 Xia Liu1
Xia Liu1 Na Yan
Na Yan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 01 November 2023
Sec. Thoracic Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1275575
Objectives: Lung adenocarcinoma (LUAD) is the most common newly diagnosed malignant tumor in older people. As older patients age, organ function decreases, leading to increased adverse reactions to treatment. The epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase tyrosine (ALK) tyrosine kinase inhibitors (TKIs) therapy are more effective and well-tolerated than chemotherapy, while the rate of genetic testing and subsequent targeted treatment among older patients remains relatively low, the clinical benefit limitation for those patients. This study aims to investigate the mutation characteristics of LUAD diver gene and its relationship with clinicopathological features in older LUAD.
Materials and methods: A total of 275 patients were diagnosed as LUAD and were over sixty years old. We utilized next-generation sequencing technology to detect and analyze gene mutations in postoperative tissue specimens, including EGFR, KRAS, ALK, ROS1, RET, MET, BRAF, HER2, PIK3CA and NRAS.
Results: A total of 90.18% (248/275) of older LUAD patients experienced genetic mutations. The EGFR (192, 69.82%) had the highest mutation rate among ten genes, followed by KRAS (21, 7.64%), MET (21, 7.64%), ERBB2 (15, 5.45%), RET (9, 3.27%), ALK (8, 2.91%), ROS1 (8, 2.91%), PIK3CA (6, 2.18%), BRAF (5, 1.82%) and NRAS (1, 0.36%). We also found thirty patients (15.63%) with EGFR mutations also having other gene mutations. The L858R mutation and exon19 deletion were the predominant EGFR mutations, accounting for 84.90% of EGFR-mutated patients. In addition, fifty-one kinds of EGFR mutations were detected, distributed in the protein tyrosine kinase catalytic domain (43, 84.31%), cysteine enriched domain (4, 7.84%), receptor binding domain (3, 5.88%), and EGFR transmembrane domain (1,1.96%). Ten cases of gene fusion mutation were detected. Two rare partner genes, PKHD1 (P60:R34) and STK39 (R33:S11), were detected by ROS1 gene fusion. RET gene fusion revealed a rare companion gene KCND2 (R11:K2). The EGFR mutations were more prevalent in female, non-smoking patients (p < 0.05), and the KRAS mutations were more common in male and smoking patients (p < 0.01). In addition, the BRAF mutations were more likely to occur in the right lung (p < 0.05).
Conclusion: Older LUAD populations exhibit diverse genetic mutations, which may also exist simultaneously. Simultaneous detection of multiple genes by NGS can accelerate and enhance targeted treatment benefits for older LUAD patients, ultimately improving their quality of life.
Lung adenocarcinoma (LUAD) is the most common pathological subtype in NSCLC, accounting for approximately 55% (1). Half of the LUAD patients are over 60 years old at the time of diagnosis, while a further 30% are over 70 years old, which are defined as older population (2). The older LUAD patients usually do not tolerate surgery. These patients are prone to heart disease, diabetes, or other primary diseases (3, 4). Therefore, choosing treatment methods with low toxicity, low side effects, and good tolerance in older LUAD patients is a critical clinical concern. With the development of precise diagnosis and treatment, more and more evidence suggests that targeted therapy guided by gene mutations has greatly improved treatment choices and survival benefits for NSCLC patients, including older LUAD patients (5–7). However, LUAD driver gene mutation vary from region to region, patient to patient, lifestyle to lifestyle, and test methodologies (8–10). This study retrospectively analyzed ten LUAD-related driving genes in 275 older LUAD patients and explored their correlation with clinicopathological indicators such as gender, smoking status, tumor location, maximum diameter, lymph node metastasis and others.
In this retrospective study, the clinical data of the patients were collected from the sample database of thoracic surgery (Supplementary Table S1). Inclusive criteria: 1) Imaging confirmed measurable lesions; 2) Patients with cytological or pathological diagnosis of LUAD in our hospital or other hospitals; 3) Preoperative radiotherapy and chemotherapy were not performed; 4) Medical records were comprehensive and fully documented; 5) Patients should be over 60 years of age. Patients were excluded based on the following criteria: 1) Cytological or pathological diagnosis was not clear; 2) Patients with malignant tumors on other organs; 3) Patients with severe liver and kidney dysfunction; 4) Without genetic test results or incomplete case data.
Specimens for gene mutation detection were obtained from formalin-fixed paraffin-embedded (FFPE) tissues after cytoreductive surgery. Tumor purity was determined by hematoxylin and eosin staining. The proportion of tumor cells in the sample should be at least 40%. The nucleic acid was extracted using the QIAamp DNA FFPE Tissue Kit following instructions provided by Qiagen in Dusseldorf, Germany. DNA concentration was measured by Qubit 3.0 (Thermo Fisher Scientific, Waltham, USA). We evaluated the distribution of nucleic acid fragment sizes using Qsep100 (Bioptic, Taiwan, China).
