 Mohamed Hassan1,2*†Julia Zimmermann3†Severin Schmid1,2Bernward Passlick1,2Julia Kovács3Rudolf Hatz3Hauke Winter4,5Laura V. Klotz4,5Martin E. Eichhorn4,5Till Markowiak6Karolina Müller7Gunnar Huppertz7Michael Koller7Hans-Stefan Hofmann6,8Michael Ried6
Mohamed Hassan1,2*†Julia Zimmermann3†Severin Schmid1,2Bernward Passlick1,2Julia Kovács3Rudolf Hatz3Hauke Winter4,5Laura V. Klotz4,5Martin E. Eichhorn4,5Till Markowiak6Karolina Müller7Gunnar Huppertz7Michael Koller7Hans-Stefan Hofmann6,8Michael Ried6- 1Department of Thoracic Surgery, Medical Center—University of Freiburg, Freiburg im Breisgau, Germany
- 2Faculty of Medicine, University of Freiburg, Freiburg im Breisgau, Germany
- 3Department of Thoracic Surgery, Ludwig-Maximilians-University of Munich, Asklepios Lung Clinic, Gauting, Germany
- 4Department of Thoracic Surgery, Thoraxklinik, University Hospital Heidelberg, Heidelberg, Germany
- 5Translational Lung Research Center (TLRC) Heidelberg, Member of the German Center for Lung Research (DZL), Heidelberg, Germany
- 6Department of Thoracic Surgery, University Hospital Regensburg, Regensburg, Germany
- 7Center for Clinical Studies, University Hospital Regensburg, Regensburg, Germany
- 8Department of Thoracic Surgery, Hospital Barmherzige Brüder Regensburg, Regensburg, Germany
Background: The role of cytoreductive surgery combined with hyperthermic intrathoracic chemotherapy (CRS+HITOC) for patients with secondary pleural metastases has scarcely been investigated.
Patients and Methods: We conducted a retrospective, multicentre study investigating the outcome of CRS+HITOC for 31 patients with pleural metastases from different primary tumours in four high-volume departments of thoracic surgery in Germany. The primary endpoint was overall survival (OS). Secondary endpoints included postoperative complications and recurrence/progression-free survival (RFS/PFS).
Results: The primary tumour was non-small cell lung cancer in 12 (39%), ovarian cancer in 5 (16%), sarcoma in 3 (10%), pseudomyxoma peritonei in 3 (10%), and others in 8 (26%) patients. A macroscopic complete resection (R/1) could be achieved in 28 (90%) patients. Major postoperative complications as classified by Clavien-Dindo (III-V) were observed in 11 (35%) patients. The postoperative mortality rate was 10% (n=3). A total of 13 patients received additive chemotherapy (42%). The median time of follow up was 30 months (95% CI = 17– 43). The median OS was 39 months (95% CI: 34-44 months) with 1-month, 3-month, 1-, 3-, and 5-year survival estimates of 97%, 89%, 77%, 66%, and 41%. There was a significantly prolonged OS in patients who received additive chemotherapy compared to patients with only CRS+HITOC (median OS 69 vs 38 months; p= 0.048). The median RFS was 14 months (95% CI: 7-21 months).
Conclusions: We observed that CRS+HITOC is a feasible approach with reasonable complications and prolonged survival as a part of multimodal concept for highly selected patients with secondary pleural metastases.
1 Introduction
For many tumours, development of synchronous or metachronous metastases correlates with poor survival (1). This is particularly true in the case of secondary pleural metastases, where local therapy options are significantly limited and only palliative treatment concepts in the sense of systemic chemotherapy or best supportive care can be offered. Either pleurodesis or an indwelling permanent pleural catheter can be performed to control the usually present malignant pleural effusion and to reduce effusion-related symptoms (2). A multimodal treatment approach combining systemic therapies with local therapies might lead to the best outcome for selected patients (3). However, in view of the advanced stage and the consequent palliative situation, it is important to identify suitable patients for multimodal therapy and to determine the best possible local pleural treatment. Additional intracavitary therapy like using hyperthermic intrathoracic chemotherapy (HITOC) after cytoreductive surgery (CRS) has been shown to be a feasible and safe treatment approach for patients with pleural malignancies, especially for malignant pleural mesothelioma or thymic tumours with pleural spread (4, 5). The combination of CRS and HITOC within the multimodal treatment of patients with secondary pleural metastases of other primary tumours has been evaluated only in few studies so far and included in particular pleural spread of lung cancer, ovarian cancer and pseudomyxoma (6–9). The aim of CRS before HITOC is to achieve macroscopic complete tumour resection (MCR) (10). The residual tumour cells are then treated with hyperthermic chemotherapeutical agents to improve local tumour control and to delay tumour recurrence with at best prolonged survival rates (11). Despite high concentrations of chemotherapeutic agents in the thoracic cavity, systemic side effects are fewer than during systemic treatment due to reduced intrathoracic absorption of the chemotherapy (12). Objective of this study was to investigate the feasibility and the outcome of radical local surgery including intracavitary chemotherapy in patients with secondary pleural metastases. Therefore, a selected and heterogenous subgroup of patients from the German HITOC-Study who underwent CRS+HITOC were analysed.
2 Patients and methods
2.1 Study design
In this retrospective multicentre study, clinical outcomes of patients with secondary pleural metastases after radical local surgery including intracavitary chemotherapy were analysed. Four high-volume departments of thoracic surgery in Germany collected data in the “German HITOC-Study” funded by the Deutsche Forschungsgemeinschaft – DFG, German Research Association (DFG, RI2905/3-1). The study group has already published first results about HITOC after CRS for pleural malignancies in general and for thymic tumours with pleural spread (5, 13, 14). Now, the focus will be on secondary pleural metastases and its surgical treatment combined with HITOC. The trial is registered in the German Registry of Clinical Studies (DRKS-ID: DRKS00015012). The approval of the ethics committee of the University of Regensburg (reference number: 18-1119-104) and of the ethics committees of the respective participating centres were obtained. All patients underwent elective CRS+HITOC within one surgery and in one of the four participating departments for thoracic surgery between January 2008 and December 2019 (13). The existing database was supplemented by an additional collection of clinical and follow-up data, which were updated until November 2021.
2.2 Definitions of variables and data collection
This subanalysis included all patients of the complete study sample (n= 350) with secondary pleural metastases (n= 31). Additive chemotherapy was defined as either induction chemotherapy and/or adjuvant chemotherapy. Postoperative complications were documented according to the Clavien-Dindo classification (15). The beginning of primary therapy was defined as date of CRS+HITOC if no induction chemotherapy was applied, or if induction chemotherapy was applied, as the date of first application of induction chemotherapy.
