
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
METHODS article
Front. Oncol., 09 January 2024
Sec. Genitourinary Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1334183
This article is part of the Research TopicThe Need for Pragmatic Trials in Genitourinary OncologyView all 3 articles
 Beth Russell1*
Beth Russell1* Poppy Leech1
Poppy Leech1 Harriet Wylie1
Harriet Wylie1 Charlotte Louise Moss1
Charlotte Louise Moss1 Anna Haire1
Anna Haire1 Deborah Enting2Suzanne Amery2Kathryn Chatterton2
Deborah Enting2Suzanne Amery2Kathryn Chatterton2 Muhammad Shamim Khan2Ramesh Thurairaja2Rajesh Nair2Sachin Malde2
Muhammad Shamim Khan2Ramesh Thurairaja2Rajesh Nair2Sachin Malde2 Kate Smith2
Kate Smith2 Cheryl Gillett3Debra Josephs2Elias Pintus2Sarah Rudman2Simon Hughes2Clare Relton4
Cheryl Gillett3Debra Josephs2Elias Pintus2Sarah Rudman2Simon Hughes2Clare Relton4 Mieke Van Hemelrijck1
Mieke Van Hemelrijck1Purpose: The Graham Roberts Study was initiated in 2018 and is the first Trials Within Cohorts (TwiCs) study for bladder cancer. Its purpose is to provide an infrastructure for answering a breadth of research questions, including clinical, mechanistic, and supportive care centred questions for bladder cancer patients.
Participants: All consented patients are those aged 18 or older, able to provide signed informedconsent and have a diagnosis of new or recurrent bladder cancer. All patients are required to have completed a series of baseline questionnaires. The questionnaires are then sent out every 12 months and include information on demographics and medical history as well as questionnaires to collect information on quality of life, fatigue, depression, overall health, physical activity, and dietary habits. Clinical information such as tumor stage, grade and treatment has also been extracted for each patient.
Findings to date: To date, a total of 125 bladder cancer patients have been consented onto the study with 106 filling in the baseline questionnaire. The cohort is made up of 75% newly diagnosed bladder cancer patients and 66% non-muscle invasive bladder cancer cases. At present, there is 1-year follow-up information for 70 patients, 2-year follow-up for 57 patients, 3-year follow-up for 47 patients and 4-year follow-up for 19 patients.
Future plans: We plan to continue recruiting further patients into the cohort study. Using the data collected within the study, we hope to carry out independent research studies with a focus on quality of life. We are also committed to utilizing the Roberts Study Cohort to set up and commence an intervention. The future studies and trials carried out using the Roberts Cohort have the potential to identify and develop interventions that could improve the prevention, diagnosis, and treatment of bladder cancer.
The Graham Roberts Study (Roberts Study), initiated in 2018, presents as the first Trials Within Cohorts (TwiCs) study for bladder cancer, designed to provide an infrastructure for answering a breadth of research questions, including clinical, mechanistic, and supportive care centred questions for bladder cancer patients (1). A detailed description of the study design has been published previously (1).
The study uses the TwiCs study design, introduced by Relton et al. (2), to obtain a cohort of patients with a new or recurrent diagnosis of bladder cancer. Patients are recruited at Guys and St Thomas’ (GSTT) National Health Service (NHS) Foundation Trust in London. Eligible patients have a basic understanding of the English language, are over the age of 18 and may have been referred to GSTT from secondary and tertiary hospitals across the UK.
All eligible patients who have already undergone diagnostic investigations and informed about a (highly likely) bladder cancer receive detailed written information about the Roberts Study while attending the Urology Centre for their initial appointment. The study uses a staged and tailored approach to informed consent. Prior to their first appointment with the consultant (urology or oncology) consent is sought to take part in the cohort and longitudinal study, to participate in the intervention arm of any future RCT, to be randomly selected to the control arm of any future RCT without further notification, to collection and storage of biological samples, including blood, urine and tissue, and linkage to routinely collected clinical data as recorded in electronic patient records.
The Graham Roberts Study collects health-related quality of life (HRQoL) patient-reported outcomes every twelve months using questionnaires that address: an assessment of bladder cancer illness, fatigue, depression, generic health status, physical activity, and diet quality.
The asymmetric informed consent nature of this study means that randomization can be proceeded by asymmetric treatment for two arms, where participants within the intervention arm will provide informed consent, and those in the control arm use the consent broadly disclosed before randomization. As such, the participants have a detailed understanding of prospective studies within the cohort before participation.
