 Ralf S. Eschbach1Markus Hofmann1Lukas Späth1
Ralf S. Eschbach1Markus Hofmann1Lukas Späth1 Gabriel T. Sheikh1Astrid Delker1Simon Lindner1
Gabriel T. Sheikh1Astrid Delker1Simon Lindner1 Klaus Jurkschat2
Klaus Jurkschat2 Carmen Wängler3Björn Wängler4Ralf Schirrmacher5
Carmen Wängler3Björn Wängler4Ralf Schirrmacher5 Reinhold Tiling1
Reinhold Tiling1 Matthias Brendel1Vera Wenter1Franziska J. Dekorsy1Mathias J. Zacherl1
Matthias Brendel1Vera Wenter1Franziska J. Dekorsy1Mathias J. Zacherl1 Andrei Todica1,6
Andrei Todica1,6 Harun Ilhan1,6Freba Grawe1,7Clemens C. Cyran7
Harun Ilhan1,6Freba Grawe1,7Clemens C. Cyran7 Marcus Unterrainer7Johannes Rübenthaler7Thomas Knösel6,8Tanja Paul6,8Stefan Boeck6,9Christoph Benedikt Westphalen6,9Christine Spitzweg6,10Christoph J. Auernhammer6,10Peter Bartenstein1,6Lena M. Unterrainer1†
Marcus Unterrainer7Johannes Rübenthaler7Thomas Knösel6,8Tanja Paul6,8Stefan Boeck6,9Christoph Benedikt Westphalen6,9Christine Spitzweg6,10Christoph J. Auernhammer6,10Peter Bartenstein1,6Lena M. Unterrainer1† Leonie Beyer1,6*†
Leonie Beyer1,6*†- 1Department of Nuclear Medicine, University Hospital, LMU Munich, Munich, Germany
- 2Fakultät für Chemie und Chemische Biologie, Technische Universität Dortmund, Dortmund, Germany
- 3Biomedical Chemistry, Clinic of Radiology and Nuclear Medicine, Medical Faculty Mannheim of Heidelberg University, Mannheim, Germany
- 4Medical Faculty Mannheim of Heidelberg University, Molecular Imaging and Radiochemistry, Clinic of Radiology and Nuclear Medicine, Mannheim, Germany
- 5Department of Oncology, Division of Oncological Imaging, University of Alberta, Edmonton, AB, Canada
- 6ENETS Centre of Excellence, Interdisciplinary Center of Neuroendocrine Tumours of the GastroEnteroPancreatic System at the University Hospital of Munich (GEPNET-KUM), University Hospital of Munich, Munich, Germany
- 7Department of Radiology, University Hospital, LMU Munich, Munich, Germany
- 8Institute of Pathology, LMU, Munich, Germany
- 9Department of Internal Medicine 3, University Hospital, Munich, Germany
- 10Department of Internal Medicine 4, University Hospital, LMU Munich, Munich, Germany
Purpose: Somatostatin analogues (SSA) are frequently used in the treatment of neuroendocrine tumours. Recently, [18F]SiTATE entered the field of somatostatin receptor (SSR) positron emission tomography (PET)/computed tomography (CT) imaging. The purpose of this study was to compare the SSR-expression of differentiated gastroentero-pancreatic neuroendocrine tumours (GEP-NET) measured by [18F]SiTATE-PET/CT in patients with and without previous treatment with long-acting SSAs to evaluate if SSA treatment needs to be paused prior to [18F]SiTATE-PET/CT.
Methods: 77 patients were examined with standardised [18F]SiTATE-PET/CT within clinical routine: 40 patients with long-acting SSAs up to 28 days prior to PET/CT examination and 37 patients without pre-treatment with SSAs. Maximum and mean standardized uptake values (SUVmax and SUVmean) of tumours and metastases (liver, lymphnode, mesenteric/peritoneal and bones) as well as representative background tissues (liver, spleen, adrenal gland, blood pool, small intestine, lung, bone) were measured, SUV ratios (SUVR) were calculated between tumours/metastases and liver, likewise between tumours/metastases and corresponding specific background, and compared between the two groups.
Results: SUVmean of liver (5.4 ± 1.5 vs. 6.8 ± 1.8) and spleen (17.5 ± 6.8 vs. 36.7 ± 10.3) were significantly lower (p < 0.001) and SUVmean of blood pool (1.7 ± 0.6 vs. 1.3 ± 0.3) was significantly higher (p < 0.001) in patients with SSA pre-treatment compared to patients without. No significant differences between tumour-to-liver and specific tumour-to-background SUVRs were observed between both groups (all p > 0.05).
Conclusion: In patients previously treated with SSAs, a significantly lower SSR expression ([18F]SiTATE uptake) in normal liver and spleen tissue was observed, as previously reported for 68Ga-labelled SSAs, without significant reduction of tumour-to-background contrast. Therefore, there is no evidence that SSA treatment needs to be paused prior to [18F]SiTATE-PET/CT.
1 Introduction
Overexpression of somatostatin receptors (SSRs) is highly relevant for both diagnostics and therapeutic options in well-differentiated neuroendocrine tumours (NET) (1, 2). According to the German and European consensus guidelines, treatment with somatostatin analogues (SSAs) is the first line treatment for proliferation control in all well-differentiated metastatic/non-resectable NET of the Gastro-Entero-Pancreatic System (GEP-NET) (3–5). Diagnostically, 68Ga-labeled SSAs are recommended for staging, re-staging and therapy monitoring (6, 7). Therapeutically, 177Lu-/90Y-labeled SSAs are used in later-stage disease in metastatic/non-resectable GEP-NETs (4, 5).
As both therapeutic and diagnostic SSAs bind to SSRs, medication with SSA could potentially reduce the specific binding of the SSA radiotracer in combined positron-emission-tomography/computed tomography (PET/CT) imaging. After treatment with SSA octreotide, in vitro studies indicated internalisation of SSR subtype 2 receptors (8–11). On the contrary, one study suggested upregulation of SSR expression after incubation of pituitary cells in culture with a SSA (12).
For imaging, a former study revealed an improved visualisation of carcinoid liver metastases by 111In-pentetreotide scintigraphy after treatment with cold SSA (13). The uptake of 68Ga-labeled SSAs DOTATATE and DOTATOC in PET/CT imaging was found to be only reduced in the normal organs but not in tumour tissue after SSA medication, leading to an even higher tumour-to-background contrast (14, 15). To rule out a potentially reduced binding and impaired therapeutic effect of radioactive SSA for peptide receptor radionuclide therapy (PRRT), medication with long-lasting SSAs needs to be paused at least 30 days and medication with short-acting SSAs for at least 24 hours prior to PRRT (16).
Currently, the first 18F-labelled SSA radioligand, [18F]SiTATE has been introduced as an alternative to 68Ga-labeled SSAs for NET SSR-PET imaging with comparable radiation exposure and promising tumour-to-background contrast (17–20). The aim of this study was to investigate the influence of SSA medication prior to [18F]SiTATE PET/CT regarding normal-tissue and tumour uptake of the radiotracer when compared to former 68Ga-labeled SSAs to validate its clinical potential.
