 Aaron Tsumura
Aaron Tsumura Daniel Levis
Daniel Levis Joseph M. Tuscano
Joseph M. Tuscano
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 17 October 2023
Sec. Hematologic Malignancies
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1288172
This article is part of the Research Topic Checkpoint Inhibition in Hematologic Malignancies View all 8 articles
Checkpoint inhibitor therapy has emerged as an effective therapeutic strategy for many types of malignancies, especially in solid tumors. Within the last two decades, numerous monoclonal antibody drugs targeting the CTLA-4 and PD-1/PD-L1 checkpoint pathways have seen FDA approval. Within hematologic malignancies, Hodgkin Lymphoma has seen the greatest clinical benefits thus far with more recent data showing efficacy in the front-line setting. As our understanding of checkpoint inhibition expands, using these pathways as a therapeutic target has shown some utility in the treatment of other hematologic malignancies as well, primarily in the relapsed/refractory settings. Checkpoint inhibition also appears to have a role as a synergistic agent to augment clinical responses to other forms of therapy such as hematopoietic stem cell transplant. Moreover, alternative checkpoint molecules that bypass the well-studied CTLA-4 and PD-1/PD-L1 pathways have emerged as exciting new therapeutic targets. Most excitingly is the use of anti-CD47 blockade in the treatment of high risk MDS and TP-53 mutated AML. Overall, there has been tremendous progress in understanding the benefits of checkpoint inhibition in hematologic malignancies, but further studies are needed in all areas to best utilize these agents. This is a review of the most recent developments and progress in Immune Checkpoint Inhibition in Hematologic Malignancies in the last decade.
One of the primary hallmarks of malignancy is a tumor cell’s ability to resist cell death (1). The inhibitory molecules cytotoxic T lymphocyte-associated protein (CTLA-4) and programmed cell death protein 1 and its ligand (PD-1 and PD-L1, respectively) are well-studied signaling molecules that serve in controlling T-cell activation, maturation, and viability. CTLA-4 on the naïve T-cell membrane competes with CD28 to bind CD80 on the antigen presenting cell (APC) and is thought to regulate T-cell function early in the immune response (2). PD-1 on the activated T-cell binds its ligand PD-L1 on the APC and represses stimulatory signaling, leading to anergy, apoptosis, and differentiation to Regulatory T-cells (Tregs). This interaction occurs later in the immune response and within peripheral tissues (2, 3). By targeting these pathways and inhibiting suppressive immune checkpoint effects, Immune Checkpoint Inhibitors (ICI) has proven to be effective for many hematologic malignancies both in the front-line and relapse/refractory setting. ICI therapy has also shown benefit as adjunctive therapy with other treatment modalities such as Hematopoietic Stem Cell Transplant, Chimeric Antigen Receptor T-Cell Therapy, and Radiation Therapy. More recently, newer immune checkpoint molecules have been discovered and serve as promising alternative targets for ICI in Hematologic Malignancies as well. This is a comprehensive review of the current state of ICI in Hematologic Malignancies.
Of all hematologic malignancies, Hodgkin Lymphoma (HL) has seen the largest benefit in ICI-based therapy thus far, especially in the relapsed/refractory (r/r) setting. The major immunosuppressive effector cells present in the Tumor Microenvironment (TME) of HL appear to be exhausted PD-1+ Th1 effector cells and active PD-1- Th1 Tregs (4). The primary malignant cell, the Reed-Sternberg cell, also has higher PD-L1 expression and lower Major Histocompatibility Complex-1 (MHC1) expression, while also having a higher concentration of surrounding CTLA-4+ CD4 T-cells (4, 5). This is consistent with existing data supporting the benefit of ICI therapy for HL as highlighted in Table 1. Both the KEYNOTE-013 and KEYNOTE-087 trials have led to the approval of Pembrolizumab while the CheckMate 205 trial led to the approval of Nivolumab for the treatment of r/r HL after multiple lines of therapy, including after autologous hematopoietic stem cell transplant (autoHCT). Though overall response rates have been reported between 60-70%, most patients still relapse (6–8). Further systematic reviews assessing PD-1/PD-L1 inhibitors in r/r HL have measured a composite Objective Response Rate (ORR) of 79%, Complete Response (CR) of 44%, and Partial Response (PR) of 34% (9). The KEYNOTE-204 trial showed a median Progression Free Survival (PFS) of 13.2 months with Pembrolizumab salvage therapy for r/r HL after autoHCT (10). Additionally, patients with r/r HL who were treated with Nivolumab saw an ORR of 70% with a CR rate of 43.3% and median PFS of 18.4 months (11). Thus, ICI has shown remarkable efficacy in the treatment in r/r HL with reported ORR ranging between 60-70%, CR ranging between 40-45%, and PFS ranging between 13-18 months, even after autoHCT.
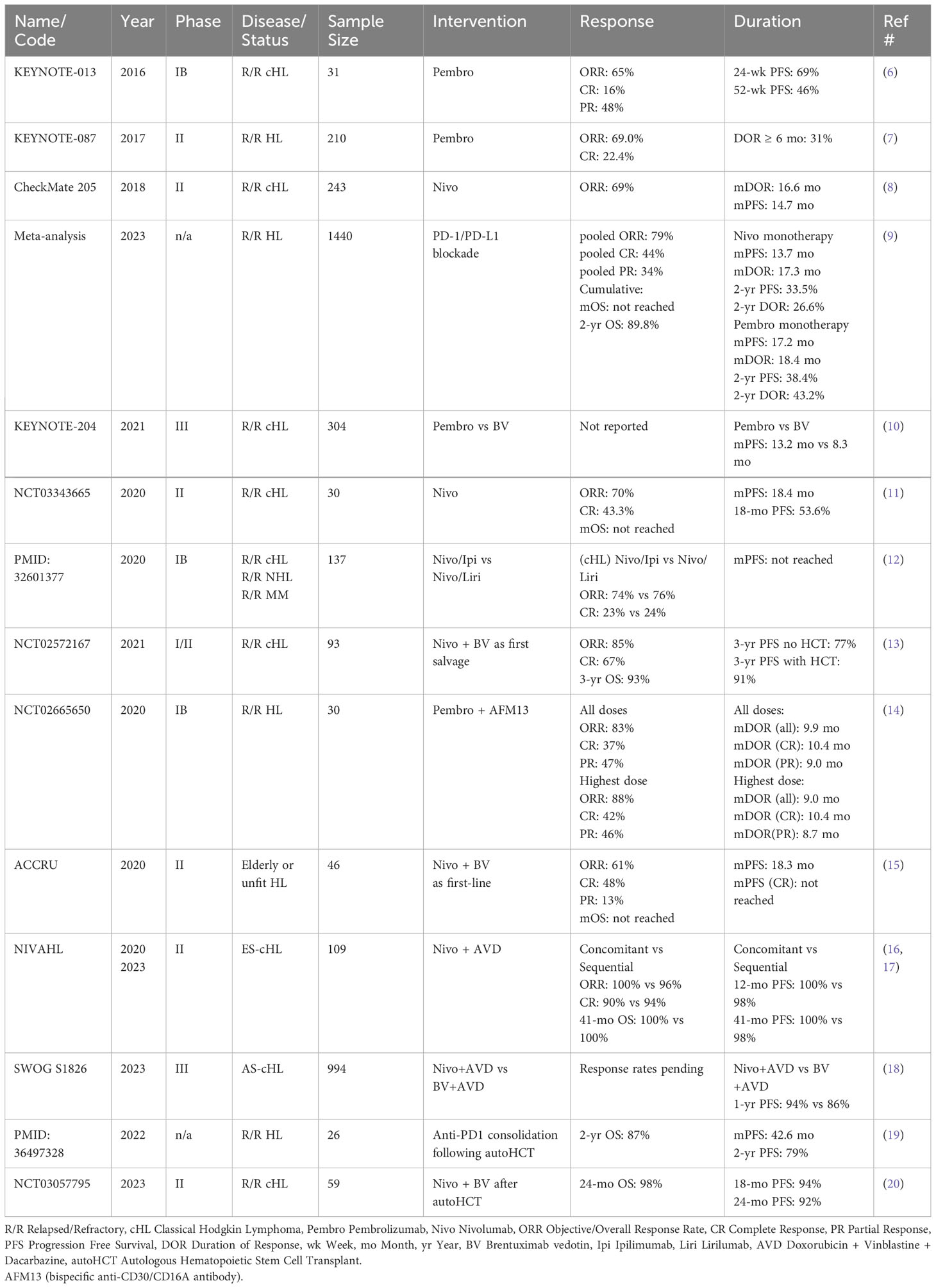
Table 1 Recent published trials evaluating CPI in HL.
While ICI monotherapy proves effective in the r/r setting, two critical knowledge gaps remain: whether ICI when used in combination therapies add additional outcome improvements and the optimal timing of ICI in relation to autoHCT. Armand et al. concluded that the addition of anti-CLTA-4 or anti-KIR to Nivolumab in treating r/r Classical HL (cHL) after autoHCT did not add benefit, but rather had higher rates of Treatment-Related Adverse Events (TRAEs). They report that though ORRs of the combinations Nivolumab/Ipilimumab (Nivo/Ipi) and Nivolumab/Lirilumab (Nivo/Liri) were 74% and 76%, respectively, rates of TRAE were 29% and 15%; higher than reported for Nivolumab alone (12). This data suggests no additional benefit to ICI use in combination therapies after autoHCT. Alternatively, there appears to be improved PFS rates when ICI is used as consolidative therapy with autoHCT, both as monotherapy and in combination. Filippi et al. report a median PFS of 42.6 months, 2-year PFS of 79%, and 2-year OS of 87% with consolidative Nivolumab or Pembrolizumab in high-risk HL with salvage autoHCT (19). Additionally, Herrera et al. report an 18-month PFS of 94% with consolidative combination Nivolumab with Brentuximab Vedotin after autoHCT (20). Thus this data would suggest a PFS benefit in using ICI as consolidative therapy following autoHCT. Furthermore, positive data also suggests improved outcomes with ICI-combination as first salvage therapy before autoHCT. Advani et al. report an 85% ORR, 67% CR, and 3-year PFS of 77% with combination Nivolumab with Brentuximab Vedotin as first salvage therapy for r/r cHL. They further report that patients who proceeded to autoHCT had an improved 3-year PFS to 91% and 3-year OS of 93% (13). Bartlett et al. reported a secondary endpoint of an 88% ORR in a heavily pretreated patient population treated with a combination of Pembrolizumab with a bispecific anti-CD30/CD16A antibody (AFM13) (14). Thus, current available data would suggest that ICI-combination therapy has greater outcome benefits when used either before autoHCT or as a consolidative regimen with autoHCT, but provides no further benefit as compared to ICI monotherapy when used as salvage therapy after autoHCT.
ICI-combination therapies are also being evaluated as first-line therapy and have shown very promising improvement in outcomes. The ACCRU trial evaluated Nivolumab plus Brentuximab Vedotin as first-line therapy for older and chemotherapy-ineligible HL patients. Although the trial was closed due to failure to meet predefined criteria, analysis of the 46 enrolled patients showed a CR rate of 48%, and PR of 13%, giving an ORR of 61%. This suggests that although combination immunotherapy may be active in older patients and patients with comorbidities, further dosing and scheduling optimization is needed (15). More significantly, the NIVAHL trial evaluated Nivolumab in combination with Doxorubicin, Vinblastine, and Dacrabazine (N-AVD) as first-line therapy for early-stage unfavorable cHL. Patients with newly diagnosed cHL were randomized to 4 cycles of concomitant N-AVD or sequentially administered 4 doses of Nivolumab followed by 2 cycles of N-AVD followed by 2 cycles of AVD alone. Each group then received 30-Gy radiation to affected sites. Initial analysis published in 2020 reported CR rates of 90% for the concomitant group and 94% for the sequential group. 12-month PFS was 100% for the concomitant group and 98% for the sequential group (16). The investigators reported their final analysis in early 2023 showing that at a median follow-up of 41 months, OS was 100% in both groups. PFS rate at last follow-up remained 100% and 98% for the concomitant and sequential groups, respectively (17). A separate analysis of the study population showed a sustained decrease in exhausted T-cell phenotype in patients receiving anti-PD1 therapy (21). Furthermore, the SWOG S1826 trial compared N-AVD to Brentuximab vedotin-AVD (BV-AVD) as first-line in advanced stage cHL. Patients with stage 3-4 HL were randomized 1:1 to either 6 cycles of N-AVD or BV-AVD. 12-month PFS was significantly superior in the N-AVD arm at 94% vs 86% for the BV-AVD arm. 11 deaths were observed in the BV-AVD arm compared to 4 in the N-AVD arm (18). Longer follow-up is needed to assess OS, but with preliminary data showing response rates and OS rates ranging from 90-100%, this data is anticipated to be practice-changing.
Data thus far has shown that ICI therapy is remarkably effective in nearly all treatment settings of HL. A list of active studies is shown in Tables 2A, B evaluating ICI activity in both the front-line and relapsed/refractory settings, respectively. There have been an abundance of data supporting the efficacy and safety of ICI therapy in the treatment of r/r HL, especially after autoHCT. More recent trials have shown significant benefits when utilizing ICI therapy prior to autoHCT and as consolidative therapy with autoHCT. Most exciting, is data supporting ICI-combination as front-line therapy as shown with the addition of Nivolumab to upfront AVD for both early-stage and advanced-stage cHL, which could potentially change our front-line treatment paradigm.
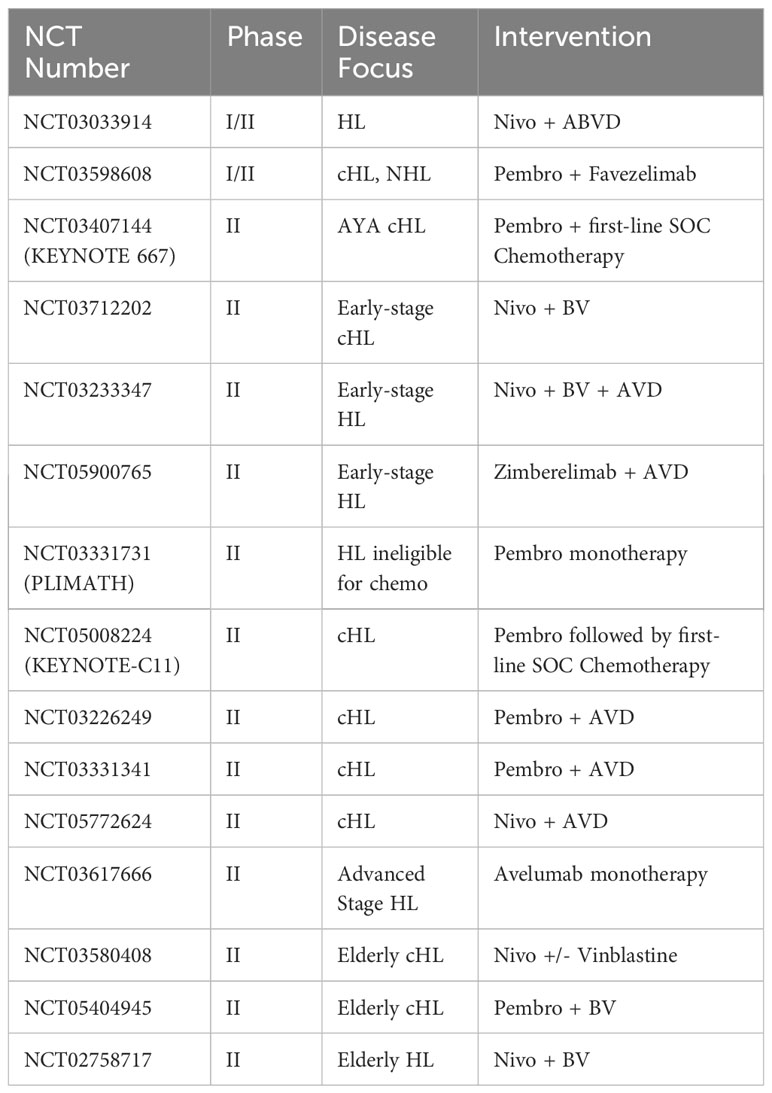
Table 2A Current clinical trials evaluating CPI in first-line treatment of HL.
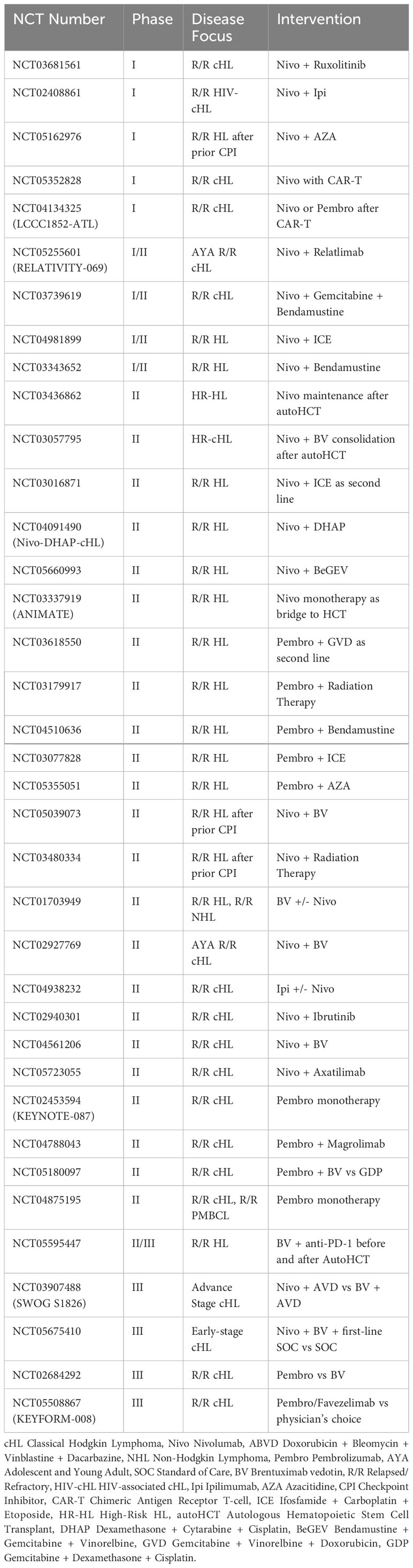
Table 2B Current clinical trials evaluating CPI in r/r HL.
