 Jie He
Jie He Wei Luo
Wei Luo Yuanyuan Huang
Yuanyuan Huang Lingmeng Song
Lingmeng Song Yang Mei
Yang Mei- 1Clinical Medical College of Chengdu Medical College, Chengdu, Sichuan, China
- 2Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, China
- 3Key Laboratory of Geriatric Respiratory Diseases of Sichuan Higher Education Institutes, Chengdu, Sichuan, China
- 4Radiology Department, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, China
- 5Medical Department, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, China
Background: Sarcopenia, often observed in the elderly, is associated with declining skeletal muscle mass and impaired muscle function. This condition has been consistently linked to a less favorable prognosis in various malignancies. Computed tomography (CT) is a frequently employed modality for evaluating skeletal muscle mass, enabling the measurement of the skeletal muscle index (SMI) at the third lumbar vertebra (L3) level. This measurement serves as a defining criterion for sarcopenia. The meta-analysis dealt with evaluating the promise sarcopenia held as a prognostic indicator in individuals with colorectal cancer.
Methods: Research relevant to the subject was determined by systematically searching PubMed, Embase, Web of Science, WANFANG, and CNKI (up to June 11, 2023, published studies). In this meta-analysis, the incidence of sarcopenia in individuals with colorectal cancer was combined to analyze the disease-free survival (DFS), overall survival (OS), and cancer-specific survival (CSS) of these individuals with and without sarcopenia. The included research was evaluated for quality per the Newcastle-Ottawa Scale (NOS) score. In the multivariate analysis of each study, the direct extraction of hazard ratio (HR) with a 95% confidence interval (CI) was executed. STATA 11.0 was applied to integrate and statistically analyze the data.
Results: Overall 20 articles participated in this meta-analysis. A 34% incidence of sarcopenia was noted in colorectal cancer. The presence of sarcopenia denoted a decrease in OS (HR=1.72,95% CI=1.45-2.03), DFS (HR=1.42,95% CI=1.26-1.60) and CSS (HR=1.48,95% CI=1.26-1.75) in individuals with colorectal cancer. In addition, the subgroup analysis depicted a pattern consistent with the overall analysis results.
Conclusion: CT-defined sarcopenia exhibits promise as an indicator of survival prognosis in individuals with colorectal cancer. Future studies need a more rigorous definition of sarcopenia to further verify these findings.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/, identifier CRD42023431435.
1 Introduction
Globally, Colorectal cancer is the third highly predominant malignancy and stands as the fourth highest contributor to cancer death in men and women, with rectal cancer accounting for approximately 30% of these cases (1, 2). Colorectal cancer has been challenging to address due to its anatomical structure and high local recurrence rate. Currently, the standard treatment encompasses surgical resection and neoadjuvant chemoradiotherapy (nCRT) for individuals with locally advanced rectal cancer (3). Preoperative nCRT has been noted to improve local infiltration and reduce toxicity in rectal cancer compared with postoperative nCRT, with no improvement in overall survival (OS) (4). Although the treatment of colon cancer has progressed greatly, including surgery or radiotherapy, the prognosis of individuals with colon cancer have not progressed significantly in recent years (5). Prognostic stratification of colorectal cancer patients relies on tumor pathology after radical surgery; however, baseline host-related factors may also negatively impact long-term survival outcomes. Therefore, identifying key risk factors linked with the prognosis of individuals with colorectal cancer patients is of great clinical value.
It is well known that the body structure of cancer patients changes as the disease progresses (6). The European Working Group on Sarcopenia in the Elderly (EWGSOP), associate sarcopenia with declining muscle mass and impairment of muscle function (strength or performance) (7). A frequently observed condition in older adults, sarcopenia has been consistently linked with a more unfavorable prognosis across diverse cancers, including head and neck, colorectal, and breast cancers (8–12). Meyer et al. found that sarcopenia was a prognostic marker for survival in gastric cancer undergoing palliative chemotherapy (13). Additionally, Gan H et al. pointed out both low skeletal muscle mass and poor muscle quality were relative with poor long term survival of patients with pancreatic cancer (14). The Computed tomography (CT) scans enable the measurement of the third lumbar spine skeletal muscle index (L3-SMI). This measurement serves as a defining criterion for sarcopenia (15). In individuals with cancer, routine CT scans are utilized for assessing tumor lesions and monitoring tumor metastases. The scan data is commonly utilized for measuring skeletal muscle mass without additional radiation.
The relationship of sarcopenia with cancer outcomes is garnering growing attention. The data of prior meta-analyses is indicative of the reduced efficacy of sarcopenia in predicting OS in colorectal cancer patients (16, 17). Several more recent studies have reported a correlation of sarcopenia with OS in individuals with colorectal cancer, however, the results remain debatable. Herein, a meta-analysis investigating the potential negative impact of sarcopenia, as defined by L3-SMI, on OS in individuals with colorectal cancer was conducted.
2 Methods
This meta-analysis study adhered to the guidelines provided in the Preferred Reporting Items for Systematic Evaluation and Meta-Analysis (PRISMA) (18).
2.1 Search strategy
Two researchers undertook the task of assessing the literature pool for relevant research independently. In case of disagreements, a third researcher was involved in resolving the issues through discussion, if required. A pre-defined protocol was utilized to conduct the research. The literature relevant to the research was filtered by assessing published articles (up to June 1, 2023) available on PubMed, Embase, Web of Science, WANFANG, and CNKI. The search was focused on the key terms and limited to the English language. The below-mentioned MeSH/main keywords were utilized: “colorectal”, “rectal”, “rectum”, “colon”, “colonic”, “myopenia”, “sarcopenia”, and “muscle mass” using datasets. In addition, studies and relevant reviews were manually searched to determine additional eligible studies.
2.2 Inclusion and exclusion criteria
Studies were part of this meta-analysis if they met the mentioned criteria: (1) individuals with colorectal cancer; (2) comparing OS, disease-free survival (DFS), and cancer-specific survival (CSS) in patients with and without sarcopenia; (3) quantitative measurement of skeletal muscle mass by CT at the L3 level; (4) studies reporting adjusted hazard ratios (HR) and 95% confidence intervals (CI) for OS, DFS, and CSS studies.
The exclusion of case reports, reviews, conference abstracts, commentaries, and animal studies were carried out. In addition, research that lacked valid data was excluded, such as HR and 95% CI.
2.3 Data extraction
Standardized forms were utilized by two researchers for pertinent data extraction from the included studies. A third researcher was involved in the resolution of disagreements through consensus and discussion. Each study involved in the research was assessed for the following data: first author, publication year, country, design of the study design, patient number, mean/median population age, percentage of males, stage of the disease, SMI measure, the cut-off point for SMI, the prevalence of sarcopenia, and HR for OS, DFS, and 95% CI for CSS. OS was termed as the occurrence of fatality due to any cause; DFS as the recurrence of the disease or fatality; and CSS as the occurrence of fatality linked with cancer.
2.4 Quality assessment
The Newcastle-Ottawa Scale (NOS) assessed the quality of the research involved in the study. This assessment was conducted by two independent reviewers, with the quality ranging from low to medium to high per respective scores of 1-3, 4-6, and 7-9 (19). The two reviewers engaged in discussion for the resolution of any discrepancy in the above studies.
2.5 Statistical analysis
This meta-analysis was executed through STATA 11.0. Direct extraction of sarcopenia-linked 95% CIs for OS, DFS, and CSS, as well as HRs was carried out utilizing the included studies. Chi-square tests and I2 statistics were employed for assessing heterogeneity across the studies with P < 0.1 and I2 > 50% suggesting statistical significance. Given the variation in cut-off points for the diagnosis of sarcopenia in SMI, some heterogeneity may exist between studies. Therefore, the random-effects model was utilized for multivariate data when P < 0.1 and I2 > 50% in this research; conversely, the fixed-effect model was employed. For combined studies with the number of studies greater than 5, a subgroup analysis was performed. Furthermore, the heterogeneity sources were explored through sensitivity analyses. Whereas possible potential bias was examined through funnel plots with low bias indicated by the symmetrical distribution of funnel plot shapes. P < 0.05 from Begg’s and Egger’s tests was considered publication bias for the combined studies.
3 Results
3.1 Characteristics of the literature
Overall, 829 published studies were determined according to our search, and duplicate publications were eliminated. Further, the titles, abstracts, and even the full articles were read, and finally, 20 articles were involved in this meta-analysis (12, 20–38). The search strategy is depicted in a flowchart in Figure 1, which covers the reasons for the exclusion criterion. Among the included studies, two study were prospective and the other 18 were retrospective studies. In addition, 13 studies were conducted in an Asian country and the other studies were from European and North American countries. Moreover, 15 study had an NOS score of >5. Table 1 depicts the summarized data concerning the features of the included studies. Furthermore, Table 2 summarizes the definition and critical values of sarcopenia in the assessed studies.