2 Materials and methods
2.1 Patient enrolment
All patients were referred for imaging by their treating endocrinologists and/-or oncologists between March 2019 and April 2021 and gave written informed consent to undergo [18F]SiTATE-PET/CT following the regulations of the German Pharmaceuticals Act. In principle, all patients with a NET were included, independent of the origin of the tumour. Patients with an unknown status of prior SSA therapy or a SSA treatment longer than 28 days ago were excluded prior to analysis. The cohort consisted of patients with and without prior SSA treatment, which was determined by the treating endocrinologist/oncologist in line with the interdisciplinary tumour board, completely independent from the imaging procedure. The study was performed in compliance with the principles of the Declaration of Helsinki and its subsequent amendments (21), and with the approval of the local ethics committee (approval number 21-0102).
2.2 PET/CT imaging
SiTATE was obtained from ABX, Advanced Biomedical Compounds (Radeberg, Germany) and [18F]SiTATE was synthesized as described previously (17, 18, 22). All quality control data met the release criteria. [18F]SiTATE-PET/CT scans were acquired at the Department of Nuclear Medicine, LMU Munich on a Siemens Biograph mCT flow (Siemens Healthineers, Erlangen, Germany). After intravenous injection of 3 ± 1 MBq/kgBw (median 232 ± 36 MBq, range 152 to 310) of [18F]SiTATE, PET scans were acquired 90 ± 15 min after injection for 15-20 min (in flow mode depending on the body height). Patients were asked to empty the bladder if necessary. In 75/77 patients, contrast-enhanced CT scans with 1.5 mL of iopromide (Ultravist 300, Bayer Healthcare, Leverkusen, Germany) per kilogram of body weight were performed for anatomic localisation; the remaining two cases received diagnostic CT scan without contrast enhancement. The PET scan was acquired by static emission data with a scan speed of 0.7 mm/s for both neck and abdominal region and 0.9 mm/s for the lung region in flow mode. With CT scans serving for attenuation correction, PET images were reconstructed with a transaxial 200 × 200 matrix using TrueX (including TOF, 2 iterations and 21 subsets, 3D Gauss post-filter of 4-mm full-width-half-maximum).
2.3 Image analysis
Image analysis was performed using a dedicated software package (Hermes Hybrid Viewer, Hermes Medical Solutions, Stockholm, Sweden). Uptake in normal organs and tumour uptake (hottest lesion for each metastatic tissue type) in patients was assessed by SUVmax and SUVmean (threshold 50% of max) measurements as described previously (18, 20). In short, spherical VOIs were placed inside the organ parenchyma using a 1-cm diameter VOI for small organs (adrenal glands) and a 2-cm diameter VOI for muscle, liver, spleen, fat tissue, aortic lumen (descending aorta), lung, bone (femur) and small intestine. Tumour-to-liver ratios (TLR) and tumour-to-background ratios (corresponding background for each lesion type, e.g. bone for osseous metastasis) were calculated for all measured tumour lesions according to the clinically relevant Krenning score which has been evaluated for SSTR-PET imaging (23, 24).
2.4 Statistical analysis
Data are reported as mean or median ± standard deviation or range as stated. Demographics and radiotracer uptake of normal organs (spleen, adrenal gland, liver small intestine, blood-pool, lung, bone) and tumour lesions were compared between group using a student’s t-test for metric variables and a Fisher exact/Chi-square test for contingency analysis of non-metric data. To compare the tumor uptake between SSA+ and SSA- patients, a lesion-based approach was used where the hottest lesion from each patient (if applicable) was included for different metastatic sites. Radiotracer uptake was correlated with the time after SSA-injection using a Pearson’s correlation coefficient. GraphPad Prism (version 8.4.3, GraphPad Software Inc., San Diego, CA) was used for statistical analysis and illustration of results. A significance level of p < 0.05 was applied in all analyses.
3 Results
3.1 Patients
All patients tolerated the examination well and did not report any unforeseen symptoms or adverse reactions. No drug-related pharmacologic effects or physiologic responses occurred. Thirty-seven male and forty female patients (SSA+ ♂22 ♀18; SSA- ♂15 ♀22) with differentiated NETs and a median age of 63 years (range 24 – 86 years) underwent a [18F]SiTATE-PET/CT. The mean age was comparable between groups and the time since initial diagnosis was significantly longer in the SSA+ group. Primary tumour locations included the small intestine (n=35), pancreas (n = 28), other gastrointestinal locations (n=5) and the primary tumour was not detectable (carcinoma of unknown primary) in n = 9 patients. Prior to PET/CT, the majority of patients were known to have hepatic (n = 51) metastases. Further metastatic sites included lymph nodes (n = 34), bone (n = 22), lung (n = 2) or peritoneal (n = 12) lesions. Most of the patients underwent surgery before (n = 45) followed by PRRT (n = 25) and chemotherapy (n = 14). In the SSA+ patients, the majority of primary tumours were located in the small intestine, whereas most of the patients in the SSA- group showed a pancreatic tumour. Also, more patients in the SSA+ group underwent surgery when compared to the SSA- and more SSA- patients received chemotherapy within their medical history compared to SSA+ patients. In SSA+ patients, the time interval between SSA treatment and PET/CT imaging was 12.9 ± 6.2 days. All SSA+ patients received the highest dose of the given SSA analogue (n=20 patients Sandostatin® LAR® 30 mg, n=20 patients Somatuline Autogel® 120 mg). Detailed patient characteristics are provided in Table 1.
