
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Oncol. , 18 January 2024
Sec. Thoracic Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1287902
This article is part of the Research Topic Treatment Strategies for Lung Cancer: A Progress Update and Future Perspectives View all 6 articles
 Ramón A. Ortiz Carrodeguas1†
Ramón A. Ortiz Carrodeguas1† Geidy Lorenzo Monteagudo2†Pedro P. Guerra Chaviano3Irene Álvarez Montané4Eva E. Salomón Saldívar5Leonardo Lobaina Lambert6Kirenia Camacho Sosa7Raúl Bermúdez Pino8Poncio Blanco Mustelier9Elba Valdés Rodríguez10Shairis González Piloto11Arelys Guerra de la Vega12
Geidy Lorenzo Monteagudo2†Pedro P. Guerra Chaviano3Irene Álvarez Montané4Eva E. Salomón Saldívar5Leonardo Lobaina Lambert6Kirenia Camacho Sosa7Raúl Bermúdez Pino8Poncio Blanco Mustelier9Elba Valdés Rodríguez10Shairis González Piloto11Arelys Guerra de la Vega12 Lizet Valdés Sánchez2Arasay Montes De Santis2Jenelly Parra Zabala3
Lizet Valdés Sánchez2Arasay Montes De Santis2Jenelly Parra Zabala3 Carmen Viada González2Nadia Calvo Aguilera3
Carmen Viada González2Nadia Calvo Aguilera3 Danay Saavedra Hernández2Orestes Santos Morales2
Danay Saavedra Hernández2Orestes Santos Morales2 Tania Crombet Ramos2*‡
Tania Crombet Ramos2*‡In spite of the advances in immunotherapy and targeted therapies, lung cancer continues to be the leading cause of cancer-related death. The epidermal growth factor receptor is an established target for non-small cell lung cancer (NSCLC), and its overactivation by the ligands can induce accelerated proliferation, angiogenesis, and metastasis as well as proinflammatory or immunosuppressive signals. CIMAvax-EGF is an epidermal growth factor (EGF)-depleting immunotherapy that is approved for the treatment of NSCLC patients in Cuba. The study was designed as a phase IV trial to characterize the safety and effectiveness of CIMAvax-EGF in advanced NSCLC patients treated in 119 community polyclinics and 24 hospitals. CIMAvax-EGF treatment consisted of four bi-weekly doses followed by monthly boosters. Overall, 741 NSCLC patients ineligible for further cancer-specific treatment were enrolled. CIMAvax-EGF was safe, and the most common adverse events consisted of mild-to-moderate injection site reactions, fever, chills, tremors, and headache. For patients completing the loading doses, the median survival was 9.9 months. For individuals achieving at least stable disease to the frontline and completing vaccination induction, the median survival was 12 months. Most of the functional activities and symptoms evaluated through the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire improved over time. In conclusion, this real-world trial demonstrated that CIMAvax-EGF was safe and effective in patients who were vaccinated in the maintenance scenario. A larger effect was seen in subjects with poor prognosis like those with squamous tumors and high EGF levels. Remarkably, this community-based intervention was very important because it demonstrated the feasibility of treating advanced lung cancer patients with active immunotherapy in primary care institutions. In addition to CIMAvax-EGF, patients received supportive care at the community clinic. Vaccine administration by the family doctors at the polyclinics reduced the patients’ burden on the medical oncology services that continued providing chemotherapy and other complex therapies. We conclude that community polyclinics constitute the optimal scenario for administering those cancer vaccines that are safe and require prolonged maintenance in patients with advanced cancer, despite the continuous deterioration of their general condition.
Clinical trial registration: https://rpcec.sld.cu/trials/RPCEC00000205-En, identifier RPCEC00000205.
Lung cancer continues to be the leading cause of cancer-related mortality worldwide. It was estimated that 2,206,771 individuals were diagnosed with lung cancer in 2020 (crude rate of 28.3 cases per 100,000 inhabitants), which represents 11.4% of all types of cancer. Likewise, regarding mortality, 1,796,144 patients died from this disease, which represents 18% of deaths from all types of cancer (1).
Non-small cell lung cancer (NSCLC) is the most common type of lung cancer, accounting for approximately 85% of all lung cancer cases. Roughly 15% of patients with NSCLC are diagnosed in the early stages and present a survival greater than 50% at 5 years. However, more than 70% of cases are diagnosed in advanced stages, stage IIIB (loco-regional advanced disease) or stage IV (metastatic disease), when there are no options for curative treatment. In these cases, the curability rate is low, and close to 90% of patients die before 5 years (2).
Therapeutic options available to treat advanced lung cancer are chemotherapy, radiotherapy, targeted therapies, and immunotherapy. Molecular therapies targeting EGFR, ALK, ROS-1, and mutated KRAS, among others, are the standard of care for patients with sensitizing mutations (3, 4). For patients without mutations, immune checkpoint inhibitors in combination with platinum-based chemotherapy or as monotherapy have been established as the first-line treatment for metastatic disease (5, 6).
The epidermal growth factor receptor (EGFR) is a validated target for NSCLC (7, 8). The overactivation of the EGFR by its ligands can induce the malignant transformation of normal cells by inhibiting apoptosis or inducing cell proliferation, angiogenesis, metastasis, and proinflammatory or immunosuppressive signals (9, 10). The induction of epidermal growth factor (EGF) deprivation through active immunotherapy is an emerging concept developed by the Center of Molecular Immunology (Havana, Cuba). Our approach consists of manipulating the individual’s immune response to generate its own effector antibodies against the growth factor (11, 12). CIMAvax-EGF consists of a chemical conjugate including recombinant EGF and P64, another recombinant protein from Neisseria meningitidis. Montanide ISA 51 VG is used as adjuvant (13). The vaccine is intended to induce a humoral response against EGF, which can prevent the binding of the ligand to the receptor in the cancer cells, thus blocking the pro-tumoral signals (11, 14, 15).
Several clinical trials have been carried out in advanced NSCLC patients, with CIMAvax-EGF approved by the Cuban Regulatory Agency as maintenance after front-line therapy (14, 16–18). The present study was designed as a phase IV trial to characterize the safety and effectiveness of CIMAvax-EGF in IIIB/IV NSCLC patients treated in 119 community polyclinics (primary healthcare institutions) and 24 hospitals (secondary healthcare institutions) of Cuba. A secondary objective of the trial was to evaluate the survival benefit in relation to the EGF basal concentration as well as the quality of life.
Patients of any sex and age ≥ 18 years, with cytology or histology confirmation of NSCLC at the IIIB/IV stage, were enrolled. Other inclusion criteria were the following: individuals who had received the available cancer-specific treatment and had no other treatment option, subjects who signed the informed consent for the investigation, patients with Eastern Cooperative Oncology Group (ECOG) performance status of 0–3 (19) and life expectancy greater than 3 months. The main exclusion criteria comprised a previous history of hypersensitivity to compounds similar to the vaccine; pregnant, lactating, or post-partum women; and subjects with brain metastases.