2.3 Endpoints
Primary endpoint of the study was Overall survival (OS) after CRS+HITOC. Secondary endpoints included postoperative morbidity/mortality and Recurrence and progression-free survival (RFS/PFS). OS was defined as time from beginning of the primary therapy until death from any cause. Recurrence and progression were defined as documented intrathoracic, ipsilateral and/or contralateral tumour detection by cytology/histology and/or imaging. RFS/PFS was defined as time from beginning of the primary therapy until first objective tumour recurrence/progression or death from any cause, which ever occurred first.
2.4 Statistical analysis
Descriptive analyses were done for demographic and baseline characteristics using frequency (n), percentage (%), mean (m), standard deviation (SD), median (med) and interquartile range (IQR). Median follow-up time was calculated using the reversed Kaplan-Meier method. OS and RFS/PFS were analysed by the Kaplan-Meier estimator. In univariable analyses (Log-Rank tests), OS and PFS/RFS were compared between cisplatin dosage (low dose ≤ 125 mg/m² BSA; high dose > 125 mg/m² BSA), chemotherapeutical agent (cisplatin alone vs cisplatin+doxorubicin), resection status, and additive chemotherapy. The estimates for the probability of surviving were presented graphically in Kaplan-Meier survival curves as well as for the specific time points: 1-month, 3-month, 1-year, 3-year, and 5-year survival rate. Moreover, the median survival time with 95% CI were presented when possible. All statistical analyses were conducted using the software package SPSS (version 26 or higher).
3 Results
3.1 Patient characteristics
Of the 31 included patients the mean age at the time of surgery was 50.3 ± 14.8 years. The primary pathology was non-small cell lung cancer (NSCLC) in 12 (39%), ovarian cancer in five (16%), sarcoma in three (10%), pseudomyxoma peritonei in three (10%), and others in eight (26%) patients. Pleural metastases were diagnosed with thoracoscopy and pleural biopsy in 18 (58%) patients (Table 1).
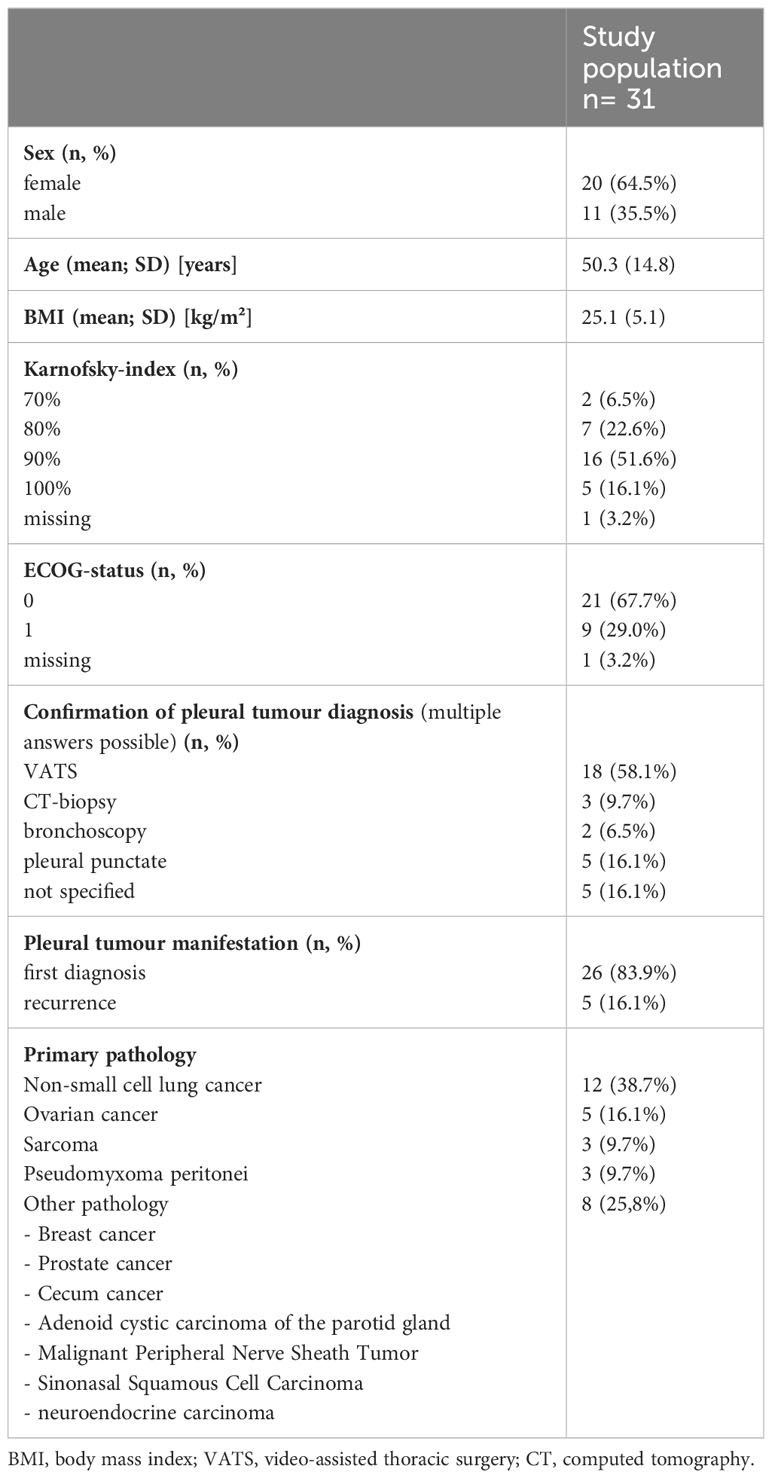
Table 1 Patient characteristics.
3.2 Operative and systemic treatments
All operations were done with a thoracotomy. Pleurectomy and decortication (P/D) was performed in five (16%), extended pleurectomy and decortication (eP/D) in 25 (81%), and extrapleural pneumonectomy (EPP) in one (3%) patient. Extended resections included additional chest wall resection in seven (23%) and anatomical lung resection in eight (26%) patients when appropriate due to tumour infiltration. A MCR (R0/1) could be achieved in 28 (90%) patients. HITOC with cisplatin only was performed in 22 (71%) and in combination with doxorubicin in nine (29%) patients. The median duration of surgery was 350.6 ± 71.6 minutes. There was no HITOC associated intraoperative complication. Additive chemotherapy was conducted in 13 patients (42%), which included neoadjuvant and/or adjuvant chemotherapy. Table 2 summarizes operative data and treatment details.