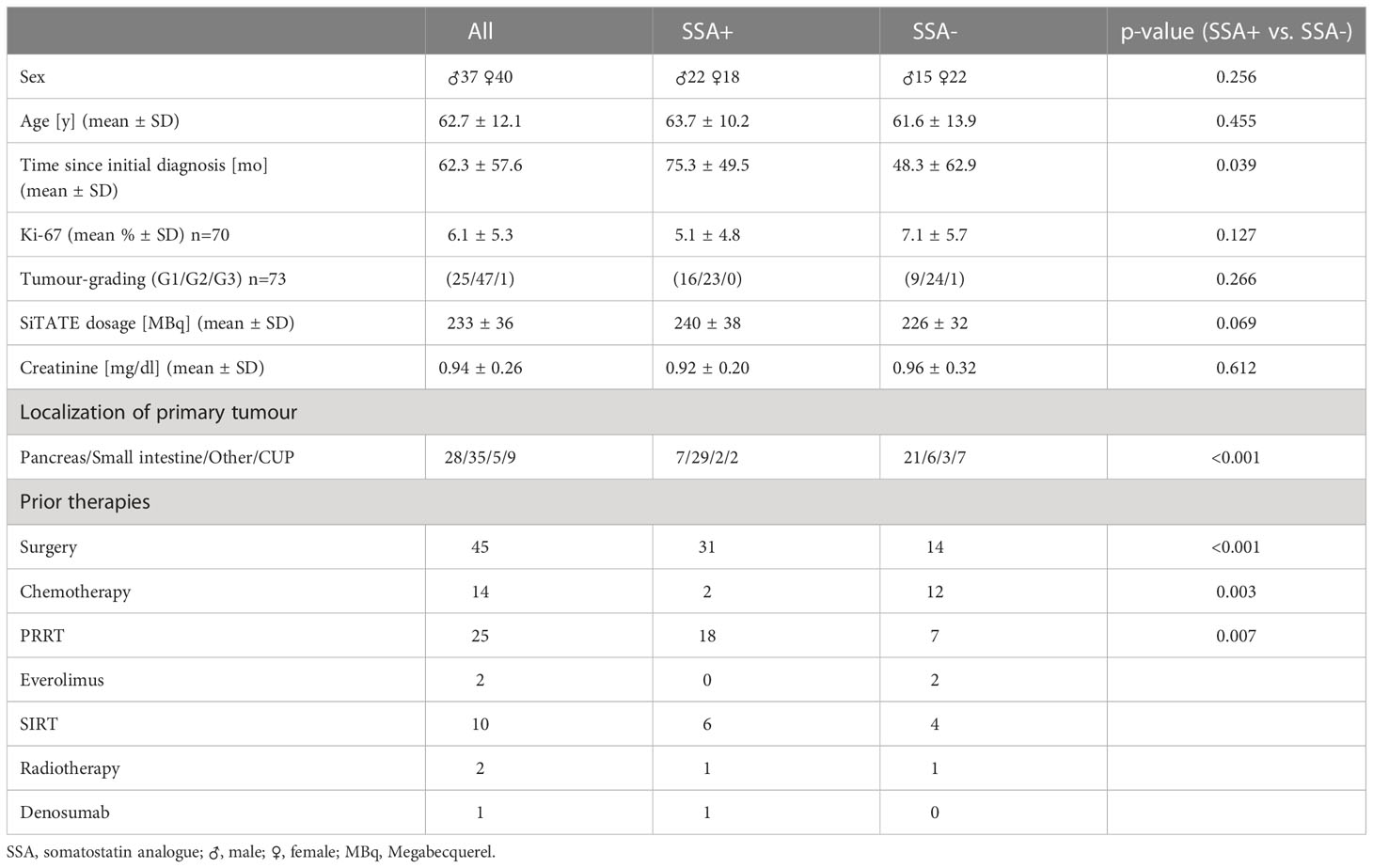
Table 1 Patient characteristics.
3.2 Biodistribution
In line with previous studies, the radiotracer uptake in the normal organs was highest in the spleen, followed by the adrenal glands and the liver. Patients undergoing a SSA treatment showed a significantly reduced radiotracer uptake in the spleen (SUVmean 17.5 vs. 36.7, p < 0.001) and the liver (SUVmean 5.4 vs. 6.8, p < 0.001) when compared to patients without SSA treatment. On the other hand, the radiotracer uptake was significantly higher in the blood pool of patients with ongoing SSA treatment (SUVmean 1.7 vs. 1.3, p < 0.001). For details of the biodistribution in normal organs see Table 2 and Figure 1.
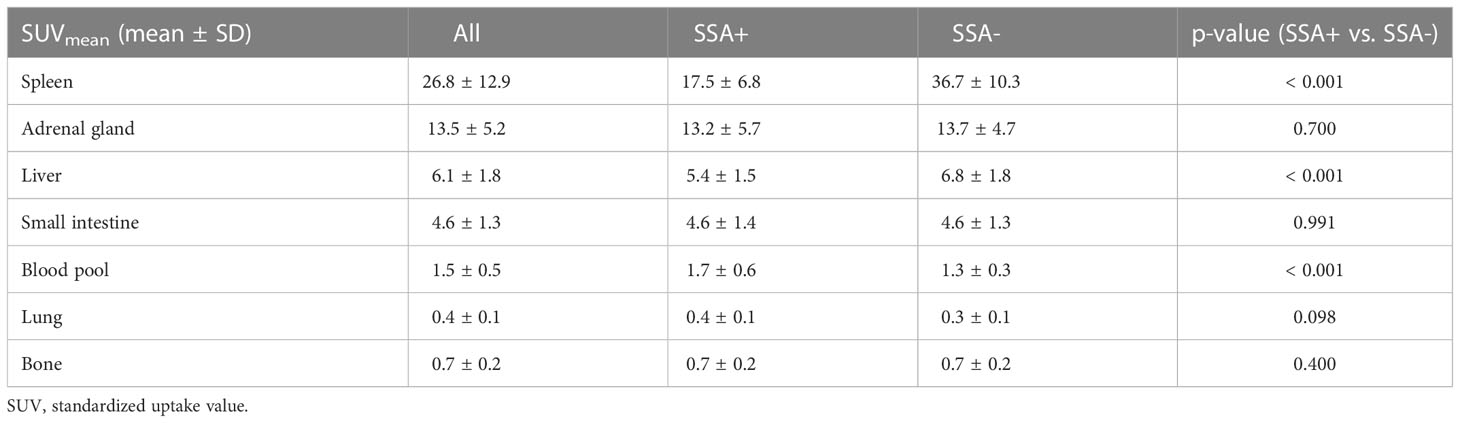
Table 2 Biodistribution of [18F]SiTATE in normal organs.