Non-Hodgkin Lymphomas (NHL) have seen some benefit to ICI therapy, though not as robust as in HL, which is thought, in part, to be due to a differing milieu of tumor infiltrating immune cells. Diffuse Large B-Cell Lymphoma (DLBCL) is known to have lower expression of CD3+ and CD4+ tumor infiltrating lymphocytes (TILs) as well as lower PD-L1 expression as compared to HL (22). Studies have also shown that a higher ratio of CD4+/CD8+ T-cells to PD-L1 tumor expression is an independent predictor of better 4-year OS of DLBCL patients treated with Standard of Care (SOC) chemotherapy of Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisone (R-CHOP) (23, 24). This supports the idea that PD-L1 expression serves an important role in immune evasion and tumor proliferation while being an important predictive measure in responsiveness to ICI-based therapies. Reported ORRs of r/r DLBCL to ICI either as monotherapy or in combination therapy range from 9-20%. Alternatively, ORRs for r/r Follicular Lymphoma (FL) have been more variable and range from 10-60% while KEYNOTE-013 reported an ORR of 48% for r/r Primary Mediastinal B-cell Lymphoma (PMBL) (12, 25–27). Thus, the variable response rates in NHLs serve as basis for further optimization of ICI use in the treatment of these malignancies.
Newer data suggests a potential role in treating Richter Transformation-DLBCL (RT-DLBCL). Studies have shown an upwards of 40% of RT-DLBCL tumors have >50% PD-1/PD-L1 expression, and >60% of tumors have >20% PD-1+ TILs. These patients also tended to have significantly better OS compared to those who had lower PD-1+ TILs (28). Jain et al. saw an ORR of 42% with a median Duration of Response (DOR) of 15 months in RT-DLBCL patients treated with Nivolumab and Ibrutinib. Median OS was 13 months (29). More notably, Herrera et al. evaluated the addition of Atezolizumab to immunogenic chemoimmunotherapy, Rituximab with Gemcitabine and Oxaliplatin (R-GEMOX) in treating RT-DLBCL from either B-NHL or Chronic Lymphocytic Leukemia (CLL). Patients who achieved CR after 6 doses of R-GEMOX with Atezolizumab went on to Rituximab with Atezolizumab maintenance for up to 2 years. The ORR was 50% with a CR rate of 29%. Of the patients who achieved CR, 2 went on to HCT while the other 4 had ongoing CR without additional therapy lasting between 5-30 months. The investigators also noted better responses to R-GEMOX with Atezolizumab in RT-DLBCL from B-NHL as compared to traditional Richter Transformation from CLL (30).
Summarized in Table 3, the benefits of the addition of ICI agents Nivolumab, Pembrolizumab, and Durvalumab for B-cell NHLs have been variable, possibly related to the variability in CD3+/CD4+ TILs and tumor PD-L1 expression. Interestingly, Atezolizumab appears to provide significant benefit when combined with R-GEMOX in the treatment of RT-DLBCL. Thus, further studies are required to optimize ICI-based therapies in B-cell NHLs.
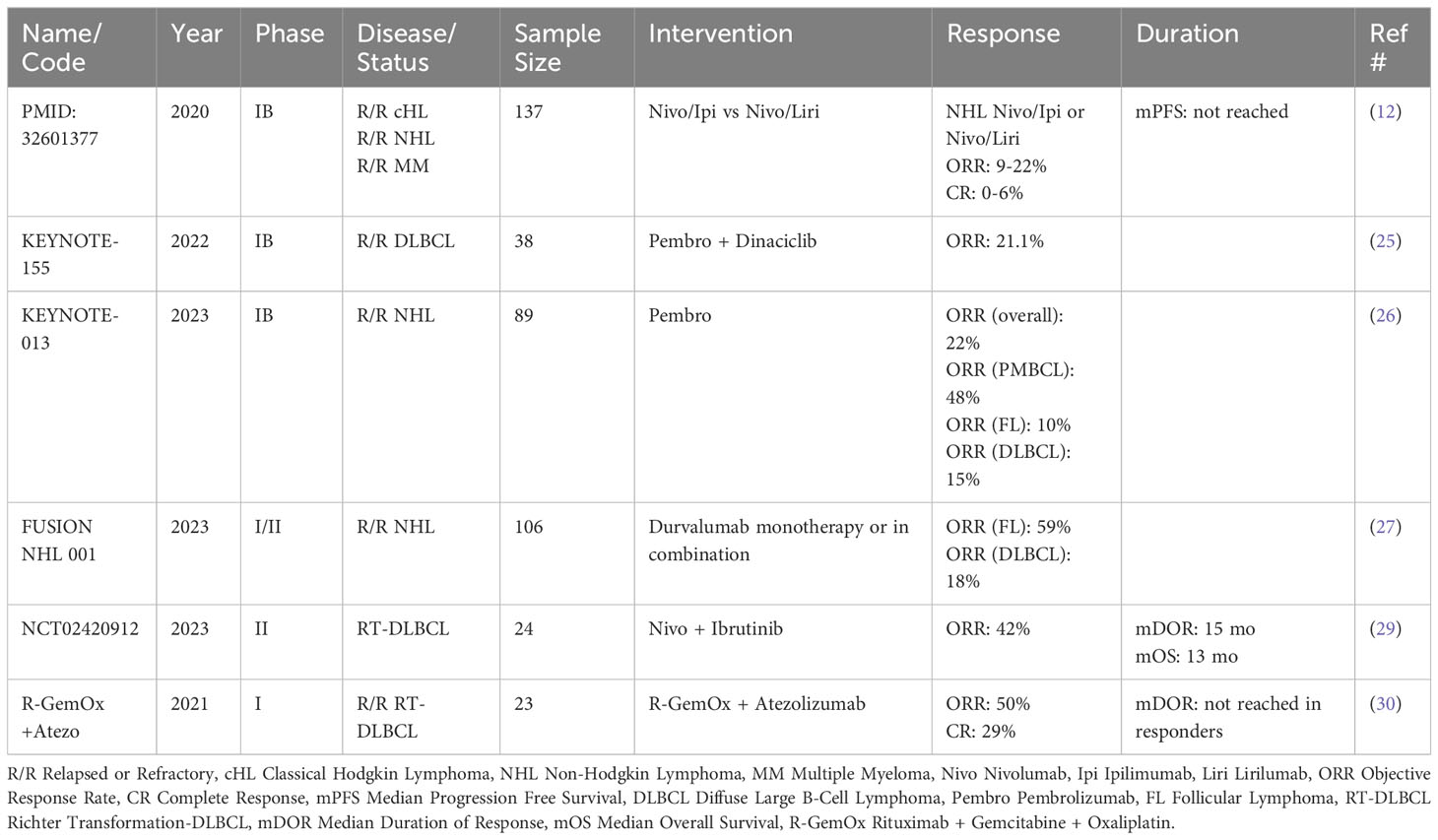
Table 3 Recent published trials evaluating CPI in NHL.
Currently active studies are evaluating Ipilimumab as potential ICI therapy in r/r B-cell NHLs (NCT00089076). There is also particular interest in taking advantage of the immunomodulatory effects of ICI to sensitize tumors to other therapies. NCT03533283 is an open-label Phase IB/II study evaluating the safety and efficacy of the CD20/CD3 bispecific antibody, Glofitamab, in combination with Atezolizumab or Polatuzumab Vedotin for adults with r/r B-NHLs. This combination is intriguing whereby blocking inhibitory Tregs may allow for the activation of tumor-specific effector T-cells via anti-PD-1 blockade. Atezolizumab would thus augment the effects of Glofitamab. Another intriguing therapeutic approach is intratumoral injection of anti-CTLA-4 ICI. NCT01769222 sets to evaluate the potential sensitizing effects of intratumoral Ipilimumab to local radiation therapy in a number of solid tumors, including NHLs that would increase neoantigen expression and expand the immune response (aka abscopal effect). In summary, ICI-based therapy has provided variable benefits on B-cell NHLs in which further investigation is needed to fully maximize its therapeutic effectiveness, which may include using ICI-based therapy as a synergistic augmentation to other effective therapies for NHLs.
Primary Central Nervous System Lymphoma (PCNSL) is a particular form of extra-nodal NHL that originates from tissue of the central nervous system (i.e. brain, spinal cord, eye, and meninges) and has been associated with Epstein-Barr Virus reactivation (EBV) as well as underlying immune deficiency (31, 32). First-line therapy is usually high-dose methotrexate-based regimens and though most will respond, relapse rates have been reported between 30-60% (31, 33). It has been well documented that EBV induces PD-L1 expression in EBV-associated tumor cells while the TME of PCNSL has been shown to significantly express PD-1 and PD-L1, especially by copy gain and chromosomal translocation of chromosome 9p24.1 (34, 35). Furthermore, PCNSL, has been shown to harbor a higher Tumor Mutational Burden (TMB), which is associated with better response to anti-PD-1 therapies in solid tumors (34, 36). This data serves as the supporting basis for trials that utilize ICI therapy in PCNSL.
Current data on the efficacy of ICI therapy in PCNSL is mainly based on a small number of case series. Nayak et al. report 5 of 5 patients (4 with r/r PCNSL and 1 with CNS relapse of Primary Testicular Lymphoma [PTL]) treated with Nivolumab having a clinical response, 3 of which had PFS between 13-17 months (37). A more recent case series reported by Gavrilenko et al. also reported activity of Nivolumab in 8 patients with PCNSL and 1 with CNS relapsed PTL in which ORR was 78%, CR rate was 33.3%, with a 2-year OS of 44% and median OS of 12 months. The 2-year PFS was 26% with a median PFS of 12 months (38). Pembrolizumab has been reported to induce prolonged remission in at least 3 of 5 patients with r/r PCNSL (39). Finally, ICI in combination with Rituximab induced a CR in 3 of 6 patients with either PCNSL or Secondary CNS Lymphoma (40).
Thus, it seems that ICI may have significant activity in the treatment of r/r disease, but no formal prospective studies have been published to date and more studies are needed. Fortunately, there are a number of active trials underway assessing ICI as monotherapy and in combination for r/r PCNSL, as shown in Table 4.
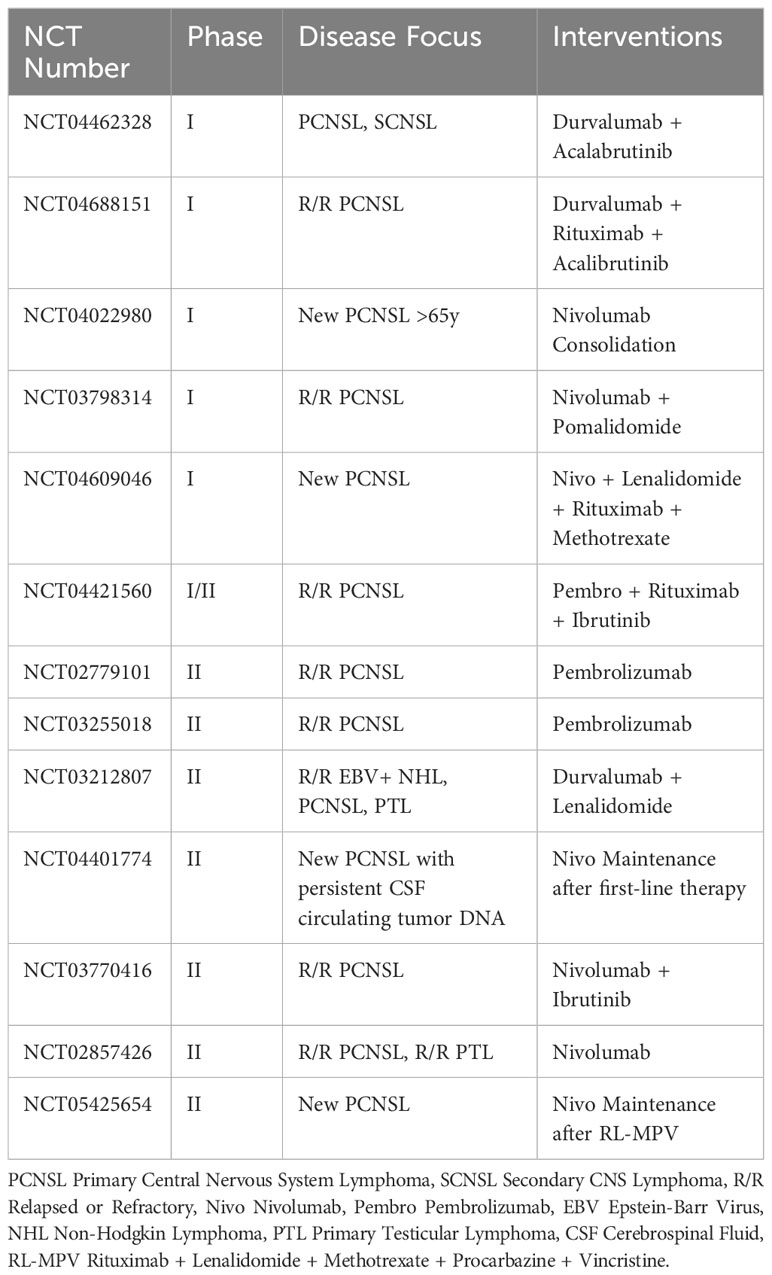
Table 4 Current clinical trials evaluating CPI in PCNSL.
Since our understanding of the underlying pathology of T-cell NHL is limited, current therapy is largely based on treatments for B-cell NHL. This includes regimens such as cyclophosphamide, doxorubicin, vincristine, and prednisone, with or without etoposide (CHOP and CHOEP, respectively). Other forms of immunotherapies have shown improved outcomes, as seen in the ECHELON-2 Trial, in which combining Brentuximab vedotin with the standard chemotherapy, cyclophosphamide, doxorubicin, prednisone (BV-CHP) had an improved 5-year PFS and 5-year OS as compared to CHOP (41). Thus, it seems that immunotherapies, including ICI, have a role in treating T-cell NHLs. Significant PD-1 expression has been reported in the TME of many subtypes of PTCL such as Angioimmunoblastic T-Cell Lymphoma (AITL), PTLD-NOS, and ALK- Anaplastic Large Cell Lymphoma (ALCL) (42, 43). Extranodal NK/T-cell Lymphoma (ENKTL), in contrast, does not seem to overexpress PD-1, though PD-L1 overexpression has been well documented in both the malignant cells and stromal cells. Still, the prognostic implications of PD-L1 expression remains mixed; though higher PD-1/PD-L1 and CTLA-4 expressing TMEs as being associated with worse prognosis (44). Further analyses suggest an inability of HCT to overcome these survival outcomes (45). Thus the prognostic implications of immune checkpoint molecules remains a significant knowledge gap that requires further investigation.
In assessing ICI activity in r/r PTCL, investigators unexpectedly saw a subset of patients experience disease hyper-progression, defined as progression within 2 months of treatment initiation, resulting in halting of clinical studies. Small studies have reported rates of hyper-progression as high as 50% while other have been terminated after interim analysis showed futility (46–48). Thus far, studies evaluating anti-PD-1-based therapy in r/r PTCL (as either monotherapy or in combination) have reported ORRs ranging from 36.4-50% and CRs from 0-35.7% (49–51). Iyer et al. reported an ORR ranging from 44-50% with just 2 patients experiencing hyper-progression with the combination of Pembrolizumab and the Histone Deacetylase Inhibitor (HDACi), Romidepsin (51). Thus, current data remains weak toward the utility for ICIs in r/r PTCL and the phenomenon of hyper-progression is not well understood. Further investigation is needed to understand the mechanisms driving hyper-progression and the optimal use of ICI-based therapy in r/r PTCL.
In contrast, ENKTL appears to have some benefit with ICI. The Orient-4 trial reported an ORR of 75% in patients treated with Sintilimab who failed a SOC asparaginase-containing regimen. The 24-month OS rate was 78% and median OS was not reached after the 30.4-month follow-up. A phenomenon of “pseudo-progression” was seen in 5 patients initially thought to have progressive disease and eventually showed a later response during the trial (52). Other studies have reported lower ORRs ranging from 38-40% and CRs 24-31% in r/r ENKTLs who have failed SOC therapies and were specifically treated with anti-PD-L1 therapies (53, 54). These findings are lower than expected given the fact that ENKTL tumors tend to have preferential PD-L1 expression in the TME as previously noted. Still, these data seem promising for r/r disease in which median OS without treatment is reportedly less than 6 months. Further investigation is needed to optimize the response rates of r/r ENKTL to ICI-based therapies. Other case reports have mentioned CRs in a small number of patients with combinations such as anti-PD-1 with a HDAC inhibitor (Chidamide), Etoposide, and Thalidomide, as published by Du et al. (55)
With responses to ICI in NK-/T-Cell Lymphomas (NKTCL) being mixed, predictors of response centered around PD-L1 expression have been well documented. Lim et al. identified a strong predictor of treatment response in patients who harbored a somatic mutation causing a structural rearrangement leading to a mutated PD-L1 (PD-L1MUT). When treated with ICI, these patients had higher ORRs and continued having a durable response as of publication (31-49 months) (56). However, additional studies have highlighted that relapsed ENKTL patients show higher frequencies of other mutations in JAK-STAT, NF-Kappa B, and PI3K-AKT pathways (57). These findings not only suggest mechanism of resistance, but also support the reasoning for ICI use in combination with other agents. Thus, further investigation is needed to evaluate effective ICI-based combination therapies with agents that target these other pathways. Table 5 summarizes currently active studies evaluating ICI in several combination regimens.
