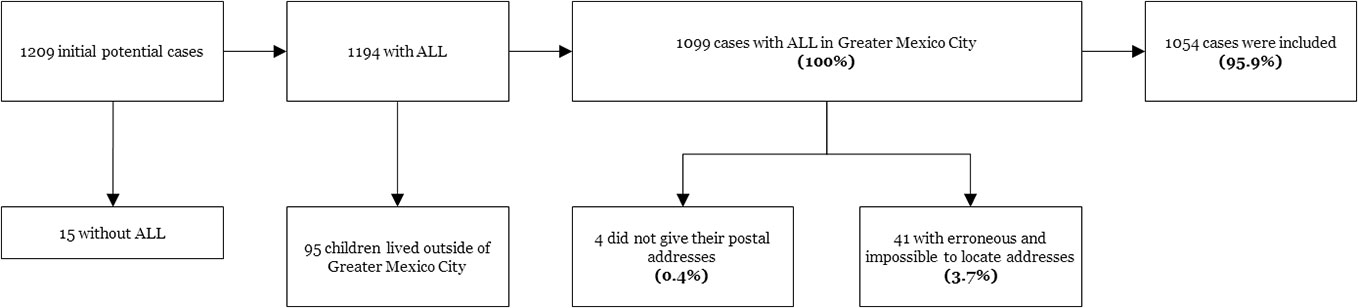
Figure 1 Geographic stratification of Greater Mexico City.
Several research studies have highlighted the potential associations between the exposure to environmental factors and the development of leukemia in the pediatric population of GMC. These factors include the exposure to extremely-low-frequency magnetic fields (ELF-MFs) (Juan C. 15, 16), the maternal and paternal ages at conception of the index child (17), a greater child´s birthweight (18), viral infections (19), father’s occupational exposure (20, 21), allergies (22), breastfeeding (J 23), and early-life infections (23). Additionally, the relationship between genetic and environment interactions has been explored. Particularly, for the exposure to fertilizers, insecticides, hydrocarbon derivatives and parental tobacco smoking (24).
The aim of the present study was to explore the geographical distribution of childhood ALL cases in GMC, a region characterized by a high incidence of the disease.
A population-based case-control study was conducted. Children <18 years old, newly diagnosed with ALL and GMC residents represented the group of cases. They were recruited from public hospitals where it has been estimated that 97.5% of children with leukemia from GMC are attended (25). Case registration required that trained personnel were assigned to each participating hospital to identify incident cases of leukemia through reviews of clinical charts. Afterwards, parents were approached and invited to participate. Given that careful case registration is essential for successful conduct of case-control studies, we followed the recommendations of the IARC for the planning and development of population-based cancer registries (26).
ALL diagnosis was established based on clinical features, and bone marrow aspirate findings, including cell morphology, immunophenotype, and genetics, as defined in 2008 by the World Health Organization (WHO) for the classification of lymphoid neoplasms.
The controls were selected from second-level hospitals of the same health institution that referred the children with ALL to the third-level care hospitals. The controls were children without leukemia who were treated at different hospital departments, such as ambulatory surgery, pediatrics, orthopedic outpatient clinics and the emergency room. Children with diagnoses of neoplasms, hematological diseases, allergies, infections, and congenital malformations were not selected as controls. A frequency-matched approach was used between cases and controls according to the following variables: child´s sex, age (at diagnosis for cases, and at the time of the interview for the controls) and health institution. Age was estimated in months, with a difference between cases and controls no greater than 12 months.
There were two different periods for the ascertainment of cases and controls: Cases (Period 1: January 1, 2006, to December 31, 2007; Period 2: January 1, 2010, to December 31, 2012); Controls (Period 1: January 1, 2000 to December 31, 2007; Period 2: January 1, 2010 to December 31, 2013).
Data collection was obtained by trained personnel through the revision of clinical charts and in-person interviews with the parents or guardians of the cases and controls (21) using a previously standardized questionnaire(J 23). The two periods for case ascertainment represent the complete years when sufficient financial support was available for conducting the interviews, clinical charts revisions and all the procedures required for the present research. Therefore, a representative sample of the incident cases with ALL diagnosed during those years in GMC was included. On the other hand, the control recruitment period started six years prior to the inclusion of cases and concluded one year after the end of the case ascertainment period. This allowed us for achieving a larger control pool for selecting the controls who had complete geolocation data and fulfilled the matching criteria.
Information recorded included: the postal addresses where the child lived the last year before the diagnosis (for cases) or at the moment of the interview (for controls). Additionally, random cross-checking telephone calls were performed by the supervisor of the personnel to ensure the accuracy of the information.
The street centroid was used for georeferencing the postal addresses, taking as the reference the intersection between the two closest streets where the child lived. Cartographic information was obtained through the country’s National Institute of Statistics and Geography (INEGI) information reported for 2010 (27) and by using Google Maps.
However, the information on postal addresses was partially obtained from the participants due to the following reasons: a) they felt distrustful, b) they did not know the postal address accurately, and c) they provided an address which differs from the officially recorded. In these situations, the neighborhood centroid strategy developed by Freire de Carvalho was followed (28).
When it was not possible to obtain the minimal information needed to geolocate or when the parents or guardians explicitly refused to provide their addresses, the individuals were excluded from the analysis.
Afterwards, Greater Mexico City was stratified into smaller spatial units: in order to differentiate between areas with different population density, the most urbanized part of the metropolis was classified as the urban area, whereas, the most external and least urbanized areas that are still quite rural were classified as rural–urban fringe area (see Figure 1), based on Duhau and Giglia (29). All the data were mapped and, to ensure the anonymity and confidentiality of the individuals participating in this work, none of the exhibited maps represent the children’s precise addresses so that they cannot be identified.
The spatial scan statistic proposed by Kulldorff (30, 31) using the SaTScan™ software was employed (Martin Kulldorff, Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, USA, https://www.satscan.org/). The probability model of Bernoulli was selected as it has been previously used in other studies on childhood leukemia (32, 33). Some of the advantages of this probability model are: 1) it is appropriate for detecting spatial clusters using case-control data (34); 2) it eliminates the disadvantage of studying areas with different population densities, as in Greater Mexico City; 3) it can control for covariates and 4) it controls for issues related to multiple testing (35). Inclusion of covariates allowed analysis of differences between urban and rural-urban fringe areas.