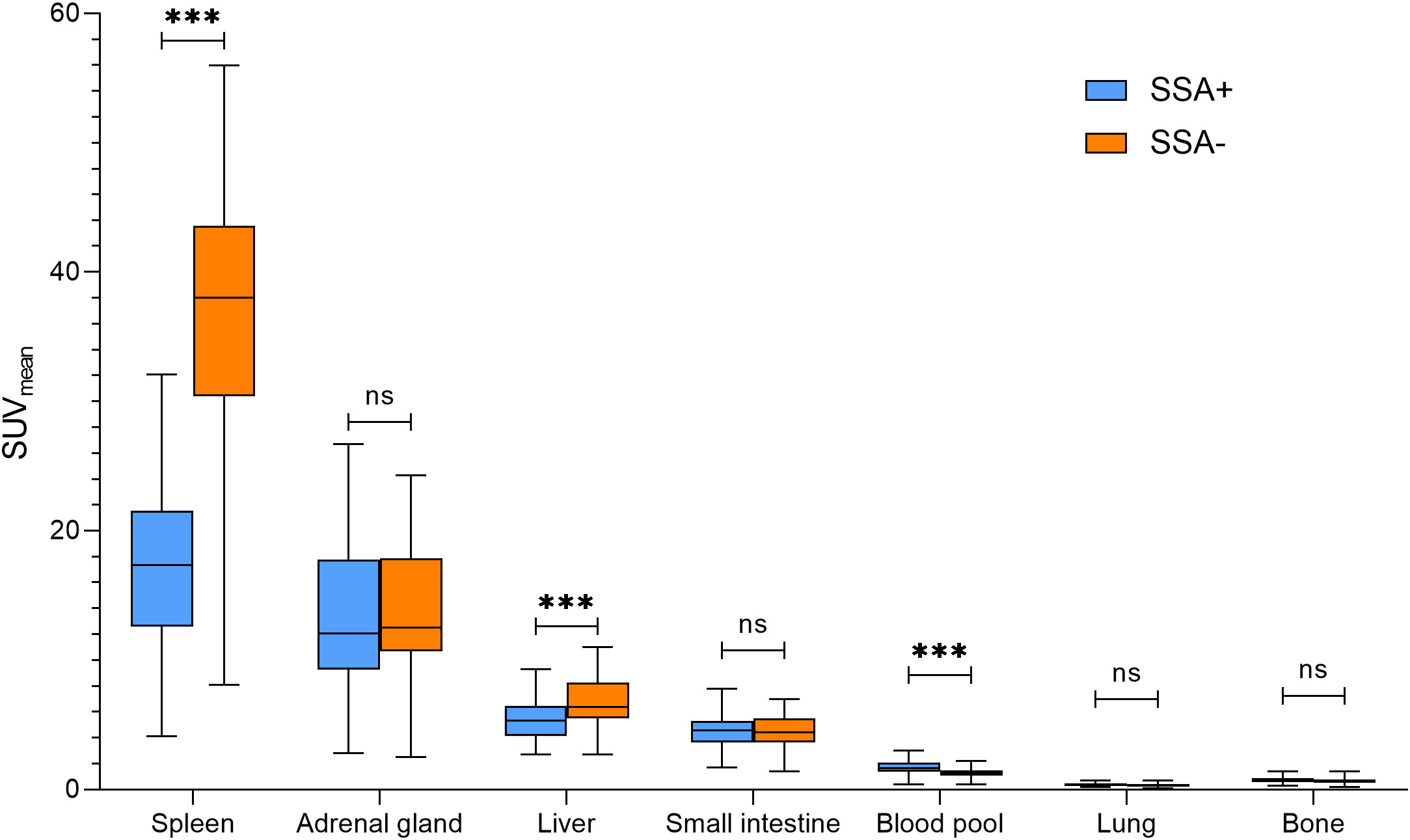
Figure 1 Biodistribution of [18F]SiTATE in normal organs in patients with (left boxplot)/without (corresponding right boxplot) SSA treatment. SUV, standardized uptake value; SSA, somatostatin analogue. *** p < 0.001, ns = p-value non-significant.
3.3 Tumour uptake and tumour-to-background ratios
Overall, the radiotracer uptake (SUVmax) to primary or metastatic tumour lesions was not significantly different between patients with/without ongoing SSA treatment. Also, tumour-to-liver and tumour-to-specific-background ratios did not significantly differ between groups. For details of both groups see Table 3 and Figure 2.

Table 3 Radiotracer uptake of [18F]SiTATE in metastatic tumour lesions.
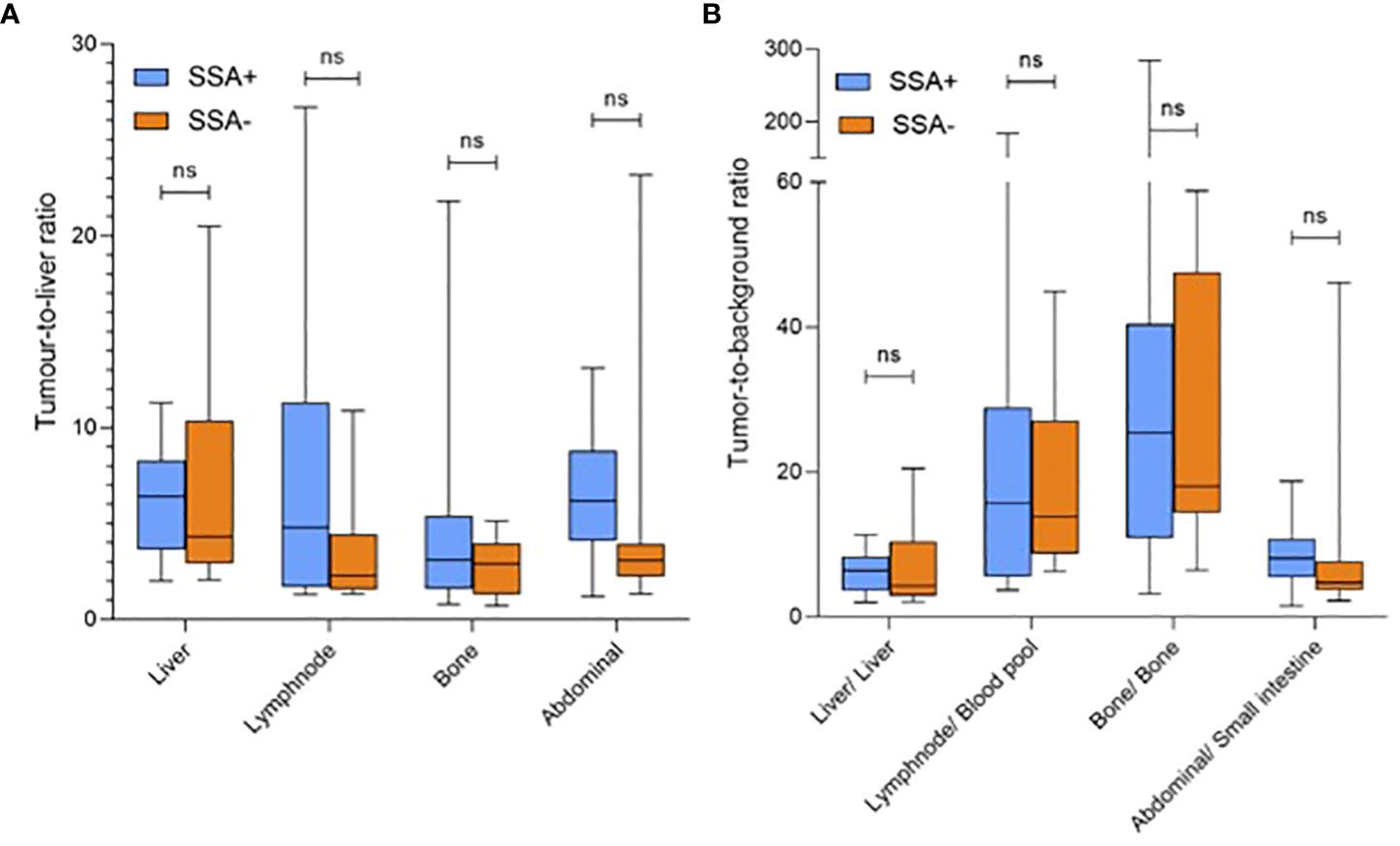
Figure 2 Radiotracer uptake of [18F]SiTATE in metastatic tumour lesions displayed as (A) tumour-to-liver and (B) tumour-to-specific background ratios (mean SUVmax/SUVmean) for patients with (left boxplot)/without (corresponding right boxplot) SSA treatment. SUV, standardized uptake value; SSA, somatostatin analogue; ns = p-value non-significant.
