 Lukas Käsmann
Lukas Käsmann Esra Degerli1
Esra Degerli1 Karim El-Marouk
Karim El-Marouk
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol. , 19 March 2024
Sec. Cancer Imaging and Image-directed Interventions
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1226422
This article is part of the Research Topic Imaging-Based Methodologies for Evaluating Drugs in Clinical Trials View all 3 articles
Durvalumab after chemotherapy in non-operable stage III non-small cell lung cancer (NSCLC) is the standard of care worldwide. We present a patient with the incidental discovery of a unilateral MALT lymphoma of the adrenal gland and adrenalitis during durvalumab maintenance treatment detected by 18F-FDG-PET/CT. We assessed the clinical and histopathological findings, radiological examinations and overall treatment. Our work emphasizes the significance of considering other differential diagnoses and the importance of multidisciplinary treatment of the findings, especially within clinical trials.
Immunotherapy plays a vital role in the treatment of lung cancer today. However, in some cases, immunotherapy-related adverse events (irAEs) develop during this therapy. They can be diagnosed in positron emission tomography–computed tomography (PET/CT) and may occur in every organ system, such as skin, gastrointestinal tract, endocrine system, respiratory system (1). Adverse events during immunotherapy do not always have to be related to it. Our patient had both irAE and MALT lymphoma of the adrenal gland, which was not likely caused by the therapy.
MALT lymphoma is a subtype of non-Hodgkin lymphoma and usually manifests extranodal in the gastrointestinal tract (2) but can also occur in other organ systems (3), for example the adrenal gland (4, 5). However, misdiagnosis may occur due to the low incidence (6). The adrenal gland is a common site for metastasis from lung cancer and enlargement of the adrenal gland can be misinterpreted as a metastasis (7, 8). Some possible differential diagnoses of an adrenal mass include adenoma, myelolipoma, cyst, lipoma, pheochromocytoma, primary adrenal cancer, hyperplasia, and tuberculosis (9).
We present a patient with the incidental discovery of a unilateral MALT lymphoma of the adrenal gland and adrenalitis during immunotherapy with durvalumab after chemoradiotherapy (CRT) in stage III non-small cell lung cancer (NSCLC) detected by 18F-FDG-PET/CT. We assessed the clinical as well as intraoperative findings, radiological examinations, and overall treatment.
We present the case of a 67-year-old Caucasian female patient who was referred to our department in May 2021 (Figure 1). The patient initially presented with progressive dyspnea and cough. A subsequent computed tomography (CT) scan revealed a suspicious malignant mass in the upper lobe of the right lung and was clinically diagnosed as locally advanced NSCLC. Histological evaluation and next-generation sequencing revealed a large cell neuroendocrine lung carcinoma (LCNEC) with S37C mutation in the CTNNB1 gene, E542 mutation in the PIK3CA gene, and inactivating mutation in the TP53 gene. Nuclear staining for Ki-67 was performed using anti-Ki67 antibody (MIB-1, 1:100, Dako). Ki-67 expression was scored as 50% evaluated semiquantitatively as a percentage of positive cells upon manual counting of 500 to 1,000 tumor cells. For the detection of programmed death-ligand 1 (PD-L1), prediluted PD-L1 rabbit monoclonal antibody (SP263; Ventana Medical Systems, Oro Valley, Arizona) was used and measured as 5% using the tumor proportion score (TPS). Both stainings were performed on a Ventana Benchmark Ultra autostainer using the ultraView diaminobenzidine kit (Ventana Medical Systems, Oro Valley, AZ).