The study did not have a pre-specified sample size but a safety hypothesis: the administration of CIMAvax-EGF to patients with advanced NSCLC will be safe given that the relative frequency of expected and unexpected serious adverse events, with a definite or probable causal relationship, will not exceed 1% of all patients. The study was opened for 3 years, during which those patients from the participating institutions who complied with the selection criteria and gave their informed consent were recruited.
CIMAvax-EGF was administered by the intramuscular route at a dose of 2.4 mg. The first four doses (induction phase) were administered every 14 days. Then, vaccination continued once a month as long as the patient’s conditions allowed, given that there were no safety concerns. Three days before the first vaccination, patients received an intravenous cyclophosphamide infusion at a low immunomodulatory dose (200 mg/m2). This treatment was administered on an outpatient basis in secondary healthcare institutions. The first CIMAvax-EGF dose was also administered at the hospitals so that trained oncologists could closely monitor the adverse events. Then, the rest of the vaccine doses were administered at the participating community polyclinics, according to the patient’s convenience. CIMAvax-EGF was administered at four injection sites in the two deltoid regions and gluteal regions.
Toxicities were graded according to the National Cancer Institute Common Toxicity Criteria, version 4.0. Lab tests included hematology (hemoglobin, complete blood count (CBC), and hematocrit) as well as alanine aminotransferase, aspartate aminotransferase, glycemia, bilirubin, alkaline phosphatase, creatinine, and urine analysis. These tests were repeated every 3 months. EGF concentration in serum at baseline was quantified with a validated enzyme immunoassay using an ultra-microanalytical system (20). In addition, survival from trial enrolment was evaluated. Several control variables including histology, ECOG performance status, response to front-line therapy, treatment compliance, and EGF concentration at baseline were evaluated in relation to survival. Quality of life was measured using the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 version 3 and the EORTC QLQ-LC13 questionnaires.
The protocol, case report forms, and informed consent were approved by centralized ethical committees (one per province), created ad hoc for this trial, to facilitate the approval process in a large number of primary (119) and secondary (24) healthcare sites. These centralized committees granted the conduction of the trial under the ethical principles embodied in the Declaration of Helsinki (21) and its subsequent updates (22). Since it was a phase IV trial with an approved drug, the national regulatory agency was notified. All patients provided signed informed consent. The trial was registered with the National Public Registry of Clinical Trials (https://rpcec.sld.cu/trials/RPCEC00000205-En).
All adverse events regardless of causality were reported. The frequency distributions of each type of event (related and unrelated) were estimated. Adverse events were also classified considering the intensity, causality, seriousness, treatment, and final results. Lab tests were evaluated considering the normal ranges defined by each clinical site. Overall survival was estimated in the intention to treat (ITT) and per-protocol population (patients who completed four induction doses) by using the standard Kaplan–Meier method. The association between other control variables and survival was evaluated using the standard Kaplan–Meier method and the log-rank test. Regarding quality of life, a longitudinal assessment was carried out every 3 months, and the data were interpreted according to the minimal relevant difference thresholds for the QLQ-C30 (23). Descriptive statistics were assessed for each of the scales before treatment and at months 3, 6, 9, and 12 from treatment. Differences with respect to baseline values for each measurement were estimated. Analyses were performed using SPSS-25.
In total, 741 subjects were included in the trial from January 2016 to December 2019. Last news data were available for all, except for one subject. At the time of follow-up termination and database lock (November 2021), 647 individuals had died, and 93 were alive. The inclusion took place in 24 hospitals nationwide, where the patients received cyclophosphamide and the first vaccine dose. Then, they were referred to 119 polyclinics according to the geographical location of their homes and the regionalization strategy established by each hospital. Before trial initiation, researchers from the polyclinics including the family doctors, nurses, pharmacists, and site coordinators were trained in good clinical practices and received courses on lung cancer, immunotherapy, and cancer vaccines, particularly on CIMAvax-EGF mechanism of action, safety, and efficacy. In addition, family doctors and nurses were qualified in CIMAvax-EGF preparation and mode of administration. Patient demographic and tumor characteristics are described in Table 1. The majority were male, older than 60 years, with stage IV NSCLC, and were current or former smokers. There was a similar proportion of subjects with squamous or adenocarcinomas, and a large percentage (87%) had previous chemotherapy with stable or progressive disease as the best response.
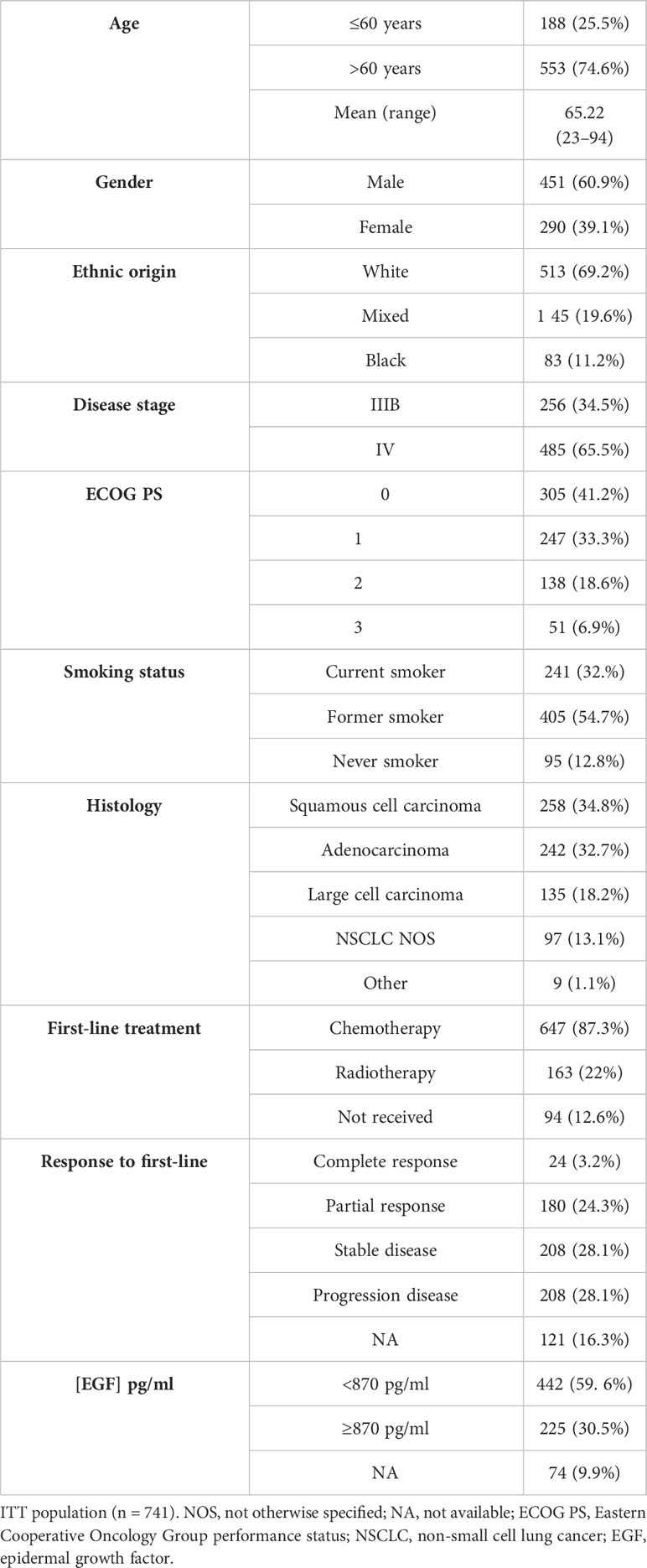
Table 1 Patient demography and baseline characteristics.