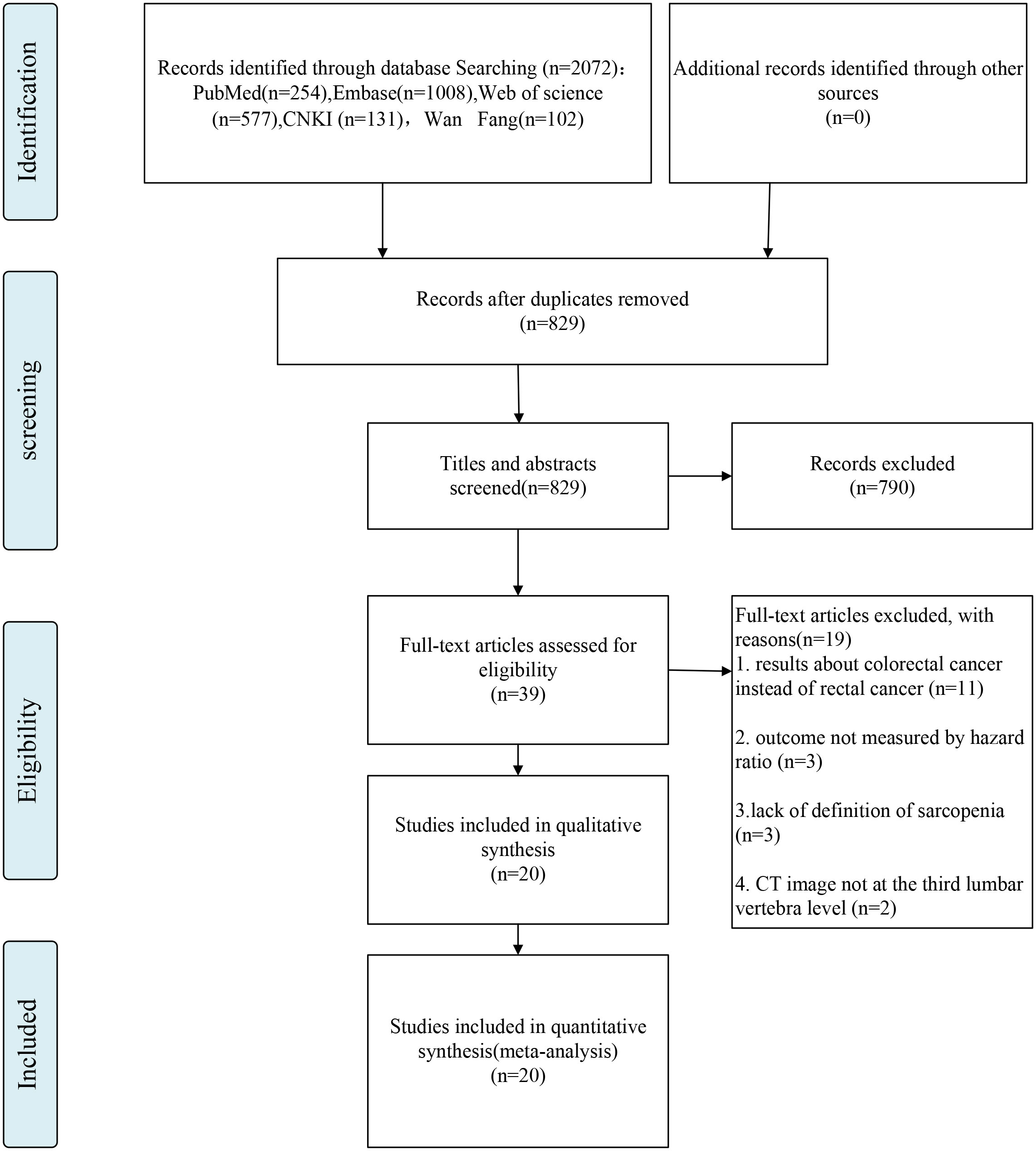
Figure 1 Flow chart of inclusion criteria in the study.
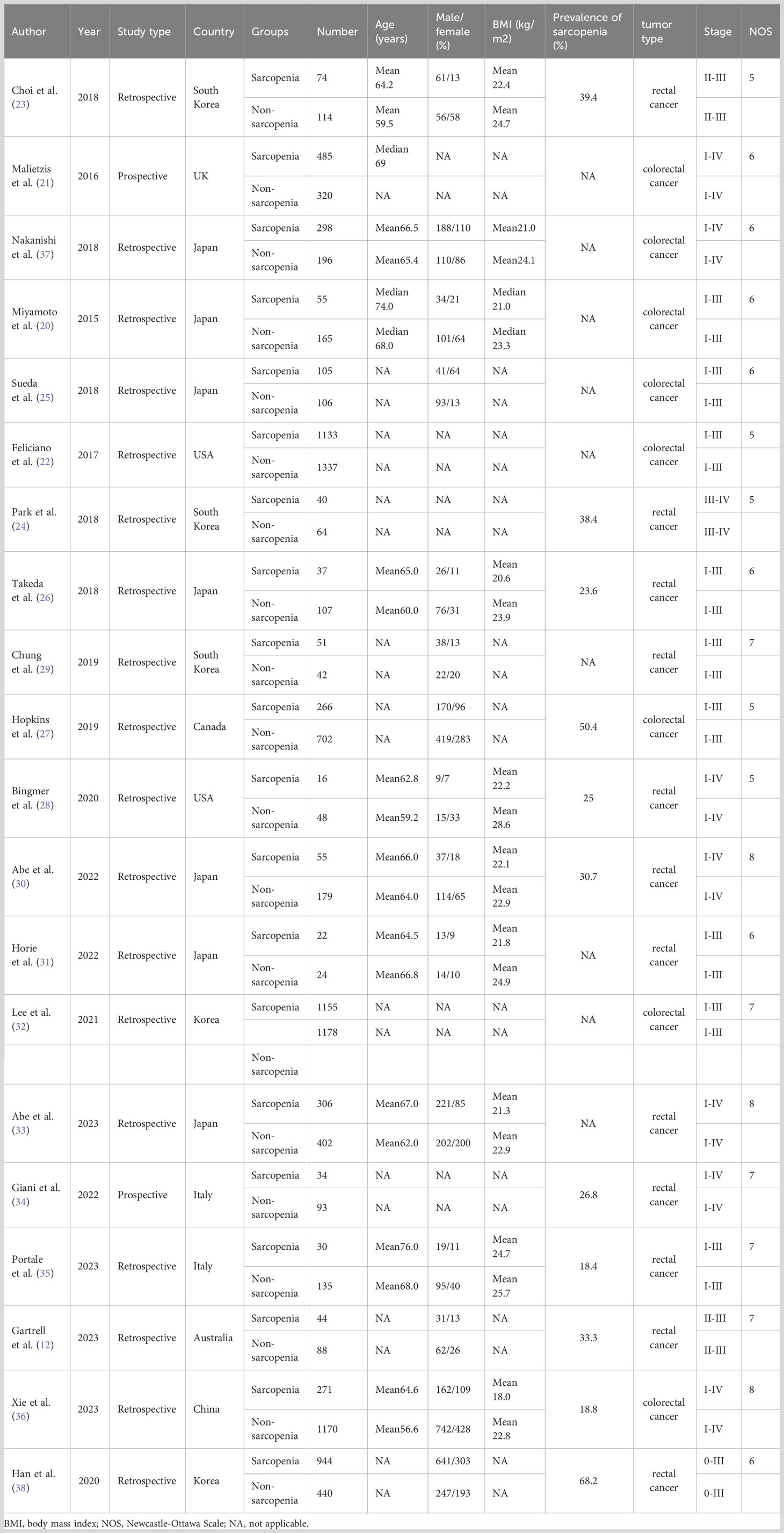
Table 1 Characteristics of included studies.
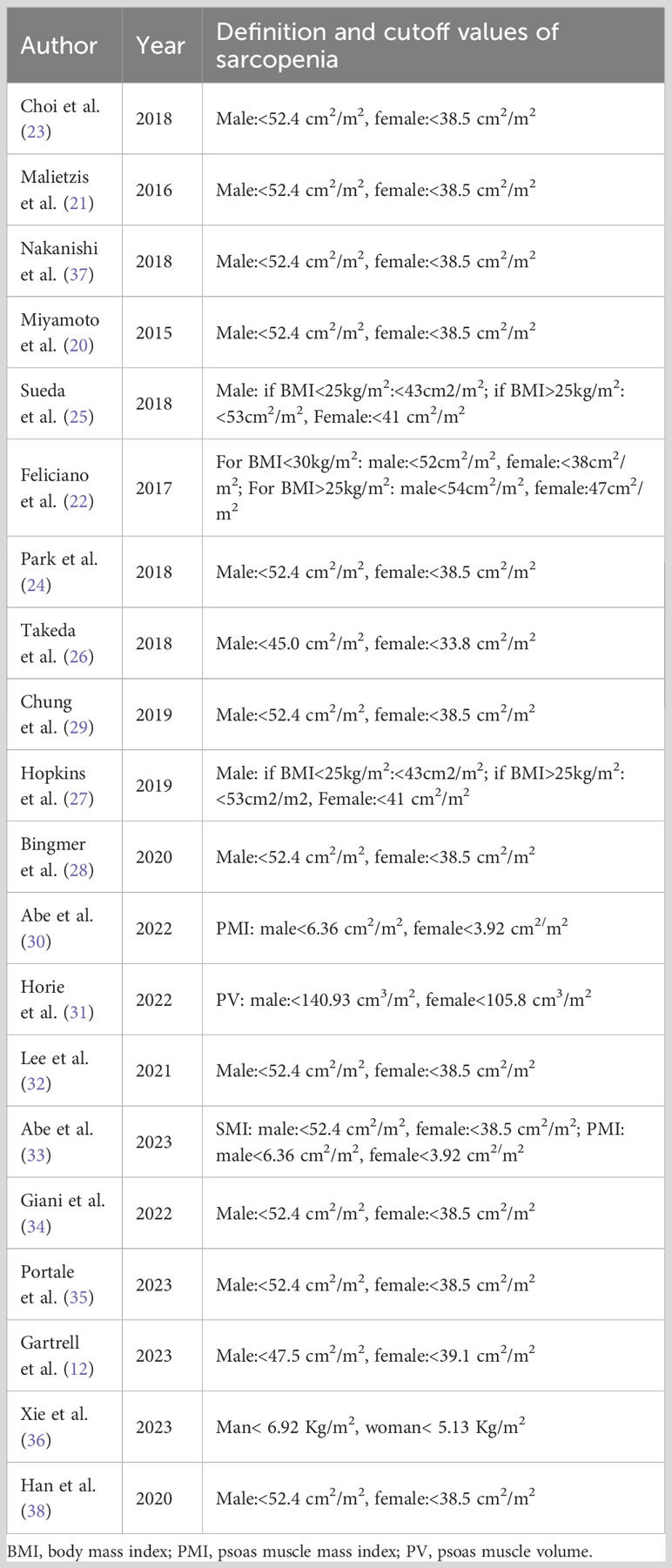
Table 2 Definition and cutoff values of sarcopenia measured by the third lumbar vertebra skeletal muscle index (L3SMI) in our included studies.
