 Ya-Fei Hu
Ya-Fei Hu Hai-Jie Hu
Hai-Jie Hu Heng-Chung Kung
Heng-Chung Kung Tian-Run Lv1
Tian-Run Lv1 Jun Yu
Jun Yu Fu-Yu Li
Fu-Yu Li- 1Department of Biliary Surgery, West China Hospital of Sichuan University, Chengdu, Sichuan, China
- 2Krieger School of Arts and Sciences, Johns Hopkins University, Baltimore, MD, United States
- 3Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States
- 4Department of Oncology, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Objective: The efficacy of platinum-based chemotherapy (PtCh) for pancreatic cancer (PC) patients with DNA damage repair gene mutations (DDRm) compared to those without DDRm remains uncertain.
Methods: After a thorough database searching in PubMed, Embase, and Web of Science, a total of 19 studies that met all the inclusion criteria were identified. The primary outcomes were overall survival (OS) and progression-free survival (PFS) for PC patients with DDRm versus those without DDRm after PtCh.
Results: Patients with advanced-stage PC who have DDRm tend to have longer OS compared to patients without DDRm, regardless of their exposure to PtCh (HR=0.63; I2 = 66%). Further analyses indicated that the effectiveness of PtCh for OS was modified by DDRm (HR=0.48; I2 = 59%). After the first- line PtCh (1L-PtCh), the PFS of advanced-stage PC with DDRm was also significantly improved (HR=0.41; I2 = 0%). For patients with resected PC, regardless of their exposure to PtCh, the OS for patients with DDRm was comparable to those without DDRm (HR=0.82; I2 = 71%). Specifically, for patients with resected PC harboring DDRm who received PtCh (HR=0.85; I2 = 65%) and for those after non-PtCh (HR=0.87; I2 = 0%), the presence of DDRm did not show a significant association with longer OS.
Conclusion: 1L-PtCh treatment is correlated with favorable survival for advanced-stage PC patients with DDRm. For resected-stage PC harboring DDRm, adjuvant PtCh had limited effectiveness. The prognostic value of DDRm needs to be further verified by prospective randomized controlled trials.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42022302275.
1 Introduction
Pancreatic cancer (PC) displaying a 5-year overall survival (OS) rate of <10% is a leading cause of cancer-related death worldwide (1). The standard therapeutic approach for patients with resectable PC involves curative surgical resection followed by adjuvant chemotherapy. Despite advancements in multiagent chemotherapy that have improved prognosis for advanced-stage of PC (2, 3), the mOS for patients with unresectable PC remains <1 year. Therefore, currently, available chemotherapy agents for advanced-stage PC demonstrate modest and/or limited effectiveness (4). As a result, there is an urgent need to gain a comprehensive understanding of the actionable molecular pathology features of PC for driving the development of novel and effective therapeutic approaches (2–5).
Pathogenic gene mutations have emerged as crucial contributors to PC development. In addition to well-established driver gene alterations such as KRAS and TP53 (6), recent investigations have elucidated that a notable proportion of PC patients (approximately 12%–25%) harbor mutations in genes involved in DNA damage repair (DDR) (7–9). These specific mutations can lead to disruptions in DNA homologous recombination (HR), resulting in deficiency and subsequent promotion of oncogenic processes in PC. In select Western cohorts (7), a notable disparity has been observed in the OS between PC patients with DDR gene mutations (DDRm) and those without DDRm. While other studies have yielded contrasting results, certain investigations have indicated that PC patients with DDRm may exhibit comparable or even worse prognoses than those without DDRm (10, 11). The prognostic value of DDRm in PC needs more confirmation. Principe et al. (12) conducted a study exploring the potential benefits of platinum-based chemotherapy (PtCh) in patients with PC who have DDRm. Their findings suggested that such patients may experience improved outcomes when treated with PtCh. Other literature additionally reported an augmented risk of disease progression or mortality in patients with DDRm who were exposed to non-first-line PtCh treatments (13, 14). These findings support that advanced-stage PC patients with DDRm may be sensitive to certain agents such as PtCh. However, the treatment efficacy of PtCh in resected-stage PC patients with DDRm remains uncertain according to existing literature (15, 16). Shun Yu et al. (17) suggested that PtCh may provide survival benefits for resected PC patients with pathogenic germline BRCA/PALB2 mutations, whereas Blair et al. (18) reported worse survival outcomes in BRCA-mutated carriers compared to wild-type counterparts after PtCh treatment. These divergent results indicate that the implications of DDRm for different stages of PC may vary and need further confirmation (7, 19–21).
DDRm genes are not tested routinely worldwide; thus, previously published studies investigating DDRm in PC have predominantly utilized small sample sizes and included patients at various stages of the disease. Consequently, a notable degree of heterogeneity exists within these studies (12, 13, 15). To address this inherent heterogeneity and consolidate the available evidence, we conducted a systematic review of the published literature focused on comparing the prognosis of advanced and resected-stage PC patients with DDRm versus those without DDRm.
2 Materials and methods
We performed the meta-analyses according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (22). The study protocol was published on PROSPERO (number CRD42020146320). Two authors (YF Hu and HJ Hu) independently screened the titles and abstracts of studies to identify literature that met all inclusion criteria. A third reviewer (Fu-Yu Li) was consulted when any disagreements were met. The Newcastle–Ottawa Scale (23) was used for quality evaluation of cohort or case–control studies; studies were selected if they had a score above 5.
2.1 Search details
We searched relevant studies published in PubMed, Embase, and Web of Science after 2015. The search strategy used a combination of Medical Subject Heading terms (MESH terms) including pancreatic cancer, DNA damage repair, Platinum, and their related words. The following search strategy was used “((((((((((Pancreatic cancer[MeSH Terms]) OR (pancreatic Neoplasms[Text Word])) OR (pancreatic neoplasm*[Text Word])) OR (pancreatic neoplasm*[Text Word])) OR (pancreatic carcinoma[Text Word])) OR (pancreatic adenocarcinoma[Text Word])) AND (DNA damage repair[MeSH Terms])) OR (DNA damage response[Text Word])) AND (Platinum[MeSH Terms])) OR (PtCh[Text Word])”. Word variations have also been searched. The search strategy was adapted according to each database configuration.
2.2 Inclusion criteria
We only included studies of high quality and met all our inclusion criteria as follows:
1) Patients: confirmed PC malignancy of resected or advanced stage.
2) Interventions: PtCh vs. non-PtCh.
3) Comparators: PC with germline or somatic DDRm versus those without DDRm or wild type.
4) Primary outcomes: including OS or PFS.
5) Study type: comparative studies on humans and of English languages.
2.3 Exclusion criteria
Exclusion criteria included the following:
a) Patients with benign pancreatic diseases or unconfirmed PC.
b) Did not provide any survival outcomes.
c) Included fewer than three patients or a case report.
d) Designed as single-arm and/or only included patients with DDRm genes.
2.4 Data extraction and quality assessments
Two reviewers (Hu YF and Hu HJ) independently extracted the following information from the selected studies: author, publication year, study type, patient characteristics, PC stages, interventions, mutation types (germline/somatic), details, and primary conclusions (Table 1). The study quality was scaled by the NOS score measurement, and PFS/OS in DDRm vs. without DDRm groups after the first or second/later line of PtCh was also presented (Supplementary Material).