Library construction and sequencing experiments were entrusted to Dian Diagnostics Group Co., Ltd. The initial amount needed to build a library was 200 ng DNA. We used Agencourt AMPure XP beads from Beckman Coulter in the United States to purify the DNA library. The Qubit 1×dsDNA Assay Kit (Thermo Fisher Scientific, Waltham, USA) was utilized to quantify the purified next-generation sequencing (NGS) library. Qsep100 (Bioptic, Taiwan, China) was used to analyze fragment size distribution. A panel of ten LUAD-related genes was used to determine the presence of single nucleotide variants, insertions, deletions, duplications, fusions, and delins mutations. LUAD-related genes include EGFR, KRAS, ALK, ROS1, RET, MET, BRAF, HER2, PIK3CA and NRAS. All experiments were conducted in a clinical laboratory improvement amendments-certified laboratory to ensure the genetic test’s quality.
Illumina Nextseq 500 (Illumina, San Diego, USA) was used for library sequencing. The average sequencing depth was at least 1000X. The detection sensitivity of genetic variation was 1%. The FASTQ library’s paired-end sequencing data undergoes mapping to the human genome (hg19) through the Burrows-Wheeler Comparator (BWA-MEM) technology. The coverage depth of fusion breakpoints and adjacent sites were calculated by searching the possible fusion detection points. Somatic SNV was detected by muTect and somatic InDel by Strelka. Functional annotation of all the genetic variants was completed by ANNOVAR 21.
For all analyses, we used R version 4.1.1 (2021–08–10). Continuous variables are usually reported as mean and standard deviations or median and interquartile ranges. The appropriate analytical tools for inter-group comparisons include the Student t-test or the Mann Whitney U-test. Subgroup analyses were evaluated using chi-square analysis, while Fisher’s exact test was used for small sample sizes. Kendall’s ratio was used for correlation analyses. The tests were two-sided, and significance was determined based on a criterion standard of P ≤ 0.05.