3.4 Individual radiotracer uptake under SSA treatment
Previous group-wise comparison suggests a reduced radiotracer uptake in normal organs but comparable tumour-to-background ratios. Figure 3 shows two exemplary patient cases that visually match those results.
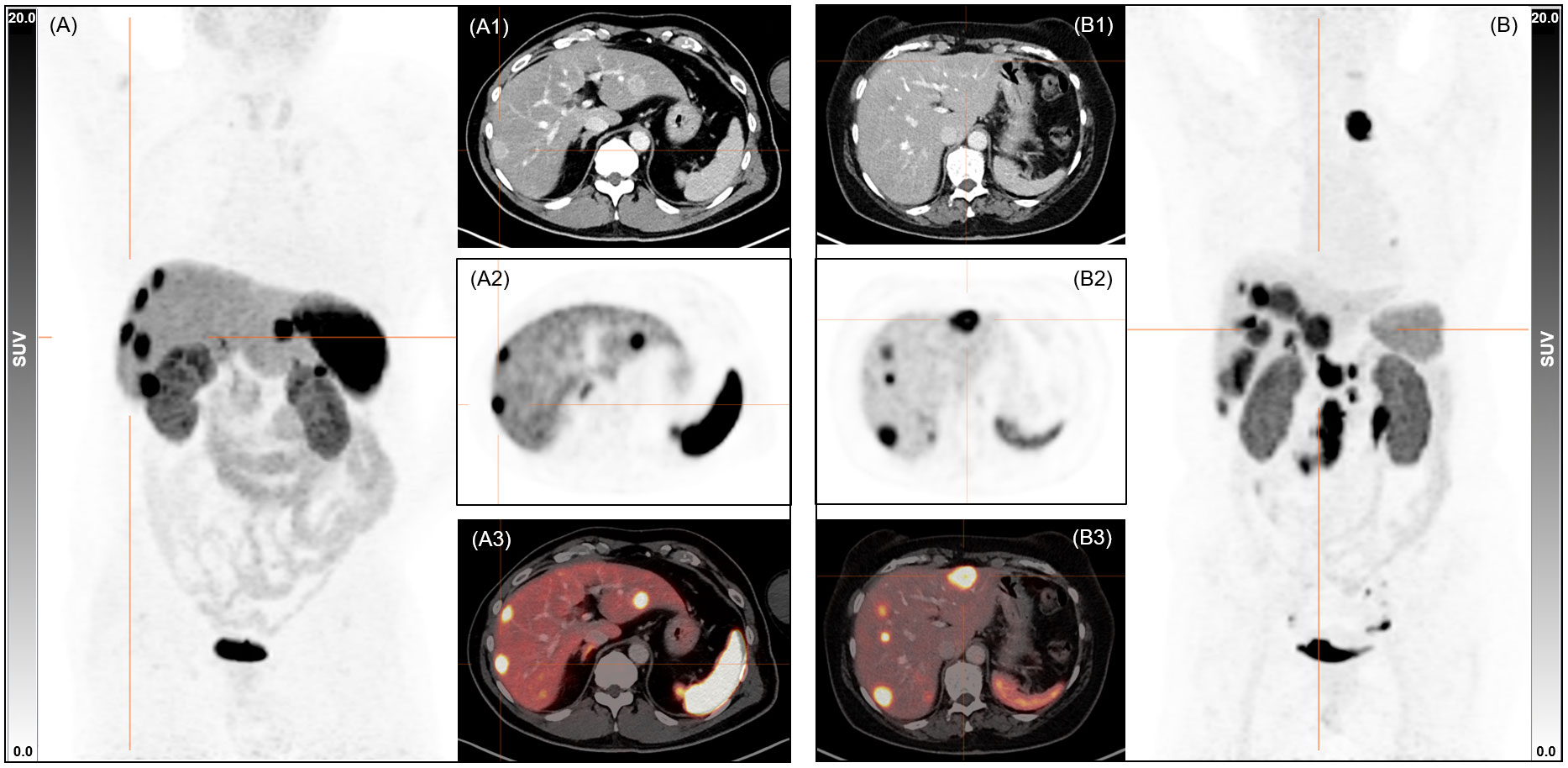
Figure 3 Exemplary maximum intensity projections images and axial sections (1 CT, 2 PET, 3 fused PET/CT) from patients (A) without SSA treatment (male, 59 y, 81 kg, 245 MBq, 89 min p.i., creatinine 1.0 mg/dl, liver SUVmean 8.3, spleen SUVmean 28.0, blood pool SUVmean 1.3) and (B) undergoing SSA treatment (female, 71 y, 64 kg, 281 MBq, 93 min p.i., creatinine 0.7 mg/dl, liver SUVmean 4.1, spleen SUVmean 10.9, blood pool SUVmean 1.6). SUV, standardized uptake value; SSA, somatostatin analogue; MBq, Megabecquerel.
Altered [18F]SiTATE uptake was time-dependent. Figure 4 shows the inter-individual correlation between liver, spleen and blood-pool SUVmean and hottest lesion SUVmax with the time after SSA injection with significant correlations for the liver and spleen radiotracer uptake (RLiver = 0.363, pLiver = 0.022; RSpleen = 0.515, pSpleen = 0.001).