3.2 Prevalence of sarcopenia in patients with colorectal cancer
The meta-analysis of sarcopenia prevalence in colorectal cancer patients included 11 studies (Table 1), involving 4855 individuals overall, with sarcopenia present in 2018 individuals and absent in 2837. In this meta-analysis, the overall prevalence of sarcopenia was calculated in individuals with colorectal cancer to be 34% (95% CI=0.20-0.48, I2 = 99.1%, P<0.001) (Figure 2).
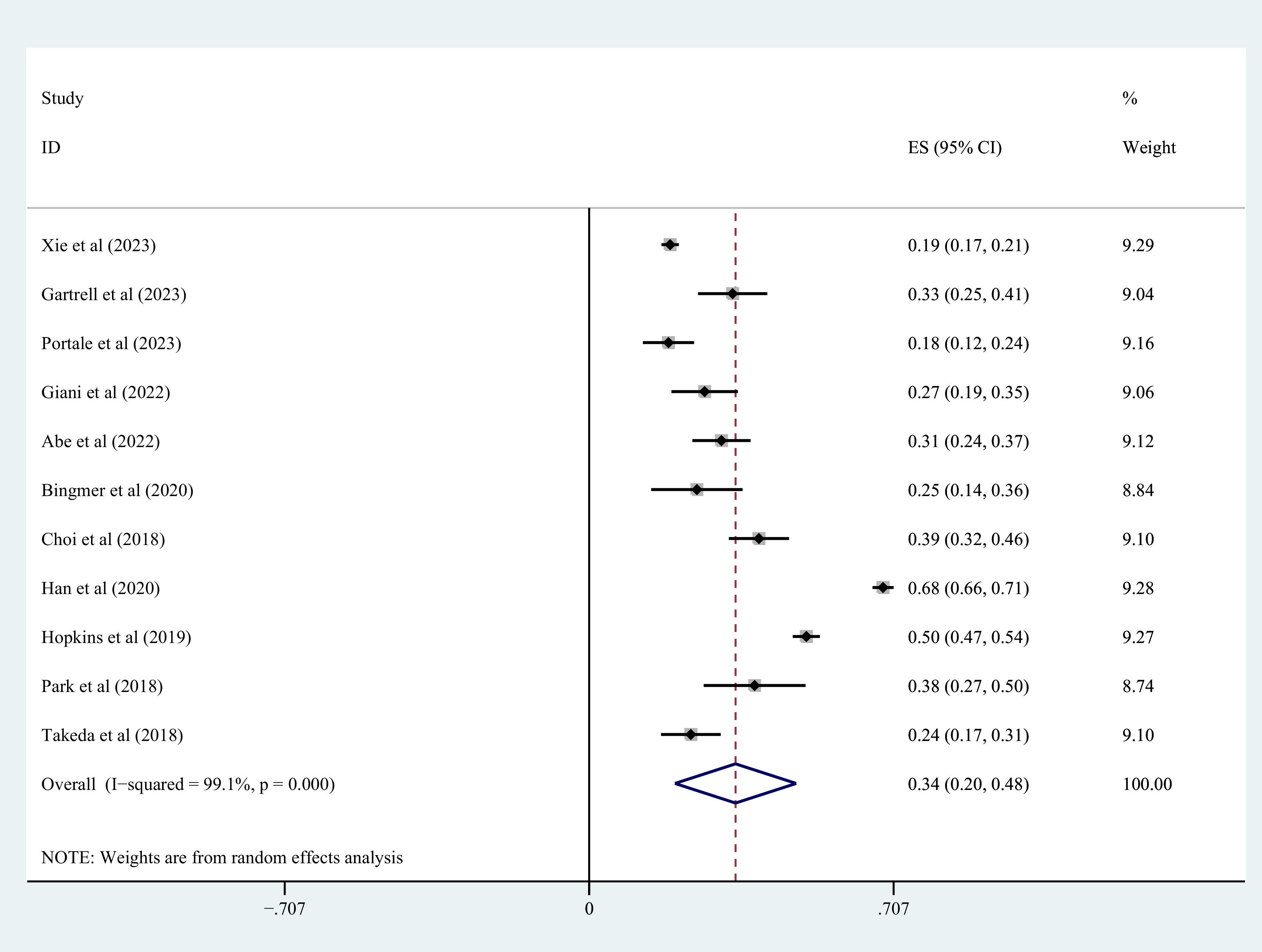
Figure 2 Incidence of sarcopenia in colorectal patients.
3.3 Overall analysis of survival outcomes
Nineteen studies contributed to the survival outcome data. The meta-analysis depicted lowered OS in the sarcopenia group in comparison with the negative-sarcopenia group (HR=1.72,95% CI=1.45-2.03), (Figure 3). Additionally, 12 studies contributed data for multivariate analysis of DFS, and five studies contributed toward multivariate analysis of CSS. The meta-analysis depicted that compared with individuals without sarcopenia, individuals with sarcopenia had notably diminished DFS and CSS (DFS: HR=1.42,95% CI=1.26-1.60; CSS: HR=1.48,95% CI=1.26-1.75) (all P<0.001), as exhibited in Figures 4, 5.
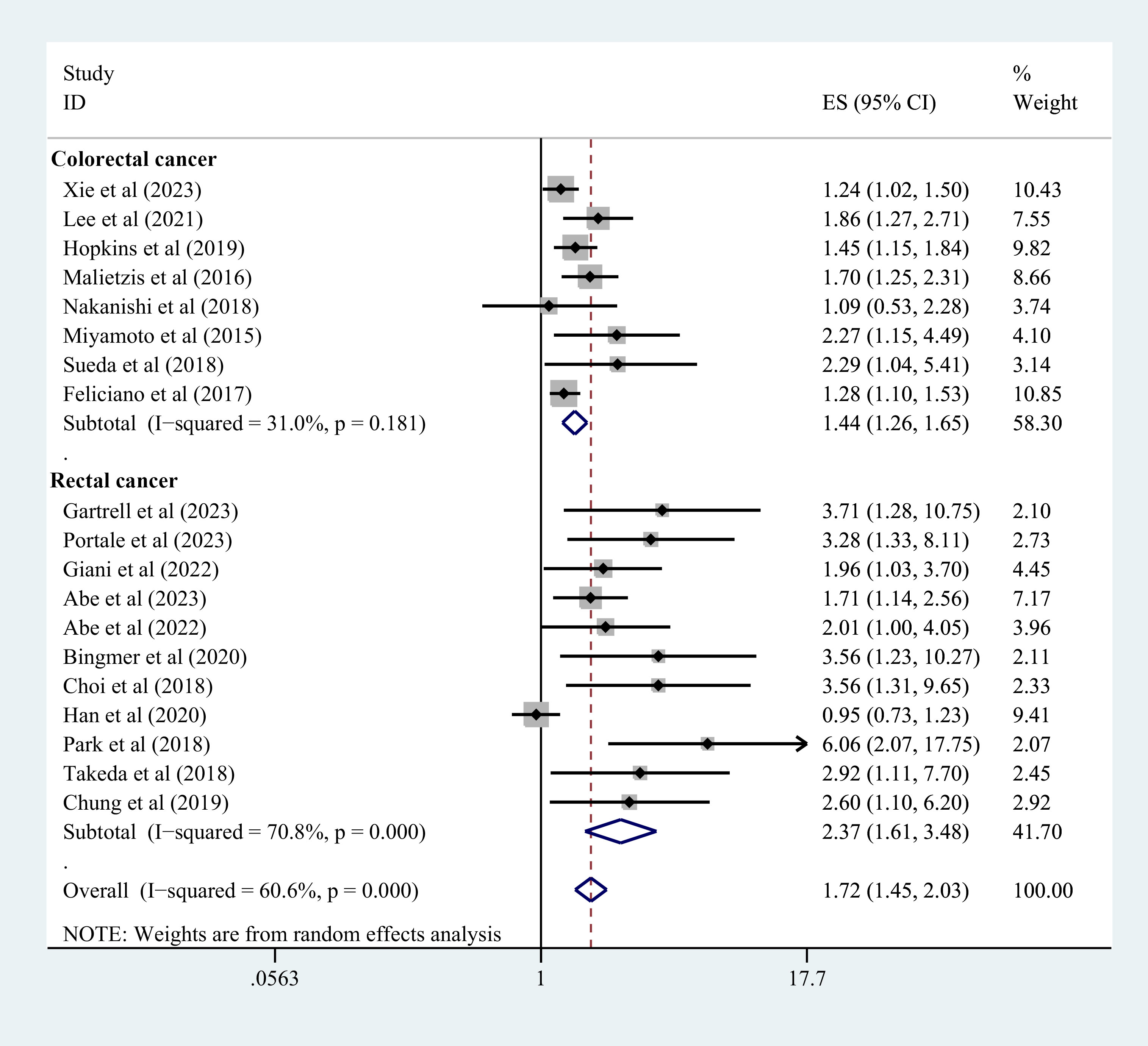
Figure 3 Forest plot of OS risk in colorectal cancer patients with and without sarcopenia. OS, overall survival.