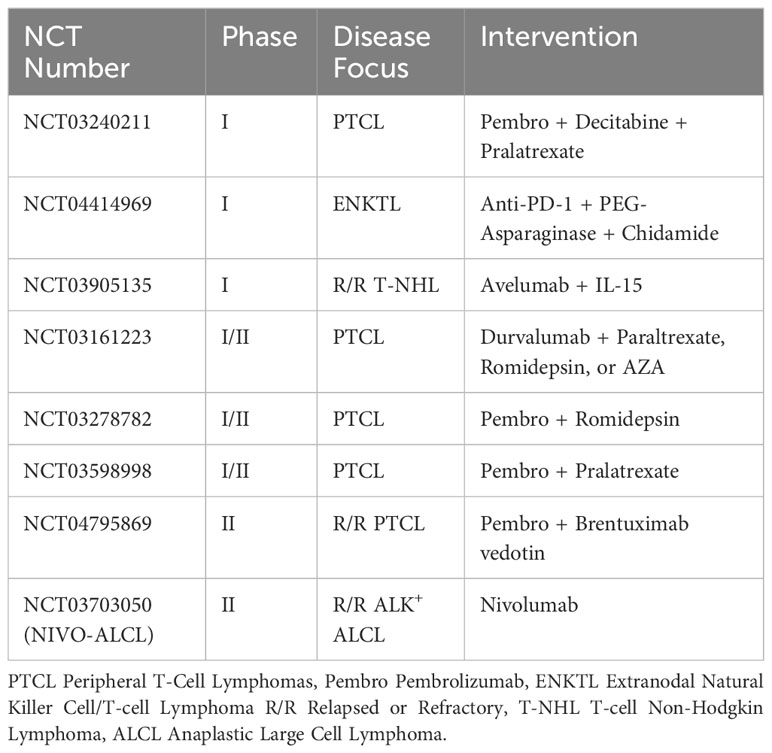
Table 5 Current clinical trial evaluating CPI in T-Cell Malignancies.
The current treatment paradigm for Multiple Myeloma (MM) involves triple combination regimens with an immunomodulatory drug (IMiD) such as Lenalidomide, a proteosome inhibitor such as Bortezomib, and a steroid followed by autoHCT. Despite a bevy of treatment options for MM, most patients will become refractory to available treatments after periods of remission and eventually succumb to their disease (58).
Circulating T-cells from r/r MM patients are known to have significantly abundant PD-1 and LAG3 expression, in which higher expression levels are predictive of poorer patient survival, suggesting a role for targeting these checkpoint molecules (59, 60). Multiple Phase I/II studies investigating Pembrolizumab in combination with an IMiD and steroid yielded ORRs ranging from 50-60% in refractory patients (61, 62). Results of these early studies spawned Phase III investigations in newly diagnosed (KEYNOTE-185) or r/r (KEYNOTE-183, CheckMate 602) MM populations. Unfortunately, these studies were prematurely halted after interim data suggested that Pembrolizumab-containing regimens had higher rates of treatment related deaths (4 vs 0) and higher rates of grade 3/4 Adverse Events (AEs) (63–65). Interestingly, KEYNOTE-183 noted that at a median follow up of 8.1 months, ORRs were similar between anti-PD-1 plus SOC and SOC alone at 62% vs 64%, respectively. Post-hoc analysis suggests that patients randomized to the Pembrolizumab group had a greater proportion of high-risk features such as stage 3 disease, high-risk cytogenetics, and extramedullary disease (65). Additionally, the previously mentioned study by Armand et al. saw a 0% ORR in a heavily pretreated MM population treated with combination Nivo/Ipi or Nivo/Liri, though the study was not powered for efficacy (12). Still, these current data provide a cautionary tale for future studies and emphasize the need to better characterize the TME of MM in order to identify those who would respond to ICI-based therapies.
Reasons for the lack of positive results remains unknown, but it could be speculated that specific polymorphisms within the PD-1 and CTLA-4 genes may affect response to ICI therapy. Gonzalez-Montes et al. identified a CTLA-4 polymorphism (CTLA4 rs231775 AA/AG) that served as an independent predictor of progressive disease (66). They reported that the AA/AG genotype was associated with median PFS of 32 months vs 96 months for the normal GG genotype while 5-year survival rate was half (25% vs 55%, respectively). Studies such as these highlight a need to find sub-populations of MM patients appropriate for ICI-based therapies. A review of active studies is outlined in Table 6 and highlights several trials evaluating ICI therapy both in the upfront and relapsed/refractory setting.
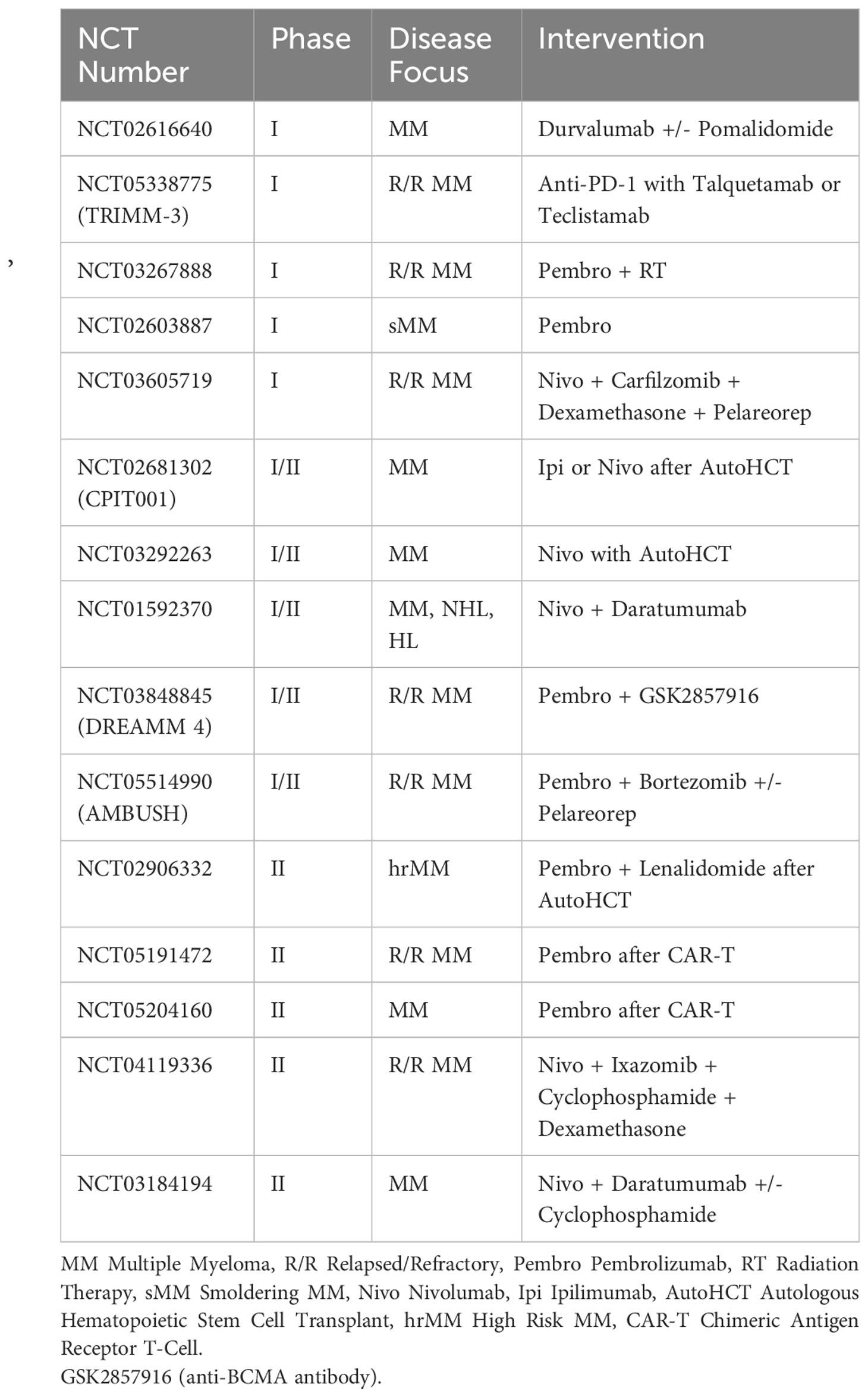
Table 6 Current clinical trials evaluating CPI in MM.
The current treatment paradigm for AML is with 7 + 3 induction consisting of an anthracycline and Cytarabine with or without Gemtuzumab ozogamicin (an anti-CD33 antibody-drug conjugate) followed by consolidative chemotherapy as a bridge to allogeneic HCT (alloHCT). It is estimated that 50% of patients will relapse after alloHCT for which several targeted immunochemotherapeutic regimens have been approved, however most patients will ultimately relapse and succumb to their disease (34).
Like other malignancies, cell surface checkpoint molecules have been identified in acute leukemia patients with some markers being predictive of outcomes. PD-L1 positivity has been documented in AML, both at initial diagnosis and in relapse (67). Furthermore, PD-L1 expression has exclusively correlated with worse outcomes in AML separate from other prognostic factors like blast count, immunophenotype, and cytogenetic mutations (68). Hypomethylating agents (HMA), commonly used in the r/r setting, are thought to induce PD-1/PD-L1 expression (69). Based on this premise, several studies have investigated the combination of HMA and PD-1/PD-L1 agents. Initial studies of r/r AML patients treated with combination PD-1/PD-L1 with HMA yielded ORRs ranging from 17-58% (70, 71). HMA-naïve and HMA-pretreated AML patients treated with Azacitidine (AZA) and Nivolumab had reported ORRs of 58% and 22%, respectively. Responders to AZA and Nivolumab had higher CD3+, CD4+ Teff, and CD8+ T cells in their pretherapy bone marrow aspirates compared with non-responders. Those same non-responders had significantly higher CTLA-4 upregulation on CD4+ effector T-cells after nivolumab dosing (70). This would suggest that selective T-lymphocyte depletion in advanced salvage patients plays a role in response to ICI-based therapy. It is possible that multiple rounds of chemoimmunotherapy selects for exhausted effector T-cells and/or selects for alternative inhibitory pathways. Other studies evaluating AZA with Nivolumab were terminated early when it was determined that the combination arm had significantly more early patient death and no difference in efficacy when compared to AZA alone (72). The authors attributed the higher death rate to the inclusion of patients with an ECOG of 2 or more, unrecognized autoimmune complications, and patients with FLT3-ITD mutations. Thus, it appears that ICI therapies may play a limited role in AML with known driver mutations and further investigation is needed to assess these mechanisms of resistance.
In the treatment of Myelodysplastic Syndrome (MDS), response to PD-1/PD-L1 signal blockade has been mixed. A Phase II study of AZA with Durvalumab vs AZA alone as first-line for High-Risk MDS patients found that although ORR was numerically greater in the combination group (61% vs 47%, P=0.18) it was not statistically significant. In contrast, OS was numerically lower, though also not statistically significant (11.6 vs 16.7 months, P=0.74). In phenotyping the tumor samples, AZA exposure did increase PD-L1 expression on monocytes and granulocytes, but not tumor blasts (72, 73). Garcia et al. report an ORR of 52% in pre-transplant patients treated with Ipilimumab and Decitabine, though responses were short lived (74). Decitabine was thought to act directly on the leukemic cells while Ipilimumab was thought to act on TILs, and was thus dependent on the immunophenotype of the infiltrating lymphocytes (74). These data suggest that ICI-therapy can potentially have a role in the treatment of MDS/AML, but further studies are needed to better understand the effects of a varying immunophenotype of TILs on response rates to ICI. Despite these mixed data, novel checkpoint targets are showing promising results in treating MDS/AML which are addressed in following sections.
Many studies aim to further assess the utility of ICI in all lines of therapy, as displayed in Table 7. Notably, the BLAST MRD AML-1 and -2 trials aim to incorporate Pembrolizumab to SOC therapies for both fit and unfit newly diagnosed AML patients. Nivolumab is being assessed by two groups as maintenance therapy to lengthen remission duration in AML patients. Also interestingly, the utility of Nivolumab is being evaluated in the treatment of TP53+ AML. As more data is reported from these studies, ICI therapy may very well have a role in treating myeloid malignancies.

Table 7 Current clinical trials evaluating CPI in MDS/AML.
SOC therapy for Acute Lymphoblastic Leukemia (ALL) is centered around consolidative chemoimmunotherapy combinations, which include Blinatumomab (an anti-CD20 monoclonal antibody) and Inotuzumab ozogamicin (an anti-CD22 antibody-drug conjugate). Chemoimmunotherapy traditionally serves as a bridge to HCT. Lately, studies characterizing the TME of ALL suggest a potential role for ICI therapy. It had been shown that relapsed TMEs had higher PD-1 expression and intensity on both CD4+ and CD8+ T-cells than TMEs that were either with persistent disease or in CR. Interestingly, despite patients who were newly diagnosed with ALL having lower overall PD-1 expression, the signal intensity on individual CD4+ or CD8+ T-cells was no different than patients with relapsed disease. There was also no difference in PD-L1 expression on the leukemic blasts when based on disease status (75). This suggests that an increase in absolute PD-1+ effector T-cells is a major driver of immune evasion and serves as a viable therapeutic target.
To assess efficacy of ICI in the treatment of ALL, Cassaday et al. investigated the ability of Pembrolizumab to convert patients with positive minimal residual disease (MRD) to CR with negative MRD. The trial was halted early due to only 1 patient achieving MRD negativity after the first 200mg cycle of Pembrolizumab (76). Other studies have documented the importance of CD4+ T-cell exhaustion in predicting outcomes for ALL patients. Tracy et al., showed that in mouse models with B-ALL, OS was better in mice treated with nilotinib plus anti-PD-L1 blockade compared to nilotinib alone. They report that anti-PD-L1 blockade lead to clonal expansion of leukemia-specific CD4+ Helper and Cytotoxic T-cells while reducing markers of T-cell exhaustion (77). This suggests potential activity in combination Tyrosine Kinase Inhibition (TKI) with ICI in Ph+ B-ALL, which was being further assessed in a Phase I study (NCT02819804), but the trial has been terminated due to funding and accrual issues. These data suggest that T-cell exhaustion plays an important role in response to ICI-therapy with ALL and is a significant area in need for further investigation to better understand the pathophysiology and mechanisms of resistance with ALL.
There are a small number of studies currently assessing ICI activity in ALL. NCT02879695 is a Phase I study assessing combination Blinatumomab plus Nivolumab with or without Ipilimumab in poor-risk CD19+ r/r B-ALL patients. Similarly, both NCT03160079 and NCT03512405 are Phase I/II studies looking at the safety and efficacy of combination Blinatumomab with Pembrolizumab in r/r B-ALL.
Chimeric Antigen Receptor T Cells (CAR-T) are effector T-cells with modified T-Cell Receptors (TCR) targeting specific cell-surface antigens and are engineered to be activated independently of MHC. Thus far, there are six manufactured CAR-T products FDA approved to treat ALL, NHL (DLBCL, FL, Mantle Cell Lymphoma), and MM (78, 79). PD-1 expression on the infused CAR-T cells has been, in part, thought to be a determining factor influencing rates of response. Studies have shown PD-1/PD-L1 blockade restored CAR-T effector function, thus suggesting this interaction may cause T-cell exhaustion within the TME (80). Porter et al. reports that patients with lower expression of CD8+PD-1+ T-cells had a better response to CAR-T, suggesting that the inhibitory effect of PD-1 signaling plays a role in controlling the anti-tumor effect of CAR-T therapy (81). Thus, ICI in combination with CAR-T has been of great interest.
The ZUMA-6 trial is currently evaluating the safety and efficacy of Axicabtagene Ciloleucel in combination with Atezolizumab for r/r DLBCL (NCT02926833). The end of Phase I analysis reported that out of 12 patients, the ORR was 90% with 6 patients achieving CR and 3 achieving PR. Using the ZUMA-1 data for comparison, CAR-T cell expansion was over 2-fold higher in ZUMA-6 (82). These results have allowed for the opening of Phase II of the ZUMA-6 trial. Additionally, Hirayama et al. reported preliminary data evaluating combination of a CD-19-specific 4-1BB-costimulated CAR-T (JCAR014) with Durvalumab in treating r/r DLBCL. Of the 12 patients evaluable, ORR was 50% (5 with CR and 1 with PR). CAR-T expansion was seen in the peripheral blood within 14 days of infusion with higher peaks observed in responding patients (83). These data serve as proof of concept to a synergistic effect of ICI with CAR-T therapy resulting in a more robust effector T-cell expansion, which in turn leads to improved outcomes and more durable responses, thus providing an exciting area for further investigation.
There has been additional interest in the utility of ICI in r/r disease after CAR-T therapy. Chong et al. evaluated the efficacy of Pembrolizumab for r/r NHL after CD-19-specific 4-1BB-costimulated CAR-T, but the best ORR seen was 25% (84). Separately, Li et al. evaluated the use of Pembrolizumab or Nivolumab with a second CAR-T infusion in pediatric patients with r/r ALL or B-lymphoblastic lymphoma early after a first CAR-T infusion. Of 14 patients enrolled, 3 patients established B-cell aplasia, 2 of which had ongoing aplasia with Pembrolizumab maintenance therapy. Of 4 patients with bulky extramedullary disease, 2 achieved CR and 2 had PR (85). These preliminary data suggest that at least a subset of r/r patients to CAR-T could benefit from subsequent ICI by inducing a re-expansion of the CAR-T population. But this appears to only be most effective when the primary mechanism of tumor persistence is checkpoint inhibitor-mediated T-cell exhaustion. As Deng et al. showed, higher PD-1 expression was associated with poorer response rates and PD-1 was only expressed in a small subset of cells. Additionally, other exhaustive markers such as LAG-3 and TIM-3 had stronger correlation to a lower response rate (86). Thus far, data seems to be more promising for ICI used adjunctively with CAR-T therapy rather than as a subsequent line of therapy, but alternative checkpoint molecules (discussed later in this review) may serve an important role in mechanisms of resistance. Further studies are needed to understand the best utilization of ICI with CAR-T and how to best target alternative checkpoint molecules. Table 8 summarizes active studies evaluating ICI given both concurrently and after CAR-T therapy in several hematologic malignancies.