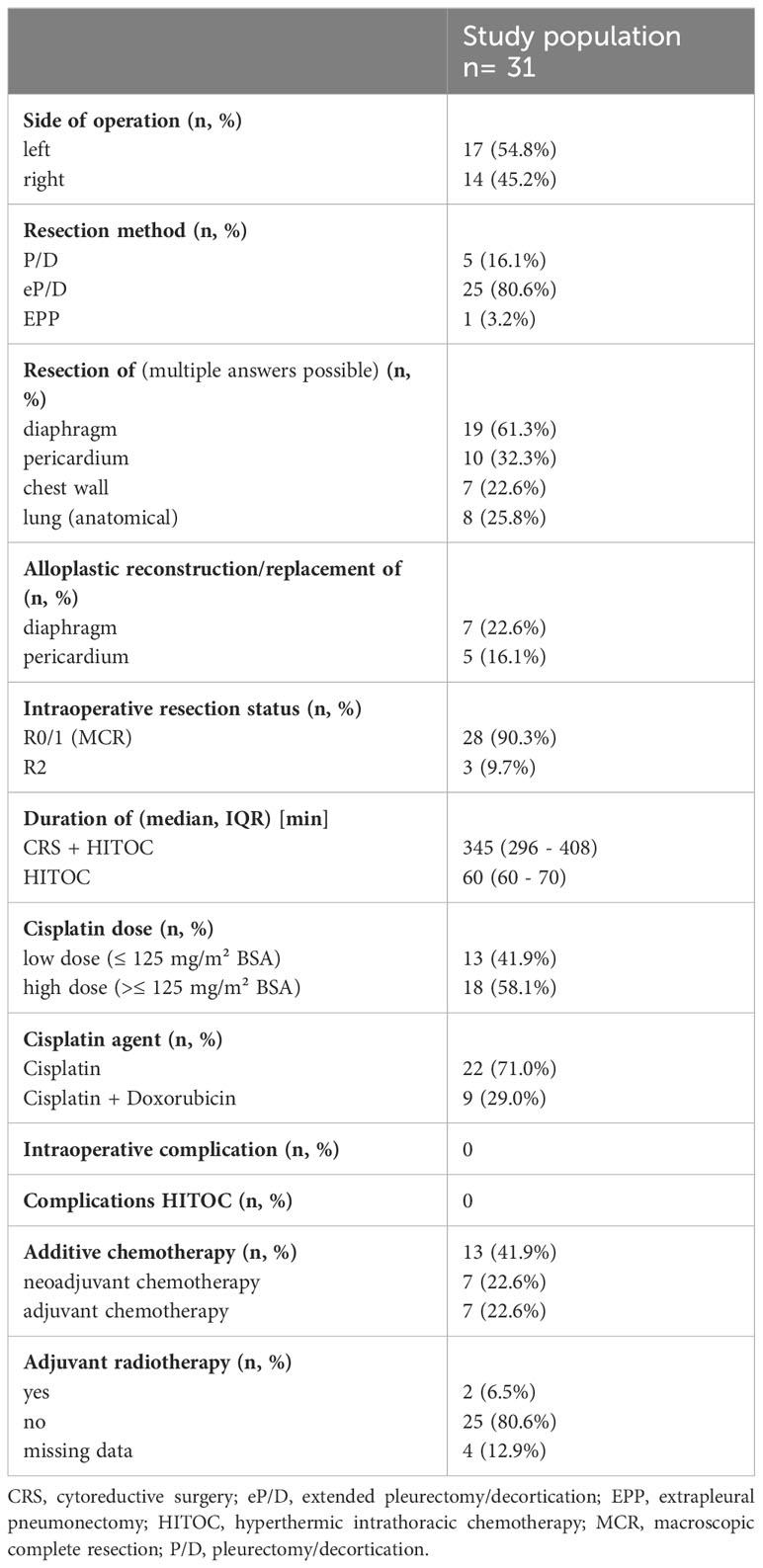
Table 2 Operative data and treatment details.
3.3 Postoperative course and complications
Major postoperative complications as classified by Clavien-Dindo (III-V) were observed in eleven patients (35%; Table 3). In total, six patients (19%) required surgical revision in consequence of hemothorax, chylothorax, pleural empyema, or prolonged air leak. Postoperative acute renal failure was observed in four patients (13%). Only one patient required postoperative dialysis. The postoperative mortality rate was 10% (n=3). The median ICU length of stay was two days (IQR: 1-4) and the median hospital length of stay was 15 days (IQR: 11 to 28).
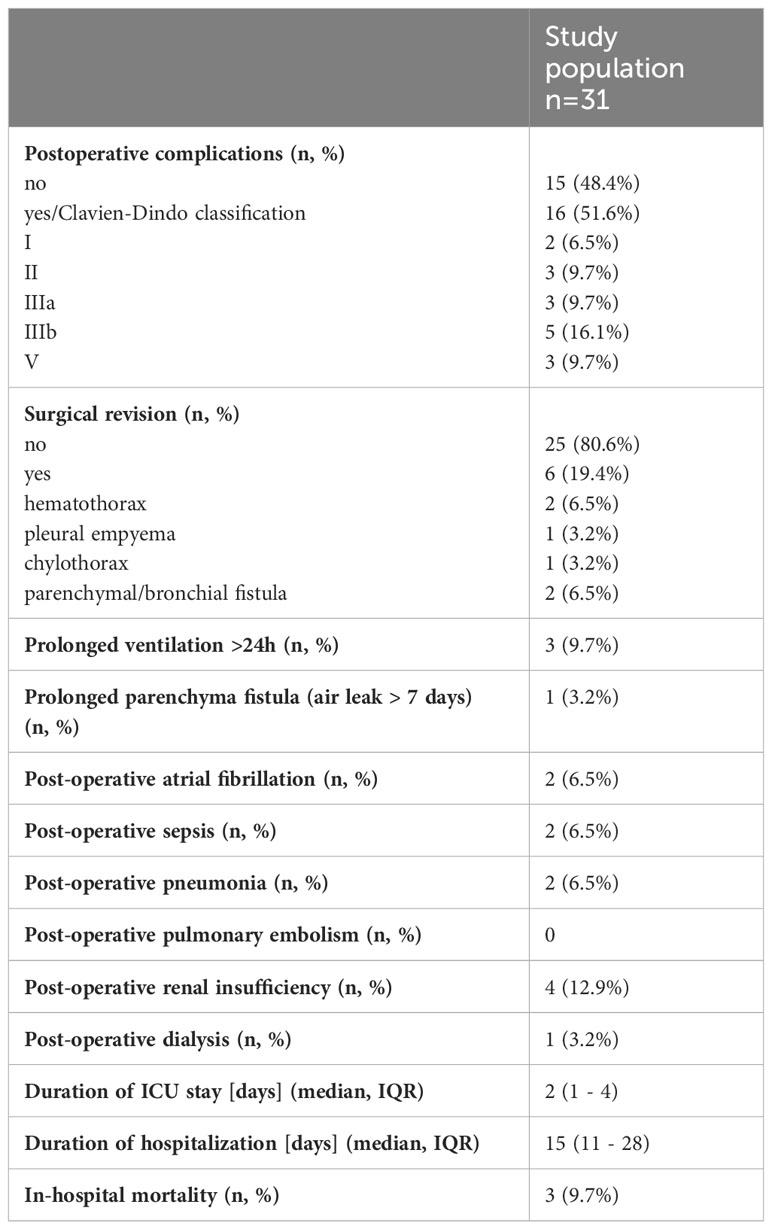
Table 3 Postoperative complications.