This study enrolled a cohort of 275 older LUAD patients, ranging in age from 61 to 88 years old, with a median age of 68 years old (Supplementary Table S1). There were 141 males and 134 females, with a male to female ratio of 1:1.05 and no sexual orientation. More than two-thirds of patients had no smoking history (199/275, 72.36%), and more than half of smokers had quit smoking (38/65, 58.46%). The incidence rate of the upper lobe was 1.89 times higher than that of the lower lobe (upper lobe 151 vs. lower lobe 80). Right lung incidence was 1.20 times higher than left lung incidence (right lung 148 vs. left lung 123). After imaging examination, multiple measurable lesions were found in 44 (16%) patients. Half of older LUAD patients were in Stage I. About one-fifth of patients experience lymph node metastasis. In addition, about one-fifth of patients experience involvement in pleural, mediastinal, bone, brain, and other metastases (Table 1).
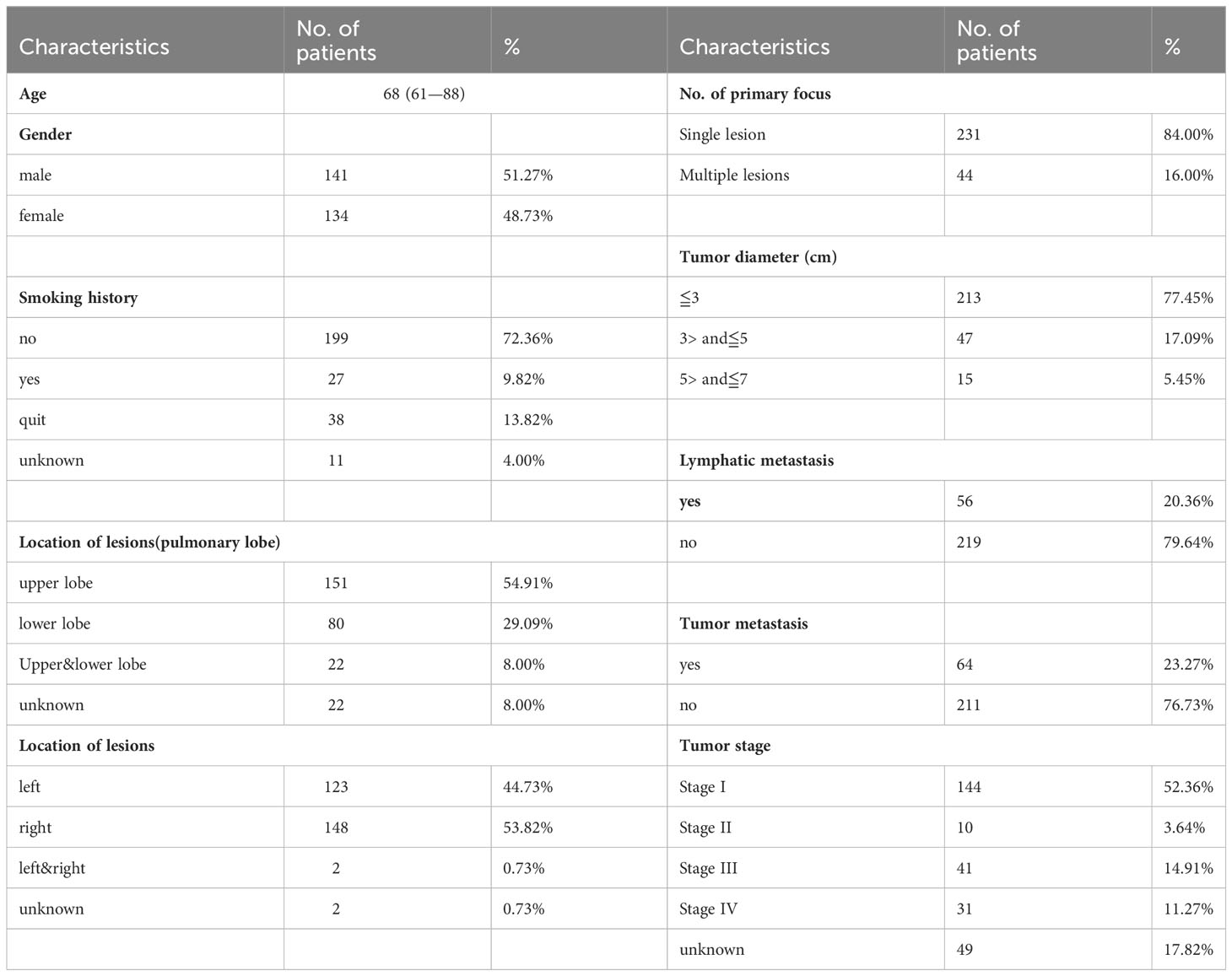
Table 1 Demographic and clinical characteristics of 275 patients with LUAD.
In this study, the prevalence of genetic mutations in older LUAD patients was as high as 90.18% (248/275), whereas only a small minority of samples tested negative for mutations (27/275, 9.82%) (Supplementary Table S2). Among older LUAD patients with genetic mutations, 2 (2/248, 0.81%) patients had three driver gene mutations simultaneously, and 33 (33/248, 13.31%) had two co-gene mutations. Two hundred and thirteen (213/248, 85.98%) patients with only one driver gene mutation. It should be noted that a subset of patients (n = 22) exhibited only one driver gene mutation, but multiple mutation sites were present. For example, one patient displayed L858R, 19del, and S768I mutations in the EGFR gene. The results of the multi-gene analysis show that EGFR (192, 69.82%) had the highest mutation rate among ten genes, followed by KRAS (21, 7.64%), MET (21, 7.64%), ERBB2 (15, 5.45%), RET (9, 3.27%), ALK (8, 2.91%), ROS1 (8, 2.91%), PIK3CA (6, 2.18%), BRAF (5, 1.82%) and NRAS (1, 0.36%) (Figure 1).