The purpose of this cohort profile is to describe the baseline demographic and medical history information for the patient cohort which have been recruited into the Roberts Study thus far including further information on their clinical and treatment characteristics.
The first patient was consented onto the Graham Roberts Study on 7th March 2018. To date (October 2023), a total of 125 bladder cancer patients have been consented onto the study with all participants presenting a recent diagnosis of bladder cancer, whether this be a new diagnosis or a diagnosis of a recurrence. Nineteen patients did not complete the baseline questionnaire (15%). As completion of the baseline questionnaire was a pre-requisite for participation in this study, 106 consented patients were included in the study.
Information on the patients’ demographic information collected within the questionnaires includes age, sex, ethnicity, marital status, employment status, living arrangements and education level. Information regarding socioeconomic status was collected using the English indices of deprivation 2019 online tool (3). Postcodes were converted into indices of multiple deprivation (IMD) deciles. The IMD deciles were then converted to quintiles, with 1 being the most deprived and 5 being the least deprived.
Information on the medical history of the patients collected using the questionnaires includes their personal history with cancer and any family history with cancer (including both all cancers and bladder cancer specifically). Furthermore, information on bladder cancer related symptoms is collected such as history of nephritic colic, or kidney, renal or bladder stones, bladder or kidney infections, issues with urination and any history of an enlarged prostate (for the males only).
As well as the questionnaires on demographical factors and medical history, information was collected on the patients’ alcohol and smoking habits. Further to this, patient reported outcomes (PROs) have been collected utilizing the following validated questionnaires:
● QoL: Functional Assessment of Chronic Illness Therapy for Bladder Cancer (4).
● Fatigue: Functional Assessment of Chronic Illness Therapy-Fatigue (5).
● Depression: Patient Health Questionnaire-9 (6).
● Health: Standardized instrument for use as a measure of health outcome (EQ-5D-5L10) (7).
● Physical activity: Short Questionnaire to Assess Health-Enhancing Physical Activity (8).
● Assessment of dietary habits: Short Questionnaire to Assess Diet Quality (9).
The items were collected as 5-point Likert scales, objective responses, and free-text answers. A summary of the items collected is outlined in Table 1. Due to the large quantity of data points a summary of this information is out of the scope of this current cohort profile.
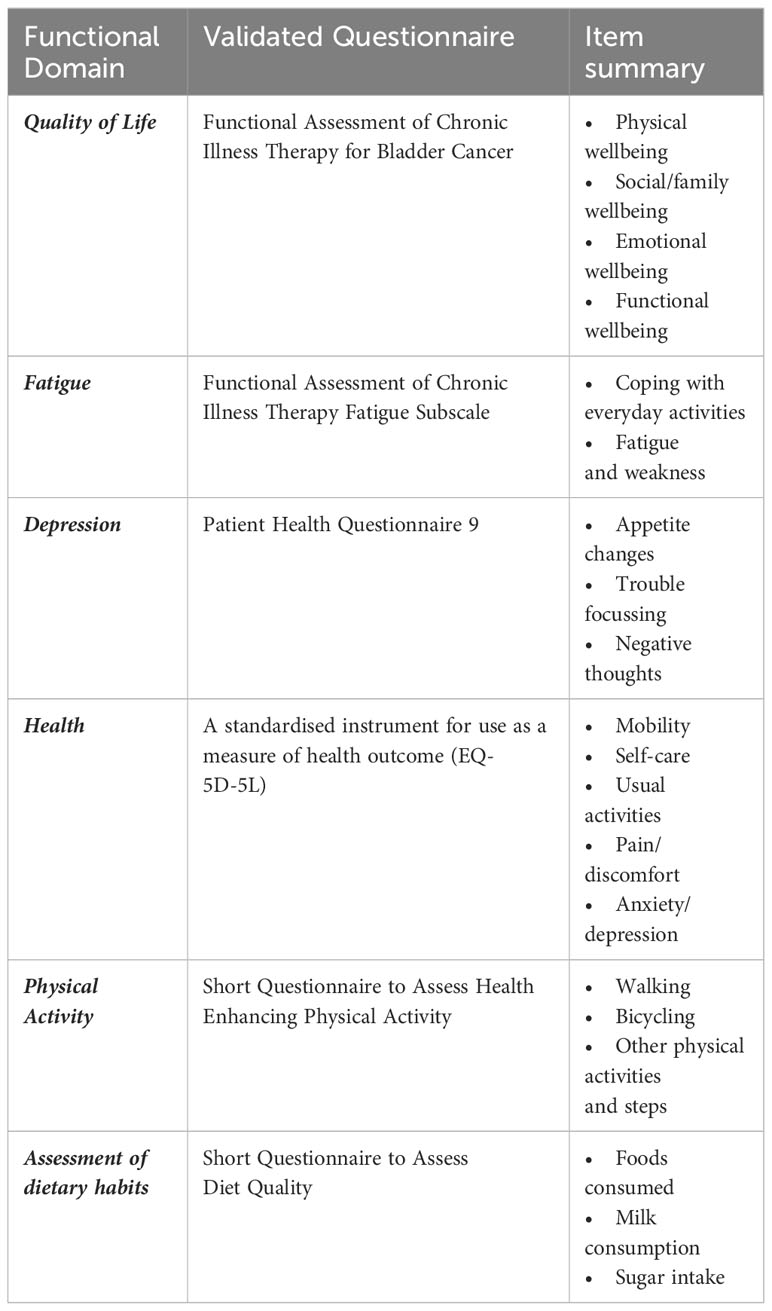
Table 1 Description of PROMs collected within the Graham Roberts Study.