In addition, the method has been described as a scanning of the study area using a window of geometric exploration (36). This window is virtual and can take a circular or ellipsoidal geometric shape. Particularly, we chose for the circular shapes windows taking into account that the urban core of Greater Mexico City has the same length from north to south as from east to west. For each window location and size, the SaTScan calculates the number of observed and expected observations inside the window (37). Then, a relative risk (RR) was estimated for each childhood ALL cluster being the RR interpreted as the ratio of the probability of being within the cluster versus the risk of being outside the cluster. Additionally, the SaTScan Bernoulli model uses a log likelihood ratio test of the probability (LLR) which allows for identifying the main SC by selecting the circular window with the maximum LLR. To assess the precision and statistical significance of the findings, SaTScan simulates many random datasets to construct a distribution of geographic points that satisfies the assumptions of the null hypothesis (no clustering). The precision (p value) was assessed using 99999 simulations using the Monte Carlo hypothesis test. A p-value less than 0.05 was considered statistically significant.
In the present study, only the non-overlapping SCs with the largest LLRs, statistically significant (<0.05), with at least ten cases per cluster were reported. This last criterion was considered because few cases with ALL were included in the remaining detected SCs. This small number would hamper any epidemiological interpretation of findings as it represents less than 1% of the population of cases analyzed (n=1,054).
A total of 1209 cases with childhood ALL were diagnosed during the study period. Of these, 1054 (95.9%) cases fulfilled the selection criteria and were included in the study (see Figure 2). The predominant sex of cases was male, accounting for 53% (n=559). The cases were distributed across the following age groups: <1 year: 38 (3.6%); 1-4 years: 417 (39.5%); 5-9 years: 305 (28.9%); 10-14: 234 (22.2%) and 15-17 years: 60 (5.6%). According to the morphological features of the malignant cells, patients with ALL were classified as: L1 (n= 708; 67.2%); L2 (n= 329; 31.2%); and L3 (n= 17; 1.6%). No statistically significant differences were observed between cases and controls according to sex, age and health institution (see Table 1: Demographic and other characteristics of cases and controls included in the present study).
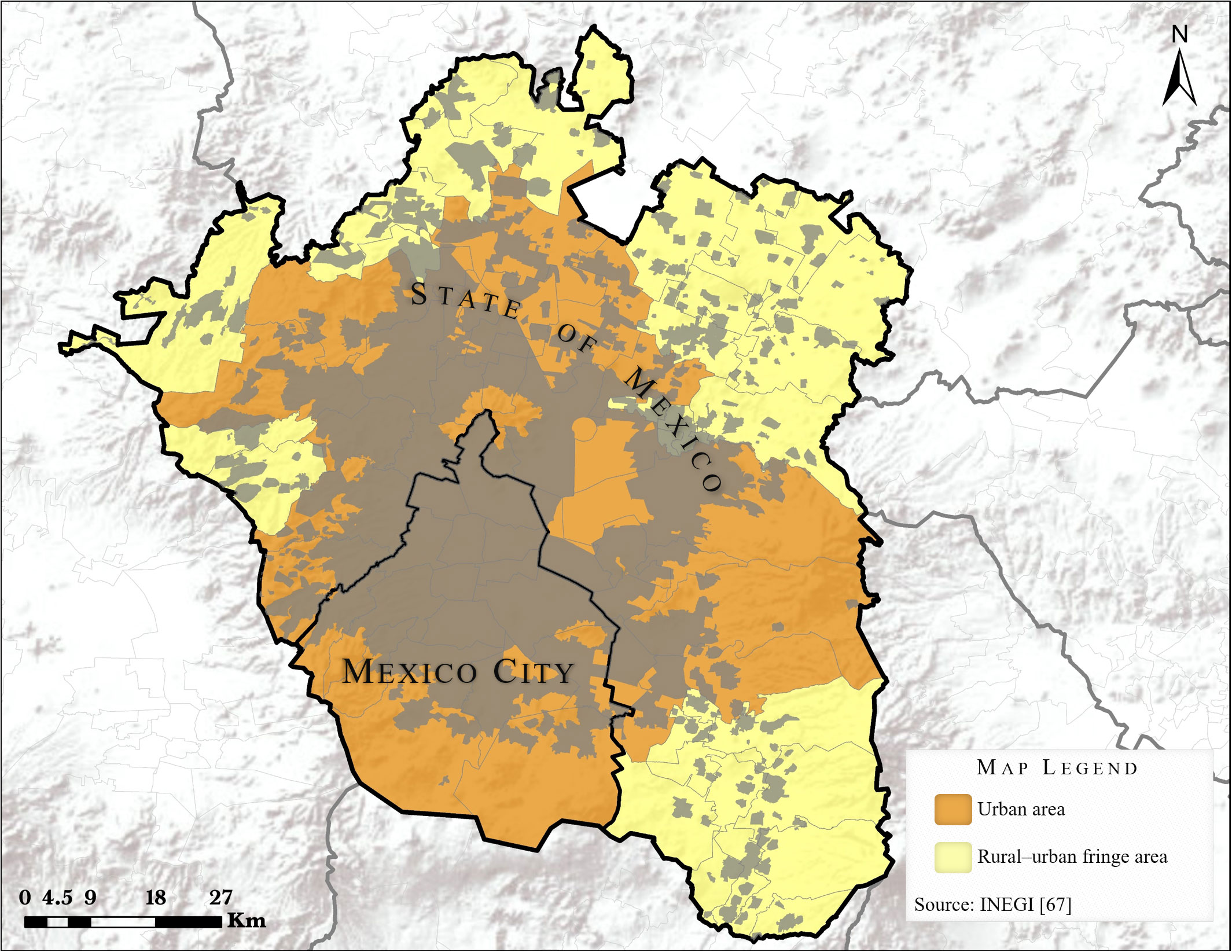
Figure 2 Selection of cases included in the study.