The CIMAvax-EGF scheme consisted of four induction and monthly maintenance doses. Overall, 544 (73.4%) individuals completed induction: 77 (10.4%) only received the first four doses, 328 (44.2%) had between five and 15 doses, 78 patients (10.5%) had 16 to 26 CIMAvax-EGF administrations, and 61 subjects (8.32%) received more than 27 injections.
Nineteen patients (2.4%) did not receive any vaccine dose on account of rapid deterioration, while 178 (24%) could not complete the induction scheme of four doses. The most frequent cause of definitive treatment interruption at any time was death (280 patients, 41.2%), followed by worsening of the patient’s condition (207 patients, 27.9%). Death or performance status deterioration was not attributed to CIMAvax-EGF but to the natural course of the disease.
For the safety analysis, 722 patients who received at least one immunization with CIMAvax-EGF were considered. Among these individuals, 459 (57.29%) had at least one adverse event. Overall, 2,389 adverse events were reported. Of these, the largest number (1,846 events) occurred between doses 1 and 6. The most frequent adverse events regardless of causality were injection site pain (268; 11.2%), dyspnea (163; 6.8%), fever (136; 5.7%), chills (83; 3.5%), headache (81; 3.4%), and nausea (80; 3.3%). Among the 2,389 events, 993 (41.6%) were classified as definitively, probably, or possibly related to CIMAvax-EGF. Concerning related adverse events, 667 (67.1%) were mild, 269 (27.0%) were moderate, and 27 (2.7%) were severe. The most common related adverse events included injection site pain, fever, chills, tremors, headache, and nausea. Three patients (0.4%) had five serious related events consisting of anaphylactic shock, tremors (two events), redness of the upper limbs, vagal reaction, and chest pain. The longitudinal evaluation of the most important hematology and biochemistry tests during the first year of CIMAvax-EGF administration is shown in Table 2.
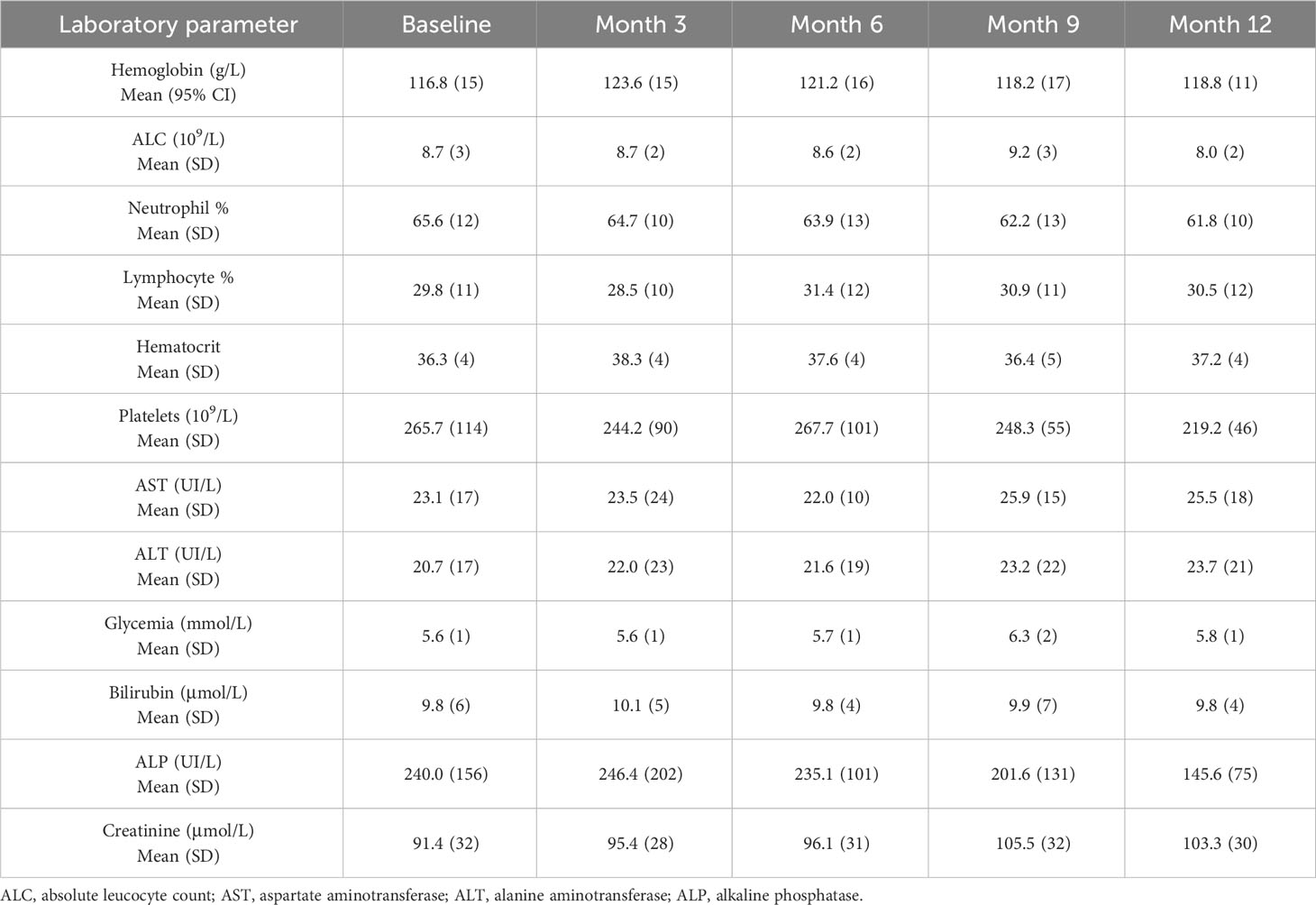
Table 2 Blood test results before and after CIMAvax-EGF treatment for the first year.
Survival was analyzed in the ITT scenario and in those patients who completed vaccination induction. The mean and median survival time (ST) for all patients irrespective of treatment compliance was 13.9 (95% CI 12.6–15.3) and 7.0 months (95% CI 6.3–7.8). The 12- and 24-month survival rates were 32% and 14.7%. For the 550 patients who received at least four vaccine doses, the mean and median STs were 17.6 (95% CI 15.9–19.3) and 9.9 months (95% CI 8.8–11), respectively. The 12- and 24-month survival rates were 42% and 19.5%, respectively.
Finally, survival was evaluated in the subgroup of patients who completed front-line therapy for the advanced disease, achieved at least stable disease (maintenance scenario), and received the four loading doses. In our data set, 412 (55.6%) individuals received front-line therapy, reaching complete, partial, or disease stabilization, and 328 (79.6%) completed induction vaccination. For this subpopulation, the mean and median survival were 20.4 months (95% CI 18–22.8) and 12 months (95% CI 10.6–13.4), respectively. Survival rates were 40.9% and 19.8% after 1 and 2 years, respectively.