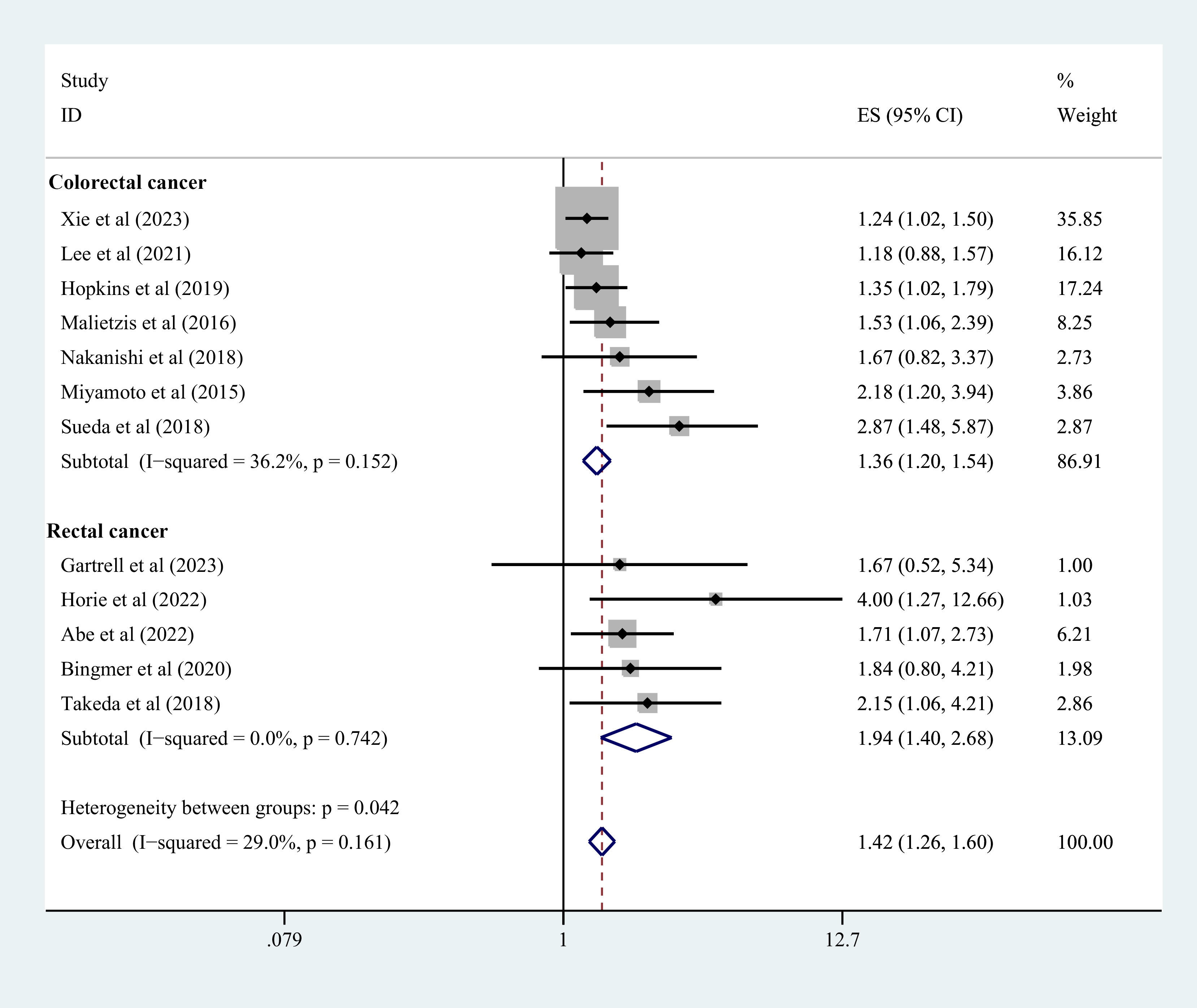
Figure 4 Forest plot of DFS risk in colorectal cancer patients with and without sarcopenia. DFS, disease-free survival.
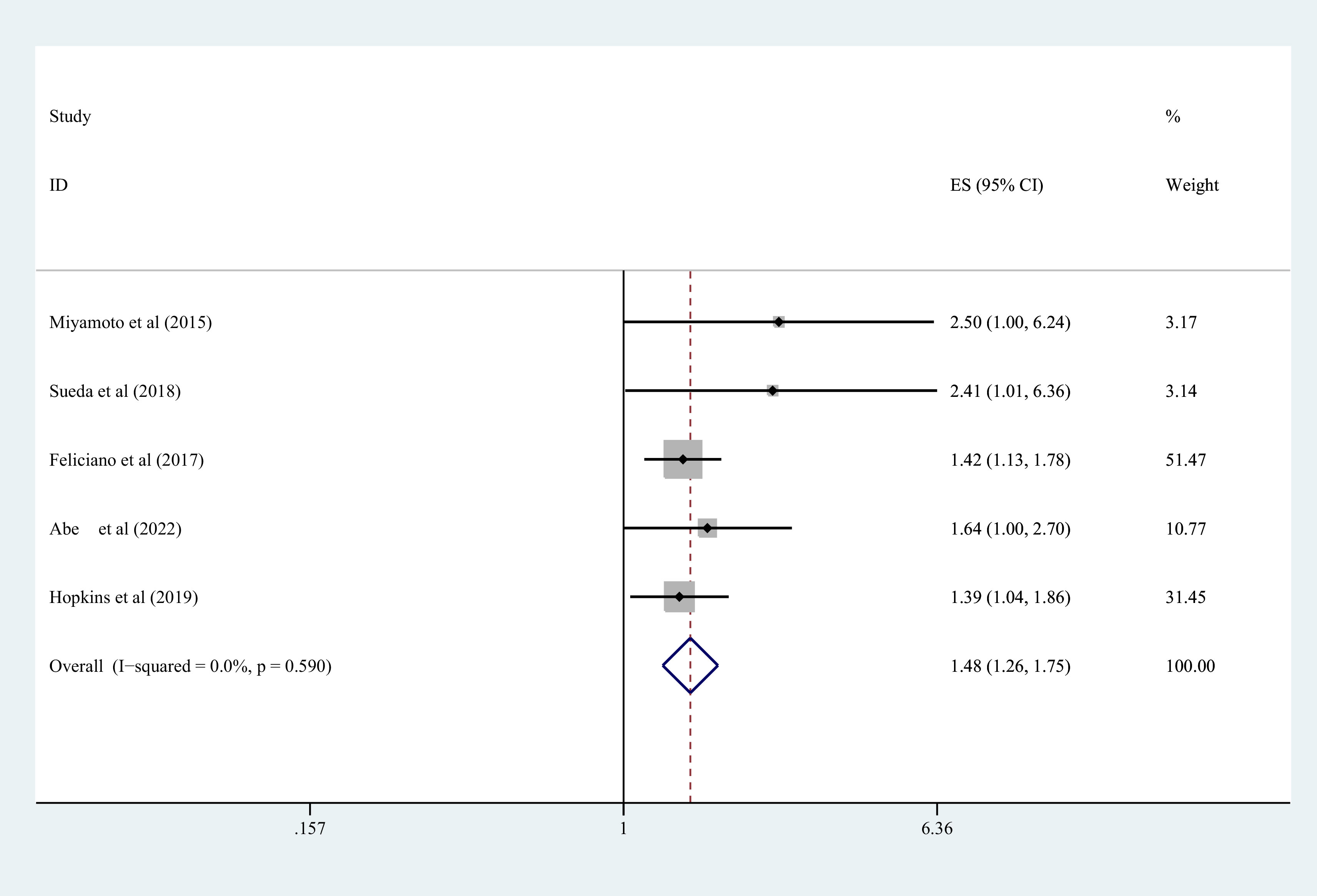
Figure 5 Forest plot of CSS risk in colorectal cancer patients with and without sarcopenia. CSS, cancer-specific survival.
3.4 Subgroup analysis
A subgroup analysis of OS and DFS per tumor type, ethnicity, study type, the total number of included samples, NOS score, and diagnostic criteria for sarcopenia was performed. The data indicated an interesting trend in the sarcopenia group of lower OS and DFS in different subgroups. Table 3 depicted the resulting data of the subgroup analysis in detail.