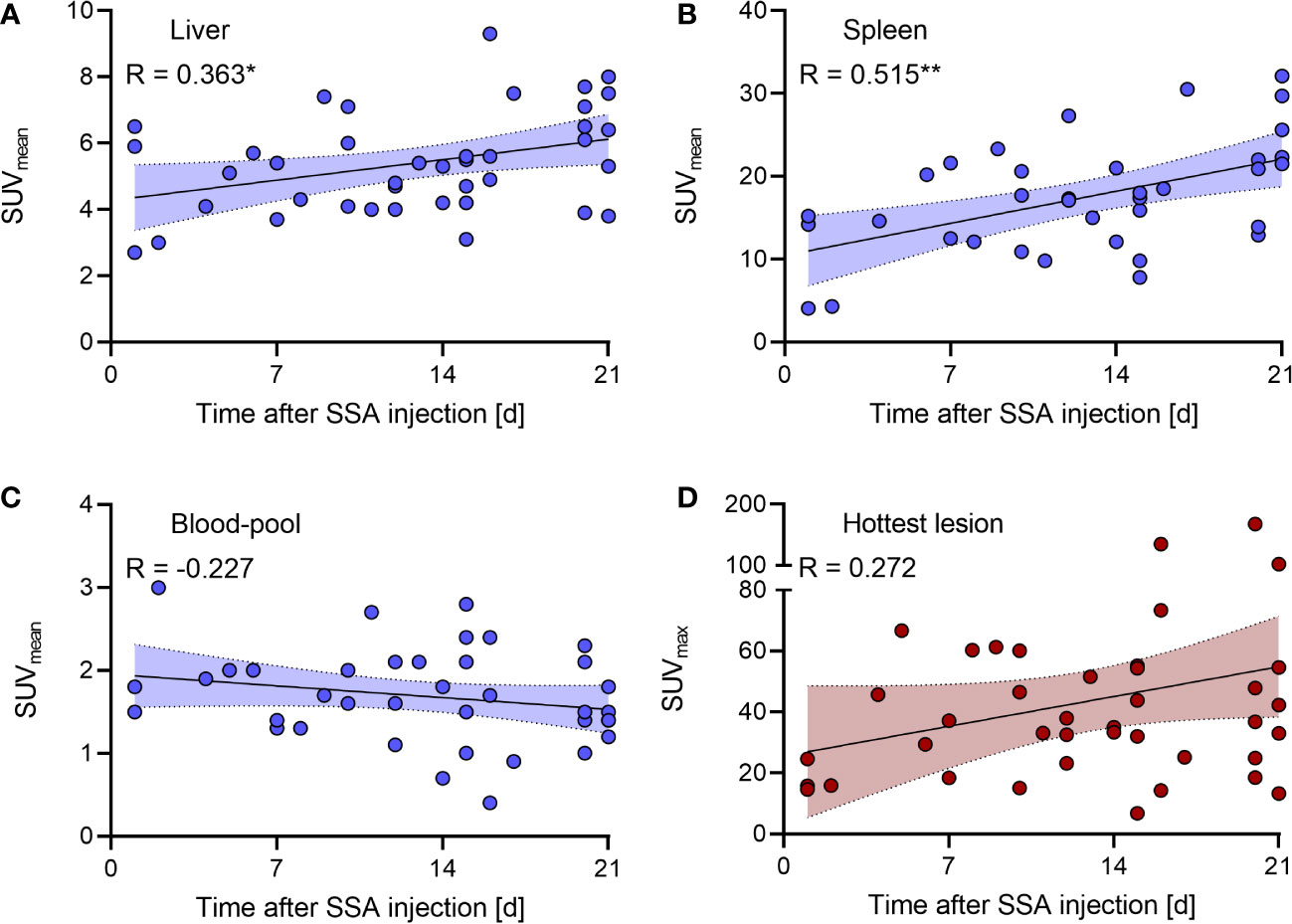
Figure 4 Inter-individual correlation of (A–C) SUVmean of the liver/spleen/blood-pool and (D) SUVmax of the hottest lesion uptake with the time after SSA injection. The coloured fields around the correlation line represent the 95% confidence interval. SUV, standardized uptake value; SSA, somatostatin analogue. * and ** means a significant correlation.
4 Discussion
In the present study we investigated the influence of a previous treatment with long-acting non-radioactive SSAs on the SSR-expression in patients with GEP-NETs measured by PET/CT with the new radioactive SSA [18F]SiTATE.
Our results with [18F]SiTATE are in line with previous clinical studies with several SSR radioligands: Haug et al. investigated 105 NET patients with [68Ga]Ga-DOTATATE of whom 35 had been pre-treated with long-acting octreotide and reported a significantly lower [68Ga]Ga-DOTATATE uptake of non-tumorous spleen and liver in patients treated with SSAs (15). Lodge et al., who prospectively investigated the effect of a pre-dose of octreotide prior to injection of the radiotracer on the distribution of [68Ga]Ga-DOTATOC in 7 patients with GEP-NETs intra-individually within 7 ± 9 days observed a decreased radiotracer uptake in normal liver by 25% and spleen by 47% with octreotide pre-therapy (14). Another prospective study of Aalbersberg et al. intra-individually evaluated 34 patients with metastatic NET before and after lantreotide therapy with the result of significantly decreased uptake of non-tumorous liver and spleen (25). This is in accordance with our results with significant lower [18F]SiTATE background uptake (SUVmean) in liver and spleen tissue in patients with previous SSA treatment, compared to patients without.
Moreover, our results with [18F]SiTATE showed a significantly higher blood pool signal in SSA treated patients. This could reflect a decreased binding and therefore higher number of circulating radioligands because of two potential explanations: a lower SSR density as a consequence of predominantly internalized SSR 2 in neoplastic and physiologic target tissues or SSR saturation with non-radioactive SSAs under therapy (26).
In contrast to Haug et al., who used [68Ga]Ga-DOTATATE, in our study with [18F]SiTATE the radioligand uptake of the non-tumorous background in liver and spleen as well as in blood pool showed a time dependency on the interval since SSA treatment with significant positive correlations between the number of days after treatment and radiotracer uptake of liver and spleen, and a trend towards an inverse correlation with the blood pool. This time dependency on the interval since SSA treatment may be explained by the fact that the non-radioactive SSAs compete with the SSR radioligands for receptor binding sites and the quantity of SSR internalization is dependent on the octreotide dose (26). This means that the more non-radioactive SSAs are circulating in the blood, the more receptors are blocked and internalized, but with reversibility of the internalization over time (27).
Aalbersberg et al. observed an increased tumour uptake leading to an increased tumour-to-liver ratio (25). Former studies using conventional scintigraphy for the detection of NET metastases before and during treatment with octreotide showed an intra-individually improved visualization of carcinoid liver metastases in 5 midgut NET patients after SSA treatment measured by 111In-pentreotide (13) and a higher tumour-to-background ratio in 8 NET patients by using 111In-octreotide scintigraphy (28). In contrast, analogously to Haug et al. and Lodge et al. (14, 15), our results reveal no significant differences in SSR expression and target-to-background-ratios. With [18F]SiTATE there were no significant differences in SUVmax in tumours/metastastic lesions between the two groups as well as no significant differences in tumour-to-liver and tumour-to-specific-background ratios. Our findings may be partially explained by the fast and efficient internalization of SSR 2 after agonist stimulation under octreotide therapy in vivo in neoplastic as well as in physiologic SSR 2 target tissues (26, 27). Furthermore, an agonist-induced up-regulation of SSR subtypes, which causes an increase of the receptor density in the tumours and metastases of SSA treated patients (12) with a consecutively higher [18F]SiTATE uptake may be partially masked by SSA occupied receptors (15). Thus, there might be a steady state of concomitant receptor internalization and overexpression. In long-acting SSAs, the initial pharmacokinetic profile after injection differs between lanreotide depot and octreotide depot formulations (15, 29), while subsequent serum concentrations remainquite stable over 28 d with both formulations (15, 29).
It has to be mentioned that the above cited scintigraphical studies are limited by several aspects: first, only a very low number of patients was investigated. Secondly, the quantifiability in conventional scintigraphy is reduced compared to PET/CT with SUV calculations. Thirdly, interpretation of these intra-individual scintigraphy results is limited by a possible tumour progression during the 12 month treatment course which may result in an increase of the uptake values.
However, all these study results consistently indicate that octreotide treatment may influence the binding and change the biodistribution of SSR radioligands, but suggest that the diagnostic reliability of somatostatin receptor imaging in NET metastases is not significantly compromised by any previous or concomitant octreotide therapy (13). Moreover, these findings even underline that SSA treatment may facilitate the detection of NET metastases, mainly driven by a decline in background binding in the liver and spleen rather than an increase in tumour binding, possibly providing an improved tumour delineation (15).