In patients who were classified as unfit for chemotherapy and those in progressive disease upon front line, the median survival was 6.9 and 7.4 months, respectively, if completed induction.
In the per-protocol scenario, a separate survival analysis was carried out for some of the control variables including response to front-line chemotherapy, histology, ECOG PS, and EGF concentration at baseline. Figure 1 illustrates the survival curves.
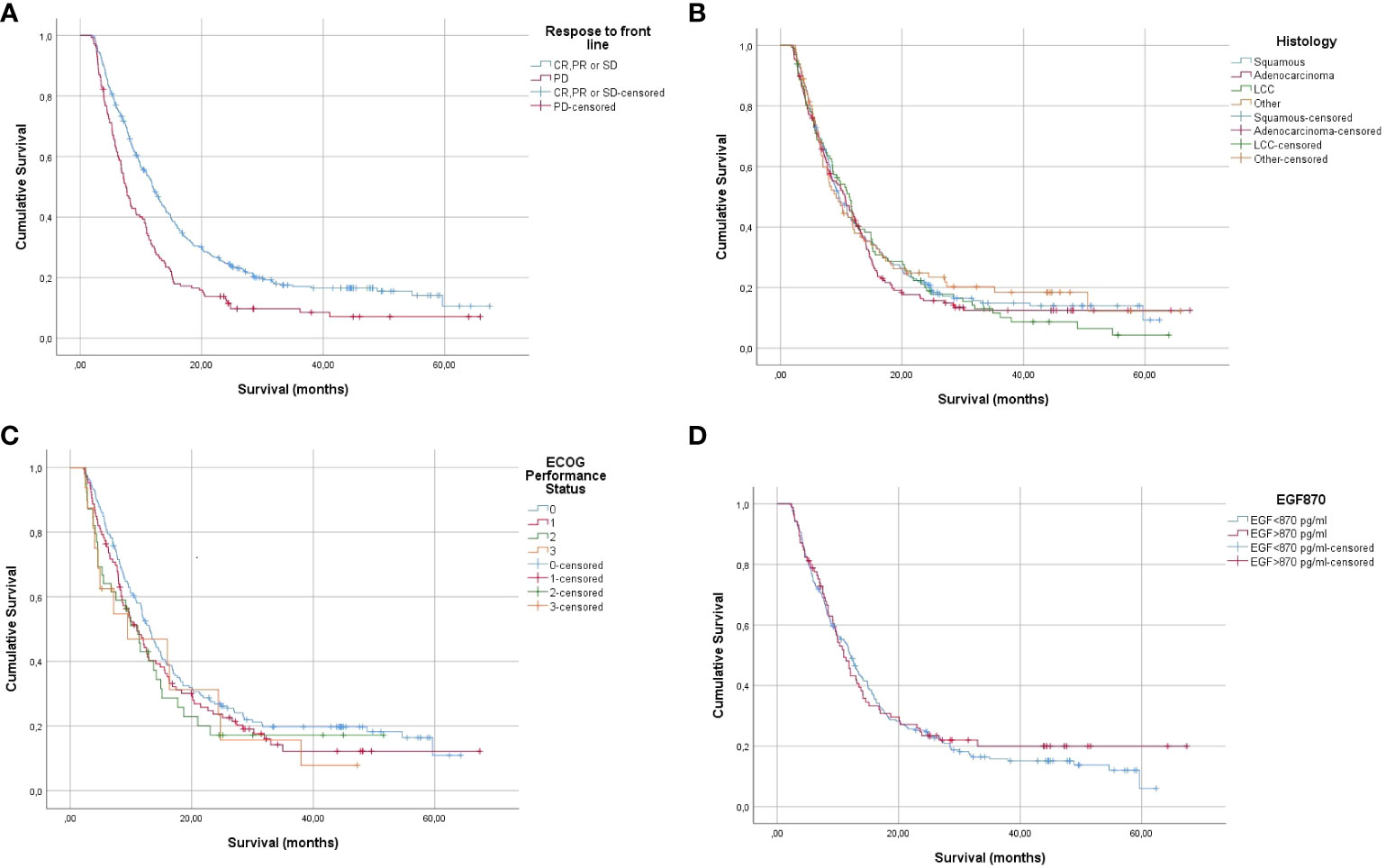
Figure 1 Kaplan–Meier estimates of overall survival of NSCLC patients completing loading CIMAvax-EGF doses according to response to front-line chemotherapy (A), histology (B), ECOG PS (C), and EGF concentration at baseline (D). CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; NSCLC, non-small cell lung cancer; ECOG PS, Eastern Cooperative Oncology Group performance status; EGF, epidermal growth factor.
As expected, significant survival differences were detected for patients achieving at least stable disease after chemotherapy (log-rank p = 0.00011). The median survival of individuals with complete, partial, or stable disease before CIMAvax-EGF was 12 months vs. 7.4 months for those patients who progressed to front-line chemotherapy. Notably, no survival differences were seen in individuals with distinct ECOG performance status, different cancer histology, and EGF concentrations above or below 870 pg/ml. The mean and median survival for subjects with squamous tumors were 20.7 and 11.6 months vs. 21.34 and 13.13 months, respectively, for the adenocarcinoma histology. The 1- and 2-year survival rates were 47.9% and 26.5% in the squamous carcinoma patients and 56.6% and 22.6% in the adenocarcinoma subset. The median survival of the patients with baseline EGF concentration lower or higher than 870 pg/ml was 12.1 and 10.9 months. The survival rate at 24 months was 25.5% and 23.4% for the referred groups.
The evaluation of the antitumor response was not an objective of this phase IV trial since it has been characterized in previous studies (12, 16, 24, 25). Overall, across several CIMAvax-EGF studies, the disease control rate ranges from 30% to 40% and consists mainly of stable disease (12, 16, 24, 25). Notably, in phase 1 where CIMAvax-EGF was combined with nivolumab after the progression of the disease (second-line setting), 33% of the patients achieved partial response, while the overall disease control rate was 50% (26).
The quality of life (QoL) analyses were performed for all the subjects who completed the questionnaires (QLQ-C30 and QLQ-L13) at different time intervals. At baseline, information was available for 665 patients (89.7%), while at month 12, 101 out of the 228 (44.2%) individuals who were alive provided QoL information. Figure 2 presents the results of the functional scales of the QLQ-C30 as well as the symptom scales from the general and lung questionnaires. Each of the items was evaluated over time, and the scoring was compared to the baseline. A difference of 5 to 10 points was classified as a small effect, while a change of 10 to 20 points was cataloged as a moderate effect (27, 28). Overall, the global quality of life, as well as the physical, role, emotional, social, and cognitive functions, improved over time. Regarding the functional scales, after 12 months (the last available evaluation), there was a small improvement in the global and physical functions. Likewise, there was a moderate improvement in the role, emotional, and social functions.