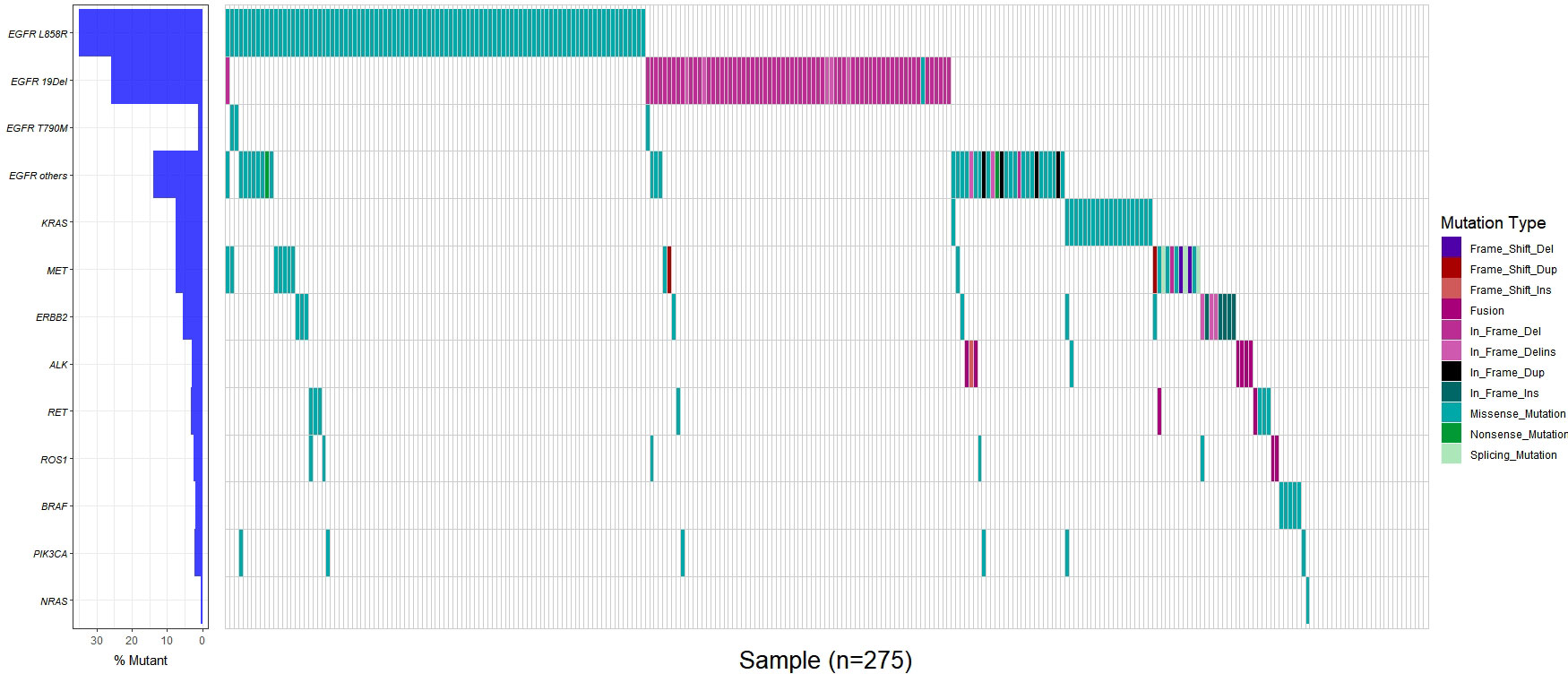
Figure 1 Genetic mutation in 275 geriatric LUAD patients.
Among 192 patients with EGFR mutations, 88.54% (170/192) patients had only single-site mutations. 10.94% (21/192) of patients had two mutations at the same time. Only one patient had three mutations in unison. The L858R mutation was identified in 50.00% of patients exhibiting EGFR mutations, while exon19 deletion was observed in 35.42% of patients with EGFR mutations. The two primary mutations found in EGFR were L858R and exon19 deletion, which account for 84.90% of patients with EGFR mutations. Rare EGFR mutations were found in 5 cases of G719X, 2 cases of S768I, and 3 cases of L861R. Three cases of classical drug resistance mutation T790M were detected. The average allele mutation frequency of EGFR L858R or 19del carried by patients with T709M mutation (average allele frequency: 38.95%) was nearly twice that of patients without T790M mutation (average allele frequency: 19.56%). Fifty-one kinds of EGFR mutations were found, distributed in the protein tyrosine kinase catalytic domain (43, 84.31%), cysteine enriched domain (4, 7.84%), receptor binding domain (3, 5.88%), and EGFR transmembrane domain (1, 1.96%) (Figure 2). Thirty patients with EGFR mutations also experienced other gene mutations. One patient developed both ROS1 and RET mutations, while the remaining patients had co-mutations with MET, RET, ERBB2, ROS1, KRAS, ALK, and PIK3CA, respectively (Table 2).

Figure 2 Distribution of mutations in EGFR functional domains.
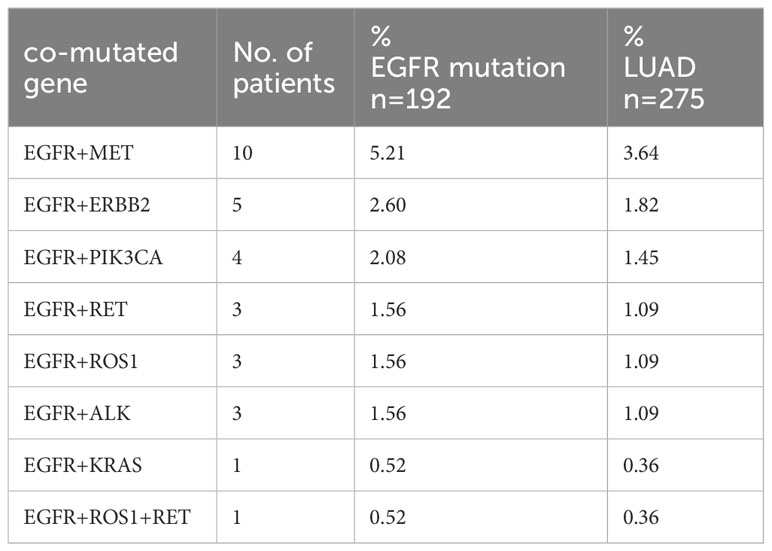
Table 2 EGFR genes incorporated mutations with other genes.