No clinical information is collected directly from patients via the Roberts study questionnaires themselves. In order to collate this information for the cohort profile, the electronic health records for each patient are searched to extract the baseline clinical and treatment information for all study participants. Clinical staging information collected included tumor (T), nodal (N) and metastases (M) stages identified within imaging, the staging from the transurethral resection of the bladder tumor (TURBT) as well as the grade and CIS involvement. Treatment information extracted included the treatment paradigm such as radical, surveillance, neo-adjuvant and palliative, and the treatment modality such as cystectomy, systemic chemotherapy, laser ablation, immunotherapy, radiotherapy, intravesical therapy and neoadjuvant chemotherapy (NAC) with cystectomy.
The questionnaires are sent to all eligible consented patients every 12 months. At the point of consent, patients give their preference as to whether they would prefer the questionnaires to be sent via email or in the post. Given the study was initiated in 2018, at present, there is a maximum of four successive follow-ups. Throughout this study time frame, 13 (12%) patients have died, and 6 (6%) have withdrawn consent. As shown in Figure 1, we have 1-year follow-up information for 70 patients, 2-year follow-up for 57 patients, 3-year follow-up for 47 patients and 4-year follow-up for 19 patients.

Figure 1 Survey population response rates.
Overall 106 patients completed the baseline questionnaire, most of which (79%) were male (Table 2). In terms of ethnicity 88% of study participants were While/Caucasian, 6% Black/Afro-Caribbean, 1% Asian and 4% other ethnic backgrounds. The majority of patients were married (55%) and/or lived with a partner (66%). Only 9% of patients were in the first (most deprived) quintile, with the majority of patients either being in the second (29%) or third (26%) quintile. When asked about their employment status, 62% were retired and 32% were in some sort of full or part time work. Two thirds of the study participants reported to have been a regular smoker at some point in their life (66%).
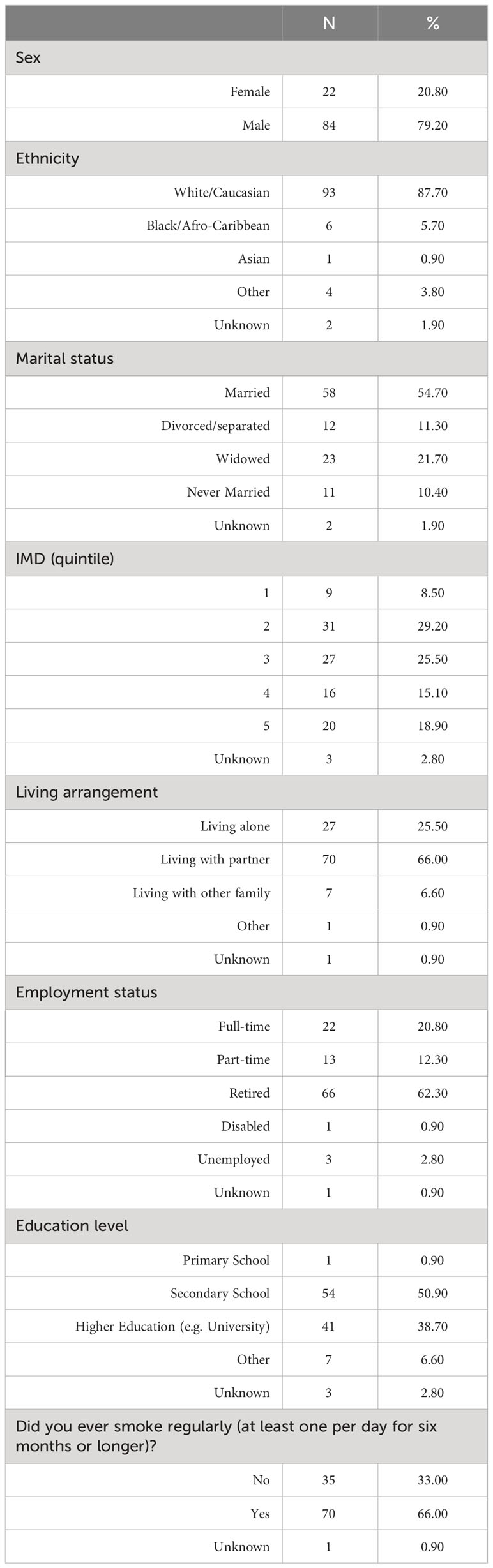
Table 2 Demographic baseline characteristics of the Roberts study cohort.