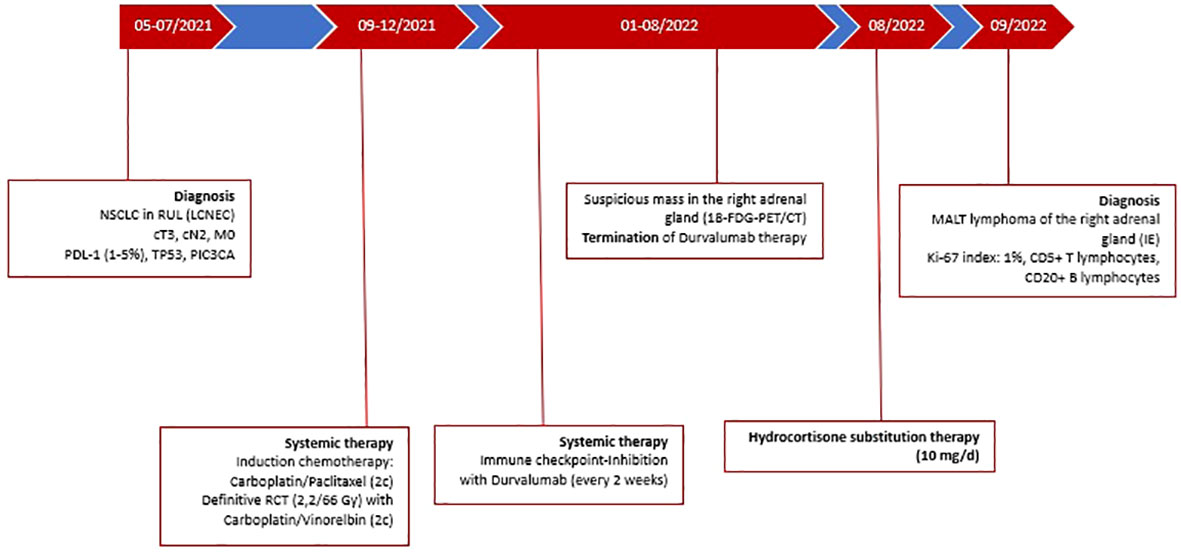
Figure 1 Timeline of patients’ treatment and follow-up.
Initial positron emission tomography/computed tomography (18-FDG-PET/CT) staging and cranial magnetic resonance imaging (cMRI) in July/August 2021 showed metastases in the hilar lymph nodes on the right side, which resulted in stage IIIB (cT3, cN2, M0) according to UICC TNM staging (8th edition) (10).
Relevant medical history findings included active smoking (50 p/y), breast cancer (diagnosed in 2006, non-active), peripheral arterial disease, and chemotherapy-associated pancytopenia CTCAE II.
Beginning in September 2021, our patient underwent induction chemotherapy with two cycles of carboplatin (AUC5) and paclitaxel (150 mg/m²). After local response, concurrent CRT (30 fractions × 2.2 Gy/66 Gy) with two cycles of concurrent platinum-based chemotherapy was administered. The patient received carboplatin (AUC5 i.v.) on day 1 of each cycle and 25 mg/m2 vinorelbine i.v. on day 1 and day 8 of each cycle.
The patient was treated with immunotherapy with PD-L1 antibody durvalumab according to the phase III PACIFIC trial (NCT02125461) (11) starting in January 2022. Immunotherapy was given every 2 weeks. During durvalumab therapy, the patient’s general condition deteriorated in August 2022 with a diagnosis of Addison’s disease due to CTCAE grade II autoimmune adrenalitis, which was potentially immune-mediated. This led to the discontinuation of durvalumab therapy.
A further 18F-FDG PET/CT scan revealed increased metabolic activity in the right adrenal gland (SUVmax: 6.7) with suspicion of possible metastasis. After multidisciplinary discussions, a laparoscopic adrenalectomy was performed in August 2022. Histological examination of the resected soft tissue (5.5 × 4.3 × 0.4 cm) revealed an enlarged adrenal gland with a maximum diameter of 3.3 cm. In fact, the patient had histomorphologically highly atypical adrenal tissue; the medullary zone was distinguishable, and the adrenal cortex tissue was completely depleted. Using conventional light microscopy, there were neither cells of the zona glomerulosa, nor zona fasciculata or zona reticularis. Instead, immunohistological evaluation showed a band-like lympho-plasmacytoid infiltration/inflammation with a dominant diffuse and focally nodular infiltration of CD5-positive T-lymphocytes and partially grouped CD20-positive B-lymphocytes. Numerous CD38-positive plasma cells were detected with a dominance of lambda over kappa-positive plasma cells. Further molecular pathological examination detected a clonality of the IgH gene but no mutation in the MyD88 gene. In summary, an indolent non-Hodgkin’s lymphoma of the B-cell lineage was found in the right adrenal gland, suggesting a MALT lymphoma. Further endoscopic diagnostic by bioptic securing showed no evidence of other manifestations of the MALT-Lymphoma (e.g., gastrointestinal tract). A bone marrow puncture was rejected by the patient.