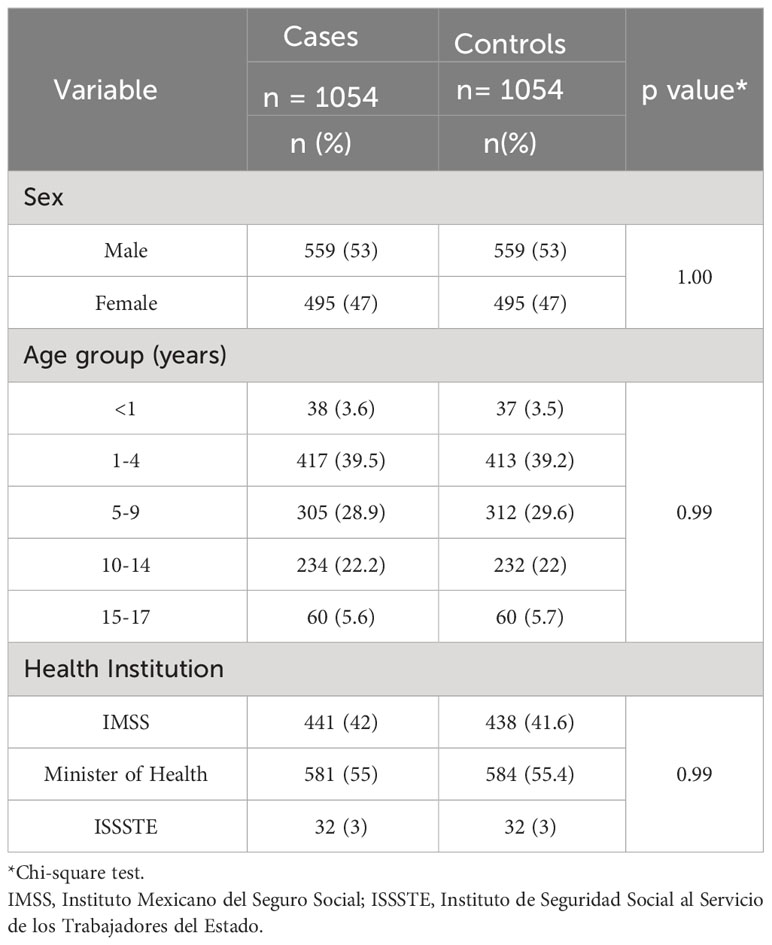
Table 1 Demographic and other characteristics of cases and controls included in the present study.
In the present research, eight SCs of cases with ALL were found in Greater Mexico City (see Figure 3). The sum of cases with ALL within the eight clusters represented 38.7% (n=408) of the total children included. The main cluster (SC #1) had an LLR=15,317.30, a RR=1.61 and a p-value <0.0001. It also included the largest number of cases (n=132) in comparison to the other clusters with a radius greater than 40 km. The other SCs included the following number of cases: #2 (n=91); #3 (n=69); #9 (n=48); #13 (n=29); #16 (n=11); #19 (n=14) and the cluster #21 included 14 cases. Similar LLRs, RRs, and p-values were noted for these SCs (see Supplementary Table 1: Characteristics of spatial clusters of children with ALL identified in Greater Mexico City). When differences were examined based on study areas, no significant distinctions were observed between urban and rural-urban fringe areas.
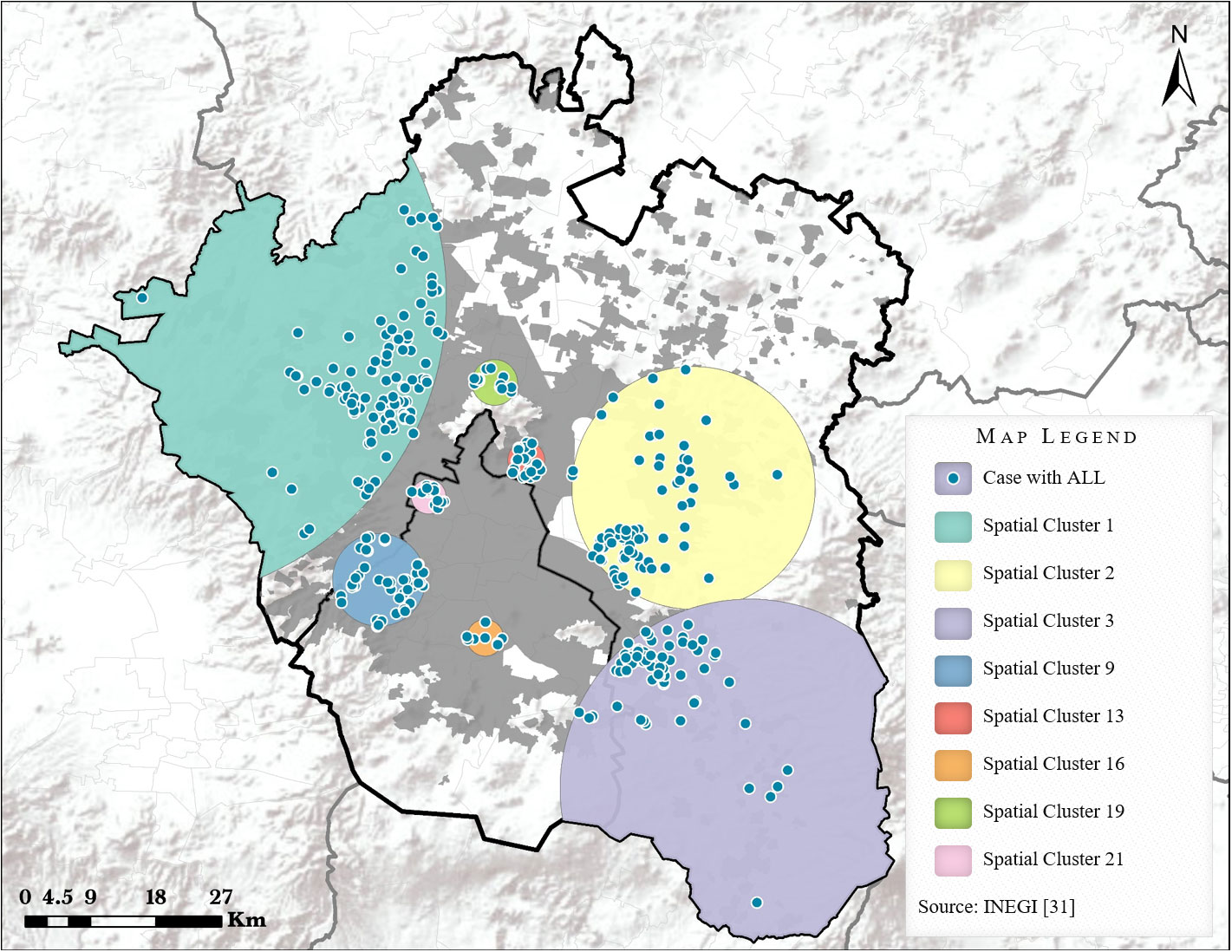
Figure 3 Spatial clusters of ALL cases in Greater Mexico City.
Notably, six out of eight SCs were closed to high−voltage electric lines and high−voltage electric installations (Figure 4). Furthermore, it was also noted that the remaining two SCs were in proximity to areas where former petrochemical industrial facilities had been located (closed a decade before the beginning of the present study). One of these facilities, was the former Azcapotzalco Refinery, and the other, was the San Juan Ixhuatepec petrochemical storage and distribution plant.