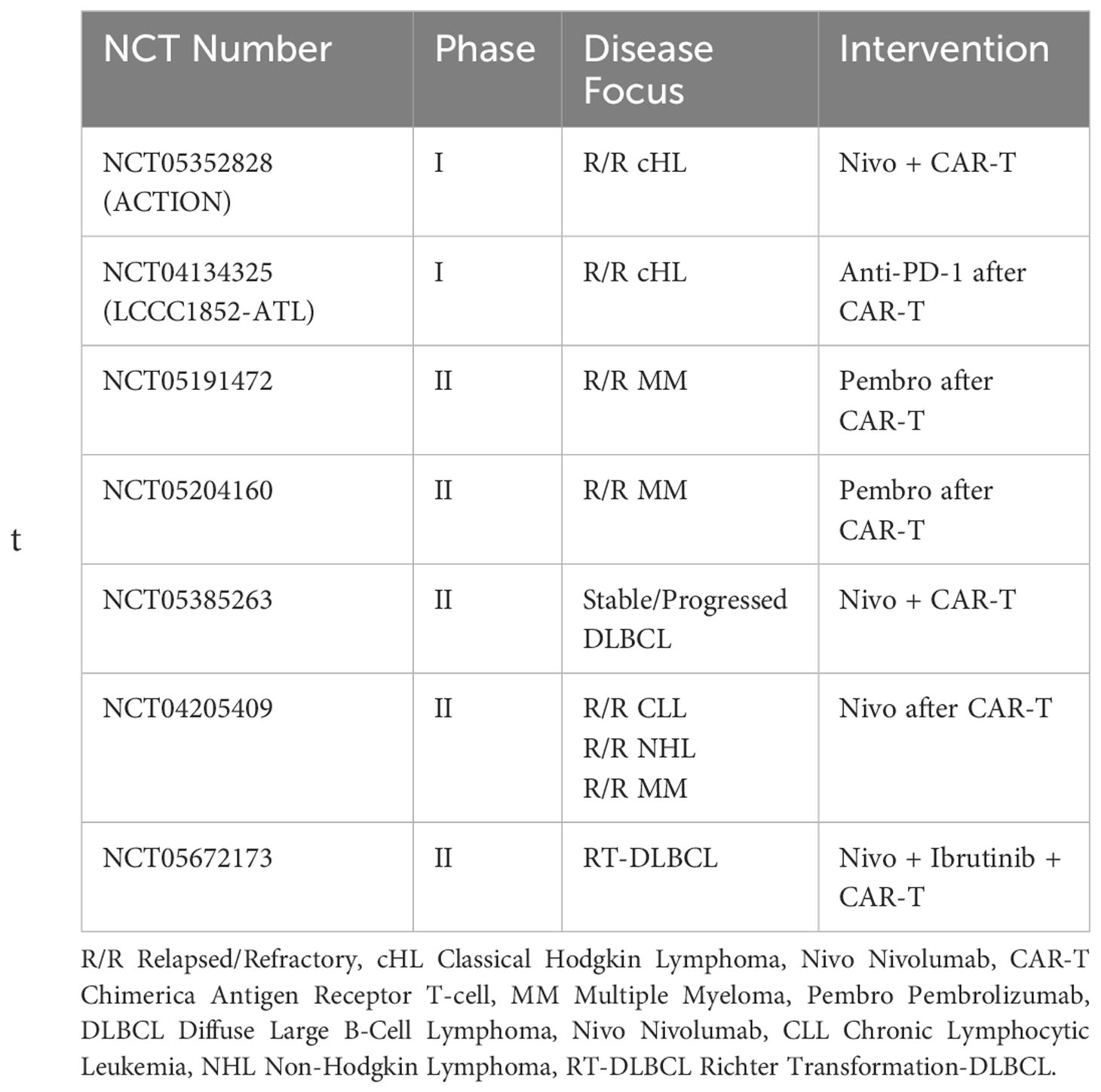
Table 8 Current clinical trials evaluating CPI with CAR-T therapy.
In the context of allogeneic stem cell transplant (alloHCT), effective response requires a delicate balance between allowing a graft-vs-leukemia effect and suppressing graft-vs-host disease (GVHD). Therefore, there is concern that the use of ICI therapy either before or after alloHCT would increase the risk and severity of GVHD. As Nguyen et al. reported in their worldwide literature review, rates of ICI-induced GVHD were found to be 57% with Nivolumab, 24.7% with Pembrolizumab, and 12.9% with Ipilimumab. Mortality rate was 25.8%. The majority of the cases reviewed were of ICI therapy after alloHCT (87).
But, despite the concern for ICI-induced GVHD, early data suggest benefit to ICI after alloHCT. Early studies evaluating ICI after alloHCT for r/r HL report ORRs ranging from 75-95%, 1-year PFS from 47-58%, and 1-year OS from 78-89%. Rates of both Acute and Chronic GVHD ranged from 15-30% (88, 89). Other early studies looking at ICI after alloHCT for r/r AML report lower ORR rates ranging from 20-32%, 1-year PFS ranging from 18.2-23%, and 1-year OS around 56% (74,) (90–92). It is speculated that the difference in responses is secondary to downregulation of HLA-1 complexes resulting in decreased antigen presentation to CD8+ TILs. It is further speculated that an increase in Tregs following ICI is a compensatory mechanism of resistance in AML (74). Thus, preliminary data would suggest activity with ICI after alloHCT at least in the treatment of HL, but further studies are needed to assess benefits in other hematologic malignancies and whether this outweighs the risk of GVHD.
In contrast, several studies, have evaluated the safety and efficacy of ICI therapy before alloHCT, mainly for r/r HL and NHL. Rates of acute GVHD ranged from 33-44% while rates of chronic GVHD (with patients receiving varying GVHD prophylaxis) ranged from 35-41%. The 1-2 year OS ranged from 77-89% and 1-2 year PFS ranged from 74-76%, thus suggesting still a significant survival benefit (93, 94). Further studies have shown improvement in controlling GVHD in these patients with posttransplant cyclophosphamide (PTCy) as prophylaxis. Ikegawa et al. showed that PTCy could successfully restore T-cell homeostasis and ameliorate clinical GVHD in mouse models (95). Additionally, Oran et al. showed that AML/MDS patients who had prior ICI therapy and later underwent alloHCT had lower rates of acute GVHD when treated with PTCy prophylaxis as compared to those who were not. Rates of acute GVHD in these patients receiving PTCy were similar to patients who underwent alloHCT without prior ICI therapy (96). Tschernia et al. further showed no difference in 1-year OS, 100-day mortality, or rates of grade 3-4 GVHD in AML patients who received high-dose Cytarabine with Pembrolizumab followed by alloHCT to a historical control group who received SOC without ICI. These patients all received PTCy as part of their GVHD prophylactic regimen (97). Thus, these data support the safety of ICI therapy prior to alloHCT and suggest that PTCy may negate the inherent increased risk of both acute and chronic GVHD observed with pre-transplant ICI therapy. Even in the setting of haploidentical transplantation with PTCy, reports show no difference on OS, nor a significant increase in 100-day incidence of grade 2-4 acute GVHD or chronic GVDH. Data also suggests a 2-year relapse incidence of 0% with prior ICI vs 20% without prior ICI (98). Overall, these data support the idea that ICI therapy prior to HCT incurs a higher risk of both acute and chronic GVHD, but the addition of PTCy likely mitigates this increased risk and thus makes HCT after ICI therapy a viable and effective treatment option of r/r hematologic malignancies. Whether there is an overall survival benefit or improved response rate remains to be answered. Though most trials have evaluated ICI after alloHCT in the context of HL, more studies have evaluated this strategy in other hematologic malignancies as well, as outlined in Table 9.
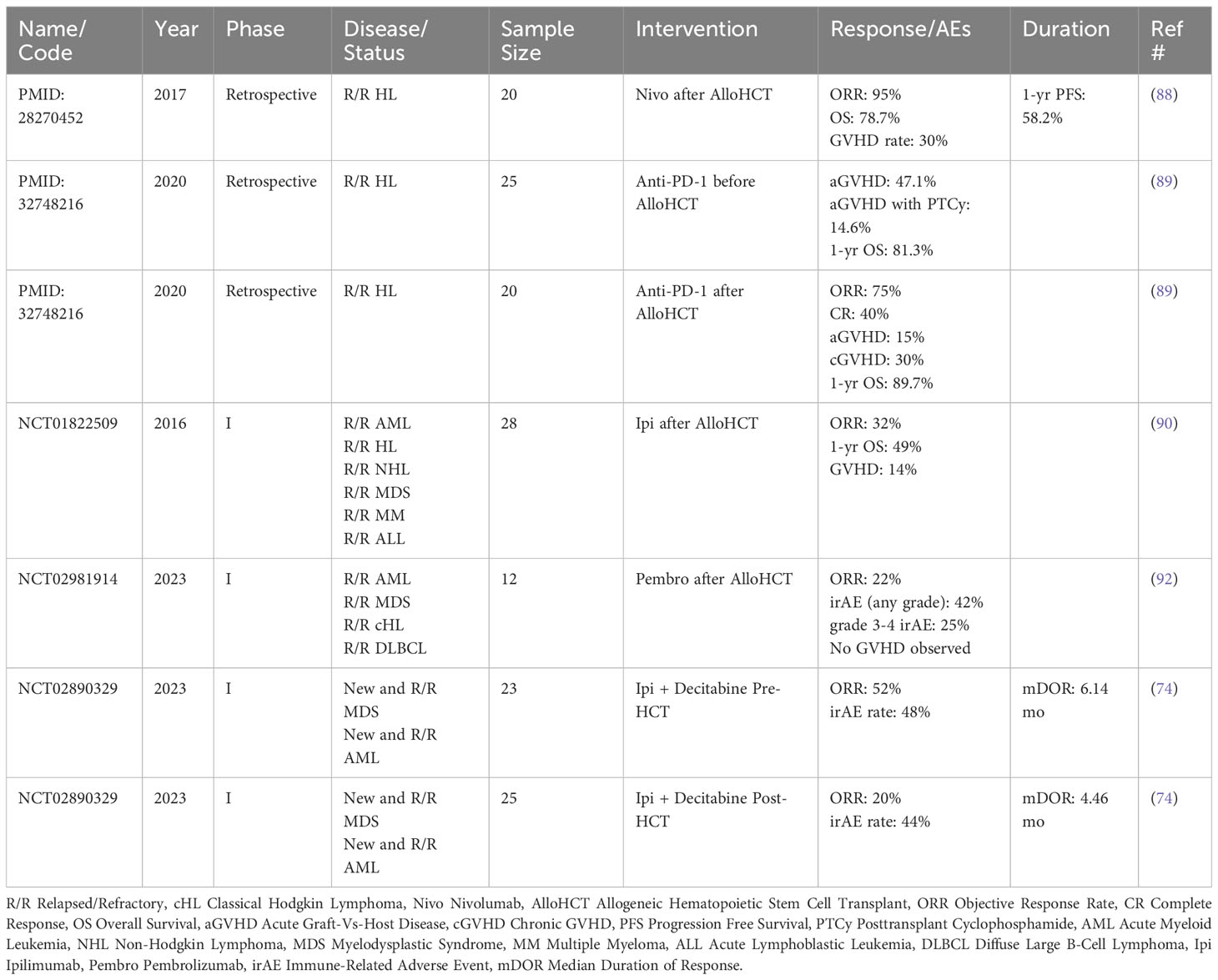
Table 9 Published trials evaluating CPI before and after AlloHCT.
As such, both ICI and alloHCT are effective treatment approaches for several hematologic malignancies with a large portion of data supporting their use in r/r HL. The optimal timing of these therapies remains to be established, but it seems the risk of GVHD after ICI therapy is at least mitigated with the use of PTCy. Thus, more studies are needed to better understand where ICI fits best in relation to alloHCT. A review of active trials shows numerous studies focusing within this field. There are several Phase I trials evaluating ICI in combination or as monotherapy after HCT for myeloid and lymphoid malignancies (NCT02846376, NCT01822509, NCT00060372, NCT03600155, NCT03146468-NIVALLO, NCT04361058). NCT01919619 is a trial reevaluating the use of Lenalidomide and Ipilimumab after HCT. NCT02981914 is a pilot study evaluating Pembrolizumab after alloHCT. NCT04128020 is a Phase I trial evaluating the combination of Azacitadine with Nivolumab following reduced-intensity alloHCT for AML and high-risk MDS. NCT04635735 is a Phase I/II trial evaluating the safety and efficacy of Ipilimumab after HCT for r/r Multiple Myeloma.
Lymphocyte-activation gene 3 (LAG-3) is a transmembrane protein expressed on T-lymphocytes and NK cells. Binding of LAG-3 to MHC-II results in suppression of autoimmune and anti-cancer immunity (99). Additionally, the binding of LAG-3 to the soluble liver-secreted Fibrinogen-Like protein 1 (FGL-1) has been shown to inhibit CD8+ T cell-mediated anti-tumor effects, but the significance of this interaction in hematologic malignancies remains to be elucidated (100). More recently, increased LAG-3 expression has been correlated to treatment resistance in a number of hematologic malignancies including CLL, FL, and DLBCL (101–104). Relatlimab (BMS-986016, Bristol-Meyers Squibb) is a human IgG4 anti-LAG-3 monoclonal antibody (mAb). In vitro studies have shown that exposure of Relatlimab to peripheral blood mononuclear cells of CLL patients induced anti-leukemic activity and increased cytokine production (105). Further industry-sponsored trials have evaluated safety, tolerability, and efficacy of Relatlimab monotherapy or in combination with Nivolumab in r/r B-cell malignancies (NCT02061761). Preliminary data shows ORRs to Relatlimab and Nivolumab of 61.9% for ICI-naïve HL patients, 6.7% for DLBCL patients, and 15.0% for HL patients with prior ICI therapy. Durations of responses were 14 months, 1 month, and 6.37 months, respectively (106). Thus, based on this preliminary data, LAG-3 appears to be a potentially effective alternative target of checkpoint inhibition for at least some treatment resistant hematologic malignancies, but further investigation is needed to optimize its use.
Currently active trials include NCT03489369, a Phase I, open-label trial assessing safety, tolerability, and antineoplastic activity of an Anti-LAG-3 mAb (Sym022) in advanced solid tumors and lymphomas. The same investigators are further assessing Anti-PD-1 therapy in combination with either Anti-LAG-3 or Anti-TIM-3 in both advanced solid tumors and lymphomas (NCT03311412). The combination of Relatlimab with Nivolumab and Azacitadine for the treatment of AML is being investigated in the trial NCT 04913922. HLX26 is another anti-LAG-3 mAb being investigated in solid tumors and lymphomas in NCT05078593.
T-cell immunoglobulin and mucin domain 3 (TIM-3) is known to be co-expressed with PD-1 on effector T-cells and binds to many ligands, though most significantly to galectin-9. This interaction is known to negatively regulate CD8+ T-cell activation and Th1-type immunity by inducing cell death (107). TIM-3 appears to be a marker of exhaustion and an increased number of exhausted PD-1+/TIM-3+ CD8+ T-cells has been associated with disease progression and poorer prognosis in AML (108, 109). Preliminary in vivo studies have shown that blockade of TIM-3 prevents engraftment of leukemic stem cells without inhibiting normal stem cell engraftment (110). Furthermore, galectin-9 knockout mice are more resistant to AML morbidity/mortality while double blockade of PD-1/PD-L1 and TIM-3/galectin-9 as associated with reduced leukemic burden (111). TIM-3 expression has also been found to correlate to poor prognosis in other hematologic malignancies such as DLBCL, ALL, MDS, Chronic Myelogenous Leukemia (CML), and Chronic Myelomonocytic Leukemia (CMML) (112–115). Thus blockade of TIM-3/galectin-9 is a potentially effective target for further treatment in several hematologic malignancies.
Sabatolimab (MBG453) is an anti-TIM-3 mAb that has been shown to enhance immune-mediated killing of TIM-3+ leukemic cells in vitro and is currently under investigation in clinical trials (116). STIMULUS-MDS1 evaluated the safety and efficacy of Sabatolimab with HMA as first line treatment in intermediate, high-risk, and very-high-risk MDS patients who were not eligible for high intensity chemotherapy. The investigators reported a median PFS of 11.1 months for patients receiving Sabatolimab compared to 8.5 months for the placebo group. ORRs were 49.2% and 37.1% with CR rates of 23% vs 21%, respectively. Median OS was 19.0 mo vs 18.0 mo. None of the aforementioned comparisons were statistically significant, though trended in favor for sabatolimab with HMA, which the authors speculated may be due to a delayed-onset of benefit (117). Subsequently, STIMULUS-MDS2 is evaluating the safety and efficacy of combination Azacitadine and Sabatolimab in high-risk MDS and CMML as first-line treatment for patients who are not eligible for high intensity chemotherapy (115). The results of this current study are anticipated to provide strong evidence toward the benefits of anti-TIM-3 blockade.
Interestingly, other mechanisms of TIM-3 blockade are also being explored, as Wu et al. have identified the small molecule, SMI402, which inhibits substrate binding of TIM-3 and has been shown to increase activity of CD8+ T cells and NK cells in vitro (118). Studies are underway to assess its safety and efficacy.
TIM-3 remains a relatively newly discovered target for ICI and there are several active early phase studies (Table 10) evaluating its benefits in hematologic malignancies. NCT03489343 is investigation Sym023, an anti-TIM-3 mAb, as monotherapy for r/r solid tumors and lymphoma for which there was no further standard of care treatment available. Preliminary data in patients receiving the highest dose of Sym023 had a reported ORR of 66.7% in ≤ 16 weeks of treatment and a median Time To Progression of 5.36 months (119). The Keyplus-001study (NCT05357651) is evaluating a bispecific antibody to PD-1 and TIM-3 (LB1410) in the treatment of both advanced solid tumors and lymphoma. NCT05216835 is a similar Phase I trial evaluated AZD7789, a different anti-PD-1/anti-TIM-3 bispecific antibody, in the treatment of r/r HL. As previously mentioned, NCT03311412 is evaluating Anti-PD-1 therapy in combination with either Anti-LAG-3 or Anti-TIM-3 in both advanced solid tumors and lymphomas. Sabatolimab is further being studied in the post-alloHCT setting in AML patients who achieve CR with positive MRD as a preemptive treatment alone or in combination with Azacitadine to potentially enhance the graft-vs-leukemia effect (NCT04623216). NCT05367401, NCT03066648, NCT03940352, and NCT04150029 are investigating Sabatolimab in combination with other novel therapies for MDS and AML.