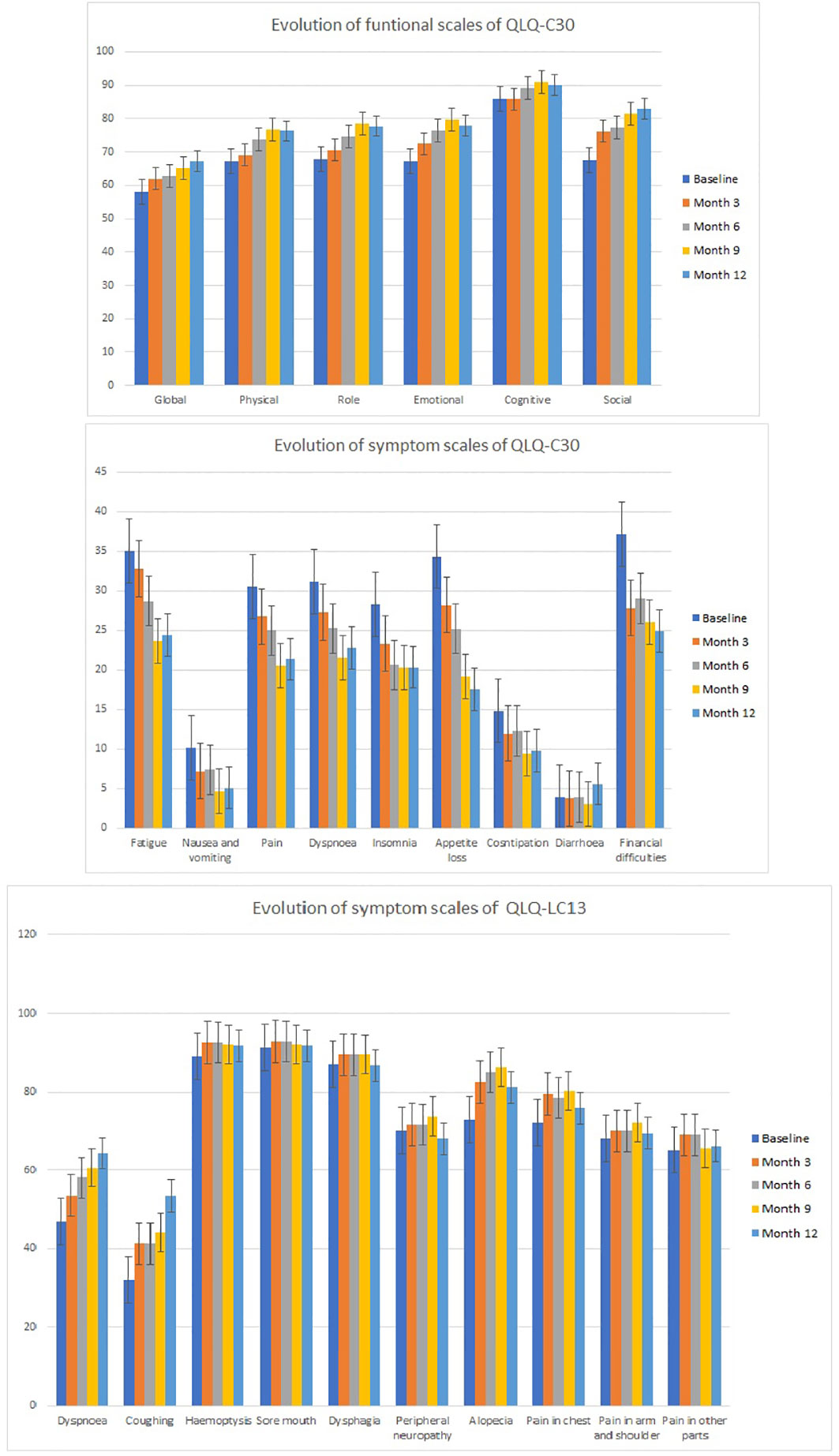
Figure 2 Evaluation of the functional and symptom scales of the EORTC QLQ-C30 questionnaire and the symptoms scale from the EORTC QLQ-L13 questionnaire. EORTC, European Organisation for Research and Treatment of Cancer.
Concerning the symptom evaluation of the QLQ-C30, all items became better with time except diarrhea. A minor recuperation was seen in nausea, pain, dyspnea, insomnia, and constipation, while a moderate improvement in fatigue, appetite loss, and financial difficulties was observed in month 12.
Finally, the QLQ-LC-13 survey detected an improvement in the dysphagia and neuropathy in addition to a small worsening (less than 5 points) in the hemoptysis as well as in the sore mouth, chest, and arm/shoulder and pain in other parts. The magnitude of the worsening had no clinical relevance and can be interpreted as a stabilization of the referred symptoms. On the contrary, in spite of vaccination, there was a moderate worsening of dyspnea and cough. These symptoms were associated with the underlying lung cancer condition and not with CIMAvax-EGF.
This was a phase IV clinical trial of CIMAvax-EGF in patients with advanced NSCLC who did not have any further therapeutic alternative according to the national guidelines. Patients were recruited by the hospitals’ oncologists, who also administered low-dose cyclophosphamide and the first vaccine doses. Then, individuals continued vaccination at the primary care institutions. Clinical evaluation was carried out by the oncologists together with the family physicians every 3 months.
The trial demonstrated that CIMAvax-EGF administration was feasible at the community polyclinics. CIMAvax-EGF is an EGF-depleting immunotherapy with a very good safety profile, which requires monthly maintenance doses that can be prolonged according to the individual response and performance status. In our data set, roughly 20% of the patients were vaccinated over 1 year or more, and remarkably, at the moment of this writing, 44 patients remained vaccinated after 3 years or more. The vaccinated subjects and caregivers acknowledged the convenience of the regular vaccine administration near their houses.
Vaccine compliance was good, and 73% of the patients completed the vaccine loading period. In the previous phase III trial at the hospitals, 81% of the patients successfully finished induction (18). Apart from the referred registration study where all the patients had had front-line platinum doublets and only 5% had progressive disease at enrolment (18), in this real-world scenario trial, 44.4% were in progression or did not have any previous therapy (unfit for chemotherapy).
CIMAvax-EGF was very well tolerated, and the trial fulfilled its safety hypothesis since less than 1% of the patients had serious related adverse events. The most frequent adverse events were consistent with those reported in the previous studies (11, 12, 15, 17, 18). CIMAvax-EGF safety profile was very good in comparison to other drugs used in the maintenance or second-line treatment of advanced NSCLC. In the case of docetaxel, hematological toxicity such as neutropenia, anemia, and thrombocytopenia, as well as non-hematological toxicity including diarrhea, nausea, and vomiting, have been reported (29). Pemetrexed suppresses bone marrow function, but patients can also develop skin reactions and serious renal events, including acute renal failure (30). Alternatively, immune checkpoint inhibitors that boost the natural immune response may induce immune-related adverse events like pneumonitis, colitis, hepatitis, and hypothyroidism (31, 32).