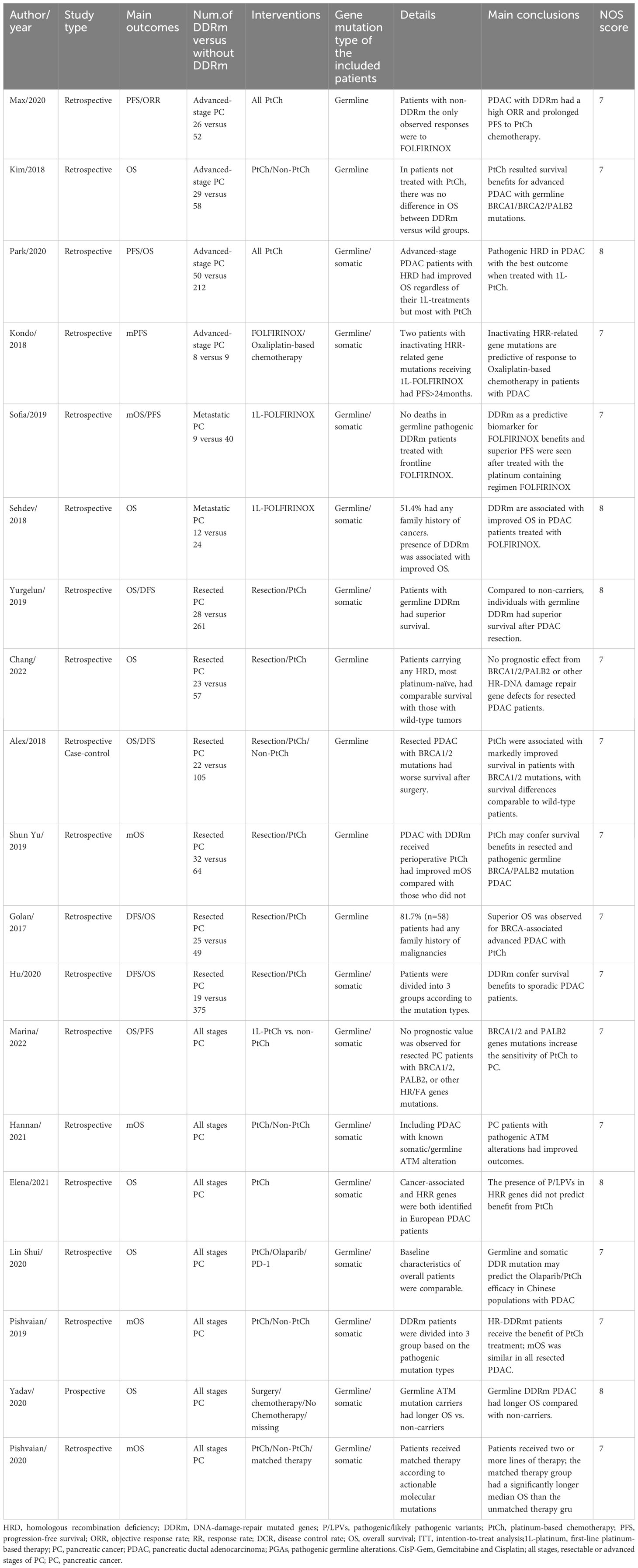
Table 1 Studies included in the systematic review.
2.5 Statistical methods
Our meta-analysis was performed with Review Manager (computer program) V.5.4 (Nordic Cochrane Center, Copenhagen) and Stata 14.0. Hazard ratio (HR) was presented as a risk ratio of compared groups with 95% certification interval (CI). The I2 test was used to confirm the homogeneity among the study results. When research results with low statistically significant heterogeneity (I2 ≤ 60%) were found, a fixed-effect model was used. Funnel-shaped graphs would be constructed if there were more than 10 studies in the analyses. Sensitivity analyses were performed on the results with multiple methods, including study exclusion.
3 Results
The flowchart of the study selection process is reported in Figure 1. After conducting a thorough databases searching including PubMed, Embase, and Web of Science, we identified a total of 8,779 relevant studies published after 2015. We eliminated 4,915 duplicate studies, leaving us with 3,864 studies for review. After screening abstract and titles, 3,558 studies were judged not relevant with reasons of non-English language literature, reviews, letters, or animal studies. After screening full texts of 306 studies, 287 studies that did not meet all the inclusion criteria were excluded. Consequently, a total of 19 studies that compared the effectiveness of PtCh for PC patients with DDRm versus those without DDRm were included in the meta-analyses (10, 11, 14, 16–20, 24–34).
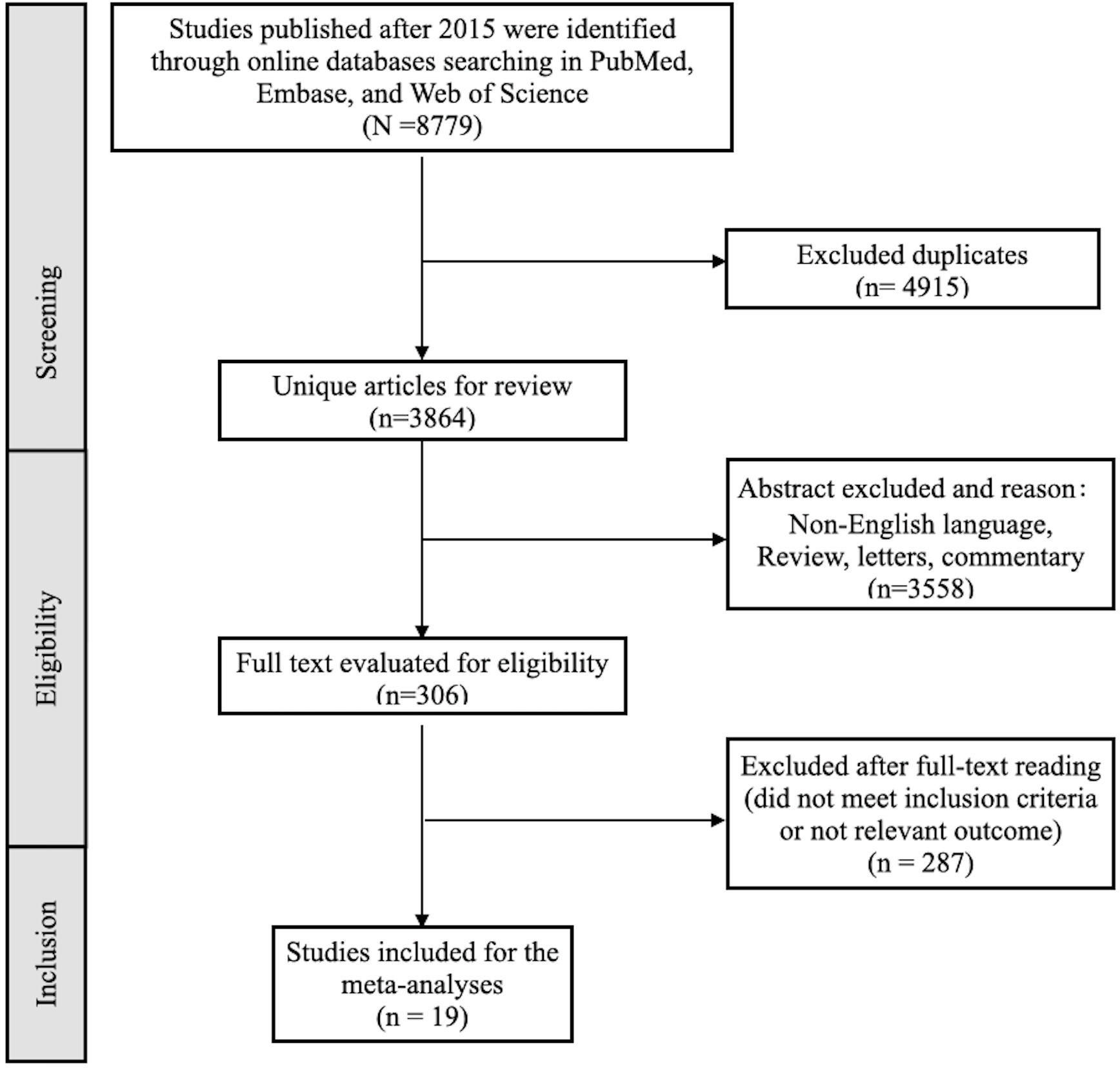
Figure 1 The flowchart of the study selection process.