One quarter (24%) of study participants reported a history of cancer, 58% said they had a family history of cancer and 9% a family history of bladder cancer (Table 3). With regards to bladder cancer symptoms, 39% had a history of bladder infections with the highest proportion of these stating they had experienced the infection 1-2 times (39%). Most patients did not have a history of nephritic colic, or kidney, renal or bladder stones. The majority of patients did however say they experienced a difficulty in starting or stopping urinating or an increased frequency of urinating during the night (56%). Of the 84 men in the study, 29% reported to have had a history of an enlarged prostate.
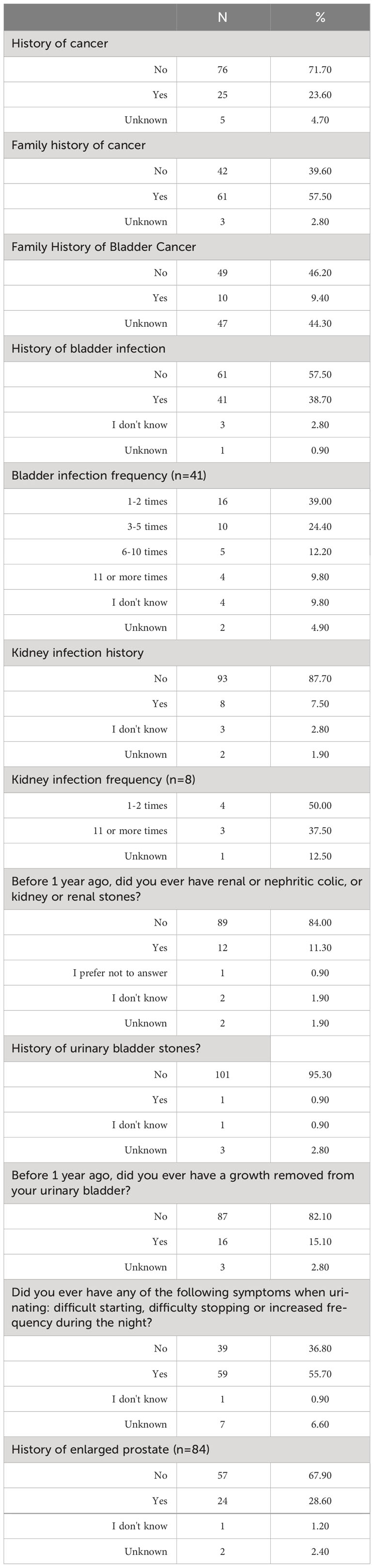
Table 3 Medical History information of the Roberts Study Cohort.
When looking at the clinical characteristics of the study cohort, 75% of the patients recruited into the Roberts study were newly diagnosed with bladder cancer, whilst 25% were patients who had been diagnosed with recurrent bladder cancer (Table 4). Two thirds of patients had non-muscle invasive disease (66%) with the remaining patients diagnosed with muscle invasive (33%). From the imaging, only a very small proportion of patients were metastatic (4%) and/or had lymph node involvement (9%). Just under half of the patients had carcinoma in situ (CIS) (46%) and most patients were deemed to have high grade tumors (89%).