3.4 Survival analysis
Due to missing data, one patient had to be excluded from the survival analysis (Table 4). The median time of follow up was 30 months (95% CI = 17– 43, n = 30). The median OS was 39 months (95% CI: 34-44) with 1-month, 3-month, 1-, 3-, and 5-year survival estimates of 97%, 89%, 77%, 66%, and 41% (Figure 1A). Adding doxorubicin to cisplatin for HITOC was not associated with improved OS (p= 0.774, Figure 2A). The use of high dose cisplatin did not lead to prolonged OS compared to low dose cisplatin (p= 0.551; Figure 2B). The median OS improved significantly in patients who received additive chemotherapy compared to patients with only CRS+HITOC (median OS 69 vs 38 months; p= 0.048, n = 28; Figure 3A). Macroscopic incomplete resection (R2) was performed only in two (6%) patients and was associated with significantly decreased OS compared to 28 patients who had macroscopic complete resection (R0/1) (median OS 3 vs 41 months, p= 0.023). No evidence of disease recurrence or progress was documented in 18 patients (58%). Locoregional recurrence was observed in five (16%) and distant metastases in five (16%) patients. Due to missing data about tumour recurrence/progression status and date of start of primary therapy, four patients were excluded from analyses. The median RFS/PFS for the included patients (n= 27) was 14 months (95% CI: 7-21 months; Figure 1B). The use of high dose cisplatin or adding doxorubicin to cisplatin was not associated with improved RFS/PFS (p values > 0.050; Figures 2C, D). Patients who received additive chemotherapy showed an advantage in RFS/PFS compared to only CRS+HITOC (36 vs 12 months; p= 0.023; Figure 3B). Macroscopic incomplete resection (R2) was performed only in one patient and was associated with significantly decreased RFS/PFS compared to 26 patients who had macroscopic complete resection (R0/1) (median OS 3 vs 41 months, p= 0.064). A subgroup analysis of twelve patients with pleural metastasis of lung carcinoma (stage IV) showed a 3- month, 1-year and 3-year OS of 100%, 80% and 80%, Median PFS/RFS was 30 months (95% CI= 0-71) with estimated survival times at 3-month, 1-year and 3-year of 100%, 60% and 30%.
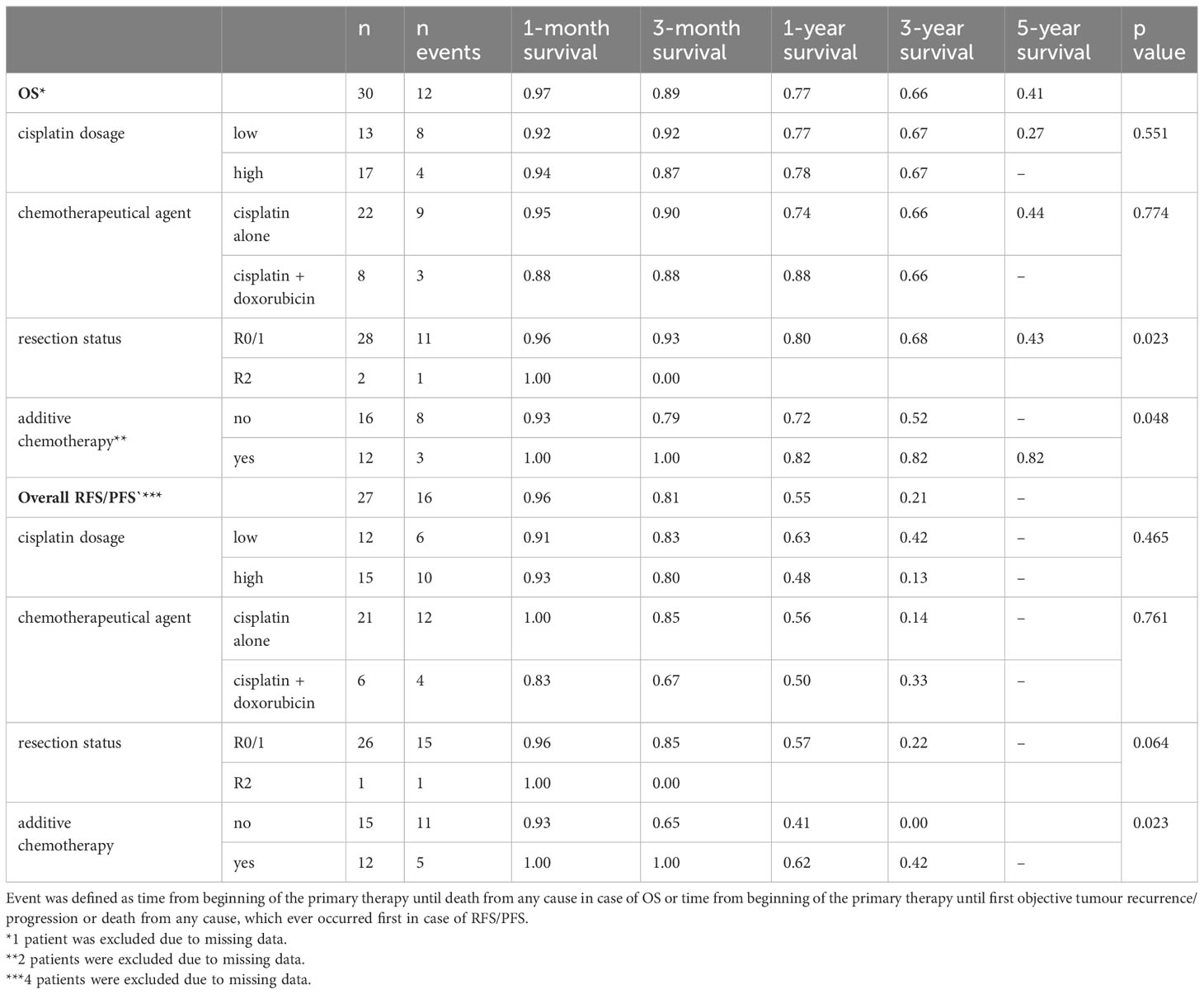
Table 4 Kaplan-Meier analysis of overall survival (OS) and recurrence/progression-free survival (RFS/PFS).