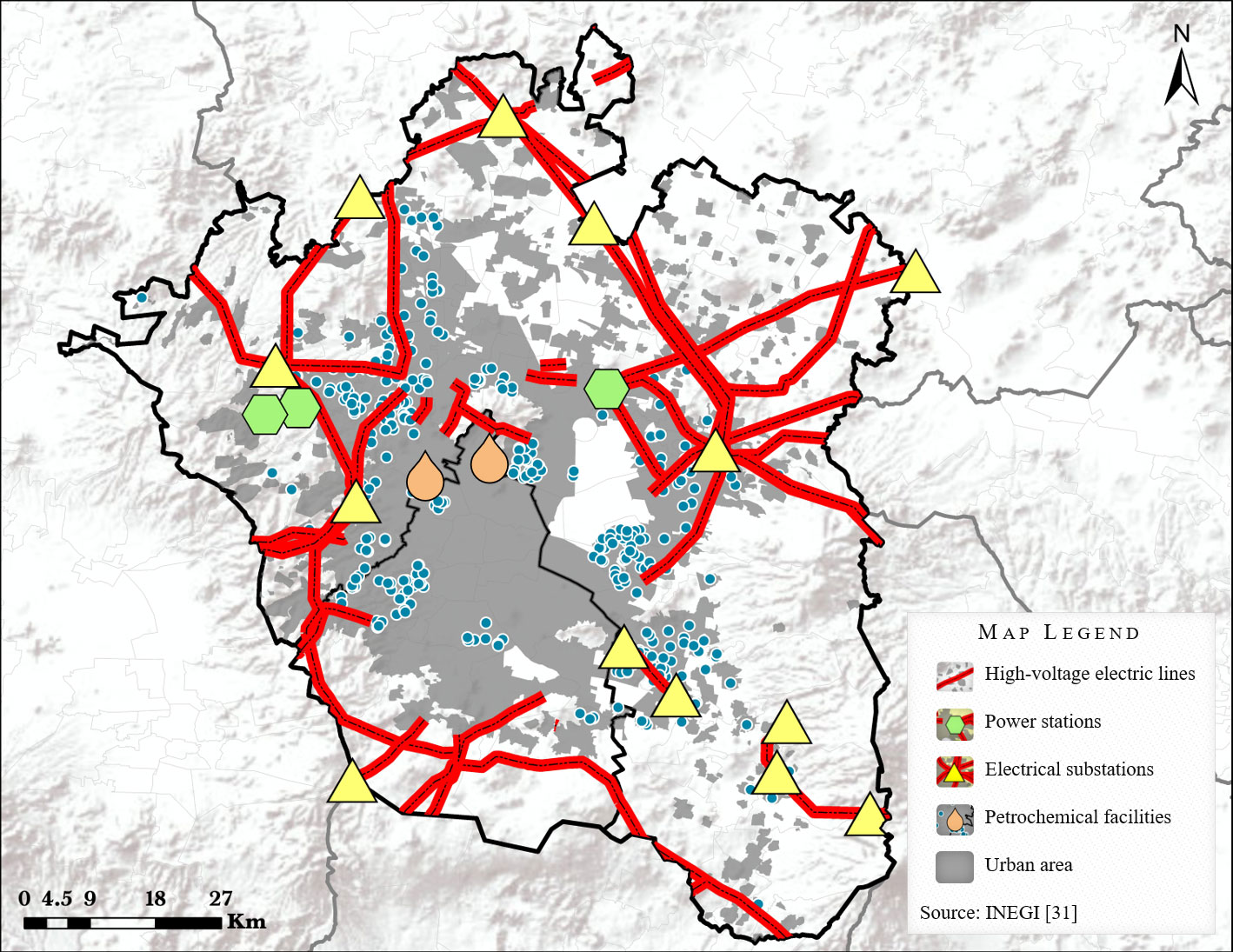
Figure 4 High-voltage electric and petrochemical installations in Greater Mexico City.
In this study, a heterogeneous spatial distribution of children with ALL living GMC was identified. Additionally, eight SCs of children with ALL in Greater Mexico City were detected using the Kulldorff’s spatial scan statistics.
To our knowledge, the present work is one of the few studies conducted in a city from a developing country aimed to investigate the spatial distribution of pediatric cases with ALL (38). The vast majority of these types of analyses have been carried out in populations from developed countries with larger and very affluent geographic areas―like European whole countries―(39–41). The disadvantages of studying greater geographical areas for identifying SCs have been explained (42). In addition, it has been suggested that the best scale of geographic analysis to identify SCs is the small-scale, or when the territory has a high population density, such as is the case of GMC (42–44).
The identification of significant SCs of childhood ALL cases in the present research supports to various hypotheses regarding risk factors potentially implicated in the development of this neoplasm. These hypotheses include the association with identifiable sources of exposure to harmful environmental agents (such as pesticides, insecticides, etc.), the possibility of an infectious etiology, among other factors (8, 9). We did not observe differences in the SCs distribution between urban and rural−urban fringe areas, as it has been reported in other investigations (14, 45–47). One possible reason for this negative result could be the minimal differences between the studied areas regarding factors such as: the population density, demographics, education, lifestyle, economic activities, transportation, day-to-day activity, among others. All these, as a consequence of the metropolitan system dynamics of GMC which tends to homogenize the distribution of these factors between regions. Therefore, it is likely that the differences between urban and rural−urban fringe areas were so small that they could not be detected by our methodological approach.
Interestingly, most of the SCs detected in the present study were closed to electrical installations whereas other SCs were in proximity to potential sources of hydrocarbons (former petrochemical facilities).
Firstly, the association between living near to high−voltage transmission lines and the risk of childhood AL has been explored in different populations (48, 49). The mechanisms that could explain this association are related with the exposure to the generated extremely-low-frequency magnetic fields (ELF-MFs) and the ionized particles of air produced by corona discharge (50) which has been suggested as a possible explanation of the high incidence rates of childhood AL in Mexico City (51).
Specifically, the association between ELF-MFs and the risk of childhood ALL development has been reported in different studies conducted in Mexico City using direct or indirect methods for assessing the exposure. Particularly, a high frequency of exposure to increased levels of ELF-MFs has been reported in our population. Moreover, an association between ELF-MFs and the risk of childhood AL has been identified in children from Mexico City, a finding that has also been reported in other populations (15, 16).
On the other hand, the relationship between exposure to derivatives from the petrochemical industrial activity and risk of childhood leukemia has also been documented (52–54). Notably, in a study conducted in Mexico City it was reported that the interaction between hydrocarbon exposure and genetic polymorphisms of NAT2 is associated with a high risk of developing childhood ALL. (24). However, these hypotheses require further study.