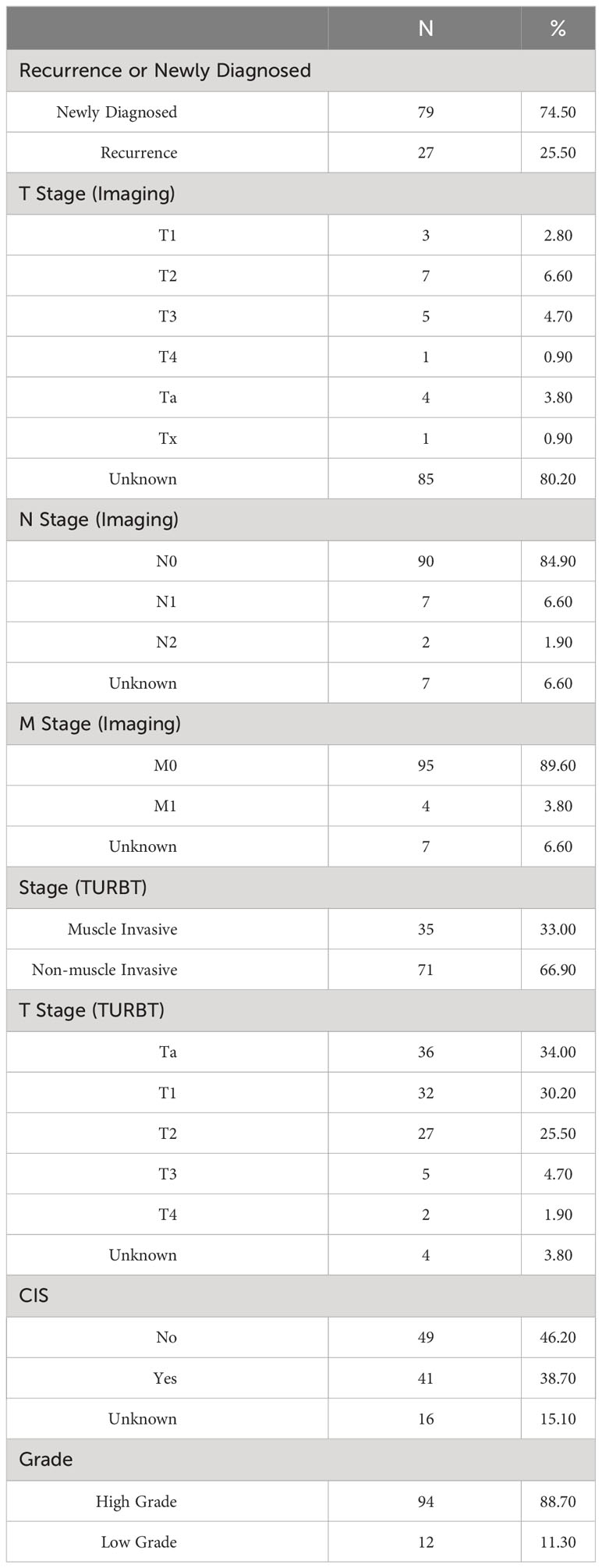
Table 4 Clinical Characteristics of the Roberts Study Cohort .
When appraising treatment paradigm, most patients were undergoing radical or curative treatments (78%) (Table 5). Fifteen percent of patients were under surveillance with a small proportion undergoing palliative (3%) or neoadjuvant therapy (3%). The treatments by NMIBC and MIBC are depicted in Figure 2. Of the MIBC patients, the overwhelming majority had undergone a cystectomy (66%), with a further 14% having undergone neoadjuvant chemotherapy (NAC) and a cystectomy. A small proportion of patients had received systemic chemotherapy (11%), or radiotherapy (6%) and one patient had received immunotherapy (3%). In the NMIBC cohort, of those undergoing active treatment, half of the patients had undergone intravesical therapy (the full breakdown of which can be found in Table 5) and almost half had undergone a cystectomy (46%). The remaining patients had either undergone NAC and a cystectomy (2%) or systemic chemotherapy (2%).