CIMAvax-EGF is being administered to advanced lung cancer patients who are immunocompromised on account of their older age, the cancer itself, and the previous platinum-based chemotherapy, in most cases (33). Apart from conventional chemotherapy that exerts its action directly, this EGF-depleting immunotherapy needs to break the tolerance against a self-growth factor. In consequence, administering a minimum number of doses (four loading doses) is needed to trigger a protective immune response that may slow the progression of the disease. According to our previous data, before completing induction, the frequency of patients achieving a good response against EGF (antibody titles >1:4,000) is less than 50% (14, 34). Our team has consistently found that repeated immunization is also correlated with a higher capacity of blocking the EGF/EGFR binding and inhibiting the EGFR phosphorylation. Furthermore, there is a significant correlation between a good antibody response and survival (11, 14, 34).
This was a phase IV trial carried out in the conditions of routine medical practice. Overall, 27% of the patients did not complete the initial four doses, including 19 individuals who were not vaccinated at all on account of rapid worsening. These figures highlight the importance of selecting the right patients for an active immunotherapy like CIMAvax-EGF. Patients with poor performance status who progressed or were deemed unfit for platinum-based chemotherapy are not the best candidates for vaccine monotherapy.
However, CIMAvax-EGF has been safely administered to stage IV NSCLC patients with progressive disease, in combination with nivolumab in a phase I/II trial, at the Roswell Park Comprehensive Cancer Center (Buffalo, NY). For all patients receiving the anti-PD1 antibody plus the vaccine, the median survival was 13.5 months, while for individuals completing CIMAvax-EGF induction, the median survival was 18.3 months. Particularly, patients with KRAS wild type had a very high median survival (21.7 months) (26). Since KRAS mutations predict resistance to the EGF/EGFR blockade, it is rational to anticipate a larger benefit of CIMAvax-EGF in patients with KRAS wild-type tumors. The same concept has been validated in colorectal cancer individuals treated with the anti-EGFR antibodies cetuximab or panitumumab (35, 36).
In our data set, patients who completed the induction after at least disease stabilization to front-line therapy had a median survival of 12 months. This is comparable with the survival achieved with other drugs used as switch maintenance—docetaxel (12.3 months) (37), pemetrexed (13.4 months) (38), and erlotinib (12.0 months) (39)—but with much lower toxicity. Nevertheless, the preferred approach in current medical practices is to use continuation maintenance with one or some of the front-line drugs for the advanced stage, comprising immune checkpoint inhibitors. The nature of the survival estimation in the continuation maintenance scenario precludes any comparison with switch maintenance, where survival is estimated from the completion of the front line.
Notably, there were no significant differences in the survival of patients with squamous or non-squamous tumors. This result suggests that subjects with squamous histology had greater benefits after vaccination since it is well accepted that the prognosis of adenocarcinoma patients is much better (40, 41). Previous randomized clinical trials have also found a bigger effect in patients with squamous carcinomas, presumably associated with the greater expression of unmutated EGFR in this tumor type (42).
Likewise, patients with low or high EGF concentration in serum had non-different survival. This is precisely what is expected. EGF concentration after front-line therapy in NSCLC has been proposed as a poor prognostic biomarker of the disease and also as a predictive biomarker of higher CIMAvax-EGF efficacy (18, 42). It means that patients with low EGF have a better prognosis, while patients with high EGF would have a poorer prognosis but a larger survival gain with CIMAvax-EGF.
Quality of life is very important since the majority of conventional antitumor treatment for lung cancer increases survival at a cost of significant toxicity and QoL deterioration (43, 44). Globally, there was a trend toward improvement over time in the functional activities and the symptoms evaluated through the general questionnaire. However, symptoms particularly associated with lung cancer evidenced small deterioration lacking clinical relevance except the dyspnea and coughing that became worse after 6 months, coinciding with the natural history of the disease. We concluded that CIMAvax-EGF did not negatively affect quality of life, but on the contrary, it improved some of the functions and symptoms of late-stage cancer patients. Major limitations of this assessment are associated with the lack of a control arm that prevents the evaluation of the symptoms and functional scales in untreated individuals and with the missing information, mainly at late time points.
In summary, this clinical trial was particularly important because it demonstrated the feasibility and advantages of treating advanced lung cancer patients with active specific immunotherapy in primary healthcare institutions. The use of CIMAvax-EGF was extended to a large number of community polyclinics for the first time. CIMAvax-EGF administration by the family doctors at the community polyclinics significantly reduced the patients’ burden on the medical oncology services that continued providing chemotherapy and other complex therapies. Family doctors also provided supportive therapy as well as end-of-life care. This real-world scenario study confirmed that CIMAvax-EGF, as monotherapy, was safe and effective in patients who were vaccinated in the maintenance setting after a good response to the front-line therapy. The importance of vaccinating the right patients with an adequate life expectancy and performance status was also confirmed. Preliminary findings also support the largest impact of CIMAvax-EGF in patients with poor prognosis like those with squamous tumors and high EGF serum levels. New clinical trials where CIMAvax-EGF is combined with other immunomodulatory drugs including anti-PD1 antibodies are ongoing in NSCLC patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Celestino Hernández Hospital ethic committee and other IRBs established at hoc in each province for the clinical trial. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ROC: Conceptualization, Formal Analysis, Investigation, Supervision, Writing – review & editing. GLM: Conceptualization, Formal Analysis, Investigation, Supervision, Writing – review & editing. PGC: Investigation, Methodology, Supervision, Writing – review & editing. IÁM: Investigation, Writing – review & editing. ESS: Investigation, Writing – review & editing. LLL: Investigation, Writing – review & editing. KCS: Investigation, Writing – review & editing. RBP: Investigation, Writing – review & editing. PBM: Investigation, Writing – review & editing. EVR: Investigation, Writing – review & editing. SGP: Investigation, Writing – review & editing. AGV: Investigation, Writing – review & editing. LSV: Data curation, Formal Analysis, Investigation, Methodology, Writing – review & editing. AMS: Data curation, Software, Writing – review & editing. JPZ: Data curation, Writing – review & editing. CVG: Data curation, Formal Analysis, Writing – review & editing. NCA: Data curation, Writing – review & editing. DSH: Investigation, Supervision, Writing – review & editing. OSM: Investigation, Project administration, Supervision, Writing – review & editing. TCR: Conceptualization, Formal Analysis, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Cuban Ministry of Health and the Center of Molecular Immunology.
The authors express their gratitude to all family doctors, oncologists, research nurses, pharmacists, and general staff working with lung cancer patients in the hospitals as well as in the 119 community polyclinics.