The primary outcomes of the study focused on OS and PFS in patients with advanced/resected PC who had DDRm compared to those without DDRm. The secondary outcomes of the study were PFS for advanced-stage PC following various lines of PtCh and mOS improvement for advanced-stage PC who had mutated ATM/ATR genes compared to a control group with wild-type genes. The findings of our meta-analyses are presented in Table 2.
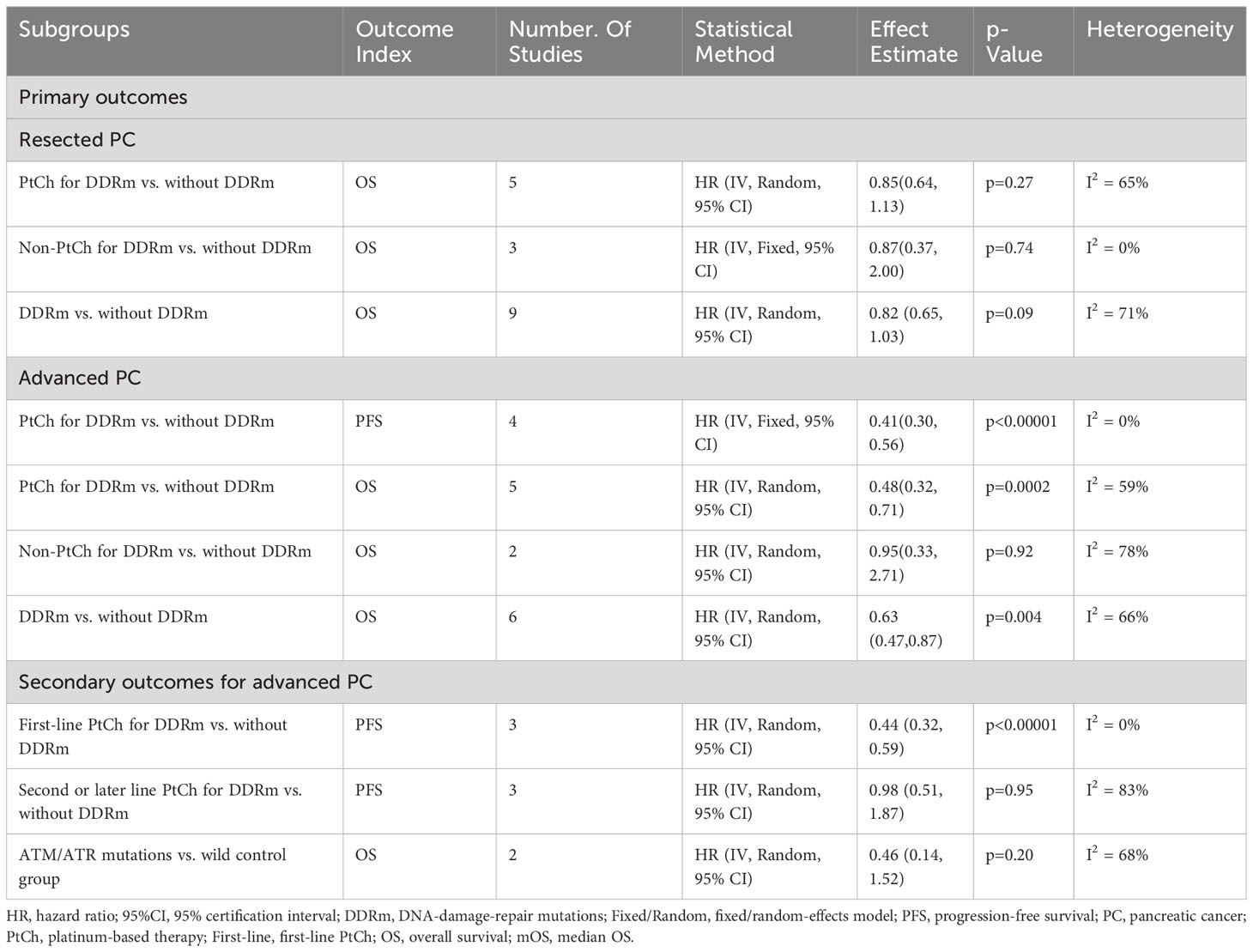
Table 2 Primary and Secondary outcomes of the meta-analyses.
3.1 Primary outcomes
3.1.1 Prognostic value of DDR
To evaluate the predictive role of DDRm on OS in patients with PC, we conducted an analysis of OS between patients with DDRm and those without DDRm, irrespective of the treatment approach employed (Figures 2A, B). For patients with advanced PC and DDRm, we observed a significantly longer OS in comparison to those without DDRm, with a hazard ratio (HR) of 0.63 (95% confidence interval [CI], 0.47–0.87; p=0.004) (Figure 2A). However, for resected stages of PC, the presence of DDRm genes did not demonstrate any significant OS benefits, with an HR of 0.82 (95% CI, 0.65–1.03; p=0.09) (Figure 2B). It is important to note that both the analyses conducted in advanced and resected PC patients exhibited notable heterogeneity, with I2 values of 66% and 71%, respectively, indicating substantial variability among the included studies.