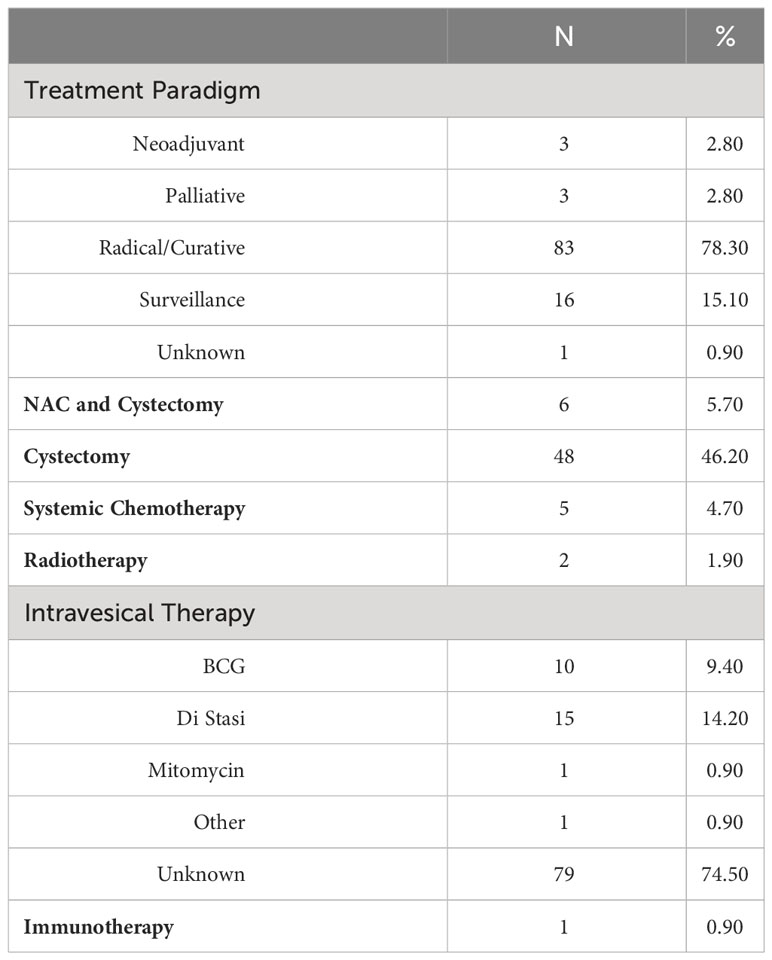
Table 5 Treatment information for the Roberts Study Cohort.
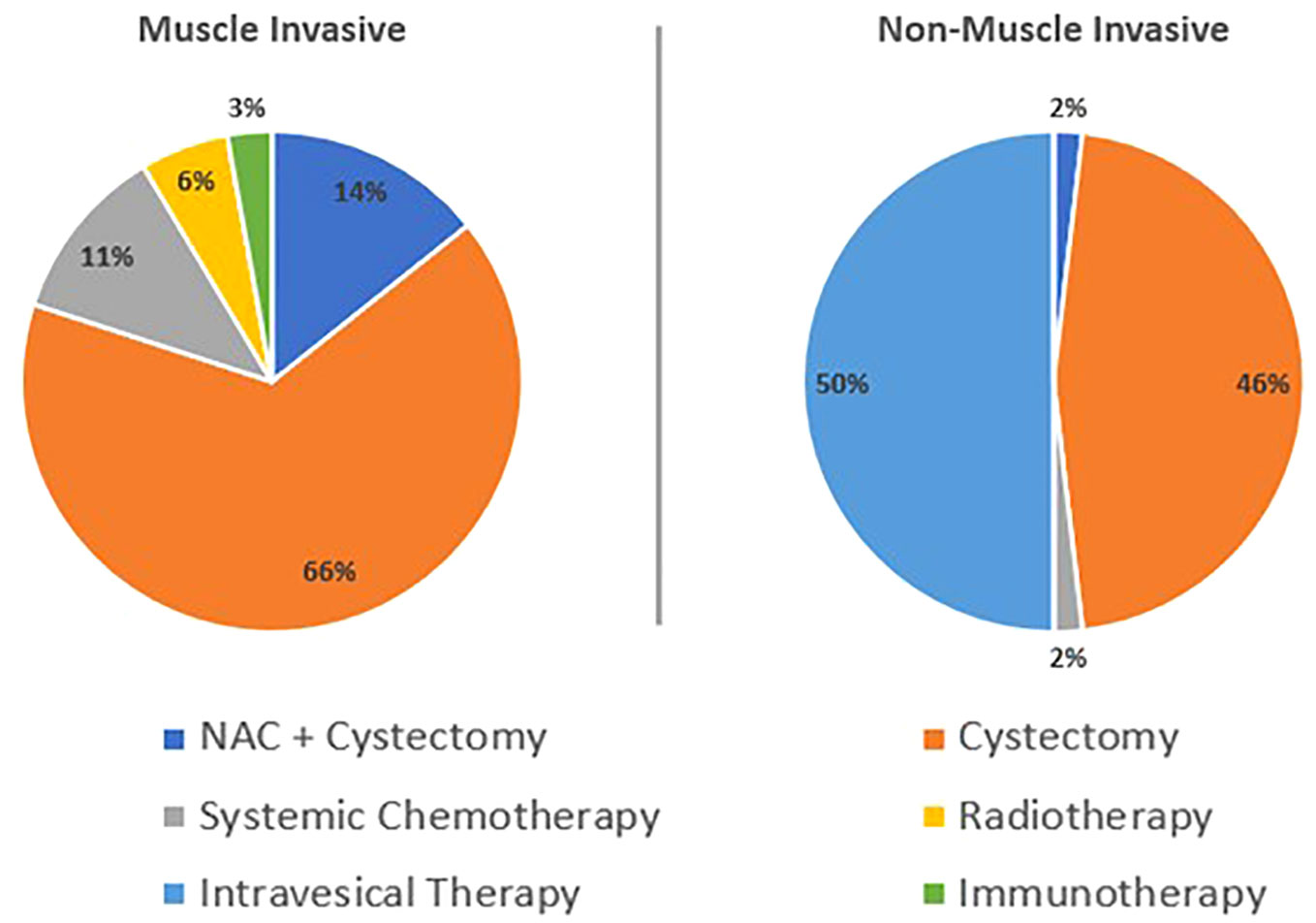
Figure 2 Treatment by Non-Muscle Invasive Bladder Cancer and Muscle Invasive Bladder Cancer.
The Graham Roberts study provides a unique opportunity to conduct multiple pragmatic trials within the cohort. One advantage of the trials within cohorts design is that that patients randomly assigned to usual care do not need to be recontacted as they have already given broad consent prior to randomization. The Graham Roberts study collects a wide range of PROMs on quality of life and lifestyle factors including diet and physical activity. When paired with the clinical information, this gives the opportunity to look at potential associations between clinical factors and treatments with quality-of-life outcomes. This provides the opportunity to address a wide range of research questions from one cohort, a strength that will only continue to grow over time as more patients recruited and longer-term follow-up data is accrued.
Despite running since 2018, we are yet to initiate a trial with a TwiCS design within the Roberts Study. This is mainly due to the COVID-19 pandemic, which, like many studies, put a halt to both recruitment and progression of the study. Furthermore, the recruitment target is somewhat below the original target set out in our first paper (1), owing to the interruption of services and an inability to recruit patients during the pandemic. From previous experiences, we are also aware that introducing interventions can often take longer than first planned (10). However, we are committed to the introduction and initiation of a TwiCS trial in the near future. Our focus for this is likely to be in the mental wellbeing space given the growing interest and emphasis on this important research area (11).