In addition, the fusion mutations were detected in 10 patients, including 5 cases of ALK fusion with two partner genes, EML4 and DCTN1 (Supplementary Table S3). In one case of DCTN1/ALK, the fusion type was D24:A20. In three cases of ROS1 fusion, the fusion partner genes were PKHD1 (P60:R34), EZR (E10:R34) and STK39 (R33:S11), respectively. Two fusion cases involving RET were identified: KIF5B/RET (K15:R12) and RET/KCND2 (R11: K2).
In older LUAD patients, female patients were more prone to genetic mutations than male patients (p = 0.0218). This feature was more pronounced in patients with EGFR mutations (p = 0.0040), though the potential significance were still unexplored (Table 3). No significant differences were observed among groups of older LUAD patients with different smoking histories regarding the occurrence of genetic mutations (p = 0.0965). However, the EGFR mutations were more likely to occur in patients without a history of smoking (p = 0.0024). No significant differences were observed in gene mutations or EGFR mutations based on lesion location, number of lesions, tumor size, lymph node metastasis, lesion metastasis and clinical stage. Kendall correlation significance test results showed that EGFR mutations were mutually exclusive with mutations in MET, KRAS, ALK, ERBB2 and BRAF (Figure 3). In the correlation analysis, we discovered a noteworthy inverse correlation between EGFR mutation and smoking, as well as a significant positive correlation with gender (p < 0.01). It also mean that the EGFR mutations were more likely to occur in female and non-smoking patients. The KRAS mutation population distribution was opposite to EGFR mutation, which was significantly positively correlated with smoking (p < 0.01) and negatively associated with gender (p < 0.05). BRAF mutations were more likely to occur in the right lung (p < 0.05). In addition, the occurrence of metastasis in the primary lesion was positively correlated with tumor diameter (p < 0.05) and lymph node metastasis (p < 0.01).
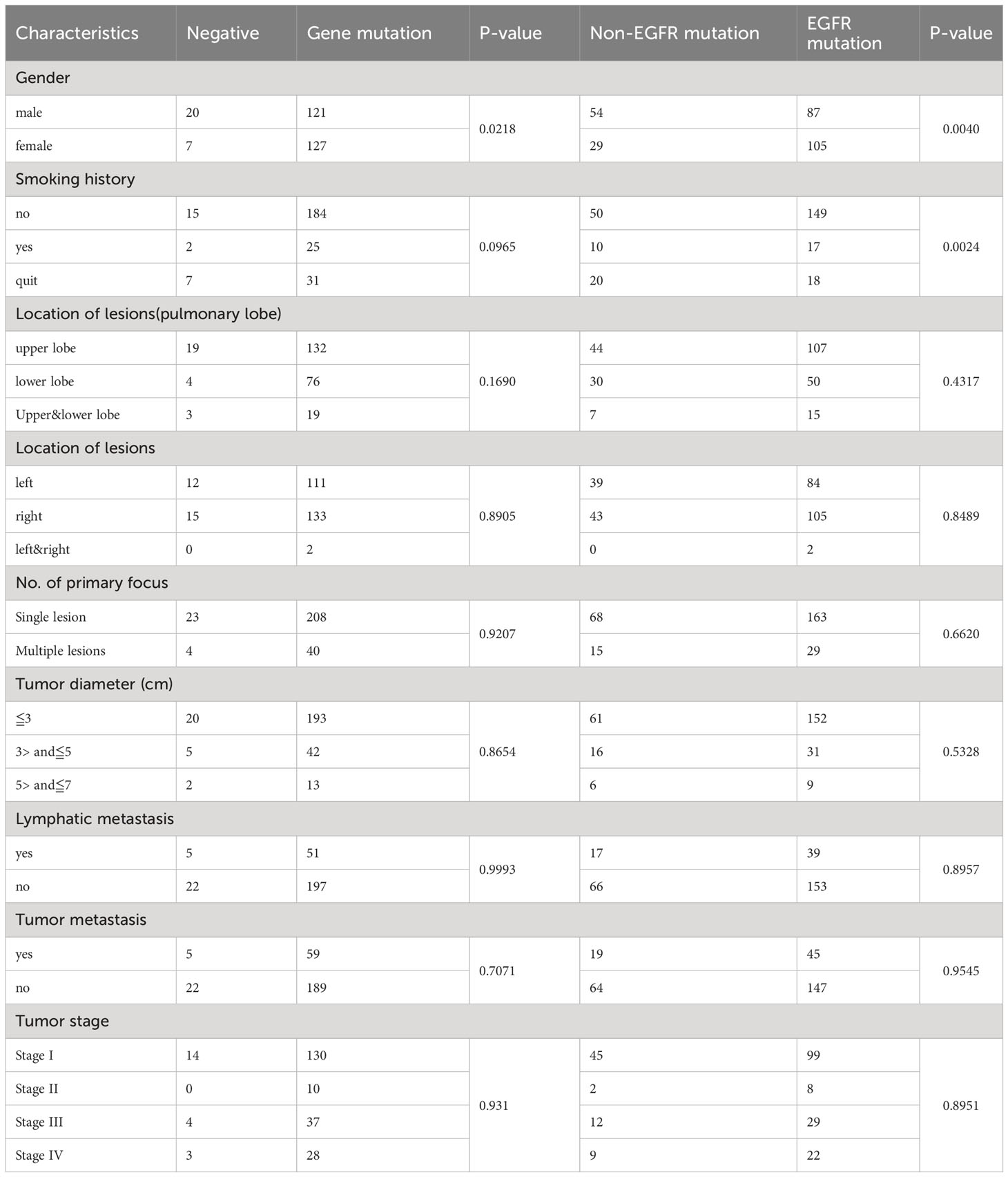
Table 3 Comparison of gene mutations among different clinical indicator groups.

Figure 3 Kendall correlation analysis between gene mutations and clinical features. Test of significance of the Kendall correlation coefficient: “*”, “**”, and “***” represent p < 0.05, p < 0.01, and p < 0.001, respectively.
The LUAD is the most common newly diagnosed malignant tumor in the older people (11, 12). As people age, older LUAD patients confront the dual challenge of declining organ function and heightened vulnerability to adverse treatment reactions (13). Previous clinical trials have found that the response rate to chemotherapy in older lung adenocarcinoma patients is only 9.9%-22.7% (14, 15). The response rate to gefitinib in LUAD patients with favorable EGFR