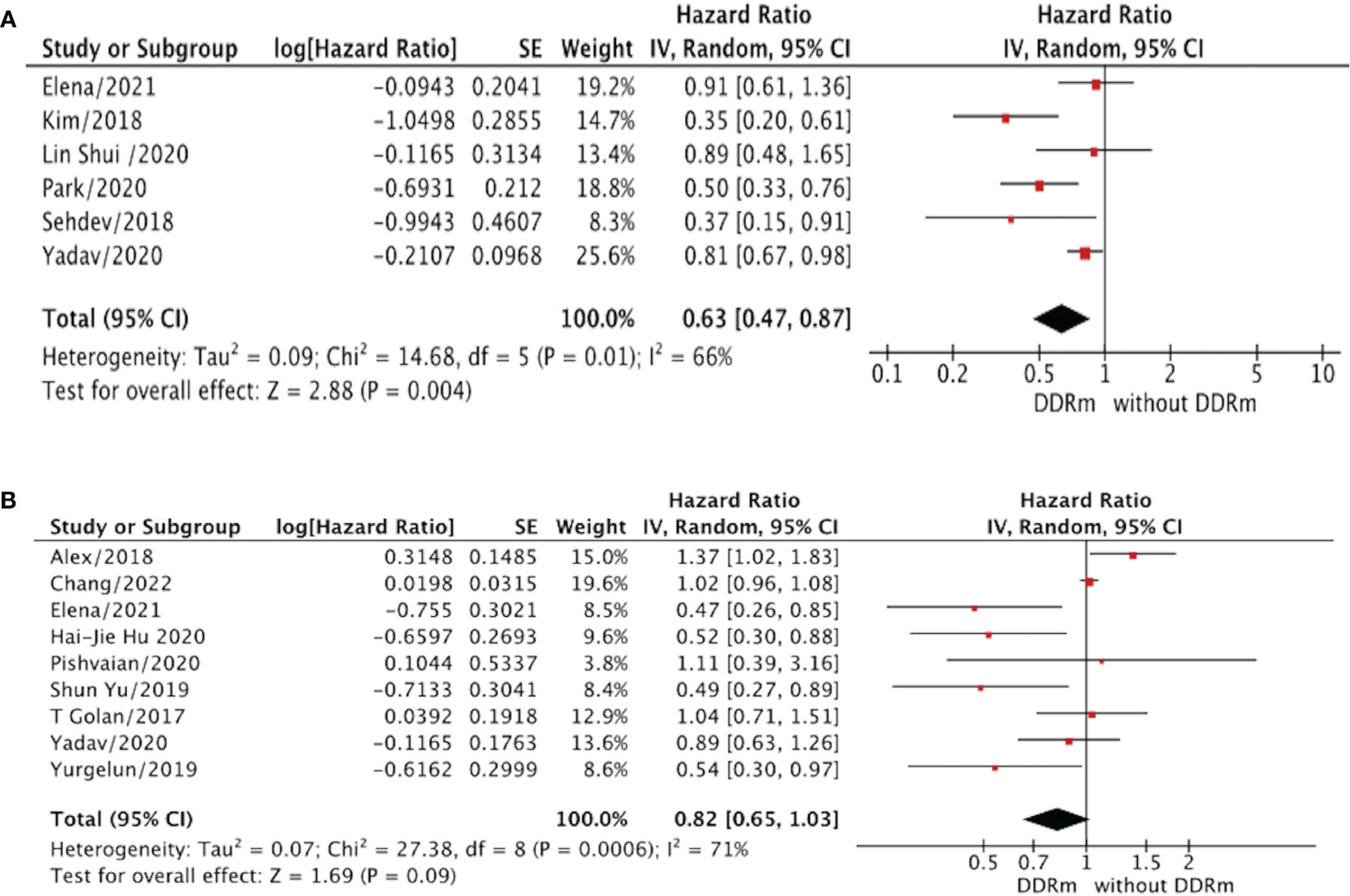
Figure 2 (A) The overall survival (OS) for advanced PC patients (DDRm vs. without DDRm). (B) The overall survival (OS) for resected PC patients (DDRm vs. without DDRm).
3.1.2 Therapeutic value of DDRm
To address the observed significant heterogeneity in our results, we conducted a subgroup analysis to evaluate the impact of DDRm in PC patients based on the type of chemotherapy received, specifically PtCh versus non-PtCh treatment. For this analysis, we included patients who received PtCh at any stage following the diagnosis of PC. We focused on the OS/PFS differences among the two treatment groups. The findings of this subgroup analysis are presented in Figures 3 and 4 of our manuscript.
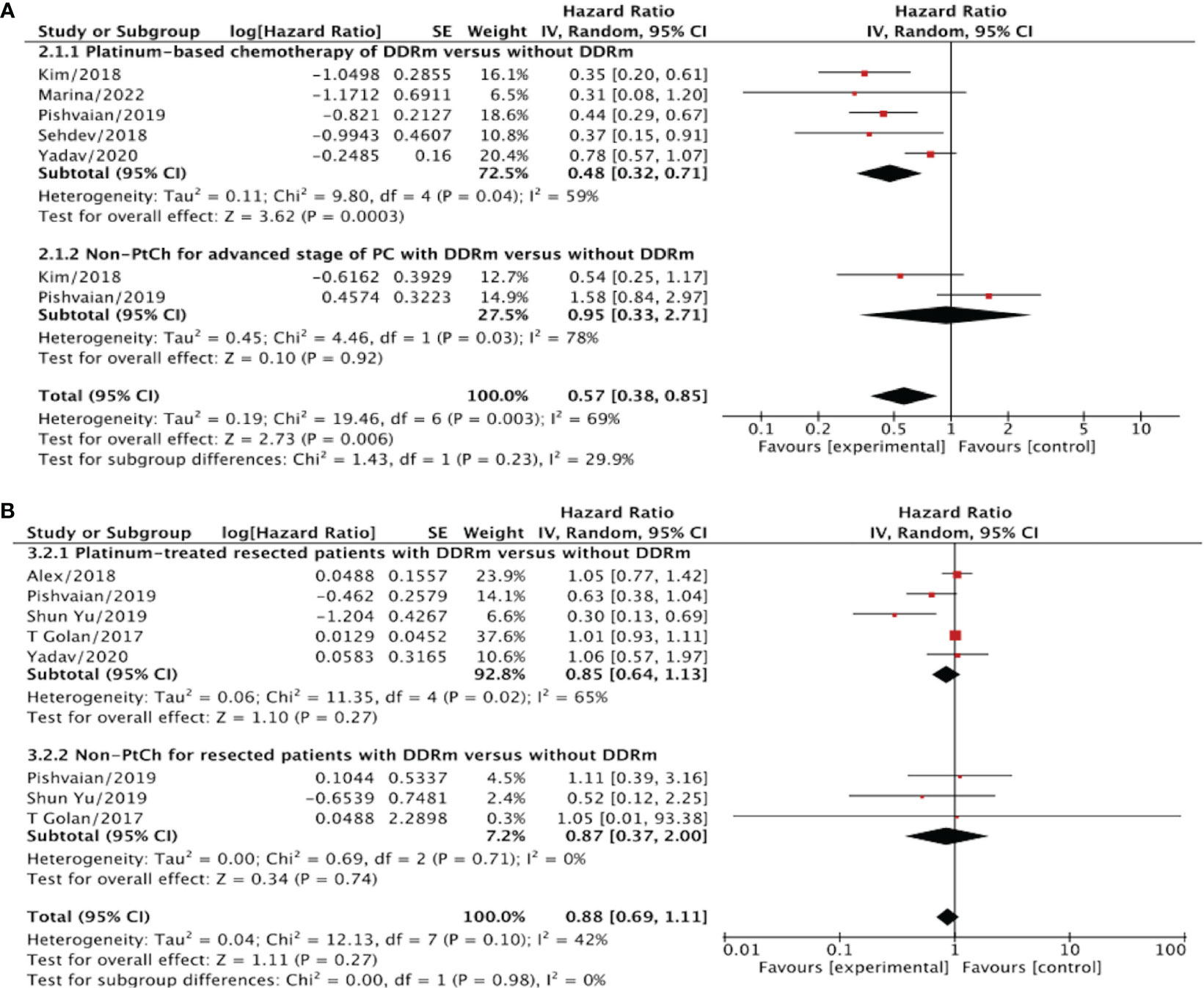
Figure 3 (A) The overall survival (OS) for advanced/metastatic PC patients without DDRm versus without DDRm after PtCh or non- PtCh. (B) The overall survival for early/resected PC patients with DDRm versus without DDRm after PtCh or non- PtCh.