Because of the heterogeneity of NETs and consequently the possibility of various biologic behaviours, it remains uncertain if these findings can be generalized to other types of NET (15). Also, the small sample size and heterogeneity of patients might impair the detection of statistically significant differences between groups. There are differences in contributions of tumor grading, metastatic sites or time since diagnosis that cannot be avoided due to the individual clinical courses of included patients in this rare disease. Consequently, one major limitation of this study lies in the inter-patient comparison of binding. In most of the patients, treatment with SSAs cannot be paused which excludes them from an intra-patient comparison. Nevertheless, the presented results are promising, but require further investigation in future clinical trials to validate our data intra-individually and also to evaluate the influence of long-acting SSA pre-treatment on radioligand binding in patients that receive PRRT with e.g. [177Lu]Lu-DOTATATE.
5 Conclusions
A treatment with long-acting SSAs does not reduce the [18F]SiTATE -binding in tumorous target lesions of GEP-NET patients and even reveals a significant lower background signal in non-tumorous liver and spleen tissues, consistently to other radioactive SSA, which could improve demarcation of metastases in these organs. Our results add support to the hypothesis that a previous or concomitant treatment with long-acting SSAs does not unfavourably/adversely influence the SSR expression and therefore confirm the clinical approach not to discontinue/interrupt any SSA medication prior to a PET/CT examination.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (LMU Munich - approval number 21-0102) and with the 1964 Helsinki declaration and its later amendments. The patients/participants provided their written informed consent to participate in this study.
Author contributions
RE: data acquisition, statistics, writing of the draft. MH, LS, LU, GS, RT, MB, VW, FD, MZ, AT, HI, FG, CC, MU, JR, PB: data acquisition, revision of the manuscript. AD: image reconstruction, revision of the manuscript. SL, KJ, CW, BW, RS: SiTATE preparation, revision of the manuscript. TK, TP: histopathological correlations, revision of the manuscript. SB, CW, CS, CA: patient referral, clinical data acquisition, revision of the manuscript; LB: concept, data acquisition, statistics, revision of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
LB and LU were funded by the Munich-Clinician-Scientist-Program (LMU Munich).
Conflict of interest
CA has received research contracts Novartis, lecture honorarium Ipsen, Novartis, Advanced Accelerator Applications and honoraria for advisory boards Advanced Accelerator Applications. HI has received research contracts Novartis. LB received honoraria for advisory boards Bayer, Advanced Accelerator Applications and is a Novartis Radiopharmaceuticals GmbH employee since 10/2022. CW has received honoraria from Amgen, Bayer, Chugai, Celgene, Falk, GSK, MSD, Merck, Janssen, Ipsen, Roche, Servier, SIRTeX, Taiho; served on advisory boards for Bayer, BMS, Celgene, Servier, Shire/Baxalta, Rafael Pharmaceuticals, RedHill, Roche, has received travel support by Bayer, Celgene, RedHill, Roche, Servier, Taiho and research grants institutional by Roche. CW serves as an officer for European Society of Medical Oncology ESMO, Deutsche Krebshilfe DKH, Arbeitsgemeinschaft internistische Onkologie AIO.
The remaining authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Reubi J, Waser B, Schaer JC, Laissue JA. Erratum to: Somatostatin receptor sst1-sst5 expression in normal and neoplastic human tissues using receptor autoradiography with subtype-selective ligands. Eur J Nucl Med (2001) 28:1433. doi: 10.1007/s002590100598
2. Reubi JC, Waser B, Schaer JC, Laissue JA. Somatostatin receptor sst1-sst5 expression in normal and neoplastic human tissues using receptor autoradiography with subtype-selective ligands. Eur J Nucl Med (2001) 28:836–46. doi: 10.1007/s002590100541
3. AWMF. Practice guideline neuroendocrine tumors - AWMF-reg. 021-27. Z fur Gastroenterologie (2018) 56:583–681. doi: 10.1055/a-0604-2924
4. Falconi M, Eriksson B, Kaltsas G, Bartsch DK, Capdevila J, Caplin M, et al. ENETS consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non-functional pancreatic neuroendocrine tumors. Neuroendocrinology (2016) 103:153–71. doi: 10.1159/000443171
5. Garcia-Carbonero R, Sorbye H, Baudin E, Raymond E, Wiedenmann B, Niederle B, et al. ENETS consensus guidelines for high-grade gastroenteropancreatic neuroendocrine tumors and neuroendocrine carcinomas. Neuroendocrinology (2016) 103:186–94. doi: 10.1159/000443172
6. Bozkurt MF, Virgolini I, Balogova S, Beheshti M, Rubello D, Decristoforo C, et al. Guideline for PET/CT imaging of neuroendocrine neoplasms with (68)Ga-DOTA-conjugated somatostatin receptor targeting peptides and (18)F-DOPA. Eur J Nucl Med Mol imaging. (2017) 44:1588–601. doi: 10.1007/s00259-017-3728-y
7. Sundin A, Arnold R, Baudin E, Cwikla JB, Eriksson B, Fanti S, et al. ENETS consensus guidelines for the standards of care in neuroendocrine tumors: Radiological, nuclear medicine & hybrid imaging. Neuroendocrinology (2017) 105:212–44. doi: 10.1159/000471879
8. Cescato R, Schulz S, Waser B, Eltschinger V, Rivier JE, Wester HJ, et al. Internalization of sst2, sst3, and sst5 receptors: Effects of somatostatin agonists and antagonists. J Nucl Med (2006) 47:502–11.