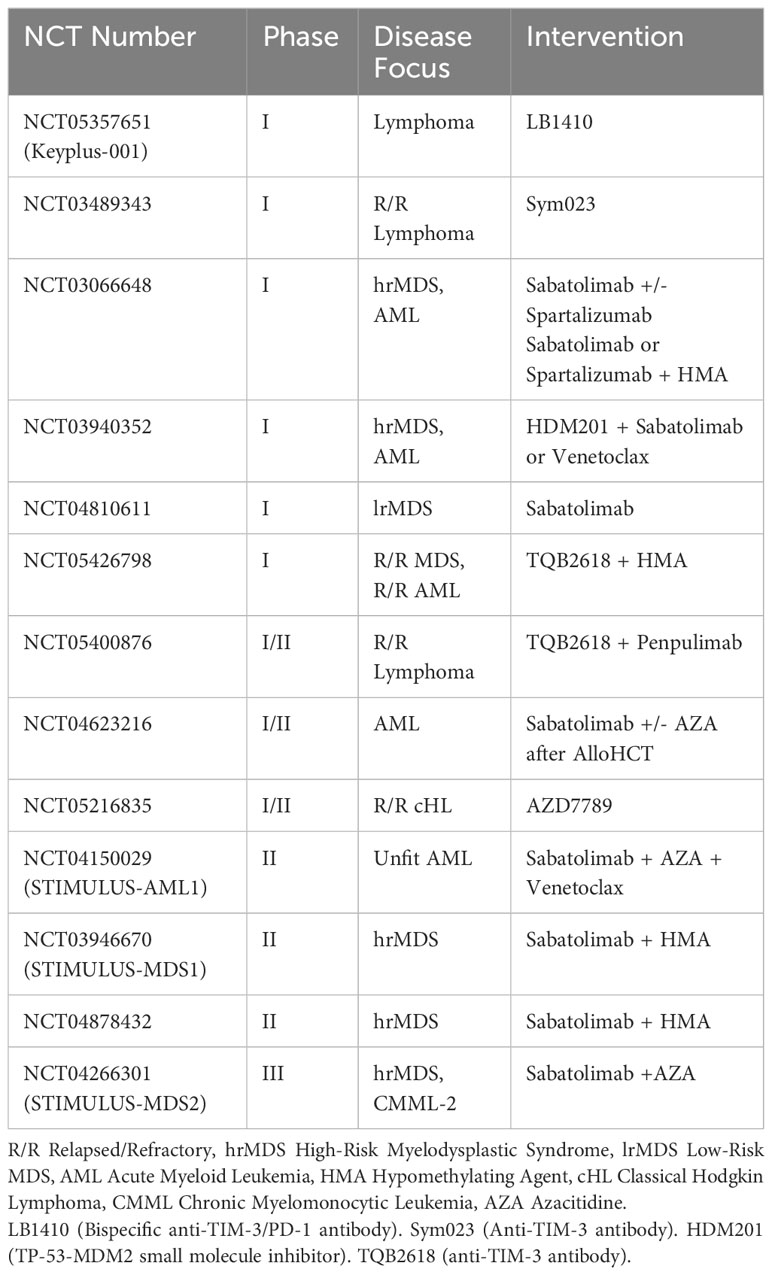
Table 10 Current clinical trials evaluating anti-TIM-3 therapy.
T cell immunoreceptor with immunoglobulin and ITIM domain (TIGIT) is a checkpoint inhibitory protein expressed on effector T-cells, regulatory T-cells, and NK cells and primarily binds to CD155 and CD112 which are mainly expressed on dendritic cells, macrophages, and lymphocytes (120, 121). CD155 appears to be the primary ligand, in which binding results in downregulation of the T-cell Receptor while also increasing the production of anti-inflammatory cytokines such as IL-10 (122–126). TIGIT is known to be upregulated in TILs in HL and has been associated with poor prognosis (127). Advanced stage CLL patients have also been seen to have higher TIGIT+ T cells (128). Additionally, both r/r AML and MM patients have been shown to have higher levels of TIGIT+ CD8+ T-cells and have been associated with relapse after stem cell transplant (129, 130). More recently, TIGIT has been implicated as a major cause of relapse after CAR-T for Mantle Cell Lymphoma (131). Thus TIGIT appears to be an important mechanism of immune evasion for hematologic malignancies, but further understanding of its significance and whether it is an effective target for therapy remains unknown.
Tiragolumab is a new anti-TIGIT mAb and has shown promising anti-cancer activity in solid tumors. There are small number of active studies looking at the benefits of TIGIT blockade in hematologic malignancies. NCT04150965 is a Phase I/II trial evaluating anti-LAG-3 and anti-TIGIT as monotherapy followed by Pomalidomide and Dexamethasone for r/r MM after prior therapy. NCT05315713 is an open-label, Phase I/II trial evaluating combination Mosunetuzumab (anti-CD20/CD3 bispecific antibody) with Tiragolumab, with or without Atezolizumab for r/r FL and DLBCL. HLX301 is a bispecific antibody to PD-L1 and TIGIT being evaluated in a Phase I study for advanced solid tumors and lymphomas (NCT05390528), while HLX53 is an anti-TIGIT Fc fusion protein also being investigated in solid tumors and lymphomas.
Cluster of differentiation 47 (CD47) is a transmembrane protein that is found on many cells, but most notably macrophages. It specifically binds to signal-regulatory protein α (SIRPα) expressed on myeloid cells which then inhibits macrophage-mediated phagocytosis and is known as a “don’t eat me signal” (132). CD47 upregulation has been reported in hematologic malignancies such as NHL, MM, and Leukemias and is associated with poorer prognosis (132–134). Blockade of the CD47-SIRPα interaction primarily leads to phagocytosis of cancer cells, but a significant AE is severe hemolysis due to RBCs expressing CD47. Blockade of this signaling also enhances antigen presentation as well as cross presentation on dendritic cells and leads to priming of CD8+ T-cells while also increasing neutrophil-mediated tumor cell death (135). Majeti et al. showed that in vivo blockade of the CD47-SIRPα interaction enabled phagocytosis of AML leukemic stem cells, reduced tumor burden, and prevented engraftment, thus laying the ground work for further clinical studies (136).
Magrolimab (Hu5F9-G4) is an anti-CD47 antibody that has shown a tolerable side effect profile in recent early phase trials, with the most common side effect being anemia. Advani et al. evaluated Magrolimab with Rituximab for r/r NHL and reported an ORR of 50% with CR of 36%. At a median follow-up of 8.1 months, 91% of responses were ongoing (137). Most notably, Magrolimab has been investigated in combination with Azacitadine in the treatment of high-risk MDS and AML patients as first-line therapy. The investigators saw an ORR in MDS of 91% and 64% in AML. Median duration of response was not reached as far out as 9.4 months. Remarkably, 6-month OS in MDS and TP-53 mutant AML were 100% and 91%, respectively (138). This promising data has led to further Phase III trials (ENHANCE trial) and provide an exciting potentially effective treatment option for a patient population with historically poor outcomes. Further ongoing trials are investigating Magrolimab in combination with Rituximab (NCT0352714), Acalbrutinib (NCT03527147), and Mogamulizumab (anti-CCR4, NCT03527147).
CD47 blockade is an exciting new therapeutic approach with drug developers finding several ways to target this molecule. CC-90002, another anti-CD47 mAb was investigated in combination with Rituximab for r/r NHL, but ORRs were merely 13% (139). It also did not seem to have any activity in r/r MDS or AML (140). No further phase II trials have been conducted thus far. Other additional anti-CD47 antibodies include IBI-88 (Letaplimab), AK117 (Ligufalimab), and TJ011133 (Lemzoparlimab) which are currently being investigated in combination therapies for the treatment of NHL, MDS, and AML. Lemzoparlimab interestingly has a unique binding epitope which spares RBC opsonization and therefore has been shown to have lower hematologic toxicity (141). When used in combination with Rituximab for r/r CD20+ NHL, early reports show an ORR of 57% (142). Other small studies have evaluated Lemzoparlimab monotherapy for r/r AML and found a tolerable AE profile with a small number of primary refractory patients achieving a morphologic leukemic-free state after two cycles (143). More studies are needed to best understand the utility of these novel agents.
Another approach to CD47 blockade is recombinant proteins using a SIRPα extracellular motif fused to a Fc fragment of the heavy chain of immunoglobulin. This approach has the particular advantage of having high affinity with a low molecular weight, suggesting better tumor infiltration by simple diffusion across vascular membranes (144). Both TTI-621 and TTI-622 are fusion proteins with a SIRPα motif link to an IgG1 Fc and IgG 4 Fc, respectively. Horwitz et al. conducted the First-In-Human Phase I trial with TTI-621 in r/r hematologic malignancies. Preliminary data shows that the most common AEs were infusion reactions (40-50%) and thrombocytopenia (30%). ORRs to single agent TTI-621thus far were found to be 20% for NHL (including CTCL, PTCL, and DLBCL) (145). Intralesional TTI-621 has also been found to be active in Mycosis Fungoides and Sezary Syndrome with a 90% response rate in the injected lesions. Interestingly, 80% of patients saw response in distal non-injected lesions as well suggesting systemic effects with intralesional injection (146). In contrast to TTI-621, TTI-622 does not bind to RBCs and is currently being studied as monotherapy for r/r NHLs as well. Preliminary data from Patel et al. reports an ORR of 33% for heavily treated r/r NHLs, which includes DLBCL, CTCL, PTCL, and FL (147). ALX148 (Evorpacept) is another high affinity SIRPα motif linked to an inactive IgG1 Fc. It is currently being studied in combination with Rituximab for r/r CD20+ NHL (ASPEN-01) in which preliminary data has reported a 14-month ORR of 40.9% and 9-month ORR of 63.6% (148). Lastly, IMM01 is a SIRPαIgG1 fusion protein with weak erythrocyte conjugation to lower the risk of hemolysis. It is currently being studied in r/r HL and NHL as monotherapy in which preliminary reported data shows an ORR of only14.3% (149). These data are a good starting point in assessing recombinant fusion proteins as a mode of CD47 blockade and could potentially allow for better tissue penetration and outcomes.
Finally, bispecific antibodies are a third approach to CD47 blockade while also combining a second immunotherapeutic target for synergistic effect. IMM0306 is a bispecific antibody to CD47 and CD20. It has shown in vitro effect with cancer killing ability while not binding to human RBCs. In mouse models for lymphoma, it had superior activity when paired with Lenalidomide as compared to other single agent therapy and combination Rituximab with Lenalidomide (150). TG-1801 is a bispecific antibody to CD47 and CD19. Similarly, preclinical studies have shown potent anticancer activity for numerous B-cell malignancies and has synergistic effect when used in combination with Rituximab (151).
CD47 is a promising and highly anticipated novel target for checkpoint-inhibitor blockade in which early trials (Table 11) are showing significant efficacy in anti-cancer activity. This becomes especially exciting in the treatment of TP-53 mutated AML for which treatment is difficult and response rates are poor. It is also exciting for treatment of other relapsed/refractory disease as this is a completely new pathway involving tumor-infiltrating macrophages and NK cells, which bypasses the PD-1/PD-L1 and CTLA4/CD80 pathways. Additionally, combination CD47 blockade with anti-CD19/CD20 suggests a synergistic effect. At the time of this review, there are numerous active studies evaluating all anti-CD47 approaches either as single-agent or in combination for many hematologic malignancies as outline in Table 12.
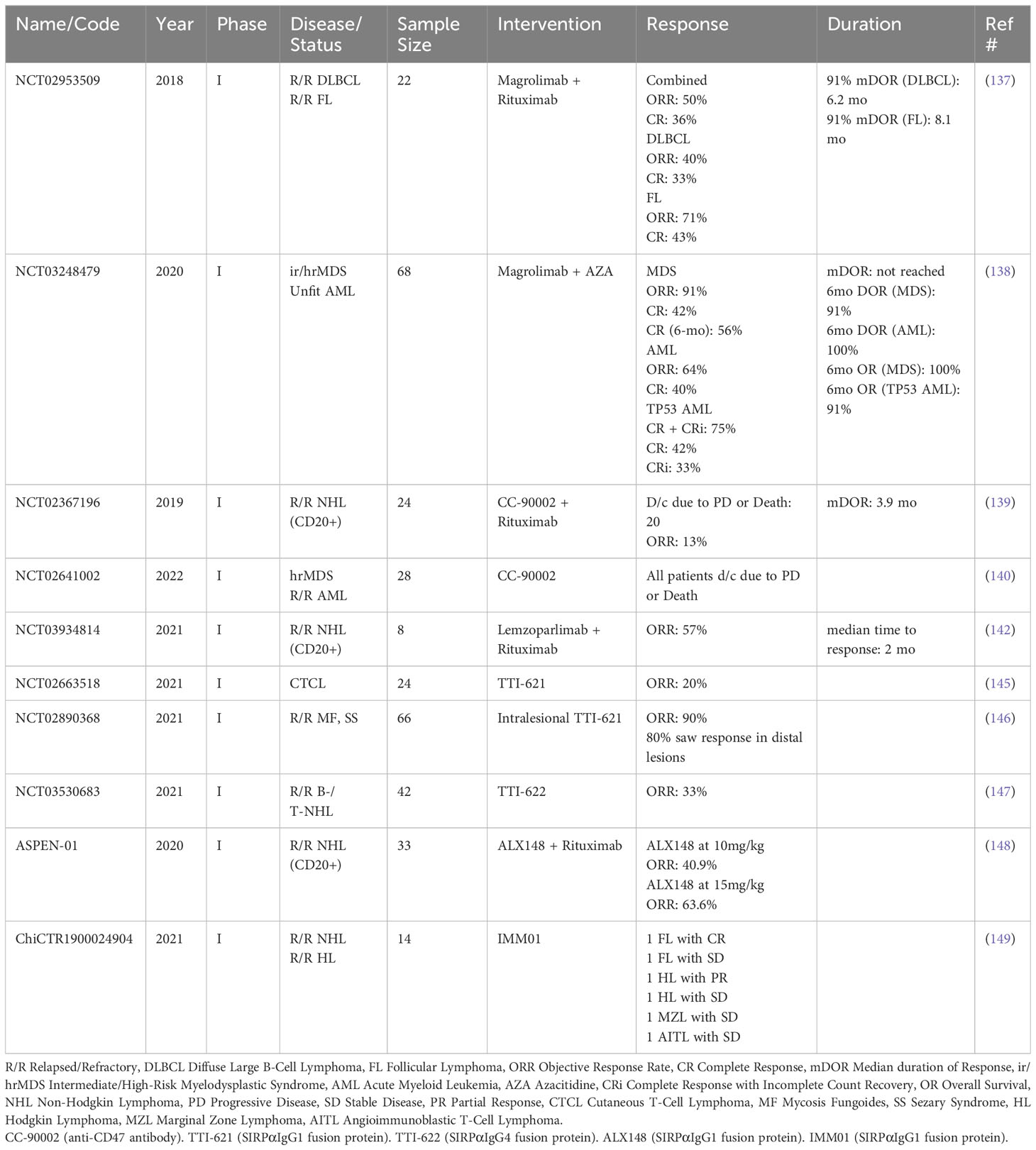
Table 11 Published trials evaluating anti-CD47 therapy.

Table 12 Current clinical trials evaluating anti-CD47 therapy.
Natural-killer group 2 member A (NKG2A) is an inhibitory receptor on both NK cells and T cells that binds to non-classical MHC-I (HLA-E) and induces a “self-recognition signal” to allow malignant cells to evade cytotoxicity. HLA-E is known to be overexpressed in various malignancies including DLBCL, MM, and AML. Monalizumab is an anti-NKG2A antibody which has shown activity in combination with Cetuximab for other solid tumor types, but studies have yet to show efficacy in hematologic malignancies. One study assessed Monalizumab in combination with ibrutinib for treatment of r/r CLL, but the study had been terminated by the sponsor (NCT02557516). More studies are needed to evaluate the utility of anti-NKG2A antibody use in hematologic malignancies.
Killer Cell immunoglobulin-like receptor (KIR) is another NK cell inhibitory receptor that binds classical MHC-1 and leads to immune evasion. IPH2102 (1-7F9) is an anti-KIR mAb that has been studied in both r/r MM and AML after first CR. These Phase I studies have at least shown a tolerable safety profile, but minimal or no ORR (152, 153). The previously mentioned study by Armand et al. evaluated the recombinant anti-KIR mAb, Lirilumab, in combination with Nivolumab in multiple hematologic malignancies, but it was concluded that there was no benefit to the addition of anti-KIR to Nivolumab (12). Available data thus far is limited on the efficacy of anti-KIR ICI therapy, but current trials are underway. NCT01256073 is assessing safety and tolerability of IPH2101 in older AML patients over 60 years of age who are not transplant eligible. The EFFIKIR Trial (NCT01687387) is evaluating efficacy of Lirilumab as maintenance therapy for elderly AML patients after first CR. Lastly, NCT02481297 is assessing the safety of Lirilumab in combination with Rituximab in patients with r/r CLL. Additionally, genetic variability in KIRs due to allelic polymorphisms has been implicated in the variability of patients’ responses in allo- and haptoidentical HCT (154). Thus, a number of current studies aim to better understand the importance of donor selection based on HLA and KIR profile matching, which could open up more avenues toward the therapeutic addition of anti-KIR ICI.