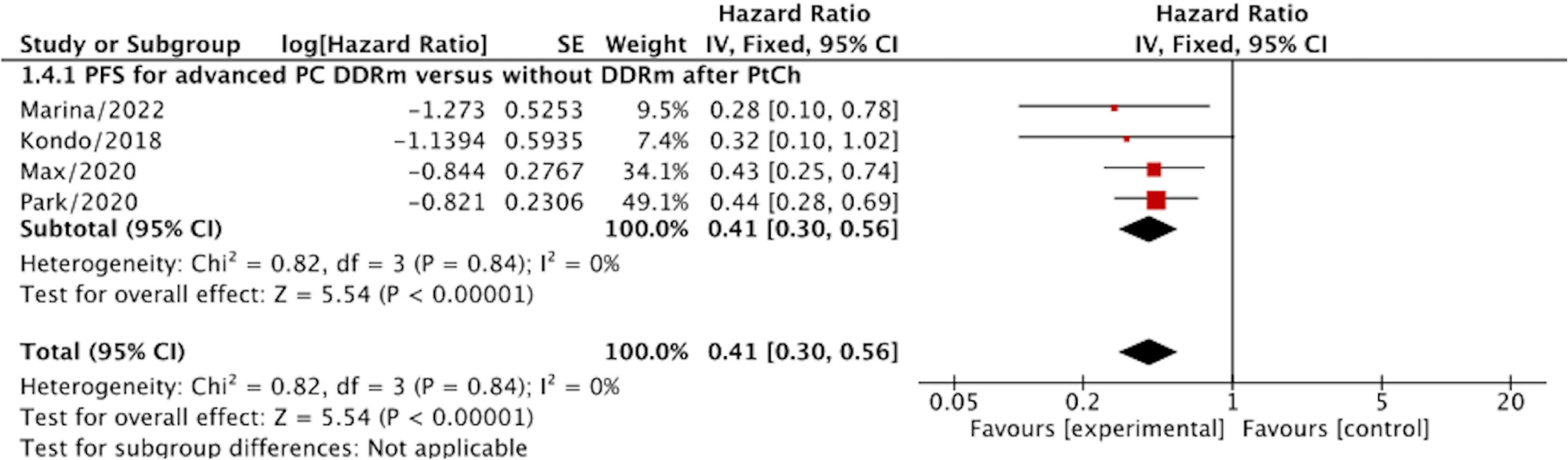
Figure 4 The progression-free survival (PFS) for advanced PC patients with DDRm versus without DDRm after PtCh.
3.1.3 OS for advanced/resected-stage PC patients after PtCh
Our analysis revealed that the presence of DDRm is associated with improved OS in advanced PC patients who received PtCh, with an HR of 0.48 (95% CI, 0.32–0.71; p=0.0003) compared to patients without DDRm (Figure 3A). However, in the case of resected PC patients with DDRm genes who received PtCh, the presence of DDRm did not show a significant association with longer OS, as the HR was 0.85 (95% CI, 0.64–1.13; p=0.27) (Figure 3B). It is worth noting that no significant heterogeneity was detected in these analyses, with I2 values of 59% and 65% for advanced and resected PC patients, respectively.
3.1.4 OS for advanced/resected-stage PC patients after non-PtCh
We evaluated survival outcomes in PC Patients with non-PtCh treatment to evaluate the prognostic value of DDRm. These patients were divided into resected and advanced stages (Figures 3A, B). Our analysis did not reveal any statistically significant differences in OS between patients with DDRm and those without DDRm in either the resected or advanced subgroups after non-PtCh treatment. Specifically, among patients with advanced PC and DDRm after non-PtCh treatment, the OS was comparable to patients without DDRm, with an HR of 0.95 (95% CI, 0.33–2.71; I2 = 78%; p=0.92) (Figure 3A). Similarly, for patients with resected PC and DDRm after non-PtCh, the pooled HR was 0.87 (95% CI, 0.37–2.00; p=0.74) (Figure 3B). Importantly, there was no heterogeneity detected in the comparison (I2 = 0%). Based on these results, it appears that the DDR status does not carry a definitive prognostic value for patients who did not undergo PtCh treatment.
3.1.5 PFS for advanced PC patients after PtCh
The value of DDRm for advanced PC after PtCh could also be demonstrated by an increased PFS with HR=0.41 (95% CI, 0.30–0.56; p<0.00001) compared to the without DDRm. The analyses were presented with no heterogeneity (I2 = 0%) (Figure 4).
3.2 Secondary outcomes
3.2.1 PFS for advanced PC patients after the first/later line of PtCh
For patients with advanced PC, the association between DDRm and PtCh had been demonstrated by an increased PFS, which was only significantly observed in the first-line PtCh setting with HR=0.44 (95% CI, 0.32–0.59; p<0.00001; I2 = 0%). No significant difference was observed for PC in DDRm versus without DDRm group after the second/later line of PtCh (HR=0.98; 95% CI, 0.51–1.87; p=0.95; I2 = 83%) (Supplementary Figure S1).
3.2.2 OS for advanced PC patients with ATM versus wild control groups
The further gene-level analysis demonstrated that germline/somatic ATM/ATR mutation carriers had comparable OS to patients without those mutations (HR=0.46; 95%CI, 0.14–1.52; p=0.20), with moderate heterogeneity (I2 = 68%) (Supplementary Figure S2).
4 Sensitivity analyses
4.1 OS for advanced-stage PC with DDRm vs. without DDRm regardless of adjuvant therapy methods
We excluded one study by Kim et al. for some patients in the cohort who did not receive any therapy. Patients with advanced tumors and harboring DDRm were found to be positively associated with a significantly longer OS after chemotherapy (HR=0.72; 95% CI, 0.55–0.94; p=0.01) with low heterogeneity in the results (I2 = 49%) (Supplementary Figure S3).
4.2 OS for resected PC with DDRm vs. without DDRm regardless of adjuvant therapy methods
We excluded the studies by Chang et al. and Alex et al., as the studies included patients who did not receive any adjuvant therapy. After analysis, we could find longer OS for resected PC patients with DDRm (HR=0.73; 95%CI, 0.61–0.88; p=0.001) with low heterogeneity in the results (I2 = 49%) (Supplementary Figure S4).