In close cooperation with our endocrinology department, a substitution therapy with Hydrocortisone 10 mg/day was initiated. Continuation of the immunotherapy with durvalumab was not planned according to the decision of the tumor board. However, adjuvant therapy for the MALT-Lymphoma was not indicated. A follow-up 18F-FDG-PET/CT performed in January 2023 showed a stable disease situation with no local progression of the NSCLC, no metastatic lesions, and no increased metabolism indicating a possible local recurrence in the field of the resected adrenal gland.
This case report demonstrates the importance of histological evaluation and differential diagnoses, especially in patients with complex patient history.
Immunotherapy, particularly the use of checkpoint inhibitors (ICIs), has revolutionized treatment of NSCLC in recent years (12). While ICIs have shown remarkable efficacy in some patients, they can also lead to irAEs, which can range from mild to severe and life-threatening (13). IrAEs can affect any organ system and can present with a wide range of symptoms, including skin rash, colitis, hepatitis, pneumonitis, and endocrinopathies (14–16). The incidence and severity of irAEs depend on the type of ICIs, the dose, and the duration of treatment (17).
The meta-analysis by Wang et al. evaluated 46 trials with a total of 12,808 patients treated with PD-1/PD-L1 inhibitors. In this analysis, the patients received treatment with nivolumab (21 studies, 45.65%), pembrolizumab (17 studies, 36.96%), atezolizumab (5 studies, 10.87%), durvalumab (one study, 2.17%), and avelumab (one study, 2.17%). On average, the incidence of irAE of any grade was 32.92% in every organ system. the following specific incidences of irAEs were determined after subdividing into the individual organ systems: skin (13%), gastrointestinal tract (10%–13%), respiratory system (3%), endocrine system (≤2%), liver (≤2%), and kidney (<1%) (1).
Early diagnosis and management of irAEs are crucial for improving patient outcomes (18). One diagnostic tool that has shown promise in detecting irAEs is 18F-FDG-PET/CT (19), which differentiates them from other disease processes such as infection or cancer progression (20).
In addition to detecting irAEs, 18F-FDG-PET/CT can also be used to predict the development of irAEs. A study by Nobashi et al. evaluated the use of 18F-FDG-PET/CT in predicting the possible outcomes of irAE in patients receiving ICIs. The study included 40 patients who underwent 18F-FDG-PET/CT before and after the ICI therapy. Patients with irAE that could be detected by 18F-FDG-PET/CT were significantly associated with a favorable long-term outcome (P = 0.002) (21).
In conclusion, 18F-FDG-PET/CT is a promising tool for the diagnosis and monitoring of irAEs in patients undergoing immunotherapy. While further research is needed to fully evaluate the utility of 18F-FDG-PET/CT in this context, existing studies suggest that 18F-FDG-PET/CT can provide valuable information for the early detection and management of irAEs.
18F-FDG-PET/CT is also a well-established imaging method for detecting, staging, and monitoring various cancer entities. The accuracy of 18F-FDG-PET/CT in cancer patients depends on several factors, such as the tumor size, location, type, and stage of disease. In recent studies, 18F-FDG-PET/CT has demonstrated good sensitivity and specificity for detecting different types of primary cancer and distant metastasis, including lung cancer and adrenal masses. A meta-analysis about the diagnostic accuracy of 18F-FDG-PET/CT for the characterization of adrenal masses performed by Kim et al. showed in 29 studies with 2,421 patients in total a sensitivity of 91% [95% CI (0.88–0.94)] and specificity of 91% [95% CI (0.87–0.93)] (22).