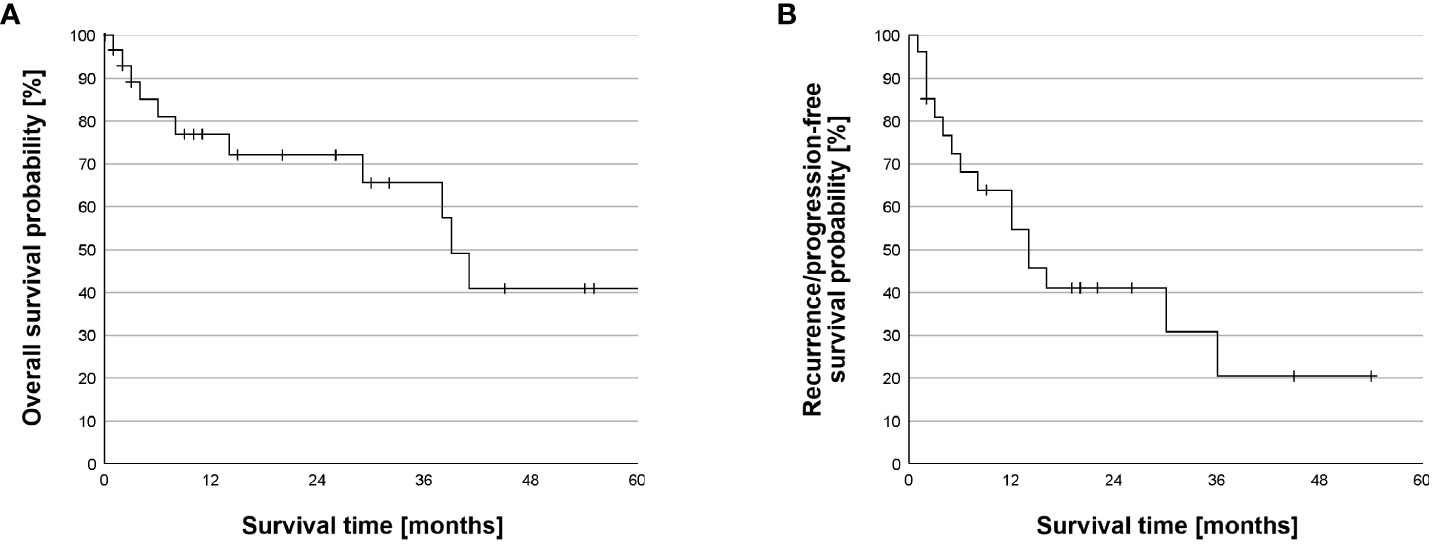
Figure 1 Overall Survival and recurrence/progression-free survival. (A) Kaplan-Meier survival analysis of overall survival (OS). The median OS was 39 months (95% CI: 34-44 months). The 1-month, 3-month, 1-, 3-, and 5-year survival estimates were 97%, 89%, 77%, 66%, and 41%. Survival time was truncated at 60 months after beginning of the primary therapy. One patient died 69 months after beginning of the primary therapy. (B) Kaplan-Meier survival analysis of recurrence/progression-free survival (RFS/PFS). The median RFS/PFS was 14 months (CI 95%: 6.9-21.1 months). The 1-month, 3-month, 1-, and 3-year survival estimates of 96%, 81%, 55%, and 21%.
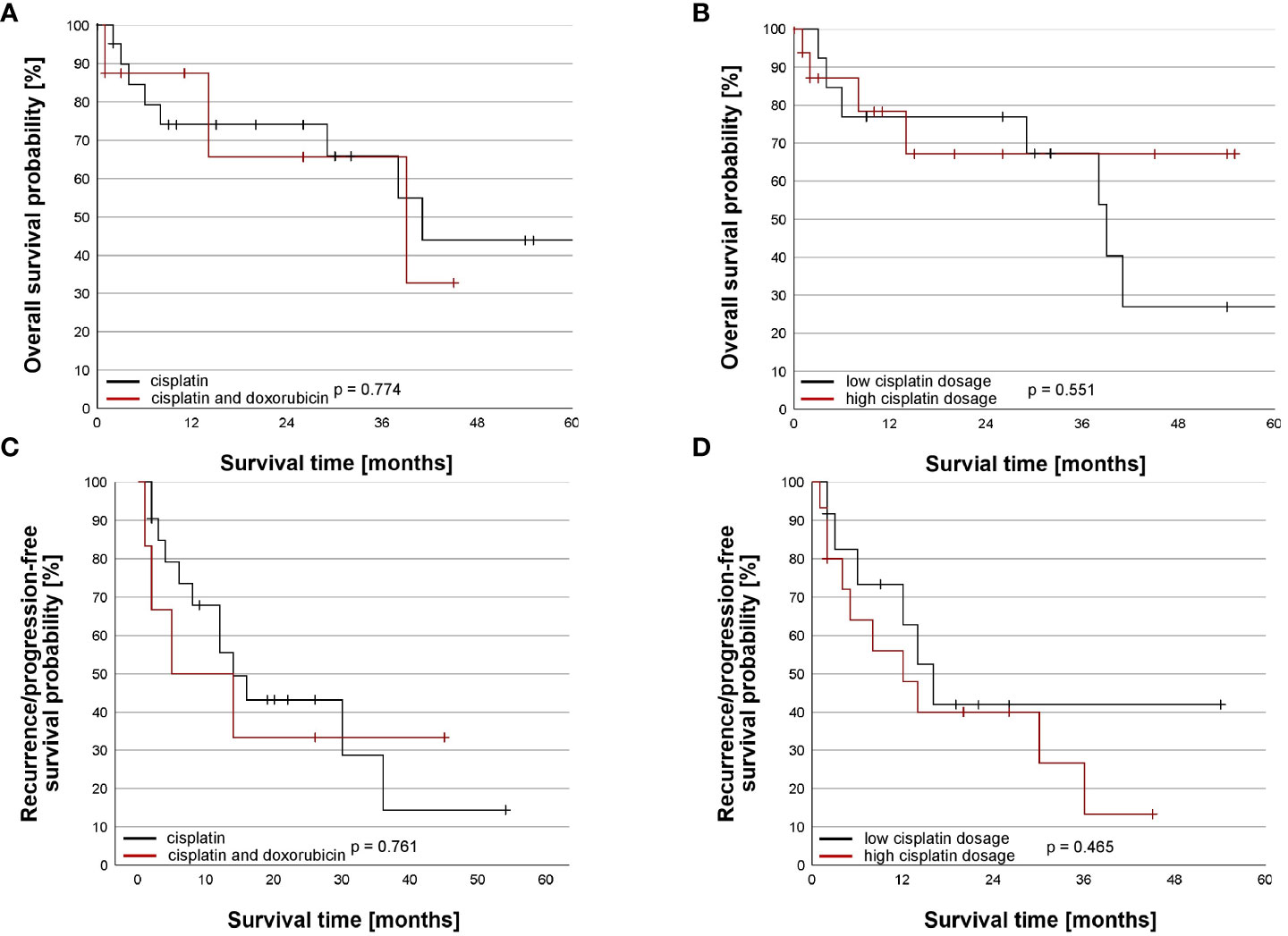
Figure 2 Impact of chemotherapeutic regime on the overall and recurrence/progression-free survival. (A) Comparison of overall survival (OS) between chemotherapeutical agent. OS did not differ between patients receiving cisplatin alone (n = 22) and cisplatin and doxorubicin (n= 8) (p=0.774). Survival time was truncated at 60 months after beginning of the primary therapy. One patient with cisplatin alone died 69 months after beginning of the primary therapy. (B) Comparison of overall survival (OS) between cisplatin dosage. OS did not differ between patients receiving low dose cisplatin (n = 13) and high dose cisplatin (n=17) (p=0.551). Survival time was truncated at 60 months after beginning of the primary therapy. One patient with low cisplatin dosage died 69 months after beginning of the primary therapy. (C) Comparison of recurrence/progression-free survival (RFS/PFS) between chemotherapeutical agent. RFS/PFS did not differ between patients receiving cisplatin alone (n = 21) and cisplatin and doxorubicin (n= 6) (p=0.761). (D) Comparison of recurrence/progression-free survival (RFS/PFS) between cisplatin dosage. RFS/PFS did not differ between patients receiving low dose cisplatin (n = 12) and high dose cisplatin (n= 15) (p=0.465).