5 Discussion
The clinical significance of DDRm cannot be overstated. Extensive research has shown that platinum-containing chemotherapy regimens exhibit enhanced efficacy against breast and ovarian cancer cells harboring DDRm (35–39). In PC, approximately 20% of patients carry DDRm. However, the relevance of DDRm in PC remains a topic of debate. Conflicting findings have emerged from studies investigating the association between DDRm and survival outcomes in PC patients, with some reports suggesting improved survival in DDRm individuals while others indicate comparable or even worse prognoses. Consequently, further investigation is imperative to ascertain the impact of DDRm on PC patients’ survival. Moreover, the underlying reasons for the observed survival benefits, whether attributed to the inherent prognostic advantage of DDRm or the therapeutic value in terms of response to PtCh, remain unclear. To address these questions, we undertook an investigation into the association between DDRm and survival prognosis in PC.
In this study, patients were classified into two categories based on PC stage: resected versus advanced. Additionally, patients were categorized according to the type of chemotherapy received: PtCh versus non-PtCh. Furthermore, patients were evaluated based on their DDRm: DDRm versus without DDRm. Our study demonstrated a significant improvement in OS specifically among the subset of advanced DDRm PC patients following PtCh. However, it was observed that only first-line PtCh resulted in superior PFS outcomes for these patients. Consistent with our findings, previous studies (13, 14) have also reported survival benefits for advanced DDRm PC patients compared to patients without DDRm when treated with PtCh. Interestingly, there was even an indication of a potential trend towards poorer prognostic outcomes for advanced DDRm PC patients receiving non-PtCh, in comparison to PC patients without DDRm (32).
Patients with advanced PC and DDRm demonstrated longer survival when exposed to PtCh compared to advanced PC patients without DDRm. These findings suggest that DDRm may hold predictive value in determining the efficacy of PtCh therapy for advanced PC.
In our analysis, we also investigated the survival difference between patients DDRm and those without DDRm who were treated with non-PtCh. Interestingly, we found that the OS outcomes were comparable between DDRm and without DDRm patients, both in the advanced and early-stage PC. These results indicate that while DDRm may possess some predictive value in selecting patients for PtCh therapy in specific cases of PC, the pure prognostic value of DDRm appears to be limited and necessitates further validation and confirmation through additional research.
In our study, we observed that advanced PC patients DDRm who received first-line platinum-based chemotherapy (1L-PtCh) experienced significantly prolonged PFS. However, no improvements in PFS were observed in the second or later treatment settings of the platinum-based chemotherapy approach. This suggests that 1L-PtCh may be the optimal treatment choice for advanced DDRm PC patients.
A study by Park et al. (14). also supports our findings, demonstrating that patients with pathogenic homologous recombination deficiency (HRD) in pancreatic cancer exhibited improved outcomes only when treated with 1L-PtCh. These findings further emphasize the potential benefits of 1L-PtCh as a treatment strategy for advanced DDRm PC patients.
The implications of our findings also extend to future clinical trial design, highlighting the significance of early germline testing in patients diagnosed with advanced PC. Early identification of DDRm (DDRm) through germline testing can aid in identifying patients who may derive benefits from 1L-PtCh and optimize treatment strategies tailored to their specific genetic profile. These insights contribute to the ongoing efforts to enhance precision medicine approaches in the treatment of pancreatic cancer.
In our study, we also investigated the survival outcomes of resected DDRm PC patients after adjuvant chemotherapy. We observed limited survival advantages for selected patients after adjuvant chemotherapy. When comparing resected DDRm PC patients to those without DDRm, neither PtCh nor non PtCh was associated with longer OS. However, it is worth mentioning that Shun Yu et al. (17) reported that perioperative PtCh in PC patients with DDRm resulted in improved mOS compared to those who did not receive perioperative PtCh. This suggests that certain adjuvant chemotherapy regimens may confer benefits to resected DDRm PC patients. Nevertheless, our analysis did not demonstrate a significant effect of DDRm on OS in resected PC patients, as comparable survival outcomes were observed between DDRm and without DDRm groups treated with either PtCh or non-PtCh.
It is important to note that Golan et al. (24) also reported no survival differences between BRCA mutation carriers and sporadic tumors. These findings highlight the necessity for more prospective studies to confirm these observations and further investigate the potential impact of DDRm on the outcomes of resected PC patients.
In conclusion, additional research is warranted to better understand the role of DDRm in resected PC patients and to elucidate the significance of surgical-related factors such as surgical margin and nodal status in determining outcomes. Prospective studies will provide more comprehensive insights into the impact of DDRm on survival outcomes and help refine treatment strategies for patients with resected PC.
Gemcitabine/nab-paclitaxel and FOLFIRINOX are the two primary first-line regimens utilized for the treatment of advanced-stage PC. Previous studies have reported an mOS of approximately 8.5 months for PC patients treated with gemcitabine/nab-paclitaxel, compared to 14 months for those treated with FOLFIRINOX (11, 26, 29, 40, 41). More recently, a study involving a smaller cohort of PC patients with DDRm genes treated with FOLFIRINOX demonstrated an improved OS (11). Currently, there are no established predictive biomarkers to identify patients who would benefit more from FOLFIRINOX treatment. However, further studies comparing the effectiveness of gemcitabine/nab-paclitaxel versus FOLFIRINOX in PC patients with DDRm genes could potentially establish DDRm as a valuable predictive biomarker for guiding decisions regarding FOLFIRINOX treatment.
Molecular studies involving sporadic PC have identified a complex mutational profile, and multiple genes have been reported to be associated with HR deficiency, but the exact related genes are not clear (5, 39, 42, 43). Additionally, not all DDRm genes play a role in the prognosis of PC. In our study, we found limited prognostic impact of the HRD-related gene ATM in PC patients, and few studies have evaluated the role of other DDRm genes. As such, we lack sufficient data to compare the prognostic impact of different types of DDRm on PC patients and the sensitivity of PC patients carrying different DDRm to PtCh therapy (2, 13, 21).
Of note, our study had several important limitations. First, most of the included studies were retrospective, and selective bias was exciting. Furthermore, the samples of some studies were small, limiting the reliability of the conclusions. Second, the basic characteristics of the included patients do not completely match, which is inevitable in meta-analyses. Third, several rarer candidate DDR genes (e.g., ATR, ATRX, CHEK1, RAD51L1, and RAD51L3) were excluded from some of our included studies; therefore, some patients in the wild group may also have undetected DDRm genes, which may influence the outcomes. Finally, the targeted-sequencing approaches and the mutation status (somatic or germline) were also different. In conclusion, large-scale prospective randomized controlled studies are needed to confirm the benefits of PtCh treatment for PC patients with DDRm.