Seven authors GLM, LSV, AMS, CVG, DSH, OSM and TCR works for the Center of Molecular Immunology, the institution that patented and manufactures CIMAvax-EGF.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Miller KD, Nogueira L, Devasia T, Mariotto AB, Yabroff KR, Jemal A, et al. Cancer treatment and survivorship statistics, 2022. CA CANCER J CLIN (2022) 72(5):409–36. doi: 10.3322/caac.21731
3. Alduais Y, Zhang H, Fan F, Chen J, Chen B. Non-small cell lung cancer (NSCLC): A review of risk factors. diagnosis Treat (2023) 102(8):e32899. doi: 10.1097/MD.0000000000032899
4. Rohilla S, Singh M, Alzarea SI, Almalki WH, Al-Abbasi FA, Kazmi I, et al. Recent developments and challenges in molecular-targeted therapy of non-small-cell lung cancer. J Environ Pathol Toxicol Oncol (2023) 42(1):27–50. doi: 10.1615/JEnvironPatholToxicolOncol.2022042983
5. Onoi K, Chihara Y, Uchino J, Shimamoto T, Morimoto Y, Iwasaku M, et al. Immune checkpoint inhibitors for lung cancer treatment: a review. J Clin Med (2020) 9(5):1362. doi: 10.3390/jcm9051362
6. Mencoboni M, Ceppi M, Bruzzone M, Taveggia P, Cavo A, Scordamaglia F, et al. Effectiveness and safety of immune checkpoint inhibitors for patients with advanced non small-cell lung cancer in real-world: review and meta-analysis. Cancers (2021) 13(6):1388. doi: 10.3390/cancers13061388
7. Sheikine Y, Rangachari D, McDonald DC, Huberman MS, Folch ES, VanderLaan PA, et al. EGFR testing in advanced non–small-cell lung cancer, a mini-review. Clin Lung Cancer (2016) 17(6):483–92. doi: 10.1016/j.cllc.2016.05.016
8. Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res (2015) 5(9):2892.
9. Herbst RS. Review of epidermal growth factor receptor biology. Int J Rad Oncol Biol Phys (2004) 59(2):S21–S6. doi: 10.1016/j.ijrobp.2003.11.041
10. Yewale C, Baradia D, Vhora I, Patil S, Misra A. Epidermal growth factor receptor targeting in cancer: a review of trends and strategies. Biomaterials (2013) 34(34):8690–707. doi: 10.1016/j.biomaterials.2013.07.100
11. Crombet-Ramos T, Rodriguez PC, Neninger-Vinageras E, Garcia-Verdecia B, Lage-Davila A. CIMAvax EGF (EGF-P64K) vaccine for the treatment of non-small-cell lung cancer. Expert Rev Vaccines (2015) 14(10):1303–11. doi: 10.1586/14760584.2015.1079488
12. Gonzalez G, Crombet T, Catala M, Mirabal V, Hernandez JC, Gonzalez Y, et al. A novel cancer vaccine composed of human-recombinant epidermal growth factor linked to a carrier protein: report of a pilot clinical trial. Ann Oncol (1998) 9(4):431–5. doi: 10.1023/a:1008261031034
13. Ascarateil S, Puget A, Gaucheron J, Koziol M-E. Sustained release of actives with Montanide™ ISA 51 VG and Montanide™ ISA 720 VG, two adjuvants dedicated to human therapeutic vaccines. J Immunother Cancer (2015) 2(Suppl 2):P429. doi: 10.1186/2051-1426-3-S2-P429
14. Garcia B, Neninger E, de la Torre A, Leonard I, Martinez R, Viada C, et al. Effective inhibition of the epidermal growth factor/epidermal growth factor receptor binding by anti-epidermal growth factor antibodies is related to better survival in advanced non-small-cell lung cancer patients treated with the epidermal growth factor cancer vaccine. Clin Cancer Res (2008) 14(3):840–6. doi: 10.1158/1078-0432.CCR-07-1050
15. Gonzalez G, Crombet T, Lage A. Chronic vaccination with a therapeutic EGF-based cancer vaccine: a review of patients receiving long lasting treatment. Curr Cancer Drug Targets. (2011) 11(1):103–10. doi: 10.2174/156800911793743583
16. Gonzalez G, Crombet T, Neninger E, Viada C, Lage A. Therapeutic vaccination with epidermal growth factor (EGF) in advanced lung cancer: analysis of pooled data from three clinical trials. Hum Vaccin. (2007) 3(1):8–13. doi: 10.4161/hv.3.1.3537
17. Neninger Vinageras E, de la Torre A, Osorio Rodriguez M, Catala Ferrer M, Bravo I, Mendoza del Pino M, et al. Phase II randomized controlled trial of an epidermal growth factor vaccine in advanced non-small-cell lung cancer. J Clin Oncol (2008) 26(9):1452–8. doi: 10.1200/JCO.2007.11.5980
18. Rodriguez PC, Popa X, Martinez O, Mendoza S, Santiesteban E, Crespo T, et al. A phase III clinical trial of the epidermal growth factor vaccine CIMAvax-EGF as switch maintenance therapy in advanced non-small cell lung cancer patients. Clin Cancer Res (2016) 22(15):3782–90. doi: 10.1158/1078-0432.CCR-15-0855
19. Datta SS, Ghosal N, Daruvala R, Chakraborty S, Shrimali RK, van Zanten C, et al. How do clinicians rate patient’s performance status using the ECOG performance scale? A mixed-methods exploration of variability in decision-making in oncology. Ecancermedicalscience (2019) 13:913. doi: 10.3332/ecancer.2019.913
20. Castells Martínez EM, Del Valle R, González EC, Melchor A, Pérez PL, González I, et al. An enzyme immunoassay for determining epidermal growth factor (EGF) in human serum samples using an ultramicroanalytical system. J Immunoassay Immunochem (2017) 38(2):190–201. doi: 10.1080/15321819.2016.1236729
21. Holm S. Declaration of helsinki. Int Encyclopedia Ethics (2013) 1-4. doi: 10.1002/9781444367072.wbiee230.pub2
22. Osuna IB, Escobar VA, Pérez MM. Helsinki Declaration: changes and interpretation. Revista Cubana de Salud Pública (2016) 42(1):132–42.
23. Osoba D. Interpreting the meaningfulness of changes in health-related quality of life scores: lessons from studies in adults. Int J Cancer (1999) 83(S12):132–7. doi: 10.1002/(SICI)1097-0215(1999)83:12+<132::AID-IJC23>3.0.CO;2-4
24. Flores Vega YI, Paramo Gonzalez DL, Alsina Sarmiento SC, Alsina Tul LE, Inguanzo Valdes IB, Rodriguez MaChado J, et al. Survival of NSCLC patients treated with cimavax-EGF as switch maintenance in the real-world scenario. J Cancer. (2023) 14(5):874–9. doi: 10.7150/jca.67189
25. Neninger E, Verdecia BG, Crombet T, Viada C, Pereda S, Leonard I, et al. Combining an EGF-based cancer vaccine with chemotherapy in advanced nonsmall cell lung cancer. J Immunother. (2009) 32(1):92–9. doi: 10.1097/CJI.0b013e31818fe167
26. Evans R, Lee K, Wallace PK, Reid M, Muhitch J, Dozier A, et al. Augmenting antibody response to EGF-depleting immunotherapy: Findings from a phase I trial of CIMAvax-EGF in combination with nivolumab in advanced stage NSCLC. Front Oncol (2022) 12:958043. doi: 10.3389/fonc.2022.958043
27. Scott NW, Fayers P, Aaronson NK, Bottomley A, de Graeff A, Groenvold M, et al. EORTC QLQ-C30 Reference Values. Brussels: EORTC Quality of Life Group (2008).