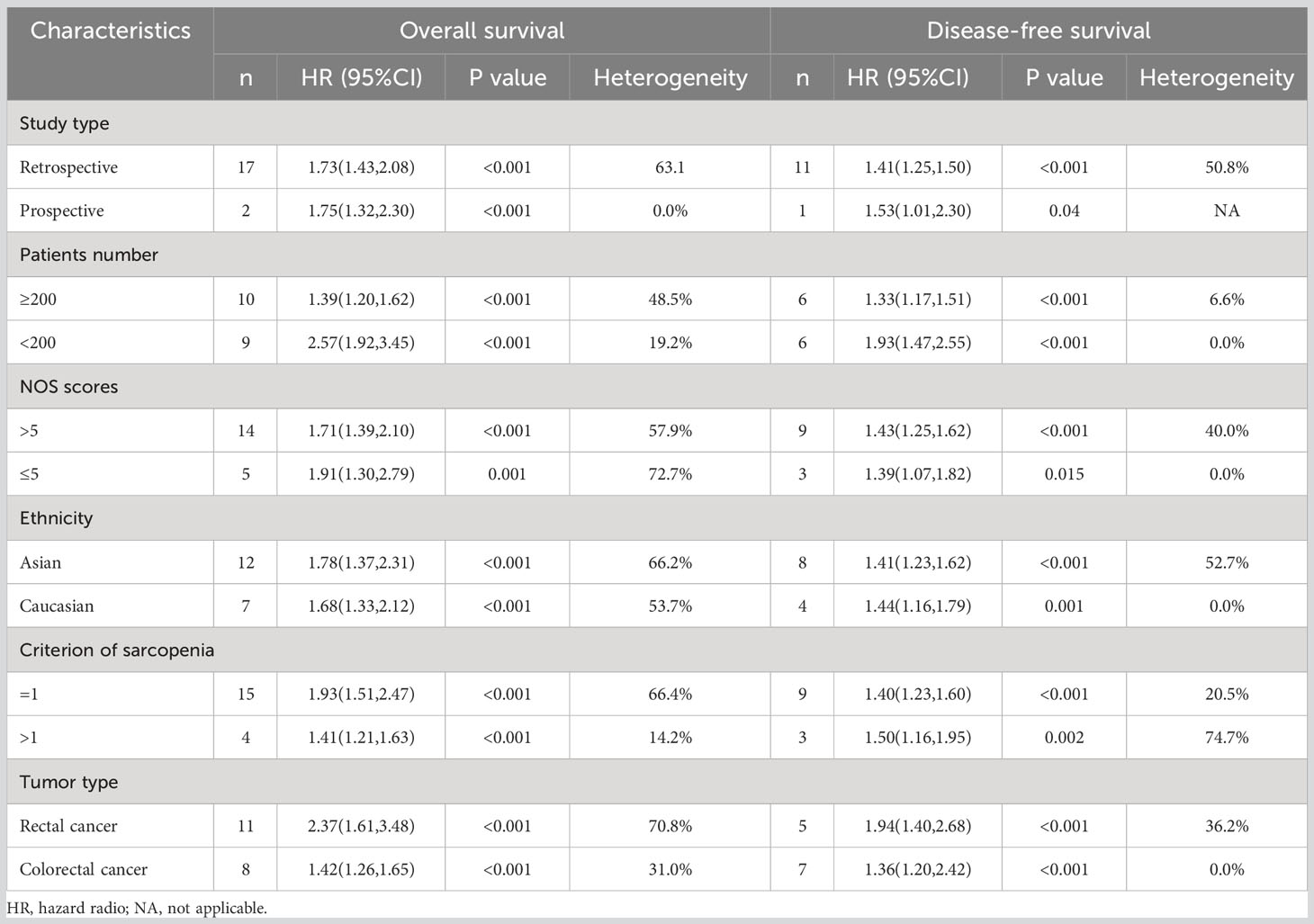
Table 3 Subgroup analyses in terms of overall survival and disease-free survival.
3.4.1 According to tumor type
Nine studies explicitly included patients with rectal cancer, and the data indicated that individuals with rectal cancer in the sarcopenia group depicted shorter OS (HR=1.78, 95%CI=1.37-2.31, P<0.001) (Figure 3) and shorter DFS (HR=1.89, 95%CI=1.53-2.33, P=0.002) (Figure 4). Three studies did not explicitly differentiate into rectal and colon cancer, and the data indicated that individuals with colorectal cancer in the sarcopenia group depicted shorter OS (HR=1.42,95% CI=1.17-1.74, P<0.001) (Figure 3) and shorter DFS (HR=1.92,95% CI=1.52-2.42, P=0.001) (Figure 4).
3.4.2 Analysis according to ethnic subgroups
The data depicted a shorter OS (HR=1.78,95%CI=1.37-2.31, P<0.001) in individuals with colorectal cancer in the sarcopenia group and a shorter DFS (HR=1.41,95%CI=1.23-1.62, P<0.001) in the Asian population. In the Caucasian population, individuals with colorectal cancer in the sarcopenia group also had shorter OS (HR=1.68, 95%CI=1.33-2.12, P<0.001) and shorter DFS (HR=1.44,95%CI=1.16-1.79, P=0.001) (Table 3).
3.4.3 Subgroup analysis per the type of study
There were two main types of studies included in the literature, that is, prospective study and retrospective study. In the prospective study, individuals with colorectal cancer in the sarcopenia group had shorter OS (HR=1.75,95% CI=1.32-2.30, P<0.001) and shorter DFS (HR=1.53,95% CI=1.02-2.30, P=0.04). Whereas in the retrospective study, these patients depicted shorter OS (HR= 1.73,95%CI=1.43-2.08, P<0.001) and shorter DFS (HR=1.41,95%CI=1.25-1.59, P<0.001) (Table 3).
3.4.4 Subgroup analysis according to the number of included samples
The data exhibited that individuals with colorectal cancer in the sarcopenia group had shorter OS (sample number >200: HR=1.39, 95%CI=1.20-1.62, P<0.001; sample number <200: HR=2.57, 95% CI=1.92-3.45, P < 0.001) and shorter DFS (sample number >200: HR=1.33, 95% CI=1.17-1.51, P < 0.001; sample number <200: HR=1.93,95% CI=1.47-2.55, P < 0.001) (Table 3).
3.4.5 Subgroup analysis according to NOS score
In studies with NOS scores greater than 5, individuals with colorectal cancer in the sarcopenia group all had shorter OS (HR=1.71,95%CI=1.39-2.10, P<0.001) and shorter DFS (HR=1.43,95%CI=1.25-1.62, P<0.001). Additionally, in studies with NOS scores less than or equal to 5, sarcopenia colorectal cancer patients all had shorter OS (HR=1.91,95%CI=1.30-2.79, P=0.001) and shorter DFS (HR=1.39, 95%CI=1.07-1.82, P=0.015) (Table 3).
3.4.6 The diagnostic criteria of sarcopenia
The resulting data depicted that sarcopenia colorectal cancer patients were linked with shorter OS (diagnostic criteria >1: HR=1.41,95% CI=1.21-1.63, P<0.001; diagnostic criteria=1: HR=1.93,95% CI=1.51-2.47, P<0.001) and shorter DFS regardless of which diagnostic criteria were followed (diagnostic criteria >1: HR =1.50,95% CI=1.16-1.95, P=0.002; diagnostic criteria=1: HR=1.40,95% CI=1.23-1.60, P<0.001) (Table 3).
3.5 Sensitivity analysis
The literature focusing on sarcopenia incidence, OS, DFS, and CCS was itemized and removed. Meta-analysis was executed on these remaining studies, and subsequent comparison of the resulting data between the remaining studies and the studies prior to exclusion was achieved. The comparison was indicative of the absence of any notable impact of itemized deletion of every study on the combined results. Figures 6A–D summarizes the sensitivity analysis of the meta-analysis for sarcopenia occurrence, OS, DFS, and CCS.
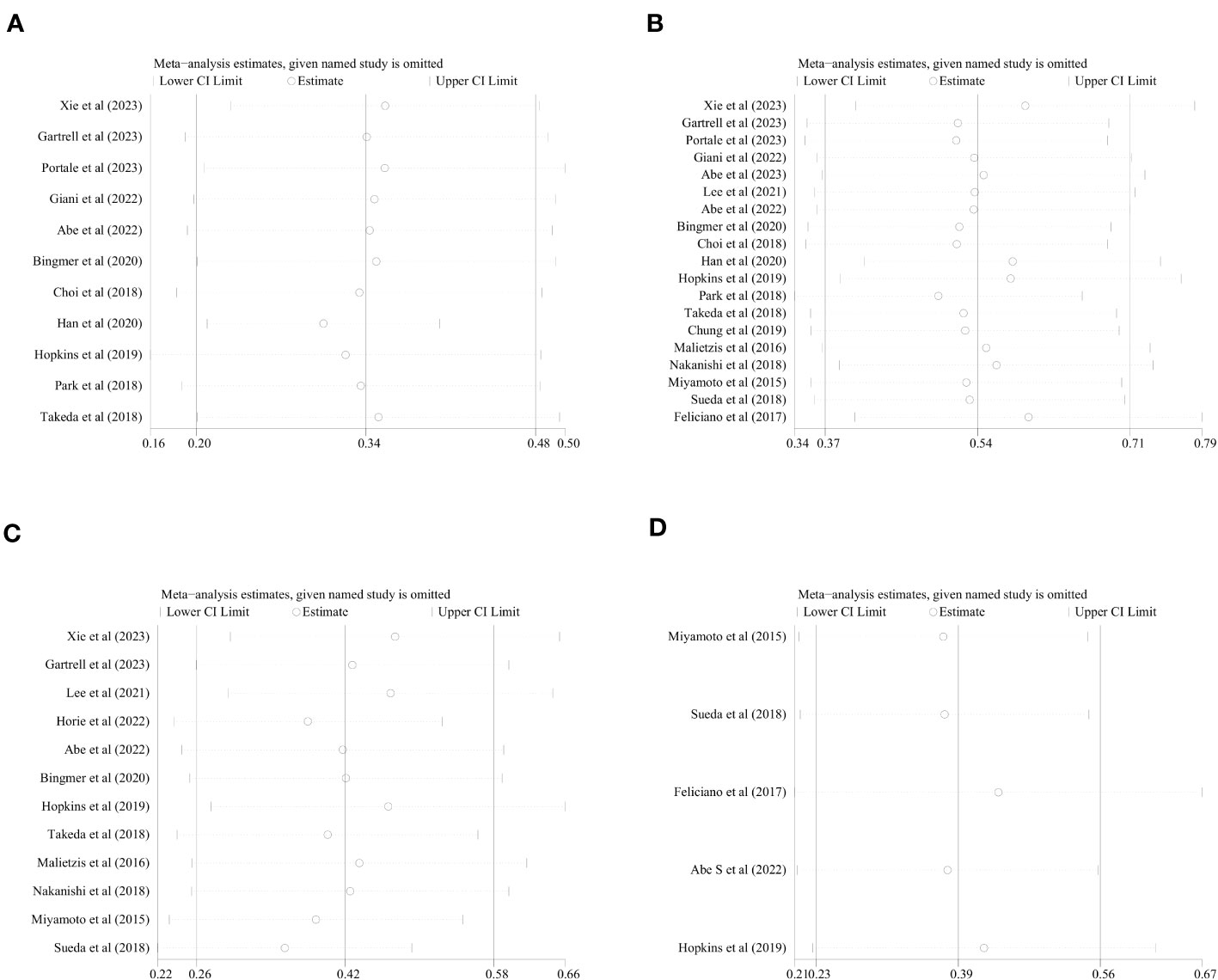
Figure 6 Sensitivity analysis of the meta-analysis. (A) incidence of sarcopenia, (B) OS, (C) DFS, (D) CSS.