9. Ben-Shlomo A, Schmid H, Wawrowsky K, Pichurin O, Hubina E, Chesnokova V, et al. Differential ligand-mediated pituitary somatostatin receptor subtype signaling: Implications for corticotroph tumor therapy. J Clin Endocrinol Metab (2009) 94:4342–50. doi: 10.1210/jc.2009-1311
10. Arnold R, Trautmann ME, Creutzfeldt W, Benning R, Benning M, Neuhaus C, et al. Somatostatin analogue octreotide and inhibition of tumour growth in metastatic endocrine gastroenteropancreatic tumours. Gut (1996) 38:430–8. doi: 10.1136/gut.38.3.430
11. Lesche S, Lehmann D, Nagel F, Schmid HA, Schulz S. Differential effects of octreotide and pasireotide on somatostatin receptor internalization and trafficking in vitro. J Clin Endocrinol Metab (2009) 94:654–61. doi: 10.1210/jc.2008-1919
12. Bruno JF, Xu Y, Berelowitz M. Somatostatin regulates somatostatin receptor subtype mRNA expression in GH3 cells. Biochem Biophys Res Commun (1994) 202:1738–43. doi: 10.1006/bbrc.1994.2136
13. Dörr U, Räth U, Sautter-Bihl ML, Guzman G, Bach D, Adrian HJ, et al. Improved visualization of carcinoid liver metastases by indium-111 pentetreotide scintigraphy following treatment with cold somatostatin analogue. Eur J Nucl Med (1993) 20:431–3. doi: 10.1007/bf00209003
14. Lodge MA, Solnes LB, Chaudhry MA, Wahl RL. Prospective within-patient assessment of the impact of an unlabeled octreotide pre-dose on the biodistribution and tumor uptake of (68)Ga DOTATOC as assessed by dynamic whole-body PET in patients with neuroendocrine tumors: Implications for diagnosis and therapy. Mol Imaging Biol (2021) 23:766–74. doi: 10.1007/s11307-021-01600-5
15. Haug AR, Rominger A, Mustafa M, Auernhammer C, Göke B, Schmidt GP, et al. Treatment with octreotide does not reduce tumor uptake of (68)Ga-DOTATATE as measured by PET/CT in patients with neuroendocrine tumors. J Nucl Med (2011) 52:1679–83. doi: 10.2967/jnumed.111.089276
16. Strosberg J, El-Haddad G, Wolin E, Hendifar A, Yao J, Chasen B, et al. Phase 3 trial of (177)Lu-dotatate for midgut neuroendocrine tumors. New Engl J Med (2017) 376:125–35. doi: 10.1056/NEJMoa1607427
17. Wängler C, Waser B, Alke A, Iovkova L, Buchholz HG, Niedermoser S, et al. One-step ¹18 F-labeling of carbohydrate-conjugated octreotate-derivatives containing a silicon-fluoride-acceptor (SiFA): In vitro and in vivo evaluation as tumor imaging agents for positron emission tomography (PET). Bioconjugate Chem (2010) 21:2289–96. doi: 10.1021/bc100316c
18. Beyer L, Gosewisch A, Lindner S, Völter F, Mittlmeier LM, Tiling R, et al. Dosimetry and optimal scan time of [(18)F]SiTATE-PET/CT in patients with neuroendocrine tumours. Eur J Nucl Med Mol Imaging (2021) 48 (11), 3571–81 . doi: 10.1007/s00259-021-05351-x
19. Ilhan H, Todica A, Lindner S, Boening G, Gosewisch A, Wängler C, et al. First-in-human (18)F-SiFAlin-TATE PET/CT for NET imaging and theranostics. Eur J Nucl Med Mol imaging. (2019) 46:2400–1. doi: 10.1007/s00259-019-04448-8
20. Ilhan H, Lindner S, Todica A, Cyran CC, Tiling R, Auernhammer CJ, et al. Biodistribution and first clinical results of (18)F-SiFAlin-TATE PET: A novel (18)F-labeled somatostatin analog for imaging of neuroendocrine tumors. Eur J Nucl Med Mol imaging. (2020) 47:870–80. doi: 10.1007/s00259-019-04501-6
21. WHO. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. J Int bioethique = Int J bioethics (2004) 15:124–9.
22. Schirrmacher R, Bradtmöller G, Schirrmacher E, Thews O, Tillmanns J, Siessmeier T, et al. 18F-labeling of peptides by means of an organosilicon-based fluoride acceptor. Angewandte Chemie (International ed English) (2006) 45:6047–50. doi: 10.1002/anie.200600795
23. Hope TA, Calais J, Zhang L, Dieckmann W, Millo C. (111)In-pentetreotide scintigraphy versus (68)Ga-DOTATATE PET: Impact on krenning scores and effect of tumor burden. J Nucl Med (2019) 60:1266–9. doi: 10.2967/jnumed.118.223016
24. Krenning EP, Valkema R, Kooij PP, Breeman WA, Bakker WH, deHerder WW, et al. Scintigraphy and radionuclide therapy with [indium-111-labelled-diethyl triamine penta-acetic acid-D-Phe1]-octreotide. Ital J Gastroenterol hepatology. (1999) 31 Suppl 2:S219–23.
25. Aalbersberg EA, de Wit-van der Veen BJ, Versleijen MWJ, Saveur LJ, Valk GD, Tesselaar MET, et al. Influence of lanreotide on uptake of (68)Ga-DOTATATE in patients with neuroendocrine tumours: A prospective intra-patient evaluation. Eur J Nucl Med Mol imaging. (2019) 46:696–703. doi: 10.1007/s00259-018-4117-x
26. Reubi JC, Waser B, Cescato R, Gloor B, Stettler C, Christ E. Internalized somatostatin receptor subtype 2 in neuroendocrine tumors of octreotide-treated patients. J Clin Endocrinol Metab (2010) 95:2343–50. doi: 10.1210/jc.2009-2487
27. Waser B, Tamma ML, Cescato R, Maecke HR, Reubi JC. Highly efficient in vivo agonist-induced internalization of sst2 receptors in somatostatin target tissues. J Nucl Med (2009) 50:936–41. doi: 10.2967/jnumed.108.061457
28. Janson ET, Kälkner KM, Eriksson B, Westlin JE, Oberg K. Somatostatin receptor scintigraphy during treatment with lanreotide in patients with neuroendocrine tumors. Nucl Med Biol (1999) 26:877–82. doi: 10.1016/s0969-8051(99)00059-1
Keywords: NET, PET/CT, [18F]SiTATE, somatostatin analogues, somatostatin receptor, molecular imaging
Citation: Eschbach RS, Hofmann M, Späth L, Sheikh GT, Delker A, Lindner S, Jurkschat K, Wängler C, Wängler B, Schirrmacher R, Tiling R, Brendel M, Wenter V, Dekorsy FJ, Zacherl MJ, Todica A, Ilhan H, Grawe F, Cyran CC, Unterrainer M, Rübenthaler J, Knösel T, Paul T, Boeck S, Westphalen CB, Spitzweg C, Auernhammer CJ, Bartenstein P, Unterrainer LM and Beyer L (2023) Comparison of somatostatin receptor expression in patients with neuroendocrine tumours with and without somatostatin analogue treatment imaged with [18F]SiTATE. Front. Oncol. 13:992316. doi: 10.3389/fonc.2023.992316
Received: 12 July 2022; Accepted: 09 January 2023;
Published: 30 January 2023.
Edited by:
Guillaume Nicolas, University Hospital of Basel, SwitzerlandReviewed by:
Håkan Geijer, Örebro University, SwedenMalgorzata Trofimiuk-Muldner, Jagiellonian University Medical College, Poland
Copyright © 2023 Eschbach, Hofmann, Späth, Sheikh, Delker, Lindner, Jurkschat, Wängler, Wängler, Schirrmacher, Tiling, Brendel, Wenter, Dekorsy, Zacherl, Todica, Ilhan, Grawe, Cyran, Unterrainer, Rübenthaler, Knösel, Paul, Boeck, Westphalen, Spitzweg, Auernhammer, Bartenstein, Unterrainer and Beyer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leonie Beyer, bGVvbmllLmJleWVyQG1lZC51bmktbXVlbmNoZW4uZGU=
†These authors have contributed equally to this work