ICI therapy has shown to be beneficial in a multitude of solid malignancies and more recently in hematologic malignancies. Hodgkin Lymphoma has seen the most benefit from ICI-based therapy, mainly in the relapsed and refractory setting after autologous stem cell transplant, but recent and current studies have shown promising data to suggest a role of ICI in earlier lines of therapy as well. Most notably, Nivolumab showed superior PFS when compared to Brentuximab vedotin when combined with first-line AVD for advanced stage cHL. Data for Non-Hodgkin Lymphomas have been less impressive, but ICI may have a role specifically in the treatment of Richter-Transformed DLBC and PCNSL. Though data to support ICI as either monotherapy or in combination is limited, more studies are looking into ICI as a sensitizing or synergistic agent with other therapies for NHL. ICI therapy has been implicated in the treatment of PCNSL, especially given the association with EBV reactivation and induction of PD-L1 expression in these tumors. T cell Lymphoma and Leukemia has seen mixed responses to ICI, though Sintilimab has had promising benefits specifically in ENKTL. ICI-containing combination regimens may also show improved activity in treating PTCL. Unfortunately, data thus far have shown limited benefit for ICI in Multiple Myeloma, suggesting that polymorphisms within the PD-1 and CTLA-4 genes may play a role in the variability of responses among all hematologic malignancies. MDS and AML have had modest benefit with ICI, most notably in combination with HMA. More promising is the activity seen with anti-CD47 antibody therapy (Magrolimab) in the treatment of high-risk MDS and TP-53 mutated AML. In contrast, ALL has not seen as robust benefit with ICI, though there may be some activity when used in combination with SOC therapies.
Aside from ICI as a component of primary systemic therapy, there seems to be a role in augmenting the efficacy of cellular therapies. When given after CAR-T therapy, ICI has been shown to induce re-expansion of the CAR-T population and may be useful as adjunctive therapy to maintain CAR-T anti-tumor activity. In the setting of allogeneic HCT, the risk of worsened GVHD from ICI is at least mitigated with the use of posttransplant cyclophosphamide. Thus, ICI is a viable treatment option both before and after cellular therapies.
PD-1/PD-L1 and CTLA-4 remain the primary targets for ICI, but recent research has revealed other checkpoint molecules of potential clinical significance. LAG-3, TIM-3, and TIGIT blockade have shown promising activity in many hematologic malignancies. Most exciting is the macrophage checkpoint inhibitor, CD47, in which blockade in combination with HMA has shown significant activity against high-risk MDS and TP-53 mutated AML. Lastly, NK/T cell checkpoint molecules such as NKG2A and KIR may also play a role in tumor immune evasion and serve as potential alternative therapeutic targets.
Overall, ICI continues to show great potential in the treatment of hematologic malignancies as either monotherapy, in combination with other systemic therapies, or as a synergistic agent. Further discovery of new novel checkpoint molecules yields more alternative approaches to enhance the immune system’s recognition of tumor cells and promises of improved outcomes.
AT: Conceptualization, Data curation, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. DL: Conceptualization, Data curation, Investigation, Visualization, Writing – original draft. JT: Conceptualization, Project administration, Supervision, Writing – review & editing.
The author(s) declare no financial support was received for the research, authorship, and/or publication of this article.
The authors would like to acknowledge the University of California, Davis, Division of Malignant Hematology/Cellular Therapy and Transplantation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell (2011) 144(5):646–74. doi: 10.1016/j.cell.2011.02.013
2. Buchbinder EI, Desai A. CTLA-4 and PD-1 pathways. Am J Clin Oncol (2016) 39(1):98–106. doi: 10.1097/COC.0000000000000239
3. Zitvogel L, Kroemer G. Targeting PD-1/PD-L1 interactions for cancer immunotherapy. Oncoimmunology (2012) 1(8):1223–5. doi: 10.4161/onci.21335
4. Cader FZ, Schackmann RCJ, Hu X, Wienand K, Redd R, Chapuy B, et al. Mass cytometry of Hodgkin lymphoma reveals a CD4+ regulatory T-cell–rich and exhausted T-effector microenvironment. Blood (2018) 132(8):825–36. doi: 10.1182/blood-2018-04-843714
5. Patel SS, Weirather JL, Lipschitz M, Lako A, Chen PH, Griffin GK, et al. The microenvironmental niche in classic Hodgkin lymphoma is enriched for CTLA-4–positive T cells that are PD-1–negative. Blood (2019) 134(23):2059–69. doi: 10.1182/blood.2019002206
6. Armand P, Shipp MA, Ribrag V, Michot JM, Zinzani PL, Kuruvilla J, et al. Programmed death-1 blockade with pembrolizumab in patients with classical hodgkin lymphoma after brentuximab vedotin failure. J Clin Oncol (2016) 34(31):3733–9. doi: 10.1200/JCO.2016.67.3467
7. Chen R, Zinzani PL, Fanale MA, Armand P, Johnson NA, Brice P, et al. Phase II study of the efficacy and safety of pembrolizumab for relapsed/refractory classic hodgkin lymphoma. J Clin Oncol (2017) 35(19):2125–32. doi: 10.1200/JCO.2016.72.1316
8. Armand P, Engert A, Younes A, Fanale M, Santoro A, Zinzani PL, et al. Nivolumab for relapsed/refractory classic hodgkin lymphoma after failure of autologous hematopoietic cell transplantation: extended follow-up of the multicohort single-arm phase II checkMate 205 trial. J Clin Oncol (2018) 36(14):1428–39. doi: 10.1200/JCO.2017.76.0793
9. Sun C, Chen H, Wang Y, Zheng C. Safety and efficacy of PD-1 and PD-L1 inhibitors in relapsed and refractory Hodgkin’s lymphoma: a systematic review and meta-analysis of 20 prospective studies. Hematology (2023) 28(1):2181749. doi: 10.1080/16078454.2023.2181749
10. Kuruvilla J, Ramchandren R, Santoro A, Paszkiewicz-Kozik E, Gasiorowski R, Johnson NA, et al. Pembrolizumab versus brentuximab vedotin in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): an interim analysis of a multicentre, randomised, open-label, phase 3 study. Lancet Oncol (2021) 22(4):512–24. doi: 10.1016/S1470-2045(21)00005-X
11. Lepik KV, Fedorova LV, Kondakova EV, Zalyalov YR, Babenko EV, Lepik EE, et al. A phase 2 study of nivolumab using a fixed dose of 40 mg (Nivo40) in patients with relapsed/refractory hodgkin lymphoma. HemaSphere (2020) 4(5):e480. doi: 10.1097/HS9.0000000000000480
12. Armand P, Lesokhin A, Borrello I, Timmerman J, Gutierrez M, Zhu L, et al. A phase 1b study of dual PD-1 and CTLA-4 or KIR blockade in patients with relapsed/refractory lymphoid Malignancies. Leukemia (2021) 35(3):777–86. doi: 10.1038/s41375-020-0939-1
13. Advani RH, Moskowitz AJ, Bartlett NL, Musso M, Donnarumma D, Morelli E, et al. Brentuximab vedotin in combination with nivolumab in relapsed or refractory Hodgkin lymphoma: 3-year study results. Blood (2021) 138(6):427–38. doi: 10.1182/blood.2020009178
14. Bartlett NL, Herrera AF, Domingo-Domenech E, Holmberg L, Johnston P, Mei M, et al. A phase 1b study of AFM13 in combination with pembrolizumab in patients with relapsed or refractory Hodgkin lymphoma. Blood (2020) 136(21):2401–9. doi: 10.1182/blood.2019004701
15. Cheson BD, Bartlett NL, LaPlant B, Vose JM, Ramchandren R, Feldman TA, et al. Brentuximab vedotin plus nivolumab as first-line therapy in older or chemotherapy-ineligible patients with Hodgkin lymphoma (ACCRU): a multicentre, single-arm, phase 2 trial. Lancet Haematol (2020) 7(11):e808–15. doi: 10.1016/S2352-3026(20)30275-1
16. Bröckelmann PJ, Goergen H, Keller U, Mehta A, Forero-Torres A, Garcia-Sanz R, et al. Efficacy of nivolumab and AVD in early-stage unfavorable classic hodgkin lymphoma. JAMA Oncol (2020) 6(6):1–9. doi: 10.1182/blood.2019004701
17. Bröckelmann PJ, Bühnen I, Meissner J, Lee HJ, Advani RJ, Christian B, et al. Nivolumab and doxorubicin, vinblastine, and dacarbazine in early-stage unfavorable hodgkin lymphoma: final analysis of the randomized german hodgkin study group phase II NIVAHL trial. J Clin Oncol (2023) 41(6):1193–9. doi: 10.1200/JCO.22.02355
18. Herrera AF, LeBlanc ML, Castellino SM, Meissner J, Ordemann R, Halbsguth TV, et al. SWOG S1826, a randomized study of nivolumab(N)-AVD versus brentuximab vedotin(BV)-AVD in advanced stage (AS) classic Hodgkin lymphoma (HL). J Clin Oncol (2023) 41(17_suppl):LBA4–4. doi: 10.1200/JCO.2023.41.17_suppl.LBA4
19. De Filippi R, Marcacci G, Derenzini E, Trautmann-Grill K, Herhaus P, Halbsguth TV, et al. Anti-PD1 Consolidation in Patients with Hodgkin Lymphoma at High Risk of Relapse after Autologous Stem Cell Transplantation: A Multicenter Real-Life Study. Cancers (2022) 14(23):5846. doi: 10.3390/cancers14235846
20. Herrera AF, Chen L, Nieto Y, Keller D, Wennhold K, Lehmann J, et al. Brentuximab vedotin plus nivolumab after autologous haematopoietic stem-cell transplantation for adult patients with high-risk classic Hodgkin lymphoma: a multicentre, phase 2 trial. Lancet Haematol (2023) 10(1):e14–23. doi: 10.1016/S2352-3026(22)00318-0
21. Garcia-Marquez MA, Thelen M, Reinke S, Li H, Rutherford SC, Evens AM, et al. Reverted exhaustion phenotype of circulating lymphocytes as immune correlate of anti-PD1 first-line treatment in Hodgkin lymphoma. Leukemia (2022) 36(3):760–71. doi: 10.1038/s41375-021-01421-z
22. Péricart S, Tosolini M, Gravelle P, Rossi C, Traverse-Glehen A, Amara N, et al. Profiling immune escape in hodgkin’s and diffuse large B-cell lymphomas using the transcriptome and immunostaining. Cancers (2018) 10(11):415. doi: 10.3390/cancers10110415
23. Keane C, Vari F, Hertzberg M, Cao KA, Green MR, Han E, et al. Ratios of T-cell immune effectors and checkpoint molecules as prognostic biomarkers in diffuse large B-cell lymphoma: a population-based study. Lancet Haematol (2015) 2(10):e445–55. doi: 10.1016/S2352-3026(15)00150-7
24. Xu-Monette ZY, Xiao M, Au Q, Padmanabhan R, Xu B, Hoe N, et al. Immune profiling and quantitative analysis decipher the clinical role of immune-checkpoint expression in the tumor immune microenvironment of DLBCL. Cancer Immunol Res (2019) 7(4):644–57. doi: 10.1158/2326-6066.CIR-18-0439
25. Gregory GP, Kumar S, Wang D, Mahadevan D, Walker P, Wagner-Johnston N, et al. Pembrolizumab plus dinaciclib in patients with hematologic Malignancies: the phase 1b KEYNOTE-155 study. Blood Adv (2022) 6(4):1232–42. doi: 10.1182/bloodadvances.2021005872
26. Kuruvilla J, Armand P, Hamadani M, Kline J, Moskowitz CH, Avigan D, et al. Pembrolizumab for patients with non-Hodgkin lymphoma: phase 1b KEYNOTE-013 study. Leuk Lymphoma (2023) 64(1):130–9. doi: 10.1080/10428194.2022.2136956
27. Casulo C, Santoro A, Cartron G, Ando K, Munoz J, Le Gouill S, et al. Durvalumab as monotherapy and in combination therapy in patients with lymphoma or chronic lymphocytic leukemia: The FUSION NHL 001 trial. Cancer Rep Hoboken NJ (2023) 6(1):e1662. doi: 10.1002/cnr2.1662
28. El Hussein S, Medeiros LJ, Gruschkus SK, Wei P, Schlette E, Fang H, et al. Immune evasion phenotype is common in Richter transformation diffuse large B-cell lymphoma variant. Virchows Arch Int J Pathol (2023) 482(6):1011–9. doi: 10.1007/s00428-023-03520-x
29. Jain N, Senapati J, Thakral B, Ferrajoli A, Thompson P, Burger J, et al. A phase 2 study of nivolumab combined with ibrutinib in patients with diffuse large B-cell Richter transformation of CLL. Blood Adv (2023) 7(10):1958–66. doi: 10.1182/bloodadvances.2022008790
30. Herrera AF, Othman T, Frankel P, Allen P, Popplewell LL, Shouse G, et al. Atezolizumab combined with immunogenic salvage chemoimmunotherapy (R-gemOx+Atezo) in patients with transformed diffuse large B-cell lymphoma. Blood (2021) 138:1407. doi: 10.1182/blood-2021-151188
31. Tao K, Wang X, Tian X. Relapsed primary central nervous system lymphoma: current advances. Front Oncol (2021) 11:649789. doi: 10.3389/fonc.2021.649789
32. Zhang N, Zuo Y, Jiang L, Peng Y, Huang X, Zuo L. Epstein-barr virus and neurological diseases. Front Mol Biosci (2022) 8:816098. doi: 10.3389/fmolb.2021.816098
33. Jahnke K, Thiel E, Martus P, Herrlinger U, Weller M, Fischer L, et al. Relapse of primary central nervous system lymphoma: clinical features, outcome and prognostic factors. J Neurooncol (2006) 80(2):159–65. doi: 10.1007/s11060-006-9165-6
34. Ou A, Sumrall A, Phuphanich S, Spetzler D, Gatalica Z, Xiu J, et al. Primary CNS lymphoma commonly expresses immune response biomarkers. Neuro-Oncol Adv (2020) 2(1):vdaa018. doi: 10.1093/noajnl/vdaa018
35. Chapuy B, Roemer MGM, Stewart C, Tan Y, Abo RP, Zhang L, et al. Targetable genetic features of primary testicular and primary central nervous system lymphomas. Blood (2016) 127(7):869–81. doi: 10.1182/blood-2015-10-673236
36. Yarchoan M, Hopkins A, Jaffee EM. Tumor mutational burden and response rate to PD-1 inhibition. N Engl J Med (2017) 377(25):2500–1. doi: 10.1056/NEJMc1713444
37. Nayak L, Iwamoto FM, LaCasce A, Mukundan S, Roemer MGM, Chapuy B, et al. PD-1 blockade with nivolumab in relapsed/refractory primary central nervous system and testicular lymphoma. Blood (2017) 129(23):3071–3. doi: 10.1182/blood-2017-01-764209
38. Gavrilenko AN, Volkov NP, Shmidt DI, Polushin AY, Kondakova E, Lepik K, et al. Nivolumab in primary CNS lymphoma and primary testicular lymphoma with CNS involvement: single center experience. Blood (2020) 136(Supplement 1):4. doi: 10.1182/blood-2020-138924
39. Graber JJ, Plato B, Mawad R, Moore DJ. Pembrolizumab immunotherapy for relapsed CNS Lymphoma. Leuk Lymphoma (2020) 61(7):1766–8. doi: 10.1080/10428194.2020.1742903
40. Ambady P, Szidonya L, Firkins J, James J, Johansson K, White T, et al. Combination immunotherapy as a non-chemotherapy alternative for refractory or recurrent CNS lymphoma. Leuk Lymphoma (2019) 60(2):515–8. doi: 10.1080/10428194.2018.1480771
41. Horwitz S, O’Connor OA, Pro B, Trümper L, Iyer S, Advani R, et al. The ECHELON-2 Trial: 5-year results of a randomized, phase III study of brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma. Ann Oncol Off J Eur Soc Med Oncol (2022) 33(3):288–98. doi: 10.1016/j.annonc.2021.12.002
42. Kim S, Kwon D, Koh J, Nam SJ, Kim YA, Kim TM, et al. Clinicopathological features of programmed cell death-1 and programmed cell death-ligand-1 expression in the tumor cells and tumor microenvironment of angioimmunoblastic T cell lymphoma and peripheral T cell lymphoma not otherwise specified. Virchows Arch (2020) 477(1):131–42. doi: 10.1007/s00428-020-02790-z
43. Manso R, Rodríguez-Perales S, Torres-Ruiz R, Santonja C, Rodríguez-Pinilla S-M. PD-L1 expression in peripheral T-cell lymphomas is not related to either PD-L1 gene amplification or rearrangements. Leuk Lymphoma (2021) 62(7):1648–56. doi: 10.1080/10428194.2021.1881511
44. Muhamad H, Suksawai N, Assanasen T, Polprasert C, Bunworasate U, Wudhikarn K. Programmed cell death 1 and programmed cell death ligands in extranodal natural killer/T cell lymphoma: expression pattern and potential prognostic relevance. Acta Haematol (2019) 143(1):78–88. doi: 10.1159/000500974
45. Onishi A, Fuji S, Kitano S, Maeshima AM, Tajima K, Yamaguchi J, et al. Prognostic implication of CTLA-4, PD-1, and PD-L1 expression in aggressive adult T-cell leukemia-lymphoma. Ann Hematol (2022) 101(4):799–810. doi: 10.1007/s00277-022-04760-8
46. Bennani NN, Kim HJ, Pederson LD, Atherton PJ, Micallef IN, Thanarajasingam G, et al. Nivolumab in patients with relapsed or refractory peripheral T-cell lymphoma: modest activity and cases of hyperprogression. J Immunother Cancer (2022) 10(6):e004984. doi: 10.1136/jitc-2022-004984
47. Ohmoto A, Fuji S. Rapid T-cell lymphoma progression associated with immune checkpoint inhibitors. Expert Rev Hematol (2023) 16(7):535–41. doi: 10.1080/17474086.2023.2215424
48. Barta SK, Zain J, MacFarlane AW, Smith SM, Ruan J, Fung HC, et al. Phase II study of the PD-1 inhibitor pembrolizumab for the treatment of relapsed or refractory mature T-cell lymphoma. Clin Lymphoma Myeloma Leuk (2019) 19(6):356–364.e3. doi: 10.1016/j.clml.2019.03.022