28. Fayers P, Bottomley A, ORTC Quality of Life Group, Quality of Life Unit. Quality of life research within the EORTC—the EORTC QLQ-C30. Eur J Cancer (2002) 38:125–33. doi: 10.1016/s0959-8049(01)00448-8
29. Pujol J-L, Paul S, Chouaki N, Peterson P, Moore P, Berry DA, et al. Survival without common toxicity criteria grade 3/4 toxicity for pemetrexed compared with docetaxel in previously treated patients with advanced non-small cell lung cancer (NSCLC): a risk-benefit analysis. J Thorac Oncol (2007) 2(5):397–401. doi: 10.1097/01.JTO.0000268672.57002.69
30. Dumoulin DW, Visser S, Cornelissen R, van Gelder T, Vansteenkiste J, von der Thusen J, et al. Renal toxicity from pemetrexed and pembrolizumab in the era of combination therapy in patients with metastatic nonsquamous cell NSCLC. J Thorac Oncol (2020) 15(9):1472–83. doi: 10.1016/j.jtho.2020.04.021
31. Suresh K, Naidoo J, Lin CT, Danoff S. Immune checkpoint immunotherapy for non-small cell lung cancer: benefits and pulmonary toxicities. Chest (2018) 154(6):1416–23. doi: 10.1016/j.chest.2018.08.1048
32. Shao J, Wang C, Ren P, Jiang Y, Tian P, Li W. Treatment-and immune-related adverse events of immune checkpoint inhibitors in advanced lung cancer. Bioscience (2020) 40(5):BSR20192347. doi: 10.1042/BSR20192347
33. Caras I, Grigorescu A, Stavaru C, Radu D, Mogos I, Szegli G, et al. Evidence for immune defects in breast and lung cancer patients. Cancer Immunol, immunother (2004) 53:1146–52. doi: 10.1007/s00262-004-0556-2
34. Popa X, García B, Fuentes KP, Huerta V, Alvarez K, Viada CE, et al. Anti-EGF antibodies as surrogate biomarkers of clinical efficacy in stage IIIB/IV non-small-cell lung cancer patients treated with an optimized CIMAvax-EGF vaccination schedule. Oncoimmunology (2020) 9(1):1762465. doi: 10.1080/2162402X.2020.1762465
35. Martinelli E, Ciardiello D, Martini G, Troiani T, Cardone C, Vitiello PP, et al. Implementing anti-epidermal growth factor receptor (EGFR) therapy in metastatic colorectal cancer: challenges and future perspectives. Ann Oncol (2020) 31(1):30–40. doi: 10.1016/j.annonc.2019.10.007
36. Sorich MJ, Wiese MD, Rowland A, Kichenadasse G, McKinnon RA, Karapetis CS. Extended RAS mutations and anti-EGFR monoclonal antibody survival benefit in metastatic colorectal cancer: a meta-analysis of randomized, controlled trials. Ann Oncol (2015) 26(1):13–21. doi: 10.1093/annonc/mdu378
37. Fidias PM, Dakhil SR, Lyss AP, Loesch DM, Waterhouse DM, Bromund JL, et al. Phase III study of immediate compared with delayed docetaxel after front-line therapy with gemcitabine plus carboplatin in advanced non-small-cell lung cancer. J Clin Oncol (2009) 27(4):591–8. doi: 10.1200/JCO.2008.17.1405
38. Ciuleanu T, Brodowicz T, Zielinski C, Kim JH, Krzakowski M, Laack E, et al. Maintenance pemetrexed plus best supportive care versus placebo plus best supportive care for non-small-cell lung cancer: a randomised, double-blind, phase 3 study. Lancet (2009) 374(9699):1432–40. doi: 10.1016/S0140-6736(09)61497-5
39. Cappuzzo F, Ciuleanu T, Stelmakh L, Cicenas S, Szczésna A, Juhász E, et al. Erlotinib as maintenance treatment in advanced non-small-cell lung cancer: a multicentre, randomised, placebo-controlled phase 3 study. Lancet Oncol (2010) 11(6):521–9. doi: 10.1016/S1470-2045(10)70112-1
40. Wang B-Y, Huang J-Y, Chen H-C, Lin C-H, Lin S-H, Hung W-H, et al. The comparison between adenocarcinoma and squamous cell carcinoma in lung cancer patients. J Cancer Res Clin Oncol (2020) 146:43–52. doi: 10.1007/s00432-019-03079-8
41. Kawase A, Yoshida J, Ishii G, Nakao M, Aokage K, Hishida T, et al. Differences between squamous cell carcinoma and adenocarcinoma of the lung: are adenocarcinoma and squamous cell carcinoma prognostically equal? Jpn J Clin Oncol (2011) 42(3):189–95. doi: 10.1093/jjco/hyr188
42. Crombet Ramos T, Santos Morales O, Dy GK, León Monzón K, Lage Dávila A. The position of EGF deprivation in the management of advanced Non-Small Cell Lung Cancer. Front Onco (2021) 11:639745. doi: 10.3389/fonc.2021.639745
43. Koller M, Warncke S, Hjermstad MJ, Arraras J, Pompili C, Harle A, et al. Use of the lung cancer–specific Quality of Life Questionnaire EORTC QLQ-LC13 in clinical trials: A systematic review of the literature 20 years after its development. Cancer (2015) 121(24):4300–23. doi: 10.1002/cncr.29682
44. Dancey J, Shepherd FA, Gralla RJ, Kim YS. Quality of life assessment of second-line docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy: results of a prospective, randomized phase III trial. Lung Cancer (2004) 43(2):183–94. doi: 10.1016/j.lungcan.2003.09.001
Keywords: CIMAvax-EGF, community polyclinics, primary health care institutions, NSCLC, realworld-data (RWD)
Citation: Ortiz Carrodeguas RA, Lorenzo Monteagudo G, Guerra Chaviano PP, Álvarez Montané I, Salomón Saldívar EE, Lobaina Lambert L, Camacho Sosa K, Bermúdez Pino R, Blanco Mustelier P, Valdés Rodríguez E, González Piloto S, Guerra de la Vega A, Valdés Sánchez L, Montes De Santis A, Parra Zabala J, Viada González C, Calvo Aguilera N, Saavedra Hernández D, Santos Morales O and Crombet Ramos T (2024) Safety and effectiveness of CIMAvax-EGF administered in community polyclinics. Front. Oncol. 13:1287902. doi: 10.3389/fonc.2023.1287902
Received: 18 September 2023; Accepted: 19 December 2023;
Published: 18 January 2024.
Edited by:
Xinhui Wu, University of Groningen, NetherlandsReviewed by:
Paul Zarogoulidis, Euromedica General Clinic, GreeceCopyright © 2024 Ortiz Carrodeguas, Lorenzo Monteagudo, Guerra Chaviano, Álvarez Montané, Salomón Saldívar, Lobaina Lambert, Camacho Sosa, Bermúdez Pino, Blanco Mustelier, Valdés Rodríguez, González Piloto, Guerra de la Vega, Valdés Sánchez, Montes De Santis, Parra Zabala, Viada González, Calvo Aguilera, Saavedra Hernández, Santos Morales and Crombet Ramos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tania Crombet Ramos, dGFuaWFjQGNpbS5zbGQuY3U=
†These authors have contributed equally to this work and share first authorship
‡ORCID: Tania Crombet Ramos, orcid.org/0000-0002-2550-7292
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.