Ma et al. displayed that SUVmax of malignant lesions (10.0 ± 5.8) was higher than that of benign lesions (5.4 ± 5.3, P < 0.05), and as a result of this finding, the SUV-ROC method has a sensitivity of 81.25% and specificity of 72.91% (23). Another study by Perry et al. demonstrated a higher sensitive accuracy of 18F-FDG-PET/CT in detection of non-gastric MALT-Lymphoma versus gastric MALT-Lymphoma (75% vs. 38.9%) (24). Despite its limitations, 18F-FDG PET/CT remains a respected method for diagnosing and monitoring suspicious tumors of the adrenal gland.
In our patient, the increased metabolic activity in the right adrenal gland seen on 18F-FDG-PET/CT raised suspicion of an adrenal metastasis of NSCLC. However, histologic examination revealed a MALT lymphoma. This emphasizes the importance of histological examination of suspected metastases. A systematic review of adrenal biopsy by Bancos et al. using 32 studies found that adrenal biopsy had a sensitivity of 87% [95% CI (0.78–0.93)] and a specificity of 100% [95% CI (0.7–1.00)] for the overall diagnosis of malignancy. For the diagnosis of metastases, the sensitivity was 87% [95% CI (0.74–0.94)] and the specificity was 96% [95% CI (0.89–0.98)] (25). Stone et al. created a diagnostic algorithm that only integrates biopsy for histopathological investigation in suspected benign adenoma with SUV max < 3.1 or SUVmax > 3.1 and SUV ratio < 2.5 in PET/CT (26). Otherwise, malignant metastasis is suspected and adrenalectomy is indicated with therapeutic and diagnostic benefit by performing ex vivo histologic examinations. As stated, SUVmax analysis in PET/CT gives information whether the adenoma is benign or malignant, but the comparison of the histological finding leads to the final diagnosis.
Retroperitoneal supra-renal masses are often diagnosed coincidentally in the context of imaging of the abdomen and are then classified as incidentaloma. The origin of these suspect adrenal masses must be evaluated to discuss the following treatment, which differs if it is an adrenal (pheochromocytoma, adrenal hyperplasia, cortical adenoma) or extra-adrenal (malignancies, infections, hemorrhage) origin. As Frey et al. state in their review, 3.5% of the adrenalectomies are mistakenly performed under the indication of an adrenal disease (27). However, most incidentalomas are metastasis of other tumorous sites. Also, rare manifestations such as ganglioneuroma, hemangioendothelioma, and hemangioma must be considered. In 2016, the European Society of Endocrinology published a Clinical Practice Guideline for the management of such findings in the adrenal gland (28).
There are few clinical trials addressing PD-L1-targeted therapy with durvalumab in hematologic malignancies such as MALT-Lymphoma. The Phase 1/2 FUSION NHL 001 study by Casulo et al. aims to evaluate the security and efficacy of durvalumab as monotherapy and in combination with other full agents in patients with lymphoma (29). They found that durvalumab monotherapy and durvalumab combinations did not provide additional benefit while adding the treatment-related toxicity of PD‐L1 blockade.
In summary, this case demonstrates the importance of multidisciplinary discussion in the management of complex cases, especially when rare histologic subtypes are given and within clinical trials.
Despite its side effects, immunotherapy is an established component in the treatment of lung cancer. 18F-FDG-PET/CT plays a crucial role in diagnosis and during treatment to detect complications early. Nevertheless, if malignant processes are suspected, histologic confirmation must be performed. Otherwise, unexpected differential diagnoses may be misinterpreted. We emphasized the significance of considering other differential diagnoses in these patients and the importance of multidisciplinary treatment of the findings, especially within clinical trials.
Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
LK, ED and KE-M wrote the manuscript. FM supervised the writing. All authors contributed to the article and approved the submitted version.