49. Shi Y, Wu J, Wang Z, Zhang L, Wang Z, Zhang M, et al. Efficacy and safety of geptanolimab (GB226) for relapsed or refractory peripheral T cell lymphoma: an open-label phase 2 study (Gxplore-002). J Hematol OncolJ Hematol Oncol (2021) 14(1):12. doi: 10.1186/s13045-021-01033-1
50. Lesokhin AM, Ansell SM, Armand P, Scott EC, Halwani A, Gutierrez M, et al. Nivolumab in patients with relapsed or refractory hematologic Malignancy: preliminary results of a phase ib study. J Clin Oncol (2016) 34(23):2698–704. doi: 10.1200/JCO.2015.65.9789
51. Iyer SP, Xu J, Becnel MR, Nair R, Steiner R, Feng L, et al. A phase II study of pembrolizumab in combination with romidepsin demonstrates durable responses in relapsed or refractory T-cell lymphoma (TCL). Blood (2020) 136(Supplement 1):40–1. doi: 10.1182/blood-2020-143252
52. Tao R, Fan L, Song Y, Hu Y, Zhang W, Wang Y, et al. Sintilimab for relapsed/refractory extranodal NK/T cell lymphoma: a multicenter, single-arm, phase 2 trial (ORIENT-4). Signal Transduct Target Ther (2021) 6:365. doi: 10.1038/s41392-021-00768-0
53. Huang H, Tao R, Zou L, Cen H, Guo Y, Huang Y, et al. Preliminary results from a multicenter, single-arm, phase 2 study of CS1001, an anti-programmed death-ligand 1 (PD-L1) human monoclonal antibody (mAb), in patients (pts) with relapsed or refractory extranodal natural killer/T cell lymphoma (rr-ENKTL). Blood (2019) 134(Supplement_1):2833. doi: 10.1182/blood-2019-121865
54. Kim SJ, Lim JQ, Laurensia Y, Cho J, Yoon SE, Lee JY, et al. Avelumab for the treatment of relapsed or refractory extranodal NK/T-cell lymphoma: an open-label phase 2 study. Blood (2020) 136(24):2754–63. doi: 10.1182/blood.2020007247
55. Du L, Zhang L, Li L, Li X, Yan J, Wang X, et al. Effective treatment with PD-1 antibody, chidamide, etoposide, and thalidomide (PCET) for relapsed/refractory natural killer/T-cell lymphoma: A report of three cases. OncoTargets Ther (2020) 13:7189–97. doi: 10.2147/OTT.S262039
56. Lim SH, Hong JY, Lim ST, Hong H, Arnoud J, Zhao W, et alBeyond first-line non-anthracycline-based chemotherapy for extranodal NK/T-cell lymphoma: clinical outcome and current perspectives on salvage therapy for patients after first relapse and progression of disease. Ann Oncol (2023) 28(9):2199–205. doi: 10.1093/annonc/mdx316
57. Gao L-M, Zhang Y-H, Shi X, Liu Y, Wang J, Zhang WY, et al. The role of PD-L1 expression in prediction and stratification of recurrent or refractory extranodal natural killer/T-cell lymphoma. Front Oncol (2022) 12:821918. doi: 10.3389/fonc.2022.821918
58. Kumar SK, Dimopoulos MA, Kastritis E, Terpos E, Nahi H, Goldschmidt H, et al. Natural history of relapsed myeloma, refractory to immunomodulatory drugs and proteasome inhibitors: a multicenter IMWG study. Leukemia (2017) 31(11):2443–8. doi: 10.1038/leu.2017.138
59. Chen M, Zhu J, Yang X, Yao J, Liu Y, Liu Q. PD-1 and LAG-3-positive T cells are associated with clinical outcomes of relapsed/refractory multiple myeloma patients. Eur J Med Res (2022) 27:296. doi: 10.1186/s40001-022-00923-5
60. Kulikowska de Nałęcz A, Ciszak L, Usnarska-Zubkiewicz L, Pawlak E, Frydecka I, Szmyrka M, et al. Inappropriate expression of PD-1 and CTLA-4 checkpoints in myeloma patients is more pronounced at diagnosis: implications for time to progression and response to therapeutic checkpoint inhibitors. Int J Mol Sci (2023) 24(6):5730. doi: 10.3390/ijms24065730
61. Badros A, Hyjek E, Ma N, Lesokhin A, Dogan A, Rapoport AP, et al. Pembrolizumab, pomalidomide, and low-dose dexamethasone for relapsed/refractory multiple myeloma. ScienceDirect (2023) 130(10):1189–97. doi: 10.1182/blood-2017-03-775122
62. Mateos M-V, Orlowski RZ, Ocio EM, Rodríguez-Otero P, Reece D, Moreau P, et al. Pembrolizumab combined with lenalidomide and low-dose dexamethasone for relapsed or refractory multiple myeloma: phase I KEYNOTE-023 study. Br J Haematol (2019) 186(5):e117–21. doi: 10.1111/bjh.15946
63. Usmani SZ, Schjesvold F, Oriol A, Karlin L, Cavo M, Rifkin RM, et al. Pembrolizumab plus lenalidomide and dexamethasone for patients with treatment-naive multiple myeloma (KEYNOTE-185): a randomised, open-label, phase 3 trial. Lancet Haematol (2019) 6(9):e448–58. doi: 10.1016/S2352-3026(19)30109-7
64. Lonial S, Richardson PG, Reece DE, Mohamed H, Shelat S, San Miguel J. CheckMate 602: An open-label, randomized, phase 3 trial of combinations of nivolumab, elotuzumab, pomalidomide and dexamethasone in relapsed/refractory multiple myeloma. J Clin Oncol (2017) 35(15_suppl):TPS8052–TPS8052. doi: 10.1200/JCO.2017.35.15_suppl.TPS8052
65. Mateos M-V, Blacklock H, Schjesvold F, Oriol A, Simpson D, George A, et al. Pembrolizumab plus pomalidomide and dexamethasone for patients with relapsed or refractory multiple myeloma (KEYNOTE-183): a randomised, open-label, phase 3 trial. Lancet Haematol (2019) 6(9):e459–69. doi: 10.1016/S2352-3026(19)30110-3
66. Gonzalez-Montes Y, Rodriguez-Romanos R, Villavicencio A, Osca-Gelis G, González-Bártulos M, Llopis F, et al. Genetic variants of CTLA4 are associated with clinical outcome of patients with multiple myeloma. Front Immunol (2023) 14:1158105. doi: 10.3389/fimmu.2023.1158105
67. Hamdan SO, Sughayer M, Khader M, Tbakhi A, Khudirat S, Hejazi A, et al. Programmed death ligand-1 is frequently expressed in primary acute myeloid leukemia and B-acute lymphoblastic leukemia. Clin Lab (2022) 68(4). doi: 10.7754/Clin.Lab.2021.210701
68. Brodská B, Otevřelová P, Šálek C, Fuchs O, Gašová Z, Kuželová K. High PD-L1 expression predicts for worse outcome of leukemia patients with concomitant NPM1 and FLT3 mutations. Int J Mol Sci (2019) 20(11):2823. doi: 10.3390/ijms20112823
69. Yang H, Bueso-Ramos C, DiNardo C, Estecio MR, Davanlou M, Geng QR, et al. Expression of PD-L1, PD-L2, PD-1 and CTLA4 in myelodysplastic syndromes is enhanced by treatment with hypomethylating agents. Leukemia (2014) 28(6):1280–8. doi: 10.1038/leu.2013.355
70. Daver N, Garcia-Manero G, Basu S, Boddu PC, Alfayez M, Cortes JE, et al. Efficacy, safety, and biomarkers of response to azacitidine and nivolumab in relapsed/refractory acute myeloid leukemia: A non-randomized, open-label, phase 2 study. Cancer Discovery (2019) 9(3):370–83. doi: 10.1158/2159-8290.CD-18-0774
71. Gojo I, Stuart RK, Webster J, Blackford A, Varela JC, Morrow J, et al. Multi-center phase 2 study of pembroluzimab (Pembro) and azacitidine (AZA) in patients with relapsed/refractory acute myeloid leukemia (AML) and in newly diagnosed (≥65 years) AML patients. Blood (2019) 134(Supplement_1):832. doi: 10.1182/blood-2019-127345
72. Assouline S, Michaelis LC, Othus M, Hay AE, Walter RB, Jacoby MA, et al. A randomized phase II/III study of “novel therapeutics” versus azacitidine in newly diagnosed patients with acute myeloid leukemia (AML), high-risk myelodysplastic syndrome (MDS), or chronic myelomonocytic leukemia (CMML), age 60 or older: a report of the comparison of azacitidine and nivolumab to azacitidine: SWOG S1612. Leuk Lymphoma (2023) 64(2):473–7. doi: 10.1080/10428194.2022.2148212
73. Zeidan AM, Boss I, Beach CL, Copeland WB, Thompson E, Fox BA, et al. A randomized phase 2 trial of azacitidine with or without durvalumab as first-line therapy for higher-risk myelodysplastic syndromes. Blood Adv (2022) 6(7):2207–18. doi: 10.1182/bloodadvances.2021005487
74. Garcia JS, Flamand Y, Penter L, Keng M, Tomlinson BK, Mendez LM, et al. Ipilimumab plus decitabine for patients with MDS or AML in posttransplant or transplant-naïve settings. Blood (2023) 141(15):1884–8. doi: 10.1182/blood.2022017686
75. Park SH, You E, Park C-J, Cho YU, Jang S, Im HJ, et al. Increased expression of immune checkpoint programmed cell death protein-1 (PD-1) on T cell subsets of bone marrow aspirates in patients with B-Lymphoblastic leukemia, especially in relapse and at diagnosis. Cytometry B Clin Cytom (2020) 98(4):336–47. doi: 10.1002/cyto.b.21879
76. Cassaday RD, Garcia K-LA, Fromm JR, Percival MM, Turtle CJ, Nghiem PT, et al. Phase 2 study of pembrolizumab for measurable residual disease in adults with acute lymphoblastic leukemia. Blood Adv (2020) 4(14):3239–45. doi: 10.1182/bloodadvances.2020002403
77. Tracy SI, Venkatesh H, Hekim C, Heltemes-Harris LM, Knutson TP. Combining nilotinib and PD-L1 blockade reverses CD4+ T-cell dysfunction and prevents relapse in acute B-cell leukemia. Blood (2022) 140(4):335–48. doi: 10.1182/blood.2021015341
78. Maude SL, Frey N, Shaw PA, Aplenc R, Barrett DM, Bunin NJ, et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N Engl J Med (2014) 371(16):1507–17. doi: 10.1056/NEJMoa1407222
79. Porter DL, Hwang W-T, Frey NV, Lacey SF, Shaw PA, Loren AW, et al. Chimeric antigen receptor T cells persist and induce sustained remissions in relapsed refractory chronic lymphocytic leukemia. Sci Transl Med (2015) 7(303):303ra139. doi: 10.1126/scitranslmed.aac5415
80. Cherkassky L, Morello A, Villena-Vargas J, Feng Y, Dimitrov DS, Jones DR, et al. Human CAR T cells with cell-intrinsic PD-1 checkpoint blockade resist tumor-mediated inhibition. J Clin Invest (2016) 126(8):3130–44. doi: 10.1172/JCI83092
81. Fraietta JA, Lacey SF, Orlando EJ, Pruteanu-Malinici I, Gohil M, Lundh S, et al. Determinants of response and resistance to CD19 chimeric antigen receptor (CAR) T cell therapy of chronic lymphocytic leukemia. Nat Med (2018) 24(5):563–71. doi: 10.1038/s41591-018-0010-1
82. Jacobson CA, Locke FL, Miklos DB, Herrera A, Westin JR, Lee J, et al. End of phase 1 results from zuma-6: axicabtagene ciloleucel (Axi-cel) in combination with atezolizumab for the treatment of patients with refractory diffuse large B cell lymphoma. Blood (2018) 132(Supplement 1):4192. doi: 10.1182/blood-2018-99-111523
83. Hirayama AV, Gauthier J, Hay KA, Sheih A, Cherlan S, Chen X, et al. Efficacy and toxicity of JCAR014 in combination with durvalumab for the treatment of patients with relapsed/refractory aggressive B-cell non-hodgkin lymphoma. Blood (2018) 132(Supplement 1):1680. doi: 10.1182/blood-2018-99-116745
84. Chong EA, Alanio C, Svoboda J, Nasta SD, Landsburg DJ, Lacey SF, et al. Pembrolizumab for B-cell lymphomas relapsing after or refractory to CD19-directed CAR T-cell therapy. Blood (2022) 139(7):1026–38. doi: 10.1182/blood.2021012634
85. Li AM, Hucks GE, Dinofia AM, Self AE, Teachey DT, Baniewicz D, et al. Checkpoint inhibitors augment CD19-directed chimeric antigen receptor (CAR) T cell therapy in relapsed B-cell acute lymphoblastic leukemia. Blood (2018) 132(Supplement 1):556. doi: 10.1182/blood-2018-99-112572
86. Deng Q, Han G, Puebla-Osorio N, Ma MCJ, Strati P, Chasen B, et al. Characteristics of anti-CD19 CAR T cell infusion products associated with efficacy and toxicity in patients with large B cell lymphomas. Nat Med (2020) 26(12):1878–87. doi: 10.1038/s41591-020-1061-7
87. Nguyen LS, Raia L, Lebrun-Vignes B, Salem J-E. Graft versus host disease associated with immune checkpoint inhibitors: A pharmacovigilance study and systematic literature review. Front Pharmacol (2021) 11:619649. doi: 10.3389/fphar.2020.619649
88. Herbaux C, Gauthier J, Brice P, Drumez E, Ysebaert L, Doyen H, et al. Efficacy and tolerability of nivolumab after allogeneic transplantation for relapsed Hodgkin lymphoma. Blood (2017) 129(18):2471–8. doi: 10.1182/blood-2016-11-749556
89. Ito A, Kim S-W, Matsuoka K, Kawakita T, Tanaka T, Inamoto Y, et al. Safety and efficacy of anti-programmed cell death-1 monoclonal antibodies before and after allogeneic hematopoietic cell transplantation for relapsed or refractory Hodgkin lymphoma: a multicenter retrospective study. Int J Hematol (2020) 112(5):674–89. doi: 10.1007/s12185-020-02960-4
90. Davids MS, Kim HT, Bachireddy P, Costello C, Liguori R, Savell A, et al. Ipilimumab for patients with relapse after allogeneic transplantation. N Engl J Med (2016) 375(2):143–53. doi: 10.1056/NEJMoa1601202
91. Davids MS, Kim HT, Costello C, Herrera AF, Locke FL, Maegawa RO, et al. A multicenter phase 1 study of nivolumab for relapsed hematologic Malignancies after allogeneic transplantation. Blood (2020) 135(24):2182–91. doi: 10.1182/blood.2019004710
92. Godfrey J, Liu H, Yu J, Tallarico M, Curran E, Artz A, et al. Pembrolizumab for the treatment of disease relapse after allogeneic hematopoietic stem cell transplantation. Blood Adv (2023) 7(6):963–70. doi: 10.1182/bloodadvances.2022008403
93. Merryman RW, Kim HT, Zinzani PL, Carlo-Stella C, Ansell SM, Perales MA, et alSafety and efficacy of allogeneic hematopoietic stem cell transplant after PD-1 blockade in relapsed/refractory lymphoma. | Blood | Am Soc Hematol (2023) 129(10):1380–8. doi: 10.1182/blood-2016-09-738385
94. Martínez C, Carpio C, Heras I, Ríos-Herranz E, Buch J, Gutierrez A, et al. Potential survival benefit for patients receiving allogeneic hematopoietic stem cell transplantation after nivolumab therapy for relapse/refractory hodgkin lymphoma: real-life experience in Spain. Biol Blood Marrow Transplant (2020) 26(8):1534–42. doi: 10.1016/j.bbmt.2020.02.003
95. Ikegawa S, Meguri Y, Kondo T, Sugiura H, Sando Y, Nakamura M, et al. PTCy ameliorates GVHD by restoring regulatory and effector T-cell homeostasis in recipients with PD-1 blockade. Blood Adv (2019) 3(23):4081–94. doi: 10.1182/bloodadvances.2019000134
96. Oran B, Garcia-Manero G, Saliba RM, Alfayez M, Al-Atrash G, Ciurea SO, et al. Posttransplantation cyclophosphamide improves transplantation outcomes in patients with AML/MDS who are treated with checkpoint inhibitors. Cancer (2020) 126(10):2193–205. doi: 10.1002/cncr.32796
97. Tschernia NP, Kumar V, Moore DT, Vincent BG, Coombs CC, Van Deventer H, et al. Safety and efficacy of pembrolizumab prior to allogeneic stem cell transplantation for acute myelogenous leukemia. Transplant Cell Ther (2021) 27(12):1021.e1–1021.e5. doi: 10.1016/j.jtct.2021.08.022
98. De Philippis C, Legrand-Izadifar F, Bramanti S, Giordano L, Montes de Oca C, Duléry R, et al. Checkpoint inhibition before haploidentical transplantation with posttransplant cyclophosphamide in Hodgkin lymphoma. Blood Adv (2020) 4(7):1242–9. doi: 10.1182/bloodadvances.2019001336
99. Maruhashi T, Sugiura D, Okazaki I, Shimizu K, Maeda TK, Ikubo J, et al. Binding of LAG-3 to stable peptide-MHC class II limits T cell function and suppresses autoimmunity and anti-cancer immunity. Immunity (2022) 55(5):912–924.e8. doi: 10.1016/j.immuni.2022.03.013
100. Wang J, Sanmamed MF, Datar I, Su TT, Ji L, Sun J, et al. Fibrinogen-like protein 1 is a major immune inhibitory ligand of LAG3. Cell (2019) 176(1–2):334–347.e12. doi: 10.1016/j.cell.2018.11.010
101. Yang Z-Z, Kim HJ, Villasboas JC, Chen YP, Price-Troska T, Jalali S, et al. Expression of LAG-3 defines exhaustion of intratumoral PD-1+ T cells and correlates with poor outcome in follicular lymphoma. Oncotarget (2017) 8(37):61425–39. doi: 10.18632/oncotarget.18251
102. Shapiro M, Herishanu Y, Katz B-Z, Dezorella N, Sun C, Kay S, et al. Lymphocyte activation gene 3: a novel therapeutic target in chronic lymphocytic leukemia. Haematologica (2017) 102(5):874–82. doi: 10.3324/haematol.2016.148965
103. Lee H, Yoon SE, Kim SJ, Kim WS, Cho J. A unique expression pattern of LAG3 distinct from that of other immune checkpoints in diffuse large B-cell lymphoma. Cancer Med (2023) 12(15):16359–69. doi: 10.1002/cam4.6268
104. Wright K, Weirather JL, Jiang S, Kao KZ, Sigal Y, Giobbie-Hurder A, et al. Diffuse large B-cell lymphomas have spatially-defined tumor-immune microenvironments revealed by high-parameter imaging. Blood Adv (2023) 7(16):4633–46. doi: 10.1182/bloodadvances.2023009813
105. Sordo-Bahamonde C, Lorenzo-Herrero S, González-Rodríguez AP, Payer ÁR, González-García E, López-Soto A, et al. LAG-3 blockade with relatlimab (BMS-986016) restores anti-leukemic responses in chronic lymphocytic leukemia. Cancers (2021) 13(9):2112. doi: 10.3390/cancers13092112
106. Study Record | Beta ClinicalTrials.gov (2023). Available at: https://clinicaltrials.gov/study/NCT02061761?cond=Leukemia%20OR%20Lymphoma&term=LAG-3%20OR%20Relatlimab&tab=results&rank=6.