3.6 Publication bias
Meanwhile, no publication bias was noted concerning the incidence of sarcopenia per the respective Begg’s and Egger’s tests (P=0.76, P=0.74), OS (P=1.00, P=0.54), DFS (P=0.06, P=0.05) and CCS (P=0.30, P=0.42) (Figures 7A–D).
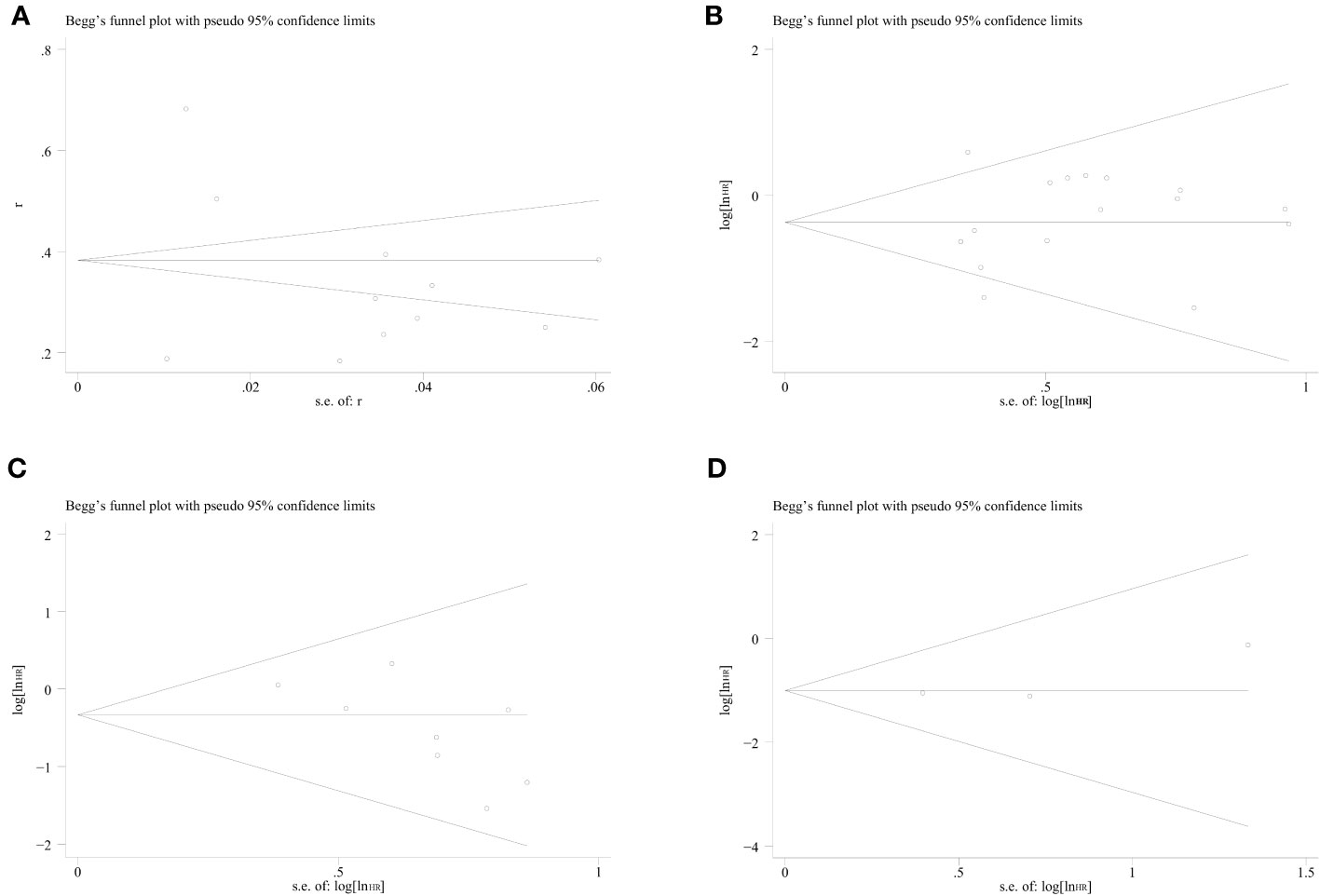
Figure 7 Funnel plots of sarcopenia incidence, OS, DFS, and CSS in colorectal cancer patients. (A) incidence of sarcopenia, (B) OS, (C) DFS, (D) CSS.
4 Discussion
This meta-analysis exhibited a relatively high incidence of sarcopenia in colorectal cancer (34%). In multivariate data, sarcopenia was linked with unfavorable OS, DFS, and CSS in individuals with colorectal cancer. This meta-analysis dealt with assessing the link between sarcopenia and OS, DFS, and CSS in individuals with colorectal cancer. The resulting data depicted congruence with the majority of prior observational studies. Hence, indicating a clinically meaningful relationship between sarcopenia and these survival parameters. The quality of evidence for the results of the multivariate analysis was considered reliable based on the NOS score.
In the past decade, research has increasingly demonstrated the predictive value of sarcopenia for the prognosis of cancer patients (39, 40). The occurrence of sarcopenia should not be neglected in clinical work-up, as the prevalence of sarcopenia in elderly individuals with cancer ranges from 12.5% to 57.7% (41). A meta-analysis depicted the presence of sarcopenia in 19%-39% of individuals with advanced colorectal cancer (42). Additionally, the proportion of colorectal cancer sarcopenia was as high as 34% in this study. This may be attributed to the fact that some of the patients included in the study received nCRT. Chemotherapy-related gastrointestinal reactions and radiotherapy-induced intestinal inflammation negatively affect the feeding habits and intestinal function of patients. These effects can result in reduced intake and impaired nutrient absorption, ultimately leading to weight loss and a high risk of malnutrition (43, 44). A study speculated upon the elements linked with sarcopenia prevalence in individuals with colorectal cancer. The resulting data of multivariate analysis determined that serum albumin, BMI, muscle wasting, and subjective overall patient scores were capable of independently predicting sarcopenia in individuals with colorectal cancer (45). Based on baseline data from our included studies (Table 1), individuals with sarcopenic colorectal cancer depicted a comparatively decreased BMI relative to non-sarcopenic patients. Therefore, variation in BMI could act as a clinical sign of early onset of sarcopenia in colorectal cancer patients. Diet and exercise are the two primary measures for preventing sarcopenia in individuals with cancer. Physical activity in such individuals is closely related to the maintenance of aerobic capacity and muscle strength (46). Hence, the proposal that appropriate nutritional supplementation and enhanced exercise can help improve the prognosis of colorectal cancer patients holds merit but needs to be verified in further clinical trials.