Figure 3 Impact of additive chemotherapy on the overall and recurrence/progression-free survival. (A) Overall survival (OS) was improved in patients receiving additive chemotherapy (n = 12, med = 69 months, 95% CI = NA) compared to patients without additive chemotherapy (n= 16, med = 38 months, 95% CI = 9, 67) (p=0.048). Survival time was truncated at 60 months after beginning of the primary therapy. One patient with additive chemotherapy died 69 months after beginning of the primary therapy. (B) Recurrence/progression-free survival (RFS/PFS) was improved in patients receiving additive chemotherapy (n = 12, med = 36 months, 95% CI = 0, 77) compared to patients without additive chemotherapy (n= 15, med = 12 months, 95% CI = 0, 25) (p=0.023).
4 Discussion
Despite advances in systemic therapy for metastatic cancers, the prognosis of secondary pleural metastases remains poor with median survival times from four to nine months (16–19). The main finding of our study was a prolonged survival in selected patients with secondary pleural metastases after CRS+HITOC as a part of multimodal treatment approach with median overall survival of 39 months and median RFS/PFS of 14 months. Retrospective studies showed an encouraging survival of patients with pleural mesothelioma or thymus tumours with pleural involvement, who underwent a multimodal treatment approach including local interventions with CRS+HITOC (5, 11, 20). However, there is paucity of studies investigating the outcome of CRS+HITOC in patients with secondary pleural metastases as a part of multimodal concept. Therefore, the role of local interventions is still limited to reduce the symptoms of pleura effusions with an indwelling pleural catheter or pleurodesis (2, 17). CRS+HITOC can be performed after interdisciplinary discussion in the context of a multimodal approach in highly selected patients with an adequate general condition. Previous analyses confirmed the feasibility and safety of this combined surgical approach (14). Our sub-analysis also showed a reasonable major postoperative complication rate of 35% and a postoperative in-hospital mortality of 10%. We could not retrospectively provide the cause of postoperative mortality in the three patients. In addition to clinical (tumour stage, thoracic tumour spread) and functional parameters (above all ECOG), the decision on this radical procedure should also depend in particular on the histology of the primary tumour. We recommend a complete staging including mediastinal staging and PET-CT, however we could not retrospectively provide this data. Our study population included pleural metastases of various histological entities as mentioned above, but 12 patients (39%) in our study underwent CRS+HITOC for pleural metastases secondary to non-small cell lung cancer with encouraging survival rates of 80% OS after 3 years. Shigemura et al. showed a mean survival of 19 months in five patients with lung cancer and pleural metastases after a 2-step approach consisting of thoracoscopic intrathoracic chemotherapy followed by radical cytoreductive surgery in the form of an EPP (8). In our cohort, lung-sparing eP/D was the most performed technique of CRS (80.6%) and only one patient underwent EPP. EPP should be avoided when possible due to the high risk of early and late postoperative complications (21). However we could not investigate this factor as only one patient underwent EPP in our study.
In a systematic review investigating 21 patients who received CRS+HITOC for lung cancer with pleural metastases from four retrospective studies, the median survival was 18 months, which represents an encouraging result compared to the poor prognosis known in the literature with median survival of only 4 months (7, 22–24). However, these results should be cautiously interpreted due to the limited number of included patients. A previous study showed that about 60% of patients with pleural metastases are secondary to extra thoracic malignancies, with breast cancer as the most common primary with incidence about 25% followed by lymphoma (10%), ovarian cancer (5%), and intraabdominal malignancies (5%) (18). The complete surgical cytoreduction of metastatic ovarian cancer in the abdominal cavity was shown to be an independent prognostic factor, however the role of CRS in thoracic cavity has scarcely been reported (25, 26). Boerner et al. showed a promising survival in patients with ovarian cancer with pleural metastases after combined abdominal and thoracic CRS (27). The use of HITOC without CRS showed to be helpful for relieving the symptoms of pleural effusion in patients with metastatic ovarian cancer (28). Nikiforchin et al. showed promising results of CRS+HITOC for pleural metastases of peritoneal surface malignancies with 1-, 3-, and 5-year OS of 93%, 68%, and 68% with a median follow up of 22 months. The CRS+HITOC was performed either as a separate procedure via thoracotomy or as a part of the CRS+HIPEC through the diaphragm. The major postoperative complication rate was 20% for the combined CRS+HIPEC/HITOC and 13% for CRS+HITOC. In our study we reported a major postoperative complication rate of 35%. The higher incidence of major postoperative complication in our cohort may be associated to the extended resections including anatomical lung resections (26%) and chest wall resections (23%) which were not performed in the study of Nikiforchin et al. (3). For the various histological entities apart from non-small cell lung cancer in this study population, we were not able to perform any meaningful survival analyses due to the different entities with correspondingly low case numbers, so that studies with larger cohorts must be awaited here. Unfortunately, this is difficult to implement due to the specific indications (3). Likewise, clear recommendations for the selection of the intrathoracic chemotherapeutic agent and its dosage are still lacking. So far, only the data on HITOC in MPM and pleural metastatic thymic tumours can be used as a guide (9). To date, the most commonly used substances are cisplatin, doxorubicin and mitomycin C (9). Sugarbaker et al. showed a persistent high intrapleural concentration of doxorubicin and mitomycin C for patients undergoing HITOC and provided a pharmacological rationale for HITOC (12). We observed no advantage in the OS or RFS/PFS using high dose of cisplatin or adding doxorubicin. Based on our results, a decisive criterion for the preoperative indication seems to be the possibility of macroscopic complete resection. The impact of the resection status after CRS+HITOC for secondary pleural metastases were mostly not even investigated. Our results indicate that macroscopic complete resection could lead to a prolonged OS and RFS/PFS. These results reveal the importance of a careful selection of patients who might profit from CRS+HITOC. However, these findings should be interpreted with caution as this analysis included a very limited number of patients with macroscopic incomplete resection (two patients for OS and only one patient for RFS/PFS). Pleural metastases are usually a sign of systemic disease with poor prognosis. However, there is a trend of improvement of the survival in patients with pleural metastases comparing earlier with most recent studies, which could reflect the evolution of systemic treatment options (29, 30). Our results also support this assumption, as patients who received additive chemotherapy showed a significantly prolonged survival compared to patient who underwent only local therapy with CRS+HITOC. Furthermore, the CRS+HITOC in our study was an individual concept as a part of multimodal treatment in selected patients without evidence of others metastases. We recommend that all patients should be discussed preoperatively in an interdisciplinary tumour board, which should recommend this treatment on a case-by-case basis.