A possible limitation of the present investigation was the fact that a hospital-based recruitment of controls was followed instead of a random recruitment of controls from the source population, which has been recommended for this type of studies (55, 56). Nevertheless, if this last strategy had been implemented, it could have generated a low participation rate and a high cost, which exceeded our budget. Another limitation was produced by the difference in the periods of recruitment of cases and controls which restricted the analysis to a spatial clustering approach instead of a space-time cluster analysis that could have provided more insights about the effect of environmental factors occurring at specific times and places; an example of this would be the ability to detect patterns of childhood ALL incidence in relation to the date of birth of the children, or in relation to the time of diagnosis of the disease. On the other hand, exploring the geographic distribution of ALL cases among different age groups would be interesting, given the variation in disease incidence across age groups. However, the limited sample size hinders the feasibility of conducting a stratified analysis with sufficient statistical power. Additionally, it is important to continue the study of the geographical distribution of childhood ALL cases by analyzing updated geolocation data considering the persistently high incidence rates of this neoplasm in GMC. Lastly, we also reiterate the relevance of developing and/or consolidating cancer registries as the base to conduct studies for identifying SCs and risk factors associated with the development of ALL in the pediatric population.
The geographical distribution of childhood ALL cases in Greater Mexico City was heterogeneous across the territory of the metropolis. The identification of spatial clusters in certain regions of GMC suggest the possible role of environmental factors in the etiology of the disease. However, further investigations are required to elucidate the environmental hazards associated.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by National Scientific Research and Ethics Committee of the Mexican Institute of Social Security. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
DD-R: Formal analysis, Investigation, Writing – review & editing, Conceptualization, Methodology, Software, Visualization, Writing – original draft. JF-L: Formal analysis, Investigation, Data curation, Validation, Writing – original draft. RM: Formal analysis, Conceptualization, Methodology, Software, Supervision, Writing – review & editing. MP-S: Writing – review & editing, Data curation, Investigation, Resources. EJ-H: Investigation, Resources, Writing – review & editing. JM-T: Resources, Writing – review & editing. LE-H: Resources, Writing – review & editing. AM-S: Resources, Writing – review & editing. RP-A: Resources, Writing – review & editing. LM-P: Resources, Writing – review & editing. MV-A: Resources, Writing – review & editing. JT-N: Resources, Writing – review & editing. RE-E: Resources, Writing – review & editing. RA-S: Resources, Writing – review & editing. JD-H: Resources, Writing – review & editing. JM-G: Resources, Writing – review & editing. JG-U: Resources, Writing – review & editing. SM-S: Resources, Writing – review & editing. GE-A: Resources, Writing – review & editing. MP-B: Resources, Writing – review & editing. PS-L: Resources, Writing – review & editing. RL-G: Resources, Writing – review & editing. RR-C: Resources, Writing – review & editing. LH-M: Resources, Writing – review & editing. MS-A: Resources, Writing – review & editing. AL-L: Resources, Writing – review & editing. AG-E: Resources, Writing – review & editing. LG-L: Resources, Writing – review & editing. PS-L: Resources, Writing – review & editing. A-AÁ: . KM-R: Resources, Writing – review & editing. AC-E: Resources, Writing – review & editing. RR-J: Resources, Writing – review & editing. JC-C: Resources, Writing – review & editing. KS-L: Resources, Writing – review & editing. RC-C: Resources, Writing – review & editing. NL-S: Resources, Writing – review & editing. LF-V: Resources, Writing – review & editing. JP-G: Resources, Writing – review & editing. AG-Á: Resources, Writing – review & editing. MS-R: Resources, Writing – review & editing. RR-L: Resources, Writing – review & editing. LR-V: . FH-P: Resources, Writing – review & editing. JO-D: Resources, Writing – review & editing. LG-C: Resources, Writing – review & editing. MM-R: Resources, Writing – review & editing. OS-R: Resources, Writing – review & editing. VB-M: Resources, Writing – review & editing. SJ-M: Resources, Writing – review & editing. JM-Z: Resources, Writing – review & editing. HR-V: Resources, Writing – review & editing. EV: Resources, Writing – review & editing. JN-E: Resources, Writing – review & editing, Formal analysis, Investigation, Project administration. JM-A: Conceptualization, Funding acquisition, Investigation, Methodology, Writing – review & editing, Project administration, Supervision.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Consejo Nacional de Ciencia y Tecnología [grant numbers: SALUD-2010-1-141026, FIS/IMSS/PROT/895; PDCPN2013-01-215726, FIS/IMSS/PROT/1364; SALUD 2015-1-262190, FIS/IMSS/PROT/1533; CB-2015-1-258042, FIS/IMSS/PROT/1548] and FONCICYT/37/2018, FIS/IMSS/PROT/1782]; and by the Instituto Mexicano del Seguro Social [grant numbers: FIS/IMSS/PROT/PRIO/11/017, FIS/IMSS/PROT/G12/1134, FIS/IMSS/PROT/PRIO/14/031, FIS/IMSS/PROT/MD13/1254, FIS/IMSS/PROT/PRIO/15/048, FIS/IMSS/PROT/MD15/1504, FIS/IMSS/PROT/G15/1477, FIS/IMSS/PROT/PRIO/18/080 and FIS/IMSS/PROT/PRIO/19/088]. National Institutes of Health (Administrative Supplement 3R01CA262263 to JM-A, 2U24ES028524 sub-award number 00011320 to JM-A), and the Consejo Nacional de Humanidades, Ciencias y Tecnologías (CONAHCYT, CF-2023-G-1399 to JM-A; and the FORDECYT-PRONACES: 303019 to JN-E). The funders had no role in the study design, in the collection and analysis of data, in the writing of the report, and in the decision to submit the article for publication and to the Instituto Nacional de Medicina Genómica (INMEGEN) (2024-01) for the payment of the publication.
We would like to recognize Irma Angélica Morelos-Rodríguez for her invaluable help in mapping this paper. Also, to Hermes David Valdez-Quiroz for his important contributions to understand the geographic distribution of potential risk factors probably involved with the SCs detected in this work, particularly, the location of former petrochemical facilities in Greater Mexico City.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer IO declared a shared affiliation with the author RE-E to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1304633/full#supplementary-material
1. Mejía-Aranguré JM, Fajardo-Gutiérrez A, Bernáldez-Ríos R, Paredes-Aguilera R, Flores-Aguilar H, Martínez-García MC. Incidencia de Las Leucemias Agudas En Niños de la Ciudad de Mexico, de 1982 a 1991. Salud Pública Mexico (2000) 42(5):431–375.