We acknowledge that the number of study participants decreases with each follow-up for reasons other than death or withdrawals from the study. One is that as patients are still being recruited into the study, not all patients have reached each follow-up yet. Another reason is that patients don’t always return their questionnaires straight away or sometimes at all. To address this decrease in adherence, the study team will start sending reminders to patients to fill in their questionnaires. During this process, we will also try and gain an understanding as to why patients are no longer returning their questionnaires and will work on solutions to resolve this. The cohort of patients so far included within the Roberts study are representative of the bladder cancer patients seen at our institution in South-East London. Furthermore, the TwiCS trial design presents several advantages over the traditional randomized controlled trial (RCT) method. Firstly, it addresses the difficulties in recruiting patients onto trials, by capitalizing on the nature of observational cohort studies being easier and less selective (12). Additionally, it means that prospective trials within the cohort do not require further recruitment efforts. In fact, a recent study revealed that recruitment for RCTs within these established cohorts is more efficient when compared with traditional recruitment without cohorts (13). A further advantage of the TwiCs study design is how obtaining informed consent can be tailored to the relevant needs of each participant. As such the TwiCS design is patient-centred, offering a process for gaining informed consent that mirrors the real-world routine in healthcare, where patients are not told about treatments that they are not offered.
The Roberts Study is the first study within bladder cancer using a ‘trials within cohorts’ study design. The data collected within the study is broad and rich and can be used independently to conduct research studies, including studies exploring the quality of life. We hope that this study will help identify and develop interventions to improve the prevention, diagnosis, and treatment of bladder cancer in the future.
The datasets presented in this article are not readily available due to patient anonymity. Requests to access the datasets should be directed to the corresponding author.