6 Conclusions
In our study, we observed an improved survival among patients with advanced PC who had DDRm after receiving PtCh. However, the effectiveness of PtCh on survival for resected DDRm PC patients was limited. Overall, our analysis did not demonstrate a significant prognostic effect of DDRm in PC patients. Nevertheless, our findings suggest that optimal therapy for advanced PC patients with DDRm may involve the use of a platinum-containing regimen. It is important to note that while appropriate chemotherapy for resected DDRm PC patients may result in a longer OS, surgery remains the only curative approach. These findings underscore the potential value of early germline testing in individuals diagnosed with PC, as it may provide insights into DDRm and guide treatment decisions. Moreover, given the limited data available, future studies should focus on assessing the variations in tumor biology and response to standard treatments among PC patients with different DDRm profiles.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
Y-FH: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. H-JH: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. H-CK: Conceptualization, Data curation, Investigation, Methodology, Software, Writing – original draft. T-RL: Conceptualization, Data curation, Investigation, Software, Writing – original draft. JY: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Resources, Software, Visualization, Writing – original draft. F-YL: Conceptualization, Funding acquisition, Investigation, Resources, Software, Visualization, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Supported by 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC21046); 1.3.5 project for disciplines of excellence Clinical Research Incubation Project, West China Hospital, Sichuan University (2021HXFH001); Natural Science Foundation of Sichuan Province (2022NSFSC0806); National Natural Science Foundation of China for Young Scientists Fund (82203650, 82203782), Sichuan Science and Technology Program (2021YJ0132, 2021YFS0100); The fellowship of China Postdoctoral Science Foundation (2021M692277); Sichuan University-Zigong School-local Cooperation project (2021CDZG-23); Sichuan University-Sui Lin School-local Cooperation project (2022CDSN-18); Science and Technology project of the Health planning committee of Sichuan (21PJ046); Post-Doctor Research Project, West China Hospital, Sichuan University (2020HXBH127).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1267577/full#supplementary-material
References
1. Park W, Chawla A, O'Reilly EM. Pancreatic cancer: A review. Jama (2021) 326(9):851–62. doi: 10.1001/jama.2021.13027
2. Azar I, Virk G, Esfandiarifard S, Wazir A, Mehdi S, et al. Treatment and survival rates of stage IV pancreatic cancer at VA hospitals: a nation-wide study. J Gastrointest Oncol (2019) 10(4):703–11. doi: 10.21037/jgo.2018.07.08
3. Tonini V, Zanni M. Pancreatic cancer in 2021: What you need to know to win. World J Gastroenterol (2021) 27(35):5851–89. doi: 10.3748/wjg.v27.i35.5851
4. Hu Y, Guo M. Synthetic lethality strategies: Beyond BRCA1/2 mutations in pancreatic cancer. Cancer Sci (2020) 111(9):3111–21. doi: 10.1111/cas.14565
5. Nguyen L, WMM J, Van Hoeck A, Cuppen E. Pan-cancer landscape of homologous recombination deficiency. Nat Commun (2020) 11(1):5584. doi: 10.1038/s41467-020-19406-4
6. Kim H, Saka B, Knight S, Borges M, Childs E, Klein A, et al. Having pancreatic cancer with tumoral loss of ATM and normal TP53 protein expression is associated with a poorer prognosis. Clin Cancer Res (2014) 20(7):1865–72. doi: 10.1158/1078-0432.CCR-13-1239
7. Goldstein JB, Zhao L, Wang X, Ghelman Y, Overman MJ, Javle MM, et al. Germline DNA sequencing reveals novel mutations predictive of overall survival in a cohort of patients with pancreatic cancer. Clin Cancer Res (2020) 26(6):1385–94. doi: 10.1158/1078-0432.CCR-19-0224
8. Yin L, Wei J, Lu Z, Huang S, Gao H, Chen J, et al. Prevalence of germline sequence variations among patients with pancreatic cancer in China. JAMA Netw Open (2022) 5(2):e2148721. doi: 10.1001/jamanetworkopen.2021.48721
9. Zeng C, Bastarache LA, Tao R, Venner E, Hebbring S, Andujar JD, et al. Association of pathogenic variants in hereditary cancer genes with multiple diseases. JAMA Oncol (2022) 8(6):835–44. doi: 10.1001/jamaoncol.2022.0373
10. Sehdev A, Gbolahan O, Hancock BA, Stanley M, Shahda S, Wan J, et al. Germline and somatic DNA damage repair gene mutations and overall survival in metastatic pancreatic adenocarcinoma patients treated with FOLFIRINOX. Clin Cancer Res (2018) 24(24):6204–11. doi: 10.1158/1078-0432.CCR-18-1472
11. Emelyanova M, Pudova E, Khomich D, Krasnov G, Popova A, Abramov I, et al. Platinum-based chemotherapy for pancreatic cancer: impact of mutations in the homologous recombination repair and Fanconi anemia genes. Ther Adv Med Oncol (2022) 14:17588359221083050. doi: 10.1177/17588359221083050
12. Principe DR. Precision medicine for BRCA/PALB2-mutated pancreatic cancer and emerging strategies to improve therapeutic responses to PARP inhibition. Cancers (Basel) (2022) 14(4). doi: 10.3390/cancers14040897
13. Casolino R, Paiella S, Azzolina D, Beer PA, Corbo V, Lorenzoni G, et al. Homologous recombination deficiency in pancreatic cancer: A systematic review and prevalence meta-analysis. J Clin Oncol (2021) 39(23):2617–31. doi: 10.1200/JCO.20.03238
14. Park W, Chen J, Chou JF, Varghese AM, Yu KH, Wong W, et al. Genomic methods identify homologous recombination deficiency in pancreas adenocarcinoma and optimize treatment selection. Clin Cancer Res (2020) 26(13):3239–47. doi: 10.1158/1078-0432.CCR-20-0418
15. Dalmasso B, Puccini A, Catalano F, Borea R, Iaia ML, Bruno W, et al. Beyond BRCA: the emerging significance of DNA damage response and personalized treatment in pancreatic and prostate cancer patients. Int J Mol Sci (2022) 23(9). doi: 10.3390/ijms23094709
16. Chang AE, Radke MR, Zhen DB, Baker KK, Coveler AL, Wong KM, et al. DNA damage repair defects and survival outcomes for patients with resected pancreatic ductal adenocarcinoma. Pancreas (2021) 50(5):e50–2. doi: 10.1097/MPA.0000000000001819
17. Yu S, Agarwal P, Mamtani R, Symecko H, Spielman K, O'Hara M, et al. Retrospective survival analysis of patients with resected pancreatic ductal adenocarcinoma and a germline BRCA or PALB2 mutation. JCO Precis Oncol (2019) 3:1–11. doi: 10.1200/PO.18.00271