2. Pérez-Saldivar MaríaL, Fajardo-Gutiérrez A, Bernáldez-Ríos R, Martínez-Avalos A, Medina-Sanson A, Espinosa-Hernández L, et al. Childhood acute leukemias are frequent in Mexico city: descriptive epidemiology. BMC Cancer (2011) 11(1):355. doi: 10.1186/1471-2407-11-355
3. Flores-Lujano J, Duarte-Rodríguez DAldebarán, Jiménez-Hernández E, Martín-Trejo JA, Allende-López A, Peñaloza-González JoséG, et al. Persistently high incidence rates of childhood acute leukemias from 2010 to 2017 in Mexico city: A population study from the MIGICCL. Front Public Health (2022) 10:918921/BIBTEX. doi: 10.3389/FPUBH.2022.918921/BIBTEX
4. Mejía-Aranguré JM. Model for the origin of acute leukemias in children: interaction of three factors—Susceptibility, exposure, and window of vulnerability. In: Mejía-Aranguré JM, editor. Etiology of Acute Leukemias in Children. Cham, Switzerland: Springer International Publishing (2016). p. 133–55. doi: 10.1007/978-3-319-05798-9_6
5. Bloom M, Maciaszek JL, Clark ME, Pui CH, Nichols KE. Recent advances in genetic predisposition to pediatric acute lymphoblastic leukemia. Expert Rev Hematol (2019) 13(1):55–705. doi: 10.1080/17474086.2020.1685866
6. Malard F, Mohty M. Acute lymphoblastic leukaemia. Lancet (2020) 395:1146–62. doi: 10.1016/S0140-6736(19)33018-1
7. Tebbi CK. Etiology of acute leukemia: A review. Cancers (2021) 13(9):2256. doi: 10.3390/CANCERS13092256
8. McNally RJQ, Eden TOB. An infectious aetiology for childhood acute leukaemia: A review of the evidence. Br J Haematology (2004) 127(3):243–635. doi: 10.1111/j.1365-2141.2004.05166.x
9. Mcnally RJQ, Parker L. Environmental factors and childhood acute leukemias and lymphomas. Leukemia Lymphoma (2006) 47(4):583–985. doi: 10.1080/10428190500420973
10. Duarte-Rodríguez DAldebarán, McNally RJQ, Núnãez-Enríquez JC, Fajardo-Gutiérrez A, Mejía-Arangure JM. Etiological research of childhood acute leukemia with cluster and clustering analysis. In: Mejía-Aranguré JM, editor. Clinical Epidemiology of Acute Lymphoblastic Leukemia - From the Molecules to the Clinic. Rijeka: InTech (2013). p. 115–44. doi: 10.5772/54456
11. Tlacuilo-Parra A, Garibaldi-Covarrubias R, Romo-Rubio H, Soto-Sumuano L, Ruiz-Chávez CF, Suárez-Arredondo M, et al. Geographical distribution and cluster detection of childhood leukemia in the metropolitan area of guadalajara, Mexico. Rev Investigación Clínica (2017) 69(3):159–65. doi: 10.24875/RIC.17002131
12. Petridou E, Alexander FE, Trichopoulos D, Revinthi K, Dessypris N, Wray N, et al. Aggregation of childhood leukemia in geographic areas of Greece. Cancer Causes Control (1997) 8(2):239–45. doi: 10.1023/A:1018480515690
13. Bastos LídiaNV, Silveira JoséC, Luna CF, Lucena-Silva N. Childhood and adolescent cancer in the state of pernambuco, Brazil: incidence, geographical distribution, and association with environmental health indicators. J Pediatr Hematology/Oncology (2018) 40(1):7–145. doi: 10.1097/MPH.0000000000001017
14. González-García H, Garrote-Molpeceres R, Urbaneja-Rodríguez E, Gutiérrez-Meléndez P, Herráiz-Cristóbal R, Pino-Vázquez MaríaAsunción, et al. Differences in incidence and survival to childhood cancer between rural and urban areas in castilla y león, Spain, (2003–2014). Medicine (2018) 97(41):e12797. doi: 10.1097/MD.0000000000012797
15. Mejia-Arangure JM, Fajardo-Gutierrez A, Perez-Saldivar ML, Gorodezky C, Martinez-Avalos A, Romero-Guzman L, et al. Magnetic fields and acute leukemia in children with down syndrome. Epidemiol (Cambridge Mass.) (2007) 18(1):158–615. doi: 10.1097/01.ede.0000248186.31452.be
16. Núñez-Enríquez JC, Correa-Correa Víctor, Flores-Lujano J, Pérez-Saldivar MaríaL, Jiménez-Hernández E, Martín-Trejo JA, et al. Extremely low-frequency magnetic fields and the risk of childhood B-lineage acute lymphoblastic leukemia in a city with high incidence of leukemia and elevated exposure to ELF magnetic fields. Bioelectromagnetics (2020) 41(8):581–97. doi: 10.1002/bem.22295
17. Jiménez-Hernández E, Duarte-Rodríguez DAldebarán, Núñez-Enriquez JC, Flores-Lujano J, Martín-Trejo JA, Espinoza-Hernández LE, et al. Maternal and paternal ages at conception of index child and risk of childhood acute leukaemia: A multicentre case-control study in greater Mexico city. Cancer Epidemiol (2020) 67:101731. doi: 10.1016/j.canep.2020.101731
18. Jiménez-Hernández E, Fajardo-Gutiérrez A, Núñez-Enriquez JC, Martín-Trejo JA, Espinoza-Hernández LE, Flores-Lujano J, et al. A greater birthweight increases the risk of acute leukemias in mexican children-experience from the mexican interinstitutional group for the identification of the causes of childhood leukemia (MIGICCL). Cancer Med (2018) 7:9. doi: 10.1002/cam4.1414
19. Arellano-Galindo José, Barrera AP, Jiménez-Hernández E, Zavala-Vega S, Campos-Valdéz G, Xicohtencatl-Cortes J, et al. Infectious agents in childhood leukemia. Arch Med Res (2017) 48(4):305–13. doi: 10.1016/j.arcmed.2017.09.001
20. Perez-Saldivar ML, Ortega-Alvarez MC, Fajardo-Gutierrez A, Bernaldez-Rios R, Del Campo-Martinez MdeLA, Medina-Sanson A, et al. Father’s occupational exposure to carcinogenic agents and childhood acute leukemia: A new method to assess exposure (a case-control study). BMC Cancer 8 (January) (2008) 7. doi: 10.1186/1471-2407-8-7
21. Pérez-Saldivar MaríaL, Fajardo-Gutiérrez A, Sierra-Ramírez JoséA, Núñez-Villegas N, Pérez-Lorenzana Héctor, Dorantes-Acosta EMaría, et al. Parental exposure to workplace carcinogens and the risk of development of acute leukemia in infants. Case-control study. Arch Med Res (2016) 47(8):684–93. doi: 10.1016/j.arcmed.2016.12.006
22. Núñez-Enríquez JC, Fajardo-Gutiérrez A, Buchán-Durán EP, Bernáldez-Ríos R, Medina-Sansón A, Jiménez-Hernández E, et al. Allergy and acute leukaemia in children with down syndrome: A population study. Report from the mexican inter-institutional group for the identification of the causes of childhood leukaemia. Br J Cancer (2013) 108(11):2334–38. doi: 10.1038/bjc.2013.237
23. Flores-Lujano J, Perez-Saldivar ML, Fuentes-Pananá EM, Gorodezky C, Bernaldez-Rios R, Del Campo-Martinez MA, et al. Breastfeeding and early infection in the aetiology of childhood leukaemia in down syndrome. Br J Cancer (2009) 101(5):860–64. doi: 10.1038/sj.bjc.6605244
24. Medina-Sanson A, Núñez-Enríquez JC, Hurtado-Cordova E, Pérez-Saldivar MaríaL, Martínez-García A, Jiménez-Hernández E, et al. Genotype-environment interaction analysis of NQO1, CYP2E1, and NAT2 polymorphisms and the risk of childhood acute lymphoblastic leukemia: A report from the mexican interinstitutional group for the identification of the causes of childhood leukemia. Front Oncol (2020) 10:571869. doi: 10.3389/FONC.2020.571869
25. Fajardo-Gutiérrez A, Sandoval-Mex AidéMaría, Mejía-Aranguré JM, Rendón-Macías ME, Martínez-García MaríadC. Clinical and social factors that affect the time to diagnosis of mexican children with cancer. Med Pediatr Oncol (2002) 39(1):25–315. doi: 10.1002/mpo.10100
26. Bray F, Znaor A, Cueva P, Korir A, Swaminathan R, Ullrich A, Wang SA, Parkin DM, et al. Planning and developing population-based cancer registration in low- or middle-income settings. In: (IARC Technical Report, No. 43.) Chapter 3, Planning and developing a population-based cancer registry. Lyon (FR: International Agency for Research on Cancer (2014). Available at: https://www.ncbi.nlm.nih.gov/books/NBK566951.