LK and FM received an unrestricted research institutional grant from AstraZeneca. LK received honoraria from AMGEN and AstraZeneca. FM received honoraria from AstraZeneca, Novartis, Roche, Lilly, Elekta and Brainlab. FM serves in the advisory board of AstraZeneca, Novartis. FM was employed by Private Practise ´Die RADIOLOGIE´.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang PF, Chen Y, Song SY, Wang TJ, Ji WJ, Li SW, et al. Immune-related adverse events associated with anti-PD-1/PD-L1 treatment for Malignancies: A meta-analysis. Front Pharmacol. (2017) 8:730. doi: 10.3389/fphar.2017.00730
2. Ghimire P, Wu GY, Zhu L. Primary gastrointestinal lymphoma. World J Gastroenterol. (2011) 17:697–707. doi: 10.3748/wjg.v17.i6.697
3. Harris GJ, Tio FO, Von Hoff DD. Primary adrenal lymphoma. Cancer. (1989) 63:799–803. doi: 10.1002/1097-0142(19890215)63:4<799::AID-CNCR2820630432>3.0.CO;2-5
4. Di Rocco A, Petrucci L, Assanto GM, Martelli M, Pulsoni A. Extranodal marginal zone lymphoma: pathogenesis, diagnosis and treatment. Cancers (Basel). (2022) 14:1742. doi: 10.3390/cancers14071742
5. Moreau L, Gobet F, Grise P, Perraudin V, Lefebvre H. Marginal-zone lymphoma mimicking adrenal myelolipoma on computed tomography scan. J Clin Endocrinol Metab. (2010) 95:4173–4. doi: 10.1210/jc.2010-0329
6. Wang Y, Ren Y, Ma L, Li J, Zhu Y, Zhao L, et al. Clinical features of 50 patients with primary adrenal lymphoma. Front Endocrinol. (2020) 11:595. doi: 10.3389/fendo.2020.00595
7. Glomset DA. The incidence of metastasis of Malignant tumors to the adrenals. Am J Cancer. (1938) 32:57–61. doi: 10.1158/ajc.1938.57
8. Libè R, Dall’Asta C, Barbetta L, Baccarelli A, Beck-Peccoz P, Ambrosi B. Long-term follow-up study of patients with adrenal incidentalomas. Eur J Endocrinol. (2002) 147:489–94. doi: 10.1530/eje.0.1470489
9. Arnold DT, Reed JB, Burt K. Evaluation and management of the incidental adrenal mass. Proc (Bayl Univ Med Cent). (2003) 16:7–12. doi: 10.1080/08998280.2003.11927882
10. Brierley JD, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumours. 8th Edition. Wiley-Blackwell, Hoboken, New Jersey (United States): Wiley (2023). Available at: https://www.wiley.com/en-es/TNM+Classification+of+Malignant+Tumours%2C+8th+Edition-p-9781119263579.
11. Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, et al. Durvalumab after chemoradiotherapy in stage III non–small-cell lung cancer. New Engl J Med. (2017) 377:1919–29. doi: 10.1056/NEJMoa1709937
12. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol. (2019) 37:537–46. doi: 10.1200/JCO.18.00149
13. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. (2019) 381:1535–46. doi: 10.1056/NEJMoa1910836
14. Grover S, Rahma OE, Hashemi N, Lim RM. Gastrointestinal and hepatic toxicities of checkpoint inhibitors: algorithms for management. Am Soc Clin Oncol Educ Book. (2018) 38:13–9. doi: 10.1200/EDBK_100013
15. Joshi MN, Whitelaw BC, Palomar MTP, Wu Y, Carroll PV. Immune checkpoint inhibitor-related hypophysitis and endocrine dysfunction: clinical review. Clin Endocrinol (Oxf). (2016) 85:331–9. doi: 10.1111/cen.13063
16. Chan KK, Bass AR. Autoimmune complications of immunotherapy: pathophysiology and management. BMJ. (2020) 369:m736. doi: 10.1136/bmj.m736
17. Martins F, Sofiya L, Sykiotis GP, Lamine F, Maillard M, Fraga M, et al. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. Nat Rev Clin Oncol. (2019) 16:563–80. doi: 10.1038/s41571-019-0218-0