mutations is approximately 70% (16, 17). Targeted therapies, which is guided by gene mutations, have significantly improved treatment choices and survival benefits in LUAD patients. In addition to common EGFR activation mutations, targets such as ALK rearrangement, ROS1 rearrangement, RET rearrangement, BRAF V600E, MET exon 14 skip mutation, KRAS G12C, etc. have been gradually approved for targeted drug application in advanced non-small cell lung cancer (6, 18). However, Sabine Schmid, et al. (2) conducted a retrospective comparative analysis of the treatment benefits of older and young patients with advanced lung cancer over the past decade. The results showed that over the past ten years, compared to the significant improvement in 12-month cancer-specific survival for younger patients, there was only a slight improvement in older patients. While EGFR or ALK tyrosine kinase inhibitors (TKIs) therapy is typically more effective and well-tolerated than chemotherapy, the rate of genetic testing and subsequent targeted treatment among older patients remains relatively low. This may lead to a reduction in cancer-specific and overall survival rates in older patients. Our study retrospectively analyzed molecular detection results in 275 patients with lung adenocarcinoma over 60 years of age. The mutation frequency of EGFR gene in older LUAD patients was remarkably high at 69.82%. Key drug targets EGFR L858R and 19DEL accounted for 84.90% of EGFR mutation patients. This indicates that more than four-fifths of patients may benefit from EGFR TKIs. Three patients carried EGFR T790M mutation and twenty-one patients developed KRAS mutation, providing reference information for drug selection. Five patients developed ALK fusion, including a rare fusion type DCTN1/ALK (D24: A20). Gao Fangfang, et al. (19) have reported that one case of DCTN1/ALK achieved partial response after receiving cabozantinib therapy. ERBB2, RET, ROS1, PIK3CA, BRAF, and NRAS were detected in older LUAD patients. NGS-based multi-gene joint detection can provide more sensitive and comprehensive reference information for drug selection.
Molecular characteristics of LUAD are influenced by environmental factors, familial factor, and lifestyle factors (20, 21). Some studies emphasize that environmental factors such as age and smoking are closely related to the molecular characteristics of lung adenocarcinoma (22). Our analysis revealed a significant association between gene mutations and clinicopathological factors such as gender, smoking, and location of lesions. EGFR mutations were more likely to occur in female and non-smoking patients. Nevertheless, KRAS mutations were likely to occur in the male patient population (p < 0.01) and smokers (p < 0.01). BRAF mutations were more likely to occur in the right lung (p < 0.05).