107. Zhu C, Anderson AC, Schubart A, Xiong H, Imitola J, Khoury SJ, et al. The Tim-3 ligand galectin-9 negatively regulates T helper type 1 immunity. Nat Immunol (2005) 6(12):1245–52. doi: 10.1038/ni1271
108. Wu Z, Ou J, Liu N, Wang Z, Chen J, Cai Z, et al. Upregulation of Tim-3 is associated with poor prognosis in acute myeloid leukemia. Cancer Med (2023) 12(7):8956–69. doi: 10.1002/cam4.5549
109. Rezaei M, Tan J, Zeng C, Li Y, Ganjalikhani-Hakemi M. TIM-3 in Leukemia; immune response and beyond. Front Oncol (2021) 11:753677. doi: 10.3389/fonc.2021.753677
110. Kikushige Y, Shima T, Takayanagi S, Urata S, Miyamoto T, Iwasaki H, et al. TIM-3 is a promising target to selectively kill acute myeloid leukemia stem cells. Cell Stem Cell (2010) 7(6):708–17. doi: 10.1016/j.stem.2010.11.014
111. Zhou Q, Munger ME, Veenstra RG, Weigel BJ, Hirashima M, Munn DH, et al. Coexpression of Tim-3 and PD-1 identifies a CD8+ T-cell exhaustion phenotype in mice with disseminated acute myelogenous leukemia. Blood (2011) 117(17):4501–10. doi: 10.1182/blood-2010-10-310425
112. Wu H, Sun H-C, Ouyang G-F. T-cell immunoglobulin mucin molecule-3, transformation growth factor β, and chemokine-12 and the prognostic status of diffuse large B-cell lymphoma. World J Clin cases (2022) 10(32):11804–11. doi: 10.12998/wjcc.v10.i32.11804
113. Naghavi Alhosseini M, Palazzo M, Cari L, Ronchetti S, Migliorati G, Nocentini G. Overexpression of potential markers of regulatory and exhausted CD8+ T cells in the peripheral blood mononuclear cells of patients with B-acute lymphoblastic leukemia. Int J Mol Sci (2023) 24(5):4526. doi: 10.3390/ijms24054526
114. Irani YD, Kok CH, Clarson J, Shanmuganathan N, Branford S, Yeung DT, et al. Association of TIM-3 checkpoint receptor expression on T cells with treatment-free remission in chronic myeloid leukemia. Blood Adv (2023) 7(11):2364–74. doi: 10.1182/bloodadvances.2022008854
115. Zeidan AM, Giagounidis A, Sekeres MA, Xiao Z, Sanz GF, Hoef MV, et al. STIMULUS-MDS2 design and rationale: a phase III trial with the anti-TIM-3 sabatolimab (MBG453) + azacitidine in higher risk MDS and CMML-2. Future Oncol (2023) 19(9):631–42. doi: 10.2217/fon-2022-1237
116. Schwartz S, Patel N, Longmire T, Jayaraman P, Jiang X, Lu H, et al. Characterization of sabatolimab, a novel immunotherapy with immuno-myeloid activity directed against TIM-3 receptor. Immunother Adv (2022) 2(1):ltac019. doi: 10.1093/immadv/ltac019
117. Zeidan AM, Ando K, Rauzy O, Turgut M, Wang MC, Cairoli R, et al. Primary results of stimulus-MDS1: A randomized, double-blind, placebo-controlled phase II study of TIM-3 inhibition with sabatolimab added to hypomethylating agents (HMAs) in adult patients with higher-risk myelodysplastic syndromes (MDS). Blood (2022) 140(Supplement 1):2063–5. doi: 10.1182/blood-2022-158612
118. Wu M, Wu A, Zhang X, Li Y, Li B, Jin S, et al. Identification of a novel small-molecule inhibitor targeting TIM-3 for cancer immunotherapy. Biochem Pharmacol (2023) 212:115583. doi: 10.1016/j.bcp.2023.115583
119. Study record | Beta clinicalTrials.gov (2023). Available at: https://clinicaltrials.gov/study/NCT03489343?cond=Leukemia%20OR%20Lymphoma&term=TIM-3%20OR%20sabatolimab&limit=25&page=1&viewType=Table&rank=3&tab=results.
120. Ge Z, Peppelenbosch MP, Sprengers D, Kwekkeboom J. TIGIT, the next step towards successful combination immune checkpoint therapy in cancer. Front Immunol (2021) 12:699895. doi: 10.3389/fimmu.2021.699895
121. Jin S, Zhang Y, Zhou F, Chen X, Sheng J, Zhang J. TIGIT: A promising target to overcome the barrier of immunotherapy in hematological Malignancies. Front Oncol (2022) 12:1091782. doi: 10.3389/fonc.2022.1091782
122. Joller N, Hafler JP, Brynedal B, Kassam N, Spoerl S, Levin SD, et al. Cutting edge: TIGIT has T cell-intrinsic inhibitory functions. J Immunol Baltim Md 1950 (2011) 186(3):1338–42. doi: 10.4049/jimmunol.1003081
123. Chen X, Lu P-H, Liu L, Fang ZM, Duan W, Liu ZL, et al. TIGIT negatively regulates inflammation by altering macrophage phenotype. Immunobiology (2016) 221(1):48–55. doi: 10.1016/j.imbio.2015.08.003
124. Masson D, Jarry A, Baury B, Blanchardie P, Laboisse C, Lustenberger P, et al. Overexpression of the CD155 gene in human colorectal carcinoma. Gut (2001) 49(2):236–40. doi: 10.1136/gut.49.2.236
125. Oshima T, Sato S, Kato J, Ito Y, Watanabe T, Tsuji I, et al. Nectin-2 is a potential target for antibody therapy of breast and ovarian cancers. Mol Cancer (2013) 12:60. doi: 10.1186/1476-4598-12-60
126. Solomon BL, Garrido-Laguna I. TIGIT: a novel immunotherapy target moving from bench to bedside. Cancer Immunol Immunother CII (2018) 67(11):1659–67. doi: 10.1007/s00262-018-2246-5
127. Josefsson SE, Huse K, Kolstad A, Beiske K, Pende D, Steen CB, et al. T cells expressing checkpoint receptor TIGIT are enriched in follicular lymphoma tumors and characterized by reversible suppression of T-cell receptor signaling. Clin Cancer Res Off J Am Assoc Cancer Res (2018) 24(4):870–81. doi: 10.1158/1078-0432.CCR-17-2337
128. Catakovic K, Gassner FJ, Ratswohl C, Zaborsky N, Rebhandl S, Schubert M, et al. TIGIT expressing CD4+T cells represent a tumor-supportive T cell subset in chronic lymphocytic leukemia. Oncoimmunology (2017) 7(1):e1371399. doi: 10.1080/2162402X.2017.1371399
129. Hattori N, Kawaguchi Y, Sasaki Y, Shimada S, Murai S, Abe M, et al. Monitoring TIGIT/DNAM-1 and PVR/PVRL2 immune checkpoint expression levels in allogeneic stem cell transplantation for acute myeloid leukemia. Biol Blood Marrow Transplant (2019) 25(5):861–7. doi: 10.1016/j.bbmt.2019.01.013
130. Minnie SA, Kuns RD, Gartlan KH, Zhang P, Wilkinson AN, Samson L, et al. Myeloma escape after stem cell transplantation is a consequence of T-cell exhaustion and is prevented by TIGIT blockade. Blood (2018) 132(16):1675–88. doi: 10.1182/blood-2018-01-825240
131. Jiang VC, Hao D, Jain P, Li Y, Cai Q, Yao Y, et al. TIGIT is the central player in T-cell suppression associated with CAR T-cell relapse in mantle cell lymphoma. Mol Cancer (2022) 21(1):185. doi: 10.1186/s12943-022-01655-0
132. Jaiswal S, Jamieson CHM, Pang WW, Park CY, Chao MP, Majeti R, et al. CD47 is upregulated on circulating hematopoietic stem cells and leukemia cells to avoid phagocytosis. Cell (2009) 138(2):271–85. doi: 10.1016/j.cell.2009.05.046
133. Chao MP, Tang C, Pachynski RK, Chin R, Majeti R, Weissman IL. Extranodal dissemination of non-Hodgkin lymphoma requires CD47 and is inhibited by anti-CD47 antibody therapy. Blood (2011) 118(18):4890–901. doi: 10.1182/blood-2011-02-338020
134. Kim D, Wang J, Willingham SB, Martin R, Wernig G, Weissman IL. Anti-CD47 antibodies promote phagocytosis and inhibit the growth of human myeloma cells. Leukemia (2012) 26(12):2538–45. doi: 10.1038/leu.2012.141
135. Hao Y, Zhou X, Li Y, Li B, Cheng L. The CD47-SIRPα axis is a promising target for cancer immunotherapies. Int Immunopharmacol (2023) 120:110255. doi: 10.1016/j.intimp.2023.110255
136. Majeti R, Chao MP, Alizadeh AA, Pang WW, Jaiswal S, Gibbs KD Jr, et al. CD47 is an adverse prognostic factor and therapeutic antibody target on human acute myeloid leukemia stem cells. Cell (2009) 138(2):286–99. doi: 10.1016/j.cell.2009.05.045
137. Advani R, Flinn I, Popplewell L, Forero A, Bartlett NL, Ghosh N, et al. CD47 blockade by hu5F9-G4 and rituximab in non-hodgkin’s lymphoma. N Engl J Med (2018) 379(18):1711–21. doi: 10.1056/NEJMoa1807315
138. Sallman DA, Al Malki M, Asch AS, Junseung Lee D, Kambhampati S, Donnellan WB, et al. Tolerability and efficacy of the first-in-class anti-CD47 antibody magrolimab combined with azacitidine in MDS and AML patients: Phase Ib results. J Clin Oncol (2020) 38(15_suppl):7507–7. doi: 10.1200/JCO.2020.38.15_suppl.7507
139. Abrisqueta P, Sancho J-M, Cordoba R, Persky DO, Andreadis C, Huntington S, et al. Anti-CD47 antibody, CC-90002, in combination with rituximab in subjects with relapsed and/or refractory non-hodgkin lymphoma (R/R NHL). Blood (2019) 134:4089. doi: 10.1182/blood-2019-125310
140. Zeidan AM, DeAngelo DJ, Palmer J, Seet CS, Tallman MS, Wei X, et al. Phase 1 study of anti-CD47 monoclonal antibody CC-90002 in patients with relapsed/refractory acute myeloid leukemia and high-risk myelodysplastic syndrome. Ann Hematol (2022) 101(3):557–69. doi: 10.1007/s00277-021-04734-2
141. Meng Z, Wang Z, Guo B, Cao W, Shen H. TJC4, a differentiated anti-CD47 antibody with novel epitope and RBC sparing properties. Blood (2019) 134:4063. doi: 10.1182/blood-2019-122793
142. Mehta A, Harb W, Xu C, Meng Y, Lee L, Yuan V, et al. Lemzoparlimab, a differentiated anti-CD47 antibody in combination with rituximab in relapsed and refractory non-hodgkin’s lymphoma: initial clinical results. Blood (2021) 138:3542. doi: 10.1182/blood-2021-150606
143. Qi J, Li J, Jiang B, Jiang B, Liu H, Cao X, et al. A phase I/IIa study of lemzoparlimab, a monoclonal antibody targeting CD47, in patients with relapsed and/or refractory acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS): initial phase I results. Blood (2020) 136:30–1. doi: 10.1182/blood-2020-134391
144. Marks JD, Griffiths AD, Malmqvist M, Clackson TP, Bye JM, Winter G. By–passing immunization: building high affinity human antibodies by chain shuffling. Bio/Technology (1992) 10(7):779–83. doi: 10.1038/nbt0792-779
145. Horwitz SM, Foran JM, Maris M, Lue JK, Sawas A, Okada C, et al. Updates from ongoing, first-in-human phase 1 dose escalation and expansion study of TTI-621, a novel biologic targeting CD47, in patients with relapsed or refractory hematologic Malignancies. Blood (2021) 138:2448. doi: 10.1182/blood-2021-154490
146. Querfeld C, Thompson JA, Taylor MH, DeSimone JA, Zain JM, Shustov AR, et al. Intralesional TTI-621, a novel biologic targeting the innate immune checkpoint CD47, in patients with relapsed or refractory mycosis fungoides or Sézary syndrome: a multicentre, phase 1 study. Lancet Haematol (2021) 8(11):e808–17. doi: 10.1016/S2352-3026(21)00271-4
147. Patel K, Zonder JA, Sano D, Maris M, Lesokhin A, von Keudell G, et al. CD47-blocker TTI-622 shows single-agent activity in patients with advanced relapsed or refractory lymphoma: update from the ongoing first-in-human dose escalation study. Blood (2021) 138:3560. doi: 10.1182/blood-2021-153683
148. Kim TM, Lakhani N, Gainor J, Kamdar M, Fanning P, Squifflet P, et al. ALX148, a CD47 blocker, in combination with rituximab in patients with non-hodgkin lymphoma. Blood (2020) 136:13–4. doi: 10.1182/blood-2020-135941
149. Sun M, Qi J, Zheng W, Song L, Jiang B, Wang Z, et al. Preliminary results of a first-in-human phase I dtudy of IMM01, SIRPα Fc protein in patients with relapsed or refractory lymphoma. J Clin Oncol (2021) 39(15_suppl):2550–0. doi: 10.1200/JCO.2021.39.15_suppl.2550
150. Yu J, Li S, Chen D, Liu D, Guo H, Yang C, et al. IMM0306, a fusion protein of CD20 mAb with the CD47 binding domain of SIRPα, exerts excellent cancer killing efficacy by activating both macrophages and NK cells via blockade of CD47-SIRPα interaction and FcɣR engagement by simultaneously binding to CD47 and CD20 of B cells. Leukemia (2023) 37(3):695–8. doi: 10.1038/s41375-022-01805-9
151. Buatois V, Johnson Z, Pires SS, Papaioannou A, Hatterer E, Chauchet X, et al. Preclinical development of a bispecific antibody that safely and effectively targets CD19 and CD47 for the treatment of B cell lymphoma and leukemia. Mol Cancer Ther (2018) 17(8):1739–51. doi: 10.1158/1535-7163.MCT-17-1095
152. Benson DM, Hofmeister CC, Padmanabhan S, Suvannasankha A, Jagannath S, Abonour R, et al. A phase 1 trial of the anti-KIR antibody IPH2101 in patients with relapsed/refractory multiple myeloma. Blood (2012) 120(22):4324–33. doi: 10.1182/blood-2012-06-438028
153. Vey N, Bourhis J-H, Boissel N, Bordessoule D, Prebet T, Charbonnier A, et al. A phase 1 trial of the anti-inhibitory KIR mAb IPH2101 for AML in complete remission. Blood (2012) 120(22):4317–23. doi: 10.1182/blood-2012-06-437558
154. Bakhtiari T, Ahmadvand M, Salmaninejad A, Ghaderi A, Yaghmaie M, Sadeghi A, et al. The influence of KIR gene polymorphisms and KIR-ligand binding on outcomes in hematologic Malignancies following haploidentical stem cell transplantation: A comprehensive review. Curr Cancer Drug Targets (2023) 23(11):868–78. doi: 10.2174/1568009623666230523155808
Keywords: hematologic malignancies, leukemia, lymphoma, checkpoint inhibitors, immunotherapy, cd47, LAG-3, TIGIT
Citation: Tsumura A, Levis D and Tuscano JM (2023) Checkpoint inhibition in hematologic malignancies. Front. Oncol. 13:1288172. doi: 10.3389/fonc.2023.1288172
Received: 03 September 2023; Accepted: 04 October 2023;
Published: 17 October 2023.
Edited by:
Jeffrey J. Pu, Harvard Medical School, United StatesReviewed by:
Jiaxiong Tan, Jinan University, ChinaCopyright © 2023 Tsumura, Levis and Tuscano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aaron Tsumura, YW10c3VtdXJhQHVjZGF2aXMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.