18. Özdemir BC, Espinosa da Silva C, Arangalage D, Monney P, Guler SA, Huynh-Do U, et al. Multidisciplinary recommendations for essential baseline functional and laboratory tests to facilitate early diagnosis and management of immune-related adverse events among cancer patients. Cancer Immunol Immunother. (2023) 72(7):1991–2001. doi: 10.1007/s00262-023-03436-0
19. Wong ANM, McArthur GA, Hofman MS, Hicks RJ. The advantages and challenges of using FDG PET/CT for response assessment in melanoma in the era of targeted agents and immunotherapy. Eur J Nucl Med Mol Imaging. (2017) 44:67–77. doi: 10.1007/s00259-017-3691-7
20. Cho SY, Huff DT, Jeraj R, Albertini MR. FDG PET/CT for assessment of immune therapy: opportunities and understanding pitfalls. Semin Nucl Med. (2020) 50:518–31. doi: 10.1053/j.semnuclmed.2020.06.001
21. Nobashi T, Baratto L, Reddy SA, Srinivas S, Toriihara A, Hatami N, et al. Predicting response to immunotherapy by evaluating tumors, lymphoid cell-rich organs, and immune-related adverse events using FDG-PET/CT. Clin Nucl Med. (2019) 44:e272–9. doi: 10.1097/RLU.0000000000002453
22. Kim SJ, Lee SW, Pak K, Kim IJ, Kim K. Diagnostic accuracy of 18F-FDG PET or PET/CT for the characterization of adrenal masses: a systematic review and meta-analysis. Br J Radiol. (2018) 91:20170520. doi: 10.1259/bjr.20170520
23. Ma G, Zhang X, Wang M, Xu X, Xu B, Guan Z. Role of 18F-FDG PET/CT in the differential diagnosis of primary benign and Malignant unilateral adrenal tumors. Quant Imaging Med Surg. (2021) 11:2013–8. doi: 10.21037/qims-20-875
24. Perry C, Herishanu Y, Metzer U, Bairey O, Ruchlemer R, Trejo L, et al. Diagnostic accuracy of PET/CT in patients with extranodal marginal zone MALT lymphoma. Eur J Haematol. (2007) 79:205–9. doi: 10.1111/j.1600-0609.2007.00895.x
25. Bancos I, Tamhane S, Shah M, Delivanis DA, Alahdab F, Arlt W, et al. DIAGNOSIS OF ENDOCRINE DISEASE: The diagnostic performance of adrenal biopsy: a systematic review and meta-analysis. Eur J Endocrinol. (2016) 175:R65–80. doi: 10.1530/EJE-16-0297
26. Stone WZ, Wymer DC, Canales BK. Fluorodeoxyglucose-positron-emission tomography/computed tomography imaging for adrenal masses in patients with lung cancer: review and diagnostic algorithm. J Endourol. (2014) 28:104–11. doi: 10.1089/end.2013.0380
27. Frey S, Caillard C, Toulgoat F, Drui D, Hamy A, Mirallié É. Non-adrenal tumors of the adrenal area; what are the pitfalls? J Visceral Surg. (2020) 157:217–30. doi: 10.1016/j.jviscsurg.2020.02.004
28. Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. (2016) 175:G1–34. doi: 10.1530/EJE-16-0467
Keywords: PET/CT, NSCLC, durvalumab, MALT lymphoma, immune-related side effect
Citation: Käsmann L, Degerli E, El-Marouk K and Manapov F (2024) Case report: Incidental MALT lymphoma of the left adrenal gland mimicking a metastatic spread within durvalumab maintenance treatment in inoperable stage III non-small cell lung cancer. Front. Oncol. 14:1226422. doi: 10.3389/fonc.2024.1226422
Received: 21 May 2023; Accepted: 29 February 2024;
Published: 19 March 2024.
Edited by:
Pierluigi Navarra, Catholic University of the Sacred Heart, ItalyReviewed by:
Luis Mas, Auna Oncosalud, PeruCopyright © 2024 Käsmann, Degerli, El-Marouk and Manapov. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lukas Käsmann, THVrYXMuS2Flc21hbm5AbWVkLnVuaS1tdWVuY2hlbi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.