18. Blair AB, Groot VP, Gemenetzis G, Wei J, Cameron JL, Weiss MJ, et al. BRCA1/BRCA2 germline mutation carriers and sporadic pancreatic ductal adenocarcinoma. J Am Coll Surg (2018) 226(4):630–637.e631. doi: 10.1016/j.jamcollsurg.2017.12.021
19. Hannan Z, Yu S, Domchek S, Mamtani R, Reiss KA. Clinical characteristics of patients with pancreatic cancer and pathogenic ATM alterations. JNCI Cancer Spectr (2021) 5(2). doi: 10.1093/jncics/pkaa121
20. Shui L, Li X, Peng Y, Tian J, Li S, He D, et al. The germline/somatic DNA damage repair gene mutations modulate the therapeutic response in Chinese patients with advanced pancreatic ductal adenocarcinoma. J Transl Med (2021) 19(1):301. doi: 10.1186/s12967-021-02972-6
21. Abe K, Kitago M, Kitagawa Y, Hirasawa A. Hereditary pancreatic cancer. Int J Clin Oncol (2021) 26(10):1784–92. doi: 10.1007/s10147-021-02015-6
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj (2021) 372:n71. doi: 10.1136/bmj.n71
23. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
24. Golan T, Sella T, O'Reilly EM, Katz MH, Epelbaum R, Kelsen DP, et al. Overall survival and clinical characteristics of BRCA mutation carriers with stage I/II pancreatic cancer. Br J Cancer (2017) 116(6):697–702. doi: 10.1038/bjc.2017.19
25. Kondo T, Kanai M, Kou T, Sakuma T, Mochizuki H, Kamada M, et al. Association between homologous recombination repair gene mutations and response to oxaliplatin in pancreatic cancer. Oncotarget (2018) 9(28):19817–25. doi: 10.18632/oncotarget.24865
26. Palacio S, McMurry HS, Ali R, Donenberg T, Silva-Smith R, Wideroff G, et al. DNA damage repair deficiency as a predictive biomarker for FOLFIRINOX efficacy in metastatic pancreatic cancer. J Gastrointest Oncol (2019) 10(6):1133–9. doi: 10.21037/jgo.2019.09.12
27. Fountzilas E, Eliades A, Koliou GA, Achilleos A, Loizides C, Tsangaras K, et al. Clinical significance of germline cancer predisposing variants in unselected patients with pancreatic adenocarcinoma. Cancers (Basel) (2021) 13(2). doi: 10.3390/cancers13020198
28. Hu H, Zhu Y, Pu N, Burkhart RA, Burns W, Laheru D, et al. Association of germline variants in human DNA damage repair genes and response to adjuvant chemotherapy in resected pancreatic ductal adenocarcinoma. J Am Coll Surg (2020) 231(5):527–535.e514. doi: 10.1016/j.jamcollsurg.2020.06.019
29. Wattenberg MM, Asch D, Yu S, O'Dwyer PJ, Domchek SM, Nathanson KL, et al. Platinum response characteristics of patients with pancreatic ductal adenocarcinoma and a germline BRCA1, BRCA2 or PALB2 mutation. Br J Cancer (2020) 122(3):333–9. doi: 10.1038/s41416-019-0582-7
30. Reiss KA, Yu S, Judy R, Symecko H, Nathanson KL, Domchek SM. Retrospective survival analysis of patients with advanced pancreatic ductal adenocarcinoma and germline BRCA or PALB2 mutations. JCO Precis Oncol (2018) 2:1–9. doi: 10.1200/PO.17.00152
31. Yurgelun MB, Chittenden AB, Morales-Oyarvide V, Rubinson DA, Dunne RF, Kozak MM, et al. Germline cancer susceptibility gene variants, somatic second hits, and survival outcomes in patients with resected pancreatic cancer. Genet Med (2019) 21(1):213–23. doi: 10.1038/s41436-018-0009-5
32. Pishvaian MJ, Blais EM, Brody JR, Lyons E, DeArbeloa P, Hendifar A, et al. Overall survival in patients with pancreatic cancer receiving matched therapies following molecular profiling: a retrospective analysis of the Know Your Tumor registry trial. Lancet Oncol (2020) 21(4):508–18. doi: 10.1016/S1470-2045(20)30074-7
33. Pishvaian MJ, Blais EM, Brody JR, Rahib L, Lyons E, De Arbeloa P, et al. Outcomes in patients with pancreatic adenocarcinoma with genetic mutations in DNA damage response pathways: results from the know your tumor program. JCO Precis Oncol (2019) 3:1–10. doi: 10.1200/PO.19.00115
34. Yadav S, Kasi PM, Bamlet WR, Ho TP, Polley EC, Hu C, et al. Effect of germline mutations in homologous recombination repair genes on overall survival of patients with pancreatic adenocarcinoma. Clin Cancer Res (2020) 26(24):6505–12. doi: 10.1158/1078-0432.CCR-20-1788
35. Perkhofer L, Gout J, Roger E, Kude de Almeida F, Baptista Simões C, Wiesmüller L, et al. DNA damage repair as a target in pancreatic cancer: state-of-the-art and future perspectives. Gut (2021) 70(3):606–17. doi: 10.1136/gutjnl-2019-319984
36. Qian Y, Gong Y, Fan Z, Luo G, Huang Q, Deng S, et al. Molecular alterations and targeted therapy in pancreatic ductal adenocarcinoma. J Hematol Oncol (2020) 13(1):130. doi: 10.1186/s13045-020-00958-3
37. Stoof J, Harrold E, Mariottino S, Lowery MA, Walsh N. DNA damage repair deficiency in pancreatic ductal adenocarcinoma: preclinical models and clinical perspectives. Front Cell Dev Biol (2021) 9:749490. doi: 10.3389/fcell.2021.749490
38. Zhu H, Wei M, Xu J, Hua J, Liang C, Meng Q, et al. PARP inhibitors in pancreatic cancer: molecular mechanisms and clinical applications. Mol Cancer (2020) 19(1):49. doi: 10.1186/s12943-020-01167-9
39. Gonzalez D, Stenzinger A. Homologous recombination repair deficiency (HRD): From biology to clinical exploitation. Genes Chromosomes Cancer (2021) 60(5):299–302. doi: 10.1002/gcc.22939
40. Dreyer SB, Upstill-Goddard R, Paulus-Hock V, Paris C, Lampraki EM, Dray E, et al. Targeting DNA damage response and replication stress in pancreatic cancer. Gastroenterology (2021) 160(1):362–377.e313. doi: 10.1053/j.gastro.2020.09.043
41. Crowley F, Park W, O'Reilly EM. Targeting DNA damage repair pathways in pancreas cancer. Cancer Metastasis Rev (2021) 40(3):891–908. doi: 10.1007/s10555-021-09983-1
42. Gout J, Perkhofer L, Morawe M, Arnold F, Ihle M, Biber S, et al. Synergistic targeting and resistance to PARP inhibition in DNA damage repair-deficient pancreatic cancer. Gut (2021) 70(4):743–60. doi: 10.1136/gutjnl-2019-319970
Keywords: progression-free survival, overall survival, DNA damage repair gene, pancreatic cancer, platinum-based chemotherapy
Citation: Hu Y-F, Hu H-J, Kung H-C, Lv T-R, Yu J and Li F-Y (2023) DNA damage repair mutations in pancreatic cancer– prognostic or predictive? Front. Oncol. 13:1267577. doi: 10.3389/fonc.2023.1267577
Received: 02 August 2023; Accepted: 10 October 2023;
Published: 25 October 2023.
Edited by:
John Gibbs, Hackensack Meridian Health, United StatesReviewed by:
Marion Harris, Monash Health, AustraliaCuiling Zheng, Chinese Academy of Medical Sciences and Peking Union Medical College, China
Copyright © 2023 Hu, Hu, Kung, Lv, Yu and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fu-Yu Li, TGZ5Xzc0QGhvdG1haWwuY29t