5 Limitations
The major limitations of our study were the retrospective nature, the absence of a comparative group and the heterogeneity of included patients. Retrospectively, we could not comprehend why some patients in our study did not receive any additional systemic chemotherapy for secondary pleural metastases. Another aspect which should be considered is the limited number of patients who underwent CRS+HITOC for secondary pleural metastases in four high volume departments for thoracic surgery in Germany over eleven years. This might reflect the high selection of patients and cannot lead to a definitive conclusion regarding the role of CRS+HITOC as a part of treatment of this condition. However, we present one of the largest series of patients who underwent this local, intracavitary treatment approach for pleural metastases which may help for better selection of patients until further studies are available.
6 Conclusions
CRS+HITOC for secondary pleural metastases is feasible and associated with reasonable postoperative morbidity and mortality. We were able to observe a prolonged survival in highly selected patients with secondary pleural metastases after CRS+HITOC as a part of a multimodality treatment concept, especially in patients with stage IV lung carcinoma. In our view, a strict indication for this surgical procedure is required, which should especially take into account the chance for MCR and the possibility of additive systemic therapy.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the ethics committee of the University of Regensburg (reference number: 18-1119-104) and of the ethics committees of the respective participating centers were obtained. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Patient consent was waived due to the retrospective design of the study and collection of routine clinical data. Data was processed in a pseudonymised manner in accordance with European Union General Data Protection Regulation (EUGDPR) and Bavarian Hospital Law (BayKrG).
Author contributions
MH: Investigation, Validation, Writing – original draft, Writing – review & editing. JZ: Investigation, Validation, Writing – original draft, Writing – review & editing. SS: Validation, Writing – review & editing, Conceptualization, Writing – original draft. BP: Conceptualization, Supervision, Writing – review & editing. JK: Investigation, Writing – original draft, Writing – review & editing. RH: Conceptualization, Supervision, Writing – review & editing. HW: Supervision, Writing – review & editing. LK: Investigation, Writing – review & editing. ME: Conceptualization, Writing – review & editing. TM: Investigation, Methodology, Resources, Writing – review & editing. KM: Data curation, Formal Analysis, Methodology, Project administration, Software, Writing – review & editing, Visualization. GH: Formal Analysis, Methodology, Software, Writing – review & editing. MK: Data curation, Formal Analysis, Methodology, Software, Writing – review & editing. HH: Conceptualization, Supervision, Writing – review & editing, Resources. MR: Conceptualization, Project administration, Writing – original draft, Writing – review & editing, Funding acquisition, Investigation, Methodology.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was founded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation), Kennedyallee 40, 53170, Bonn, Germany.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin (2016) 66:7–30. doi: 10.3322/caac.21332
2. Hofmann H-S, Scheule AM, Markowiak T, Ried M. The treatment of Malignant pleural effusion with permanent indwelling pleural catheters. Dtsch Arzteblatt Int (2022) 119:595–600. doi: 10.3238/arztebl.m2022.0229
3. Nikiforchin A, Gushchin V, King MC, Baron E, Lopez-Ramirez F, Sardi A. Cytoreductive surgery with hyperthermic intrathoracic chemotherapy for patients with intrapleural dissemination of peritoneal surface Malignancies. Ann Surg Oncol (2021) 28:9126–35. doi: 10.1245/s10434-021-10298-2
4. Ried M, Kovács J, Markowiak T, Müller K, Huppertz G, Koller M, et al. Hyperthermic intrathoracic chemotherapy (HITOC) after cytoreductive surgery for pleural Malignancies-A retrospective, multicentre study. Cancers (2021) 13:4580. doi: 10.3390/cancers13184580
5. Ried M, Hassan M, Passlick B, Schmid S, Markowiak T, Müller K, et al. Surgical cytoreduction and hyperthermic intrathoracic chemotherapy for thymic tumours with pleural spread is effective on survival: results from the multicentre German HITOC-study. Interdiscip Cardiovasc Thorac Surg (2023) 36:ivad032. doi: 10.1093/icvts/ivad032
6. Ried M, Potzger T, Braune N, Neu R, Zausig Y, Schalke B, et al. Cytoreductive surgery and hyperthermic intrathoracic chemotherapy perfusion for Malignant pleural tumours: perioperative management and clinical experience. Eur J Cardio-Thorac Surg (2013) 43:801–7. doi: 10.1093/ejcts/ezs418
7. Migliore M, Calvo D, Criscione A, Viola C, Privitera G, Spatola C, et al. Cytoreductive surgery and hyperthermic intrapleural chemotherapy for Malignant pleural diseases: preliminary experience. Future Oncol (2015) 11:47–52. doi: 10.2217/fon.14.256
8. Shigemura N, Akashi A, Ohta M, Matsuda H. Combined surgery of intrapleural perfusion hyperthermic chemotherapy and panpleuropneumonectomy for lung cancer with advanced pleural spread: a pilot study. Interact Cardiovasc Thorac Surg (2003) 2:671–5. doi: 10.1016/S1569-9293(03)00197-X
9. Zhou H, Wu W, Tang X, Zhou J, Shen Y. Effect of hyperthermic intrathoracic chemotherapy (HITHOC) on the Malignant pleural effusion: A systematic review and meta-analysis. Med (Baltimore) (2017) 96:e5532. doi: 10.1097/MD.0000000000005532
10. Sugarbaker DJ. Macroscopic complete resection: the goal of primary surgery in multimodality therapy for pleural mesothelioma. J Thorac Oncol (2006) 1:175–6. doi: 10.1097/01243894-200602000-00014