27. INEGI. Proyecto Básico de Información 2010. In: Mapa Digital de Mexico. Mexico: Instituto Nacional de Estadística, Geografía e Informática (2010). Available at: https://www.inegi.org.mx/img/ico/ico_zip.png.
28. Freire de Carvalho MH. The Spatial and Environmental Predictors of Adult Mortality in the Northern Mexico Border Region. The University of Michigan (2009).
29. Duhau E, Giglia Ángela. Las Reglas Del Desorden: Habitar La Metrópoli. Ciudad de Mexico: UAM-AZC (2008). Siglo XXI.
30. Kulldorff M, Nagarwalla N. Spatial disease clusters: detection and inference. Stat Med (1995) 14(8):799–8105. doi: 10.1002/sim.4780140809
31. Kulldorff M. A spatial scan statistic. Commun Stat - Theory Methods (1997) 26(6):1481–96. doi: 10.1080/03610929708831995
32. Hjalmars U, Kulldorff M, Gustafsson G, Nagarwalla N. Childhood leukaemia in Sweden: using GIS and a spatial scan statistic for cluster detection. Stat Med (1996) 15(7–9):707–15. doi: 10.1002/(SICI)1097-0258(19960415)15:7/9<707::AID-SIM242>3.0.CO;2-4
33. Wheeler DC. A comparison of spatial clustering and cluster detection techniques for childhood leukemia incidence in ohio 1996-2003. Int J Health Geographics (2007) 6(13):13. doi: 10.1186/1476-072X-6-13
34. Jung I, Kulldorff M, Richard OJ. A spatial scan statistic for multinomial data. Stat Med (2010) 29(18):1910–185. doi: 10.1002/sim.3951
35. Kulldorff M, Huang L, Pickle L, Duczmal L. An elliptic spatial scan statistic. Stat Med (2006) 25(22):3929–435. doi: 10.1002/sim.2490
36. Duczmal L, Duarte AR, Tavares R. Extensions of the scan statistic for the detection and inference of spatial clusters. In: Glaz J, Pozdnyakov V, Wallenstein S, editors. Scan Statistics: Methods and Applications. Statistics for Industry and Technology. Boston: Birkhäuser Boston (2009). p. 153–77. doi: 10.1007/978-0-8176-4749-0_7
37. Warden CR. Comparison of Poisson and Bernoulli spatial cluster analyses of pediatric injuries in a fire district. Int J Health Geogr (2008) 7:51. doi: 10.1186/1476-072X-7-51
38. Kaatsch P, Mergenthaler A. Incidence, time trends and regional variation of childhood leukaemia in Germany and Europe. Radiat Prot Dosimetry (2008) 132(2):107–35. doi: 10.1093/rpd/ncn259
39. Bellec S, Hémon D, Rudant J, Goubin A, Clavel J. Spatial and space-time clustering of childhood acute leukaemia in France from 1990 to 2000: A nationwide study. Br J Cancer (2006) 94(5):763–70. doi: 10.1038/sj.bjc.6602980
40. Schmiedel S, Blettner M, Kaatsch P, Schüz J. Spatial clustering and space–time clusters of leukemia among children in Germany 1987–2007. Eur J Epidemiol (2010) 25(9):627–335. doi: 10.1007/s10654-010-9488-7
41. McNally RJQ, Stiller C, Vincent TJ, Murphy MFG. Cross-space-time clustering of childhood cancer in great britain: evidence for a common aetiology. Int J Cancer (2014) 134(1):136–435. doi: 10.1002/ijc.28332
42. Kulkarni K, Stobart K, Witol A, Rosychuk RJ. Leukemia and lymphoma incidence in children in alberta, Canada: A population-based 22-year retrospective study. Pediatr Hematol Oncol (2011) 28(8):649–05. doi: 10.3109/08880018.2011.613091
43. Alexander FE, Boyle P, Carli PM, Coebergh JW, Draper GJ, Ekbom A, et al. Spatial clustering of childhood leukaemia: summary results from the EUROCLUS project. Br J Cancer (1998) 77(5):818–24. doi: 10.1038/bjc.1998.133
44. Goujon-Bellec Stéphanie, Demoury C, Guyot-Goubin Aurélie, Hémon D, Clavel J. Detection of clusters of a rare disease over a large territory: performance of cluster detection methods. Int J Health Geographics (2011) 10(1):535. doi: 10.1186/1476-072X-10-53
45. Rajabli N, Naeimi-Tabeie M, Jahangirrad A, Sedaghat SM, Semnani S, Roshandel G. Epidemiology of leukemia and multiple myeloma in golestan, Iran. Asian Pacific J Cancer Prev (2013) 14(4):2333–365. doi: 10.7314/APJCP.2013.14.4.2333
46. Malagoli C, Malavolti M, Costanzini S, Fabbi S, Teggi S, Palazzi G, et al. Increased incidence of childhood leukemia in urban areas: A population-based case-control study. Epidemiologia e Prevenzione (2017) 39(4 Suppl. 1):102–7.