The studies involving humans were approved by London–Fulham Research Ethics Committee as part of gaining Health Research Authority approval (17/LO/1975). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
BR: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. PL: Data curation, Writing – review & editing. HW: Data curation, Project administration, Validation, Writing – review & editing. CM: Project administration, Validation, Writing – review & editing. AH: Data curation, Project administration, Validation, Writing – review & editing. DE: Data curation, Writing – review & editing. SA: Writing – review & editing. KC: Writing – review & editing. MK: Writing – review & editing. RT: Writing – review & editing. RN: Writing – review & editing. SM: Writing – review & editing. KS: Writing – review & editing. CG: Writing – review & editing. DJ: Writing – review & editing. EP: Writing – review & editing. SR: Writing – review & editing. SH: Writing – review & editing. CR: Writing – review & editing. MV: Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Funding for the initial set up of the study was kindly provided by the Graham and Dianne Roberts Charitable Settlement.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wylie H, Cahill F, Santaolalla A, Moss CL, Enting D, Amery S, et al. Graham Roberts Study protocol: First “trials within cohort study” for bladder cancer. BMJ Open (2019) 9(9):1–5. doi: 10.1136/bmjopen-2019-029468
2. Relton C, Torgerson D, O’Cathain A, Nicholl J. Rethinking pragmatic randomised controlled trials: Introducing the “cohort multiple randomised controlled trial” design. BMJ [Internet] (2010) 340(7753):963–7. doi: 10.1136/bmj.c1066
3. Office of National Statistics. English Indices of Deprivation 2020 (2011). Available at: https://www.gov.uk/government/statistics/english-indices-of-deprivatio-2010.
4. Cella D. Manual of the functional assessment of chronic illness therapy (FACIT) scales version 4.0. (1997).
5. Lai J-S, Cella D, Chang C-H, Bode RK, Heinemann WAW. Item banking to improve, shorten and computerize self-reported fatigue: An illustration of steps to create a core item bank from the FACIT-Fatigue Scale. Qual Life Res (2003) 12(5):485–501. doi: 10.1023/A:1025014509626
6. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
7. Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res (2011) 20(10):1727–36. doi: 10.1007/s11136-011-9903-x
8. Wendel-Vos GCW, Schuit AJ, Saris WHM, Kromhouta D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J Clin Epidemiol (2003) 56(12):1163–9. doi: 10.1016/S0895-4356(03)00220-8
9. Robinson SM, Jameson KA, Bloom I, Ntani G, Crozier SR, Syddal H, et al. Development of a short questionnaire to assess diet quality. J Nutr Heal Aging (2017) 21(3):247–53. doi: 10.1007/s12603-016-0758-2
10. Bessa A, Bosco C, Cahill F, Russell B, Fox L, Moss C, et al. Designing a pragmatic intervention to help improve the bladder cancer patient experience. Inq (United States) (2021) 58:1–8. doi: 10.1177/00469580211030217
11. Haire A, Russell B, Stewart R, Enting D, Khan MS, Malde S, et al. Investigating the interplay between a Bladder Cancer (BC) Diagnosis and subsequent contact with Mental Health Services in a local BC population. In: BAUN (2023).
12. Hayward RA, Porcheret M, Mallen CD, Thomas E. Recruiting patients and collecting data for an observational study using computerised record pop-up prompts: the PROG-RES study. Prim Health Care Res Dev (2013) 14:21–28. doi: 10.1017/S1463423612000047
Keywords: trials within cohorts, cohort profile, non-muscle invasive bladder cancer (NMIBC), muscle invasive bladder cancer (MIBC), questionnaires
Citation: Russell B, Leech P, Wylie H, Moss CL, Haire A, Enting D, Amery S, Chatterton K, Khan MS, Thurairaja R, Nair R, Malde S, Smith K, Gillett C, Josephs D, Pintus E, Rudman S, Hughes S, Relton C and Van Hemelrijck M (2024) A cohort profile of the Graham Roberts study cohort. Front. Oncol. 13:1334183. doi: 10.3389/fonc.2023.1334183
Received: 06 November 2023; Accepted: 11 December 2023;
Published: 09 January 2024.
Edited by:
Parthasarathy Seshacharyulu, University of Nebraska Medical Center, United StatesReviewed by:
Marco Maruzzo, Veneto Institute of Oncology (IRCCS), ItalyCopyright © 2024 Russell, Leech, Wylie, Moss, Haire, Enting, Amery, Chatterton, Khan, Thurairaja, Nair, Malde, Smith, Gillett, Josephs, Pintus, Rudman, Hughes, Relton and Van Hemelrijck. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Beth Russell, YmV0aC5ydXNzZWxsQGtjbC5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.