11. Sugarbaker DJ, Gill RR, Yeap BY, Wolf AS, DaSilva MC, Baldini EH, et al. Hyperthermic intraoperative pleural cisplatin chemotherapy extends interval to recurrence and survival among low-risk patients with Malignant pleural mesothelioma undergoing surgical macroscopic complete resection. J Thorac Cardiovasc Surg (2013) 145:955–63. doi: 10.1016/j.jtcvs.2012.12.037
12. Sugarbaker PH, Stuart OA, Eger C. Pharmacokinetics of hyperthermic intrathoracic chemotherapy following pleurectomy and decortication. Gastroenterol Res Pract (2012) 2012:471205. doi: 10.1155/2012/471205
13. Markowiak T, Koller M, Zeman F, Huppertz G, Hofmann H-S, Ried M. Protocol of a retrospective, multicentre observational study on hyperthermic intrathoracic chemotherapy in Germany. BMJ Open (2020) 10:e041511. doi: 10.1136/bmjopen-2020-041511
14. Ried M, Kovács J, Markowiak T, Müller K, Huppertz G, Koller M, et al. Hyperthermic intrathoracic chemotherapy (HITOC) after cytoreductive surgery for pleural Malignancies—A retrospective, multicentre study. Cancers (2021) 13:4580. doi: 10.3390/cancers13184580
15. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications. Ann Surg (2004) 240:205–13. doi: 10.1097/01.sla.0000133083.54934.ae
16. Chernow B, Sahn SA. Carcinomatous involvement of the pleura: an analysis of 96 patients. Am J Med (1977) 63:695–702. doi: 10.1016/0002-9343(77)90154-1
17. Martínez-Moragón E, Aparicio J, Sanchis J, Menéndez R, Rogado MC, Sanchis F. Malignant pleural effusion: prognostic factors for survival and response to chemical pleurodesis in a series of 120 cases. Respiration (1998) 65:108–13. doi: 10.1159/000029240
18. Migliore M, Milosevic M, Koledin B. Pleural carcinosis caused by extrathoracic Malignancies. AME Med J (2021) 6. doi: 10.21037/amj-2019-mpe-07
19. Zamboni MM, da Silva CT, Baretta R, Cunha ET, Cardoso GP. Important prognostic factors for survival in patients with Malignant pleural effusion. BMC Pulm Med (2015) 15:29. doi: 10.1186/s12890-015-0025-z
20. Piso P, Hofmann HS. Aktuelle Entwicklungen in der regionalen Behandlung von peritonealen und pleuralen Tumoren (inkl. HIPEC und HITOC). Zentralblatt Für Chir - Z Für Allg Visz Thorax- Gefäßchirurgie (2019) 144:235–41. doi: 10.1055/a-0882-6545
21. Migliore M, Combellack T, Williams J, Kornaszewska M, Valtzoglou V, Pirtnieks A. Hyperthermic intrathoracic chemotherapy in thoracic surgical oncology: future challenges of an exciting procedure. Future Oncol (2021) 17:3901–4. doi: 10.2217/fon-2021-0317
22. Işık AF, Sanlı M, Yılmaz M, Meteroğlu F, Dikensoy O, Sevinç A, et al. Intrapleural hyperthermic perfusion chemotherapy in subjects with metastatic pleural Malignancies. Respir Med (2013) 107:762–7. doi: 10.1016/j.rmed.2013.01.010
23. Monneuse O, Beaujard AC, Guibert B, Gilly FN, Mulsant P, Carry PY, et al. Long-term results of intrathoracic chemohyperthermia (ITCH) for the treatment of pleural Malignancies. Br J Cancer (2003) 88:1839–43. doi: 10.1038/sj.bjc.6601000
24. Migliore M, Nardini M. Does cytoreduction surgery and hyperthermic intrathoracic chemotherapy prolong survival in patients with N0-N1 nonsmall cell lung cancer and Malignant pleural effusion? Eur Respir Rev (2019) 28:190018. doi: 10.1183/16000617.0018-2019
25. Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, et al. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol Oncol (2006) 103:559–64. doi: 10.1016/j.ygyno.2006.03.051
26. Tseng JH, Cowan RA, Zhou Q, Iasonos A, Byrne M, Polcino T, et al. Continuous improvement in primary debulking surgery for advanced ovarian cancer: do increased complete gross resection rates independently lead to increased progression-free and overall survival? Gynecol Oncol (2018) 151:24–31. doi: 10.1016/j.ygyno.2018.08.014
27. Boerner T, Filippova OT, Chi AJ, Iasonos A, Zhou QC, Roche KL, et al. Video-assisted thoracic surgery in the primary management of advanced ovarian carcinoma with moderate to large pleural effusions: A memorial sloan kettering cancer center team ovary study. Gynecol Oncol (2020) 159:66–71. doi: 10.1016/j.ygyno.2020.07.101
28. Karampinis I, Dionysopoulou A, Galata C, Almstedt K, Grilli M, Hasenburg A, et al. Hyperthermic intrathoracic chemotherapy for the treatment of Malignant pleural effusion caused by breast and ovarian cancer: A systematic literature review and pooled analysis. Thorac Cancer (2022) 13:883–8. doi: 10.1111/1759-7714.14361
29. Roberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ. Management of a Malignant pleural effusion: British Thoracic Society pleural disease guideline 2010. Thorax (2010) 65:ii32–40. doi: 10.1136/thx.2010.136994
Keywords: HITOC, cytoreductive surgery, pleural metastases, non-small cell lung cancer, hyperthermic intrathoracic chemotherapy
Citation: Hassan M, Zimmermann J, Schmid S, Passlick B, Kovács J, Hatz R, Winter H, Klotz LV, Eichhorn ME, Markowiak T, Müller K, Huppertz G, Koller M, Hofmann H-S and Ried M (2023) Outcome after cytoreductive surgery combined with hyperthermic intrathoracic chemotherapy in patients with secondary pleural metastases. Front. Oncol. 13:1259779. doi: 10.3389/fonc.2023.1259779
Received: 16 July 2023; Accepted: 13 November 2023;
Published: 28 November 2023.
Edited by:
Ulrich Ronellenfitsch, Medical Faculty of the Martin-Luther-University Halle-Wittenberg, GermanyReviewed by:
Joachim Pfannschmidt, HELIOS Klinikum Emil von Behring, GermanyDavid Morris, University of New South Wales, Australia
Marcello Migliore, University of Catania, Italy
Copyright © 2023 Hassan, Zimmermann, Schmid, Passlick, Kovács, Hatz, Winter, Klotz, Eichhorn, Markowiak, Müller, Huppertz, Koller, Hofmann and Ried. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohamed Hassan, Mohamed.r.hassan@outlook.com
†These authors have contributed equally to this work and share first authorship