There are several limitations to this study. This study was limited by the limited capacity of targeted sequencing panels, which may not reveal all mutations in older LUAD patients. Whole exome sequencing is a recommended methods for the comprehensive understanding of gene alterations. Furthermore, the study does not provide follow-up information on older LUAD patients. Therefore, we cannot analyze the correlation between molecular mutation characteristics and prognosis.
In conclusion, different molecular variations drive the occurrence and development of older LUAD patients. NGS can effectively expand our understanding about gene mutations and enable an integrated analysis of multiple gene mutations in older patients with LUAD, providing crucial evidence for targeted treatment.
The datasets generated and/or analyzed during the current study are available in the CNGB Nucleotide Sequence Archive (CNSA, https://db.cngb.org/cnsa/) repository with accession CNP0004388.
The datasets presented in this study can be found in the CNGB Nucleotide Sequence Archive (CNSA, https://db.cngb.org/cnsa/) repository with accession number CNP0004388 and can be found in the article/Supplementary Material.
The studies involving humans were approved by Medical Ethics Committee of the Affiliated Hospital of the Shandong University of Chinese Medicine (Ethical No. KY2023-081). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because our institutional review board waived Informed consent because of the retrospective nature of our study.
XL: Conceptualization, Project administration, Writing – original draft, Writing – review & editing. GJ: Data curation, Writing – review & editing. XS: Data curation, Writing – review & editing. GS: Data curation, Writing – review & editing. XZ: Formal Analysis, Methodology, Writing – review & editing. DS: Methodology, Writing – review & editing. NY: Conceptualization, Software, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by Shandong Traditional Chinese Medicine Technology Project of Shandong Province (Grant No. Q-2022067).
The authors would like to thank all members of Affiliated Hospital of Shandong University of Traditional Chinese Medicine for their assistance in managing case information. At the same time, the authors would like to thank Jia Jia of Jinan Dean Medical Laboratory Center Co., Ltd. for coordinating the sequencing data. We thank the editor and reviewers for their helpful feedback that improved this paper.
Author NY, XZ and DS was employed by Dian Diagnostics Group Co., Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1275575/full#supplementary-material
1. Chang Y-S, Tu S-J, Chen Y-C, Liu T-Y, Lee Y-T, Yen J-C, et al. Mutation profile of non-small cell lung cancer revealed by next generation sequencing. Respir Res (2021) 22(1):3. doi: 10.1186/s12931-020-01608-5
2. Schmid S, Suipyte J, Herrmann C, Mousavi M, Hitz F, Früh M. Does progress achieved in the treatment of patients with metastatic non-small-cell lung cancer reach the older population? A cohort study from a cancer centre from Eastern Switzerland. Eur J Cancer Care (2020) 29(2):e13206. doi: 10.1111/ecc.13206
3. Wang S, Liang Q, Chi Y, Zhuo M, An T, Duan J, et al. Retrospective analysis of the effectiveness and tolerability of nab-paclitaxel in Chinese older patients with advanced non-small-cell lung carcinoma. Thorac cancer (2020) 11(5):1149–59. doi: 10.1111/1759-7714.13356
4. Daste A, Chakiba C, Domblides C, Gross-Goupil M, Quivy A, Ravaud A, et al. Targeted therapy and older people: A review. Eur J Cancer (Oxford Engl 1990). (2016) 69:199–215. doi: 10.1016/j.ejca.2016.10.005
5. Gridelli C, Rossi A, Carbone D, Guarize J, Karachaliou N, Mok T, et al. Non-small-cell lung cancer. Nat Rev Dis primers (2015) 1:15009. doi: 10.1038/nrdp.2015.9
6. Ettinger D, Wood D, Aisner D, Akerley W, Bauman J, Bharat A, et al. Non-small cell lung cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Network JNCCN (2022) 20(5):497–530. doi: 10.6004/jnccn.2022.0025
7. Skoulidis F, Heymach JV. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat Rev Cancer (2019) 19(9):495–509. doi: 10.1038/s41568-019-0179-8
8. Chen J, Yang H, Teo A, Amer L, Sherbaf F, Tan C, et al. Genomic landscape of lung adenocarcinoma in East Asians. Nat Genet (2020) 52(2):177–86. doi: 10.1038/s41588-019-0569-6