47. Sun K, Zheng R, Zhang S, Zeng H, Wang S, Chen Ru, et al. Patterns and trends of cancer incidence in children and adolescents in China 2011–2015: A population-based cancer registry study. Cancer Med (2021) 10(13):4575–865. doi: 10.1002/CAM4.4014
48. Feizi AAHP, Arabi MAAA. Acute childhood leukemias and exposure to magnetic fields generated by high voltage overhead power lines - a risk factor in Iran. Asian Pacific J Cancer Prevention: APJCP (2007) 8(1):69–725.
49. Sohrabi M-R, Tarjoman T, Abadi A, Yavari P. Living near overhead high voltage transmission power lines as a risk factor for childhood acute lymphoblastic leukemia: A case-control study. Asian Pacific J Cancer Prevention: APJCP (2010) 11(2):423–275.
50. Lowenthal RM, Tuck DM, Bray IC. Residential exposure to electric power transmission lines and risk of lymphoproliferative and myeloproliferative disorders: A case-control study. Internal Med J (2007) 37(9):614–19. doi: 10.1111/j.1445-5994.2007.01389.x
51. Sidaway GH. Powerline bioactivity - more than magnetism. SpringerPlus (2013) 2:454. doi: 10.1186/2193-1801-2-454
52. Yu C-LL, Wang S-FF, Pan P-CC, Wu M-TT, Ho C-KK, Smith TJ, et al. Residential exposure to petrochemicals and the risk of leukemia: using geographic information system tools to estimate individual-level residential exposure. Am J Epidemiol (2006) 164(3):200–2075. doi: 10.1093/aje/kwj182
53. Weng H-H, Tsai S-S, Chiu H-F, Wu T-N, Yang C-Y. Association of childhood leukemia with residential exposure to petrochemical air pollution in Taiwan. Inhalation Toxicol (2008) 20(1):31–365. doi: 10.1080/08958370701758734
54. Kirkeleit J, Riise T, Bjørge T, Christiani DC, Bråtveit M, Baccarelli A, et al. Maternal exposure to gasoline and exhaust increases the risk of childhood leukaemia in offspring – a prospective study in the norwegian mother and child cohort study. Br J Cancer (2018) 119(8):1028–355. doi: 10.1038/s41416-018-0295-3
55. Kreis C, Grotzer M, Hengartner H, Spycher BD, Swiss Paediatric Oncology Group, the Swiss National Cohort Study Group, et al. Space-time clustering of childhood cancers in Switzerland: A nationwide study. Int J Cancer (2016) 138(9):2127–35. doi: 10.1002/ijc.29955
Keywords: leukemia, child, spatial clustering, SaTScan software to analyze spatial, electromagnetic fields, environmental exposure, urban population, developing countries
Citation: Duarte-Rodríguez DA, Flores-Lujano J, McNally RJQ, Pérez-Saldivar ML, Jiménez-Hernández E, Martín-Trejo JA, Espinoza-Hernández LE, Medina-Sanson A, Paredes-Aguilera R, Merino-Pasaye LE, Velázquez-Aviña MM, Torres-Nava JR, Espinosa-Elizondo RM, Amador-Sánchez R, Dosta-Herrera JJ, Mondragón-García JA, González-Ulibarri JE, Martínez-Silva SI, Espinoza-Anrubio G, Paz-Bribiesca MM, Salcedo-Lozada P, Landa-García RÁ, Ramírez-Colorado R, Hernández-Mora L, Santamaría-Ascencio M, López-Loyola A, Godoy-Esquivel AH, García-López LR, Anguiano-Ávalos AI, Mora-Rico K, Castañeda-Echevarría A, Rodríguez-Jiménez R, Cibrian-Cruz JA, Solís-Labastida KA, Cárdenas-Cardos R, López-Santiago N, Flores-Villegas LV, Peñaloza-González JG, González-Ávila AI, Sánchez-Ruiz M, Rivera-Luna R, Rodríguez-Villalobos LR, Hernández-Pérez F, Olvera-Durán JÁ, García-Cortés LR, Mata-Rocha M, Sepúlveda-Robles OA, Bekker-Méndez VC, Jiménez-Morales S, Meléndez-Zajgla J, Rosas-Vargas H, Vega E, Núñez-Enríquez JC and Mejía-Aranguré JM (2024) Evidence of spatial clustering of childhood acute lymphoblastic leukemia cases in Greater Mexico City: report from the Mexican Inter-Institutional Group for the identification of the causes of childhood leukemia. Front. Oncol. 14:1304633. doi: 10.3389/fonc.2024.1304633
Received: 29 September 2023; Accepted: 11 January 2024;
Published: 14 February 2024.
Edited by:
Hajo Zeeb, Leibniz Institute for Prevention Research and Epidemiology (LG), GermanyReviewed by:
Irma Olarte, Hospital General de Mexico Dr. Eduardo Liceaga, MexicoCopyright © 2024 Duarte-Rodríguez, Flores-Lujano, McNally, Pérez-Saldivar, Jiménez-Hernández, Martín-Trejo, Espinoza-Hernández, Medina-Sanson, Paredes-Aguilera, Merino-Pasaye, Velázquez-Aviña, Torres-Nava, Espinosa-Elizondo, Amador-Sánchez, Dosta-Herrera, Mondragón-García, González-Ulibarri, Martínez-Silva, Espinoza-Anrubio, Paz-Bribiesca, Salcedo-Lozada, Landa-García, Ramírez-Colorado, Hernández-Mora, Santamaría-Ascencio, López-Loyola, Godoy-Esquivel, García-López, Anguiano-Ávalos, Mora-Rico, Castañeda-Echevarría, Rodríguez-Jiménez, Cibrian-Cruz, Solís-Labastida, Cárdenas-Cardos, López-Santiago, Flores-Villegas, Peñaloza-González, González-Ávila, Sánchez-Ruiz, Rivera-Luna, Rodríguez-Villalobos, Hernández-Pérez, Olvera-Durán, García-Cortés, Mata-Rocha, Sepúlveda-Robles, Bekker-Méndez, Jiménez-Morales, Meléndez-Zajgla, Rosas-Vargas, Vega, Núñez-Enríquez and Mejía-Aranguré. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Manuel Mejía-Aranguré, am1lamlhQGlubWVnZW4uZ29iLm14; YXJhbmd1cmVqbUBnbWFpbC5jb20=; anVhbi5tZWppYWFAY29tdW5pZGFkLnVuYW0ubXg=; Juan Carlos Núñez-Enríquez, anVhbi5udW5lemVAaW1zcy5nb2IubXg=; amNhcmxvc19udUBob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.