Cancer is the main factor contributing to the development of secondary sarcopenia. In current cancer research, sarcopenia diagnosis primarily relies on assessing decreased SMI, while fewer studies have evaluated muscle strength and physical performance (e.g., 4 m gait speed, 6 min walking test, and Time up and go test). To achieve more reliable conclusions, it is imperative to establish a more inclusive and comprehensive definition of sarcopenia. Since a CT scan is a routine method for the clinical staging of cancer patients, it is a practical technique for the assessment of body composition. The meta-analysis primarily explored the impact of sarcopenia on colorectal cancer prognosis, as a series of new studies have emerged in recent years and the conclusions may differ. In the 21 studies that were included, sarcopenia was measured by obtaining SMI values from CT scans of L3 levels, which is a common measure. The notion that it reduces heterogeneity and helps to draw relatively reliable conclusions may be plausible. These findings suggest that sarcopenia is negatively linked with the long-term prognosis of individuals with colorectal cancer. Additionally, research has exhibited that sarcopenia in individuals with cancer is linked with an elevated risk of cardiovascular disorders (47). Additionally, Nipp et al. (48) noted that sarcopenia influenced depression and quality of life in individuals with advanced cancer. Thus, the detrimental impact of sarcopenia highlights the significance of preventive measures and therapeutic interventions for sarcopenia among healthcare providers and individuals with cancer. To date, the reason for the negative association of sarcopenia with prognosis in individuals with colorectal cancer remains unclear. Abe S et al. (30) suggested that overall and grade 3 or higher variables of Common Terminology Criteria for Adverse Events were not increased in the post-chemoradiotherapy sarcopenic patients. However, Nakanishi et al. (37) thought that sarcopenia was significantly correlated with infections at locations other than surgical sites. Sun et al. observed that patients with sarcopenia showed a significant higher rate of incidence of postoperative infected when compared with non-sarcopenia patients by means of meta-analysis (17). A post-operative infection can affect long term survival. This may partly explain why patients with sarcopenia have worse prognosis. On the other hand, it can be speculated that systemic inflammation could possibly be one of the causes. The systemic inflammatory response severely affects muscle protein degradation metabolic processes and accelerates muscle wasting (49). Sarcopenia is indicative of an elevated catabolic state and is linked to a heightened inflammatory response following colorectal cancer surgery (50, 51). Moreover, the presence of both inflammation and sarcopenia contributes to a heightened risk of mortality (52). However, the precise mechanism needs further study.
This meta-analysis is limited in some aspects. Firstly, all the assessed studies used cut-off values of SMI to define sarcopenia. However, many studies did not address the assessment of muscle strength and fitness and should be supplemented with diagnostic criteria for sarcopenia according to EWGSOP. Second, the cut-off value of SMI was diverse across studies, which may be a source of heterogeneity. Moreover, neoadjuvant radiotherapy and nCRT are also vital elements affecting the prognosis of individuals with colorectal cancer. Nonetheless, the absence of comprehensive information and data based on neoadjuvant or adjuvant chemotherapy was noted in the studies assessed. Therefore, there is a possibility of these variables influencing the resulting data. Thus, future studies incorporating individual-level data are essential to validate our findings. Ultimately, we cannot perform a subgroup analysis based on the primary site of tumor occurrence, for example, rectal cancer, right hemicolectomy, or left hemicolectomy. Patients with colorectal cancer have different prognoses depending on the primary site. Though we designated the adjusted HR value as effect value, distant metastasis, lymph node metastases, involved surgical margin, lymph vascular invasion and histological grade were still dominant factors affecting survival time. The effect of sarcopenia on colorectal cancer should be framed in the context of former factors. Therefore, confounding baseline information may limit our ability to further explore the relevance of sarcopenia in colorectal cancer.
5 Conclusion
Sarcopenia is more prevalent in individuals with colorectal cancer. In such individuals, sarcopenia is independently linked with an unfavorable prognosis. Future studies need a comprehensive definition of sarcopenia to strengthen the evidence and further validate our conclusions.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
JH developed the research idea, performed data collection, performed data analysis, prepared the first manuscript draft, refined the research idea, and edit manuscript. WL, YH, YM, and LS validated data collection, developed the research idea, and proofread the article. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Sichuan Medical Research Project Foundation (S21054). Priming Scientific Research Foundation for the Introduced Talents of The First Affiliated Hospital of Chengdu Medical College (CYFY-GQ59).
Acknowledgments
We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Li L, Liu L, Kang H, Zhang L. The influence of predictive nursing on the emotions and self-management abilities of post-colostomy rectal cancer patients. Am J Transl Res (2021) 13:6543–51.
2. Tan Y, Shao R, Li J, Huang H, Wang Y, Zhang M, et al. PITPNC1 fuels radioresistance of rectal cancer by inhibiting reactive oxygen species production. Ann Transl Med (2020) 8:126. doi: 10.21037/atm.2020.02.37
3. Vuijk FA, van de Water C, Lent-van Vliet S, van der Valk MJM, Simmer F, van de Velde CJH, et al. Intra-tumoral genomic heterogeneity in rectal cancer: mutational status is dependent on preoperative biopsy depth and location. Cancers (Basel) (2021) 13:2271. doi: 10.3390/cancers13092271
4. Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med (2004) 351:1731–40. doi: 10.1056/NEJMoa040694
5. Ferlay J, Colombet M, Soerjomataram I, Dyba T, Randi G, Bettio M, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer (2018) 103:356–87. doi: 10.1016/j.ejca.2018.07.005
6. Jiang N, Zhang J, Cheng S, Liang B. The role of standardized phase angle in the assessment of nutritional status and clinical outcomes in cancer patients: A systematic review of the literature. Nutrients (2022) 15:50. doi: 10.3390/nu15010050
7. Derstine BA, Holcombe SA, Ross BE, Wang NC, Su GL, Wang SC. Optimal body size adjustment of L3 CT skeletal muscle area for sarcopenia assessment. Sci Rep (2021) 11:279. doi: 10.1038/s41598-020-79471-z
8. Gray C, MacGillivray TJ, Eeley C, Stephens NA, Beggs I, Fearon KC, et al. Magnetic resonance imaging with k-means clustering objectively measures whole muscle volume compartments in sarcopenia/cancer cachexia. Clin Nutr (2011) 30:106–11. doi: 10.1016/j.clnu.2010.07.012
9. Erul E, Guven DC, Onur MR, Yazici G, Aksoy S. Role of sarcopenia on survival and treatment-related toxicity in head and neck cancer: a narrative review of current evidence and future perspectives. Eur Arch Otorhinolaryngol (2023) 280:3541–56. doi: 10.1007/s00405-023-08014-9
10. Martinez-Tapia C, Rougette K, Fossey-Diaz V, Cudennec T, Taleb C, Balardy L, et al. Prevalence of four sarcopenia criteria in older patients with cancer, and their predictive value for 6-month mortality: the nutriAgeCancer national prospective cohort study. Nutrients (2023) 15:1508. doi: 10.3390/nu15061508
11. Yamanouchi K, Murakami S, Sato A, Ogawa S, Shinagawa H, Kamohara Y. Integrated evaluation of inflammatory, nutritional, and sarcopenia markers to predict survival in metastatic breast cancer patients. In Vivo (2023) 37:811–7. doi: 10.21873/invivo.13146
12. Gartrell R, Qiao J, Kiss N, Faragher I, Chan S, Baird PN, et al. Can sarcopenia predict survival in locally advanced rectal cancer patients? ANZ J Surg (2023) 93:2166–71. doi: 10.1111/ans.18512
13. Meyer HJ, Wienke A, Surov A. Sarcopenia as a prognostic marker for survival in gastric cancer patients undergoing palliative chemotherapy. A systematic review and meta analysis. Nutr Cancer (2022) 74:3518–26. doi: 10.1080/01635581.2022.2077387
14. Gan H, Lan J, Bei H, Xu G. The impact of sarcopenia on prognosis of patients with pancreatic cancer: A systematic review and meta-analysis. Scott Med J (2023), 14:369330231187655. doi: 10.1177/00369330231187655
15. Dong D, Shi JY, Shang X, Liu B, Xu WL, Cui GZ, et al. Prognostic significance of sarcopenia in patients with hepatocellular carcinoma treated with lenvatinib: a retrospective analysis. Med (Baltimore) (2022) 101:e28680. doi: 10.1097/MD.0000000000028680
16. Zhu Y, Guo X, Zhang Q, Yang Y. Prognostic value of sarcopenia in patients with rectal cancer: A meta-analysis. PloS One (2022) 17:e0270332. doi: 10.1371/journal.pone.0270332
17. Sun G, Li Y, Peng Y, Lu D, Zhang F, Cui X, et al. Can sarcopenia be a predictor of prognosis for patients with non-metastatic colorectal cancer? a systematic review and meta-analysis. Int J Colorectal Dis (2018) 33:1419–27. doi: 10.1007/s00384-018-3128-1
18. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ (2015) 350:g7647. doi: 10.1136/bmj.g7647
19. Hall R, Shaughnessy M, Boll G, Warner K, Boucher HW, Bannuru RR, et al. Drug use and postoperative mortality following valve surgery for infective endocarditis: A systematic review and meta-analysis. Clin Infect Dis (2019) 69:1120–9. doi: 10.1093/cid/ciy1064
20. Miyamoto Y, Baba Y, Sakamoto Y, Ohuchi M, Tokunaga R, Kurashige J, et al. Sarcopenia is a negative prognostic factor after curative resection of colorectal cancer. Ann Surg Oncol (2015) 22:2663–8. doi: 10.1245/s10434-014-4281-6
21. Malietzis G, Currie AC, Athanasiou T, Johns N, Anyamene N, Glynne-Jones R, et al. Influence of body composition profile on outcomes following colorectal cancer surgery. Br J Surg (2016) 103:572–80. doi: 10.1002/bjs.10075
22. Feliciano EMC, Kroenke CH, Meyerhardt JA, Prado CM, Bradshaw PT, Kwan ML, et al. Association of systemic inflammation and sarcopenia with survival in nonmetastatic colorectal cancer: results from the C SCANS study. JAMA Oncol (2017) 3:e172319. doi: 10.1001/jamaoncol.2017.2319
23. Choi MH, Oh SN, Lee IK, Oh ST, Won DD. Sarcopenia is negatively associated with long-term outcomes in locally advanced rectal cancer. J Cachexia Sarcopenia Muscle (2018) 9:53–9. doi: 10.1002/jcsm.12234
24. Park SE, Hwang IG, Choi CH, Kang H, Kim BG, Park BK, et al. Sarcopenia is poor prognostic factor in older patients with locally advanced rectal cancer who received preoperative or postoperative chemoradiotherapy. Med (Baltimore) (2018) 97:e13363. doi: 10.1097/MD.0000000000013363
25. Sueda T, Takahasi H, Nishimura J, Hata T, Matsuda C, Mizushima T, et al. Impact of low muscularity and myosteatosis on long-term outcome after curative colorectal cancer surgery: A propensity score-matched analysis. Dis Colon Rectum (2018) 61:364–74. doi: 10.1097/DCR.0000000000000958
26. Takeda Y, Akiyoshi T, Matsueda K, Fukuoka H, Ogura A, Miki H, et al. Skeletal muscle loss is an independent negative prognostic factor in patients with advanced lower rectal cancer treated with neoadjuvant chemoradiotherapy. PloS One (2018) 13:e0195406. doi: 10.1371/journal.pone.0195406
27. Hopkins JJ, Reif RL, Bigam DL, Baracos VE, Eurich DT, Sawyer MB. The impact of muscle and adipose tissue on long-term survival in patients with stage I to III colorectal cancer. Dis Colon Rectum (2019) 62:549–60. doi: 10.1097/DCR.0000000000001352
28. Bingmer K, Kondray V, Ofshteyn A, Bliggenstorfer JT, Dietz DW, Charles R, et al. Sarcopenia is associated with worse overall survival in patients with anal squamous cell cancer. J Surg Oncol (2020) 121:1148–53. doi: 10.1002/jso.25887
29. Chung E, Lee HS, Cho ES, Park EJ, Baik SH, Lee KY, et al. Prognostic significance of sarcopenia and skeletal muscle mass change during preoperative chemoradiotherapy in locally advanced rectal cancer. Clin Nutr (2020) 39:820–8. doi: 10.1016/j.clnu.2019.03.014
30. Abe S, Kawai K, Nozawa H, Sasaki K, Murono K, Emoto S, et al. Preoperative sarcopenia is a poor prognostic factor in lower rectal cancer patients undergoing neoadjuvant chemoradiotherapy: a retrospective study. Int J Clin Oncol (2022) 27:141–53. doi: 10.1007/s10147-021-02062-z
31. Horie K, Matsuda T, Yamashita K, Hasegawa H, Utsumi M, Urakawa N, et al. Sarcopenia assessed by skeletal muscle mass volume is a prognostic factor for oncological outcomes of rectal cancer patients undergoing neoadjuvant chemoradiotherapy followed by surgery. Eur J Surg Oncol (2022) 48:850–6. doi: 10.1016/j.ejso.2021.10.018
32. Lee C, Park IJ, Kim KW, Shin Y, Lim SB, Kim CW, et al. Influence of postoperative changes in sarcopenia on long-term survival in non-metastatic colorectal cancer patients. Cancers (Basel) (2021) 13:2410. doi: 10.3390/cancers13102410
33. Abe S, Nozawa H, Sasaki K, Murono K, Emoto S, Yokoyama Y, et al. Sarcopenia is associated with oncological prognosis and the incidence of secondary cancer in patients with middle/lower rectal cancer. Clin Colorectal Cancer (2023) 22:143–52. doi: 10.1016/j.clcc.2022.10.001
34. Giani A, Famularo S, Fogliati A, Riva L, Tamini N, Ippolito D, et al. Skeletal muscle wasting and long-term prognosis in patients undergoing rectal cancer surgery without neoadjuvant therapy. World J Surg Oncol (2022) 20:51. doi: 10.1186/s12957-021-02460-7
35. Portale G, Zuin M, Spolverato YC, Bartolotta P, Gregori D, Rettore C, et al. Prognostic effect of sarcopenia in patients undergoing laparoscopic rectal cancer resection. ANZ J Surg (2023) 93:1631–7. doi: 10.1111/ans.18269
36. Xie H, Wei L, Gao S, Liu M, Liang Y, Yuan G, et al. Prognostic significance of sarcopenia diagnosed based on the anthropometric equation for progression-free survival and overall survival in patients with colorectal cancer. Front Nutr (2023) 10:1076589. doi: 10.3389/fnut.2023.1076589
37. Nakanishi R, Oki E, Sasaki S, Hirose K, Jogo T, Edahiro K, et al. Sarcopenia is an independent predictor of complications after colorectal cancer surgery. Surg Today (2018) 48:151–7. doi: 10.1007/s00595-017-1564-0
38. Han JS, Ryu H, Park IJ, Kim KW, Shin Y, Kim SO, et al. Association of body composition with long-term survival in non-metastatic rectal cancer patients. Cancer Res Treat (2020) 52:563–72. doi: 10.4143/crt.2019.249
39. Anker MS, Lena A, Roeland EJ, Porthun J, Schmitz S, Hadzibegovic S, et al. Patient-reported ability to walk 4 m and to wash: New clinical endpoints and predictors of survival in patients with pre-terminal cancer. J Cachexia Sarcopenia Muscle (2023) 14:1670–81. doi: 10.1002/jcsm.13247
40. Detopoulou P, Voulgaridou G, Papadopoulou S. Cancer, phase angle and sarcopenia: the role of diet in connection with lung cancer prognosis. Lung (2022) 200:347–79. doi: 10.1007/s00408-022-00536-z
41. Dunne RF, Loh KP, Williams GR, Jatoi A, Mustian KM, Mohile SG, et al. Cachexia and sarcopenia in older adults with cancer: A comprehensive review. Cancers (Basel) (2019) 11:1861. doi: 10.3390/cancers11121861
42. Shachar SS, Williams GR, Muss HB, Nishijima TF. Prognostic value of sarcopenia in adults with solid tumours: A meta-analysis and systematic review. Eur J Cancer (2016) 57:58–67. doi: 10.1016/j.ejca.2015.12.030
43. Abe S, Nozawa H, Kawai K, Sasaki K, Murono K, Emoto S, et al. Poor nutrition and sarcopenia are related to systemic inflammatory response in patients with rectal cancer undergoing preoperative chemoradiotherapy. Int J Colorectal Dis (2022) 37:189–200. doi: 10.1007/s00384-021-04039-w
44. Okugawa Y, Toiyama Y, Oki S, Ide S, Yamamoto A, Ichikawa T, et al. Feasibility of assessing prognostic nutrition index in patients with rectal cancer who receive preoperative chemoradiotherapy. JPEN J Parenter Enteral Nutr (2018) 42:998–1007. doi: 10.1002/jpen.1041
45. Souza BU, Souza NCS, Martucci RB, Rodrigues VD, Pinho NB, Gonzalez MC, et al. Factors associated with sarcopenia in patients with colorectal cancer. Nutr Cancer (2018) 70:176–83. doi: 10.1080/01635581.2018.1412480
46. Suderman K, Skene T, Sellar C, Dolgoy N, Pituskin E, Joy AA, et al. Virtual or in-person: A mixed methods survey to determine exercise programming preferences during COVID-19. Curr Oncol (2022) 29:6735–48. doi: 10.3390/curroncol29100529
47. Lee SJ, Park YJ, Cartmell KB. Sarcopenia in cancer survivors is associated with increased cardiovascular disease risk. Support Care Cancer (2018) 26:2313–21. doi: 10.1007/s00520-018-4083-7
48. Nipp RD, Fuchs G, El-Jawahri A, Mario J, Troschel FM, Greer JA, et al. Sarcopenia is associated with quality of life and depression in patients with advanced cancer. Oncologist (2018) 23:97–104. doi: 10.1634/theoncologist.2017-0255
49. Argiles JM, Busquets S, Felipe A, Lopez-Soriano FJ. Molecular mechanisms involved in muscle wasting in cancer and ageing: cachexia versus sarcopenia. Int J Biochem Cell Biol (2005) 37:1084–104. doi: 10.1016/j.biocel.2004.10.003
50. Reisinger KW, van Vugt JL, Tegels JJ, Snijders C, Hulsewe KW, Hoofwijk AG, et al. Functional compromise reflected by sarcopenia, frailty, and nutritional depletion predicts adverse postoperative outcome after colorectal cancer surgery. Ann Surg (2015) 261:345–52. doi: 10.1097/SLA.0000000000000628
51. Reisinger KW, Derikx JP, van Vugt JL, Von Meyenfeldt MF, Hulsewe KW, Olde Damink SW, et al. Sarcopenia is associated with an increased inflammatory response to surgery in colorectal cancer. Clin Nutr (2016) 35:924–7. doi: 10.1016/j.clnu.2015.07.005
Keywords: sarcopenia, skeletal muscle mass, colorectal cancer, prognosis, meta-analysis
Citation: He J, Luo W, Huang Y, Song L and Mei Y (2023) Sarcopenia as a prognostic indicator in colorectal cancer: an updated meta-analysis. Front. Oncol. 13:1247341. doi: 10.3389/fonc.2023.1247341
Received: 25 June 2023; Accepted: 09 October 2023;
Published: 27 October 2023.
Edited by:
Antonio Mario Scanu, University of Sassari, ItalyReviewed by:
Paolo Mercantini, Sapienza University of Rome, ItalyJenny Georgina Turcott, National Institute of Cancerology (INCAN), Mexico
Copyright © 2023 He, Luo, Huang, Song and Mei. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie He, MTM1NDAyNDY5NzRAMTYzLmNvbQ==
†These authors have contributed equally to this work