9. Shi H, Seegobin K, Heng F, Zhou K, Chen R, Qin H, et al. Genomic landscape of lung adenocarcinomas in different races. Front Oncol (2022) 12:946625. doi: 10.3389/fonc.2022.946625
10. Arauz R, Byun J, Tandon M, Sinha S, Kuhn S, Taylor S, et al. Whole-exome profiling of NSCLC among african americans. J Thorac Oncol (2020) 15(12):1880–92. doi: 10.1016/j.jtho.2020.08.029
11. Qiu H, Cao S, Xu R. Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020. Cancer Commun (London England) (2021) 41(10):1037–48. doi: 10.1002/cac2.12197
12. Subramanian J, Madadi A, Dandona M, Williams K, Morgensztern D, Govindan R. Review of ongoing clinical trials in non-small cell lung cancer: a status report for 2009 from the ClinicalTrials.gov website. J Thorac Oncol (2010) 5(8):1116–9. doi: 10.1097/JTO.0b013e3181e76159
13. Takayuki N, Keiko T, Junji U, Yoshiko K, Nobuyo T, Tadaaki Y, et al. Advanced non-small-cell lung cancer in older patients: patient features and therapeutic management. BioMed Res Int (2018) 2018:8202971. doi: 10.1155/2018/8202971
14. Uruga H, Kishi K, Fujii T, Beika Y, Enomoto T, Takaya H, et al. Efficacy of gefitinib for older patients with advanced non-small cell lung cancer harboring epidermal growth factor receptor gene mutations: a retrospective analysis. Internal Med (Tokyo Japan) (2010) 49(2):103–7. doi: 10.2169/internalmedicine.49.2531
15. Kudoh S, Takeda K, Nakagawa K, Takada M, Katakami N, Matsui K, et al. Phase III study of docetaxel compared with vinorelbine in older patients with advanced non-small-cell lung cancer: results of the West Japan Thoracic Oncology Group Trial (WJTOG 9904). J Clin Oncol (2006) 24(22):3657–63. doi: 10.1200/jco.2006.06.1044
16. Tamura K, Okamoto I, Kashii T, Negoro S, Hirashima T, Kudoh S, et al. Multicentre prospective phase II trial of gefitinib for advanced non-small cell lung cancer with epidermal growth factor receptor mutations: results of the West Japan Thoracic Oncology Group trial (WJTOG0403). Br J cancer (2008) 98(5):907–14. doi: 10.1038/sj.bjc.6604249
17. Asahina H, Yamazaki K, Kinoshita I, Sukoh N, Harada M, Yokouchi H, et al. A phase II trial of gefitinib as first-line therapy for advanced non-small cell lung cancer with epidermal growth factor receptor mutations. Br J cancer (2006) 95(8):998–1004. doi: 10.1038/sj.bjc.6603393
18. Planchard D, Popat S, Kerr K, Novello S, Smit E, Faivre-Finn C, et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29:iv192–237. doi: 10.1093/annonc/mdy275
19. Gao F, Gao F, Wu H, Lu J, Xu Y, Zhao Y. Response to ALK-TKIs in a lung adenocarcinoma patient harboring dual DCTN1-ALK and ALK-CLIP4 rearrangements. Thorac cancer (2022) 13(7):1088–90. doi: 10.1111/1759-7714.14345
20. Molina J, Yang P, Cassivi S, Schild S, Adjei A. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clinic Proc (2008) 83(5):584–94. doi: 10.4065/83.5.584
21. Sacher A, Dahlberg S, Heng J, Mach S, Jänne P, Oxnard G. Association between younger age and targetable genomic alterations and prognosis in non-small-cell lung cancer. JAMA Oncol (2016) 2(3):313–20. doi: 10.1001/jamaoncol.2015.4482
22. Vineis P, Airoldi L, Veglia F, Olgiati L, Pastorelli R, Autrup H, et al. Environmental tobacco smoke and risk of respiratory cancer and chronic obstructive pulmonary disease in former smokers and never smokers in the EPIC prospective study. BMJ (Clinical Res ed). (2005) 330(7486):277. doi: 10.1136/bmj.38327.648472.82
Keywords: lung adenocarcinoma, geriatric patients, gene mutation, clinicopathological features, next-generation sequencing
Citation: Liu X, Jiang G, Sun X, Su G, Zhang X, Shen D and Yan N (2023) Relationship between driver gene mutations and clinical pathological characteristics in older lung adenocarcinoma. Front. Oncol. 13:1275575. doi: 10.3389/fonc.2023.1275575
Received: 14 August 2023; Accepted: 19 October 2023;
Published: 01 November 2023.
Edited by:
Paolo Graziano, IRCCS Casa Sollievo della Sofferenza Hospital, ItalyReviewed by:
Gianluca Tedaldi, Scientific Institute of Romagna for the Study and Treatment of Tumors (IRCCS), ItalyCopyright © 2023 Liu, Jiang, Sun, Su, Zhang, Shen and Yan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Na Yan, eWFubmFAZGF6ZC5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.